 Lina Naseralallah
Lina Naseralallah Malkan Khatib
Malkan Khatib Azhar Al-Khulaifi3
Azhar Al-Khulaifi3
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol., 10 February 2023
Sec. Drugs Outcomes Research and Policies
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1122898
Background and objectives: Polypharmacy and chronic kidney disease (CKD) are becoming increasingly common due to an ageing population and the rise of multimorbidity. In line with the therapeutic guidelines, managing CKD and its complications necessitates prescribing multiple medications, which predisposes patients to polypharmacy. The aim of this systematic review and meta-analysis is to describe the prevalence of polypharmacy in patients with CKD and to explore the global trends of factors driving any apparent variability in prevalence estimates.
Methods: PubMed, Scopus, the Cochrane Database of Systematic Reviews (CDSR), and Google Scholar were searched from 1999 to November 2021. Study selection, data extraction, and critical appraisal were conducted by two independent reviewers. The pooled prevalence of polypharmacy was estimated utilizing the random effects model using the default double arcsine transformation.
Results: This review involved 14 studies comprising of 17 201 participants, a significant proportion of which were males (56.12%). The mean age of the review population was 61.96 (SD ± 11.51) years. The overall pooled prevalence of polypharmacy amongst patients with CKD was 69% (95% CI: 49%–86%) (I2 = 100%, p < 0.0001), with a proportionately higher prevalence in North America and Europe as compared to Asia.
Conclusion: The results from this meta-analysis showed a high pooled prevalence estimates of polypharmacy amongst patient cohorts with CKD. The exact interventions that are likely to significantly mitigate its effect remain uncertain and will need exploration by future prospective and systematic studies.
Systematic Review Registration: [https://www.crd.york.ac.uk/prospero/], identifier [CRD42022306572].
Chronic kidney disease (CKD) is a relatively common condition that affects up to 16% of the population globally (Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group, 2013; Gansevoort et al., 2011). It has been associated with adverse health outcomes including cardiovascular disease (CVD) events, poor quality of life, significant morbidity, and CVD or all-cause mortality (Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group, 2013; Couser et al., 2011; James et al., 2010; Yuan et al., 2017; Bansal et al., 2017; Jankowski et al., 2021). CKD is a gradually progressive disease that is linked to a range of complications, such as anemia, bone and mineral disorder, electrolyte imbalance, acid-base abnormalities, hypertension and other CVD, and sexual dysfunction (Widmer et al., 1979; Delmez and Slatopolsky, 1992; Stefanski et al., 1996; Hsu et al., 2002; Bello et al., 2017). Therefore, therapeutic guidelines have been developed to prevent/slow the progression of CKD and to provide therapeutic approaches to manage each clinical manifestation (Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group, 2013). As a consequence of the advanced therapeutics that followed our rising understanding of the pathophysiology, the number of medications taken per patient has substantially increased, which made polypharmacy and its expensive consequences a commonplace across this cohort of patients.
Polypharmacy exhibits a pronounced risk for medication non-adherence, adverse drug events, problematic interactions (drug-drug, drug-food, and pharmacogenetic), emergency department visits, hospitalizations, and sometimes avoidable mortality (Whittaker and Fink, 2017). Consequent upon this, a hefty medical and financial burdens have been imposed on patients, societies, and healthcare systems (Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group, 2013; Jankowski et al., 2021). It is not clear if this polypharmacy is appropriate, as despite the medication burden in CKD patients that could reach more than 30 drugs per patient, the morbidity and mortality rates remain high which raises questions about the effectiveness of these medications in this cohort of patients (Whittaker and Fink, 2017; Schmidt et al., 2019). Additionally, the altered pharmacodynamic and pharmacokinetic parameters in the unique milieu of renal insufficiency further complicates the situation as dosage adjustments and cessation of certain therapies might be required (Parker and Wong, 2019).
Whilst the growing polypharmacy epidemic has garnered attention in the medical community, it is still challenging to address this issue as uncertainty still exist regarding the exact prevalence of polypharmacy in CKD patients as well as the socio-demographic factors that influence its global trends. Understanding the burden of polypharmacy in patients with CKD and identifying vulnerable populations will enable clinicians to develop and implement interventions (e.g., deprescribing) to mitigate polypharmacy and its unfavorable outcomes. Therefore, the aim of this systematic review and meta-analysis is to estimate the prevalence of polypharmacy in CKD patients and to explore the global trends of factors driving any apparent variability in prevalence estimates.
This systematic review and meta-analysis followed the recommendations provided by the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) guidelines. The current review has been registered with PROSPERO under the registration number: CRD42022306572. This authorization encompasses patient cohorts with both CKD and chronic liver disease (CLD).
Searches were undertaken using the following electronic databases and search engines from 1999 to November 2021: PubMed, Scopus, the Cochrane Database of Systematic Reviews (CDSR), and Google Scholar (first 50 pages). The process also included cross-referencing of included papers. The choice of these databases as primary areas of our literature search was based on their validation as repositories of the most current medical literature; in addition to their continued update and renewal.
The following search terms were used: “polypharmacy” [TIAB], AND “kidney” [MeSH] OR “CKD” OR “chronic kidney disease” [MeSH]. We additionally searched grey literature for similar articles that are not captured in the aforementioned databases. The search was limited to “English language” and “Human species” as applicable to each database.
This systematic review and meta-analysis examined studies of patient populations with CKD who had medication counts adjudicated as polypharmacy and reported as such. The main outcome is the pooled estimate of polypharmacy period prevalence amongst these studies. Our review does not involve a new investigational medicinal product (IMP), hence no conceivable need for an intervention and comparator arms.
Studies were considered eligible if they met the following criteria: (1) reported numerical data on the prevalence of polypharmacy; (2) included patients with CKD; (3) included participants of ≥18 years; (4) published in English language. We included studies regardless of what the authors considered to be the threshold for diagnosis of polypharmacy (e.g., ≥5, ≥10 medications, etc.). Case report, case series, and reviews were excluded as were studies that only included patients with polypharmacy (patients who have CKD without polypharmacy were excluded) as this means that the control/denominator is missing which will prevent calculating the prevalence.
All retrieved studies were exported to EndNote 20® (2021 Clarivate), duplicates were removed, and the remaining papers were imported to Rayyan Qatar Computing Research Institute (QCRI) software. Two independent reviewers (LN and MD) screened the titles, abstracts, and full texts of the records to ascertain eligibility for inclusion. Disagreements between reviews were resolved through consensus discussion with a third reviewer (MK).
Two independent reviewers (LN and MD) initially trialed a sample data collection sheet on five randomly selected studies to determine the robustness of this sheet in abstracting patient data. After which the following variables were extracted from the studies: author, year of publication, study design, site, country, population, age, gender distribution, sample size, proportion of CKD patients with polypharmacy, iteration of polypharmacy definition (where available), and duration of study.
The risk of bias of the included studies was carried out using the Loney’s criteria. Exhaustive description of this appraisal tool has been done elsewhere (Loney et al., 1998). Briefly, the tool is comprised of eight domains returning a total score of eight for studies with optimal methodological quality. Two reviewers (LN and MD) independently assessed the methodological quality. Disagreements were resolved by consensus or by involving a third reviewer (AA).
Continuous Variables were presented as means (± standard deviation [SD]) or median (interquartile range [IQR]) as appropriate; whilst categorical variables were presented as numbers (percentages). We quantified the pooled prevalence estimates of polypharmacy (utilizing the random effects model) amongst patients with CKD using the default double arcsine transformation. We did not apply any continuity correction because this transformation does not need one. To ascertain the source of significant heterogeneity amongst the included studies (where this exists), we subsequently carried out a subgroup analyses to examine the effect of age, gender, source of primary data, as well as the risk of bias scores of the reviewed studies on the final point prevalence estimates. We assessed the heterogeneity between studies with I2 statistic and τ2 statistic (Higgins et al., 2003). We considered the I2 thresholds of 25%, 50%, and 75% to represent low, moderate, and high heterogeneity between-study variances, respectively. Where τ2 was reported to be zero, this was indicative of no heterogeneity (Quintana, 2015). We utilized funnel and Doi plots to visualize small-study effect and publication bias (Furuya-Kanamori et al., 2018). We finally carried out sensitivity analysis excluding each study to ascertain its effect on the final point prevalence estimate. All statistical analyses were carried out with Meta XL, version 5.3 (EpiGear International, Queensland, Australia).
A total of 487 citations were retrieved from the literature search. After duplicate removal (n = 478), the remaining articles were screened by title and abstract. A total of 14 studies were included in the systematic review and meta-analysis (Figure 1). The most common reason for exclusion was the absence of data that allows the estimation of the prevalence of polypharmacy.
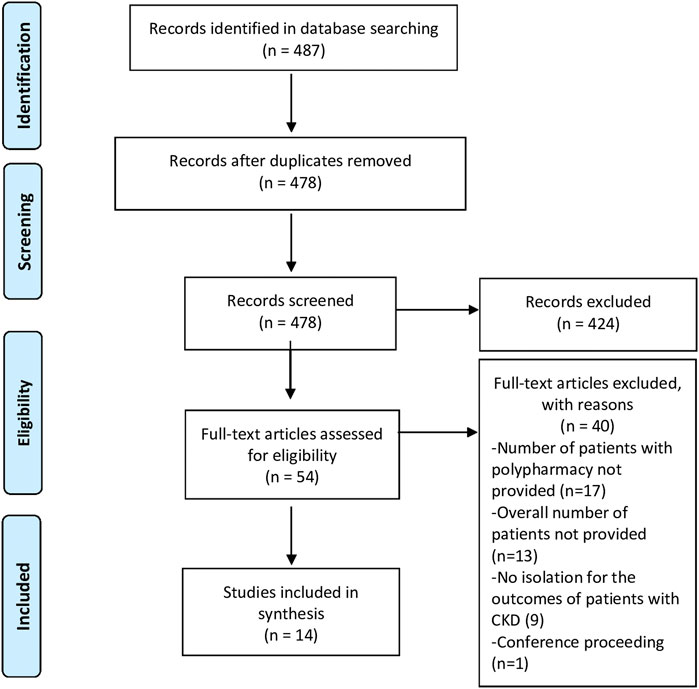
FIGURE 1. PRISMA flow diagram of the study selection process.
Table 1 summarizes the characteristics of the included studies. The reviewed studies were distributed across four continents with three studies conducted in the USA (Bowling et al., 2014; Sutaria et al., 2016; Hawley et al., 2019), two in Germany (König et al., 2017; Schmidt et al., 2019), and one each in Canada (Battistella et al., 2018), Saudi Arabia (Meraya and Alwhaibi, 2020), Lebanon (Chahine, 2020), Italy (Cojutti et al., 2016), India (Subeesh et al., 2020), Korea (Min et al., 2021), Japan (Kimura et al., 2021), and Ethiopia (Garedow et al., 2019). The last study took place across multiple European countries (Hayward et al., 2020). Of the 14 studies included, six were undertaken in outpatient settings (clinics, community dwelling) (Bowling et al., 2014; König et al., 2017; Battistella et al., 2018; Hawley et al., 2019; Schmidt et al., 2019; Hayward et al., 2020), four in hospitals (Garedow et al., 2019; Chahine, 2020; Subeesh et al., 2020; Kimura et al., 2021), two in multiple settings (Cojutti et al., 2016; Min et al., 2021), and two did not report (Sutaria et al., 2016; Meraya and Alwhaibi, 2020). Most studies were retrospective or prospective cohort studies (n = 6) (Sutaria et al., 2016; Garedow et al., 2019; Hawley et al., 2019; Schmidt et al., 2019; Hayward et al., 2020; Min et al., 2021), followed by cross–sectional observational studies (n = 5) (König et al., 2017; Battistella et al., 2018; Chahine, 2020; Meraya and Alwhaibi, 2020; Subeesh et al., 2020), longitudinal studies (n = 2) (Bowling et al., 2014; Kimura et al., 2021), and point-prevalence study (n = 1) (Cojutti et al., 2016). The follow-up duration ranged from 6 months (Garedow et al., 2019; Chahine, 2020; Subeesh et al., 2020) to 10 years across included studies (Min et al., 2021).
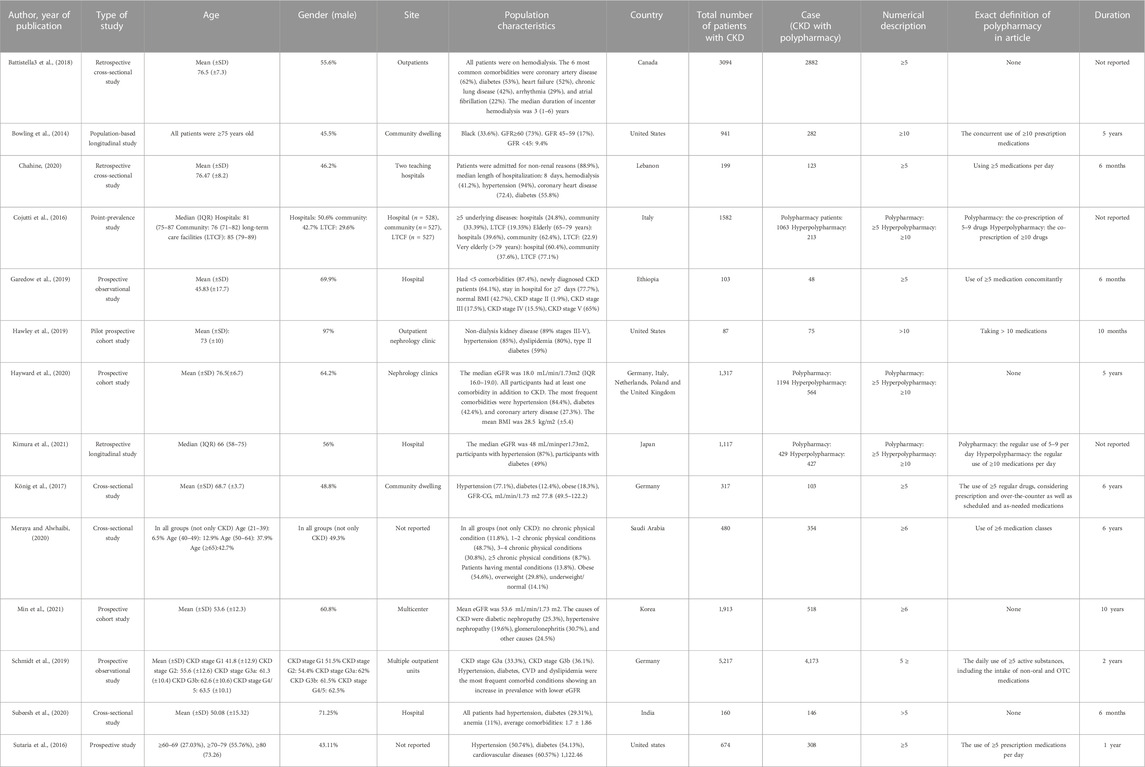
TABLE 1. Characteristics of included studies.
Overall, a total of N = 17 201 participants were included in this systematic review and meta-analysis, of which 43.88% were females. Among studies that reported the average age (n = 9), the mean age was 61.96 (SD ± 11.51) years. All the constituent studies had patients with at least one medical condition alongside the CKD, with hypertension being the most frequently reported. Other common co-morbidities were diabetes, coronary artery disease, and other cardiovascular diseases (Table 1). The stage of the CKD amongst the reviewed studies was variable. For instance, Battistella et al. (2018) focused exclusively on patients on hemodialysis (stage 5, glomerular filtration rate (GFR) <15 mL/min), while the majority of patients in Bowling et al. (2014) study and Schmidt et al. (2019) were in stage 2 (GFR >60 mL/min) and stage 3 (GFR 30–60 mL/min), respectively.
The overall quality of included studies was moderate to good mainly due to issues related to the sample size calculation and the appropriateness of outcome measures (Table 2).
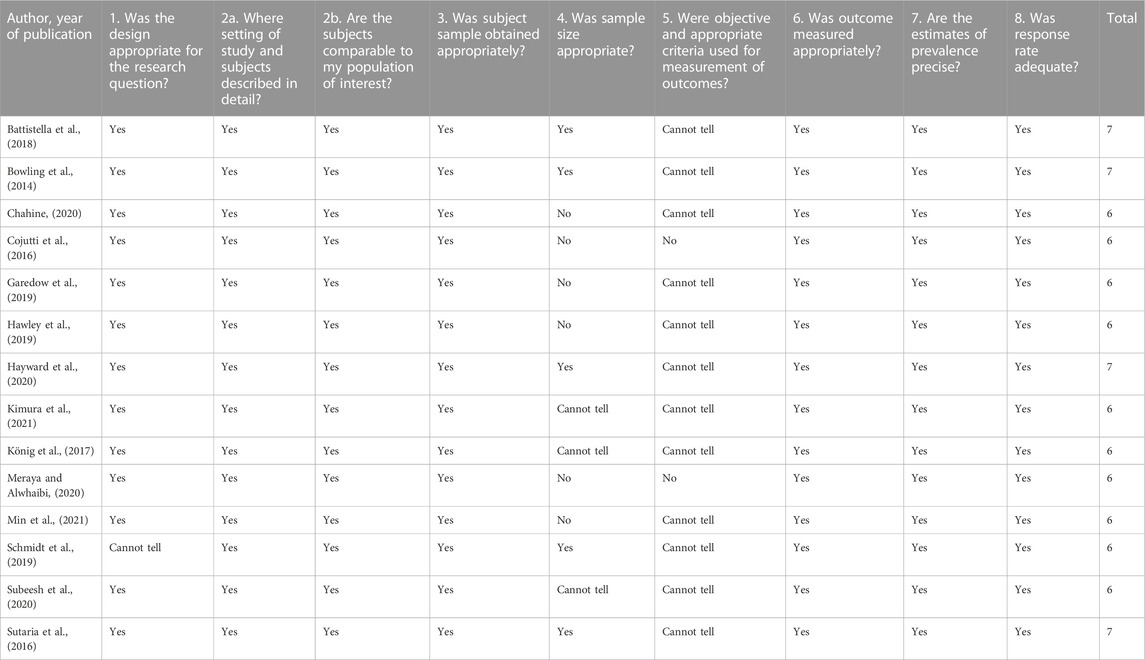
TABLE 2. Quality assessment of included studies.
Figure 2 presents the pooled estimates of the included studies. The overall pooled prevalence of polypharmacy amongst patients with CKD was 69% (95% CI: 49%–86%). The overall heterogeneity among the included studies was significant (I2 = 100%, p < 0.0001).
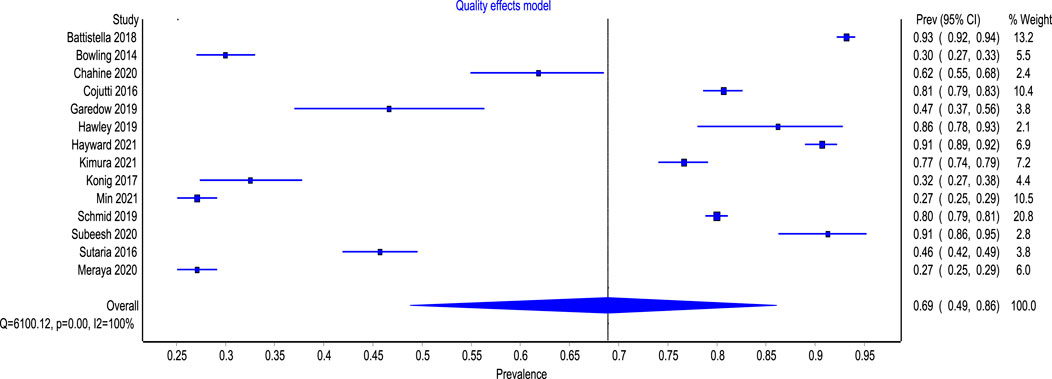
FIGURE 2. Forest plot of the prevalence of polypharmacy among patient with CKD.
Figures 3, 4 show the comparison adjusted funnel plot and Doi plot of the included studies. The plots demonstrated major (LFK 2.05) asymmetry which indicates major publication bias. This could also be attributed to the substantial between-study heterogeneity and small-study effect. No continuity correction was applied because the double arcsine prevalence transformation does not require one.
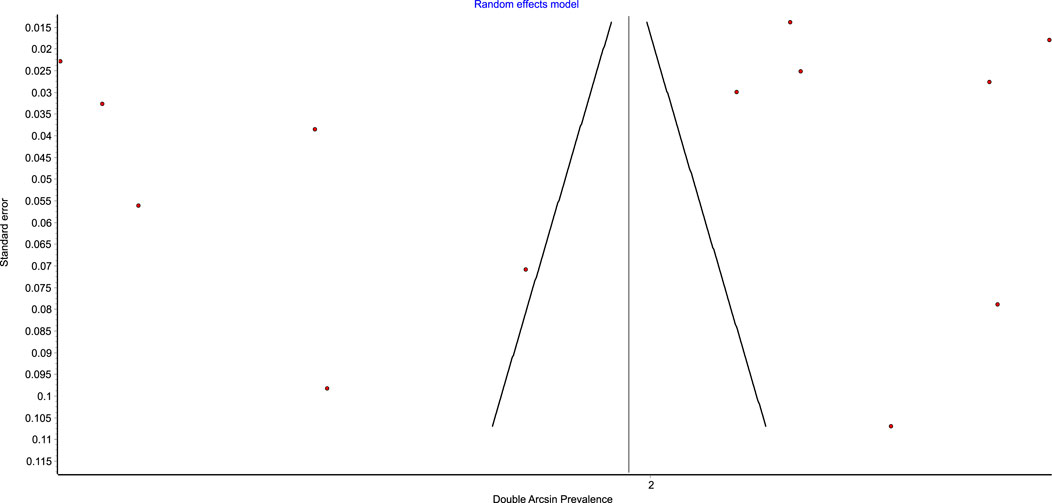
FIGURE 3. Funnel plot of the prevalence of polypharmacy among patient with CKD.
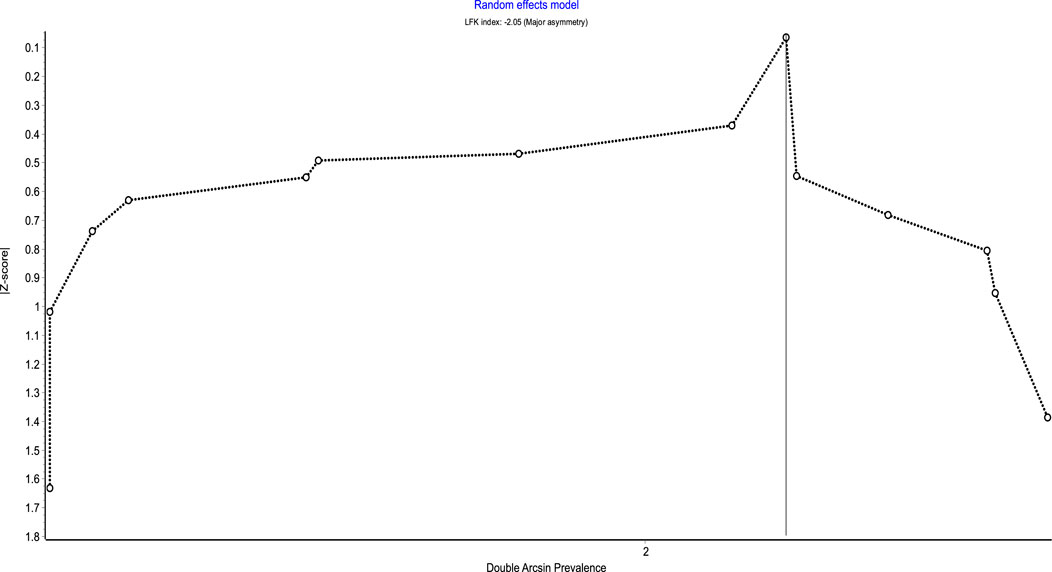
FIGURE 4. Doi plot of the prevalence of polypharmacy among patient with CKD.
A sensitivity analysis was also performed by excluding one study each time and recalculating the pooled prevalence of polypharmacy for the remaining studies (Table 3). Based on this, the estimated pooled prevalence of polypharmacy in patients with CKD ranged between 61% and 67%.
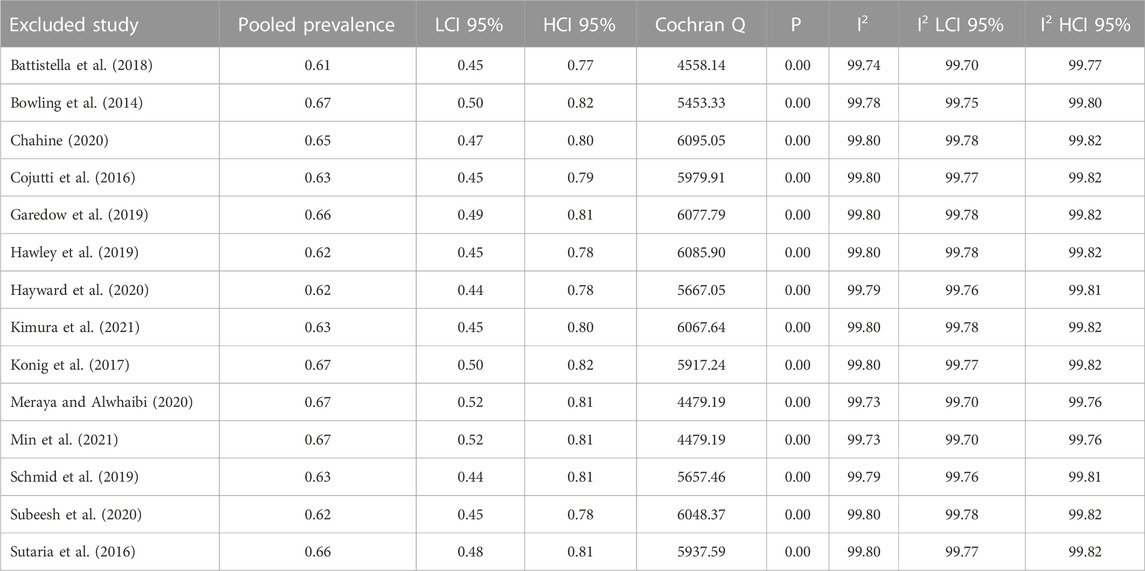
TABLE 3. Point estimates of the various included studies following sensitivity analysis.
The subgroup meta-regression showed a higher pooled prevalence of polypharmacy of 78% (95% CI: 63%–92%) in Europe and 78% (95% CI: 15%–100%) in North America as compared with 48% (95% CI: 0%–100%) in Asia (Figure 5). The overall heterogeneity was significant for both overall analysis (I2 = 100%, p < 0.0001) and subgroup analyses (I2 = 99%, p < 0.01), (I2 = 100%, p < 0.01), (I2 = 100%, p < 0.01) for the European, North American, and Asian studies, respectively.
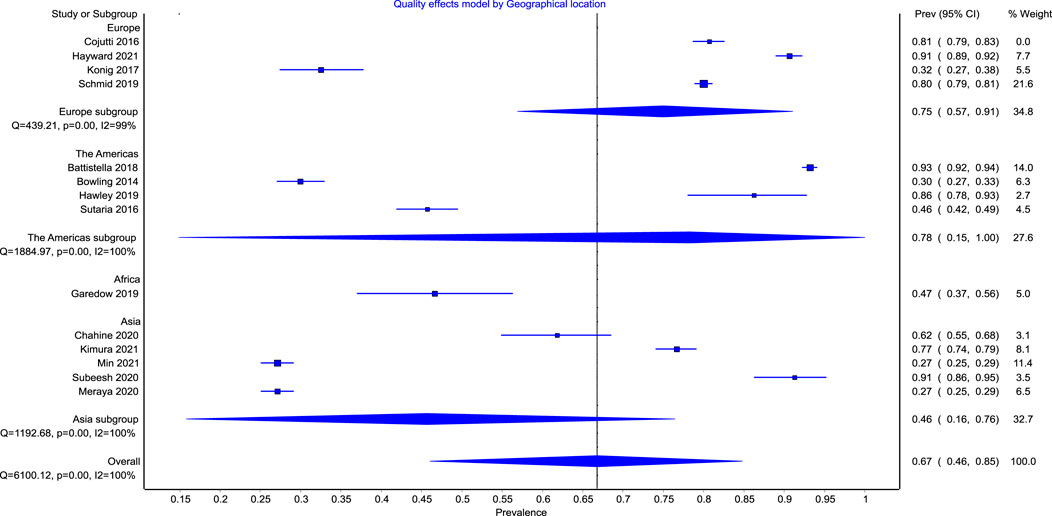
FIGURE 5. Forest plot of the prevalence of polypharmacy among patient with CKD across continents.
Only one study was identified from Africa (Garedow et al., 2019), therefore estimating the pooled prevalence was not feasible. Similarly, we could not calculate the prevalence in South America, Antarctica, or Australia as no relevant studies were identified from these continents.
To the best of our knowledge, this systematic review and meta-analysis represents the first comprehensive synthesis of the prevalence of polypharmacy and the global trends associated with its variability among patients with CKD. We explored the longitudinal data of 17,201 patients from 13 countries in 4 continents. The overall pooled prevalence of polypharmacy amongst patients with CKD was 69% with a proportionately higher prevalence in North America and Europe as compared to Asia. Despite the apparent disparity in the stage of CKD amongst the included studies, our period prevalence estimate provides the first attempt at exploring the burden of this growing therapeutic morbidity in this cohort of patients.
The prevalence estimates reported in this review are substantially higher than the general population including cohorts at high risk of experiencing polypharmacy such as elderly (Veehof et al., 2000), patients with chronic liver disease (Danjuma et al., 2022a), and people living with HIV (Danjuma et al., 2022b). However, the estimates were comparable to other populations that are also known to be more exposed to polypharmacy such as heart failure patients (Beezer et al., 2021).
This remarkably high prevalence is alarming particularly in CKD patients as they represent a more challenging and therapeutically vulnerable population; principally due to the central role of the kidney in drug metabolism (including other aspects of pharmacokinetics and pharmacodynamics) (Laville et al., 2020). This therefore imposes higher risk of adverse drug reactions (ADR) and their sequalae on patients with CKD (Laville et al., 2020).
Additionally, patients included in our review had an average age of 61.96 (SD ± 11.51) years, which is expected as CKD in more prevalent in people older than 60 years old (Aging and Kidney, 2022). This further complicates the situation as there is mounting evidence of the increased risk of mortality in response to increased drug counts, especially in the elderly (Patel et al., 2017; Davies et al., 2022). For instance, the Newcastle 85 + study showed that for each additional medication prescribed in patients aged 85 years and older, there is a 3% associated risk of increased mortality (hazard ratio: 1.03, 95% CI: 1.00–1.06) (Davies et al., 2022).
Our findings underscore the gravity of the rising burden of polypharmacy among patients with CKD and highlight the pressing need to adopt some of the interventions that have been proposed to reduce the burden of polypharmacy in the general population. This includes comprehensive medication reviews, deprescribing algorithms, potentially inappropriate medications (PIM) screening tools (e.g., Beers criteria), and clinical pharmacist-led interventions (Cooper et al., 2015; El-Awaisi et al., 2022; Isleem et al., 2022). It is noteworthy that these interventions are not widespread and that the research on the effectiveness of such strategies on clinically important outcomes is limited (Cooper et al., 2015). Hence, future research efforts should focus on measuring the effectiveness of these interventions. Moreover, experts should attempt at developing multifaceted theory-based interventions that are tailored to patients with CKD. This approach is expected to yield promising outcomes as other methods of interventions development [i.e., pragmatic approach or ISLAGIATT (It Seemed Like A Good Idea At The Time) principle] were checkered, with some showing unfavorable outcomes or no benefit at all (Michie et al., 2005; Hughes et al., 2016; Steinmo et al., 2016).
The principal strength of this synthesis lies in its novelty at estimating the overall pooled prevalence of polypharmacy among patients with CKD. This will enable clinicians, as well as policy makers, and other stakeholders to more robustly estimate the burden of polypharmacy and more appropriately allocate intervention strategies aimed at mitigating their downstream effects (including bidirectional interactions as well as adverse drug reactions). The review also involved comprehensive searching of three large databases using established methods and was reported following a standardized method. Despite this, there were several limitations. Firstly, only English language publications were included. Secondly, polypharmacy prevalence was not the primary outcome measure in many of the included studies which resulted in the lack of in-depth information relating to it. Finally, significant heterogeneity was noted across the included studies. This could be attributed to the variation in the definition of polypharmacy among included studies. Other factors include the various study design, the geographical disposition of areas where the studies were carried out, and the difference in the mean age of the constituent studies.
The results from this meta-analysis showed a high pooled prevalence estimates of polypharmacy amongst patient cohorts with CKD. The exact interventions that are likely to significantly mitigate its effect remain uncertain and will need exploration by future prospective and systematic studies.
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author.
Conceptualization: LN and MD. Literature search: LN, AA, MK, and MD. Independent review and risk of bias assessment: LN, AA, MK, and MD. Data curation: AA and MK. Data analysis and synthesis: LN and MD. Initial draft of manuscript: LN and MD. Final manuscript: LN, AA, MK, and MD.
Open Access funding provided by the Qatar National Library.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Bansal, N., Katz, R., Robinson-Cohen, C., Odden, M., Dalrymple, L., Shlipak, M., et al. (2017). Absolute rates of heart failure, coronary heart disease, and stroke in chronic kidney disease: An analysis of 3 community-based cohort studies. JAMA Cardiol. 2 (3), 314–318. doi:10.1001/jamacardio.2016.4652
Battistella, M., Jandoc, R., Ng, J., McArthur, E., and Garg, A. (2018). A province-wide, cross-sectional study of demographics and medication use of patients in hemodialysis units across ontario. Can. J. Kidney Health Dis. 5, 2054358118760832. doi:10.1177/2054358118760832
Beezer, J., Al Hatrushi, M., Husband, A., Kurdi, A., and Forsyth, P. (2021). Polypharmacy definition and prevalence in heart failure: A systematic review. Heart Fail. Rev. 27 (2), 465–492. doi:10.1007/s10741-021-10135-4
Bello, A., Alrukhaimi, M., Ashuntantang, G., Basnet, S., Rotter, R., Douthat, W., et al. (2017). Complications of chronic kidney disease: Current state, knowledge gaps, and strategy for action. Kidney Int. Suppl. 7 (2), 122–129. doi:10.1016/j.kisu.2017.07.007
Bowling, C., Booth, J., Gutiérrez, O., Kurella Tamura, M., Huang, L., Kilgore, M., et al. (2014). Nondisease-specific problems and all-cause mortality among older adults with CKD: The REGARDS study. Clin. J. Am. Soc. Nephrol. 9 (10), 1737–1745. doi:10.2215/CJN.00880114
Chahine, B. (2020). Potentially inappropriate medications prescribing to elderly patients with advanced chronic kidney by using 2019 American Geriatrics Society Beers Criteria. Health Sci. Rep. 3 (4), e214. doi:10.1002/hsr2.214
Cojutti, P., Arnoldo, L., Cattani, G., Bruniferro, S., and Pea, F. (2016). Polytherapy and the risk of potentially inappropriate prescriptions (PIPs) among elderly and very elderly patients in three different settings (hospital, community, long-term care facilities) of the friuli venezia giulia region, Italy: Are the very elderl. Pharmacoepidemiol. Drug Saf. 25 (9), 1070–1078. doi:10.1002/pds.4026
Cooper, J., Cadogan, C., Patterson, S., Kerse, N., Bradley, M., Ryan, C., et al. (2015). Interventions to improve the appropriate use of polypharmacy in older people: A Cochrane systematic review. BMJ Open 5 (12), e009235. doi:10.1136/bmjopen-2015-009235
Couser, W., Remuzzi, G., Mendis, S., and Tonelli, M. (2011). The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney Int. 80 (12), 1258–1270. doi:10.1038/ki.2011.368
Danjuma, M., Adegboye, O., Aboughalia, A., Soliman, N., Almishal, R., Abdul, H., et al. (2022). Prevalence and global trends of polypharmacy among people living with HIV: A systematic review and meta-analysis. Ther. Adv. Drug Saf. 13, 20420986221080795. doi:10.1177/20420986221080795
Danjuma, M., Naseralallah, L., Ansari, S., Alshibly, R., Elhams, M., Alshamri, M., et al. (2022). Prevalence and global trends of polypharmacy in patients with chronic liver disease: A systematic review and meta-analysis (preprint).
Davies, L., Kingston, A., Todd, A., and Hanratty, B. (2022). Is polypharmacy associated with mortality in the very old: Findings from the Newcastle 85+ Study. Br. J. Clin. Pharmacol. 88 (6), 2988–2995. doi:10.1111/bcp.15211
Delmez, J., and Slatopolsky, E. (1992). Hyperphosphatemia: Its consequences and treatment in patients with chronic renal disease. Am. J. Kidney Dis. 19 (4), 303–317. doi:10.1016/s0272-6386(12)80446-x
El-Awaisi, A., Al-Shaibi, S., Al-Ansari, R., Naseralallah, L., and Awaisu, A. (2022). A systematic review on the impact of pharmacist-provided services on patients’ health outcomes in Arab countries. J. Clin. Pharm. Ther. 47 (7), 879–896. doi:10.1111/jcpt.13633
Furuya-Kanamori, L., Barendregt, J. J., and Doi, S. A. R. (2018). A new improved graphical and quantitative method for detecting bias in meta-analysis. Int. J. Evidence-Based Healthc. 16 (4), 195–203. doi:10.1097/XEB.0000000000000141
Gansevoort, R., Matsushita, K., van der Velde, M., Astor, B., Woodward, M., Levey, A., et al. (2011). Lower estimated GFR and higher albuminuria are associated with adverse kidney outcomes. A collaborative meta-analysis of general and high-risk population cohorts. Kidney Int. 80 (1), 93–104. doi:10.1038/ki.2010.531
Garedow, A., Mulisa Bobasa, E., Desalegn Wolide, A., Kerga Dibaba, F., Gashe Fufa, F., Idilu Tufa, B., et al. (2019). Drug-related problems and associated factors among patients admitted with chronic kidney disease at jimma university medical center, jimma zone, jimma, southwest Ethiopia: A hospital-based prospective observational study. Int. J. Nephrol. 2019, 1504371–1504379. doi:10.1155/2019/1504371
Hawley, C., Triantafylidis, L., and Paik, J. (2019). The missing piece: Clinical pharmacists enhancing the interprofessional nephrology clinic model. J. Am. Pharm. Assoc. 59 (5), 727–735. doi:10.1016/j.japh.2019.05.010
Hayward, S., Hole, B., Denholm, R., Duncan, P., Morris, J., Fraser, S., et al. (2020). International prescribing patterns and polypharmacy in older people with advanced chronic kidney disease: Results from the European quality study. Nephrol. Dial. Transplant. 36 (3), 503–511. doi:10.1093/ndt/gfaa064
Higgins, J. P. T., Thompson, S. G., Deeks, J. J., and Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ [Internet] 327 (7414), 557–560. doi:10.1136/bmj.327.7414.557
Hsu, C., McCulloch, C., and Curhan, G. (2002). Epidemiology of anemia associated with chronic renal insufficiency among adults in the United States: Results from the third national health and nutrition examination survey. J. Am. Soc. Nephrol. 13 (2), 504–510. doi:10.1681/ASN.V132504
Hughes, C. M., Cadogan, C. A., and Ryan, C. A. (2016). Development of a pharmacy practice intervention: Lessons from the literature. Int. J. Clin. Pharm. 38 (3), 601–606. doi:10.1007/s11096-015-0180-6
Isleem, N., Shoshaa, S., AbuGhalyoun, A., Khatib, M., Naseralallah, L., Ibn-Mas'ud Danjuma, M., et al. (2022). Critical care tele-pharmacy services during covid -19 pandemic: A qualitative exploration of healthcare practitioners' perceptions. J. Clin. Pharm. Ther. 47, 1591–1599. doi:10.1111/jcpt.13709
James, M., Hemmelgarn, B., and Tonelli, M. (2010). Early recognition and prevention of chronic kidney disease. Lancet 375 (9722), 1296–1309. doi:10.1016/S0140-6736(09)62004-3
Jankowski, J., Floege, J., Fliser, D., Böhm, M., and Marx, N. (2021). Cardiovascular disease in chronic kidney disease: Pathophysiological insights and therapeutic options. Circulation 143 (11), 1157–1172. doi:10.1161/CIRCULATIONAHA.120.050686
Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group (2013). KGIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 3 (1), 1–150.
Kimura, H., Tanaka, K., Saito, H., Iwasaki, T., Oda, A., Watanabe, S., et al. (2021). Association of polypharmacy with kidney disease progression in adults with CKD. Clin. J. Am. Soc. Nephrol. 16 (12), 1797–1804. doi:10.2215/CJN.03940321
König, M., Gollasch, M., Demuth, I., and Steinhagen-Thiessen, E. (2017). Prevalence of impaired kidney function in the German elderly: Results from the berlin aging study II (BASE-II). Gerontology 63 (3), 201–209. doi:10.1159/000454831
Laville, S., Gras-Champel, V., Moragny, J., Metzger, M., Jacquelinet, C., Combe, C., et al. (2020). Adverse drug reactions in patients with CKD. Clin. J. Am. Soc. Nephrol. 15 (8), 1090–1102. doi:10.2215/CJN.01030120
Loney, P. L., Chambers, L. W., Bennett, K. J., Roberts, J. G., and Stratford, P. W. (1998). Critical appraisal of the health research literature: Prevalence or incidence of a health problem. Chronic Dis. Can. 19 (4), 170–176.
Meraya, A., and Alwhaibi, M. (2020). Health related quality of life and healthcare utilization among adults with diabetes and kidney and eye complications in the United States. Health Qual. Life Outcomes 18 (1), 85. doi:10.1186/s12955-020-01336-w
Michie, S., Johnston, M., Abraham, C., Lawton, R., Parker, D., Walker, A., et al. (2005). Making psychological theory useful for implementing evidence based practice: A consensus approach. Qual. Saf. Health Care 14 (1), 26–33. doi:10.1136/qshc.2004.011155
Min, H., Sung, S., Chung, W., Kim, Y., Chae, D., Ahn, C., et al. (2021). Polypharmacy and the progression of chronic kidney disease: Korean cohort study for outcome in patients with chronic kidney disease. Kidney Blood Press. Res. 46 (4), 460–468. doi:10.1159/000516029
Parker, K., and Wong, J. (2019). Is polypharmacy an increasing burden in chronic kidney disease? The German experience. Clin. Kidney J. 12 (5), 659–662. doi:10.1093/ckj/sfz072
Patel, P., Hayward, K., Rudra, R., Horsfall, L., Hossain, F., Williams, S., et al. (2017). Multimorbidity and polypharmacy in diabetic patients with NAFLD: Implications for disease severity and management. Medicine 96 (26), e6761. doi:10.1097/MD.0000000000006761
Quintana, D. S. (2015). From pre-registration to publication: A non-technical primer for conducting a meta-analysis to synthesize correlational data. Front. Psychol. 6, 1549. doi:10.3389/fpsyg.2015.01549
Schmidt, I., Hübner, S., Nadal, J., Titze, S., Schmid, M., Bärthlein, B., et al. (2019). Patterns of medication use and the burden of polypharmacy in patients with chronic kidney disease: The German chronic kidney disease study. Clin. Kidney J. 12 (5), 663–672. doi:10.1093/ckj/sfz046
Stefanski, A., Schmidt, K., Waldherr, R., and Ritz, E. (1996). Early increase in blood pressure and diastolic left ventricular malfunction in patients with glomerulonephritis. Kidney Int. 50 (4), 1321–1326. doi:10.1038/ki.1996.444
Steinmo, S. H., Michie, S., Fuller, C., Stanley, S., Stapleton, C., and Stone, S. P. (2016). Bridging the gap between pragmatic intervention design and theory: Using behavioural science tools to modify an existing quality improvement programme to implement “sepsis six”. Implement. Sci. 11 (1), 14. doi:10.1186/s13012-016-0376-8
Subeesh, V., Abraham, R., Satya Sai, M., and Koonisetty, K. (2020). Evaluation of prescribing practices and drug-related problems in chronic kidney disease patients: A cross-sectional study. Perspect. Clin. Res. 11 (2), 70–74. doi:10.4103/picr.PICR_110_18
Sutaria, A., Liu, L., and Ahmed, Z. (2016). Multiple medication (polypharmacy) and chronic kidney disease in patients aged 60 and older: A pharmacoepidemiologic perspective. Ther. Adv. Cardiovasc. Dis. 10 (4), 242–250. doi:10.1177/1753944716634579
Veehof, L., Stewart, R., Haaijer-Ruskamp, F., and Jong, B. (2000). The development of polypharmacy. A longitudinal study. Fam. Pract. 17 (3), 261–267. doi:10.1093/fampra/17.3.261
Whittaker, C., and Fink, J. (2017). Deprescribing in CKD: The proof is in the process. Am. J. Kidney Dis. 70 (5), 596–598. doi:10.1053/j.ajkd.2017.05.025
Widmer, B., Gerhardt, R. E., Harrington, J. T., and Cohen, J. J. (1979). Serum electrolyte and acid base composition. The influence of graded degrees of chronic renal failure. Archives Intern. Med. 139 (10), 1099–1102. doi:10.1001/archinte.139.10.1099
Keywords: polypharmacy, chronic kidney disease (CKD), epidemiology, systematic review, meta-analysis
Citation: Naseralallah L, Khatib M, Al-Khulaifi A and Danjuma M (2023) Prevalence and global trends of polypharmacy in patients with chronic kidney disease: A systematic review and meta-analysis. Front. Pharmacol. 14:1122898. doi: 10.3389/fphar.2023.1122898
Received: 23 December 2022; Accepted: 30 January 2023;
Published: 10 February 2023.
Edited by:
Robert L. Lins, Independent researcher, Antwerp, BelgiumReviewed by:
Uda Venkat Mateti, Nitte (Deemed to be University), IndiaCopyright © 2023 Naseralallah, Khatib, Al-Khulaifi and Danjuma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lina Naseralallah, TE5hc2VyYWxhbGxhaEBoYW1hZC5xYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.