
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 09 March 2023
Sec. Drug Metabolism and Transport
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1118788
 Fang Huang1†
Fang Huang1† Wen-Xiang Cao1†
Wen-Xiang Cao1† Yu-Ying Yan2Tian-Tian Mao3Xian-Wen Wang3Dan Huang3Yu-Shuang Qiu1Wen-Jie Lu1
Yu-Ying Yan2Tian-Tian Mao3Xian-Wen Wang3Dan Huang3Yu-Shuang Qiu1Wen-Jie Lu1 Dong-Jie Li1*Yu-Gang Zhuang3*
Dong-Jie Li1*Yu-Gang Zhuang3*Objective: The influence of continuous renal replacement therapy (CRRT) on the steady-state plasma concentration of high-dose tigecycline was investigated in septic shock patients to provide references for drug dosing.
Methods: In this prospective observational study, 17 septic shock patients presenting with severe infections needing a broad-spectrum antibiotic therapy with high-dose tigecycline (100 mg per 12 h) in the intensive care unit were included and divided into CRRT group (n = 6) or non-CRRT group (n = 11). The blood samples were collected and plasma drug concentration was determined by SHIMADZU LC-20A and SHIMADZU LCMS 8040. The steady-state plasma concentration was compared between groups using unpaired t-test. Furthermore, between-groups comparisons adjusted for baseline value was also done using multivariate linear regression model.
Results: Peak concentration (Cmax) of tigecycline was increased in CRRT group compared to non-CRRT group, but there were no statistical differences (505.11 ± 143.84 vs. 406.29 ± 108.00 ng/mL, p-value: 0.129). Trough concentration (Cmin) of tigecycline was significantly higher in CRRT group than in non-CRRT group, with statistical differences (287.92 ± 41.91 vs. 174.79 ± 33.15 ng/mL, p-value: 0.000, adjusted p-value: 0.000). In safety, Cmin was reported to be a useful predictor of hepatotoxicity with a cut-off of 474.8 ng/mL. In our studies, Cmin of all patients in CRRT group was lower than 474.8 ng/mL.
Conclusion: The plasma concentration of tigecycline was increased in septic shock patients with CRRT treatment and only Cmin shown statistical differences. No dose adjustment seems needed in the view of hepatotoxicity.
Clinical Trial Registration: https://www.chictr.org.cn/, identifier ChiCTR2000037475.
Tigecycline, a novel tetracycline, has been approved by the Chinese Food and Drug Administration for the treatment of complicated intraabdominal infection, complicated skin and skin structure infections, and adult community-acquired pneumonia since 2005 (Pankey, 2005; Zhou et al., 2022). By inhibiting the protein synthesis of bacteria by binding to the 30 S ribosomal subunit and blocking the entry of aminoacyl tRNA into the A side of the ribosome, tigecycline exhibits broad-spectrum antibacterial activity against G-positive bacteria, G-negative bacteria, and anaerobic bacteria, especially multidrug-resistant bacteria, making it an important antibiotic for critically infected patients (Qu et al., 2009; Hawser et al., 2010; Dowzicky and Chmelařová, 2011; Hu et al., 2012; Gilbert et al., 2020).
Septic shock is a major cause of death in intensive care units (ICUs), with a mortality rate of 15%–30% or even higher (Singer et al., 2016; Howell and Davis, 2017; de Grooth et al., 2018). Sepsis leads to approximately 50% of acute kidney injury (AKI) cases; therefore, septic shock patients often require continuous renal replacement therapy (CRRT), which replaces the kidney’s function of blood filtration and affects the metabolism of drugs, including anti-infective agents (Bellomo et al., 2017; Li et al., 2020). Antibiotics are the core of sepsis therapy (Marshall, 2014). Tigecycline is one of the limited options for treatment of septic shock, and high-dose tigecycline (100 mg every 12 h) is widely used in clinical practice (De Pascale et al., 2014; Geng et al., 2018; Alsemari et al., 2020; Zhao et al., 2020). Consequently, septic shock patients who undergo CRRT often require antibiotic therapy with high-dose tigecycline. Providing appropriate antibiotic exposure is extremely pivotal for these patients to improve clinical outcomes, but the influence of CRRT on the plasma concentration of high-dose tigecycline remains unclear, making drug dosing more challenging in such settings (MacArthur et al., 2004; Roggeveen et al., 2022). Broeker et al. proposed that no dose adjustment of tigecycline was necessary in critically ill patients undergoing CRRT, but Patrick M. Honoure et al. pointed out that the view was somewhat premature (Broeker et al., 2018; Honore et al., 2020).
In the present study, the influence of CRRT on the steady-state plasma concentration of high-dose tigecycline was investigated in septic shock patients to provide references for drug dosing.
A prospective observational study was performed in the 23-bed ICU of the 10th People’s Hospital of Tongji University between 2020 and 2021. The protocol was approved by the hospital’s Ethical Committee (approval number 2020KT62) and has also been registered on chictr.org.cn (ChiCTR2000037475). This study was performed in accordance with the Helsinki Declaration and its later amendments. Written informed consent was obtained from the patients or their legally authorized representatives. ICU patients meeting the criteria of septic shock according to the sepsis-3 criteria were eligible for inclusion (Singer et al., 2016). The major exclusion criteria were an age <18 years, severe hepatic failure (Child–Pugh C), hyperbilirubinemia (bilirubin level higher than 3 mg/dL), or a history of allergy to tigecycline. Seventeen patients were included and completed this study. Patients were divided into two groups according to continuous renal replacement therapy (CRRT) conditions: a non-CRRT group for patients who did not require CRRT and a CRRT group for patients who underwent CRRT at least once. The criteria for CRRT included both metabolic emergencies and persistent acute kidney injury.
Patients were treated with continuous veno-venous haemodiafiltration (CVVHDF) using the Baxter system equipped with AN69-ST membrane (Baxter Healthcare, Chicago, United States). The bicarbonate replacement solution was used for both dialysis at a rate of 2000 mL/h and postfilter fluid replacement (postdilution) at the same rate. The blood flow rate was 160 mL/min. Additionally, the fluid clearance was 200 mL/h. Anticoagulation was achieved with unfractionated heparin, targeting an activated clotting time 1.5-times greater than that at baseline.
The demographic and outcome data were collected by doctors and pharmacists, including age, gender, site of infection, comorbidities, clinical outcomes, the Acute Physiology and Chronic Health Evaluation II (APACHE II) score and the sequential organ failure assessment (SOFA) score. Laboratory parameters such as alanine transaminase (ALT), aspartate aminotransferase (AST), total bilirubin (TB), conjugated bilirubin (CB), serum albumin (ALB), pre-BNP, creatinine (Cr), and urea nitrogen (BUN) were also collected.
Patients were treated with 100 mg of tigecycline every 12 h intravenously. From each patient, at least two blood samples were taken after at least six doses when the serum tigecycline reached steady state: blood sample A (Cmax) was collected at 0.5 h after the completion of an intravenous infusion of tigecycline for the determination of the peak concentration, and blood sample B (Cmin) was a predose concentration taken at the end of a dosing interval (within 0.5 h before the next dose) (Xu et al., 2019). Blood samples were collected using anticoagulation tubes, centrifuged at 1,500 rpm for 10 min, and stored at −80°C until assayed.
Serum tigecycline samples were analyzed by a validated liquid chromatography with mass spectrometry (LC–MS-MS) method using SHIMADZU LC-20A and SHIMADZU LCMS 8040 Triple Quadruple MS/MS (Shimane Shimadzu Corporation, Japan). The mobile phase consisted of 0.1% formic acid water (A)—0.1% formic acid acetonitrile (B). The elution gradient was as follows: 0–1.5 min 5% B; 1.5–5 min 5%–95% B; 5–5.1 min 95%–5% B; 5.1–8 min 5% B. Tigecycline and the internal standard were eluted from an XSelect@HSS T3 column with a total run time of 8 min. Detection was carried out using mass spectrometry. For sample preparation of serum, a 50 μL serum sample was mixed with 150 μL of internal standard working solution (internal standard concentration: 100 ng/mL), vortexed for 1 min, and centrifuged for 15 min at 13,000 rpm, 4°C. Finally, the supernatant was tested. The internal standard 2-chlorophenylalanine was purchased from Sigma‒Aldrich (St. Louis, Missouri, United States).
The endpoint of the study was the steady-state tigecycline concentration in the serum, which was compared between non-CRRT and CRRT patients who experienced severe infections and needed broad-spectrum antibiotic therapy with tigecycline. The steady-state tigecycline concentration in the serum was labelled Cmax and Cmin for each patient.
Data are presented as the mean ± SD, median ± interquartile range (interquartile range, IQR) or numbers (%) and were compared between the non-CRRT and CRRT groups using unpaired t-test, the Mann‒Whitney U test, or Fisher’s exact test according to the distribution and category of the variables.
Adjusted analyses for the tigecycline concentration were performed using a multivariate linear regression analysis model, considering potential cofounders that were not fully balanced at baseline. In order to meet the requirements of Event Per Variable, related variables CRRT, ALB, ALT, AST, and TB were selected by bootstrapped stepwise regression method (Henderson et al., 2016). CB was not included because TB contained CB. At the same time, Cr was also not included due to CRRT replaces the kidney’s function. Bootstrapping created 1,000 resampling randomly. Backwards stepwise variable selection was performed on each bootstrap dataset, separately for each outcome (Cmin or Cmax). The frequency that a variable was selected by the variable selection procedure on the 1,000 bootstrap samples (bootstrap inclusion frequency, BIF) was used to identify important variables that should be further investigated. Variables with BIF ≥ 50% were included in the final multivariate linear regression model.
Statistical analyses were performed by IBM SPSS Statistics, version 19, and SAS, version 9.4. A p-value of <0.05 was deemed statistically significant.
According to the inclusion criteria, a total of 17 septic shock patients in the ICU were enrolled in this study and were categorized into the CRRT group (n = 6) or non-CRRT group (n = 11) considering CRRT status (Table 1).
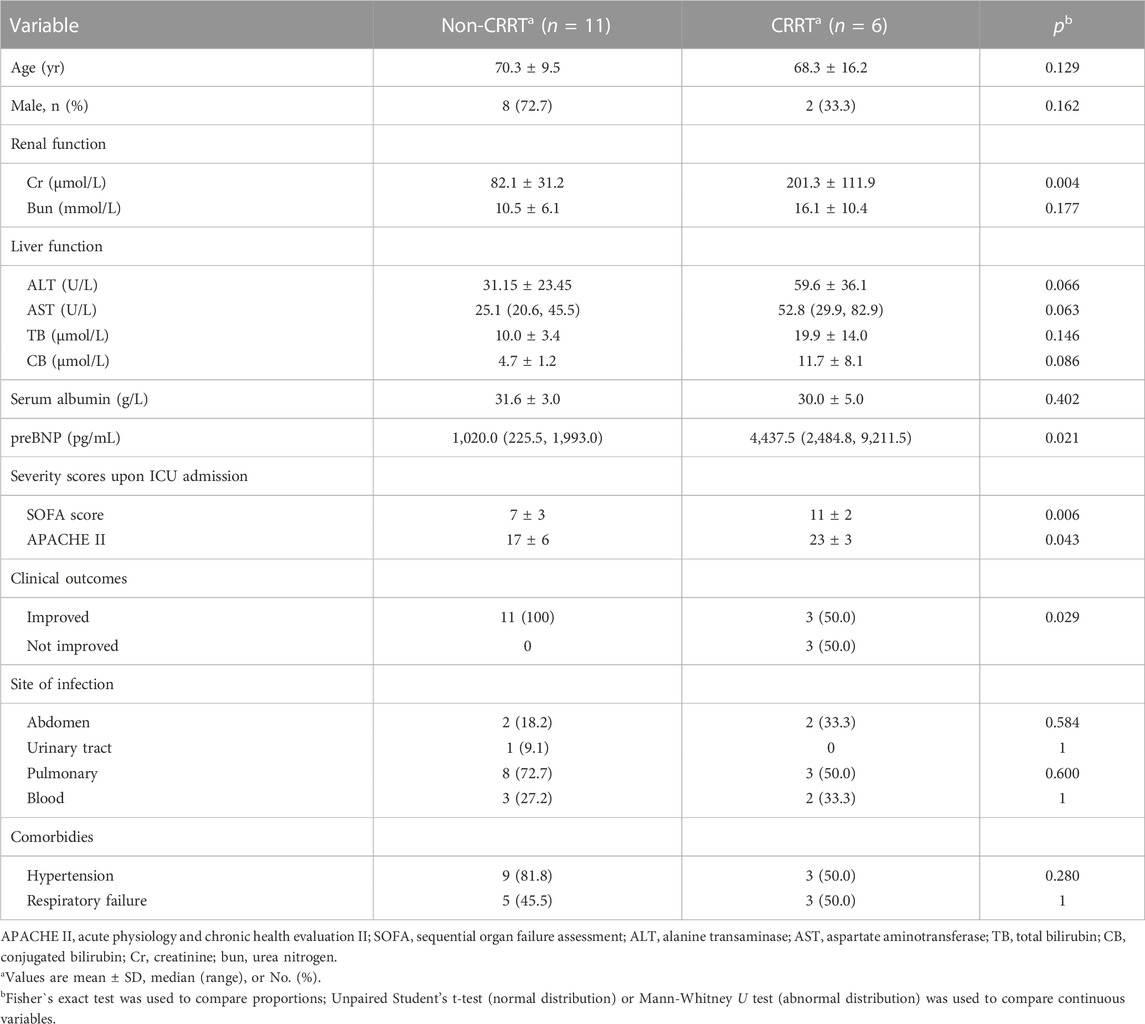
TABLE 1. Characteristics of enrolled patients.
Patients were treated with 100 mg of tigecycline every 12 h due to infections in the abdomen (n = 4), lungs (n = 11), blood (n = 5), and urinary tract (n = 1) (Table 1). The major infection type was pneumonia, and four patients had more than one infection site. The levels of preBNP (p-value: 0.021) and Cr (p = 0.004) and the SOFA (p-value: 0.006) and APACHE II scores (p-value: 0.043) were much higher in the CRRT group than in the non-CRRT group (Table 1). The clinical outcome of the non-CRRT group was better than that of the CRRT group (p-value: 0.029). There were no significant differences in the remaining clinical characteristics between the two groups.
The serum steady-state tigecycline concentrations in each patient are shown in Table 2; Table 3. The mean serum tigecycline concentrations for each group were calculated and are presented as the mean ± SD. The peak concentration (Cmax) of tigecycline was increased in the CRRT group compared to the non-CRRT group, but there were no significant differences between the two groups (505.11 ± 143.84 vs. 406.29 ± 108.00 ng/mL, p-value: 0.129) (Table 2). The trough concentration (Cmin) of tigecycline was significantly higher in the CRRT group than in the non-CRRT group, with significant differences (287.92 ± 41.91 vs. 174.79 ± 33.15 ng/mL, p-value: 0.000) (Table 3).
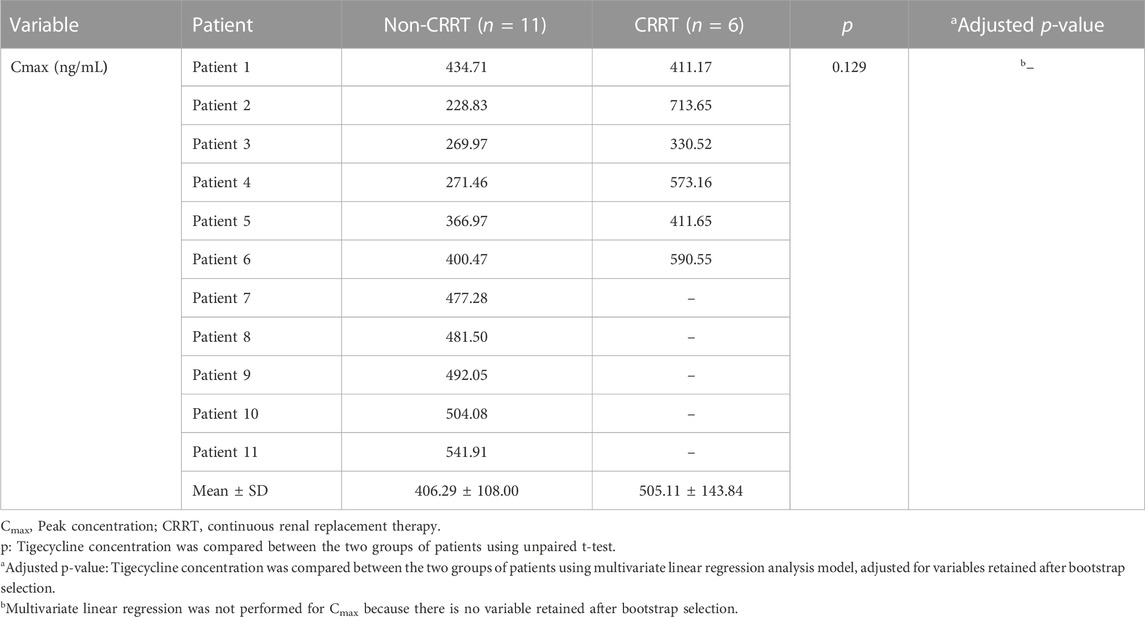
TABLE 2. Peak concentration of tigecycline in septic shock patients.
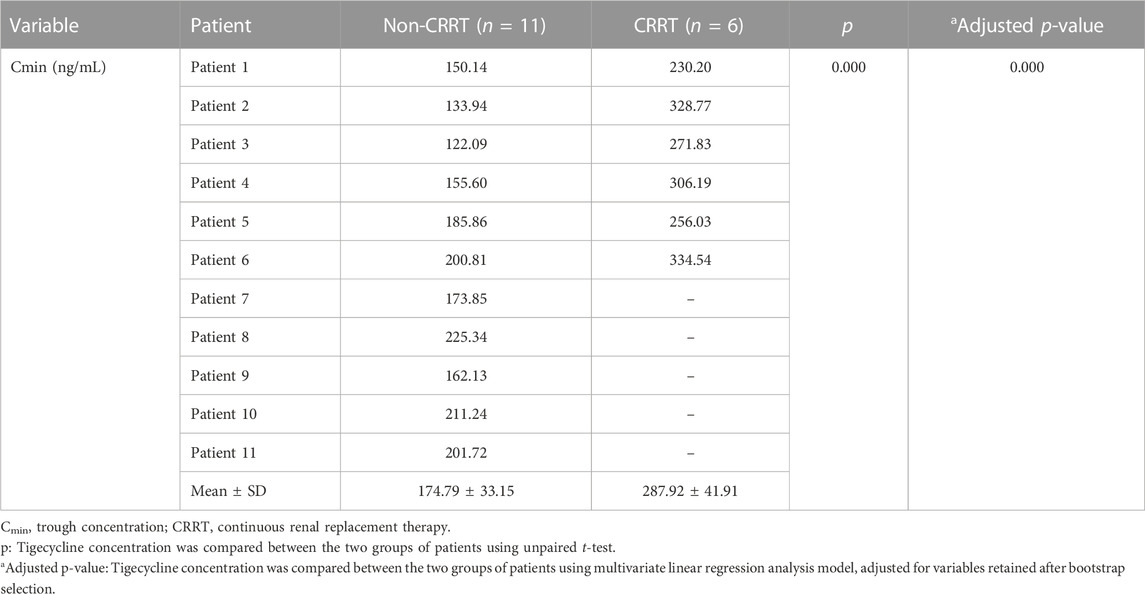
TABLE 3. Trough concentration of tigecycline in septic shock patients.
Adjusted analyses for the tigecycline concentration were performed using a multivariate linear regression analysis model, including variables retained after bootstrap selection. CRRT and ALT were included into the final multivariate linear regression model for Cmin. As for Cmax, there is no variable with a BIF of ≥50% after selection (Supplementary Table S1). The differences between the two groups were statistically significant in Cmin after adjusted for the effect of cofounding variable ALT (adjusted p-value for Cmin: 0.000) (Table 3). Multivariate linear regression was not performed for Cmax because there is no variable retained after bootstrap selection (Table 2).
Regarding safety, Cmin was reported to be a useful predictor of hepatotoxicity with a cut-off of 474.8 ng/mL. In our studies, Cmin was lower than 474.8 ng/mL for all patients in the CRRT group (Table 3).
Therefore, both Cmax and Cmin of tigecycline were increased in patients receiving CRRT treatment, but only Cmin showed significant differences. The increase in Cmin may not contribute to hepatotoxicity.
In the present study, the influence of CRRT on the steady-state plasma concentration of high-dose tigecycline was investigated in septic shock patients. Seventeen patients were divided into the CRRT or non-CRRT group and received high-dose tigecycline at 100 mg every 12 h intravenously. Both Cmax and Cmin were increased in the CRRT group, but only Cmin had significant differences. In multivariate regression, CRRT significantly contributed to the increase in Cmin after adjustment for ALT. Regarding safety, all the Cmin values in the CRRT group were lower than 474.8 ng/mL, which was reported to be a cut-off of hepatotoxicity related to Cmin. No dose adjustment seems necessary in such settings.
Septic shock is one of the most common critical illnesses in the ICU, with a mortality rate of 15%–30% or even higher (Singer et al., 2016; Howell and Davis, 2017; de Grooth et al., 2018). High-dose tigecycline is recommended and widely used in septic shock patients who often receive CRRT due to sepsis-related AKI, but the influence of CRRT on the steady-state plasma concentration of tigecycline remains unclear, making the drug dosing of tigecycline more challenging in these patients (De Pascale et al., 2014; Garnacho-Montero and Ferrándiz-Millón, 2014; Bellomo et al., 2017). The work of Zhao et al. (2020) proposed that there were no significant differences in the plasma concentration of tigecycline between the CRRT and non-CRRT groups; therefore, CRRT might have little influence on tigecycline metabolism. However, in our research, an increase in the steady-state plasma concentration of tigecycline was observed in septic shock patients, and significant differences were observed in the trough concentration (Table 2). The following reasons might have contributed to the elevated tigecycline plasma concentration: first, in the patients with severe renal impairment, tigecycline clearance was decreased, and the area under the concentration-time curve was increased. Dialysis could not efficiently remove tigecycline (Korth-Bradley et al., 2012). Second, the duration of CRRT did not exceed 11 h for most patients in our study, which further decreased dialysis clearance (Broeker et al., 2018).
CRRT is one of the key issues in our research. Compared with the work of Broeker et al. (2018), there are some differences in CRRT. First, Broeker et al. selected the Ultraflux AV 1,000 S polysulfone membrane, while we chose the AN69-ST membrane (Broeker et al., 2018). Compared with the polysulfone membrane, the AN69-ST membrane absorbed more tigecycline (Onichimowski et al., 2020). However, there were still tigecycline adsorption losses inside the Ultraflux AV 1000 S polysulfone membrane (Broeker et al., 2018). Second, only the CVVHDF modality was applied in our research, while both CVVHDF and continuous veno-venous haemodialysis (CVVHD) were chosen by Broeker et al. (2018). Tigecycline clearance during CVVHDF (2.71 L/h) was more efficient compared to CVVHD (1.69 L/h) (Honore et al., 2020). Third, tigecycline is highly dialytic. The duration of CRRT did not exceed 11 h for most patients in our study, while it reached 24 h in the work of Broeker et al. (2018), which largely reduced dialysis clearance in our research and may account for our results.
In our research, Cmax of tigecycline was elevated in the CRRT group, but there were no significant differences between the groups. Cmin of tigecycline was significantly increased in the CRRT group (Table 2). An increased plasma concentration might lead to toxicity. Previous studies suggested that high-dose tigecycline was safe for critically ill patients (De Pascale et al., 2014; Zha et al., 2020). Hepatotoxicity is a serious adverse reaction related to tigecycline. Cmin was reported to be a useful predictor of hepatotoxicity with a cut-off of 474.8 ng/mL (Fan et al., 2020). In our studies, Cmin of all patients in CRRT group was lower than 474.8 ng/mL, which means the increase of Cmin did not contribute to hepatotoxicity in our research. Therefore, we proposed that no dose adjustment seems necessary in such settings. We would be much more cautious to recommend therapeutic drug monitoring of tigecycline for patients undergoing CRRT considering individual variations (Zhao et al., 2020).
Despite the interesting findings in our research, some limitations exist. First, in our research, we mainly focused on the impact of CRRT with the most widely used unfractionated heparin anticoagulation on septic shock patients, and partially compensated for the lack of population pharmacokinetic data for these patients (Brandenburger et al., 2017; Frías et al., 2022). However, citric acid anticoagulants have been increasingly used in clinical practice. Since the protein binding of tigecycline is affected by divalent cations such as calcium, citric acid anticoagulants may theoretically affect the concentration of tigecycline (Dorn et al., 2018). Therefore, the potential effects of CRRT with citrate anticoagulation on the tigecycline concentration should be further investigated in future studies. Second, in the present study, the correlation between hypoalbuminemia and high-dose tigecycline was not studied due to low incidence, which should be further investigated in large clinical trials in the future. Third, our sample size was relatively small, resulting in insufficiently robust results. However, we still showed them in this article since the results were interpretable. Larger studies are needed in the future. Despite the limitations, our research partially compensates for the lack of population pharmacokinetic data in a vulnerable population and provides references for drug dosing.
In conclusion, CRRT increased the steady-state plasma concentration of tigecycline in septic shock patients who received a high dosage at 100 mg per 12 h. Only Cmin showed significant differences, and the increased Cmin in CRRT patients may not contribute to hepatotoxicity. Therefore, no dose adjustment seems needed in view of hepatotoxicity. Therapeutic drug monitoring of tigecycline is recommended in such settings.
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethical Committee of Shanghai Tenth People’s Hospital (approval number 2020KT62). The patients/participants provided their written informed consent to participate in this study.
Study conception and design: Y-GZ and D-JL; Material preparation and data collection: FH, Y-YY, T-TM, X-WW, DH, Y-SQ, and W-JL; Data analysis: W-XC and FH; Writing—original draft preparation: W-XC; Writing—review and editing: D-JL and FH; Supervision: Y-GZ and D-JL. All authors read and approved the final manuscript.
This work was supported by the National Natural Science Foundation of China (No. 82003638) and Shanghai “Rising Stars of Medical Talents” Youth Development Program-Youth Medical Talents: Clinical Pharmacist Program [SHWSRS (2021)_099].
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1118788/full#supplementary-material
Alsemari, M. A., Hakeam, H. A., Alsalman, H., and Amin, T. (2020). Cutaneous hyperpigmentation secondary to high-dose tigecycline: A case report. Ther. Adv. Infect. Dis. 7, 2049936120952605. doi:10.1177/2049936120952605
Bellomo, R., Kellum, J. A., Ronco, C., Wald, R., Martensson, J., Maiden, M., et al. (2017). Acute kidney injury in sepsis. Intensive Care Med. 43, 816–828. doi:10.1007/s00134-017-4755-7
Brandenburger, T., Dimski, T., Slowinski, T., and Kindgen-Milles, D. (2017). Renal replacement therapy and anticoagulation. Best. Pract. Res. Clin. Anaesthesiol. 31, 387–401. doi:10.1016/j.bpa.2017.08.005
Broeker, A., Wicha, S. G., Dorn, C., KrAtzer, A., Schleibinger, M., Kees, F., et al. (2018). Tigecycline in critically ill patients on continuous renal replacement therapy: A population pharmacokinetic study. Crit. Care 22, 341. doi:10.1186/s13054-018-2278-4
de Grooth, H. J., Postema, J., Loer, S. A., Parienti, J. J., Oudemans-van Straaten, H. M., and Girbes, A. R. (2018). Unexplained mortality differences between septic shock trials: A systematic analysis of population characteristics and control-group mortality rates. Intensive Care Med. 44, 311–322. doi:10.1007/s00134-018-5134-8
De Pascale, G., Montini, L., Pennisi, M., Bernini, V., Maviglia, R., Bello, G., et al. (2014). High dose tigecycline in critically ill patients with severe infections due to multidrug-resistant bacteria. Crit. care 18, R90. doi:10.1186/cc13858
Dorn, C., Kratzer, A., Liebchen, U., Schleibinger, M., Murschhauser, A., Schlossmann, J., et al. (2018). Impact of experimental variables on the protein binding of tigecycline in human plasma as determined by ultrafiltration. J. Pharm. Sci. 107, 739–744. doi:10.1016/j.xphs.2017.09.006
Dowzicky, M. J., and Chmelařová, E. (2011). Global in vitro activity of tigecycline and linezolid against Gram-positive organisms collected between 2004 and 2009. Int. J. Antimicrob. Agents 37, 562–566. doi:10.1016/j.ijantimicag.2011.02.004
Fan, G., Jin, L., Bai, H., Jiang, K., Xie, J., and Dong, Y. (2020). Safety and efficacy of tigecycline in intensive care unit patients based on therapeutic drug monitoring. Ther. Drug Monit. 42, 835–840. doi:10.1097/ftd.0000000000000784
Frías, A., Gacitua, I., Torres, R., Toro, L., Segovia, E., Alvo, M., et al. (2022). Efectividad de anticoagulación regional con citrato en terapia de reemplazo renal continua. Rev. Med. Chil. 150, 283–288. doi:10.4067/s0034-98872022000300283
Garnacho-Montero, J., and Ferrándiz-Millón, C. (2014). High dose of tigecycline for extremely resistant gram-negative pneumonia: Yes, we can. Crit. Care 18, 157. doi:10.1186/cc13942
Geng, T. T., Xu, X., and Huang, M. (2018). High-dose tigecycline for the treatment of nosocomial carbapenem-resistant Klebsiella pneumoniae bloodstream infections: A retrospective cohort study. Med. Baltim. 97, e9961. doi:10.1097/MD.0000000000009961
Gilbert, D. N., Chambers, H. F., Saag, M. S., Pavia, A. T., Black, D., Boucher, H. W., et al. (2020). The Sanford guide to antimicrobial therapy. Beijing: Peking Union Medical College Press.
Hawser, S. P., Hackel, M., Person, M. B., Higgins, P. G., Seifert, H., and Dowzicky, M. (2010). In vitro activity of tigecycline against carbapenemase-producing Acinetobacter baumannii. Int. J. Antimicrob. Agents 36, 289–290. doi:10.1016/j.ijantimicag.2010.04.009
Henderson, J. M., Pitcher, D., Steenkamp, R., Fowler, S., and Keeley, F. X. (2016). Patient and disease factors predictive of adverse perioperative outcomes after nephrectomy. Ann. R. Coll. Surg. Engl. 98, 314–319. doi:10.1308/rcsann.2016.0126
Honore, P. M., Barreto Gutierrez, L., Kugener, L., Redant, S., Attou, R., Gallerani, A., et al. (2020). High doses of tigecycline are associated with satisfactory plasmatic and pulmonary concentrations for the treatment of severe infections due to fully susceptible bacteria: Do we need even higher doses in patients under CRRT? Ann. Intensive Care 10, 139. doi:10.1186/s13613-020-00758-5
Howell, M. D., and Davis, A. M. (2017). Management of sepsis and septic shock. Jama 317, 847–848. doi:10.1001/jama.2017.0131
Hu, F., Chen, S., Xu, X., Guo, Y., Liu, Y., Zhu, D., et al. (2012). Emergence of carbapenem-resistant clinical Enterobacteriaceae isolates from a teaching hospital in Shanghai, China. J. Med. Microbiol. 61, 132–136. doi:10.1099/jmm.0.036483-0
Korth-Bradley, J. M., Troy, S. M., Matschke, K., Muralidharan, G., Fruncillo, R. J., Speth, J. L., et al. (2012). Tigecycline pharmacokinetics in subjects with various degrees of renal function. J. Clin. Pharmacol. 52, 1379–1387. doi:10.1177/0091270011416938
Li, L., Li, X., Xia, Y., Chu, Y., Zhong, H., Li, J., et al. (2020). Recommendation of antimicrobial dosing optimization during continuous renal replacement therapy. Front. Pharmacol. 11, 786. doi:10.3389/fphar.2020.00786
MacArthur, R. D., Miller, M., Albertson, T., Panacek, E., Johnson, D., Teoh, L., et al. (2004). Adequacy of early empiric antibiotic treatment and survival in severe sepsis: Experience from the MONARCS trial. Clin. Infect. Dis. 38, 284–288. doi:10.1086/379825
Marshall, J. C. (2014). Why have clinical trials in sepsis failed? Trends Mol. Med. 20, 195–203. doi:10.1016/j.molmed.2014.01.007
Onichimowski, D., Ziolkowski, H., Nosek, K., Jaroszewski, J., Rypulak, E., and Czuczwar, M. (2020). Comparison of adsorption of selected antibiotics on the filters in continuous renal replacement therapy circuits: In vitro studies. J. Artif. Organs 23, 163–170. doi:10.1007/s10047-019-01139-x
Qu, T. T., Zhang, J. l., Zhou, Z. h., Wei, Z. q., Yu, Y. s., Chen, Y. g., et al. (2009). Heteroresistance to teicoplanin in Enterococcus faecium harboring the vanA gene. J. Clin. Microbiol. 47, 4194–4196. doi:10.1128/jcm.01802-09
Roggeveen, L. F., Guo, T., Fleuren, L. M., Driessen, R., Thoral, P., van Hest, R. M., et al. (2022). Right dose, right now: Bedside, real-time, data-driven, and personalised antibiotic dosing in critically ill patients with sepsis or septic shock-a two-centre randomised clinical trial. Crit. Care 26, 265. doi:10.1186/s13054-022-04098-7
Singer, M., Deutschman, C. S., Seymour, C. W., Shankar-Hari, M., Annane, D., Bauer, M., et al. (2016). The third international consensus definitions for sepsis and septic shock (Sepsis-3). Jama 315, 801–810. doi:10.1001/jama.2016.0287
Xu, Y., Jin, L., Liu, N., Luo, X., Dong, D., Tang, J., et al. (2019). Evaluation of the ratio of the estimated area under the concentration-time curve to minimum inhibitory concentration (estimated AUIC) as a predictor of the outcome for tigecycline treatment for pneumonia due to multidrug-resistant bacteria in an intensive care unit. Int. J. Infect. Dis. 82, 79–85. doi:10.1016/j.ijid.2019.03.011
Zha, L., Pan, L., Guo, J., French, N., Villanueva, E. V., and Tefsen, B. (2020). Effectiveness and safety of high dose tigecycline for the treatment of severe infections: A systematic review and meta-analysis. Adv. Ther. 37, 1049–1064. doi:10.1007/s12325-020-01235-y
Zhao, H. H., Tang, W. J., Yang, Y. X., Cen, Z. R., and Wang, L. Q. (2020). PK/PD study of tigecycline in severely infected patients with continuous renal replacement therapy. Int. J. Clin. Pharmacol. Ther. 58, 531–538. doi:10.5414/cp203669
Keywords: high-dose tigecycline, continuous renal replacement therapy, septic shock, plasma concentration, dose adjustment
Citation: Huang F, Cao W-X, Yan Y-Y, Mao T-T, Wang X-W, Huang D, Qiu Y-S, Lu W-J, Li D-J and Zhuang Y-G (2023) Influence of continuous renal replacement therapy on the plasma concentration of tigecycline in patients with septic shock: A prospective observational study. Front. Pharmacol. 14:1118788. doi: 10.3389/fphar.2023.1118788
Received: 09 December 2022; Accepted: 22 February 2023;
Published: 09 March 2023.
Edited by:
Yan Li, Auckland University of Technology, New ZealandReviewed by:
Marios Karvouniaris, University General Hospital of Thessaloniki AHEPA, GreeceCopyright © 2023 Huang, Cao, Yan, Mao, Wang, Huang, Qiu, Lu, Li and Zhuang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dong-Jie Li, ZGpsaUB0b25namkuZWR1LmNu; Yu-Gang Zhuang, emh1YW5neWcwN0BzaW5hLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.