 Beatriz Dietl1
Beatriz Dietl1 Lucía Boix-Palop1,2*Laura Gisbert1Aina Mateu1
Lucía Boix-Palop1,2*Laura Gisbert1Aina Mateu1 Gemma Garreta3Mariona Xercavins4Cristina Badía1María López-Sánchez5Josefa Pérez4
Gemma Garreta3Mariona Xercavins4Cristina Badía1María López-Sánchez5Josefa Pérez4 Esther Calbo1,2*
Esther Calbo1,2*- 1Department of Infectious Diseases, Hospital Universitari Mútua de Terrassa, Barcelona, Spain
- 2Faculty of Medicine, Infectious Diseases, Universitat Internacional de Catalunya, Barcelona, Spain
- 3Department of Clinical Pharmacy, Hospital Universitari Mútua de Terrassa, Barcelona, Spain
- 4CatLab, Department of Microbiology, Barcelona, Spain
- 5Infection Control Nursing Team, Hospital Universitari Mútua de Terrassa, Barcelona, Spain
Introduction: Bloodstream infections (BSI) are a major cause of mortality all over the world. Inappropriate empirical antimicrobial treatment (i-EAT) impact on mortality has been largely reported. However, information on related factors for the election of i-EAT in the treatment of BSI in adults is lacking. The aim of the study was the identification of risk-factors associated with the use of i-EAT in BSI.
Methods: A retrospective, observational cohort study, from a prospective database was conducted in a 400-bed acute-care teaching hospital including all BSI episodes in adult patients between January and December 2018. The main outcome variable was EAT appropriation. Multivariate analysis using logistic regression was performed.
Results: 599 BSI episodes were included, 146 (24%) received i-EAT. Male gender, nosocomial and healthcare-associated acquisition of infection, a high Charlson Comorbidity Index (CCI) score and the isolation of multidrug resistant (MDR) microorganisms were more frequent in the i-EAT group. Adequation to local guidelines’ recommendations on EAT resulted in 91% of appropriate empirical antimicrobial treatment (a-EAT). Patients receiving i-EAT presented higher mortality rates at day 14 and 30 when compared to patients with a-EAT (14% vs. 6%, p = 0.002 and 22% vs. 9%, p < 0.001 respectively). In the multivariate analysis, a CCI score ≥3 (OR 1.90 (95% CI 1.16–3.12) p = 0.01) and the isolation of a multidrug resistant (MDR) microorganism (OR 3.79 (95% CI 2.28–6.30), p < 0.001) were found as independent risk factors for i-EAT. In contrast, female gender (OR 0.59 (95% CI 0.35–0.98), p = 0.04), a correct identification of clinical syndrome prior to antibiotics administration (OR 0.26 (95% CI 0.16–0.44), p < 0.001) and adherence to local guidelines (OR 0.22 (95% CI 0.13–0.38), p < 0.001) were identified as protective factors against i-EAT.
Conclusion: One quarter of BSI episodes received i-EAT. Some of the i-EAT related factors were unmodifiable (male gender, CCI score ≥3 and isolation of a MDR microorganism) but others (incorrect identification of clinical syndrome before starting EAT or the use of local guidelines for EAT) could be addressed to optimize the use of antimicrobials.
1 Introduction
Bloodstream infections are one of the main causes of morbidity and mortality worldwide (Weinstein et al., 1997; Wisplinghoff et al., 2004; Rodriguez-Creixems et al., 2008) and even in 2019, septicemia remained the 12th leading cause of mortality in the United States (Xu et al., 2021).
Appropriation of empirical antimicrobial treatment (EAT) has become a difficult decision due to the increase of antimicrobial resistance to antibiotics in the past few years, both in the healthcare and the community (Arias and Murray, 2009). This decision needs to find the adequate balance between using a broad-spectrum antibiotic, which may not be necessary and has a negative impact on the environment, leading to an increase in the emergence of antibiotic-resistant bacteria, and choosing a proper option, which targets the most frequently implied pathogens in the suspected infection (Paterson and Rice, 2003).
Inadequate EAT (i-EAT) has been largely associated with an increased mortality, compared with an antibiotic regimen that is adequately active against the organisms causing the infection. Many studies have focused on assessing the impact on mortality of an inadequate empirical antimicrobial treatment not only in specific scenarios, like the intensive care units (ICU) (Alvarez-Lerma; Ibrahim et al.; Kollef et al.; Luna et al.; Rello et al.; Kreger et al., 1980; Savage et al., 2016) but also it has been analysed in a broad spectrum of infections (Mettler et al., 2007; Paul et al., 2010). Concretely in patients with bacteremia, inadequate therapy has demonstrated to negatively impact on mortality in specific populations like oncohematological patients with febrile neutropenia (Martinez-Nadal et al., 2020; Chumbita et al., 2022) or cirrhotic patients (Park, 2015). Also, results from a very recent meta-analysis indicated that i-EAT substantially had a negative impact on survival of patients with BSIs at short and long term (Hung et al., 2022).
Despite of the relevance of choosing i-EAT, there is much less evidence on the risk factors associated with this practice. Some studies have focused on concrete patient-related factors (McDonald et al., 2005; Retamar et al., 2013) while others have analysed heterogeneous clinical syndromes (Mettler et al., 2007), have small sample size (Bai et al., 2021) or have focused on specific populations like neonates (Hsu et al., 2015) or immunosuppressed patients (Martinez-Nadal et al., 2020; Chumbita et al., 2022), which makes their findings ungeneralizable to general adult population. More recently, some studies have focused on the impact of isolation of multidrug resistant (MDR) strains on the adequation of empirical antimicrobial treatment choice (Girometti et al., 2014; Carrara et al., 2018) showing higher rates of i-EAT when a MDR microorganism was identified and thus, a negative impact on mortality. In a very recent study designed to assess the predictors and mortality risk of discordant EAT for BSI in a large cohort of US hospitals (Kadri et al., 2021) it was also identified the isolation of a MDR microorganism as the main factor associated with receiving i-EAT (in-vitro susceptibility-discordant).
Therefore, it is understandable that in the past few years, the efforts of the Antimicrobial Stewardship Programs (ASP) had moved towards the design of EAT local guidelines, considering the possibility of participation of resistant microorganisms (according to their local rates of resistant strains), not only in the healthcare setting, but also in community-acquired infections. The use of these guidelines has been associated with appropriate EAT (a-EAT) and thus with reduced mortality (Enoch et al., 2011).
Hence, despite some studies have pointed out risk factors for inappropriate empirical antimicrobial treatment for bloodstream infections in specific settings, information on factors related to i-EAT is still scarce. To address this, the aim of the present study was to identify the risk factors associated with the use of inappropriate empirical antimicrobial treatment in bloodstream infections. We hypothesised that there might be some potentially modifiable factors (prescription-related factors) that could be addressed to optimize the EAT choice.
2 Material and methods
2.1 Study design, setting and patients
A retrospective, observational, cohort study carried out in a 400-bed teaching hospital in Spain (Hospital Universitari Mútua de Terrassa, with a mean annual admission of 24,000 patients, catchment area of 350,000 inhabitants).
All consecutive episodes of clinically significant bloodstream infection (BSI) in adults (≥16 years old) have been prospectively recorded since 1989, by the Bloodstream Infection Surveillance Program, a multidisciplinary team which makes a prospective clinical follow-up of all patients with documented bacteremia. All BSI cases identified from this database, between January 2018 and December 2018, were included and retrospectively reviewed by three independent Infectious Diseases consultants. A patient could be included in the study more than once if they have different BSIs at different times. Patients were followed-up for 30 days.
The need for informed consent was waived because this is an observational quality control study without any effect on patients’ medical management. STROBE recommendations were followed to strengthen the reporting of the study results (Supplementary Table S1) (von Elm et al., 2014).
2.2 Variables and definitions
Main exposure variable was empirical antimicrobial treatment (EAT) appropriation. The administration of an antimicrobial with in-vitro activity (according to susceptibility data) at recommended doses within the first 24 h after the blood cultures had been performed (Savage et al., 2016) was defined as a-EAT. Otherwise, it was defined as i-EAT, including also BSI episodes in which EAT was not prescribed (no-EAT).
Other clinical variables collected included age, gender, comorbidities based on Charlson Comorbidity Index (CCI) (Charlson et al., 1987); severity of the BSI using the Pitt bacteremia score (Hilf et al., 1989); shock according to the usual definitions (Levy et al., 2003); lieu of acquisition; ability to identify the clinical syndrome by prescribing physicians, defined as the concordance between the recorded diagnosis before the initiation of EAT by the prescriber and the final diagnosis at hospital discharge; adherence to recommendations made on local guidelines for EAT; source of BSI, defined according to the CDC criteria (Horan et al., 2008) and aetiology. Outcomes were all-cause mortality at days 14th and 30th.
The acquisition lieu of the infection was recorded based on Friedman et al. definitions (Friedman et al., 2002): a nosocomial BSI was considered when it occurred 48 h after admission or if it developed in a patient discharged from hospital in the previous 14 days; healthcare-associated (HC-A) BSI was diagnosed if the patient fulfilled at least one of the following criteria: i) Resided in a nursing home or long-term care facility 30 days before the episode; ii) Had been hospitalized in an acute care hospital for ≥48 h, 90 days before the episode; iii) Attended a hospital or hemodialysis clinic or received intravenous therapy, 30 days before the episode; and/or iv) Had received intravenous therapy, wound care, enteral nutrition or healthcare at home, 30 days before the episode. Otherwise, the BSI was considered as community acquired.
Local guidelines for EAT have been developed at our institution since 2012–2013 by the Antimicrobial Stewardship Program (ASP). They include 13 different syndromes. Local guidelines’ recommendations suggest active in-vitro EAT for every of these syndromes according with the most frequent aetiology in our setting. A clinical syndrome which had already been included in the local guidelines, with a specific EAT recommendation was considered as an Antimicrobial Stewardship Program syndrome (ASP-syndrome).
When the origin of the BSI was uncertain despite of careful examination of the clinical and microbiological data, BSI was considered as unknown origin.
Pathogens were considered multidrug resistant (MDR) if they met resistance criteria according to Magiorakos et al. (Magiorakos et al., 2012) or if they were among the ESKAPE microorganisms previously defined (Boucher et al., 2009).
Data were collected from the medical charts and electronic medical records.
2.3 Microbiological studies
The recommendations of the Spanish Society of Infectious Diseases and Clinical Microbiology (SEIMC) were followed for performing, processing, and interpreting the blood cultures (Cisneros-Herreros et al., 2007). Antibiotic susceptibility and extended-spectrum beta-lactamase (ESBL) production were interpreted according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST 2018).
2.4 Statistical analysis
All statistical analyses were performed using the STATA RELEASE 14 software (StataCorp LP, College Station, TX, United States). Categorical variables are presented using counts and percentages and continuous variables as means and standard deviation (SD) or medians and interquartile range (IQR). Univariate analysis was performed using the chi-squared or Fisher exact test, and the Student t-test or Mann–Whitney U-test for comparison of categorical and continuous variables, respectively. A 2-sided p < 0.05 was considered statistically significant.
Multivariate analysis was performed by logistic regression. Starting with all variables that showed a trend towards an association (p < 0.2), a best subset regression procedure was used to identify the most suitable and parsimonious multivariate model, i.e., the one with the lowest Akaike information criterion, which is a well-known parameter of the goodness of fit of the model (Akaike, 1992). Differences were considered statistically significant at the two-sided p < 0.05 level.
The validity of the models was evaluated using the Hosmer-Lemeshow test for estimating goodness of fit to the data, and its discrimination ability by the area under the Receiver Operating Characteristics (ROC) curve.
3 Results
3.1 Baseline characteristics and outcomes
A total of 599 BSI episodes were included during the study period, 453 (75.6%) received a-EAT and 146 (24.4%) i-EAT.
Table 1 shows the epidemiological and clinical characteristics at admission and the outcomes of the 599 episodes of BSI, as well as the comparison between BSI episodes receiving a-EAT and i-EAT by univariate analysis.
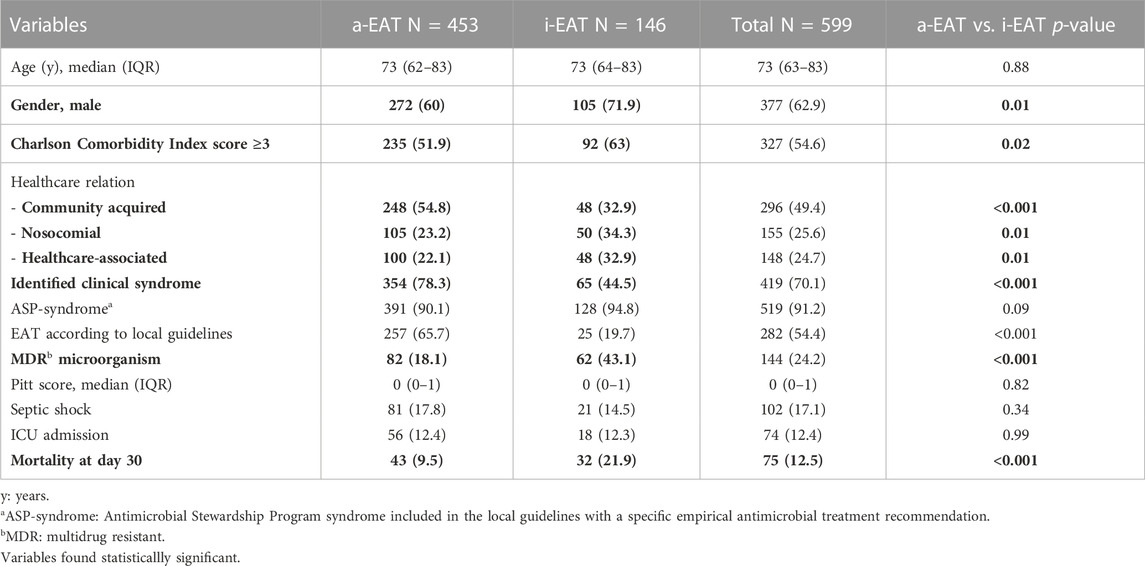
TABLE 1. General characteristics of the BSI episodes, and comparison between a-EAT and i-EAT.
Mortality at days 14 and 30 was higher in the i-EAT episodes (14.4% vs. 6.2%, p = 0.002 at day 14% and 21.9% vs. 9.5%, p < 0.001 at day 30 respectively). There was no association between i-EAT and mortality. Data of univariate and multivariate analysis for mortality at days 14 and 30 are shown in Supplementary Table S2.
3.2 Source, aetiology and antimicrobial resistance of bloodstream infections
Figure 1 shows EAT appropriation according to the BSI source and Table 2 the most frequently isolated microorganisms. Within the 599 BSI episodes, 35 (5.8%) were polymicrobial. Escherichia coli was the most frequently isolated pathogen (47% of all the bacteremia episodes).

FIGURE 1. Empirical antimicrobial treatment appropriation according to infection source.

TABLE 2. Etiology of the BSI episodes and antimicrobial appropriation.
According to the previous definitions, 24.2% of isolated microorganisms were considered MDR. Within the episodes in which a-EAT was administered, 82/453 (18.1%) were caused by a MDR microorganism (vs. 62/146 (43.1%) which received i-EAT, p < 0.001).
Mortality rates in BSI episodes caused by a MDR microorganism were 12.5% at day 14% and 17.4% at day 30 with no statistical differences between i-EAT and a-EAT groups (55.6% vs. 44.4%, p = 0.25 at day 14% and 52% vs. 48%, p = 0.32 at day 30 respectively). Regarding the lieu of acquisition, 32.6% of the BSI episodes caused by a MDR microorganism were community-acquired, 28.5% were nosocomial and 38.9% were HC-A (p < 0.001). Differences in the appropriateness of EAT caused by a MDR microorganism according to the healthcare delivery setting were not found (p = 0.70).
3.3 Adequate identification of clinical syndrome and EAT regimens
In 177 BSI episodes physicians did not identify the clinical syndrome before the antibiotic prescription (misdiagnosis rate of 29.6%).
EAT before microbiologic information was prescribed in 549 BSI episodes (91.7%). Considering BSI episodes with no-EAT (49), 23 (47%) were patients without clinical suspicion of infection; in 18 (36.7%) a delayed-initiating antibiotic strategy was chosen due to the clinical stability of the patients and, in the remaining 8 (16.3%), antibiotics were not prescribed because of limitation of therapeutic effort. When the 26 BSI episodes with no-EAT due to clinical decisions (clinical stability of the patient or limitation of therapeutic effort) were excluded, the i-EAT rate decreased to 20.9%. Excluding all the BSI episodes with no-EAT, the i-EAT rate was 17.5%.
Among all the episodes, 519 (91.2%) were considered ASP-syndromes. Antibiotics according to local guidelines’ recommendations were prescribed in 282 out of 519 ASP-syndromes (54.3%); among these, 25 (8.9%) received i-EAT. Eleven of these patients (44%) had a BSI caused by a MDR organism but with no identifiable risk factors for a MDR microorganisms.
Regarding BSI episodes in which the clinical syndrome had been correctly identified but local guidelines’ recommendations were not followed, in 64 out of 127 episodes (50.3%) patients received unnecessary broad-spectrum antibiotics.
The most frequently used antimicrobials for EAT are shown in Table 3. Monotherapy regimens were used in 63% of BSI episodes. Combination therapy was more frequent in the a-EAT group (86% vs. 14%, p < 0.001).
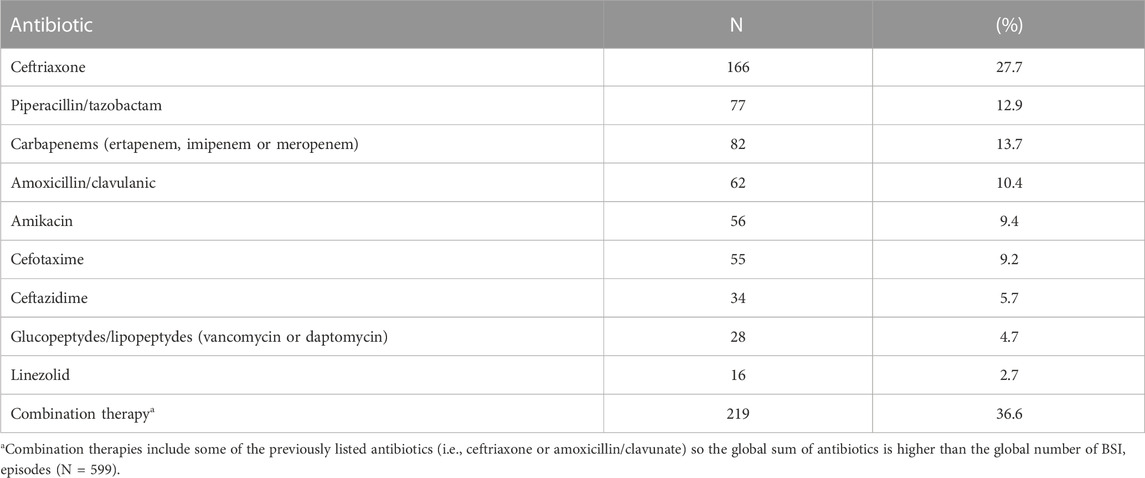
TABLE 3. Most frequent antibiotics used for empirical therapy.
The unit of admission for the BSI episodes is described in Table 4.
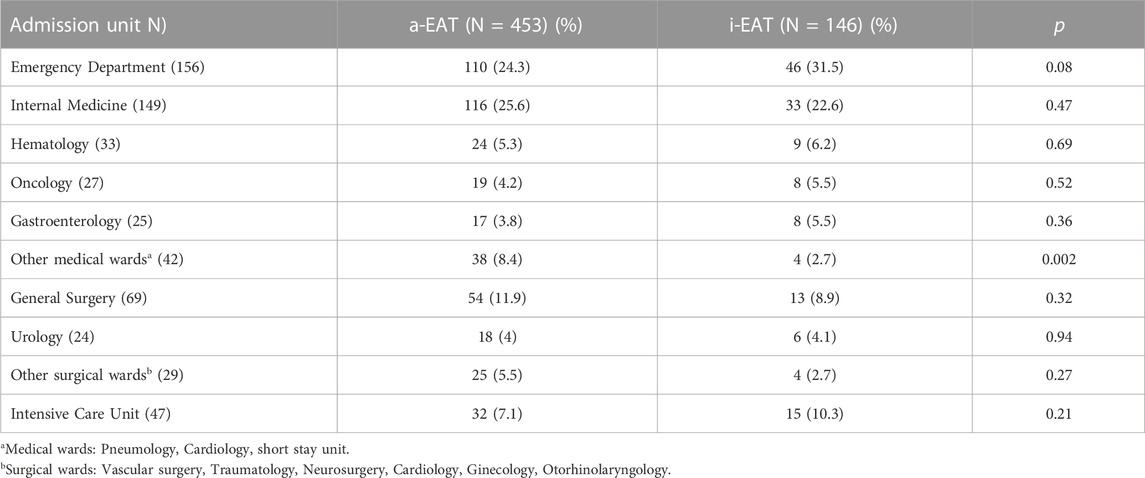
TABLE 4. Admission Unit of the BSI episodes and comparison between the a-EAT and i-EAT episodes in relation with the global antimicrobial appropriation.
3.4 Risk factors associated with EAT appropriateness
The multivariable logistic regression model used to assess variables associated with i-EAT is shown in Table 5. Male gender, a high CCI score (≥3 points), inadequate identification of clinical syndrome before initiating EAT, not prescribing EAT according to local guidelines and the isolation of MDR microorganisms were identified as risk factors for inappropriate choice of antimicrobial empirical therapy in BSI. The risk factors associated with i-EAT excluding the BSI episodes with no-EAT due to clinical decisions have been also analysed. Data are shown in Supplementary Table S2.

TABLE 5. Multivariate analysis.
4 Discussion
In this cohort study of 599 BSI in adults, EAT was inappropriate in 24.2% cases. We identified that male gender, host comorbidities, incorrect identification of clinical syndrome, lack of adherence to local guidelines and the isolation of MDR microorganisms were independent risk factors for i-EAT.
The i-EAT rate in our study (24.2%) was similar to previous studies (McDonald et al., 2005; Mettler et al., 2007; Retamar et al., 2012; Bai et al., 2021; Kadri et al., 2021) and even smaller than the pooled estimate of 32% in a systematic review of studies on i-EAT (Carrara et al., 2018). The differences between these rates among the studies are probably related to, on one hand, the heterogenicity of the definitions for appropriate empirical antimicrobial treatment and on the other, the variability of evaluated infections and the different rates of resistant microorganisms in every setting. Besides, there are some important differences in the design as well: i.e., in contrast to Kadri’s study, we did not exclude from the appropriateness analysis patients who had not received EAT on the day blood samples were drawn.
Evidence on the risk factors for i-EAT in adult patients with BSI is scarce. Previous studies have tried to point them out, but they either limited the analysis to the impact of MDR (Girometti et al., 2014; Kadri et al., 2021), were small studies (Bai et al., 2021) or identified some predictors to receive i-EAT even though the study was not designed for this purpose (Retamar et al., 2013). Regarding risk factors for i-EAT identified in our study, they could be classified in patient-related (and, therefore, unmodifiable risk factors) and modifiable risk factors.
Gender differences in the prescription of antibiotics had been previously reported (Norris et al., 2005). In our cohort, female gender was a protective factor for receiving a-EAT (OR 0.59 (95% CI 0.35–0.98), p = 0.04) as it was in the study conducted by Mettler et al. (Mettler et al., 2007). As the investigators in this study, we also find difficult to explain why women are more suitable to receive a-EAT in a BSI episode. On the other hand, we found that a CCI score of ≥3 was an independent risk factor for i-EAT with an estimated OR 1.90. Cancer (which scores 6 points in the CCI itself) has already been identified as a risk factor for i-EAT (Retamar et al., 2013). Some comorbidities included in the CCI have been identified as risk factors for certain types of pathogens or mechanisms of resistance (Rodríguez-Baño et al., 2010), so they should be taken into account when considering empirical therapy. However, the most important patient-related risk factor identified in our study was the isolation of a MDR microorganism. We found that 24% of all the episodes were due to a MDR microorganism, which is a much lower incidence of MDR than previously reported in recent studies (with variable rates of MDR isolation between 19% and 65%) (Girometti et al., 2014; Kadri et al., 2021). In our study, we found high rates of i-EAT in BSI caused by MDR strains (43%), which was consistent with the reported rates by Girometti (varying between 23% in ESBL-producing K. pneumoniae strains and 77% in KPC-producing strains) and Kadri (49%) and identified that a BSI episode caused by a MDR has nearly a 4-fold greater probability of receiving i-EAT. Prevalence of MDR was also identified as the main unmodifiable risk factor associated with i-EAT in Kadri’s study (OR 9.09, 95% CI 7.68–10.76). Moreover, in a 2018 meta-analysis, isolation of MDR pathogens was independently associated with i-EAT (OR 1.11 95% CI 1.07–1.15) (Carrara et al., 2018) but also with higher mortality rates. This scenario deserves some reflections: on one hand, it is essential to consider the potential participation of MDR microorganisms to design active EATs, which is especially relevant in clinical syndromes associated with high mortality. On the other, the use of broad-spectrum antibiotics has been associated with i-EAT itself (Mettler et al., 2007) but, most important, it can have a negative impact on the environment and lead to the emergence of more resistant, difficult-to-treat microorganisms (Paterson and Rice, 2003) for which active drugs are not always available, forcing the use of “second-line” drugs which are less effective and can cause more adverse effects (Rodriguez-Bano et al., 2018; Paul et al., 2022). Hence the importance of avoiding the use of broad spectra antibiotics in clinical syndromes with low mortality risk (i.e., uncomplicated urinary tract infections).
Interestingly, we found some important modifiable factors related to i-EAT in BSI episodes. First, a right clinical diagnosis of the site of infection before antibiotics administration is a protective factor against i-EAT (OR 0.23, (95% CI 0.13–0.38), p < 0.001). Recently, the impact of misdiagnoses of infection site previous to antibiotic administration has been analysed (Dregmans et al., 2022). This study identified a misdiagnoses rate of 11.6%, although investigators could not find association between misdiagnoses and worse clinical outcomes as previous studies did (Abe et al., 2019; Hautz et al., 2019; Hussain et al., 2019). Investigators speculated that these controversial results could have been influenced because most patients with misdiagnoses received a broad-spectrum antimicrobial treatment, which was effective in different sites of infection, despite the correct site was not identified. Thus, they also contemplate the possibility that the effects of incorrect diagnosis of the infection site on clinical outcomes may be much wider, and not only limited to the impact on mortality. Some of these related-to-misdiagnosis effects could be (a) The unnecessary use of antibiotics (in our cohort 18% of misdiagnoses received unnecessary broad-spectrum antibiotics, like in Dregmans’ study, where 20% of misdiagnosed patients received unnecessarily antibiotics) or (b) The choice of i-EAT in serious infections like bacteremia which had been related to poor prognosis (Ortega et al., 2007; Paul et al., 2010; Retamar et al., 2012; Carrara et al., 2018), despite we could not find this association in our cohort. Regarding this absence of association between i-EAT and mortality, we contemplate that it could probably been explained by different reasons: 1) The global i-EAT in our cohort was smaller than previous studies (Carrara et al., 2018; Kadri et al., 2021) so the vast majority of the patients received a-EAT which could impact on the global mortality rate; 2) Our participation rate of MDR microorganisms was relatively low (24%) compared to previous studies, where resistance had a significant impact on mortality (Girometti et al., 2014) and 3) Patients from our cohort had low severe infections (septic shock rate 17%, ICU admission rate 12% and a median Pitt score of 0). In 2010 and 2022’s meta-analysis, i-EAT had higher impact on mortality among patients with septic shock at infection onset (Paul et al., 2010; Hung et al., 2022). Thus, in our cohort with mild BSI episodes, this effect could have been lessened.
Second, the lack of adherence to local guidelines for EAT is the other main risk factor identified for i-EAT in our study. We observed a non-adherence to local guidelines’ recommendations rate of 45.6%. In a recent study, adherence to local guidelines was evaluated by annual Point Prevalence Surveys. When prescriptions were incorrect according to local guidelines, after the evaluation of many different aspects (dosing, route of administration, duration, etc.), they were considered as inadequate (Nunez-Nunez et al., 2022). Result from PPS showed a 49.2% of inadequate prescriptions’ rate, similar to the findings in our cohort. In our study, adherence to local guidelines resulted in a-EAT in 91% of episodes (which was a protective factor for i-EAT, with a OR 0.22 (95% CI 0.13–0.38), p < 0.001). This finding agrees with a recent study, with a smaller sample size, but with similar design (Bai et al., 2021), which reported that adherence to guidelines produced an a-EAT in 72% of cases in their population. The importance of ASP has been largely studied underlying their beneficial impact on clinical outcomes (better use of antimicrobials, reduction of infections caused by MDR microorganisms and mortality rates, etc.) and also on economic outcomes (Nathwani et al., 2019). There are many types of interventions available for optimizing the use of antimicrobials (Mendelson et al., 2020). Although educational measures could have a modest impact on antimicrobial stewardship, they are usually necessary. First, we found that the adherence to local guidelines can be a protective factor against i-EAT choice. In the study conducted by Kadri et al., investigators suggested that some unmeasured factors could have led antibiotic choices, such as the absence of ASP or the unavailability of appropriate protocols or local guidelines on EAT. Our findings reinforce the essential role of ASP teams. It is indispensable to assure that EAT local guidelines are constantly adapted to, on one hand, the local epidemiology data and, on the other, to patients’ associated factors with the participation of certain microorganisms, to guarantee a proper choice of EAT by physicians who may not be such familiarized with the antimicrobial use. Second, another important protective factor is the correct identification of clinical syndrome before antibiotics prescription. Educational audits or systematic advice should be a cornerstone of the ASP, offered to the clinicians who may be at the front-line of the diagnosis process in order to improve their diagnostic abilities and drive them to a better choice of EAT. All these strategies are focused on improving the appropriateness of EAT which can in turn improve clinical outcomes, considering that i-EAT in bloodstream infections has been largely related with higher mortality (Ortega et al., 2007; Paul et al., 2010; Retamar et al., 2012; Carrara et al., 2018; Hung et al., 2022). The identification of these modifiable risk factors in our study offers many opportunities for improvement and emphasize the importance of the ASP teams.
In 2005 McDonald et al. assessed the specific relationship between HC-A status and ineffective initial therapy (McDonald et al., 2005). Unlike this study, where HC-A was identified as an independent risk factor for i-EAT, we did not find this association. Nevertheless, patients who received i-EAT were more likely to have a nosocomial or HC-A BSI episodes, compared to the community-acquired.
The most frequent sources of BSI were urinary and intraabdominal infections. Urinary and respiratory tract infections received more frequently a-EAT while intraabdominal infections and catheter-related were more frequent sources among i-EAT episodes. Escherichia coli was the most frequently isolated pathogen, which is consistent with the most frequent sources of infection where E. coli plays a major role.
Our study has many strengths: 1) It provides a relevant sample size and identifies modifiable related factors for i-EAT in BSI episodes, which leads to opportunities for improvement in the ASP strategies. Other previous studies had smaller sample sizes or have focused on concrete, unmodifiable factors (McDonald et al., 2005; Retamar et al., 2013; Girometti et al., 2014; Bai et al., 2021; Kadri et al., 2021). 2) All consecutive adult BSI episodes have been prospectively recorded, and followed for routine clinical practice, so there is no selection bias and there is no patient-loss for the analysis. 3) Local guidelines for EAT have been established in our centre for many years and are well known by all the physicians who make antibiotic prescriptions, so it has been possible to perform a deep analysis on the adherence to the guidelines and the appropriateness of the recommendations. Still, it has some limitations: it is a retrospective, observational study, so conclusions may be interpretated carefully, since more studies need to be performed to confirm the results. Also, it is a single-centre study, performed in a hospital with a consolidated ASP team and low prevalence of MDR microorganisms so the study findings could impact differently in other locations and should not be extrapolated to other institutions without careful assessment of local environment. Finally, we only assessed mortality, but we did not measure other outcomes, like the length of hospital stay or the impact of unnecessary antimicrobial regimens, considering that the effect of i-EAT may be broader (Bai et al., 2021).
In conclusion, one quarter of this cohort of BSI episodes in adults received i-EAT. Some related factors for the choice of i-EAT for bacteremia were unmodifiable, as male gender, high comorbidity or the isolation of a MDR microorganism. However, some important factors were positively associated with a-EAT, as the correct identification of the clinical syndrome before starting EAT and the adherence to local guidelines for EAT, which generate a-EAT in 91% of BSI episodes. The good news is that these modifiable factors could be addressed by the ASP teams to optimize the use of antimicrobials.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
LB-P and EC participated on the conception and design of the study. BD, AM, LG, GG, CB, and ML-S have contributed to the collection of participants’ data. MX and JP have performed the microbiologic studies. LB-P did the formal analysis of the data. BD and LB-P wrote the original version of the manuscript. All the authors have contributed by reviewing and editing the manuscript to its final version.
Acknowledgments
The authors want to thank the Bloodstream Infection Surveillance Program for their daily work on identifying, monitoring and registering all patients with bloodstream infection, to improve investigation and clinical management. We also want to thank the Antimicrobial Stewardship Program to optimize the use of antimicrobials in the routine clinical practice.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1132530/full#supplementary-material
References
Abe, T., Tokuda, Y., Shiraishi, A., Fujishima, S., Mayumi, T., Sugiyama, T., et al. (2019). In-hospital mortality associated with the misdiagnosis or unidentified site of infection at admission. Crit. Care 23 (1), 202. doi:10.1186/s13054-019-2475-9
Akaike, H. (1992). “Information theory and an extension of the maximum likelihood principle,” in Breakthroughs in statistics: Foundations and basic theory. Editors S. Kotz, and N. L. Johnson (New York, NY: Springer New York), 610–624.
Arias, C. A., and Murray, B. E. (2009). Antibiotic-resistant bugs in the 21st century — a clinical super-challenge. N. Engl. J. Med. 360 (5), 439–443. doi:10.1056/nejmp0804651
Bai, A. D., Irfan, N., Main, C., El-Helou, P., and Mertz, D. (2021). Local audit of empiric antibiotic therapy in bacteremia: A retrospective cohort study. PLOS ONE 16 (3), e0248817. doi:10.1371/journal.pone.0248817
Boucher, H. W., Talbot, G. H., Bradley, J. S., Edwards, J. E., Gilbert, D., Rice, L. B., et al. (2009). Bad bugs, no drugs: No ESKAPE! An update from the infectious Diseases society of America. Clin. Infect. Dis. 48 (1), 1–12. doi:10.1086/595011
Carrara, E., Pfeffer, I., Zusman, O., Leibovici, L., and Paul, M. (2018). Determinants of inappropriate empirical antibiotic treatment: Systematic review and meta-analysis. Int. J. Antimicrob. Agents 51 (4), 548–553. doi:10.1016/j.ijantimicag.2017.12.013
Charlson, M. E., Pompei, P., Ales, K. L., and MacKenzie, C. R. (1987). A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 40 (5), 373–383. doi:10.1016/0021-9681(87)90171-8
Chumbita, M., Puerta-Alcalde, P., Gudiol, C., Garcia-Pouton, N., Laporte-Amargos, J., Ladino, A., et al. (2022). Impact of empirical antibiotic regimens on mortality in neutropenic patients with bloodstream infection presenting with septic shock. Antimicrob. Agents Chemother. 66 (2), e0174421. doi:10.1128/AAC.01744-21
Cisneros-Herreros, J. M., Cobo-Reinoso, J., Pujol-Rojo, M., Rodríguez-Baño, J., and Salavert-Lletí, M. (2007). Guía para el diagnóstico y tratamiento del paciente con bacteriemia. Guías de la Sociedad Española de Enfermedades Infecciosas y Microbiología Clínica (SEIMC). Enfermedades Infecc. Microbiol. Clínica 25 (2), 111–130. doi:10.1016/s0213-005x(07)74242-8
Dregmans, E., Kaal, A. G., Meziyerh, S., Kolfschoten, N. E., Van Aken, M. O., Schippers, E. F., et al. (2022). Analysis of variation between diagnosis at admission vs discharge and clinical outcomes among adults with possible bacteremia. JAMA Netw. Open 5 (6), e2218172. doi:10.1001/jamanetworkopen.2022.18172
Enoch, D. A., Phillimore, N., Mlangeni, D. A., Salihu, H. M., Sismey, A., Aliyu, S. H., et al. (2011). Outcome for Gram-negative bacteraemia when following restrictive empirical antibiotic guidelines. QJM 104 (5), 411–419. doi:10.1093/qjmed/hcq228
Friedman, N. D., Kaye, K. S., Stout, J. E., McGarry, S. A., Trivette, S. L., Briggs, J. P., et al. (2002). Health care-associated bloodstream infections in adults: A reason to change the accepted definition of community-acquired infections. Ann. Intern Med. 137 (10), 791–797. doi:10.7326/0003-4819-137-10-200211190-00007
Girometti, N., Lewis, R. E., Giannella, M., Ambretti, S., Bartoletti, M., Tedeschi, S., et al. (2014). Klebsiella pneumoniae bloodstream infection: Epidemiology and impact of inappropriate empirical therapy. Med. Baltim. 93 (17), 298–309. doi:10.1097/MD.0000000000000111
Hautz, W. E., Kämmer, J. E., Hautz, S. C., Sauter, T. C., Zwaan, L., Exadaktylos, A. K., et al. (2019). Diagnostic error increases mortality and length of hospital stay in patients presenting through the emergency room. Scand. J. Trauma, Resusc. Emerg. Med. 27 (1), 54. doi:10.1186/s13049-019-0629-z
Hilf, M., Yu, V. L., Sharp, J., Zuravleff, J. J., Korvick, J. A., and Muder, R. R. (1989). Antibiotic therapy for Pseudomonas aeruginosa bacteremia: Outcome correlations in a prospective study of 200 patients. Am. J. Med. 87 (5), 540–546. doi:10.1016/s0002-9343(89)80611-4
Horan, T. C., Andrus, M., and Dudeck, M. A. (2008). CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am. J. Infect. Control 36 (5), 309–332. doi:10.1016/j.ajic.2008.03.002
Hsu, J. F., Chu, S. M., Huang, Y. C., Lien, R., Huang, H. R., Lee, C. W., et al. (2015). Predictors of clinical and microbiological treatment failure in neonatal bloodstream infections. Clin. Microbiol. Infect. 21 (5), 482.e9–482.17. doi:10.1016/j.cmi.2015.01.009
Hung, Y. P., Lee, C. C., and Ko, W. C. (2022). Effects of inappropriate administration of empirical antibiotics on mortality in adults with bacteraemia: Systematic review and meta-analysis. Front. Med. (Lausanne) 9, 869822. doi:10.3389/fmed.2022.869822
Hussain, F., Cooper, A., Carson-Stevens, A., Donaldson, L., Hibbert, P., Hughes, T., et al. (2019). Diagnostic error in the emergency department: Learning from national patient safety incident report analysis. BMC Emerg. Med. 19 (1), 77. doi:10.1186/s12873-019-0289-3
Kadri, S. S., Lai, Y. L., Warner, S., Strich, J. R., Babiker, A., Ricotta, E. E., et al. (2021). Inappropriate empirical antibiotic therapy for bloodstream infections based on discordant in-vitro susceptibilities: A retrospective cohort analysis of prevalence, predictors, and mortality risk in US hospitals. Lancet Infect. Dis. 21 (2), 241–251. doi:10.1016/s1473-3099(20)30477-1
Levy, M. M., Fink, M. P., Marshall, J. C., Abraham, E., Angus, D., Cook, D., et al. (2003). 2001 SCCM/ESICM/ACCP/ATS/SIS international sepsis definitions conference. Intensive Care Med. 29 (4), 530–538. doi:10.1007/s00134-003-1662-x
Magiorakos, A. P., Srinivasan, A., Carey, R. B., Carmeli, Y., Falagas, M. E., Giske, C. G., et al. (2012). Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 18, 268–281. doi:10.1111/j.1469-0691.2011.03570.x
Martinez-Nadal, G., Puerta-Alcalde, P., Gudiol, C., Cardozo, C., Albasanz-Puig, A., Marco, F., et al. (2020). Inappropriate empirical antibiotic treatment in high-risk neutropenic patients with bacteremia in the era of multidrug resistance. Clin. Infect. Dis. 70 (6), 1068–1074. doi:10.1093/cid/ciz319
McDonald, J. R., Friedman, N. D., Stout, J. E., Sexton, D. J., and Kaye, K. S. (2005). Risk factors for ineffective therapy in patients with bloodstream infection. Arch. Intern Med. 165 (3), 308–313. doi:10.1001/archinte.165.3.308
Mendelson, M., Morris, A. M., Thursky, K., and Pulcini, C. (2020). How to start an antimicrobial stewardship programme in a hospital. Clin. Microbiol. Infect. 26 (4), 447–453. doi:10.1016/j.cmi.2019.08.007
Mettler, J., Simcock, M., Sendi, P., Widmer, A. F., Bingisser, R., Battegay, M., et al. (2007). Empirical use of antibiotics and adjustment of empirical antibiotic therapies in a University hospital: A prospective observational study. BMC Infect. Dis. 7 (1), 21. doi:10.1186/1471-2334-7-21
Nathwani, D., Varghese, D., Stephens, J., Ansari, W., Martin, S., and Charbonneau, C. (2019). Value of hospital antimicrobial stewardship programs [ASPs]: A systematic review. Antimicrob. Resist. Infect. Control 8 (1), 35. doi:10.1186/s13756-019-0471-0
Norris, P., Becket, G., Ecke, D., Skellett, L., Hoo, J., Va'ai, C., et al. (2005). Advertising of medicines on New Zealand television. N. Z. Med. J. 118 (1211), U1462.
Nunez-Nunez, M., Perez-Galera, S., Giron-Ortega, J. A., Sandoval Fernandez-Del-Castillo, S., Beltran-Garcia, M., De Cueto, M., et al. (2022). Predictors of inappropriate antimicrobial prescription: Eight-year point prevalence surveys experience in a third level hospital in Spain. Front. Pharmacol. 13, 1018158. doi:10.3389/fphar.2022.1018158
Ortega, M., Almela, M., Martinez, J. A., Marco, F., Soriano, A., Lopez, J., et al. (2007). Epidemiology and outcome of primary community-acquired bacteremia in adult patients. Eur. J. Clin. Microbiol. Infect. Dis. 26 (7), 453–457. doi:10.1007/s10096-007-0304-6
Park, H., Jang, K. J., Jang, W., Park, S. H., Park, J. Y., Jeon, T. J., et al. (2015). Appropriate empirical antibiotic use and 30-d mortality in cirrhotic patients with bacteremia. World J. Gastroenterology 21 (12), 3587–3592. doi:10.3748/wjg.v21.i12.3587
Paterson, D. L., and Rice, L. B. (2003). Empirical antibiotic choice for the seriously ill patient: Are minimization of selection of resistant organisms and maximization of individual outcome mutually exclusive? Clin. Infect. Dis. 36 (8), 1006–1012. doi:10.1086/374243
Paul, M., Carrara, E., Retamar, P., Tängdén, T., Bitterman, R., Bonomo, R. A., et al. (2022). European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant Gram-negative bacilli (endorsed by European society of intensive care medicine). Clin. Microbiol. Infect. 28 (4), 521–547. doi:10.1016/j.cmi.2021.11.025
Paul, M., Shani, V., Muchtar, E., Kariv, G., Robenshtok, E., and Leibovici, L. (2010). Systematic review and meta-analysis of the efficacy of appropriate empiric antibiotic therapy for sepsis. Antimicrob. Agents Chemother. 54 (11), 4851–4863. doi:10.1128/aac.00627-10
Retamar, P., Lopez-Prieto, M. D., Natera, C., de Cueto, M., Nuno, E., Herrero, M., et al. (2013). Reappraisal of the outcome of healthcare-associated and community-acquired bacteramia: A prospective cohort study. BMC Infect. Dis. 13, 344. doi:10.1186/1471-2334-13-344
Retamar, P., Portillo, M. M., Lopez-Prieto, M. D., Rodriguez-Lopez, F., de Cueto, M., Garcia, M. V., et al. (2012). Impact of inadequate empirical therapy on the mortality of patients with bloodstream infections: A propensity score-based analysis. Antimicrob. Agents Chemother. 56 (1), 472–478. doi:10.1128/AAC.00462-11
Rodriguez-Bano, J., Gutierrez-Gutierrez, B., Machuca, I., and Pascual, A. (2018). Treatment of infections caused by extended-spectrum-beta-lactamase-AmpC-and carbapenemase-producing enterobacteriaceae. Clin. Microbiol. Rev. 31 (2), e00079–17. doi:10.1128/CMR.00079-17
Rodríguez-Baño, J., López-Prieto, M. D., Portillo, M. M., Retamar, P., Natera, C., Nuño, E., et al. (2010). Epidemiology and clinical features of community-acquired, healthcare-associated and nosocomial bloodstream infections in tertiary-care and community hospitals. Clin. Microbiol. Infect. 16 (9), 1408–1413. doi:10.1111/j.1469-0691.2009.03089.x
Rodriguez-Creixems, M., Alcala, L., Munoz, P., Cercenado, E., Vicente, T., and Bouza, E. (2008). Bloodstream infections: Evolution and trends in the microbiology workload, incidence, and etiology, 1985-2006. Med. Baltim. 87 (4), 234–249. doi:10.1097/MD.0b013e318182119b
Savage, R. D., Fowler, R. A., Rishu, A. H., Bagshaw, S. M., Cook, D., Dodek, P., et al. (2016). The effect of inadequate initial empiric antimicrobial treatment on mortality in critically ill patients with bloodstream infections: A multi-centre retrospective cohort study. PLOS ONE 11 (5), e0154944. doi:10.1371/journal.pone.0154944
von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gotzsche, P. C., Vandenbroucke, J. P., et al. (2014). The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 12 (12), 1495–1499. doi:10.1016/j.ijsu.2014.07.013
Weinstein, M. P., Towns, M. L., Quartey, S. M., Mirrett, S., Reimer, L. G., Parmigiani, G., et al. (1997). The clinical significance of positive blood cultures in the 1990s: A prospective comprehensive evaluation of the microbiology, epidemiology, and outcome of bacteremia and fungemia in adults. Clin. Infect. Dis. 24 (4), 584–602. doi:10.1093/clind/24.4.584
Wisplinghoff, H., Bischoff, T., Tallent, S. M., Seifert, H., Wenzel, R. P., and Edmond, M. B. (2004). Nosocomial bloodstream infections in US hospitals: Analysis of 24,179 cases from a prospective nationwide surveillance study. Clin. Infect. Dis. 39 (3), 309–317. doi:10.1086/421946
Keywords: bacteremia, bloodstream infections (BSI), anti-bacterial agents-therapeutic use, risk factors, antimicrobial therapy, antimicrobial stewardship (ASP) intervention
Citation: Dietl B, Boix-Palop L, Gisbert L, Mateu A, Garreta G, Xercavins M, Badía C, López-Sánchez M, Pérez J and Calbo E (2023) Risk factors associated with inappropriate empirical antimicrobial treatment in bloodstream infections. A cohort study. Front. Pharmacol. 14:1132530. doi: 10.3389/fphar.2023.1132530
Received: 27 December 2022; Accepted: 13 March 2023;
Published: 24 March 2023.
Edited by:
Pasquale Pagliano, University of Salerno, ItalyReviewed by:
Andre Almeida, NOVA University of Lisbon, PortugalCecilia G. Carvalhaes, JMI Laboratories, United States
Copyright © 2023 Dietl, Boix-Palop, Gisbert, Mateu, Garreta, Xercavins, Badía, López-Sánchez, Pérez and Calbo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lucía Boix-Palop, bGJvaXhAbXV0dWF0ZXJyYXNzYS5jYXQ=, bHVjaWFib2l4QGhvdG1haWwuY29t; Esther Calbo, ZWNhbGJvQG11dHVhdGVycmFzc2EuZXM=, ZXN0aGVyY2FsYm9AaG90bWFpbC5jb20=