
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Pharmacol., 23 March 2023
Sec. Pharmacology of Anti-Cancer Drugs
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1154377
This article is part of the Research TopicChronic Myeloid Leukemia: From Targeted Therapy to Treatment-Free RemissionView all 9 articles
 A. Iurlo1*
A. Iurlo1* D. Cattaneo1,2
D. Cattaneo1,2 D. Consonni3
D. Consonni3 F. Castagnetti4
F. Castagnetti4 M. C. Miggiano5
M. C. Miggiano5 G. Binotto6
G. Binotto6 M. Bonifacio7
M. Bonifacio7 G. Rege-Cambrin8
G. Rege-Cambrin8 M. Tiribelli9F. Lunghi10A. Gozzini11P. Pregno12
M. Tiribelli9F. Lunghi10A. Gozzini11P. Pregno12 E. Abruzzese13
E. Abruzzese13 I. Capodanno14
I. Capodanno14 C. Bucelli1
C. Bucelli1 M. Pizzuti15S. Artuso1M. Iezza4
M. Pizzuti15S. Artuso1M. Iezza4 E. Scalzulli16
E. Scalzulli16 G. La Barba17A. Maggi18S. Russo19
G. La Barba17A. Maggi18S. Russo19 C. Elena20A. R. Scortechini21
C. Elena20A. R. Scortechini21 A. Tafuri22
A. Tafuri22 R. Latagliata23
R. Latagliata23 G. Caocci24
G. Caocci24 M. Bocchia25S. Galimberti26
M. Bocchia25S. Galimberti26 L. Luciano27
L. Luciano27 C. Fava28R. Foà16
C. Fava28R. Foà16 G. Saglio28G. Rosti29
G. Saglio28G. Rosti29 M. Breccia16
M. Breccia16TKIs long-term treatment in CML may lead to persistent adverse events (AEs) that can promote relevant morbidity and mortality. Consequently, TKIs dose reduction is often used to prevent AEs. However, data on its impact on successful treatment-free remission (TFR) are quite scarce. We conducted a retrospective study on the outcome of CML subjects who discontinued low-dose TKIs from 54 Italian hematology centers participating in the Campus CML network. Overall, 1.785 of 5.108 (35.0%) regularly followed CML patients were treated with low-dose TKIs, more frequently due to relevant comorbidities or AEs (1.288, 72.2%). TFR was attempted in 248 (13.9%) subjects, all but three while in deep molecular response (DMR). After a median follow-up of 24.9 months, 172 (69.4%) patients were still in TFR. TFR outcome was not influenced by gender, Sokal/ELTS risk scores, prior interferon, number and last type of TKI used prior to treatment cessation, DMR degree, reason for dose reduction or median TKIs duration. Conversely, TFR probability was significantly better in the absence of resistance to any prior TKI. In addition, patients with a longer DMR duration before TKI discontinuation (i.e., >6.8 years) and those with an e14a2 BCR::ABL1 transcript type showed a trend towards prolonged TFR. It should also be emphasized that only 30.6% of our cases suffered from molecular relapse, less than reported during full-dose TKI treatment. The use of low-dose TKIs does not appear to affect the likelihood of achieving a DMR and thus trying a treatment withdrawal, but might even promote the TFR rate.
The therapeutic armamentarium of chronic myeloid leukemia (CML) has greatly improved after small molecule tyrosine kinase inhibitors (TKIs) targeting BCR::ABL1 became available. The 10-year survival rate in CML-chronic phase increased from about 20% to 80%–90%, allowing for near-normal life expectancy (Bower et al., 2016).
While highly effective, these drugs also have an often mild to moderate, but sometimes severe, toxicity profile. Indeed, long-term treatment with TKIs may lead to chronic adverse events (AEs) that can negatively affect patients’ quality of life (QoL) and can promote relevant morbidity and mortality. In particular, there has been increasing evidence of more serious AEs with second- or third-generation TKIs, such as pleural effusion and pulmonary arterial hypertension with dasatinib (Campbell and Copland, 2013), hyperglycemia, dyslipidemia and arterial occlusive events (AOEs) with nilotinib (Emir et al., 2013; Hiwase et al., 2013), gastrointestinal toxicities with bosutinib (Cortes et al., 2012), and hypertension, AOEs and pancreatic dysfunction with ponatinib (Cortes et al., 2018).
Dose reductions due to AEs are part of the daily management of TKIs (Copland, 2019): often these dose reductions are kept stable over the long term, particularly in patients who have already achieved a durable response. This optimization of the TKI dose is related to better adherence, improved QoL and in most cases do not jeopardize a stable response once achieved, thus confirming, as studies on intermittent TKI treatment have already shown (Russo et al., 2013; Malagola et al., 2021), that responding patients are often overtreated. Furthermore, as also demonstrated by the UK DESTINY study (Clark et al., 2017; Clark et al., 2019) and real-world data from Hammersmith Hospital (Claudiani et al., 2021), a TKI de-escalation strategy, in addition to not compromising the possibility of treatment discontinuation, could also improve the success of treatment-free remission (TFR) protocols.
However, while discontinuing therapy appears as a safe option for approximately half of the patients obtaining an optimal response (Ross and Hughes, 2020), so far, data on the impact of long-term TKI dose de-escalation on successful TFR are rather scarce.
The aim of our study was therefore to evaluate the propensity of Italian hematologists to attempt TFR in CML patients treated with low-dose TKIs, both at diagnosis and during follow-up.
We conducted a retrospective analysis on the outcome of CML patients who discontinued low-dose TKIs between May 2010 and September 2022 from 54 Italian hematology centers participating to the “Campus CML”, an active research network of physicians involved in CML management throughout Italy, with the aim of investigating different aspects of the disease (Iurlo et al., 2022).
Each center was asked to complete an online survey which included questions regarding the use of low-dose TKIs in real-life clinical practice and the willingness of physicians to offer TFR even to subjects treated with reduced doses of TKI for AEs and/or relevant comorbidities or to patients who have already achieved an optimal molecular response.
The following key disease characteristics were then required for each patient attempting TFR after low-dose TKI treatment: socio-demographic variables, risk scores (i.e., Sokal and ELTS), all treatments (including interferon) before and after discontinuation, duration of each treatment, reasons for dose reduction, and best response to each treatment.
Molecular monitoring and classification of responses were defined according to current ELN recommendations (Hochhaus et al., 2020): in particular, major molecular response (MMR) as a BCR::ABL/ABL ratio ≤ 0.1%, and deep molecular response (DMR) as MR4 (BCR::ABL1/ABL ratio ≤ 0.01%), MR4.5 (BCR::ABL1/ABL ratio ≤ 0.0032%), or MR5 (BCR::ABL1/ABL ratio ≤ 0.001%). Molecular relapse was defined as loss of MMR. Consequently, TFR was calculated from TKI discontinuation to loss of MMR.
Follow-up began on the day of TKI discontinuation and ended at the earliest of molecular relapse or 31 December 2022. As only 65 (26.2%) patients were followed up for more than 4 years and no molecular recurrence was observed among them, we truncated follow-up time at 4 years.
We analyzed time since to molecular relapse based on selected variables using the Kaplan-Meier survivor function and the log-rank-test. Statistical analyses were performed with Stata 17 (StataCorp. 2021).
Overall, 1.785 of 5.108 (35.0%) regularly followed CML-chronic phase patients were treated with low-dose TKIs. More specifically, a TKI dose reduction was reported in 727 (27.5%) out of 2.648 patients treated with imatinib, 362/1.133 (32.0%) with nilotinib, 304/813 (37.4%) with dasatinib, 213/294 (72.5%) with bosutinib and 179/220 (81.4%) with ponatinib. The TKI dose was reduced in the majority of patients (1.288, 72.2%) due to AEs (916, 51.3%) or relevant comorbidities (372, 20.8%), while in the remaining subjects (497, 27.8%) TKIs were reduced for physicians’ decision, after obtaining a stable molecular response (MMR/DMR), with the aim of preventing the development of AEs, thereby improving TKIs tolerability. No progression toward advanced-phase disease was observed during treatment with low-dose TKIs.
TFR was attempted in 248 (13.9%) out of 1.785 patients, 138 of whom were female and 110 were male, with a median age at CML diagnosis of 49.3 years (Table 1). As expected, dose reduction was due to AEs in more than half of the cases (149 patients, 60.1%), while in the remaining subjects TKIs were reduced after reaching an optimal molecular response (Supplementary Table S1). Interestingly, 47 (18.9%) patients experienced TKI resistance before treatment discontinuation, in the absence of any BCR::ABL1 kinase domain mutation.
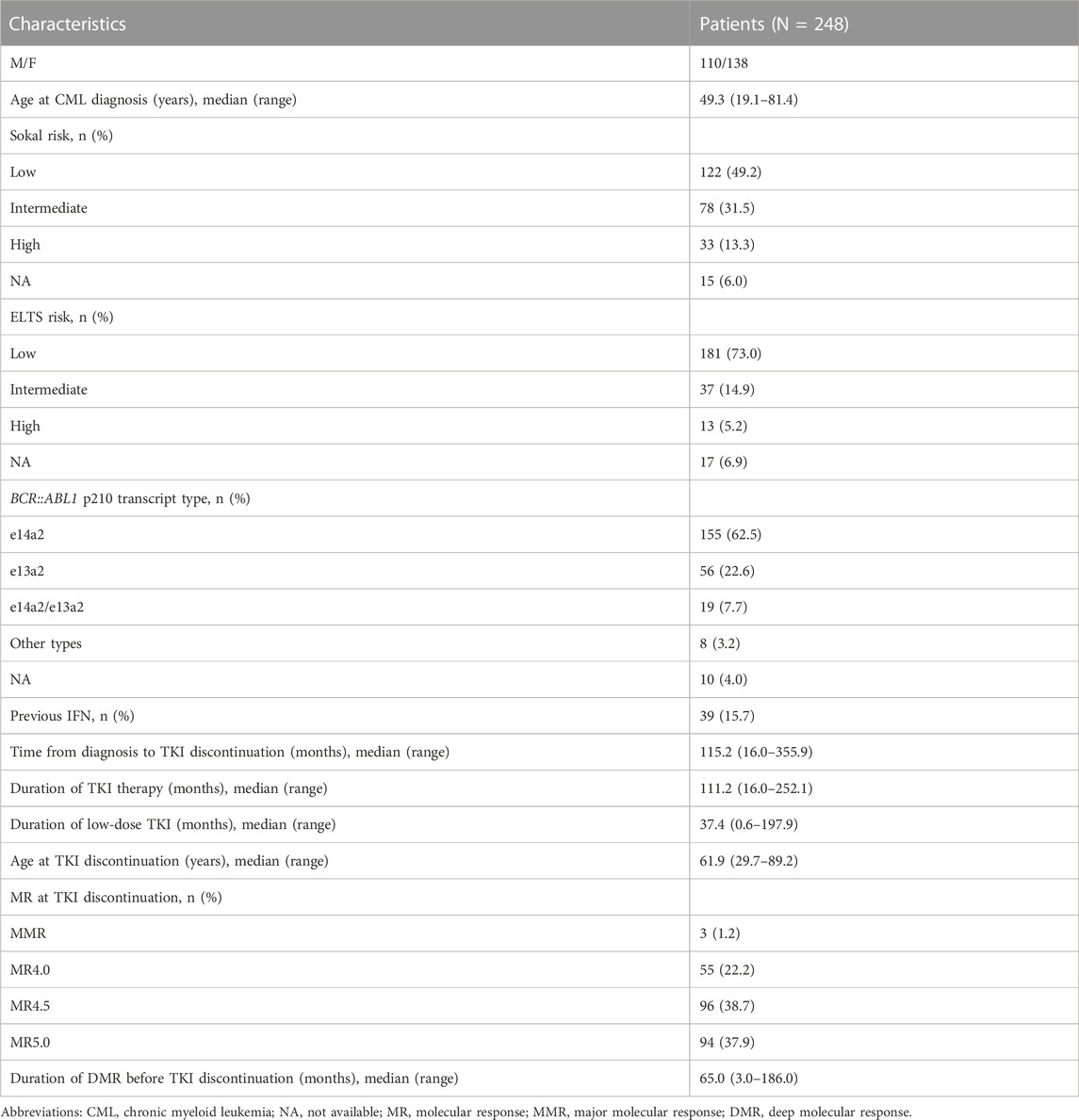
TABLE 1. Baseline demographics and clinical characteristics of 248 CML patients.
The most widely used low-dose TKI before attempting TFR was imatinib (99 patients out of 727–13.6%), followed by nilotinib (90 patients out of 362–24.9%), dasatinib (51 patients out of 304–16.8%) and, to a lesser extent, ponatinib (five patients out 179–2.8%) and bosutinib (three patients out of 213–1.4%). Overall, 117 (47.2%) patients experienced a ≥ 50% reduction in TKI dose from baseline (Supplementary Table S2).
Before attempting TFR, 152 (61.3%) patients were treated with a single TKI, while 80 and 16 patients had received second or later-line therapy, respectively, with a median TKI treatment duration of 111.2 months (range, 16.0–252.1). At the time of TFR, 245 (98.8%) patients had already achieved a DMR, with a median duration of 65.0 months (range, 3.0–186.0).
After a median follow-up from TKIs discontinuation of 24.9 months (range, 1.1–149.2), 172 (69.4%) patients were still in TFR (Figure 1). Interestingly, TFR outcome was not affected by any of the following parameters (Supplementary Table S3): gender, Sokal or ELTS risk scores, prior interferon treatment, number and last type of TKIs used before discontinuation of therapy, degree of DMR (i.e., MR4 vs. MR4.5 or better), reason for dose reduction (i.e., AEs vs. DMR achievement) or median duration of therapy with TKIs (Supplementary Figures S1, S2). In contrast, TFR was markedly better in the absence of a history of resistance to any previous TKI (Table 2; Figure 2); furthermore, as expected, patients with a longer DMR duration (i.e., >6.8 years) (Supplementary Figure S2) and those with an e14a2 BCR::ABL1 transcript type showed a trend toward prolonged TFR (Table 2).

FIGURE 1. Treatment-free remission (TFR) after tyrosine kinase inhibitor (TKI) therapy (Kaplan-Meier survivor function).
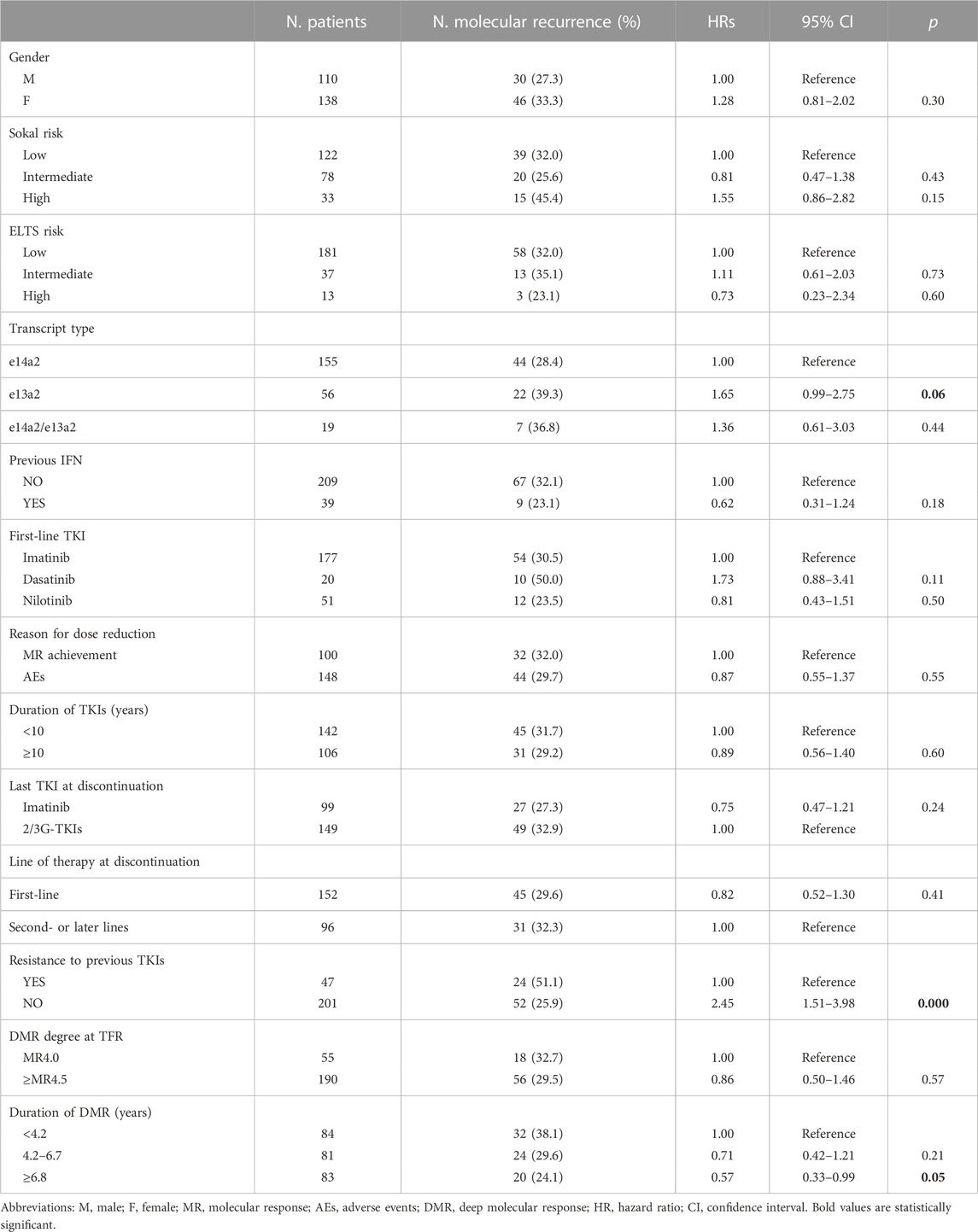
TABLE 2. Molecular recurrence risk and hazard ratios from univariate Cox models according to selected variables.
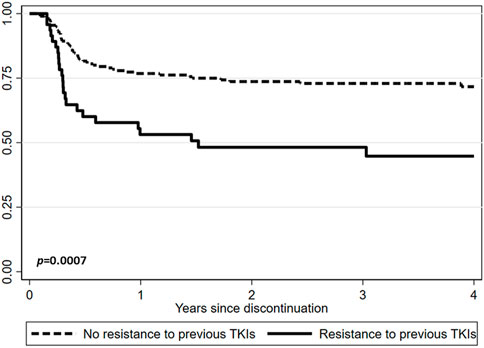
FIGURE 2. Treatment-free remission (TFR) after tyrosine kinase inhibitor (TKI) therapy (Kaplan-Meier survivor function) according to resistance to previous TKIs.
Seventy-six (30.6%) patients experienced molecular recurrence (≤MMR) after a median time from treatment interruption of 4.1 months (range, 0.8–47.3), representing an early relapse (within 6 months) in 54/76 patients (71.1%). All of these cases who had a molecular relapse restarted the same dose of TKI treatments they had before the TFR attempt and regained at least an MMR within 8 months of TKI resumption.
In this large, real-life series of CML patients regularly followed in Italy, TKIs treatment at a reduced dose represents an important reality, being bosutinib and ponatinib the drugs that most frequently required a dose reduction. More notably, TKI treatment has usually been initiated at full dose (excluding the elderly or patients with relevant comorbidities), with nearly 30% of TKI dose reductions performed in clinical practice with the goal of long-term treatment improvement once an optimal molecular response has been obtained, while at the same time preventing the development of AEs, thus improving TKIs tolerability.
Indeed, it should be emphasized that TKI dose optimization should be taken into account from the outset as, after the development of chronic toxicities, the true possibility of complete resolution of AEs is still a matter of debate, especially in some specific contexts (Okamoto et al., 2020).
In fact, while all the information on the prescription of TKIs used in CML treatment indicate a starting dose and rules and suggestions for transiently suspending or reducing the dose in case of clinical and biochemical AEs, suggesting a return to the ideal dose once the AEs disappear or alleviate, in daily clinical practice many physicians prescribe TKI starting dose lower than those foreseen in the product information in case of patients of advanced age or with relevant comorbidities. Furthermore, when an AEs improves or disappears, the TKI is maintained at a reduced dose over the long term, essentially to avoid recurrence of the same AE or, generically, to promote a better QoL and to ensure or reassure a good adherence, thus allowing a broader use of even those second- or third-generation TKIs not adequately indicated in the presence of specific comorbidities (Iurlo et al., 2021).
Furthermore, while most studies of TFR in CML subjects abruptly discontinued TKIs, more recently some authors have evaluated a new treatment strategy based on gradual therapy withdrawal before TKI interruption in the context of clinical trials or real-life experiences (Clark et al., 2017; Clark et al., 2019; Cayssials et al., 2020; Claudiani et al., 2021): among others, the DESTINY study examined TKI de-escalation treatment in 174 patients with stable MMR or MR4, after at least 3 years of treatment with full-dose imatinib, nilotinib, or dasatinib (Clark et al., 2017). There was no progression or cytogenetic recurrence, with monthly monitoring allowing rapid identification of all cases of molecular relapse. Furthermore, chronic AEs improved in most cases (Clark et al., 2019).
More recently, the prospective, multicenter phase II DANTE study (NCT03874858) aimed to evaluate the safety of first-line nilotinib de-escalation and its impact on TFR success in Italian CML-chronic phase subjects. While in a previously interim analysis 1 year of nilotinib de-escalation prior to TFR in patients with stable DMR was shown to be safe and effective (Breccia et al., 2021), a molecular recurrence rate of approximately 32% 1 year after stopping nilotinib was reported, thus demonstrating that de-escalation of this drug before attempting TFR may be a successful dose optimization strategy (Stagno et al., 2022).
Accordingly, we then evaluated the potential effect of low-dose TKIs on TFR outcome in a large real-life series of 248 CML-chronic phase patients managed in Italy.
In this context, as already reported in a previous paper (Iurlo et al., 2022), we confirm in a larger patients’ population that the use of low-dose TKIs does not seem to affect the possibility of achieving a DMR and therefore attempting a suspension of therapy.
While being aware of the limitations of this study, mainly represented by its retrospective nature, it should be emphasized that only 30.6% of our cases suffered from molecular relapse, less than reported in patients previously treated with full-dose TKIs (Hernández-Boluda et al., 2018; Fava et al., 2019).
In addition, we have now demonstrated that the only clinical variable associated with molecular recurrence was resistance to prior TKIs (Figure 2), thus confirming observations from previous studies, for example, the DADI trial in which patients who switched to dasatinib because of resistance to imatinib had worse outcomes than those who switched for other reasons (Imagawa et al., 2015). Similarly, in the more recent STOP 2G-TKI French study a history of suboptimal response or resistance to imatinib prior to dasatinib or nilotinib was the only baseline factor associated with significantly worse TFR (Rea et al., 2017). Consequently, it must be admitted that in this context only a select subset of patients has the possibility of achieving a successful TFR, probably for a less aggressive disease.
In fact, approximately 14.0% of our patients treated with TKIs at a reduced dose were considered eligible to discontinue therapy, thus demonstrating that TFR was not compromised using low-dose TKIs. Furthermore, treatment dose adjustments have important prognostic implications even in those patients who do not wish to attempt TFR, with the clinical potential to reduce both therapy-related AEs and overall treatment costs without jeopardizing the possibility of maintaining a good response.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
AI conceptualized and designed the study. AI, DCa, FC, MM, GB, MBn, GR-C, MT, FL, AG, PP, EA, IC, CB, MP, SA, MI, ES, GL, AM, SR, CE, AS, AT, RL, GC, MBc, SG, LL, CF, RF, GS, GR, and MBr. collected and assembled the data. DCo performed the statistical analysis. AI and DCa wrote the manuscript. RF, GS, GR, and MBr. critically reviewed the manuscript. AI, DCa, DCo, FC, MM, GB, MBn, GR-C, MT, FL, AG, PP, EA, IC, CB, MP, SA, MI, ES, GL, AM, SR, CE, AS, AT, RL, GC, MBc, SG, LL, CF, RF, GS, GR, and MBr approved the final version of the manuscript.
This study was partially funded by Italian Ministry of Health—Current research IRCCS.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1154377/full#supplementary-material
SUPPLEMENTARY FIGURE S1 | Treatment-free remission (TFR) after tyrosine kinase inhibitor (TKI) therapy (Kaplan-Meier survivor function). (A) TFR according to gender. (B) TFR according to pretreatment with interferon. (C) TFR according to Sokal risk score. (D) TFR according to TKIs used before therapy cessation.
SUPPLEMENTARY FIGURE S2 | Treatment-free remission (TFR) after tyrosine kinase inhibitor (TKI) therapy (Kaplan-Meier survivor function). (A) TFR according to BCR::ABL1 transcript type. (B) TFR according to lines of therapy. (C) TFR according to median duration of TKIs therapy. (D) TFR according to median duration of DMR. (E) TFR according to the degree of DMR. (F) TFR according to the main reason for TKIs dose reduction.
Bower, H., Björkholm, M., Dickman, P. W., Höglund, M., Lambert, P. C., and Andersson, T. M. (2016). Life expectancy of patients with chronic myeloid leukemia approaches the life expectancy of the general population. J. Clin. Oncol. 34, 2851–2857. doi:10.1200/JCO.2015.66.2866
Breccia, M., Abruzzese, E., Stagno, F., Iurlo, A., Pane, F., Attolica, I., et al. (2021). First interim analysis of the Italian dante study: De-escalation before treatment-free remission in patients with chronic myeloid leukemia treated with first-line nilotinib. Blood 138, 1474. doi:10.1182/blood-2021-145411
Campbell, V. E., and Copland, M. (2013). Dasatinib for the treatment of chronic phase chronic myeloid leukemia. Clin. Pract. 10, 415–425. doi:10.2217/cpr.13.43
Cayssials, E., Torregrosa-Diaz, J., Gallego-Hernanz, P., Tartarin, F., Systchenko, T., Maillard, N., et al. (2020). Low-dose tyrosine kinase inhibitors before treatment discontinuation do not impair treatment-free remission in chronic myeloid leukemia patients: Results of a retrospective study. Cancer 126, 3438–3447. doi:10.1002/cncr.32940
Clark, R. E., Polydoros, F., Apperley, J. F., Milojkovic, D., Pocock, C., Smith, G., et al. (2017). De-escalation of tyrosine kinase inhibitor dose in patients with chronic myeloid leukaemia with stable major molecular response (DESTINY): An interim analysis of a non-randomised, phase 2 trial. Lancet Haematol. 4, e310–e316. doi:10.1016/S2352-3026(17)30066-2
Clark, R. E., Polydoros, F., Apperley, J. F., Milojkovic, D., Rothwell, K., Pocock, C., et al. (2019). De-escalation of tyrosine kinase inhibitor therapy before complete treatment discontinuation in patients with chronic myeloid leukaemia (DESTINY): A non-randomised, phase 2 trial. Lancet Haematol. 6, e375–e383. doi:10.1016/S2352-3026(19)30094-8
Claudiani, S., Apperley, J. F., Szydlo, R., Khan, A., Nesr, G., Hayden, C., et al. (2021). TKI dose reduction can effectively maintain major molecular remission in patients with chronic myeloid leukaemia. Br. J. Haematol. 193, 346–355. doi:10.1111/bjh.17286
Copland, M. (2019). Is there a role for dose modification of TKI therapy in CML? Curr. Hematol. Malig. Rep. 14, 337–345. doi:10.1007/s11899-019-00524-w
Cortes, J. E., Kim, D. W., Kantarjian, H. M., Brummendorf, T. H., Dyagil, I., Griskevicius, L., et al. (2012). Bosutinib versus imatinib in newly diagnosed chronic-phase chronic myeloid leukemia: Results from the BELA trial. J. Clin. Oncol. 30, 3486–3492. doi:10.1200/JCO.2011.38.7522
Cortes, J. E., Kim, D. W., Pinilla-Ibarz, J., le Coutre, P. D., Paquette, R., Chuah, C., et al. (2018). Ponatinib efficacy and safety in Philadelphia chromosome-positive leukemia: Final 5-year results of the phase 2 PACE trial. Blood 132, 393–404. doi:10.1182/blood-2016-09-739086
Emir, H., Albrecht-Schgoer, K., Huber, K., Grebien, F., Eisenwort, G., Schgoer, W., et al. (2013). Nilotinib exerts direct pro-atherogenic and antiangiogenic effects on vascular endothelial cells: A potential explanation for drug-induced vasculopathy in CML. Blood 122, 257. doi:10.1182/blood.v122.21.257.257
Fava, C., Rege-Cambrin, G., Dogliotti, I., Cerrano, M., Berchialla, P., Dragani, M., et al. (2019). Observational study of chronic myeloid leukemia Italian patients who discontinued tyrosine kinase inhibitors in clinical practice. Haematologica 104, 1589–1596. doi:10.3324/haematol.2018.205054
Hernández-Boluda, J. C., Pereira, A., Pastor-Galán, I., Alvarez-Larrán, A., Savchuk, A., Puerta, J. M., et al. (2018). Feasibility of treatment discontinuation in chronic myeloid leukemia in clinical practice: Results from a nationwide series of 236 patients. Blood Cancer J. 8, 91. doi:10.1038/s41408-018-0125-0
Hiwase, D. K., Carne, L., Ross, D., Grigg, A., and Hughes, T. P. (2013). Hypercholesterolemia in imatinib intolerant/resistant CML-CP patients treated with nilotinib: A retrospective analysis. Blood 122, 1503. doi:10.1182/blood.v122.21.1503.1503
Hochhaus, A., Baccarani, M., Silver, R. T., Schiffer, C., Apperley, J. F., Cervantes, F., et al. (2020). European leukemianet 2020 recommendations for treating chronic myeloid leukemia. Leukemia 34, 966–984. doi:10.1038/s41375-020-0776-2
Imagawa, J., Tanaka, H., Okada, M., Nakamae, H., Hino, M., Murai, K., et al. (2015). Discontinuation of dasatinib in patients with chronic myeloid leukaemia who have maintained deep molecular response for longer than 1 year (DADI trial): A multicentre phase 2 trial. Lancet Haematol. 2, e528–e535. doi:10.1016/S2352-3026(15)00196-9
Iurlo, A., Cattaneo, D., Bucelli, C., and Breccia, M. (2021). Dose optimization of tyrosine kinase inhibitors in chronic myeloid leukemia: A new therapeutic challenge. J. Clin. Med. 10, 515. doi:10.3390/jcm10030515
Iurlo, A., Cattaneo, D., Artuso, S., Consonni, D., Abruzzese, E., Binotto, G., et al. (2022). Treatment-free remission in chronic myeloid leukemia patients treated with low-dose TKIs: A feasible option also in the real-life. A Campus CML study. Front. Oncol. 12, 839915. doi:10.3389/fonc.2022.839915
Malagola, M., Iurlo, A., Abruzzese, E., Bonifacio, M., Stagno, F., Binotto, G., et al. (2021). Molecular response and quality of life in chronic myeloid leukemia patients treated with intermittent TKIs: First interim analysis of OPTkIMA study. Cancer Med. 10, 1726–1737. doi:10.1002/cam4.3778
Okamoto, S., Ureshino, H., Kawaguchi, A., Miyazono, M., Ikeda, Y., and Kimura, S. (2020). Assessment of estimated glomerular filtration rate in patients with chronic myeloid leukemia following discontinuation of tyrosine kinase inhibitors. Int. J. Hematol. 112, 41–45. doi:10.1007/s12185-020-02880-3
Rea, D., Nicolini, F. E., Tulliez, M., Guilhot, F., Guilhot, J., Guerci-Bresler, A., et al. (2017). Discontinuation of dasatinib or nilotinib in chronic myeloid leukemia: Interim analysis of the STOP 2G-TKI study. Blood 129, 846–854. doi:10.1182/blood-2016-09-742205
Ross, D. M., and Hughes, T. P. (2020). Treatment-free remission in patients with chronic myeloid leukaemia. Nat. Rev. Clin. Oncol. 17, 493–503. doi:10.1038/s41571-020-0367-1
Russo, D., Martinelli, G., Malagola, M., Skert, C., Soverini, S., Iacobucci, I., et al. (2013). Effects and outcome of a policy of intermittent imatinib treatment in elderly patients with chronic myeloid leukemia. Blood 121, 5138–5144. doi:10.1182/blood-2013-01-480194
Stagno, F., Abruzzese, E., Iurlo, A., Pane, F., Attolico, I., Sportoletti, P., et al. (2022). Treatment-free remission outcome in patients with chronic myeloid leukemia in chronic phase following one year of nilotinib de-escalation: 96-Week update of dante study. Blood 140, 9614–9616. doi:10.1182/blood-2022-157700
Keywords: chronic myeloid leukemia, tyrosine kinase inhibitors, treatment-free remission, low dose, resistance, outcome
Citation: Iurlo A, Cattaneo D, Consonni D, Castagnetti F, Miggiano MC, Binotto G, Bonifacio M, Rege-Cambrin G, Tiribelli M, Lunghi F, Gozzini A, Pregno P, Abruzzese E, Capodanno I, Bucelli C, Pizzuti M, Artuso S, Iezza M, Scalzulli E, La Barba G, Maggi A, Russo S, Elena C, Scortechini AR, Tafuri A, Latagliata R, Caocci G, Bocchia M, Galimberti S, Luciano L, Fava C, Foà R, Saglio G, Rosti G and Breccia M (2023) Treatment discontinuation following low-dose TKIs in 248 chronic myeloid leukemia patients: Updated results from a campus CML real-life study. Front. Pharmacol. 14:1154377. doi: 10.3389/fphar.2023.1154377
Received: 30 January 2023; Accepted: 14 March 2023;
Published: 23 March 2023.
Edited by:
Michele Massimino, University of Catania, ItalyReviewed by:
Dragana Milojkovic, Imperial College London, United KingdomCopyright © 2023 Iurlo, Cattaneo, Consonni, Castagnetti, Miggiano, Binotto, Bonifacio, Rege-Cambrin, Tiribelli, Lunghi, Gozzini, Pregno, Abruzzese, Capodanno, Bucelli, Pizzuti, Artuso, Iezza, Scalzulli, La Barba, Maggi, Russo, Elena, Scortechini, Tafuri, Latagliata, Caocci, Bocchia, Galimberti, Luciano, Fava, Foà, Saglio, Rosti and Breccia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: A. Iurlo, YWxlc3NhbmRyYS5pdXJsb0Bwb2xpY2xpbmljby5taS5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.