
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 16 May 2023
Sec. Pharmacology of Infectious Diseases
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1161526
 Sha Diao1,2,3,4
Sha Diao1,2,3,4 Zheng Liu1,2,3,4,5
Zheng Liu1,2,3,4,5 Dan Liu1,2,3,4,6
Dan Liu1,2,3,4,6 Xiao Cheng1,2,3,4
Xiao Cheng1,2,3,4 Linan Zeng1,2,3,4
Linan Zeng1,2,3,4 Xue-Feng Jiao1,2,3,4
Xue-Feng Jiao1,2,3,4 Zhe Chen1,2,3,4,6Xiaofeng Ni1,2,3,4Siyi He1,2,3,4,6
Zhe Chen1,2,3,4,6Xiaofeng Ni1,2,3,4Siyi He1,2,3,4,6 Bin Wu7
Bin Wu7 Deying Kang8
Deying Kang8 Chaomin Wan4,9Rongsheng Zhao10Huiqing Wang11*
Chaomin Wan4,9Rongsheng Zhao10Huiqing Wang11* Lingli Zhang1,2,3,4,8*
Lingli Zhang1,2,3,4,8*Background: Tuberculosis continues to be a significant global burden. Purified protein derivative of tuberculin (TB-PPD) is one type of tuberculin skin test (TST) and is used commonly for the auxiliary diagnosis of tuberculosis. The recombinant Mycobacterium tuberculosis fusion protein (EC) test is a new test developed in China.
Objective: Evaluate the long-term economic implications of using the EC test compared with the TB-PPD test to provide a reference for clinical decision-making.
Methods: The target population was people at a high risk persons of being infected with Mycobacterium tuberculosis. The outcome indicator was quality-adjusted life years (QALY). A cost–utility analysis was used to evaluate the long-term economic implications of using the EC test compared with the TB-PPD test. We employed a decision tree–Markov model from the perspective of the whole society within 77 years.
Results: Compared with the TB-PPD test, the EC test had a lower cost but higher QALY. The incremental cost–utility ratio was −119,800.7381 CNY/QALY. That is, for each additional QALY, the EC test could save 119,800.7381 CNY: the EC test was more economical than the TB-PPD test.
Conclusion: Compared with the TB-PPD test, the EC test would be more economical in the long term for the diagnosis of M. tuberculosis infection according our study.
Tuberculosis is a chronic infectious disease caused by Mycobacterium tuberculosis (MTB) infection. According to estimates published by the World Health Organization (WHO), tuberculosis is the 13th leading cause of death worldwide and the number-one cause of death from a single infectious agent. In 2020, it was anticipated that tuberculosis will rank as the second leading cause of death from a single infectious agent, after Coronavirus disease-2019 (GBD 2019 Diseases and Injuries Collaborators, 2020; World Health Organization, 2021). According to the Global Tuberculosis Report 2021 published by the WHO, nearly one-third of the worldwide population is infected with MTB, with ∼2 billion infected people, ∼9.9 million new patients with tuberculosis, and ∼1.514 million deaths from tuberculosis. In China, the number of MTB infections is ∼350 million, and there are 842,000 new patients with tuberculosis, of which ∼32,000 people will die of tuberculosis (Cui et al., 2020; World Health Organization, 2020; World Health Organization, 2021). If people are infected with MTB, 95% will have latent tuberculosis infection (LTBI), and there will be a 5%–10% probability of developing into active tuberculosis (ATB) in their lifetime. Once they have ATB, they will become a new source of tuberculosis infection (He et al., 2018; World Health Organization, 2019).
To eliminate tuberculosis, early identification of LTBI and providing preventive treatment are required (World Health Organization, 2015; Chinese Center for Disease Control and Prevention, 2021). LTBI does not carry the corresponding clinical symptoms, and evidence cannot be provided by imaging or bacteriological tests, so it can be diagnosed only by immunological methods (Zhou et al., 2021).
Purified protein derivative of tuberculin (TB-PPD) is a type of tuberculin skin test (TST). The TB-PPD test is employed commonly for diagnosing of LTBI in clinical practice. The criteria for a positive result is as follows: 1) Average diameter (sum of transverse and longitudinal diameters, divided by 2) of induration ≥6 mm 48–72 h later; 2) Blister, necrosis (skin breakdown) or lymphadenitis are interpreted as strong positive reactions. However, TB-PPD has many identical or similar antigenic components with those in Bacille Calmette-Guérin (BCG) vaccine and non-tuberculous mycobacteria (Pai et al., 2014; Ma et al., 2022).
Testing using recombinant Mycobacterium tuberculosis fusion protein (EC) was approved for marketing by China in 2020. EC is made from recombinant-EC obtained after fermentation, isolation and purification of Escherichia coli showing high expression of the specific ESAT6-CFP10 gene of MTB. The criteria for a positive result is as follows: 1) Average diameter (sum of transverse and longitudinal diameters, divided by 2) of redness or induration ≥5 mm 48–72 h later; 2) Blister, necrosis (skin breakdown) or lymphadenitis are interpreted as strong positive reactions.
Here, we constructed a decision tree–Markov model and used a cost–utility analysis to evaluate the long-term economic implications of using the EC test compared with using the TB-PPD test within 77 years. In this way, we aimed to provide a reference for clinical decision-making.
The target population was high-risk persons with MTB infection: close contacts of people with etiologically positive pulmonary tuberculosis; individuals infected with the human immunodeficiency virus (HIV); people receiving immunosuppressive treatment or other immunocompromised people (Pai et al., 2014; Chinese Center for Disease Control and Prevention, 2021; Zhou et al., 2021; Ma et al., 2022).
The outcome indicator was quality-adjusted life years (QALY). The cost–utility analysis was used with a decision tree–Markov model from the perspective of the whole society. EC was 0.3 mL/bottle. TB-PPD was 1 mL:50 IU/bottle. In our model, the duration of conventional anti-tuberculosis treatment was from 6 months to 12 months. The duration of preventive treatment was from 3 months to 9 months. Therefore, the model took 1 year as one cycle. People of all ages are susceptible to tuberculosis, so the starting age of the model was set to 0 years, and the end of the cycle was set to 77 years (average life expectancy in China).
The disease were divided into five Markov states: “health”, “LTBI”, “ATB”, “cured or self-healed” and “death”. In our model, the target population would receive an EC test or TB-PPD skin test, respectively. If the result was negative, then they would not receive clinical treatment. If the result was positive, then they would be diagnosed as having ATB or LTBI through further clinical examinations (medical history, imaging, etiology). Patients diagnosed with ATB would receive conventional anti-tuberculosis treatment. Patients diagnosed with LTBI would receive preventive treatment. All patients receiving treatment had the potential to develop drug-induced liver injury (DILI). The target population was entered into the Markov model based on different states, and was cycled according to the transition probability between states (Figure 1; Figure 2).
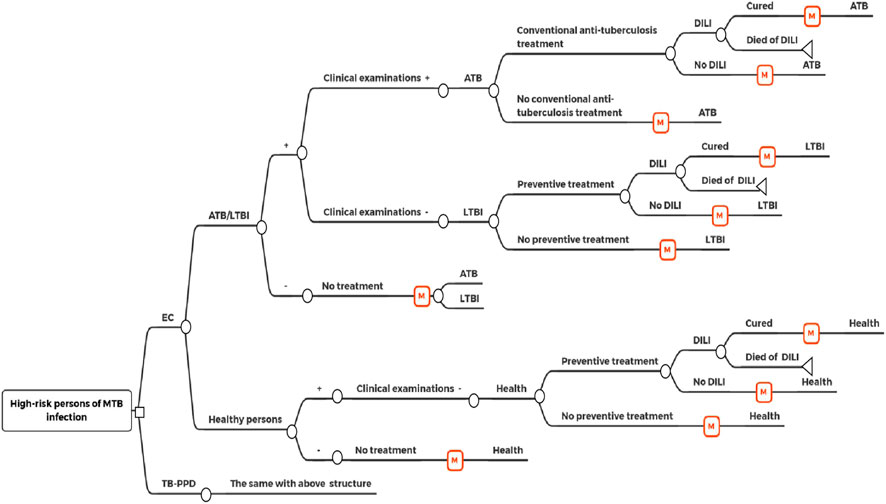
FIGURE 1. Decision tree-markov model.
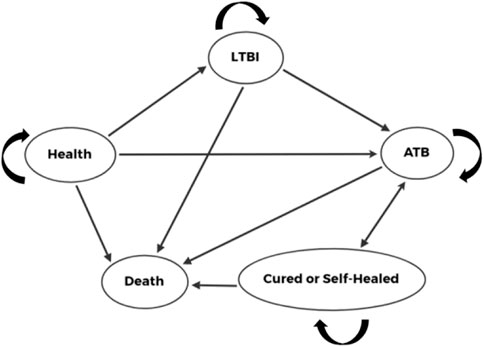
FIGURE 2. Markov states.
MTB: Mycobacterium tuberculosis; EC: Recombinant Mycobacterium tuberculosis fusion protein (EC); TB-PPD: Purified protein derivative of tuberculin (TB-PPD); ATB: Active tuberculosis; LTBI: Latent tuberculosis infection; DILI: Drug-induced liver injury.
The target population was vaccinated with BCG. All study participants complied with treatment. Each person could be in only one state, and undergo state transition only after treatment cessation. The probability of each event occurring in patients during the cycle remained unchanged.
The parameters of our model were: branch probabilities; transition probabilities between each Markov state; cost value; utility value. Branch probabilities comprised the: sensitivity and specificity of the EC test and TB-PDD test; prevalence of ATB and LTBI; proportion of participants receiving conventional treatment and preventive treatment; prevalence of and mortality due to DILI.
Costs included the: cost of the EC test or TB-PDD test; cost of clinical examination; cost of DILI treatment; treatment-related cost of ATB or LTBI. The treatment-related cost included: direct medical cost (cost of outpatient visits, hospitalization, self-purchased drugs); direct non-medical cost (cost of travel and meals for patients and their families); indirect cost (wage loss of patients and their families due to illness). Utility values were measured by QALY. The discount rate was also included.
The average level of the whole age group for each parameter was taken as a model parameter. The latest research based on a Chinese population was preferred. If there were different values for the same parameter in multiple studies, the weighted average was calculated as the baseline value, and the upper limit and lower limit among all studies were taken as the range of the parameter. If the range could not be obtained, the upper limit and lower limit were estimated based on ± 5% of the baseline value. For parameters that could not be obtained, studies based on non-Chinese populations or expert consultation were used.
The incremental cost–utility ratio (ICUR) was calculated based on our model. The willing-to-pay (WTP) threshold was equal to 1–3-times the gross domestic product (GDP) per capita (GDP per capita of China in 2021 was 80,976 CNY). If ICUR < 1-time GDP per capita, then the increased costs were worthwhile, so the model was very economical. If 1-time GDP per capita < ICUR < 3-times GDP per capita, then the increased costs were acceptable, so the model was economical. If ICUR >3-times GDP per capita, then the increased costs were not worthwhile, so the model was not economical.
Univariate sensitivity analysis and probabilistic sensitivity analysis were undertaken by varying the values of the parameters mentioned above, and we assessed the impact on the ICUR.
The values of model parameters are shown in Table 1.
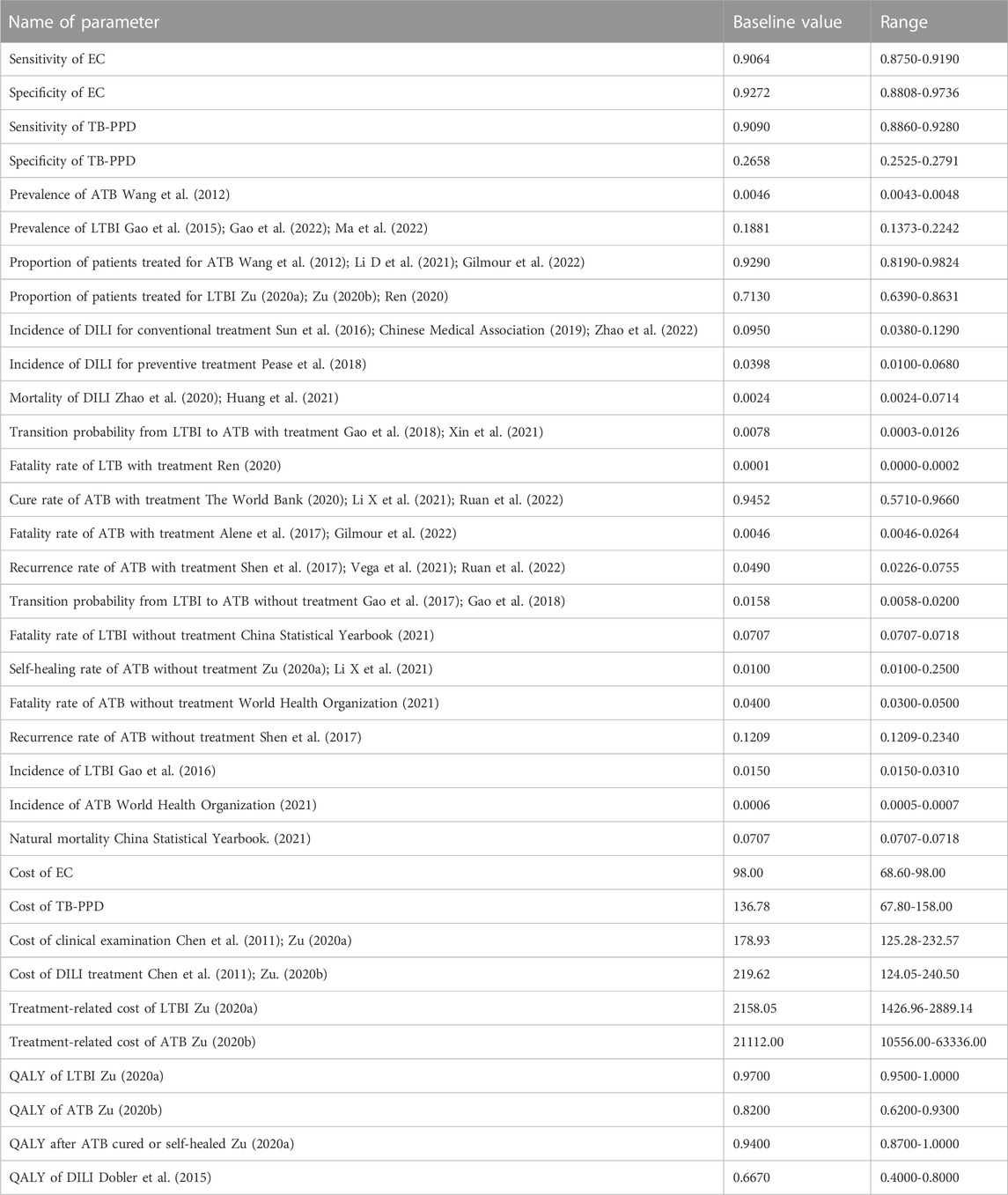
TABLE 1. Values of parameters
The total cost of the EC test was 7,607.5323 CNY. The total cost of the TB-PPD test was 15,430.5205 CNY. QALY in the EC test was 9.4645. QALY in the TB-PPD test was 9.3992. Compared with the TB-PPD test, the EC test had a lower cost but higher QALY. The ICUR was −119,800.7381 CNY/QALY. That is, for each additional QALY, the EC test could save 119,800.7381 CNY. The EC test was more economical than the TB-PPD test.
Univariate sensitivity analysis showed that the three parameters with the greatest impact on the result were: QALY of ATB; sensitivity of the EC test; fatality prevalence of ATB without treatment. The result was robust if these parameters fluctuated within the range (Figure 3).
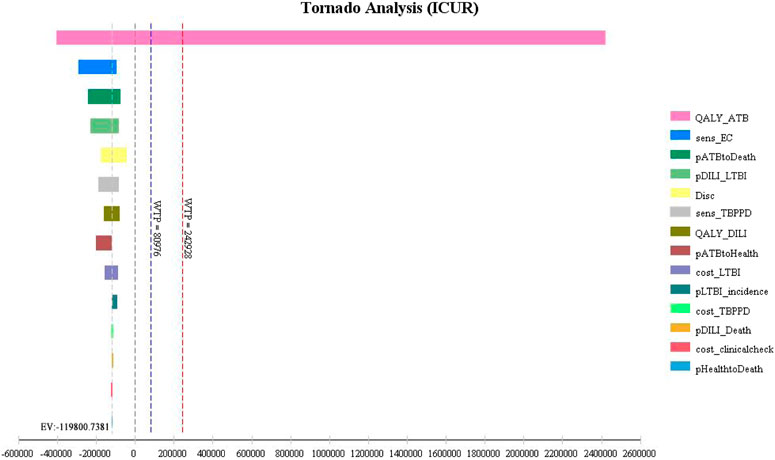
FIGURE 3. Tornado chart of univariate sensitivity analysis.
QALY_ATB: QALY of ATB; sens_EC: Sensitivity of EC; pATBtoDeath: Fatality rate of ATB without treatment; pDILI_LTBI: Incidence of DILI for preventive treatment; Disc; discount rate; sens_TBPPD: Sensitivity of TB-PPD; QALY_DILI: QALY of DILI; pATBtoHealth: Recurrence rate of ATB with treatment; cost_LTBI: Treatment-related cost of LTBI; pLTBI_incidence: Incidence of LTBI; cost_TBPPD: Cost of TB-PPD; pDILI_Death:Mortality of DILI; cost_clinicalcheck: Cost of clinical examination; pHealthtoDeath: Natural mortality.
Probabilistic sensitivity analysis showed that the acceptable probability of the EC test was always higher than that of TB-PPD test within the WTP threshold range (Figure 4). The probability of being economical in the EC test was 82.20% if WTP was equal to GDP per capita, but 92.80% if WTP was equal to 3-times GDP per capita (Figure 5).
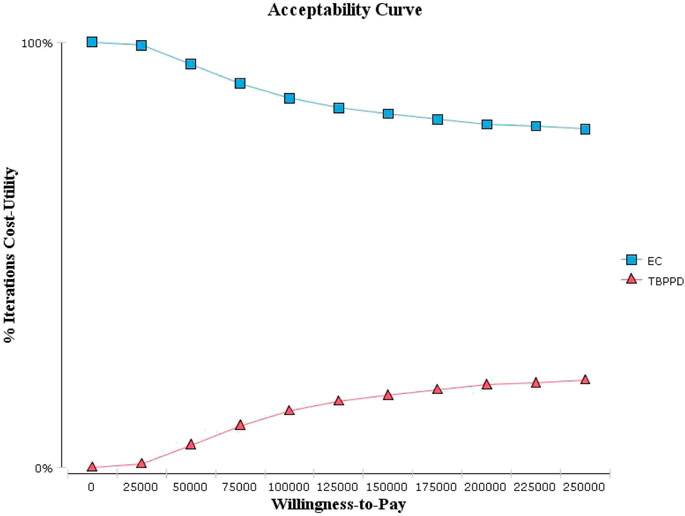
FIGURE 4. Acceptability curve of cost-utility analysis.
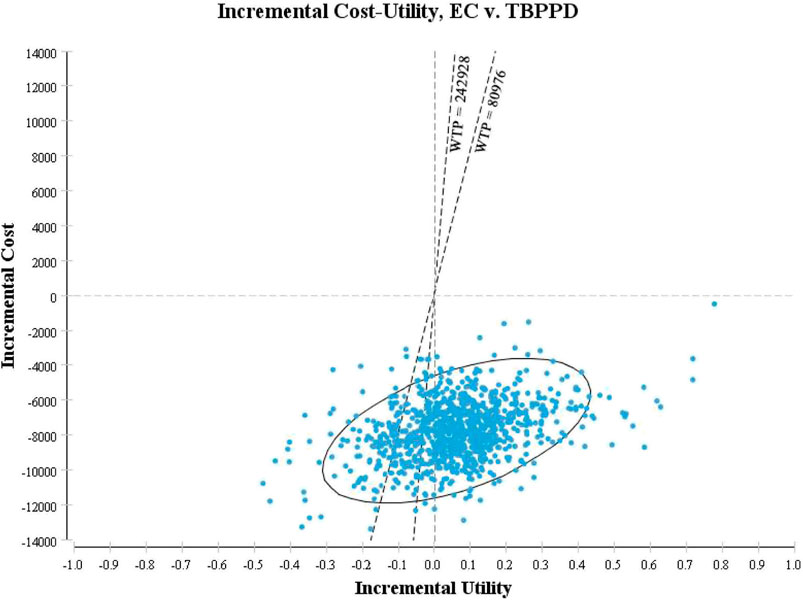
FIGURE 5. Scatter plot of cost-utility analysis.
EC: Recombinant Mycobacterium tuberculosis fusion protein (EC); TBPPD: Purified protein derivative of tuberculin (TB-PPD).
Tuberculosis is a major public-health problem worldwide. Early identification of patients suffering from tuberculosis and LTBI detection are the most important measures for prevention and control (Chinese Center for Disease Control and Prevention, 2021). The EC test is a new skin test for detection of MTB infection developed in China. The EC test has been shown to have higher specificity and to be able to distinguish MTB infection from BCG vaccination or other non-MTB infections effectively compared with that using the TB-PPD test (Zhou et al., 2021).
We evaluated the economic viability of using the EC test compared with using the TB-PPD test within the long-term (77 years). We discovered that the EC test was more economical for the diagnosis of MTB infection and subsequent treatment than the TB-PPD test according our study.
A “gold standard” for the diagnosis of LTBI is lacking. Hence, the diagnosis of LTBI can be made only by immunological detection methods such as the EC test or TB-PPD test. The accuracy of the detection method has a crucial and direct influence on the treatment paths of patients. Patients whose diagnosis has been missed will carry a poor prognosis due to a lack of appropriate examination and timely treatment. Healthy people who are misdiagnosed would have a higher economic burden and lower QALY compared with healthy people because they will have received inappropriate examination and treatment. The sensitivity of the EC test was similar to that of the TB-PPD test, but the EC test had higher specificity. Fewer people would be misdiagnosed using the EC test, and they would have lower costs and higher QALY, so the EC test is more economical.
According to the univariate sensitivity analysis, QALY of ATB, the sensitivity of the EC test, and the prevalence of fatality of ATB without treatment had the most prominent impact on the results. The result fluctuated greatly within the range of QALY of ATB, but the conclusion was consistent. If QALY of ATB ≤ 0.65, then the ICUR >3-times GDP per capita. This result meant that the TB-PPD test had higher costs and higher QALY compared with the EC test, but the increased costs were not worthwhile. If QALY of ATB >0.65, then the ICUR < 0. This result meant that the EC test had lower costs but higher QALY compared with the TB-PPD test. According to the probabilistic sensitivity analysis, the probability of the EC test being economical increased with increasing WTP thresholds. In summary, the result of the cost–utility analysis was robust.
The EC test was approved for marketing by China in 2020, but economic-evaluation studies related to the EC test are scarce. The WHO (World Health Organization, 2022) conducted a rapid evaluation in 2022 to compare the efficacy, safety and economy of three newer MTB antigen-based skin tests (TBSTs) compared with traditional TSTs and interferon-gamma release assays (IGRAs). The three TBSTs were C-Tb (Serum Institute of India, Pune, India), C-TST (known formerly as the ESAT6-CFP10 test; Anhui Zhifei Longcom, Anhui, China) and Diaskintest (Generium, Moscow, Russian Federation). The C-TST in China is EC mentioned in our study. TBSTs were more accurate and more economical compared with TSTs and IGRAs, though the safety was consistent with that of TSTs. Also, the WHO mentioned that economic evaluation of the EC test was insufficient. Steffen and others (Steffen et al., 2020) compared the cost-effectiveness of Diaskintest, EC test, TB-PPD test and QuantiFERON-TB Gold Plus (QFT-Plus) for the diagnosis of MTB in Brazilian HIV-infected patients by constructing a Markov model: Diaskintest was more economical than other methods. Diaskintest is a new skin test with the same methodology as the EC test developed in 2009 in Russia, but it has not been approved for marketing in China. Steffen and others (Steffen et al., 2020) showed that the EC test had the same effect as that of Diaskintest but had a higher cost. However, the cost of the EC test in China is lower, and we found it to be more economical.
Our study had two main limitations. First, the model parameters were taken from the average level of all age groups in China, so the results may not be applicable to a specific group. Second, the economic evaluation was conducted based only on a model because real-world studies are lacking. Therefore, carrying out an economic evaluation with a prospective study simultaneously would be the best option.
Compared with the TB-PPD test, the EC test would be more economical in the long term for the diagnosis of MTB infection according our study.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
ZL and HW contributed to the conception and design of the study. SD, ZL, DL, and XC designed the model and did the analysis. LZ, X-FJ, ZC, XN, and SH looked for the model parameters. SD and ZL wrote the manuscript. BW, DK, CW, and RZ gave vital clinical advice for the model construction. All authors revised it critically and gave their approval of the final version. All authors contributed to the article and approved the submitted version.
We thank the following experts who have given strong support to this research. Ying B (Department of Laboratory Medicine, West China Hospital, Sichuan University); Zhang H (Department of Infection Management, West China Hospital, Sichuan University); Miao L (Department of Pharmacy, The First Affiliated Hospital of Soochow University); Wang Z (Department of Pharmacy, Shanghai Changhai Hospital, Naval Medical University); Li X (Department of Pharmacy, Zhongshan Hospital, Fudan University); Liu M (Department of Pharmacy, Fujian Medical University Union Hospital); Cai B (Department of Pharmacy at The Second Affiliated Hospital, Harbin Medical University); Qiu F (Department of Pharmacy, The First Affiliated Hospital of Chongqing Medical University); Sun F (International Research Center for Medicinal Administration, Peking University); Chu N (Tuberculosis Department, Beijing Chest Hospital, Capital Medical University); Lin M (Department of Infection, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua University); Sha W (Department of Tuberculosis, Shanghai Pulmonary Hospital Affiliated to Tongji University).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Alene, K. A., Yi, H., Viney, K., McBryde, E. S., Yang, K., Bai, L., et al. (2017). Treatment outcomes of patients with multidrug-resistant and extensively drug resistant tuberculosis in Hunan Province, China. BMC Infect. Dis. 17, 573. doi:10.1186/s12879-017-2662-8
Chen, Q., Wang, L., Li, Y., Yang, X., and Li, D. (2011). Cost-effectiveness analysis of screening latent tuberculosis patients with interferon-gamma release assay. Chin. J. Evidence-Based Med. 11, 768–774. (in Chinese).
China Statistical Yearbook (2021). National bureau of statistics of people's Republic of China. Beijing: China Statistics Press. (in Chinese).
Chinese Center for Disease Control and Prevention (2021). Technical guidelines for prevention and control of tuberculosis in China. Beijing: People's Health Technology Press. (in Chinese).
Chinese Medical Association (2019). Guidelines for the diagnosis and treatment of anti-tuberculosis drug-induced liver injury(2019). Chin. J. Tuberc. Respir. 5, 343–356. (in Chinese).
Cui, X., Gao, L., and Cao, B. (2020). Management of latent tuberculosis infection in China: Exploring solutions suitable for high-burden countries. Int. J. Infect. Dis. 92S, S37–S40. doi:10.1016/j.ijid.2020.02.034
Dobler, C. C., Martin, A., and Marks, G. B. (2015). Benefit of treatment of latent tuberculosis infection in individual patients. Eur. Respir. J. 6, 1594–1595. doi:10.1183/13993003.00175-2016
Gao, L., Bai, L., Liu, J., Lu, W., Wang, X., Li, X., et al. (2016). Annual risk of tuberculosis infection in rural China: A population-based prospective study. Eur. Respir. J. 48, 168–178. doi:10.1183/13993003.00235-2016
Gao, L., Li, X., Liu, J., Wang, X., Lu, W., Bai, L., et al. (2017). Incidence of active tuberculosis in individuals with latent tuberculosis infection in rural China: Follow-up results of a population-based, multicentre, prospective cohort study. Lancet Infect. Dis. 17, 1053–1061. doi:10.1016/S1473-3099(17)30402-4
Gao, L., Lu, W., Bai, L., Wang, X., Xu, J., Catanzaro, A., et al. (2015). Latent tuberculosis infection in rural China: Baseline results of a population-based, multicentre, prospective cohort study. Lancet Infect. Dis. 15, 310–319. doi:10.1016/S1473-3099(14)71085-0
Gao, L., Zhang, H., Hu, M., Xu, C., and Xia, Y. (2022). Estimation of latent infection rate of mycobacterium tuberculosis in China based on multicenter survey data and spatial statistical model. Chin. J. Antituberc. 44, 54–59. (in Chinese).
Gao, L., Zhang, H., Xin, H., Liu, J., Pan, S., Li, W., et al. (2018). Short-course regimens of rifapentine plus isoniazid to treat latent tuberculosis infection in older Chinese patients: A randomised controlled study. Eur. Respir. J. 52, 1801470. doi:10.1183/13993003.01470-2018
GBD 2019 Diseases and Injuries Collaborators (2020). global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A systematic analysis for the global burden of disease study 2019. Lancet 396, 1204–1222. doi:10.1016/S0140-6736(20)30925-9(
Gilmour, B., Xu, Z., Bai, L., Alene, K. A., and Clements, A. C. A. (2022). Risk factors associated with unsuccessful tuberculosis treatment outcomes in Hunan Province, China. Trop. Med. Int. Health 27, 290–299. doi:10.1111/tmi.13720
He, W., Huang, X., and Zhen, L. (2018). Prevention and control of tuberculosis infection. Wuhan: Huazhong University of Science and Technology Press. (in Chinese).
Huang, J., Ye, M., and Zhou, X. (2021). Literature analysis of liver damage caused by anti-tuberculosis drugs from 2015 to 2020. Mod. Med. Clin. 36, 823–827. (in Chinese).
Li D, D., Yu, Y., Lu, Q., and Yao, Z. (2021). Analysis of current situation of drug-resistant tuberculosis treatment and cost of anti-tuberculosis drug treatment in Jiangxi Province. Mod. Prev. Med. 48, 3425–3429. (in Chinese).
Li X, X., Ruan, Y., Liu, X., Xu, C., Chen, W., Du, X., et al. (2021). Analysis of funding input and benefit output of tuberculosis prevention and control in China from 2011 to 2019. Chin. J. Antituberc. 43, 702–707. (in Chinese).
Ma, Y., Lu, W., Gao, L., Chu, N., Zhou, L., Cheng, S., et al. (2022). Promoting the quality and transparency of health research in China. Chin. J. Antituberc. 44, 209–217. (in Chinese). doi:10.1016/j.jclinepi.2022.10.004
Pai, M., Denkinger, C. M., Kik, S. V., Zwerling, A., Rangaka, M. X., Zwerling, A., et al. (2014). Gamma interferon release assays for detection of Mycobacterium tuberculosis infection. Clin. Microbiol. Rev. 27, 3–20. doi:10.1128/CMR.00034-13
Pease, C., Hutton, B., Yazdi, F., Wolfe, D., Hamel, C., Barbeau, P., et al. (2018). A systematic review of adverse events of rifapentine and isoniazid compared to other treatments for latent tuberculosis infection. Pharmacoepidemiol Drug Saf. 27, 557–566. doi:10.1002/pds.4423
Ren, Z. (2020). A study on the acceptability of preventive treatment in close contacts of pulmonary tuberculosis patients. Chinese Center for Disease Control and Prevention. (in Chinese).
Ruan, Q., Yang, Q., Sun, F., Liu, W., Shen, Y., Wu, J., et al. (2022). Recurrent pulmonary tuberculosis after treatment success: A population-based retrospective study in China. Clin. Microbiol. Infect. 28, 684–689. doi:10.1016/j.cmi.2021.09.022
Shen, X., Yang, C., Wu, J., Lin, S., Gao, X., Wu, Z., et al. (2017). Recurrent tuberculosis in an urban area in China: Relapse or exogenous reinfection? Tuberculosis 103, 97–104. doi:10.1016/j.tube.2017.01.007
Steffen, R. E., Pinto, M., Kritski, A., and Trajman, A. (2020). Cost-effectiveness of newer technologies for the diagnosis of Mycobacterium tuberculosis infection in Brazilian people living with HIV. Sci. Rep. 10, 21823. doi:10.1038/s41598-020-78737-w
Sun, Q., Zhang, Q., Gu, J., Sun, W. W., Wang, P., Bai, C., et al. (2016). Prevalence, risk factors, management, and treatment outcomes of first-line antituberculous drug-induced liver injury: A prospective cohort study. Pharmacoepidemiol Drug Saf. 25, 908–917. doi:10.1002/pds.3988
The World Bank (2020). Tuberculosis treatment success rate-China. Available from: https://data.worldbank.org/indicator/SH.TBS.CURE.ZS?locations=CN.
Vega, V., Rodríguez, S., Van der Stuyft, P., Stuyft, P. V., Seas, C., and Otero, L. (2021). Recurrent TB: A systematic review and meta-analysis of the incidence rates and the proportions of relapses and reinfections. Thorax 76, 494–502. doi:10.1136/thoraxjnl-2020-215449
Wang, N., Cheng, S., Chen, M., Zhao, Y., and Zhang, H. (2012). Report on the fifth national tuberculosis epidemiological sampling survey in 2010. Chin. J. Antituberc. 34, 485–508. (in Chinese).
World Health Organization (2022). Rapid communication: TB antigen-based skin tests for the diagnosis of TB infection.
World Health Organization (2020). WHO consolidated guidelines on tuberculosis: Tuberculosis preventive treatment.
Xin, H., Cao, X., Zhang, H., Feng, B., Du, Y., Zhang, B., et al. (2021). Protective efficacy of 6-week regimen for latent tuberculosis infection treatment in rural China: 5-year follow-up of a randomised controlled trial. Eur. Respir. J. 60, 2102359. doi:10.1183/13993003.02359-2021
Zhao, H., Wang, Y., Zhang, T., Wang, Q., and Xie, W. (2020). Drug-induced liver injury from anti-tuberculosis treatment: A retrospective cohort study. Med. Sci. Monit. 26, e920350. doi:10.12659/MSM.920350
Zhao, P., Chen, J., Yang, G., and Peng, Y. (2022). Construction of Nomogram risk prediction model for anti-tuberculosis drug-induced liver injury in hospitalized tuberculosis patients. Chin. J. Tuberc. Respir. 45, 171–176. (in Chinese). doi:10.3760/cma.j.cn112147-20210705-00467
Zhou, L., Chu, N., and Lu, W. (2021). Expert consensus on detection and preventive treatment of latent Mycobacterium tuberculosis infection in high-risk groups. Chin. J. Antituberc. 43, 874–878. (in Chinese).
Zu, X. (2020b). Acceptance of 6-month isoniazid prophylactic regimen alone among close contacts of pulmonary tuberculosis patients. Chin. Public Health 36, 369–374. (in Chinese).
Keywords: recombinant Mycobacterium tuberculosis fusion protein (EC), purified protein derivative of tuberculin (TB-PPD), Mycobacterium tuberculosis infection, decision tree-markov model, cost-utility
Citation: Diao S, Liu Z, Liu D, Cheng X, Zeng L, Jiao X-F, Chen Z, Ni X, He S, Wu B, Kang D, Wan C, Zhao R, Wang H and Zhang L (2023) Long-term economic evaluation of the recombinant Mycobacterium tuberculosis fusion protein (EC) test for the diagnosis of Mycobacterium tuberculosis infection. Front. Pharmacol. 14:1161526. doi: 10.3389/fphar.2023.1161526
Received: 08 February 2023; Accepted: 05 May 2023;
Published: 16 May 2023.
Edited by:
Sabrina Ingrid Green, KU Leuven, BelgiumReviewed by:
Katiany Rizzieri Caleffi Ferracioli, State University of Maringá, BrazilCopyright © 2023 Diao, Liu, Liu, Cheng, Zeng, Jiao, Chen, Ni, He, Wu, Kang, Wan, Zhao, Wang and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Huiqing Wang, MTM2NjgxMzYyNThAMTYzLmNvbQ==; Lingli Zhang, emhhbmdsaW5nbGlAc2N1LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.