 Yanan Xu
Yanan Xu Haijing Guan
Haijing Guan Kefu Yu
Kefu Yu Nan Ji
Nan Ji Zhigang Zhao
Zhigang Zhao- 1Department of Pharmacy, Beijing Tiantan Hospital, Capital Medical University, Beijing, China
- 2School of Pharmacy, Capital Medical University, Beijing, China
- 3Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, China
Objective: To compare the efficacy and safety of treatments for patients with recurrent high-grade gliomas.
Methods: Electronic databases including Pubmed, Embase, Cochrane Library and ClinicalTrials.gov were searched for randomized controlled trials (RCT) related to high-grade gliomas. The inclusion of qualified literature and extraction of data were conducted by two independent reviewers. The primary clinical outcome measures of network meta-analysis were overall survival (OS) while progression-free survival (PFS), objective response rate (ORR) and adverse event of grade 3 or higher were secondary measures.
Results: 22 eligible trials were included in the systematic review, involving 3423 patients and 30 treatment regimens. Network meta-analysis included 11 treatments of 10 trials for OS and PFS, 10 treatments of 8 trials for ORR, and 8 treatments of 7 trials for adverse event grade 3 or higher. Regorafenib showed significant benefits in terms of OS in paired comparison with several treatments such as bevacizumab (hazard ratio (HR), 0.39; 95% confidence interval (CI), 0.21–0.73), bevacizumab plus carboplatin (HR, 0.33; 95%CI, 0.16–0.68), bevacizumab plus dasatinib (HR, 0.44; 95%CI, 0.21–0.93), bevacizumab plus irinotecan (HR, 0.4; 95%CI, 0.21–0.74), bevacizumab plus lomustine (90 mg/m2) (HR, 0.53; 95%CI, 0.33–0.84), bevacizumab plus lomustine (110 mg/m2) (HR, 0.21; 95%CI, 0.06–0.7), bevacizumab plus vorinostat (HR, 0.42; 95%CI, 0.18–0.99), lomustine (HR, 0.5; 95%CI, 0.33–0.76), and nivolumab (HR, 0.38; 95%CI, 0.19–0.73). For PFS, only the hazard ratio between bevacizumab plus vorinostat and bevacizumab plus lomustine (90 mg/m2) was significant (HR,0.51; 95%CI, 0.27–0.95). Lomustine and nivolumab conferred worse ORR. Safety analysis showed fotemustine as the best and bevacizumab plus temozolomide as the worst.
Conclusion: The results suggested that regorafenib and bevacizumab plus lomustine (90 mg/m2) provide improvements in terms of survival but may have poor ORR in patients with recurrent high-grade glioma.
Introduction
According to the latest criteria of World Health Organization classification in 2021 (Louis et al., 2021), high-grade gliomas encompass various types, including grade 3 and 4 astrocytoma, grade 3 oligodendroglioma, and grade 4 glioblastomas (GBM), with GBM being the most common. Despite the fact that high-grade gliomas account for approximately 25% of all brain tumors, they are characterized by high aggression and malignancy, with an inevitable tendency for recurrence (Ostrom et al., 2018). The median progression-free survival (PFS) after recurrence is only 1.8 months (McKinnon et al., 2021), and the median overall survival (OS) ranges between 7.1 and 9.8 months, with a 5-year survival rate of only about 5% (Ostrom et al., 2018).
Surgical resection remains a viable option for treating recurrent high-grade gliomas, particularly in the case of symptomatic or large lesions. Nonetheless, successful outcomes are largely dependent on complete resection (Wen et al., 2020). Due to the extensive and invasive nature of tumor tissue, often infiltrating into healthy surrounding tissue, the success rate of re-operation is limited by factors such as tumor location and structural complexities (Ma et al., 2021).
In cases where radiotherapy is repeated, careful consideration must be given to variables such as the initial radiation dose, time interval since treatment, and the location and volume of the recurrent tumor (Cabrera et al., 2016). However, there are few randomized trials to definitively prove whether radiotherapy prolongs survival time (Wen et al., 2020).
Alternatively, drug therapies have relatively fewer limitations and are often the primary choice for relapsed patients. The drugs currently available for high-grade glioma include bevacizumab, lomustine, temozolomide, regorafenib, PCV (procarbazine, lomustine, and vincristine), and relative drug combinations. However, the clinical benefit of these therapies is limited, as evidenced by the results of numerous clinical trials (Nabors et al., 2020; Weller et al., 2021). With the abundance of clinical trials with inconclusive results (Omuro and DeAngelis, 2013), it becomes perplexing for clinicians to make informed decisions. Therefore, performing a network meta-analysis that compares treatments from varying clinical trials becomes pivotal.
An analysis focusing on recurrent GBM has been previously conducted, (McBain et al., 2021), while it lacked a collection of evidence on grade 3 glioma treatment. Furthermore, fresh clinical study outcomes have emerged that necessitate evaluation. Hence, we performed this systematic review and Bayesian network meta-analysis to amass and summarize the treatment evidence for both grade 3 and 4 gliomas. Additionally, we reconstruct data from published Kaplan-Meier survival curves to include as much clinical evidence as possible and enable comprehensive results. The results of direct and indirect comparisons were integrated to evaluate the efficacy and safety of various drug therapies. We also ranked the clinical measures of each therapeutic regimen to provide a comprehensive assessment for clinical decision-making and to improve prognosis for patients experiencing tumor recurrence.
Methods
This study was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement (Supplementary Table S1) (Page et al., 2021). The protocol was registered with the international prospective register of systematic reviews (PROSPERO CRD42022383881).
Data sources and search strategy
A thorough search of PubMed, Embase, Cochrane Central Register, China National Knowledge Infrastructure, WanFang Data Knowledge Service Platform and China Science and Technology Journal Database was conducted for published randomized controlled trials (RCTs) with the inclusion of an additional search of ClinicalTrials.gov for unpublished RCTs. The search terms included “high-grade gliomas,” “anaplastic astrocytoma,” “glioblastoma,” “anaplastic oligoastrocytoma,” “recurren*,“ “relapse,” and drug names. Details of the literature search strategy can be found in Supplementary Table S2, with the search results collected up until 3 August 2022. The listing status of drugs was confirmed through the U.S. Food and Drug Administration (FDA) and drug-approval agencies in other countries.
Selection criteria
RCTs were included based on the following criteria:
1) Adult patients (≥18 years) with histologically confirmed recurrent high-grade gliomas, including GBM and anaplastic gliomas.
2) Trials that compared two or more arms of drug therapies, such as chemotherapy, immunotherapy and targeted therapy.
3) Trials that reported at least one of the following outcomes:
(i) OS, defined as the time from randomization to death;
(ii) PFS, defined as the time from randomization to first progression (local or distant) or death;
(iii) Objective response rate (ORR), defined as the proportion of patients achieving an objective response;
(iv) The incidence of grade 3 or higher adverse events (AE), determined according to the common terminology criteria for adverse events.
Duplicate studies and trials that were terminated or closed, along with trials in which drugs had not been approved for marketing by any nation were excluded. Furthermore, study arms that included operation or radiotherapy were disallowed.
Xu and Guan independently excluded irrelevant results by screening titles and abstracts, and included eligible articles by browsing through full texts. Any divergences during selection were resolved through arbitration by all reviewers.
Data extraction and quality evaluation
The details of the included articles were extracted to a pre-designed form, including publication information (title, first author, year of publication, journal of publication, country, etc.), trial information (trial start and cut-off time, disease, patient inclusion criteria, number of enrolled patients, baseline characteristics of the population, follow-up time), treatment regimens, and outcomes. If the OS and PFS were incomplete, missing data were estimated based on Kaplan-Meier curves following the methods provided by Tierney et al. (2007).
The Cochrane Risk of Bias 2 tool (Cumpston et al., 2019) assessed the individual study’s risk of bias in five areas: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome and selection of the reported result. Trials were categorized as low risk, high risk, or unclear concern of bias based on the above criteria.
Data extraction was conducted by Xu and Guan, and quality evaluation was conducted independently by Xu and Yu. Any discrepancies that emerged during the evaluation process were resolved through consensus among all reviewers.
Data synthesis and statistical analysis
The primary study outcome in this study was OS, with secondary outcomes being PFS, ORR, and grade 3 or higher AE. Survival data were presented as the hazard ratio (HR) with corresponding 95% confidence interval (CI), while categorical variables were expressed as the odds ratio (OR) with corresponding 95% CI.
Bayesian network meta-analysis was conducted due to its adaptability with complicated situations and its ability to explain the effects of study-specific covariates, leading to accurate estimates with limited information. Additionally, it provides a straightforward approach to carry out probabilistic statements and treatment effect predictions (Salanti et al., 2011). Network diagrams were generated for different treatment outcomes using Stata (version 17) (Chaimani et al., 2013). Fixed-effects and random-effects models were established separately through a Markov Chain Monte Carlo simulation technique in R (version 4.2.2) with 150000 iterations, 30000 burn-ins and a thinning interval of 1, based on the Bayesian framework (Salanti et al., 2011). The final appropriate analytical model was chosen based on the model parameters. Convergence was assessed through visual inspection of trace plots, density plots and Brooks-Gelman Rubin diagnosis plots (Supplementary Figure S1). Heterogeneity was evaluated using I2 statistics, with values categorized as low, medium and high heterogeneity for I2 values < 25%, 25%–50% and >50%, respectively, (Higgins et al., 2003). Global consistency was assessed by comparing the consistent and inconsistent models (Dias et al., 2010). The inconsistency of the models was assessed using the node splitting method (Higgins et al., 2003). Probability plots and surface under the cumulative ranking curve (SUCRA) were used to predict and evaluate the efficacy and safety of each treatment.
A sensitivity analysis was conducted to evaluate the reliability and stability of network meta-analysis results, with articles causing greater heterogeneity excluded for sensitive analysis.
Results
Systematic review and characteristics
In this study, a total of 104 out of 4933 records for full-text reading and 22 RCTs (Boiardi et al., 1992; Yung et al., 2000; Friedman et al., 2009; Brada et al., 2010; Dresemann et al., 2010; Song et al., 2010; Sun et al., 2013; Taal et al., 2014; Field et al., 2015; Reardon et al., 2015; Brandes et al., 2016; Gilbert et al., 2017; Wick et al., 2017; Duerinck et al., 2018; Brandes et al., 2019; Galanis et al., 2019; Lombardi et al., 2019; Puduvalli et al., 2020; Reardon et al., 2020; Nayak et al., 2021; Twelves et al., 2021; Patil et al., 2022) were included for analysis (Figure 1). The study population consisted of 3423 patients who received 30 different treatments. Bevacizumab, lomustine and temozolomide were the most commonly studied. The characteristics of the tumor types, number of tumor recurrences, sex ratio, age, Karnofsky performance status (KPS), and specific treatment regimens were summarized in Table 1. The risk of bias assessment in the literature was evaluated and presented in Supplementary Figure S2.

FIGURE 1. Study selection.
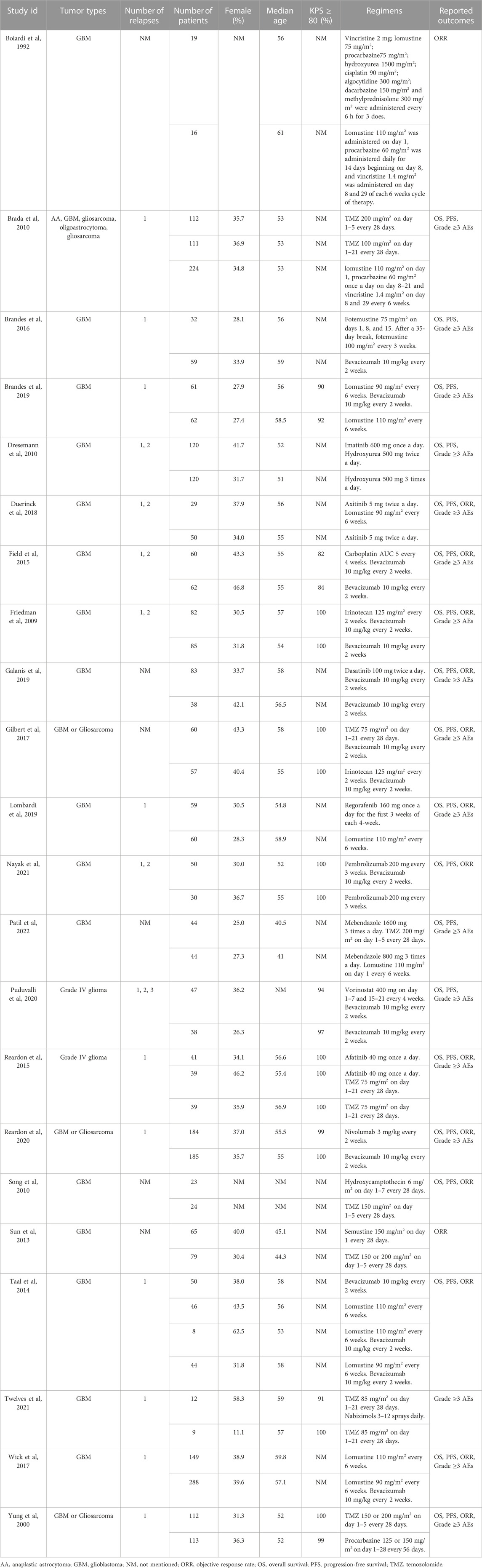
TABLE 1. Baseline characteristic of included studies of patients with high-grade glioma.
Network meta-analysis
Network evidence plots
A network meta-analysis was conducted to assess the efficacy and safety of the different treatment regimens. A total of 11 treatment regimens from 10 studies (Friedman et al., 2009; Taal et al., 2014; Field et al., 2015; Gilbert et al., 2017; Wick et al., 2017; Brandes et al., 2019; Galanis et al., 2019; Lombardi et al., 2019; Puduvalli et al., 2020; Reardon et al., 2020) constituted the analysis network for OS and PFS (Figures 2A, B), and 10 treatment regimens from 8 studies (Friedman et al., 2009; Taal et al., 2014; Field et al., 2015; Gilbert et al., 2017; Wick et al., 2017; Galanis et al., 2019; Lombardi et al., 2019; Reardon et al., 2020) constituted the analysis network for ORR (Figure 2C). Furthermore, 8 treatment regimens from 7 studies (Friedman et al., 2009; Field et al., 2015; Brandes et al., 2016; Gilbert et al., 2017; Galanis et al., 2019; Puduvalli et al., 2020; Reardon et al., 2020) constituted the analysis network for AEs (Figure 2D).
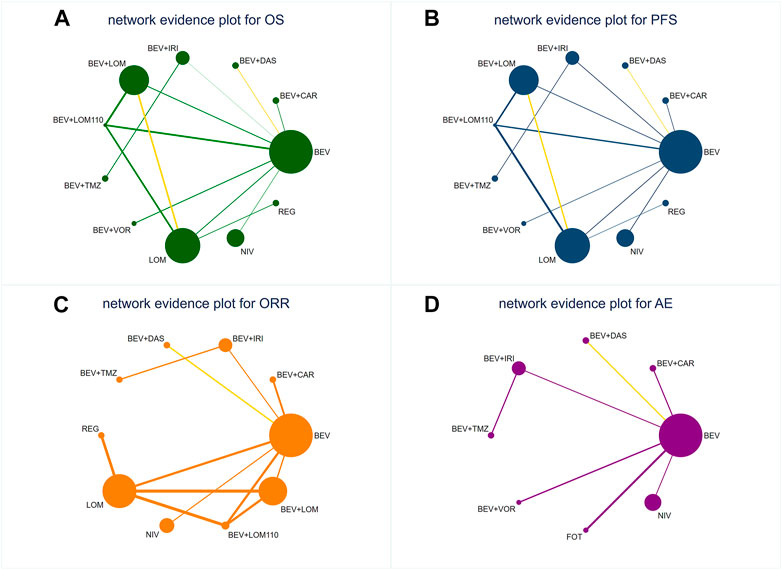
FIGURE 2. Network diagrams of comparisons on different outcomes of treatments s in different groups for patients with recurrent high-grade glioma. The yellow line indicates that there are studies in this comparison group that implemented a blinded approach. (A) Comparison of network diagrams for OS in high-grade glioma. (B) Comparison of network diagrams for PFS in high-grade glioma. (C) Comparison of network diagrams for ORR in high-grade glioma. (D) Comparison of network diagrams for grade 3 or higher AEs in high-grade glioma. BEV, bevacizumab; CAR, carboplatin; DAS, dasatinib; IRI, irinotecan; LOM, lomustine (90 mg/m2); LOM110, lomustine (110 mg/m2); TMZ, temozolomide; VOR, vorinostat; NIV, nivolumab; REG, regorafenib; FOT, fotemustine.
Heterogeneity and inconsistency assessment
A fixed-effects model was used for the analysis of OS, ORR and AEs (I2 < 25%) and a random-effects model for the analysis of PFS (I2 > 50%). The results of heterogeneity test were presented in Supplementary Figure S3. The heterogeneity of the comparison group of lomustine and bevacizumab plus lomustine was high (I2 = 69.6%), which was mainly due to the Brandes2019 study. After removing this trial, the I2 decreased to 32.4% (Supplementary Figure S3E). A closed-loop structure was present in the network of OS, PFS, and ORR, but since the arms that comprised the loop were from one literature, (Taal et al., 2014), there was no need to check the consistency of the direct evidence (van Valkenhoef et al., 2016).
Comparison of efficacy and safety
The direct and indirect evidence of different treatments in terms of survival and binary outcomes were synthesized and reported as HR and OR, respectively.
Regorafenib was found to have the best benefit for OS (Figure 3A), compared to other treatment regimens. In terms of PFS (Figure 3A), only bevacizumab plus lomustine (90 mg/m2) was significantly effective than lomustine alone (HR = 0.51, 95% CI 0.27-0.95). The HR of bevacizumab plus lomustine (90 mg/m2) was less than 1, which had a therapeutic advantage compared to the other nine regimens, though the confidence interval spanned 1.
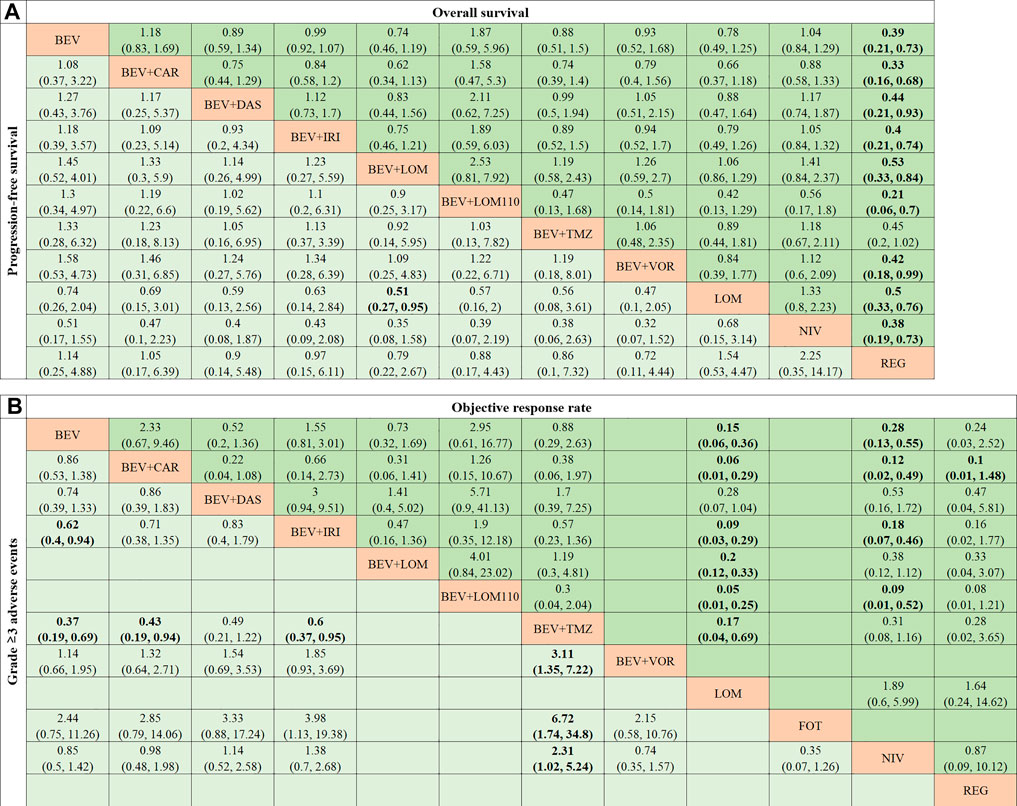
FIGURE 3. Pooled estimates of the network meta-analysis. (A) Pooled HRs (95% credible intervals) for OS in the upper triangle and PFS in the lower triangle. (B) Pooled ORs (95% credible intervals) for ORR in the upper triangle and 3 or higher AEs in the lower triangle. BEV, bevacizumab; CAR, carboplatin; DAS, dasatinib; IRI, irinotecan; LOM, lomustine (90 mg/m2); LOM110, lomustine (110 mg/m2); TMZ, temozolomide; VOR, vorinostat; NIV, nivolumab; REG, regorafenib; FOT, fotemustine.
Lomustine and nivolumab performed poorly on ORR (Figure 3B). The range of ORs were from 0.05 to 0.28 for lomustine compared to bevacizumab, bevacizumab plus carboplatin, bevacizumab plus dasatinib, bevacizumab plus irinotecan, bevacizumab plus lomustine (including 90 mg/m2 and 110 mg/m2) and bevacizumab plus temozolomide. The range of ORs were from 0.09 to 0.53 for nivolumab compared to the above regimens.
For grade 3 or higher AE (Figure 3B), bevacizumab plus temozolomide suffered the worst safety. The primary adverse event of bevacizumab plus temozolomide was myelotoxicity (Gilbert et al., 2017).
A two-dimensional graph was drawn to visualize the effect of different treatments on OS and PFS, taking bevacizumab as control (Figure 4). The diagram showed that regorafenib, bevacizumab plus lomustine (90 mg/m2), bevacizumab plus temozolomide, bevacizumab plus dasatinib, and bevacizumab plus vorinostat had better efficacy than bevacizumab in terms of OS and PFS, athough the confidence interval for HR of most regimens crossed 1 with no significant difference.
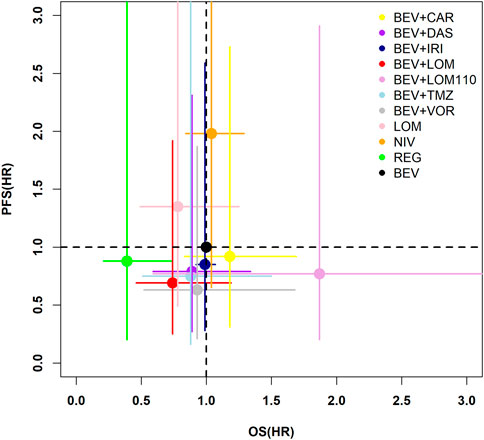
FIGURE 4. Two-dimensional plot of OS and PFS for difference treatments. The horizontal coordinate indicates the risk ratio for OS of the study regimen with bevacizumab as the control, and the vertical coordinate indicates the risk ratio for PFS of the study regimen with bevacizumab as the control. The dots indicate the estimated risk ratios for the study regimens, and the horizontal line indicates the 95% confidence interval for HR. BEV, bevacizumab; CAR, carboplatin; DAS, dasatinib; IRI, irinotecan; LOM, lomustine (90 mg/m2); LOM110, lomustine (110 mg/m2); TMZ, temozolomide; VOR, vorinostat; NIV, nivolumab; REG, regorafenib.
Rank probabilities
The ranking and SUCRA of comparable treatments for patients with high-grade glioma obtained by network meta-analysis (Figures 5, 6) were consistent with HR and OR.
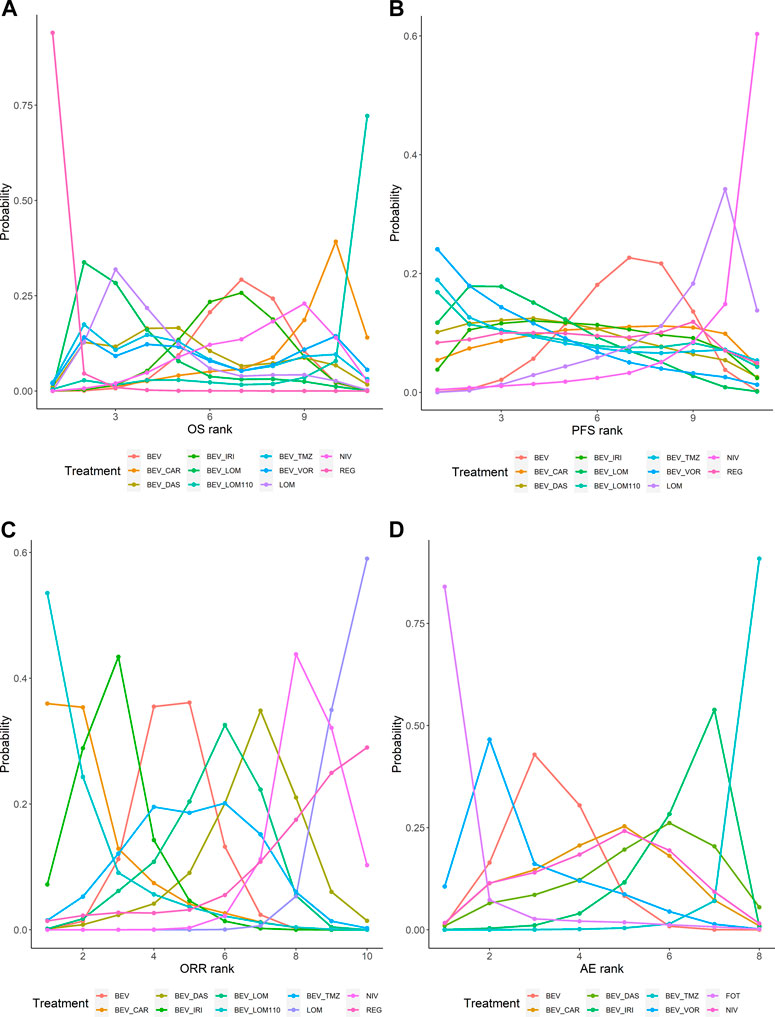
FIGURE 5. Bayesian ranking profiles of comparable treatments on efficacy and safety for patients with high-grade gliomas. Profiles indicate the probability of each treatment being ranked from first to last on OS (A), PFS (B), ORR (C), and grade 3 or higher AEs (D). Ranking curves are described according to the Bayesian ranking results presented in Supplementary Table S3. BEV, bevacizumab; CAR, carboplatin; DAS, dasatinib; IRI, irinotecan; LOM, lomustine (90 mg/m2); LOM110, lomustine (110 mg/m2); TMZ, temozolomide; VOR, vorinostat; NIV, nivolumab; REG, regorafenib; FOT, fotemustine.
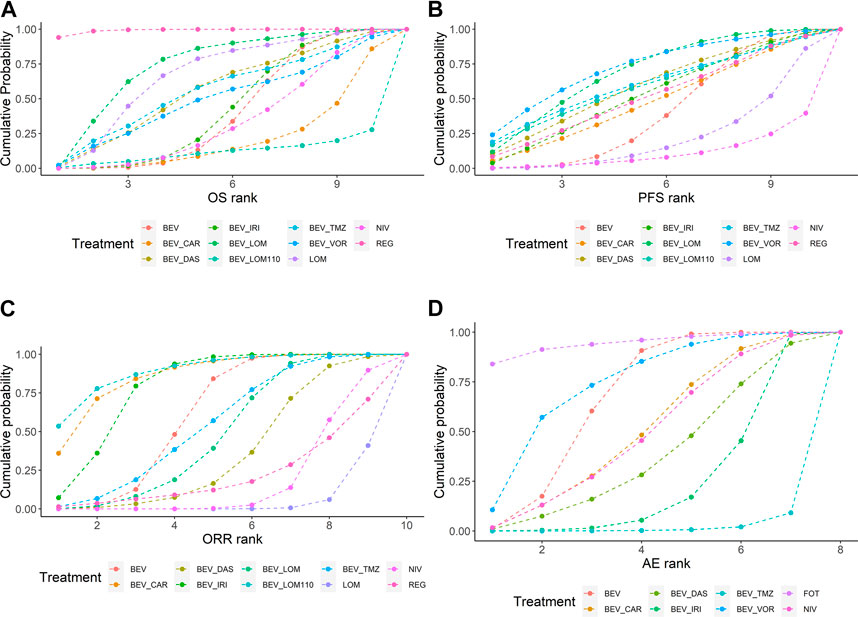
FIGURE 6. SUCRA ranking of comparable treatments on efficacy and safety for patients with high-grade gliomas. Profiles indicate the cumulative probability of each treatment being ranked in the top on OS (A), PFS (B), ORR (C), and grade 3 or higher AEs (D). SUCRA are described according to the Bayesian cumulative ranking results presented in Supplementary Table S4. BEV, bevacizumab; CAR, carboplatin; DAS, dasatinib; IRI, irinotecan; LOM, lomustine (90 mg/m2); LOM110, lomustine (110 mg/m2); TMZ, temozolomide; VOR, vorinostat; NIV, nivolumab; REG, regorafenib; FOT, fotemustine.
Patients with recurrent high-grade glioma treated with regorafenib are likely to experience the longest OS (94% probability). The SUCRA of regorafenib was much higher than other regimens. Patients treated with bevacizumab plus vorinostat may attain the longest PFS (24% probability). However, the SUCRA of bevacizumab plus lomustine (90 mg/m2) and bevacizumab plus vorinostat were similar. Patients treated with bevacizumab plus lomustine (110 mg/m2) may have better ORRs (54% probability). Lomustine and nivolumab performed poorly for ORR. Patients treated with lomustine were minimally at risk for a grade ≥3 AEs (84% probability), whereas bevacizumab-based regimens tended to have higher toxicity than bevacizumab alone.
Sensitivity analysis
There was a large heterogeneity of PFS after combining various trials. Therefore, a sensitivity analysis was conducted, excluding each trial in turn. As a result, it was identified that Brandes2019 was the primary source of heterogeneity in the PFS network. With this information in mind, sensitivity analyses of PFS outcomes were performed using the remaining studies, excluding Brandes 2019. Supplementary Figure S4 display the results of pairwise comparison, probability ranking, and the SUCRA.
The sensitivity analysis outcomes aligned with those yielded by the Bayesian network meta-analysis. In the pairwise comparison, it remained that bevacizumab plus lomustine (90 mg/m2) achieved a significantly enhanced PFS, as compared to lomustine. The HRs of other comparisons were not found to be significant.
Similarly, in the ranking of PFS, the curves followed the same pattern as the network meta-analysis. Additionally, there was a slight increase in the probability that bevacizumab plus lomustine (90 mg/m2) would rank in the top four. Global results obtained from the network meta-analysis were robust.
Discussion
In this systematic review and Bayesian network meta-analysis, we present a comprehensive summary and comparison of the efficacy and safety profiles of various interventions for high-grade gliomas, including bevacizumab monotherapy, bevacizumab-based therapies, nitrosoureas, PD-1 inhibitors, and multi-targeted kinase inhibitors. To bolster the study’s clinical utility in real-world practice, we excluded investigations on experimental drugs that remain unavailable commercially.
The results of the study suggest that regorafenib is likely to be the most effective treatment for improving survival outcomes in patients with longer OS and PFS, although the options may not provide the same benefit in terms of ORR. The efficacy of the combination therapy of bevacizumab and lomustine (90 mg/m2) was inferior to that of regorafenib. Nevertheless, it outperformed other treatment options in terms of survival outcomes and is recommended as the second option according to our findings. However, the ORR was unsatisfactory as well. Notably, bevacizumab plus lomustine (110 mg/m2) ranked high in ORR outcomes, which may be attributed to the dose administered. However, the limited sample size of patients in original studies may have introduced some bias into our results.
In terms of safety, no drug had an absolutely good safety profile. Regorafenib and bevacizumab plus lomustine (90 mg/m2) were not included in the safety evaluation network due to incomplete safety data. Grade 3 or higher AEs for regorafenib were dominated by elevated lipase and hand-foot skin reactions (both incidences were over 10%) (Lombardi et al., 2019). Main AEs for bevacizumab plus lomustine (90 mg/m2) were hypertension, hematologic effects, and fatigue (Taal et al., 2014; Wick et al., 2017). Our investigation revealed that fotemustine exhibited the most favorable safety profile. Given that it belongs to the same class of nitrosourea as lomustine, it appears reasonable to assert that nitrosourea drugs may generally confer a measure of therapeutic advantage in terms of safety.
The study by Brandes in 2019 exhibited a greater degree of heterogeneity in contrast to the research conducted by Taal in 2014 and Wick in 2017 in paired comparison of lomustine and bevacizumab plus lomustine (90 mg/m2). This may be attributed to the ratio of O-6-methylguanine-DNA methyltransferase (MGMT) methylation and unmethylation, which was approximately 1/2 in the Brandes2019 study, compared to a near 1:1 ratio seen in the other two studies. A multitude of investigations have demonstrated an association between MGMT unmethylation and resistance to chemotherapeutic agents (Oldrini et al., 2020). This may plausibly account for the observed larger HR for PFS in the Brandes2019 study, in contrast to the Taal2014 and Wick2017 studies, where the HR values were quite similar. However, we are reassured that our final results were not impacted by heterogeneity through sensitivity analyses.
The study enrolled predominantly patients with recurrent GBM. The National Comprehensive Cancer Network (NCCN) clinical practice guidelines for central nervous system cancers (Nabors et al., 2020) recommend preferential use of bevacizumab, temozolomide, lomustine or carmustine, PCV and regorafenib for recurrent GBM. The European Association of Neuro-Oncology (EANO) guidelines of diffuse glioma in adults (Weller et al., 2021) endorse nitrosoureas, temozolomide and bevacizumab for progression or relapse of GBM. The findings of our analysis support the use of regorafenib for recurrent GBM based on its association with significant survival benefits. However, experience with regorafenib in recurrent GBM is limited compared with other recommended therapeutic options in the guidelines. Regorafenib is a multi-kinase inhibitor. Its anti-tumor mechanism remains elusive despite several clinical trials. A recent investigation delving into its mode of action has unearthed regorafenib’s ability to stabilize the critical enzyme PSAT1 (phosphoserine aminotransferase 1) involved in serine synthesis. This unfavorable activity in GBM cells leads to fatal autophagy arrest and tumor suppression (Jiang et al., 2020). The promising results suggest that the levels of PSAT1 play a key regulatory role in the success of regorafenib-induced GBM therapy. Additional research has identified molecular features correlated with prolonged survival rate in regorafenib-treated GBM patients. These features include EGFR mutations (Chiesa et al., 2022), gene transcripts such as HIF1A and CDKN1A, miRNAs like miR-3607–3p, miR-301a-3p, miR-93–5p (Santangelo et al., 2021), and MAPK pathway mutations that may associate with a poor prognosis (Chiesa et al., 2022). However, limited evidence restricts the scope of individualized dosing of regorafenib, hence, greater evidence is required to increase its widespread acceptance.
The Chinese guidelines (Jiang et al., 2021) recommended bevacizumab plus lomustine (90 mg/m2), while it is not a preferred regimen in NCCN(7) and EANO(8) guidelines. Clinicians need to carefully consider the AEs and patient status when selecting this combination. Additionally, cost effectiveness is also an important factor to consider (Cagney and Alexander, 2017), but there is a paucity of evidence in this area at present.
There are commendable aspects to our review, particularly the emphasis placed on high-grade glioma, as opposed to recurrent GBM, although the latter still featured prominently in the final analysis. We established a comprehensive network pertaining to all drug treatments, and judiciously applied analytical methods to estimate hazard ratios founded upon Kaplan-Meier curves, yielding the added benefit of integrating studies that did not report hazard ratios, thus allowing for a more comprehensive evaluation of the many treatments evaluated. Our review presents valuable information for clinical decision-making, which we achieved by carefully scrutinizing and assessing the outcomes of various treatments, and performing rigorous analyses, including sensitivity analysis of network heterogeneity and consistency, thus ensuring robust and dependable results.
Our research, though valuable, still presents some limitations. Firstly, the scope of this study was limited to patients with recurrent high-grade glioma. However, upon examining relevant literature, we discovered a dearth of randomized controlled trials pertaining to grade 3 glioma or anaplastic glioma. Furthermore, we were unable to perform a comprehensive subgroup analysis of grade 3 glioma due to insufficient data. It is thus imperative to acknowledge that the results of our work may not fully represent the ideal treatment strategies for grade 3 recurrent glioma. Another shortcoming of the study was incomplete reporting of results, which prevented the integration of certain guidelines-recommended treatments, such as temozolomide and PCV, into the network. Despite these limitations, pertinent data of clinical trials can be gleaned from Table 1. Language bias may also have some impact on the results. The literature in this article is from English and Chinese databases and may miss potential and qualified studies from other language databases.
As per our research findings, conventional drugs appear to be ineffective in producing significant impacts towards recurrent high-grade glioma. The large molecular phenotype heterogeneity is likely a contributing factor (Nicholson and Fine, 2021). Targeting specific pathways may be a more effective approach (Le Rhun et al., 2019). Among the targeted agents analyzed in this study, both bevacizumab and regorafenib interact with vascular endothelial growth factor (VEGF), which inhibits neoangiogenesis and thus exerts anti-tumor effects. In addition, regorafenib targets multiple gene and kinase such as BRAF, KIT, and RET, which may be potential therapeutic targets but need to be confirmed by further studies. The latest study has found that patients presenting a BRAF-V600E mutation showed improved ORR with dabrafenib and trametinib, providing a clear indication of the potential benefits of individualized treatment strategies (Wen et al., 2022). Likewise, a phase 3 clinical trial of a vaccine has shown promising results in the treatment of recurrent glioma. As demonstrated by Liah et al.’s study, the addition of an autologous tumor lysate-loaded dendritic cell vaccine has resulted in significant clinical benefits resulting in a statistically significant increase in survival time for patients with relapsed GBM (Liau et al., 2023). Whether by targeting specific molecules, pathways, or through autologous tumor lysates, individualized therapy holds significant promise for the treatment of recurrent high-grade gliomas. However, current advancements in this critical area have been insufficient to fully realize the potential of personalized medicine in this setting. In the present context, emerging data emphasizes that regorafenib and bevacizumab in combination with lomustine, represents the most promising therapeutic alternative for high-grade glioma.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
ZZ conceived and designed the study, and revised the manuscript. YX searched and screened the literature, evaluated the quality of random controlled trials, extracted and processed the data, and completed the first draft. HG screened the literature and extracted the data. KY evaluated the quality of trials and processed the data. NJ made the final decisions for the disagreements in the study. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by Capital Health Development Research Special Project: research on precision treatment of recurrent high-grade glioma based on PTC drug screening technology (No. SF 2022-2-2047).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer FL declared a shared parent affiliation with the author(s) to the handling editor at the time of review.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1191480/full#supplementary-material
References
Boiardi, A., Silvani, A., Milanesi, I., Broggi, G., and Fariselli, L. (1992). Efficacy of '8-drugs-in-one-day' combination in treatment of recurrent GBM patients. J. Neurooncol 12 (2), 153–158. doi:10.1007/bf00172666
Brada, M., Stenning, S., Gabe, R., Thompson, L. C., Levy, D., Rampling, R., et al. (2010). Temozolomide versus procarbazine, lomustine, and vincristine in recurrent high-grade glioma. J. Clin. Oncol. 28 (30), 4601–4608. doi:10.1200/JCO.2009.27.1932
Brandes, A. A., Finocchiaro, G., Zagonel, V., Reni, M., Caserta, C., Fabi, A., et al. (2016). Avareg: A phase II, randomized, noncomparative study of fotemustine or bevacizumab for patients with recurrent glioblastoma. Neuro-oncology 18 (9), 1304–1312. doi:10.1093/neuonc/now035
Brandes, A. A., Gil-Gil, M., Saran, F., Carpentier, A. F., Nowak, A. K., Mason, W., et al. (2019). A randomized phase II trial (TAMIGA) evaluating the efficacy and safety of continuous bevacizumab through multiple lines of treatment for recurrent glioblastoma. Oncologist 24 (4), 521–528. doi:10.1634/theoncologist.2018-0290
Cabrera, A. R., Kirkpatrick, J. P., Fiveash, J. B., Shih, H. A., Koay, E. J., Lutz, S., et al. (2016). Radiation therapy for glioblastoma: Executive summary of an American society for radiation oncology evidence-based clinical practice guideline. Pract. Radiat. Oncol. 6 (4), 217–225. doi:10.1016/j.prro.2016.03.007
Cagney, D. N., and Alexander, B. M. (2017). The cost and value of glioblastoma therapy. Expert Rev. Anticancer Ther. 17 (8), 657–659. doi:10.1080/14737140.2017.1351355
Chaimani, A., Higgins, J. P., Mavridis, D., Spyridonos, P., and Salanti, G. (2013). Graphical tools for network meta-analysis in STATA. PLoS One 8 (10), e76654. doi:10.1371/journal.pone.0076654
Chiesa, S., Mangraviti, A., Martini, M., Cenci, T., Mazzarella, C., Gaudino, S., et al. (2022). Clinical and NGS predictors of response to regorafenib in recurrent glioblastoma. Sci. Rep. 12 (1), 16265. doi:10.1038/s41598-022-20417-y
Cumpston, M., Li, T., Page, M. J., Chandler, J., Welch, V. A., Higgins, J. P., et al. (2019). Updated guidance for trusted systematic reviews: A new edition of the Cochrane handbook for systematic reviews of interventions. Cochrane database Syst. Rev. 10, Ed000142. doi:10.1002/14651858.Ed000142
Dias, S., Welton, N. J., Caldwell, D. M., and Ades, A. E. (2010). Checking consistency in mixed treatment comparison meta-analysis. Statistics Med. 29 (7-8), 932–944. doi:10.1002/sim.3767
Dresemann, G., Weller, M., Rosenthal, M. A., Wedding, U., Wagner, W., Engel, E., et al. (2010). Imatinib in combination with hydroxyurea versus hydroxyurea alone as oral therapy in patients with progressive pretreated glioblastoma resistant to standard dose temozolomide. J. Neuro-Oncology 96 (3), 393–402. doi:10.1007/s11060-009-9976-3
Duerinck, J., Du Four, S., Bouttens, F., Andre, C., Verschaeve, V., Van Fraeyenhove, F., et al. (2018). Randomized phase II trial comparing axitinib with the combination of axitinib and lomustine in patients with recurrent glioblastoma. J. Neuro-Oncology 136 (1), 115–125. doi:10.1007/s11060-017-2629-z
Field, K. M., Simes, J., Nowak, A. K., Cher, L., Wheeler, H., Hovey, E. J., et al. (2015). Randomized phase 2 study of carboplatin and bevacizumab in recurrent glioblastoma. Neuro-oncology 17 (11), 1504–1513. doi:10.1093/neuonc/nov104
Friedman, H. S., Prados, M. D., Wen, P. Y., Mikkelsen, T., Schiff, D., Abrey, L. E., et al. (2009). Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J. Clin. Oncol. 27 (28), 4733–4740. doi:10.1200/JCO.2008.19.8721
Galanis, E., Anderson, S. K., Twohy, E. L., Carrero, X. W., Dixon, J. G., Tran, D. D., et al. (2019). A phase 1 and randomized, placebo-controlled phase 2 trial of bevacizumab plus dasatinib in patients with recurrent glioblastoma: Alliance/north central cancer treatment group N0872. Cancer 125 (21), 3790–3800. doi:10.1002/cncr.32340
Gilbert, M. R., Pugh, S. L., Aldape, K., Sorensen, A. G., Mikkelsen, T., Penas-Prado, M., et al. (2017). NRG oncology RTOG 0625: A randomized phase II trial of bevacizumab with either irinotecan or dose-dense temozolomide in recurrent glioblastoma. J. Neuro-Oncology 131 (1), 193–199. doi:10.1007/s11060-016-2288-5
Higgins, J. P., Thompson, S. G., Deeks, J. J., and Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ Clin. Res. ed) 327 (7414), 557–560. doi:10.1136/bmj.327.7414.557
Jiang, J., Zhang, L., Chen, H., Lei, Y., Zhang, T., Wang, Y., et al. (2020). Regorafenib induces lethal autophagy arrest by stabilizing PSAT1 in glioblastoma. Autophagy 16 (1), 106–122. doi:10.1080/15548627.2019.1598752
Jiang, T., Nam, D. H., Ram, Z., Poon, W. S., Wang, J., Boldbaatar, D., et al. (2021). Clinical practice guidelines for the management of adult diffuse gliomas. Cancer Lett. 499, 60–72. doi:10.1016/j.canlet.2020.10.050
Le Rhun, E., Preusser, M., Roth, P., Reardon, D. A., van den Bent, M., Wen, P., et al. (2019). Molecular targeted therapy of glioblastoma. Cancer Treat. Rev. 80, 101896. doi:10.1016/j.ctrv.2019.101896
Liau, L. M., Ashkan, K., Brem, S., Campian, J. L., Trusheim, J. E., Iwamoto, F. M., et al. (2023). Association of autologous tumor lysate-loaded dendritic cell vaccination with extension of survival among patients with newly diagnosed and recurrent glioblastoma: A phase 3 prospective externally controlled cohort trial. JAMA Oncol. 9 (1), 112–121. doi:10.1001/jamaoncol.2022.5370
Lombardi, G., De Salvo, G. L., Brandes, A. A., Eoli, M., Rudà, R., Faedi, M., et al. (2019). Regorafenib compared with lomustine in patients with relapsed glioblastoma (REGOMA): A multicentre, open-label, randomised, controlled, phase 2 trial. lancet Oncol. 20 (1), 110–119. doi:10.1016/S1470-2045(18)30675-2
Louis, D. N., Perry, A., Wesseling, P., Brat, D. J., Cree, I. A., Figarella-Branger, D., et al. (2021). The 2021 WHO classification of tumors of the central nervous system: A summary. Neuro Oncol. 23 (8), 1231–1251. doi:10.1093/neuonc/noab106
Ma, R., Taphoorn, M. J. B., and Plaha, P. (2021). Advances in the management of glioblastoma. J. neurology, Neurosurg. psychiatry 92 (10), 1103–1111. doi:10.1136/jnnp-2020-325334
McBain, C., Lawrie, T. A., Rogozińska, E., Kernohan, A., Robinson, T., and Jefferies, S. (2021). Treatment options for progression or recurrence of glioblastoma: A network meta-analysis. Cochrane Database Syst. Rev. 2021 (12), 2020. doi:10.1002/14651858.CD013579.pub2
McKinnon, C., Nandhabalan, M., Murray, S. A., and Plaha, P. (2021). Glioblastoma: Clinical presentation, diagnosis, and management. BMJ Clin. Res. ed) 374, n1560. doi:10.1136/bmj.n1560
Nabors, L. B., Portnow, J., Ahluwalia, M., Baehring, J., Brem, H., Brem, S., et al. (2020). Central nervous system cancers, version 3.2020, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. JNCCN 18 (11), 1537–1570. doi:10.6004/jnccn.2020.0052
Nayak, L., Molinaro, A. M., Peters, K., Clarke, J. L., Jordan, J. T., de Groot, J., et al. (2021). Randomized phase II and biomarker study of pembrolizumab plus bevacizumab versus pembrolizumab alone for patients with recurrent glioblastoma. Clin. cancer Res. 27 (4), 1048–1057. doi:10.1158/1078-0432.CCR-20-2500
Nicholson, J. G., and Fine, H. A. (2021). Diffuse glioma heterogeneity and its therapeutic implications. Cancer Discov. 11 (3), 575–590. doi:10.1158/2159-8290.Cd-20-1474
Oldrini, B., Vaquero-Siguero, N., Mu, Q., Kroon, P., Zhang, Y., Galán-Ganga, M., et al. (2020). MGMT genomic rearrangements contribute to chemotherapy resistance in gliomas. Nat. Commun. 11 (1), 3883. doi:10.1038/s41467-020-17717-0
Omuro, A., and DeAngelis, L. M. (2013). Glioblastoma and other malignant gliomas: A clinical review. Jama 310 (17), 1842–1850. doi:10.1001/jama.2013.280319
Ostrom, Q. T., Gittleman, H., Truitt, G., Boscia, A., Kruchko, C., and Barnholtz-Sloan, J. S. (2018). CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2011-2015. Neuro Oncol. 20, iv1–iv86. doi:10.1093/neuonc/noy131
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ Clin. Res. ed) 372, n71. doi:10.1136/bmj.n71
Patil, V. M., Menon, N., Chatterjee, A., Tonse, R., Choudhari, A., Mahajan, A., et al. (2022). Mebendazole plus lomustine or temozolomide in patients with recurrent glioblastoma: A randomised open-label phase II trial. EClinicalMedicine 49, 101449. doi:10.1016/j.eclinm.2022.101449
Puduvalli, V. K., Wu, J., Yuan, Y., Armstrong, T. S., Vera, E., Wu, J., et al. (2020). A Bayesian adaptive randomized phase II multicenter trial of bevacizumab with or without vorinostat in adults with recurrent glioblastoma. Neuro-oncology 22 (10), 1505–1515. doi:10.1093/neuonc/noaa062
Reardon, D. A., Brandes, A. A., Omuro, A., Mulholland, P., Lim, M., Wick, A., et al. (2020). Effect of nivolumab vs bevacizumab in patients with recurrent glioblastoma: The CheckMate 143 phase 3 randomized clinical trial. JAMA Oncol. 6 (7), 1003–1010. doi:10.1001/jamaoncol.2020.1024
Reardon, D. A., Nabors, L. B., Mason, W. P., Perry, J. R., Shapiro, W., Kavan, P., et al. (2015). Phase I/randomized phase II study of afatinib, an irreversible ErbB family blocker, with or without protracted temozolomide in adults with recurrent glioblastoma. Neuro-Oncology 17 (3), 430–439. doi:10.1093/neuonc/nou160
Salanti, G., Ades, A. E., and Ioannidis, J. P. (2011). Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 64 (2), 163–171. doi:10.1016/j.jclinepi.2010.03.016
Santangelo, A., Rossato, M., Lombardi, G., Benfatto, S., Lavezzari, D., De Salvo, G. L., et al. (2021). A molecular signature associated with prolonged survival in glioblastoma patients treated with regorafenib. Neuro Oncol. 23 (2), 264–276. doi:10.1093/neuonc/noaa156
Song, W. G., Wang, Y. F., Liu, R., Yang, Z. H., Fang, F., Wang, R. L., et al. (2010). Efficacy comparison of hydroxycamptothecine and temozolomide for recurrent high-grade gliomas. Chin. J. Cancer Prev. Treat. 17 (20), 1676–1678.
Sun, J., Yang, X. J., and Yang, S. Y. (2013). Multicenter randomized controlled study of temozolomide versus semustine in the treatment of recurrent malignant glioma. Natl. Med. J. China 93 (3), 165–168. doi:10.3760/cma.j.issn.0376-2491.2013.03.003
Taal, W., Oosterkamp, H. M., Walenkamp, A. M., Dubbink, H. J., Beerepoot, L. V., Hanse, M. C., et al. (2014). Single-agent bevacizumab or lomustine versus a combination of bevacizumab plus lomustine in patients with recurrent glioblastoma (BELOB trial): A randomised controlled phase 2 trial. Lancet Oncol. 15 (9), 943–953. doi:10.1016/s1470-2045(14)70314-6
Tierney, J. F., Stewart, L. A., Ghersi, D., Burdett, S., and Sydes, M. R. (2007). Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 8, 16. doi:10.1186/1745-6215-8-16
Twelves, C., Sabel, M., Checketts, D., Miller, S., Tayo, B., Jove, M., et al. (2021). A phase 1b randomised, placebo-controlled trial of nabiximols cannabinoid oromucosal spray with temozolomide in patients with recurrent glioblastoma. Br. J. Cancer 124 (8), 1379–1387. doi:10.1038/s41416-021-01259-3
van Valkenhoef, G., Dias, S., Ades, A. E., and Welton, N. J. (2016). Automated generation of node-splitting models for assessment of inconsistency in network meta-analysis. Res. synthesis methods 7 (1), 80–93. doi:10.1002/jrsm.1167
Weller, M., van den Bent, M., Preusser, M., Le Rhun, E., Tonn, J. C., Minniti, G., et al. (2021). EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat. Rev. Clin. Oncol. 18 (3), 170–186. doi:10.1038/s41571-020-00447-z
Wen, P. Y., Stein, A., van den Bent, M., De Greve, J., Wick, A., de Vos, F., et al. (2022). Dabrafenib plus trametinib in patients with BRAF(V600E)-mutant low-grade and high-grade glioma (ROAR): A multicentre, open-label, single-arm, phase 2, basket trial. Lancet Oncol. 23 (1), 53–64. doi:10.1016/s1470-2045(21)00578-7
Wen, P. Y., Weller, M., Lee, E. Q., Alexander, B. M., Barnholtz-Sloan, J. S., Barthel, F. P., et al. (2020). Glioblastoma in adults: A society for neuro-oncology (SNO) and European society of neuro-oncology (EANO) consensus review on current management and future directions. Neuro Oncol. 22 (8), 1073–1113. doi:10.1093/neuonc/noaa106
Wick, W., Gorlia, T., Bendszus, M., Taphoorn, M., Sahm, F., Harting, I., et al. (2017). Lomustine and bevacizumab in progressive glioblastoma. N. Engl. J. Med. 377 (20), 1954–1963. doi:10.1056/NEJMoa1707358
Keywords: high-grade glioma, recurrent, pharmacotherapy, network meta-analysis, systematic review, efficacy, safety
Citation: Xu Y, Guan H, Yu K, Ji N and Zhao Z (2023) Efficacy and safety of pharmacotherapy for recurrent high-grade glioma: a systematic review and network meta-analysis. Front. Pharmacol. 14:1191480. doi: 10.3389/fphar.2023.1191480
Received: 22 March 2023; Accepted: 22 May 2023;
Published: 01 June 2023.
Edited by:
Sheng Zhong, Sun Yat-sen University Cancer Center, ChinaCopyright © 2023 Xu, Guan, Yu, Ji and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhigang Zhao, MTAyMnp6Z0BzaW5hLmNvbQ==