 Lana Kairey1
Lana Kairey1 Esther Joy Bowles
Esther Joy Bowles Jon Wardle
Jon Wardle Romy Lauche
Romy Lauche
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol. , 24 March 2023
Sec. Ethnopharmacology
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1116077
Introduction: Leaves of the Australian tea tree plant Melaleuca alternifolia were used traditionally by First Nations Australians for treating wounds, burns, and insect bites. Tea tree oil, the essential oil steam-distilled from M. alternifolia, is well-known for its medicinal properties, the evidence for most applications however is limited. This review aimed to critically appraise evidence from clinical trials examining the therapeutic efficacy and safety of tea tree oil on outcomes.
Methods: Randomized controlled trials with participants of any age, gender, or health status, comparing tea tree oil to any control were included, without limit on publication date. Electronic databases were searched on 12 August 2022 with additional records sourced from article reference sections, reviews, and industry white papers. Risk of bias was assessed by two authors independently using the Cochrane risk-of-bias 1.0 tool. Results were summarized and synthesized thematically.
Results: Forty-six articles were eligible from the following medical fields (Dentistry n = 18, Dermatology n = 9, Infectious disease n = 9, Ophthalmology n = 6, Podiatry n = 3; and Other n = 1). Results indicate that oral mouthwashes with 0.2%–0.5% tea tree oil may limit accumulation of dental plaque. Gels containing 5% tea tree oil applied directly to the periodontium may aid treatment of periodontitis as an adjunctive therapy to scaling and root planing. More evidence is needed to confirm the benefits of tea tree oil for reducing acne lesions and severity. Local anti-inflammatory effects on skin, if any, also require further elucidation. Topical tea tree oil regimens show similar efficacy to standard treatments for decolonizing the body from methicillin-resistant Staphylococcus aureus, although intra-nasal use of tea tree oil may cause irritation to mucous membranes. Tea tree oil with added iodine may provide an effective treatment for molluscum contagiosum lesions in young children. More evidence on efficacy of tea tree oil-based eyelid wipes for Demodex mite control are needed. Side effects were reported in 60% of included studies and were minor, except where tea tree oil was applied topically in concentrations ≥ 25%.
Discussion: Overall, the quality of research was poor to modest and higher quality trials with larger samples and better reporting are required to substantiate potential therapeutic applications of tea tree oil.
Systematic Review Registration: PROSPERO, identifier [CRD42021285168].
Tea tree oil is the essential oil derived from the M. alternifolia (Maiden & Betche) Cheel plant, an Australian native plant endemic to north-eastern New South Wales and Southern Queensland (Carson et al., 2006; Montreal Process Implementation Group for Australia and National Forest Inventory Steering Committee, 2019). While the whole above-ground structure is harvested and turned into biomass, only the leaves contribute to the constituents in tea tree oil, which are extracted by steam distillation. The resulting essential oil has a unique and distinct medicinal, camphoraceous odor (Rhind, 2020). The oil of M. alternifolia (Maiden & Betche) Cheel contains more than 100 components. For the purpose of assessing the quality of manufactured tea tree oil, the International Organization for Standardization has defined minimum and maximum concentrations for 15 of these components, with the primary active constituent being terpinen-4-ol, comprising 35%–48% of tea tree oil (International Organization for Standardization, 2017).
While tea tree oil may be manufactured from other species of the Melaleuca genus, M. alternifolia (Maiden & Betche) Cheel accounts for nearly 100% of tea tree oil manufactured worldwide and is therefore the most common form of tea tree oil available for purchase. Tea tree oil may be purchased over the counter or online as pure essential oil (100%), retailing for around $2-5 USD per 10 ml, or diluted to 5%–15% in a carrier oil. The majority of tea tree oil production occurs in Australia, although China, South Africa, Zimbabwe and Kenya also produce tea tree oil for commercial sale (Thomas and Deshmukh, 2019). In 2021, Australia account for 81% of the global production for steam-distilled, ISO4730:2017 compliant tea tree oil. Tea tree oil is used in healthcare/household, cosmetic, pharmaceutical, and aromatherapy products. Given the antimicrobial, anti-inflammatory and analgesic properties of tea tree oil and relative safety for topical use, tea tree oil is increasingly being used in cosmetic and pharmaceutical products (e.g., shampoos, soaps and liquid body wash, mouth washes, as well as over-the-counter treatments for cold sores, acne, burns, bites, lice, and fungal nail infections) (Thomas and Deshmukh, 2019; Rhind, 2020).
First Nations Australians have a long oral history of using the tea tree plant for medicinal purposes, of which they still practice today (Carson et al., 2006). The earliest written record of its use by First Nations Australians was the Bundjalung people of northern New South Wales who use it to treat wounds, burns, insect bites and upper respiratory infections (Braun et al., 2005; Carson et al., 2006). Arthur Penfold described the medicinal value of tea tree essential oil in 1925 (Carson et al., 2006), although the first official Australian report of its use in western medicine was in a 1930 article published in the Medical Journal of Australia (MJA) where it was described as having ‘impressive wound healing and antiseptic qualities’ (Murray, 1992; Braun et al., 2005). According to the European Medical Agency (EMA) monograph, tea tree oil has a well-established use as a traditional herbal medicinal product for 1) the treatment of small superficial wounds and insect bites, 2) the treatment of small boils (furuncles and mild acne), 3) relief of itching and irritation in cases of mild athlete’s foot, and 4) symptomatic treatment of minor inflammation of the oral mucosa, based upon its’ long-standing use for these indications (European Medical Agency, 2012). Similarly, the World Health Organization (1999) monograph on tea tree oil states the primary evidence-based therapeutic indications include symptomatic treatment of common skin disorders (e.g., acne, tinea pedis, furunculosis, and onychomycosis), as well as vaginitis (World Health Organization, 1999). However, the use of tea tree oil for oral inflammatory conditions including gingivitis, stomatitis, and tonsillitis, is described as folk medicine due to a lack of experimental or clinical data (World Health Organization, 1999). Further, due to a lack of safety data, the use of tea tree oil is contraindicated in those with hypersensitivity to the active substance or colophony, those pregnant, lactating, or trying to conceive, or aged < 12 years (International Organization for Standardization, 2017). While tea tree oil is considered safe for topical application at concentrations < 15% (Tisserand and Young, 2014), application via oral, ocular, otic or inhalation routes is not recommended (International Organization for Standardization, 2017).
Studies have reported positive benefits of tea tree oil against a range of bacteria, fungi and protozoa (Carson et al., 2006; Deyno et al., 2019). In vitro evidence has demonstrated tea tree oil to have broad spectrum antimicrobial activity, as well as anti-fungal and anti-viral actions, and to increase peripheral blood flow (Carson et al., 2006; Rhind, 2020). Tea tree oil has been proposed to alter the integrity and permeability of the cell wall of the bacteria, inhibit cell respiration, and alter the ability to of cells to maintain homeostatic conditions, inhibiting functions related to cell growth and replication (Carson et al., 2006).
Despite having an established historical and traditional use for selected therapeutic indications, supported by in vitro data, clinical human trials investigating the efficacy and safety of tea tree oil are required to permit evidence-based treatment advice. Previous systematic reviews have been limited to demodectic conditions and periodontitis (Casarin et al., 2018; Lam et al., 2020; Savla et al., 2020). Further, in 2000 Ernst and Huntley reviewed randomized clinical trials on topically applied tea tree oil for dermatological conditions (Ernst and Huntley, 2000). To date no comprehensive systematic review on the efficacy and safety of tea tree oil for human therapeutic use has been conducted. The aim of this review, therefore, was to critically appraise evidence from human trials (i.e., randomized control trials; RCTs) testing the therapeutic efficacy and/or safety of tea tree oil on any outcome(s) related to human health.
The protocol for this review was registered prospectively with the International Prospective Register of Systematic Reviews (PROSPERO) CRD42021285168. The research was funded by AgriFutures Australia (Grant No. PRJ-012616). Reporting of this systematic review is in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Page et al., 2021).
We included randomized controlled trials (RCTs) testing the effect of tea tree oil on any health-related outcome in human participants. Participants of any age, gender and health status were included. Interventions included tea tree oil from the species M. alternifolia present in any dilution and within any type of carrier (e.g., gels, creams, salves). We excluded interventions testing tea tree oil within a product containing other active ingredients known to have the same anticipated effect(s) as tea tree oil, e.g., an herbal shampoo with other essential oils, as the effect of tea tree oil was not studied in isolation. We also excluded interventions using tea tree oil in combination with other therapies unless these therapies were present in both intervention and comparison groups (i.e., co-interventions). Comparison groups eligible for inclusion were inactive controls (i.e., placebo, no treatment, wait list, usual or standard care) or an active control testing the same product without tea tree oil added or testing some variation of the tea tree oil intervention (e.g., different concentration, form, or dosage). Eligible studies measured the effect of tea tree oil on outcomes related to human health or disease including mortality, physiological (clinical) measures, quality of life and functional capacity, and safety outcomes such as toxicity or adverse reactions. Both self-reported and objectively measured outcomes were included. We included all types of RCTs, i.e., parallel, cluster, factorial, cross-over, as well as “split-body” and “split-mouth” designs where different treatments were applied to separate parts of the body or mouth, respectively, provided allocation was randomized, e.g., treatments allocated at random to right and left hands. Furthermore, we limited publication type to peer reviewed journal articles and included articles published in languages in which the review authors were fluent (i.e., English, German and Russian) which enabled an accurate translation of the text to be obtained within available resources.
Electronic databases PubMed, Scopus, and the Cochrane Central Register of Controlled Trials (CENTRAL) were searched on 12 August 2022 using pre-defined search strategies (see Supplementary Material). No limit regarding the publication date was applied. Titles and abstracts of all records from electronic database searches were exported to Endnote X9 (Clarivate Analytics). Additional records were sourced by examining references from 1) reference lists of included studies, 2) reference lists of relevant reviews, and 3) reference lists of industry white papers (Down Under Enterprises, 2016a; Down Under Enterprises, 2016b; Down Under Enterprises, 2017a; Down Under Enterprises, 2017b). All records identified were exported or entered manually into Microsoft Excel version 16 to permit recording and analysis of eligibility assessments. One author screened all identified records by title and abstract against eligibility criteria. For eligible abstracts, the full-text article was located and downloaded. Full-text articles were then assessed against eligibility criteria by two authors (LK and RL) with any discrepancies in judgements discussed and, where required, the opinion of a third author sought.
One author (LK) extracted the following data from all included articles first author, year of publication, trial registration (if applicable), study design, country, study setting, participant characteristics, eligibility criteria, details of the intervention including tea tree oil source and dose(s), details of comparison group(s) including product name(s), brand(s) and manufacturer(s), outcome measures including their methods and timepoints of assessment, main findings (efficacy) and safety, funding source(s) and any potential conflicts of interest. Where one or more data items required for extraction were missing from the article text, an attempt was made to contact the corresponding author(s) for these data. Data were verified by another author (RL).
Risk of bias within included studies was assessed using the Cochrane risk-of-bias 1.0 tool for assessing risk of bias in randomized trials (RoB 1.0) (Higgins et al., 2011). The RoB 1.0 tool comprises six domains of bias, i.e., selection bias, performance bias, detection bias, attrition bias, reporting bias, and other sources of other bias. Selection bias occurs when participants are allocated treatments using a non-random (or quasi-random) sequence, e.g., alternating allocation based on hospital admission. This may also allow personnel allocating treatments to foresee assignment and result in biased allocations. Performance bias may occur when participants know which treatment they have been allocated and systematically change their behavior as a result or when personnel are aware of participants’ allocations and systematically change their delivery of the intervention(s). Detection bias may arise if those assessing the outcome(s) measured in the study are unblinded, as this may alter how these outcome(s) are assessed. Attrition bias occurs when participants drop-out from the study creating missing data, particularly where numbers or reasons for drop-out are imbalanced between treatment arms. Reporting bias arises from the selective reporting of study outcomes, e.g., five outcomes were reportedly measured in the study, but the results of only three outcomes are reported. Two authors (LK and RL) independently assessed each of the included studies against these domains and, for each study, provided a rating (i.e., low, unclear, or high risk of bias) for each domain. Any disagreements were discussed, and judgement of a third independent author sought if required. Assessments for performance and detection bias were based on primary outcomes measured (or all outcomes if no primary outcomes were defined) and were further divided according to the nature of outcomes measured (i.e., objective, or subjective). Risk of bias assessments were tabulated and summarized thematically under each main topic (e.g., dentistry or dermatology). Where information in the full-text article text was inadequate to permit a decision on eligibility or risk of bias, or where data items required for extraction were missing, an attempt was made to contact the corresponding author(s) for this information.
Figure 1 presents the PRISMA flow diagram for study inclusion and exclusion. Of the total 974 records screened by title and/or abstract, 76 full-text articles were retrieved and assessed for eligibility. Thirty were excluded, primarily due to use of a study design other than a RCT, resulting in 46 full-text articles being included in this review (Figure 1).
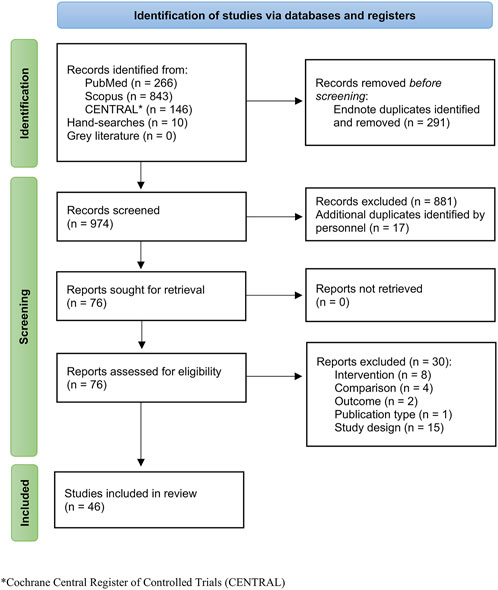
FIGURE 1. PRISMA flow diagram for study identification, screening, and inclusion.
Five fields of medicine categorized 45 of the 46 included studies, i.e., dermatology, dentistry, infectious disease, ophthalmology, and podiatry. The remaining study tested the effect of tea tree oil on anxiety and sleep disturbance in patients receiving chemotherapy (Ozkaraman et al., 2018). Eighteen studies were published in the field of dentistry addressing control of microbial plaque [n = 12; (Groppo et al., 2002; Saxer et al., 2003; Soukoulis and Hirsch, 2004; Prabhakar et al., 2009; Chandrdas et al., 2014; Rahman et al., 2014; Salvatori et al., 2017; Casarin et al., 2019; Bharadwaj et al., 2020; Kamath et al., 2020; Reddy et al., 2020; Ripari et al., 2020)], periodontitis [n = 3; (Elgendy et al., 2013; Raut and Sethi, 2016; Taalab et al., 2021)], denture stomatitis [n = 1; (Catalán et al., 2008)], oral halitosis [n = 1; (Srikumar et al., 2022)], or prevention of patient-clinician cross-contamination during dental procedures [n = 1; (Shetty et al., 2013)]. Nine studies were published in the field of dermatology addressing acne vulgaris [n = 3; (Bassett et al., 1990; Enshaieh et al., 2007; Najafi-Taher et al., 2022)], seborrheic dermatitis [n = 1; (Beheshti Roy et al., 2014)], inflammatory skin disease [n = 1; (Beikert et al., 2013)], wound healing [n = 2; (Rothenberger et al., 2016; Cho and Choi, 2017)], skin photo-aging [n = 1; (Hugo Infante et al., 2023)], or dandruff [n = 1; (Satchell et al., 2002a)]. Nine studies were published in the field of infectious disease addressing hand disinfection [n = 3; (Gnatta et al., 2013; Gnatta et al., 2021; Youn et al., 2021)], MRSA decolonization [n = 4; (Caelli et al., 2000; Dryden et al., 2004; Blackwood et al., 2013; Lee et al., 2014)] or prevention of MRSA colonization [n = 1; (Blackwood et al., 2013)], molluscum contagiosum [n = 1; (Markum and Baillie, 2012)], or oral Candida infection [n = 1; (Maghu et al., 2016)]. Six studies were published in the field of ophthalmology addressing Demodex infestation [n = 4; (Koo et al., 2012; Karakurt and Zeytun, 2018; Wong et al., 2019; Craig et al., 2022)], dry eye post cataract surgery [n = 1; (Mohammadpour et al., 2020)], or meibomian gland dysfunction [n = 1; (Zarei-Ghanavati et al., 2021)]. Three studies were published in the field of podiatry addressing onychomycosis [n = 1; (Buck et al., 1994)], or tinea pedis [n = 2; (Tong et al., 1992; Satchell et al., 2002b)]. Tables 1–6 summarize the characteristics of included studies i.e., country, setting, sample size and demographic profile, interventions, comparisons, and outcome measures, as well as results for efficacy and safety, according to the health problem studied e.g. denture stomatitis or MRSA decolonization.
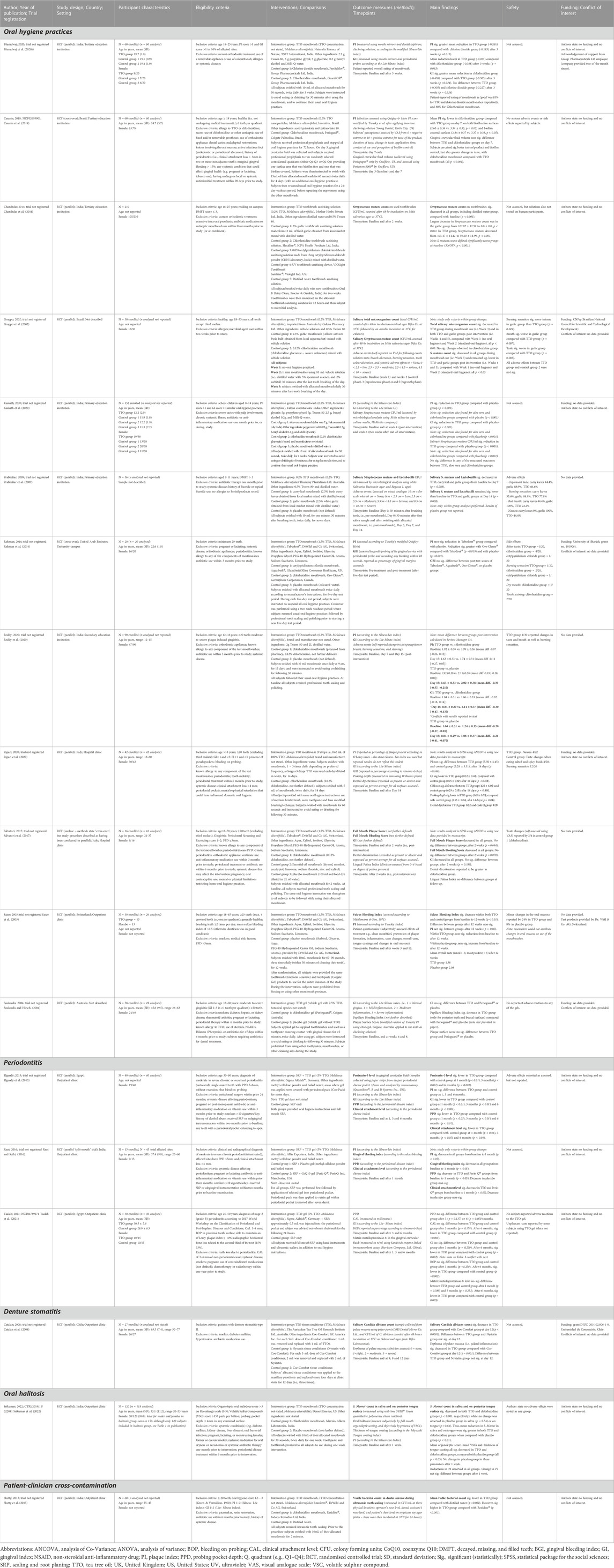
TABLE 1. Characteristics of included studies—Dentistry.
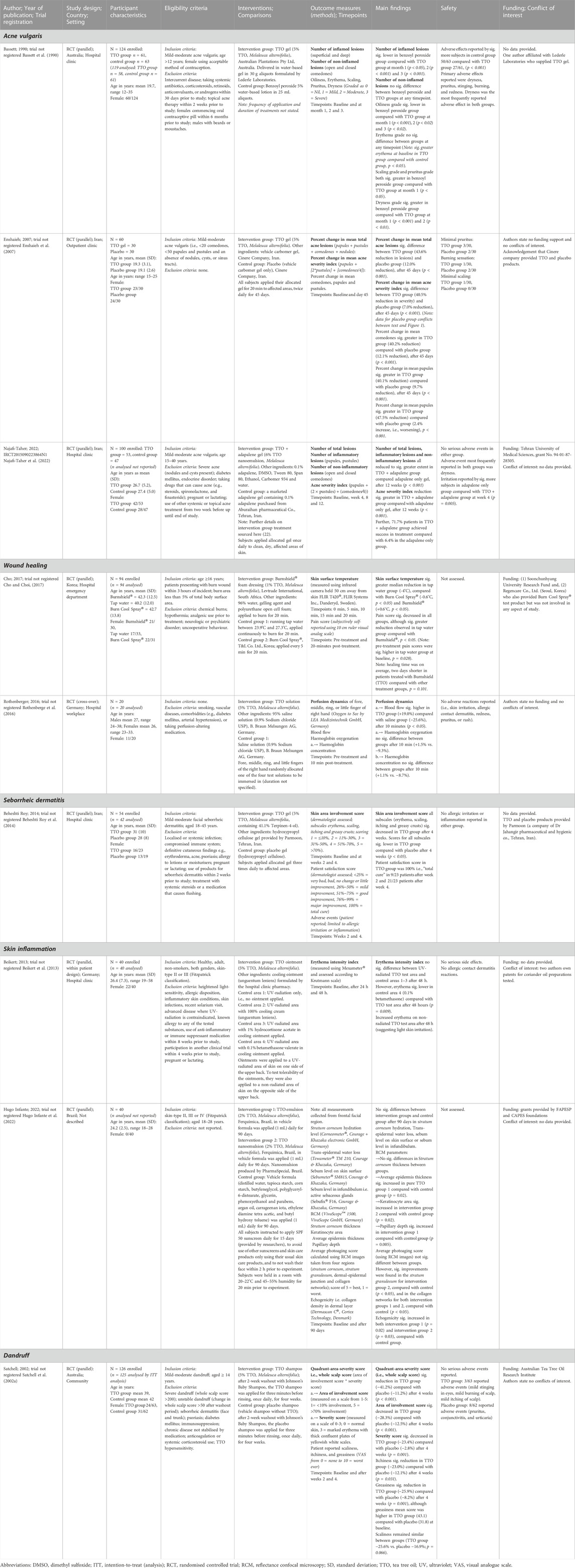
TABLE 2. Characteristics of included studies—Dermatology.
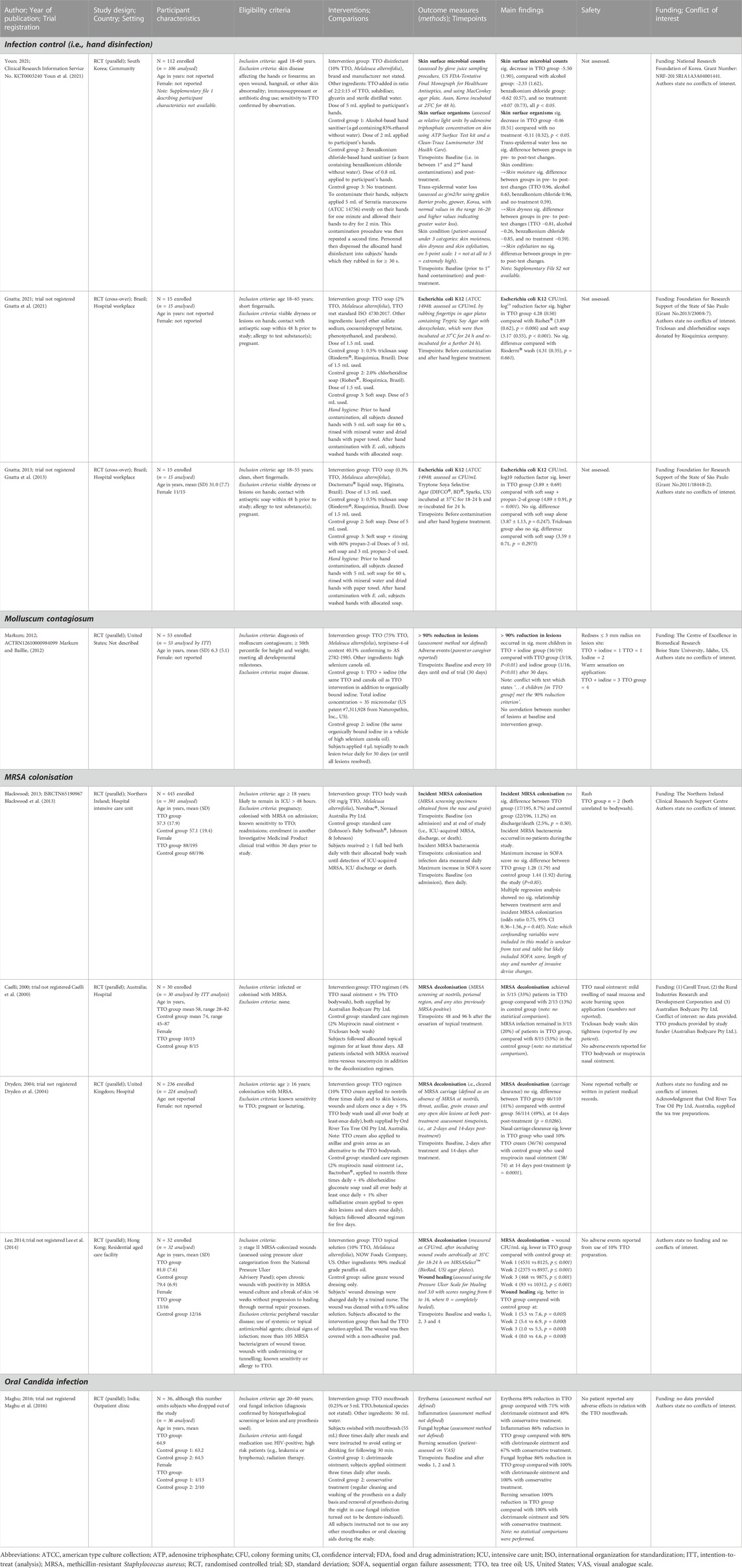
TABLE 3. Characteristics of included studies—Infectious disease.
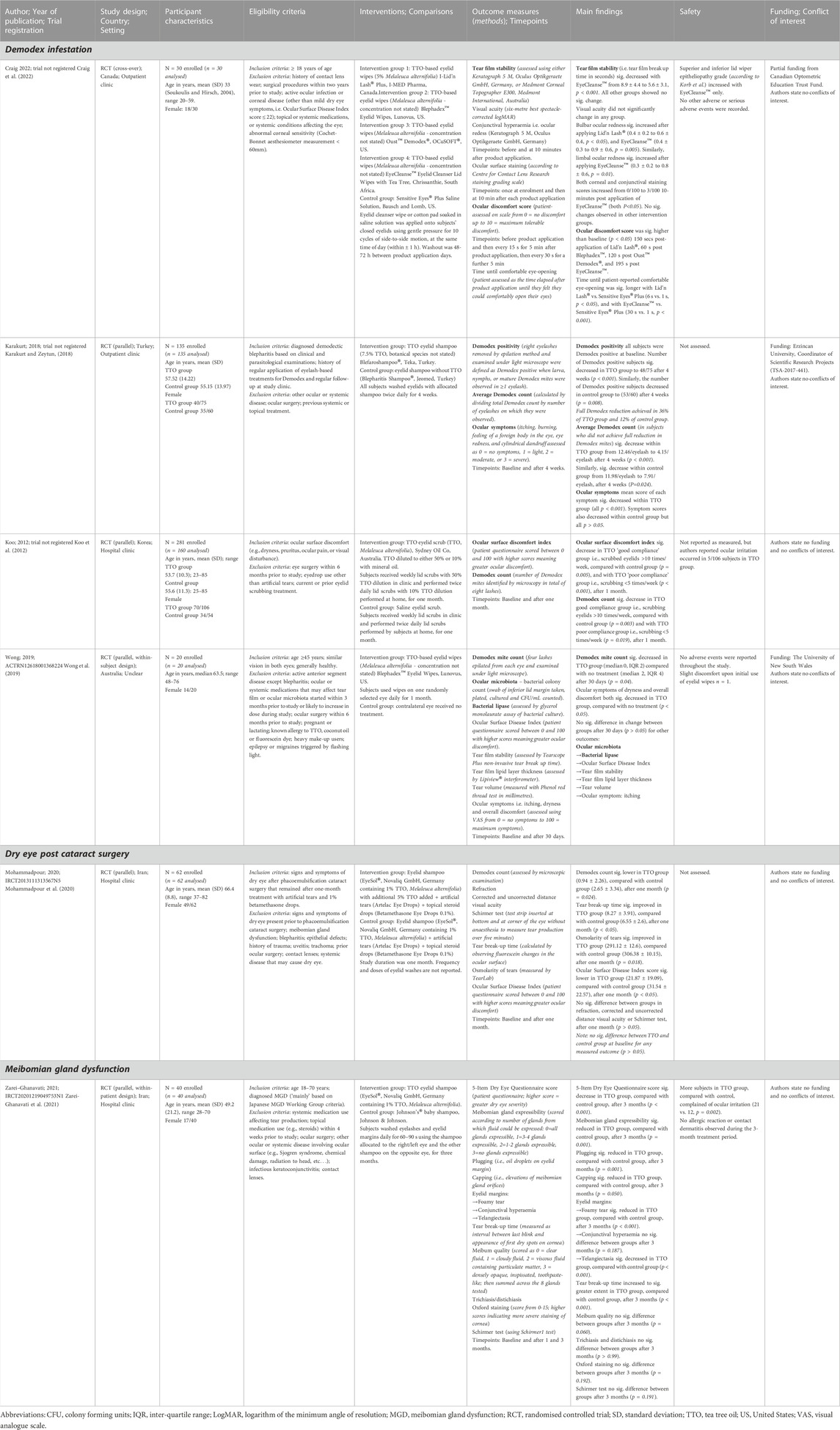
TABLE 4. Characteristics of included studies—Ophthalmology.
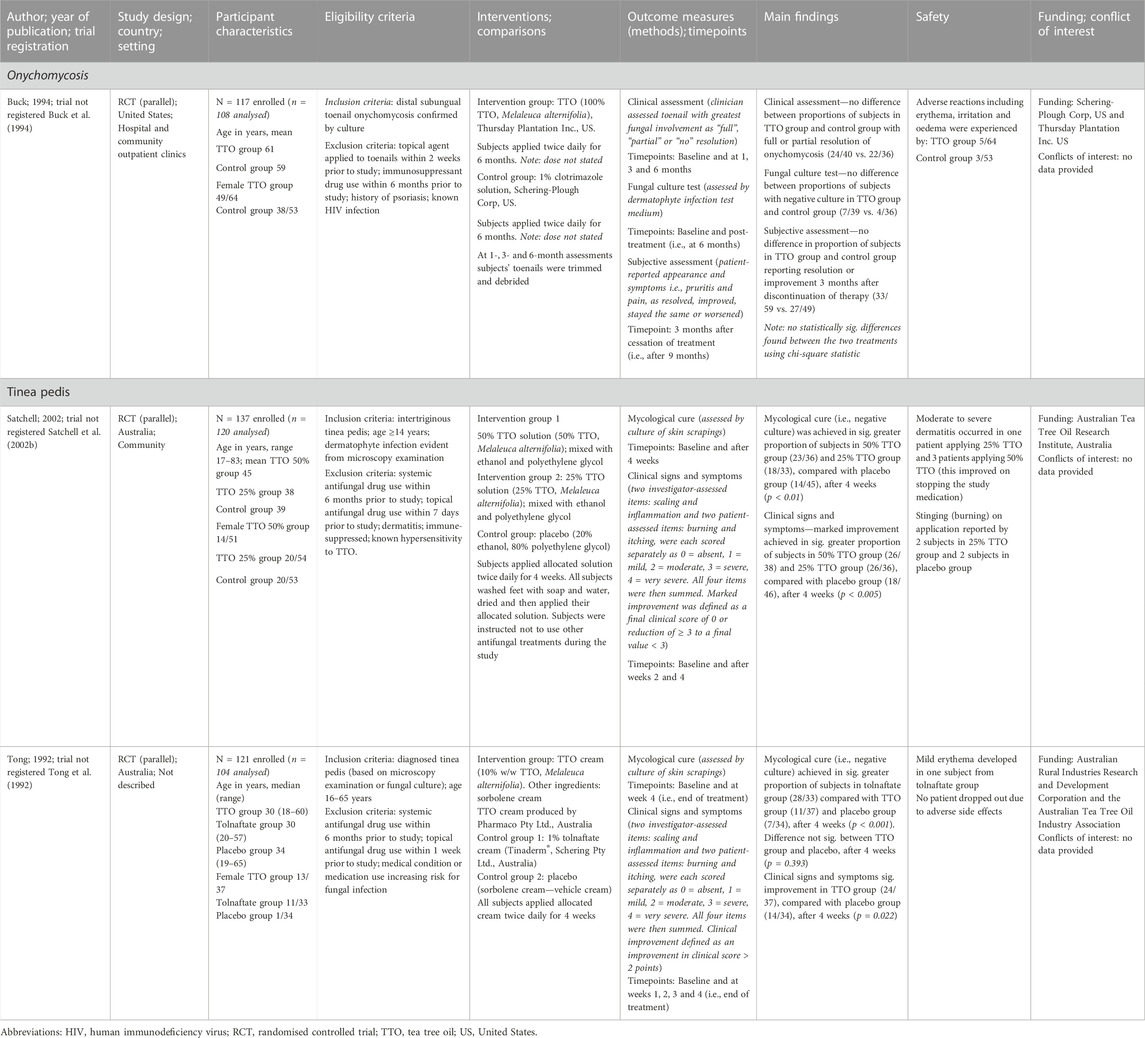
TABLE 5. Characteristics of included studies—Podiatry.
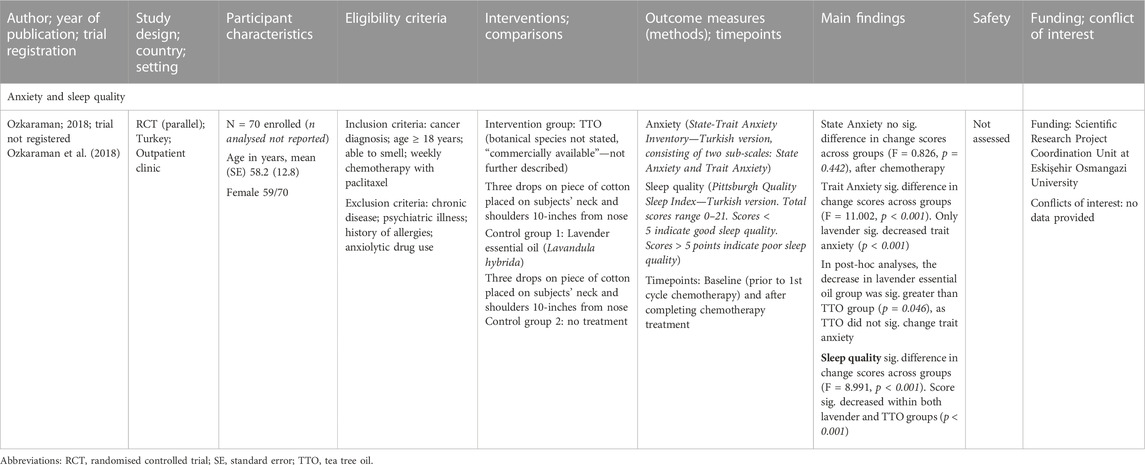
TABLE 6. Characteristics of included studies—Other.
Eighteen trials were published from 2002 to 2022 and were conducted in Australia (Soukoulis and Hirsch, 2004), Brazil (Casarin et al., 2019), Chile (Catalán et al., 2008), Egypt (Elgendy et al., 2013; Taalab et al., 2021), India (Groppo et al., 2002; Prabhakar et al., 2009; Shetty et al., 2013; Chandrdas et al., 2014; Raut and Sethi, 2016; Bharadwaj et al., 2020; Kamath et al., 2020; Reddy et al., 2020; Srikumar et al., 2022), Italy (Salvatori et al., 2017; Ripari et al., 2020), Switzerland (Saxer et al., 2003), or United Arab Emirates (Rahman et al., 2014), within a primary, secondary or tertiary education setting or within a hospital or outpatient clinic setting.
Oral hygiene practices focus on the use of tooth brushing, interdental aides, and mouthwashes to limit the accumulation of microbial plaque. Twelve trials tested the efficacy of tea tree oil for control of microbial plaque on the tooth surface (Groppo et al., 2002; Saxer et al., 2003; Soukoulis and Hirsch, 2004; Prabhakar et al., 2009; Chandrdas et al., 2014; Rahman et al., 2014; Salvatori et al., 2017; Casarin et al., 2019; Bharadwaj et al., 2020; Kamath et al., 2020; Reddy et al., 2020; Ripari et al., 2020). Outcomes assessed in these trials included plaque indices or scores (Saxer et al., 2003; Soukoulis and Hirsch, 2004; Rahman et al., 2014; Salvatori et al., 2017; Casarin et al., 2019; Bharadwaj et al., 2020; Reddy et al., 2020; Ripari et al., 2020), gingival indices (Soukoulis and Hirsch, 2004; Salvatori et al., 2017; Bharadwaj et al., 2020; Kamath et al., 2020; Reddy et al., 2020; Ripari et al., 2020), bleeding indices or scores (Saxer et al., 2003; Soukoulis and Hirsch, 2004; Rahman et al., 2014; Salvatori et al., 2017; Ripari et al., 2020), salivary Streptococcus mutans (S. mutans) count (Groppo et al., 2002; Prabhakar et al., 2009; Chandrdas et al., 2014; Kamath et al., 2020) or, in one study, salivary Lactobacillus count (Prabhakar et al., 2009). Only one study measured gingival crevicular fluid as a biomarker of gingival inflammation (Casarin et al., 2019), while two measured dental discoloration (Salvatori et al., 2017; Ripari et al., 2020), and another measured probing pocket depth (Ripari et al., 2020). Ten trials tested a tea tree oil-based mouthwash for controlling microbial plaque (Saxer et al., 2003; Rahman et al., 2014; Salvatori et al., 2017; Casarin et al., 2019; Bharadwaj et al., 2020; Kamath et al., 2020; Reddy et al., 2020; Ripari et al., 2020) and/or salivary microorganisms (Groppo et al., 2002; Prabhakar et al., 2009; Kamath et al., 2020). Of these, two tested Tebodont® (Saxer et al., 2003; Rahman et al., 2014), while others were either formulated for research containing 0.2%–0.5% tea tree oil or, in one study, the tea tree oil was diluted by participants themselves (Ripari et al., 2020).
Three trials tested a tea tree oil-based mouthwash in children aged between 8 and 15 years (Prabhakar et al., 2009; Kamath et al., 2020; Reddy et al., 2020). Kamath et al. (2020), compared the efficacy of a 0.5% tea tree oil mouthwash with three other mouthwashes (one based on aloe vera and peppermint oil, a chlorhexidine mouthwash and a placebo, i.e., distilled water) in 152 subjects aged 8–14 years (Kamath et al., 2020). After 4 weeks, dental plaque, gingival inflammation, and S. mutans count significantly decreased with twice daily use of the tea tree oil, aloe vera, and chlorhexidine-based mouthwashes compared with placebo (p < 0.001). No differences were observed in these parameters between the tea tree oil, aloe vera and chlorhexidine mouthwashes (Kamath et al., 2020). Prabhakar et al. (2009), also tested a 0.2% tea tree oil mouthwash on S. mutans and Lactobacillus counts in 36 children aged 9–11 years (Prabhakar et al., 2009). The tea tree oil mouthwash reduced both S. mutans and Lactobacillus counts after 7 days of using the mouthwash twice daily after meals. Counts of these micro-organisms remained significantly lower than baseline after 14 days (i.e., 7 days after ceasing use of tea tree oil mouthwash). These results however, were not compared to the placebo group, for which, the authors reported no data (Prabhakar et al., 2009). Lastly, Reddy et al. (2020), compared the effects of a 0.2% tea tree oil mouthwash with a chlorhexidine mouthwash or placebo (not defined) on plaque and gingival indices in children (Reddy et al., 2020). After 15 days, both dental plaque and gingival inflammation decreased with use of both tea tree oil and chlorhexidine mouthwashes (Reddy et al., 2020). Compared with chlorhexidine, the tea tree oil mouthwash was more effective in reducing gingival inflammation (mean difference −0.30 [−0.47, −0.13], based on re-analysis of data (see Tables 1–6). Compared with placebo, the tea tree oil mouthwash was more effective at reducing dental plaque.
Adverse effects were only assessed in two of these trials (Prabhakar et al., 2009; Reddy et al., 2020). Children using a 0.2% tea tree oil mouthwash reported unpleasant taste, burning sensation, bad breath and nausea, although these effects were more frequently reported with use of a garlic mouthwash (Prabhakar et al., 2009). In the other trial, 1/30 children reported taste changes and burning sensation with use of a 0.2% tea tree oil mouthwash (Reddy et al., 2020).
Seven trials tested tea tree oil-based mouthwashes in adults 18 years of age or older (Groppo et al., 2002; Saxer et al., 2003; Rahman et al., 2014; Salvatori et al., 2017; Casarin et al., 2019; Bharadwaj et al., 2020; Ripari et al., 2020). Bharadwaj et al. (2020), compared twice daily rinses with a tea tree oil-based mouthwash, to Freshclor (a chlorine dioxide-based mouthwash) or Guard-OR (a chlorhexidine-based mouthwash) for 3 weeks in 60 adults aged 18–25 years (Bharadwaj et al., 2020). All mouthwashes reduced both dental plaque accumulation and gingival inflammation after 3 weeks. However, tea tree oil was more effective in reducing dental plaque accumulation than Freshchlor, but less effective in reducing gingival inflammation compared with Guard-OR. Casarin et al. (2019), compared twice daily rinses with a mouthwash containing 0.3% tea tree oil nanoparticles or with Periogard® (a chlorhexidine gluconate-based mouthwash) in 60 adult subjects. Participants using Periogard® had less dental plaque after 4 days than those using the tea tree oil mouthwash on both biofilm free and biofilm covered surfaces (both p < 0.05). However, as this parameter was not measured at baseline, it is not possible to know whether those in the Periogard® group had less dental plaque at baseline. No significant difference was observed in gingival crevicular volume between the two groups. Groppo et al. (2002), tested the anti-microbial effect against S. mutans of a 0.2% tea tree oil mouthwash, compared with a 2.5% garlic mouthwash or 0.12% chlorhexidine mouthwash in 30 adults aged 18–35 years (Groppo et al., 2002). After 1 week of rinsing with their allocated mouthwash, salivary S. mutans count significantly decreased within all groups. Use of either the TTO or garlic mouthwashes resulted in significantly lower S. mutans in the 2 weeks after ceasing mouth rinsing (Groppo et al., 2002). Rahman et al. (2014), compared twice daily rinses with Tebodont® (a tea tree oil-based mouthwash) with a 0.05% cetylpyridinium chloride mouthwash (Aquafresh®), a 0.12% chlorhexidine mouthwash (Oro-Clense®), or a placebo (colored water) (Rahman et al., 2014). After 5 days using their allocated mouthwash, Tebodont® reduced dental plaque, although this reduction was not significantly different to placebo. Oro-Clense® was more effective at reducing plaque compared with Tebodont® (p = 0.019). Gingival bleeding was found to decrease to a similar extent with all mouthwashes (including placebo). Salvatori et al. (2017), also tested Tebodont®, comparing this to a 0.12% chlorhexidine mouthwash, an essential oil mouthwash (without tea tree oil) and a placebo mouthwash (i.e., red food dye in water) in 16 participants aged 21–37 years (Salvatori et al., 2017). Participants used their allocated mouthwash for 2 weeks—frequency of use was not reported. No significant differences were observed between groups in dental plaque, bleeding, or gingival inflammation after 2 weeks (Salvatori et al., 2017). Saxer et al. (2003), was the third study to test Tebodont®, comparing this to a placebo mouthwash without TTO provided by the same manufacturer in 30 subjects aged 18–65 years (Saxer et al., 2003). Participants rinsed three times daily with their allocated mouthwash for 12 weeks. No differences were observed in plaque or bleeding indices between groups after 12 weeks Ripari et al. (2020), compared a tea tree oil mouthwash used 1–3 times daily with a 0.12% chlorhexidine mouthwash used twice daily, for 14 days in 42 subjects aged 18–60 years (Ripari et al., 2020). Participants diluted the tea tree oil mouthwash themselves and were instructed to use a total of 9 drops per day, hence the variable mouthwash frequency for this group. The TTO mouthwash produced significantly greater reductions in both gingival inflammation and probing depth compared with the chlorhexidine mouthwash (p < 0.001). However, both mouthwashes reduced dental plaque and gingival bleeding to a similar extent (Ripari et al., 2020).
Adverse effects of tea tree oil mouthwashes in adult participants were assessed in all but one study (Bharadwaj et al., 2020), while a further study reported no participants to have experienced a “serious adverse events or side effects” (Casarin et al., 2019). Of the remaining studies, the following adverse effects were reported: burning sensation (Groppo et al., 2002; Rahman et al., 2014), bitter taste (Rahman et al., 2014), altered taste perception (Salvatori et al., 2017), nausea (Ripari et al., 2020), and minor changes to the oral mucosa (Saxer et al., 2003). Both burning sensation and bitter taste were also reported by intervention groups using a mouthwash not based on tea tree oil (Groppo et al., 2002; Rahman et al., 2014), and burning sensation was reportedly more intense with a garlic-based mouthwash than with the tea tree oil mouthwash tested (Groppo et al., 2002). While 4/22 participants using a tea tree oil mouthwash reported nausea, 2/22 participants in this group were pregnant (Ripari et al., 2020).
Rather than targeting salivary micro-organisms, Chandrdas et al. (2014), tested a tea tree oil solution for sanitizing toothbrushes in 210 subjects aged 18–25 years (Chandrdas et al., 2014). Participants brushed their teeth with a sterile toothbrush twice daily for 2 weeks, after which toothbrushes were either treated with a UV toothbrush sanitizing device or immersed for 12 h in one of the following sanitizing solutions: 0.2% tea tree oil solution, 3% fresh garlic solution, 0.2% chlorhexidine solution, 0.05% cetylpyridinium chloride solution, or distilled water. All treatments significantly reduced the count of S. mutans after 2 weeks, including the distilled water. However, any between group comparisons were compromised by the significant difference in S. mutans counts observed between groups at baseline (p < 0.001) (Chandrdas et al., 2014). Finally, Soukoulis et al., 2004, tested a 2.5% tea tree oil gel which was used as a toothpaste to brush gingival tissue in 58 adult subjects with moderate to severe gingivitis (Soukoulis and Hirsch, 2004). Twice daily brushing with a 2.5% tea tree oil gel was compared with Perioguard® and a placebo gel (same vehicle gel as tea tree oil gel, without tea tree oil), for 8 weeks (Soukoulis and Hirsch, 2004). No differences were found between the gels in gingival inflammation or staining score. During the trial no adverse reactions to the tea tree oil gel were reported (Soukoulis and Hirsch, 2004).
Three studies tested the application of a tea tree oil-based gel to the periodontium as a treatment for periodontitis (Elgendy et al., 2013; Raut and Sethi, 2016; Taalab et al., 2021). Two trials tested a 5% tea tree oil-based gel applied to the periodontal pocket in addition to scale and root planing (SRP) and compared this to SRP alone (Elgendy et al., 2013; Taalab et al., 2021). Elgendy et al. (2013), found the 5% tea tree oil-based gel + SRP was superior to SRP alone for reducing gingival inflammation, probing pocket depth and clinical attachment loss among 40 subjects aged 30–60 years (Elgendy et al., 2013). Similarly, Taalab et al. (2021), found application of a 5% tea tree oil gel, adjunctive to SRP, significantly reduced clinical attachment level, gingival inflammation, bleeding on probing and level of matrix metalloproteinase-8 in the gingival crevicular fluid (a biomarker of local periodontal disease), after 6 months in 30 subjects aged 25–50 years (Taalab et al., 2021). Raut and Sethi (2016), compared three gel treatments (i.e., 5% tea tree oil gel, a Co-Q10 gel, or a placebo gel) within each patient by using a ‘split mouth’ study design (Raut and Sethi, 2016). Here, three sites in the periodontium affected by periodontitis were identified for each patient and one of the treatment gels was randomly applied to each of these three affected sites, such that each patient received all three treatment gels. All participants also received SRP as a co-intervention. Dental plaque and gingival inflammation decreased within all groups, although probing pocket depth and clinical attachment level decreased only within the tea tree oil and Co-Q10 groups. Adverse effects only assessed in one study (Taalab et al., 2021), where no participants reported an adverse reaction, and some (number not provided) reported an unpleasant taste from the tea tree oil gel applied.
Catalán et al. (2008), compared a Coe-Comfort tissue conditioner with added tea tree oil to the same Coe-Comfort tissue conditioner alone or with the anti-fungal medicine Nystatin added, on growth inhibition of Candida albicans on the palate mucosa (Catalán et al., 2008). Both tea tree oil and Nystatin significantly reduced C. albicans count after 12 days, compared with Coe-Comfort alone. Palatal inflammation also significantly decreased with both tea tree oil and Nystatin, compared with Coe-Comfort alone. Adverse events were not assessed.
Srikumar et al. (2022), compared a tea tree oil based mouthwash to a chlorhexidine mouthwash (Maxxio®) and placebo mouthwash, for treatment for oral halitosis (Srikumar et al., 2022). Halitosis was measured subjectively by full mouth organoleptic scoring and objectively by presence of Volatile Sulfur Compounds (VSCs). Further, presence of Solobacterium moorei (S. moorei) bacteria on the tongue has been positively correlated with oral halitosis. In this study, researchers found 100% of participants diagnosed with oral halitosis (n = 120) had S. moorei bacteria in their saliva and on the posterior tongue surface, compared with 17% and 24%, respectively, of participants who did not have oral halitosis (n = 40). Participants with halitosis (n = 120) rinsed daily with 30 ml of their allocated mouthwash for 1 week. A significantly greater reduction in S. moorei count in saliva and on tongue was found for the tea tree oil and chlorhexidine mouthwashes, compared with the placebo group—which showed no change in S. moorei counts. Both organoleptic score and VSCs also significantly decreased with the tea tree oil and chlorhexidine mouthwashes relative to placebo—which showed no change in these parameters after 1 week. Researchers noted no adverse effects of the mouthwashes (Srikumar et al., 2022).
Shetty et al. (2013), compared a tea tree oil mouthwash (Emoform®—same manufacturer as Tebodont®) to a chlorhexidine mouthwash (Rexidine®) or distilled water, for reducing the bacterial count of dental aerosol (i.e., in patients’ breath) released during ultrasonic tooth scaling (Shetty et al., 2013). The purpose was to investigate prophylactic mouthwashes that may be used to limit patient-to-clinician cross infection during such procedures. Emoform® was more effective in reducing the total Colony Forming Units per milliliter (CFU/ml) in dental aerosol compared with distilled water (p < 0.001). However, Rexidine® was found to be more effective than Emoform® for this parameter (p < 0.001). Safety of the mouthwashes was not assessed.
All domains were assessed as low risk or unclear risk (Table 7), except for two studies assessed as high risk for “other bias” (Ripari et al., 2020; Srikumar et al., 2022). These two trials were assessed as high risk due to conflicting data within published article and between trial registry and published article (Srikumar et al., 2022), or participants diluting their own tea tree oil mouthwash without an assessment of compliance (Ripari et al., 2020). Selection bias due to use of a non-random or quasi-random allocation sequence was assessed as low risk in 11 of the 18 dentistry studies; the remainder assessed as unclear risk as the method for randomizing participants was not defined (Saxer et al., 2003; Soukoulis and Hirsch, 2004; Catalán et al., 2008; Prabhakar et al., 2009; Chandrdas et al., 2014; Salvatori et al., 2017; Kamath et al., 2020). Selection bias arising from inadequate concealment was assessed as low risk in nine of 18 studies; the remainder as unclear risk largely due to providing no information on methods used for allocation concealment (Groppo et al., 2002; Saxer et al., 2003; Soukoulis and Hirsch, 2004; Catalán et al., 2008; Prabhakar et al., 2009; Elgendy et al., 2013; Shetty et al., 2013; Chandrdas et al., 2014; Ripari et al., 2020). Five of ten studies measuring objective outcomes (Groppo et al., 2002; Prabhakar et al., 2009; Elgendy et al., 2013; Taalab et al., 2021; Srikumar et al., 2022), and eight of 13 studies measuring subjective outcomes (Saxer et al., 2003; Elgendy et al., 2013; Rahman et al., 2014; Salvatori et al., 2017; Reddy et al., 2020; Ripari et al., 2020; Taalab et al., 2021; Srikumar et al., 2022), were assessed as unclear risk for performance bias due to 1) lack of information on blinding, or 2) potential breaking of blinding and this potentially influencing participant and/or personnel behavior with regards to the intervention(s), e.g., it was plausible that participants could detect TTO and this may have influenced their behavior on-trial. All studies measuring objective outcomes were assessed as low risk for detection bias, as were seven of 13 studies measuring subjective outcomes (Table 7). The remainder were assessed as unclear risk, due to lack of information on outcome assessor blinding. Studies assessed as low risk for attrition bias (8/18) either clearly reported attrition within results text or flow diagram, reported that all participants completed the study, or were of short enough duration that attrition was highly unlikely, e.g., conducted all assessments before and after an ultrasonic tooth scaling procedure (Shetty et al., 2013). Only three studies had been registered on a public trial registry platform (Casarin et al., 2019; Taalab et al., 2021; Srikumar et al., 2022), and were therefore assessed as having low risk for reporting bias; all other trials were assessed as unclear risk for this domain. Finally, 2 out of 18 studies were assessed as high risk for other bias due to concerns about the study design, and the data validity. Another 9 of the 18 studies were assessed as unclear risk for other bias due to insufficient reporting of study design, or methodology.
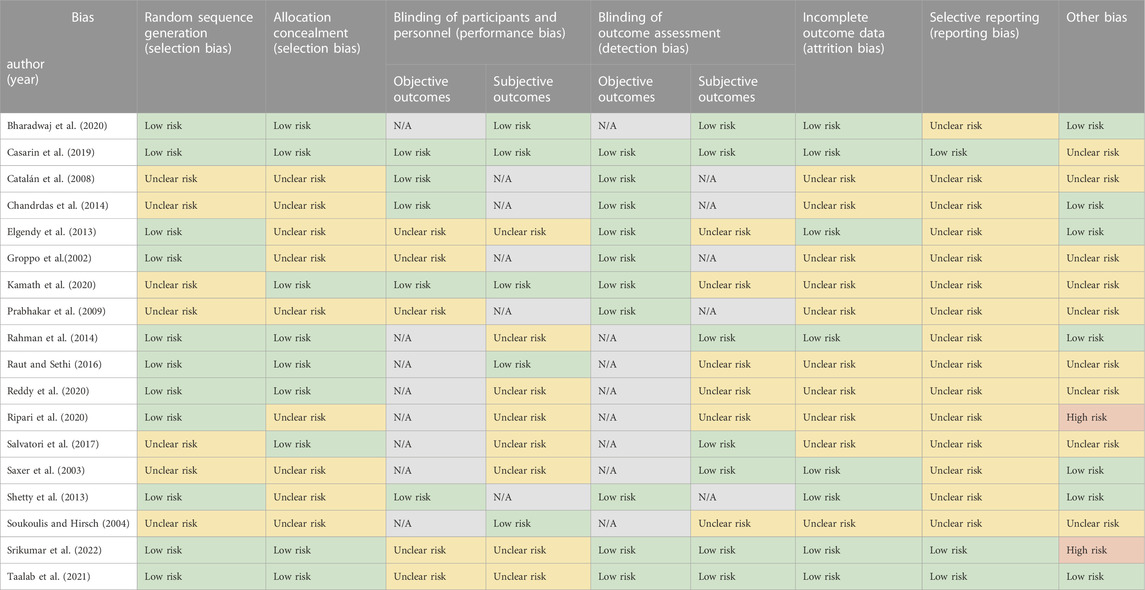
TABLE 7. Risk of bias assessment of the included studies—Dentistry.
Trials conducted in the field of dermatology were published 1990 to 2022, and conducted in Australia (Bassett et al., 1990; Satchell et al., 2002a), Germany (Beikert et al., 2013; Rothenberger et al., 2016), Iran (Enshaieh et al., 2007; Beheshti Roy et al., 2014; Najafi-Taher et al., 2022), Brazil (Hugo Infante et al., 2023), or Korea (Cho and Choi, 2017), either within a hospital, an outpatient setting or a community setting.
Three trials tested the effect of tea tree oil-based gels containing 5%–6% tea tree oil on acne lesion counts and acne severity in subjects with mild to moderate acne vulgaris (Bassett et al., 1990; Enshaieh et al., 2007; Najafi-Taher et al., 2022). Bassett et al. (1990), compared a 5% tea tree oil gel to a 5% benzoyl peroxide lotion in 124 subjects aged 12–35 years. Both treatments significantly reduced the number of inflamed and non-inflamed acne lesions. The benzoyl peroxide lotion was more effective in reducing the number of inflamed lesions after 1, 2 and 3 months, although resulted in a greater degree of facial skin scaling and pruritus compared to the tea tree oil gel. Enshaieh et al. (2007), compared twice daily application of a 5% tea tree oil gel to a placebo carbomer gel for 45 days, in 60 subjects aged 15–25 years (Enshaieh et al., 2007). Reductions in both total lesion count and acne severity were significantly greater in subjects applying the tea tree oil gel compared with placebo (p < 0.001). Finally, Najai-Taher et al. (2022), compared once daily application of a 6% tea tree oil nano-emulsion gel with 0.1% adapalene to a commercial gel containing only 0.1% adapalene, over 12 weeks, in 100 subjects aged 15–40 years. Reductions observed in acne severity and in counts of inflammatory, non-inflammatory and total lesions were all significantly greater in subjects applying the tea tree oil + adapalene gel compared with adapalene only gel (p < 0.001).
Safety was measured in all three studies. Application of a 5% tea tree oil gel resulted in minimal pruritis (3/30), burning sensation (1/30), and minimal scaling (1/30), although similar numbers of subjects applying a placebo gel reported these events (Enshaieh et al., 2007). However, Basset et al. (1990), found subjects using a 5% tea tree oil gel reported less adverse effects (e.g., dryness, stinging and burning), than those using the benzoyl peroxide lotion (27/61 vs. 50/63, p < 0.001). Najafi-Taher et al. (2022) found a higher proportion of subjects using a 6% tea tree oil + adapalene gel reported irritation after 4 weeks use, compared with an adapalene only gel (43% vs.17%, p = 0.005), although, after 12 weeks, there was no difference between groups in irritation.
Two trials tested tea tree oil for improving outcomes related to wound healing (i.e., blood flow, hemoglobin oxygenation and concentration, and skin surface temperature in the case of burns) (Rothenberger et al., 2016; Cho and Choi, 2017). Cho and Choi (2017), compared Burnshield® foam wound dressings containing tea tree oil with Burn Cool Spray® or running tap water, in 94 adult subjects (Cho and Choi, 2017). Subjects presenting to hospital emergency with a burn wound(s) within 3 hours of the incident were allocated one of the afore-mentioned treatments for 20 min. Running tap water was significantly more effective than Burnshield® and Burn Cool Spray® for reducing skin surface temperature. Safety was not assessed. Rothenberger et al. (2016), tested a saline solution with or without 5% tea tree oil on skin perfusion dynamics in 20 healthy subjects aged 23–38 years (Rothenberger et al., 2016). Blood flow was significantly higher in fingers immersed in the saline with tea tree oil solution, compared with saline alone. No difference was found in hemoglobin concentration or oxygenation. Subjects did not report any adverse reactions.
Beheshti Roy et al. (2014), compared application of a 5% tea tree oil gel to a placebo (vehicle gel) three times daily to facial areas affected with seborrheic dermatitis in 54 subjects aged 18–45 years (Beheshti Roy et al., 2014). Clinical signs of erythema, scaling, itching, and greasy crusts were all significantly lower in subjects applying the tea tree oil gel compared with placebo gel after 4 weeks. No subject reported allergic irritation or inflammation.
Beikert et al. (2013), tested the anti-inflammatory effect of a cooling ointment (100% Unguentum leniens) to which 5% tea tree oil was added, in 40 subjects aged 19–58 years (Beikert et al., 2013). One side of the subjects’ upper back was subject to UV-B irradiation to induce a local inflammatory response, while the other side was not. Using Fin Chambers®, the tea tree oil ointment was applied within one chamber and placed on the radiated skin and within another chamber placed on the non-radiated skin. In the other empty chambers, six different plant extracts, 1% hydrocortisone acetate, or 0.1% betamethasone valerate, each in the same vehicle ointment 100% Unguentum leniens, were applied, as well as the vehicle ointment alone. Local inflammation, measured by degree of skin erythema, did not significantly differ between the treatments 48 h post-irradiation. Skin areas where the tea tree oil ointment had been applied to non-irradiated skin showed increased skin erythema suggesting mild irritation. No serious side effects or contact dermatitis occurred in subjects during the trial.
Hugo Infante et al. (2023), compared the effect of an oil-in-water emulsion (vehicle formula) to this same vehicle formula with either 2% pure tea tree oil or 2% tea tree oil in nano-emulsion form added, on skin photoaging (Hugo Infante et al., 2023). No significant changes were observed in hydration or sebum levels between groups. Compared with controls, the tea tree oil nano-emulsion resulted in improvements to the stratum granulosum, including a significant increase in keratinocyte area, while the pure tea tree oil significantly increased the average epidermis thickness and papillary depth. Further, collagen density and observed collagen networks significantly increased in both tea tree oil intervention groups, compared with the control vehicle formula (Table 1). Safety was not assessed (Hugo Infante et al., 2023).
Satchell et al. (2002a), compared daily hair washing with a 5% tea tree oil shampoo or a placebo shampoo (i.e., same shampoo without tea tree oil) for treatment of dandruff in 126 subjects aged 16 and older (Satchell et al., 2002a). Reduction in both the area of scalp involved and severity of dandruff was significantly greater in subjects washing their hair with the tea tree oil shampoo compared with placebo. Adverse events reported by subjects using the tea tree oil shampoo (3/63) included mild stinging in eyes, mild burning of scalp, and mild itching of scalp. Those in the placebo group (8/62) reported pruritus, conjunctivitis, and urticaria.
Table 8 Selection bias due to use of a non-random or quasi-random allocation sequence was assessed as low risk in four of the nine trials conducted in the field of dermatology as a computer-generated sequence was used (Enshaieh et al., 2007; Cho and Choi, 2017; Hugo Infante et al., 2023; Najafi-Taher et al., 2022). The remainder provided insufficient information to assess this domain and were assessed as unclear risk. All nine dermatology trials were assessed as having an unclear risk of selection bias arising from inadequate concealment, as methods to conceal allocation sequences were not described. Primary outcomes in four of the nine trials were measured objectively (Beikert et al., 2013; Rothenberger et al., 2016; Cho and Choi, 2017; Hugo Infante et al., 2023). One of these trials was assessed as high risk, as personnel applying treatments also assessed the primary outcome and were not blinded to allocation (Cho and Choi, 2017). All four were assessed as low risk for detection bias as it was highly unlikely that the objective outcomes were affected by any lack of blinding and in one trial the assessor was blinded (Beheshti Roy et al., 2014). Five studies had subjectively assessed primary outcomes (Bassett et al., 1990; Satchell et al., 2002a; Enshaieh et al., 2007; Najafi-Taher et al., 2022). Three of these were assessed as high risk for performance bias as it is likely that blinding was broken through detection of tea tree oil odor (or lack thereof), and those receiving placebo may have altered their behavior as a result of unblinding (Satchell et al., 2002a; Enshaieh et al., 2007; Beheshti Roy et al., 2014). Intervention compliance was also not assessed in these studies. All subjective outcomes were assessed as low risk for detection bias. Attrition bias was mostly assessed as low risk, although one study was assessed as high risk given that twice the number of participants allocated to placebo dropped out and the reason provided (i.e., lost to follow-up “due to personal reasons”) is inadequate to eliminate a risk of bias (Beheshti Roy et al., 2014). Only one study had been registered on a public trial registry platform and was therefore assessed as low risk for reporting bias (Najafi-Taher et al., 2022), the remainder were assessed as unclear risk. Four trials were assessed as unclear risk for other bias as the source of tea tree oil used was not defined (Satchell et al., 2002a; Beikert et al., 2013; Rothenberger et al., 2016; Najafi-Taher et al., 2022).
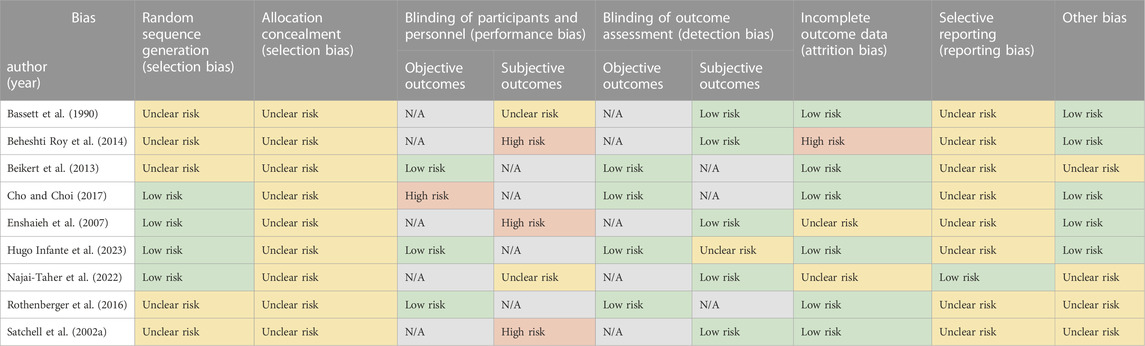
TABLE 8. Risk of bias assessment of the included studies—Dermatology.
Infectious diseases and/or infection control were addressed in nine trials published 2000 to 2021, conducted in Australia (Caelli et al., 2000), Brazil (Gnatta et al., 2013; Gnatta et al., 2021), Hong Kong (Lee et al., 2014), India (Maghu et al., 2016), Korea (Youn et al., 2021), Northern Ireland (Blackwood et al., 2013), United Kingdom (Dryden et al., 2004), or the United States (Markum and Baillie, 2012) within the hospital, outpatient, residential aged care, or community setting.
Four trials tested the effect of topically applied tea tree oil-based products for the prevention of MRSA colonization (Blackwood et al., 2013), or eradication of MRSA bacteria from the body (Caelli et al., 2000; Dryden et al., 2004; Lee et al., 2014), in hospital care settings.
Blackwood et al. (2013), compared Novobac® 5% tea tree oil body wash with standard care (i.e., Johnson’s Baby Softwash®) for preventing colonization with MRSA in 391 patients across two hospital intensive care units (Blackwood et al., 2013). Subjects received daily full bed baths with their allocated body wash until detection of ICU-acquired MRSA, discharge from ICU, or death. Compared with standard care, there was no reduction in the incidence of ICU-acquired MRSA infection (p = 0.50). A limitation to this study was that subjects using the Novobac® 5% tea tree oil had a longer admission, longer duration of ventilation, greater number of days with devices in place, and a higher percentage of these patients were nursed adjacent to a patient infected with MRSA. However, in a multiple regression analysis including the strongest independent predictors of MRSA colonization, there remained no statistically significant difference between treatment group (tea tree oil or standard care) and incident MRSA colonization (Blackwood et al., 2013). Caelli et al. (2000), compared a standard care topical regimen for MRSA decolonization to a tea tree oil topical regimen in patients infected or colonized with MRSA (Caelli et al., 2000). MRSA decolonization was achieved in 5/15 patients who received the tea tree oil regimen and 2/15 patients who received standard care, after a minimum 3 day treatment. However, patients in the tea tree oil group had, on average, a longer length of stay, and thus, longer duration of treatment. In a similar, yet larger, study, Dryden et al. (2004), also compared a standard care regimen to a tea tree oil topical regimen (10% tea tree oil cream applied to nostrils, skin lesions, wounds, and ulcers as well as a 5% tea tree oil body wash) for MRSA decolonization (Dryden et al., 2004). Fourteen days post-treatment, a similar proportion of patients achieved MRSA decolonization (tea tree oil regimen 46/110 versus standard care regimen 56/114, p = 0.0286). The 10% tea tree oil cream which was applied to the nostrils three times daily, was however, found to be less effective at clearing MRSA from nasal passages when compared with Bactroban® nasal ointment. Lastly, Lee et al. (2014), tested a topical tea tree oil solution (i.e., 10% tea tree oil with paraffin oil) for healing and decolonizing wounds infected with MRSA (Lee et al., 2014). All subjects received standard wound care, i.e., daily wound cleaning with 0.9% saline solution followed by application of a wound dressing for 4 weeks. Subjects allocated to receive the tea tree oil solution had this applied after cleaning the wound with the saline solution. CFU/ml of MRSA were found to be significantly lower in the wounds of patients who had the 10% tea tree oil solution applied to their wound at weeks 1, 2, 3 and week 4 (post-intervention). At these same timepoints, wound healing (based on wound size, exudate, and type of wound tissue) was significantly better with the tea tree oil solution compared with saline alone. Adverse events were measured in all four studies. No adverse events were reported by subjects receiving a tea tree oil topical regimen (10% tea tree oil cream and 5% tea tree oil body wash) (Dryden et al., 2004), or a topical 10% tea tree oil wound preparation (Lee et al., 2014). In the other two trials, using a tea tree oil body wash, no adverse events were reported in one trial (Caelli et al., 2000), while in the other, two subjects reported a rash which later were both found to be unrelated to the tea tree oil body wash used (Blackwood et al., 2013). However, subjects (numbers not stated) reported mild swelling of the nasal mucosa and acute burning upon application of the 4% tea tree oil nasal ointment (Caelli et al., 2000).
Three trials tested the effect of tea tree oil soaps (Gnatta et al., 2013; Gnatta et al., 2021), or a tea tree oil-based hand disinfectant (Youn et al., 2021) on microbial counts on the skin surface of hands. Youn et al. (2021), compared a tea tree oil-based hand disinfectant to a standard alcohol-based hand sanitizer, a benzalkonium chloride-based hand sanitizer and a no treatment control in 112 subjects aged 18–60 years (Youn et al., 2021). Skin surface log10 microbial count decreased in all groups, except in the no treatment control group. The greatest reduction was with use of the tea tree oil-based hand disinfectant, which achieved a significantly greater reduction compared with the alcohol-based hand sanitizer, the benzalkonium chloride-based hand sanitizer and no treatment (all p < 0.05). In two similar studies, Gnatta et al. (2013) and Gnatta et al. (2021), tested a tea tree oil hand soap for reducing the concentration of Escherichia coli K12 on the hand surface (Gnatta et al., 2013; Gnatta et al., 2021). Both studies enrolled 15 participants from a hospital workplace setting and used a cross-over design to compare a tea tree oil soap (0.2%–0.3% tea tree oil) to either Rioderm®, Soft Soap, or Soft Soap with 60% propan-2-ol hand rinse (in the 2013 study) (Gnatta et al., 2013), or to Rioderm®, Riohex®, and Soft Soap (in the 2021 study) (Gnatta et al., 2021). In the 2013, trial the tea tree oil soap (Doctornatu® liquid soap), used to wash hands after E. coli K12 contamination, reduced the CFU/mL count E. coli K12 to a similar extent as Soft Soap and was inferior to Soft Soap with 60% propan-2-ol (p = 0.001). In the 2021 trial, the tea tree oil soap (2% tea tree oil) used significantly reduced E. coli K12 compared with chlorhexidine (p = 0.006), and with Soft Soap (p < 0.001), although no difference was found between tea tree oil soap and Rioderm®. Adverse events were not assessed in these three trials (Gnatta et al., 2013; Gnatta et al., 2021; Youn et al., 2021).
Markum and Baillie (2012), compared a topical formulation containing tea tree oil organically bound to iodine in a high selenium canola oil to the same vehicle oil with tea tree oil or with organically bound iodine (i.e., tea tree oil + iodine vs. tea tree oil alone vs. iodine alone), for the treatment of molluscum contagiosum lesions in 53 children (Markum and Baillie, 2012). A significantly greater number of children resolved > 90% of their lesions with the tea tree oil + iodine formulation (16/19), compared with tea tree oil alone (3/18) or iodine alone (1/16), after 30 days (both p < 0.01). Adverse events included redness at lesion site reported by one subject each in the tea tree oil + iodine and tea tree oil alone groups and by two subjects in the iodine alone group. A warm sensation on application was also reported in groups receiving tea tree oil i.e., tea tree oil + iodine (3/19) and tea tree oil (4/18).
Maghu et al. (2016), compared a 0.25% tea tree oil mouthwash to an anti-fungal (clotrimazole) topical ointment or a standard care regime for the treatment of oral Candida infection in 36 subjects aged 20–60 years (Maghu et al., 2016). Clinician- assessed signs of erythema, inflammation, and fungal hyphae (highly diagnostic of infection with Candida), decreased in all groups, although larger reductions were seen in the tea tree oil mouthwash and clotrimazole ointment groups, compared with standard care (note: no statistical comparisons were performed). Adverse effects were not reported by any subjects using the tea tree oil mouthwash.
All domains were mostly assessed as low or unclear risk of bias (Table 9). Two trials were assessed as high risk for selection bias, due to the use of an allocation sequence that could have been predicted by those allocating interventions (Gnatta et al., 2013; Gnatta et al., 2021). High risk of detection bias was also found in one trial using subjectively assessed outcomes, as any attempt at blinding outcome assessors was likely broken due to the different treatment modalities used (Maghu et al., 2016). Only three trials had published their trial protocol on a public register (Markum and Baillie, 2012; Blackwood et al., 2013; Youn et al., 2021), and were thus assessed as having low risk of reporting bias. Three trials were assessed as having unclear risk of performance bias, as it was not reported whether personnel applying tea tree oil products were blinded and, this may have influenced doses used on subjects (Caelli et al., 2000; Dryden et al., 2004; Lee et al., 2014). Finally, six of the nine infectious disease studies were assessed as having an unclear risk of selection bias due to insufficient information on how a random sequence was generated (Caelli et al., 2000; Markum and Baillie, 2012; Gnatta et al., 2013; Lee et al., 2014; Maghu et al., 2016; Gnatta et al., 2021).

TABLE 9. Risk of bias assessment of the included studies—Infectious Disease.
Six trials were published in the field of ophthalmology from 2012 to 2021, and were conducted in Australia (Wong et al., 2019), Canada (Craig et al., 2022), Iran (Mohammadpour et al., 2020; Zarei-Ghanavati et al., 2021), Korea (Koo et al., 2012), or Turkey (Karakurt and Zeytun, 2018), within the hospital or outpatient clinic setting.
Three studies tested tea tree oil-based eyelid wipes, washes or scrubs for control of Demodex mites in subjects with diagnosed demodectic blepharitis (Karakurt and Zeytun, 2018), ocular surface discomfort (Koo et al., 2012), or in generally healthy adults (Wong et al., 2019).
Karakurt and Zeytun (2018), compared twice daily eyelid washes with Blefaroshampoo® (with 7.5% tea tree oil) with Blepharitis Shampoo (without tea tree oil) in 135 adult subjects (Karakurt and Zeytun, 2018). Koo et al. (2012), compared twice daily eyelid scrubs with 10% tea tree oil diluted in mineral oil to a saline eyelid scrub in 281 adult subjects (Koo et al., 2012). In addition to these twice daily eyelid scrubs performed at home, weekly eyelid scrubs were also performed within a clinic with 50% tea tree oil diluted in mineral oil (used in tea tree oil group) or with saline (for saline control group). Wong et al. (2019), compared BlephaDex™ eyelid wipes (containing tea tree oil) to a no treatment control in only 20 subjects aged 45 years and older (Wong et al., 2019). Subjects were randomly allocated BlephaDex™ eyelid wipes to use on their right or left eye in this within-group trial, while the contralateral eye received no treatment. In all three trials, interventions were 1 month in duration and all measured Demodex mite count at baseline and after 1 month. In two trials, use of tea tree oil significantly reduced Demodex mite count to a greater extent than saline or no treatment (Koo et al., 2012; Wong et al., 2019). Karakurt and Zeytun (2018), also found a larger reduction in Demodex mite count in those using Blefaroshampoo (with tea tree oil), compared with those using Blepharitis Shampoo (without tea tree oil), although no between group comparison was performed. Two of these trials measured patient-assessed ocular symptoms at baseline and after 1 month (Koo et al., 2012; Karakurt and Zeytun, 2018). Koo et al. (2012) found a greater reduction in patient-reported ocular discomfort after 1 month with twice daily eyelid scrubs with 10% tea tree oil diluted in mineral oil, compared with saline eyelid scrubs, but only among subjects who performed tea tree oil eyelid scrubs at home > 10 times per week (i.e., had good compliance with the intervention). Karakurt and Zeytun (2018) found patient-reported ocular symptoms including itching, burning, feeling of a foreign body in the eye, eye redness, and cylindrical dandruff all significantly decreased with use of the Blefaroshampoo (with tea tree oil), while those subjects using the Blepharitis Shampoo (without tea tree oil) had similar symptom scores after 4 weeks.
To provide data on the tolerability of different tea tree oil-based eyelid wipe products, Craig et al. (2022), compared four commercial tea tree oil-based eyelid wipes (i.e., Oust™ Demodex®, I-Lid’n Lash® Plus, Blephadex™ and Eye Cleanse™) to a saline solution (i.e., Sensitive Eyes® Plus Saline Solution), in terms of tear film break up time, as well as ocular discomfort and redness (Craig et al., 2022). Ten-minutes after application, Eye Cleanse™ lid cleansing wipes was the only product to significantly decrease tear film break up time. Eye Cleanse™ wipes also increased ocular redness (both bulbar and limbal) and corneal and conjunctival staining—a measure of damage to ocular surfaces. I-Lid’n Lash® Plus also caused a significant, yet smaller, increase in bulbar ocular redness. Patient-assessed ocular discomfort remained significantly higher than baseline for a median 195 s after applying Eye Cleanse™, 150 s after I-Lid’n Lash® Plus, 120 s after Oust™, and 60 s after Blephadex™ (Craig et al., 2022). Median time after which participants could comfortably open their eyes was one second for the saline solution, compared with 3 s for Oust™, 5 s for Blephadex™, 6 s for I-Lid’n Lash® Plus (p < 0.05), and 30 s for EyeCleanse™ (p < 0.001) (Craig et al., 2022). Only EyeCleanse™ significantly increased lid wiper epitheliopathy, although all cases were resolved within 24 h and no other adverse events were recorded.
Mohammadpour et al. (2020), compared a tea tree oil-based eyelid shampoo (Eyesol®, with 5% tea tree oil), with and without an additional 5% tea tree oil added, for treating dry eye post phacoemulsification cataract surgery (Mohammadpour et al., 2020). After 1 month, subjects Eyesol® with 5% additional TTO shampoo had significantly lower Demodex counts, improved tear osmolarity and break-up time and less ocular discomfort, compared with Eyesol® shampoo alone. Safety not assessed.
Zarei-Ghanavati et al. (2021), also tested the tea tree oil-based eyelid shampoo Eyesol® and compared this to Johnson’s baby shampoo for treating meibomian gland dysfunction (Zarei-Ghanavati et al., 2021). In this within-patient RCT, Eyesol® was randomly allocated to either the right or left eye, with Johnson’s baby shampoo used on the contralateral eye. Compared with Johnson’s baby shampoo, improvement in patient-assessed severity of dry eye was significantly greater in those using Eyesol® and clinician-assessed signs of meibomian gland expressibility, plugging, capping, foamy tear, telangiectasia and tear break-up time also significantly improved with Eyesol®, after 3 months of daily eyelid washing. All other outcomes assessed showed no significant difference between groups (Table 4).
Adverse events were measured in three of the five ophthalmology trials (Koo et al., 2012; Wong et al., 2019; Zarei-Ghanavati et al., 2021). Ocular irritation was the main side effect of tea tree oil use reported by 5/106 subjects using a tea tree oil-based mineral oil solution (Koo et al., 2012) and 21/40 subjects using tea tree oil-based Eyesol® shampoo (compared with 12/40 reporting this symptom from use of baby shampoo) (Zarei-Ghanavati et al., 2021). Further, 1/20 subjects using Blephadex™ eyelid wipes reported slight discomfort upon initial use which later resolved (Wong et al., 2019).
All domains were mostly assessed as low or unclear risk of bias (Table 10). Two trials measuring patient-reported ocular symptoms were assessed as high risk for detection bias as any attempt at blinding was likely broken due to the distinct odor of tea tree oil in the eyelid products used (Koo et al., 2012; Karakurt and Zeytun, 2018). The study by Koo et al. (2012) was also assessed as having high risk for attrition bias with 43.1% (160/281) attrition after only 1 month. Attrition was also twice as high in the tea tree oil intervention group with no reasons for drop-out reported.
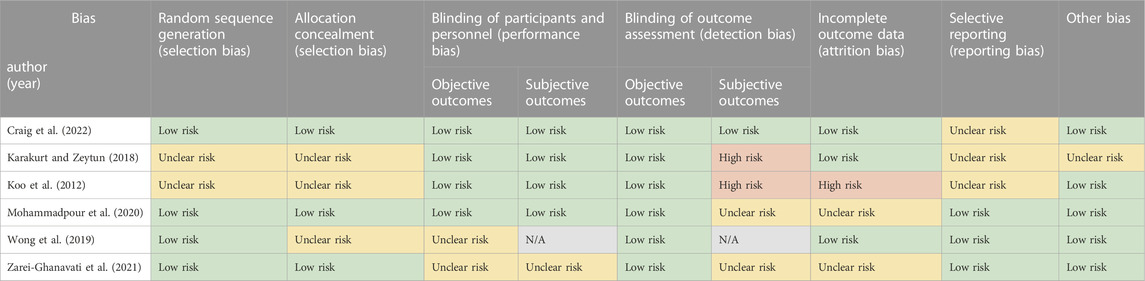
TABLE 10. Risk of bias assessment of the included studies—Ophthalmology.
Three trials were published in the field of podiatry from 1992 to 2002, and conducted in Australia (Tong et al., 1992; Satchell et al., 2002b) or the United States (Buck et al., 1994), within hospital or community outpatient clinics.
Both Australian trials tested tea tree oil for the treatment of tinea pedis (Athlete’s foot), compared with a placebo (i.e., vehicle solution) (Tong et al., 1992; Satchell et al., 2002b), or with Tinaderm® (Tong et al., 1992). Satchell et al. (2002b), compared a solution containing tea tree oil (either 50% or 25% concentration) to a placebo solution (vehicle solution), applied topically for 4 weeks in 137 subjects aged 17–83 years (Satchell et al., 2002b). After 4 weeks, a higher proportion of subjects treated with either the 50% or 25% tea tree oil solution had a negative mycological culture, compared with subjects receiving the vehicle solution (23/36 or 18/33 versus 14/45, p < 0.01) (Satchell et al., 2002b). In a separate trial, Tong et al. (1992), compared a sorbolene cream with 10% tea tree oil to a placebo vehicle cream (i.e., 100% sorbolene cream) applied topically for 4 weeks in 121 subjects aged 16–65 years. After 4 weeks, there was no significant difference in the number of patients achieving a negative mycological culture (p = 0.393) (Tong et al., 1992). When compared to Tinaderm®, a higher proportion of subjects applying Tinaderm® had a negative mycological culture, compared with tea tree oil (p < 0.001). In both trials, clinical signs, and symptoms of tinea pedis (i.e., scaling, inflammation, burning and itching) improved in a greater proportion of subjects using tea tree oil, compared with placebo (Tong et al., 1992; Satchell et al., 2002b). Adverse events were assessed in both trials (Tong et al., 1992; Satchell et al., 2002b). Three of the 69 subjects treated with a 50% tea tree oil solution and one treated with a 25% tea tree oil solution developed moderate to severe dermatitis which improved upon ceasing treatment (Satchell et al., 2002b). One subject applying Tinaderm® developed mild erythema (Tong et al., 1992).
Buck et al. (1994), tested twice daily topical application of 100% tea tree oil, compared with a 1% clotrimazole antifungal solution, for 6 months for the treatment of onychomycosis—a fungal toenail infection (Buck et al., 1994). Tea tree oil was found to be as effective as the clotrimazole solution based on negative fungal culture at 6 months (i.e., post-intervention). The toenail assessed as having the greatest fungal involvement at baseline showed “full” or “partial” resolution in a similar proportion of patients in tea tree oil and clotrimazole groups. Further, after 9 months (i.e., 3 months post-intervention), a similar proportion of patients reported that their toenail appearance and symptoms had either improved or completely resolved. Adverse events (i.e., erythema, irritation, and edema) were experienced by 5/64 using 100% tea tree oil compared with 3/53 using the clotrimazole solution.
All domains were mostly assessed as low or unclear risk of bias (Table 11). Unclear risk was assigned for absence of information on methods for randomizing participants to intervention groups, and the lack of publicly available trial protocols either in a published manuscript or on a trial registry platform. Two trials were assessed as high risk for detection bias for patient-reported symptoms, given the likely breaking of blinding due to the distinct odor of tea tree oil (Tong et al., 1992; Buck et al., 1994).
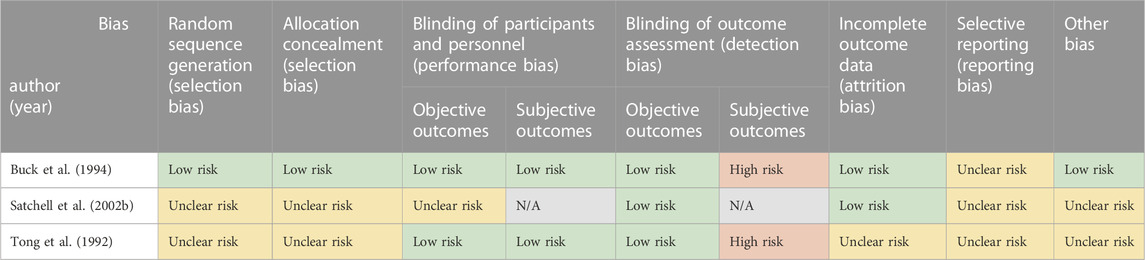
TABLE 11. Risk of bias assessment of the included studies—Podiatry.
Ozkaraman et al. (2018), tested the effect of Lavender essential oil, in comparison to tea tree oil or no treatment, on anxiety and sleep quality in 70 patients undergoing weekly chemotherapy (Ozkaraman et al., 2018). Three drops of a commercially available tea tree oil (source not defined) were placed on a piece of cotton and positioned on the patient’s neck during their chemotherapy session. Patients were also instructed to smell their allocated oil at home every evening at 9 p.m. for 5 min for 1 month. Lavender essential oil significantly decreased trait anxiety (e.g., being a steady person, not worrying too much over something that doesn’t matter), while no change was observed with tea tree oil. No difference was found between groups in the change in state anxiety scores (e.g., being tense or worried). Tea tree oil was found to be as effective as lavender essential oil in improving sleep quality, although baseline scores for sleep quality were higher in the tea tree oil group (Ozkaraman et al., 2018). Safety was not assessed.
Table 12 Given the distinct smell of lavender and tea tree and the use of a no treatment control, it would not have been possible to blind participants to treatment allocation (Ozkaraman et al., 2018). Thus, performance and detection bias were assessed as high risk for the two primary patient-reported outcomes assessed: State-Trait Anxiety Inventory and Pittsburgh Sleep Quality Index. Attrition bias and reporting bias were both assessed as unclear risk as there was no information on attrition and the trial protocol was not made publicly available. Finally, other bias was assessed as unclear risk given the tea tree oil used was not described.

TABLE 12. Risk of bias assessment of the included studies—Other.
This review aimed to critically appraise evidence from randomized control trials examining the therapeutic efficacy and safety of tea tree oil on outcomes related to human health. The search yielded 46 eligible studies spanning the fields of dentistry, dermatology, infectious disease, ophthalmology, podiatry, as well as anxiety and sleep quality—a substantial expansion in research since the 2000 review by Ernst & Huntley which identified only four trials (Ernst and Huntley, 2000).
Mouthwashes containing 0.2%–0.5% tea tree oil may be more effective in reducing dental plaque accumulation than a placebo mouthwash (Kamath et al., 2020; Reddy et al., 2020), or a 0.1% chlorine dioxide mouthwash (Bharadwaj et al., 2020), but not in comparison to a 0.12% chlorhexidine mouthwash (Casarin et al., 2019; Kamath et al., 2020). Evidence on the effects of tea tree oil mouthwashes on gingival inflammation and gingival bleeding is conflicting, and further studies are needed to confirm observed antimicrobial effects of tea tree oil mouthwashes on salivary S. mutans (Prabhakar et al., 2009; Kamath et al., 2020). Side effects of tea tree oil mouthwashes were minor with burning sensation most frequently reported, although this was also reported with other mouthwashes tested. Adjunctive therapy with a 5% tea tree oil gel delivered locally to the periodontium may improve SRP treatment outcomes in patients with periodontitis (Elgendy et al., 2013; Raut and Sethi, 2016; Taalab et al., 2021). We found insufficient evidence for the use of tea tree oil in treating C. albicans induced denture stomatitis, oral C. albicans infection, or in prevention of patient-clinician cross-contamination (Catalán et al., 2008; Shetty et al., 2013; Maghu et al., 2016).
For the treatment of acne, a 5% tea tree oil-based topical gel may be effective in reducing the number of lesions and severity of acne, in comparison to a placebo (Enshaieh et al., 2007). However, tea tree oil was less effective for reducing the number of inflamed lesions compared with topical benzoyl peroxide (i.e., standard care) (Bassett et al., 1990). A combination of a tea tree oil nano-emulsion with adapalene in a topical gel shows potential as a novel treatment option for reducing lesion counts and severity of acne (Najafi-Taher et al., 2022). Clinical signs and symptoms of seborrheic dermatitis might be improved with a 5% tea tree oil topical gel, although findings are based on one small poor-quality trial (Beheshti Roy et al., 2014). Available evidence does not support the use of a tea tree oil dressing for treating burn wounds, with running tap water being more effective in cooling burns (Cho and Choi, 2017). Topical application of a 5% tea tree oil ointment was also found to be ineffective for reducing skin erythema in a UVB radiation model (Beikert et al., 2013). Topical application of tea tree oil in the concentrations used in these trials can result in mild reactions, such as burning sensation or itching upon application.
While daily bed baths with a 5% tea tree oil body wash did not prevent patient colonization with MRSA (Blackwood et al., 2013), a topical tea tree oil-based regime showed similar efficacy to a routine topical regimen for MRSA decolonization in patients already colonized with MRSA bacteria (Caelli et al., 2000; Dryden et al., 2004). One smaller trial found 10% tea tree oil in paraffin oil applied to wounds colonized with MRSA improved wound healing and reduced MRSA bacterial counts (Lee et al., 2014). Adverse effects in MRSA trials were limited to mild swelling of the nasal mucosa and acute burning upon application of a 4% tea tree oil nasal ointment. Treating molluscum contagiosum lesions in young children may also be possible with topical application of 75% tea tree oil with iodine, with adverse events limited to mild redness at lesion site and warm sensation on application (Markum and Baillie, 2012).
Tea tree oil-based eyelid wipes or scrubs aid reduction of ocular Demodex mite counts when compared with saline or no treatment (Koo et al., 2012; Wong et al., 2019). This finding is consistent with the review by Lam et al. (2020), who reported tea tree oil showed efficacy in controlling Demodex mite populations. Use of wipes may be safer, as ocular irritation can occur with tea tree oil eyelid scrubs (Koo et al., 2012). There is substantial difference however in the tolerability of commercially available eyelid cleansers (Craig et al., 2022). Further, more evidence is required to confirm efficacy and safety of tea tree oil-based eyelid shampoos for treating dry eye and meibomian gland dysfunction (Mohammadpour et al., 2020; Zarei-Ghanavati et al., 2021).
Dermatophyte fungi causing tinea pedis may effectively be treated with tea tree oil applied topically in either 25% or 50% concentration, although moderate to severe dermatitis may present as a side effect and efficacy of this treatment has not been compared with standard care (Satchell et al., 2002b).
Finally, there was insufficient evidence to advise use of tea tree oil for improving anxiety or quality of sleep, with lavender essential oil being potentially more efficacious for reducing anxiety, at least during chemotherapy (Ozkaraman et al., 2018).
Several systematic reviews on tea tree oil have been conducted previously. About 20 years ago, Ernst and Huntley identified only four randomized controlled trials addressing acne, tinea pedis or onychomycosis (Ernst and Huntley, 2000). Since then, a further three systematic reviews have been published, although all focus on specific therapeutic indications only (Casarin et al., 2018; Lam et al., 2020; Savla et al., 2020). Savla et al. (2020), included six RCTs examining efficacy of tea tree oil for Demodex blepharitis with a total of 562 participants (Savla et al., 2020). While they found lower number of mites compared to the control interventions, they concluded that there was uncertainty whether 5%–50% tea tree oil was effective for treating Demodex blepharitis (Savla et al., 2020). With the lack of long-term studies, they also concluded that lower concentrations may be preferred to reduce potential side effects such as skin irritation. Lam et al. (2020), compared current pharmaceutical treatments for human demodicosis, and examined 95 studies, including trials on tea tree oil (Lam et al., 2020). They concluded that tea tree oil was the most effective, followed by metronidazole, ivermectin and permethrin, and the authors recommended tea tree oil as a first-line therapy. In our opinion, this recommendation is not supported by existing evidence. While the results for treating Demodex are promising, the lack of high-quality evidence, and the concerns around safety, especially with higher concentrations of tea tree oil, need to be considered, and further research is needed before such recommendations can be made. Casarin et al. (2018), included 25 studies addressing periodontal disease, however only six of those were clinical trials, whereas the present systematic review found 15 RCTs addressing periodontal disease prevention and treatment (Casarin et al., 2018). Casarin et al., 2018, suggested that tea tree oil has potential anti-inflammatory and antimicrobial properties, although we found that existing evidence for anti-inflammatory outcomes (i.e., gingival inflammation) is conflicting, and further trials are needed to confirm antimicrobial effects.
This review has several limitations, the most important concerning the source and quality of tea tree oils. Only 24 of the 43 included studies stated the brand of tea tree oil or tea tree oil product that was used for the intervention. The remainder only stated that M. alternifolia was used or, in four trials (Soukoulis and Hirsch, 2004; Maghu et al., 2016; Karakurt and Zeytun, 2018; Ozkaraman et al., 2018), it was only stated that “tea tree oil” was used. Few stated the chemical composition of the tea tree oil used or the storage conditions. While tea tree oil is stable for more than 12 months under optimal conditions, exposure to oxygen, heat and light can cause rapid degradation of tea tree oil (AgriFutures Australia, 2021). Oxidized tea tree oil leads to a decrease in α-terpinene and γ-terpinene, and an increase in p-cymene and peroxide, which are main drivers of sensitization, and skin irritation (Hammer et al., 2006). Further to this, a recent study identified that nearly 50% of commercial tea tree oil samples showed signs of adulteration (Bejar, 2017). Adulterated tea tree oil is prepared by blending fractions of cheaper oils as well as adding synthetic analogues of terpinen-4-ol, and without detailed information about the product, the brand, and the composition of the tea tree oil product investigated, results of the trials included in this review cannot be attributed to M. alternifolia essential oil with certainty. Adulterated tea tree oil may also cause adverse reactions that would otherwise not occur with pure tea tree oil essential oil, leading to potentially erroneous safety profiles.
A general limitation to clinical research investigating tea tree oil is the difficulty in blinding of participants and personnel due to the strong unique aroma of tea tree oil. It is well understood that tea tree oil has a strong odor and taste, which can easily be distinguished by trial participants. While many trials claimed that participants were blinded, it is unclear whether the blinding was successful, and no data were collected to ascertain blinding in most studies. Researchers have previously been able to successfully blind participants by use of deception, i.e., falsely advising patients that the aroma of their treatment had been changed to prevent detection of tea tree oil (Carson et al., 2008). In addition, most trials did not assess compliance/adherence with the trial interventions, or, adverse events, including in very recent trials, highlighting the importance of comprehensive evaluation of efficacy and safety outcomes. Concerningly, some trials did not state the doses or frequency at which the tea tree oil interventions were used.
Another limitation to consolidating evidence from trials investigating tea tree oil is the heterogeneity of tea tree oil-based product formulations. Variations in formulations can result in huge differences in product efficacy, for example a sorbolene base for tea tree oil used for acne was shown to inhibit its efficacy (personal communication), and acne products may require an alternative carrier. In the last decade, many novel formulations have been developed for drug delivery, and it is essential to understand the limitations and benefits of delivery systems to design appropriate tea tree oil products with improved effectiveness and safety, adequate stability, and shelf-life. As such, it is recommended that all new tea tree oil formulations are rigorously tested in-vitro, in-vivo, and in clinical trials prior to release onto the market. Finally, researchers must adhere to standard research design and reporting guidelines, as well as register their trials prospectively in national/international trial databases for transparency.
The question of the safety of tea tree oil has been a controversial topic for decades. Issues have been raised around its ability to cause dermal irritation and its potential as an allergic sensitizer. Several studies have been conducted, and while tea tree oil was ranked twenty-third on the list of most frequent allergens reported in Australia (Toholka et al., 2015), studies in North America and Europe found relatively low allergenicity rates to tea tree oil (de Groot and Schmidt, 2016). It is however accepted, that most allergic reactions occur with aged/oxidized tea tree oil due to the degradation of its components. In addition, case reports have linked tea tree oil with gynecomastia in young boys (Henley et al., 2007), although recent studies refuted these findings and found that it was implausible for tea tree oil to cause endocrine disruptions (Hawkins et al., 2020; Hawkins et al., 2021). Lastly, a recent report by Lee et al. (2020), found that 17% of adverse events due to exposure to essential oils were caused by tea tree oil (Lee et al., 2020). According to US data from the National Electronic Injury Surveillance System (NEISS) from 2010 to 2020 (https://www.cpsc.gov/Research--Statistics/NEISS-Injury-Data), most injuries associated with tea tree oil were due to ingestion in toddlers and children, with an overall low hospitalization rate, and no deaths. The large number of incidents (nearly 350 in 2017), however, warrants better consumer protection, such as mandatory child-proof safety caps on tea tree oil bottles.
This systematic review provides the first comprehensive appraisal of human trials testing the therapeutic efficacy and safety of tea tree oil. Therapeutic indications for which tea tree oil has been tested span multiple fields of medicine including dentistry, dermatology, infectious disease, ophthalmology, and podiatry.
In contrast to the well-established traditional uses of tea tree plant, no trials were identified for the treatment of minor wounds, furuncles, or insect bites of tea tree oil. Such analgesic and antipruritic properties of tea tree oil are not well documented, and further research into the modes of action are warranted. One recent trial was located on the treatment of vaginitis, suggesting tea tree oil pessaries were an effective treatment for vaginitis, although this trial was excluded on the basis of study design (Durić et al., 2021). While tea tree leaves have traditionally been used for treating coughs and colds, no clinical trials testing tea tree oil for these indications were found, and the safety of tea tree oil for inhalation is poorly understood.
Reliability of the evidence from many of these trials suffered from inadequate reporting, particularly reporting of the source and quality of tea tree oils used on patients. Future investment in rigorous human clinical trials is warranted to clarify potential benefits of tea tree oil for treatment of acne, molluscum contagiosum lesions, microbial causes of tooth decay, periodontal disease, and oral fungal conditions, infections caused by antibiotic-resistant bacteria, and ocular conditions caused by Demodex mite infestation. In future trials, emphasis should focus on comparing tea tree oil to current standard care as well as an appropriate placebo. Novel formulations should also be considered to enhance localized delivery of active components of tea tree oil. Further, it is critical to assess safety of tea tree oil treatments to better understand the risks to patients and consumers of these products.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
RL wrote search strategies for electronic databases and executed the searches. LK and RL reviewed titles and abstracts of retrieved records for eligibility. LK and RL assessed risk of bias. LK drafted the methods, results, figures, and tables. TA and LK drafted the introduction. LK and RL drafted the discussion. LK, TA, BB, JW, EB, and RL reviewed, edited, and approved the final manuscript.
The work was funded the by AgriFutures (Grant No. PRJ-012616; 15 June 2020).
The authors wish to thank the contribution of Tony Larkman of ATTIA Ltd. for providing access to literature from the to the ATTIA tea tree oil database. For supporting the project with their expertise of tea tree oil research and industry, we further wish to extend our gratitude to Gae Plunkett and Ellen Buckle of AgriFutures Australia, Tony Larkman of ATTIA Ltd., Philip Prather of Down Under Enterprises, and to John Price of CP Holdings Pty. Ltd.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1116077/full#supplementary-material
Bassett, I. B., Pannowitz, D. L., and Barnetson, R. S. (1990). A comparative study of tea-tree oil versus benzoylperoxide in the treatment of acne. Med. J. Aust. 153 (8), 455–458. doi:10.5694/j.1326-5377.1990.tb126150.x
Beheshti Roy, A., Tavakoli-Far, B., Fallah Huseini, H., Tousi, P., Shafigh, N., and Rahimzadeh, M. (2014). Efficacy of melaleuca alternifolia essential oil in the treatment of facial seborrheic dermatitis: A double-blind, randomized, placebo-controlled clinical trial. J. Med. Plants 13 (51), 26–32.
Beikert, F. C., Schonfeld, B. S., Frank, U., and Augustin, M. (2013). Antiinflammatory potential of seven plant extracts in the ultraviolet erythema test. A randomized, placebo-controlled study. Hautarzt 64 (1), 40–46. doi:10.1007/s00105-012-2505-x
Bejar, E. (2017). Adulteration of tea tree oil (Melaleuca alternifolia and M. linariifolia). Botanical Adulterants Prevention Bulletin, 1–8.
Bharadwaj, A. N., Byatappa, V., Raju, R., Umakanth, R., and Alayadan, P. (2020). Antiplaque and antigingivitis effectiveness of tea tree oil and chlorine dioxide mouthwashes among young adults: A randomized controlled trial. World J. Dent. 11 (6), 451–456. doi:10.5005/jp-journals-10015-1765
Blackwood, B., Thompson, G., McMullan, R., Stevenson, M., Riley, T. V., Alderdice, F. A., et al. (2013). Tea tree oil (5%) body wash versus standard care (Johnson's Baby Softwash) to prevent colonization with methicillin-resistant Staphylococcus aureus in critically ill adults: a randomized controlled trial. J. Antimicrob. Chemother. 68 (5), 1193–1199. doi:10.1093/jac/dks501
Braun, L., Cohen, M., and Monographs, A-Z. (2005). in Herbs & natural supplements: An evidence-based guide (Sydney: Elsevier Mosby).
Buck, D. S., Nidorf, D. M., and Addino, J. G. (1994). Comparison of two topical preparations for the treatment of onychomycosis: Melaleuca alternifolia (tea tree) oil and clotrimazole. J. Fam. Pract. 38 (6), 601–605.
Caelli, M., Porteous, J., Carson, C. F., Heller, R., and Riley, T. V. (2000). Tea tree oil as an alternative topical decolonization agent for methicillin-resistant Staphylococcus aureus. J. Hosp. Infect. 46 (3), 236–237. doi:10.1053/jhin.2000.0830
Carson, C. F., Hammer, K. A., and Riley, T. V. (2006). Melaleuca alternifolia (tea tree) oil: A review of antimicrobial and other medicinal properties. Clin. Microbiol. Rev. 19 (1), 50–62. doi:10.1128/CMR.19.1.50-62.2006
Carson, C. F., Smith, D. W., Lampacher, G. J., and Riley, T. V. (2008). Use of deception to achieve double-blinding in a clinical trial of Melaleuca alternifolia (tea tree) oil for the treatment of recurrent herpes labialis. Contemp. Clin. Trials 29 (1), 9–12. doi:10.1016/j.cct.2007.04.006
Casarin, M., Pazinatto, J., Oliveira, L. M., Souza, M. E., Santos, R. C. V., and Zanatta, F. B. (2019). Anti-biofilm and anti-inflammatory effect of a herbal nanoparticle mouthwash: a randomized crossover trial. Braz Oral Res. 33, e062. doi:10.1590/1807-3107bor-2019.vol33.0062
Casarin, M., Pazinatto, J., Santos, R. C. V., and Zanatta, F. B. (2018). Melaleuca alternifolia and its application against dental plaque and periodontal diseases: A systematic review. Phytother. Res. 32 (2), 230–242. doi:10.1002/ptr.5974
Catalán, A., Pacheco, J. G., Martínez, A., and Mondaca, M. A. (2008). In vitro and in vivo activity of melaleuca alternifolia mixed with tissue conditioner on Candida albicans. Oral Surg. Oral Med. Oral Pathology, Oral Radiology Endodontology 105 (3), 327–332. doi:10.1016/j.tripleo.2007.08.025
Chandrdas, D., Jayakumar, H. L., Chandra, M., Katodia, L., and Sreedevi, A. (2014). Evaluation of antimicrobial efficacy of garlic, tea tree oil, cetylpyridinium chloride, chlorhexidine, and ultraviolet sanitizing device in the decontamination of toothbrush. Indian J. Dent. 5 (4), 183–189. doi:10.4103/0975-962x.144718
Cho, Y. S., and Choi, Y. H. (2017). Comparison of three cooling methods for burn patients: A randomized clinical trial. Burns 43 (3), 502–508. doi:10.1016/j.burns.2016.09.010
Craig, J. P., Bitton, E., Dantam, J., Jones, L., Ngo, W., and Wang, M. T. M. (2022). Short-term tolerability of commercial eyelid cleansers: A randomised crossover study. Cont. Lens Anterior Eye 45, 101733. doi:10.1016/j.clae.2022.101733
de Groot, A. C., and Schmidt, E. (2016). Essential Oils, Part IV: Contact Allergy. Dermatitis 27 (4), 170–175. doi:10.1097/der.0000000000000197
Deyno, S., Mtewa, A. G., Abebe, A., Hymete, A., Makonnen, E., Bazira, J., et al. (2019). Essential oils as topical anti-infective agents: A systematic review and meta-analysis. Complementary Ther. Med. 47, 102224. doi:10.1016/j.ctim.2019.102224
Down Under Enterprises (2017a). Pure Australian tea tree oil: Medicinal applications of tea tree oil. Available at: https://www.downunderenterprises.com/teatreeoil-antivirus-mechanism.
Down Under Enterprises (2016a). Pure Australian tea tree oil: Personal care applications for skin and hair. Available at: https://www.downunderenterprises.com/.
Down Under Enterprises (2017b). Pure Australian tea tree oil: Tea tree oil in household care products. Available at: https://www.downunderenterprises.com/tto-homecare.
Down Under Enterprises (2016b). Pure Australian tea tree oil: Tea tree oil in oral care applications. Available at: https://www.downunderenterprises.com/.
Dryden, M. S., Dailly, S., and Crouch, M. (2004). A randomized, controlled trial of tea tree topical preparations versus a standard topical regimen for the clearance of MRSA colonization. J. Hosp. Infect. 56 (4), 283–286. doi:10.1016/j.jhin.2004.01.008
Durić, K., Kovčić Hadžiabdić, S., Durić, M., Nikšić, H., Uzunović, A., and Džudžević Čančar, H. (2021). Efficacy and safety of three plant extracts based formulations of vagitories in the treatment of vaginitis: a randomized controlled trial. Med. Glas. (Zenica) 18 (1), 47–54. doi:10.17392/1261-21
Elgendy, E. A., Ali, S. A., and Zineldeen, D. H. (2013). Effect of local application of tea tree (Melaleuca alternifolia) oil gel on long pentraxin level used as an adjunctive treatment of chronic periodontitis: A randomized controlled clinical study. J. Indian Soc. Periodontol. 17 (4), 444–448. doi:10.4103/0972-124x.118314
Enshaieh, S., Jooya, A., Siadat, A. H., and Iraji, F. (2007). The efficacy of 5% topical tea tree oil gel in mild to moderate acne vulgaris: A randomized, double-blind placebo-controlled study. Indian J. Dermatology, Venereol. Leprology 73 (1), 22–25. doi:10.4103/0378-6323.30646
Ernst, E., and Huntley, A. (2000). Tea tree oil: A systematic review of randomized clinical trials. Forsch. Komplementarmedizin Klass. Naturheilkd. 7 (1), 17–20. doi:10.1159/000057164
European Medical Agency (2012). European Union herbal monograph on Melaleuca alternifolia (Maiden and Betch) Cheel, M. linariifolia Smith, M. dissitiflora F. Mueller and/or other species of Melaleuca, aetheroleum EMA/HMPC/320930/2012. Available at: https://www.ema.europa.eu/documents/herbal-monograph/final-european-union-herbal-monograph-melaleuca-alternifolia-maiden-betch-cheel-m-linariifolia-smith/other-species-melaleuca-aetheroleum-first-version_en.pdf.
Montreal Process Implementation Group for Australia and National Forest Inventory Steering Committee (2019). Australia’s State of the Forests Report 2018. Canberra: ABARES. Available at: https://www.awe.gov.au/abares/forestsaustralia/profiles/melaleuca-2019 (Accessed December 1, 2021 2021).
Gnatta, J. R., de Brito Poveda, V., Padoveze, M. C., Graziano, K. U., Turrini, R. N. T., and da Silva, M. J. P. (2021). Melaleuca alternifolia essential oil soap: a potential alternative for hand hygiene. Eur. J. Clin. Microbiol. Infect. Dis. 40 (7), 1517–1520. doi:10.1007/s10096-021-04190-w
Gnatta, J. R., Pinto, F. M., Bruna, C. Q., Souza, R. Q., Graziano, K. U., and Silva, M. J. (2013). Comparison of hand hygiene antimicrobial efficacy: Melaleuca alternifolia essential oil versus triclosan. Rev. Lat. Am. Enferm. 21 (6), 1212–1219. doi:10.1590/0104-1169.2957.2356
Groppo, F. C., Ramacciato, J. C., Simões, R. P., Flório, F. M., and Sartoratto, A. (2002). Antimicrobial activity of garlic, tea tree oil, and chlorhexidine against oral microorganisms. Int. Dent. J. 52 (6), 433–437. doi:10.1111/j.1875-595X.2002.tb00638.x
Hammer, K. A., Carson, C. F., Riley, T. V., and Nielsen, J. B. (2006). A review of the toxicity of Melaleuca alternifolia (tea tree) oil. Food Chem. Toxicol. 44 (5), 616–625. doi:10.1016/j.fct.2005.09.001
Hawkins, J., Hires, C., Dunne, E., and Baker, C. (2020). The relationship between lavender and tea tree essential oils and pediatric endocrine disorders: A systematic review of the literature. Complement. Ther. Med. 49, 102288. doi:10.1016/j.ctim.2019.102288
Hawkins, J., Hires, C., Dunne, E., and Keenan, L. (2021). Prevalence of endocrine disorders among children exposed to Lavender Essential Oil and Tea Tree Essential Oils. Int. J. Pediatr. Adolesc. Med. 9, 117–124. doi:10.1016/j.ijpam.2021.10.001
Henley, D. V., Lipson, N., Korach, K. S., and Bloch, C. A. (2007). Prepubertal gynecomastia linked to lavender and tea tree oils. N. Engl. J. Med. 356 (5), 479–485. doi:10.1056/NEJMoa064725
Higgins, J. P. T., Altman, D. G., Gøtzsche, P. C., Jüni, P., Moher, D., Oxman, A. D., et al. (2011). The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343, d5928. doi:10.1136/bmj.d5928
Hugo Infante, V., Maria Maia Campos, P., Darvin, M., Lohan, S., Schleusener, J., Schanzer, S., et al. (2023). Cosmetic Formulations with Melaleuca alternifolia Essential Oil for the Improvement of Photoaged Skin: A Double-Blind, Randomized, Placebo-Controlled Clinical Study. Photochem Photobiol 99 (1), 176–183. doi:10.1111/php.13660
International Organization for Standardization (2017). ISO 4730:2017(en) Essential oil of Melaleuca, terpinen-4-ol type (Tea Tree oil). 3rd ed. Vernier, Geneva. Switzerland: ISO copyright office (www.iso.org).
Kamath, N. P., Tandon, S., Nayak, R., Naidu, S., Anand, P. S., and Kamath, Y. S. (2020). The effect of aloe vera and tea tree oil mouthwashes on the oral health of school children. Eur. Archives Paediatr. Dent. 21 (1), 61–66. doi:10.1007/s40368-019-00445-5
Karakurt, Y., and Zeytun, E. (2018). Evaluation of the Efficacy of Tea Tree Oil on the Density of Demodex Mites (Acari: Demodicidae) and Ocular Symptoms in Patients with Demodectic Blepharitis. J. Parasitol. 104 (5), 473–478. doi:10.1645/18-46
Koo, H., Kim, T. H., Kim, K. W., Wee, S. W., Chun, Y. S., and Kim, J. C. (2012). Ocular surface discomfort and Demodex: effect of tea tree oil eyelid scrub in Demodex blepharitis. J. Korean Med. Sci. 27 (12), 1574–1579. doi:10.3346/jkms.2012.27.12.1574
Lam, N. S. K., Long, X. X., Li, X., Yang, L., Griffin, R. C., and Doery, J. C. (2020). Comparison of the efficacy of tea tree (Melaleuca alternifolia) oil with other current pharmacological management in human demodicosis: A Systematic Review. Parasitology 147 (14), 1587–1613. doi:10.1017/S003118202000150X
Lee, K. A., Harnett, J. E., and Cairns, R. (2020). Essential oil exposures in Australia: analysis of cases reported to the NSW Poisons Information Centre. Med. J. Aust. 212 (3), 132–133. doi:10.5694/mja2.50403
Lee, R. L. P., Leung, P. H. M., and Wong, T. K. S. (2014). A randomized controlled trial of topical tea tree preparation for MRSA colonized wounds. Int. J. Nurs. Sci. 1 (1), 7–14. doi:10.1016/j.ijnss.2014.01.001
Maghu, S., Desai, V. D., and Sharma, R. (2016). Comparison of efficacy of alternative medicine with allopathy in treatment of oral fungal infection. J. Tradit. Complement. Med. 6 (1), 62–65. doi:10.1016/j.jtcme.2014.11.023
Markum, E., and Baillie, J. (2012). Combination of essential oil of Melaleuca alternifolia and iodine in the treatment of molluscum contagiosum in children. J. Drugs Dermatol 11 (3), 349–354.
Mohammadpour, M., Maleki, S., and Khorrami-Nejad, M. (2020). The effect of tea tree oil on dry eye treatment after phacoemulsification cataract surgery: A randomized clinical trial. Eur. J. Ophthalmol. 30 (6), 1314–1319. doi:10.1177/1120672119867642
Najafi-Taher, R., Jafarzadeh Kohneloo, A., Eslami Farsani, V., Mehdizade Rayeni, N., Moghimi, H. R., Ehsani, A., et al. (2022). A topical gel of tea tree oil nanoemulsion containing adapalene versus adapalene marketed gel in patients with acne vulgaris: a randomized clinical trial. Arch. Dermatol Res. 314 (7), 673–679. doi:10.1007/s00403-021-02267-2
Ozkaraman, A., Dugum, O., Ozen Yilmaz, H., and Usta Yesilbalkan, O. (2018). Aromatherapy: The Effect of Lavender on Anxiety and Sleep Quality in Patients Treated With Chemotherapy. Clin. J. Oncol. Nurs. 22 (2), 203–210. doi:10.1188/18.CJON.203-210
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Rev. Esp. Cardiol. Engl. Ed. 74 (9), 790–799. doi:10.1016/j.rec.2021.07.010
Prabhakar, A. R., Vipin, A. H. U. J. A., and Basappa, N. (2009). Effect of Curry Leaves, Garlic and Tea Tree Oil on Streptococcus Mutans and Lactobacilli in Children: A Clinical and Microbiological Study. Pesqui. Bras. em Odontopediatria Clínica Integr. 9 (3), 259–263. doi:10.4034/1519.0501.2009.0093.0002
Rahman, B., Alkawas, S., Al Zubaidi, E. A., Adel, O. I., and Hawas, N. (2014). Comparative antiplaque and antigingivitis effectiveness of tea tree oil mouthwash and a cetylpyridinium chloride mouthwash: A randomized controlled crossover study. Contemp. Clin. Dent. 5 (4), 466–470. doi:10.4103/0976-237X.142813
Raut, C. P., and Sethi, K. S. (2016). Comparative evaluation of co-enzyme Q10 and Melaleuca alternifolia as antioxidant gels in treatment of chronic periodontitis: A clinical study. Contemp. Clin. Dent. 7 (3), 377–381. doi:10.4103/0976-237X.188572
Reddy, V., Bennadi, D., Satish, G., Divya, G., and Reddy, C. V. K. (2020). Effectiveness of tea tree oil and chlorhexidine as mouth rinse in the control of dental plaque and chronic gingivitis -A comparative study. Eur. J. Mol. Clin. Med. 7 (8), 1576–1582.
Rhind, J. P. (2020). “Melaleuca alternifolia - tea tree,” in Essential oils: A comprehensive handbook for aromatic therapy (United Kingdom: Singing Dragon), 488–493.
Ripari, F., Cera, A., Freda, M., Zumbo, G., Zara, F., and Vozza, I. (2020). Tea Tree Oil versus Chlorhexidine Mouthwash in Treatment of Gingivitis: A Pilot Randomized, Double Blinded Clinical Trial. Eur. J. Dent. 14 (1), 55–62. doi:10.1055/s-0040-1703999
Rothenberger, J., Krauss, S., Tschumi, C., Rahmanian-Schwarz, A., Schaller, H. E., and Held, M. (2016). The Effect of Polyhexanide, Octenidine Dihydrochloride, and Tea Tree Oil as Topical Antiseptic Agents on in vivo Microcirculation of the Human Skin: A Noninvasive Quantitative Analysis. Wounds 28 (10), 341–346.
Salvatori, C., Barchi, L., Guzzo, F., and Gargari, M. (2017). A comparative study of antibacterial and anti-inflammatory effects of mouthrinse containing tea tree oil. Oral Implantol. (Rome) 10 (1), 59–70. doi:10.11138/orl/2017.10.1.059
Satchell, A. C., Saurajen, A., Bell, C., and Barnetson, R. S. (2002a). Treatment of dandruff with 5% tea tree oil shampoo. J. Am. Acad. Dermatol 47 (6), 852–855. doi:10.1067/mjd.2002.122734
Satchell, A. C., Saurajen, A., Bell, C., and Barnetson, R. S. (2002b). Treatment of interdigital tinea pedis with 25% and 50% tea tree oil solution: a randomized, placebo-controlled, blinded study. Australas. J. Dermatol 43 (3), 175–178. doi:10.1046/j.1440-0960.2002.00590.x
Savla, K., Le, J. T., and Pucker, A. D. (2020). Tea tree oil for Demodex blepharitis. Cochrane Database Syst. Rev. 6 (6), CD013333. doi:10.1002/14651858.CD013333.pub2
Saxer, U. P., Stauble, A., Szabo, S. H., and Menghini, G. (2003). Effect of mouthwashing with tea tree oil on plaque and inflammation. Schweiz Monatsschr Zahnmed. 113 (9), 985–996.
Shetty, S. K., Sharath, K., Shenoy, S., Sreekumar, C., Shetty, R. N., and Biju, T. (2013). Compare the effcacy of two commercially available mouthrinses in reducing viable bacterial count in dental aerosol produced during ultrasonic scaling when used as a preprocedural rinse. J. Contemp. Dent. Pract. 14 (5), 848–851. doi:10.5005/jp-journals-10024-1414
Soukoulis, S., and Hirsch, R. (2004). The effects of a tea tree oil-containing gel on plaque and chronic gingivitis. Aust. Dent. J. 49 (2), 78–83. doi:10.1111/j.1834-7819.2004.tb00054.x
Srikumar, K. P., Bhagyashree, B. N., Srirangarajan, S., Ravi, R. J., and Vinaya, R. (2022). Efficacy of Melaleuca alternifolia and chlorhexidine mouth rinses in reducing oral malodor and Solobacterium moorei levels. A 1 week, randomized, double-blind, parallel study. Indian J. Pharmacol. 54 (2), 77–83. doi:10.4103/ijp.ijp_772_20
Taalab, M. R., Mahmoud, S. A., Moslemany, R. M. E., and Abdelaziz, D. M. (2021). Intrapocket application of tea tree oil gel in the treatment of stage 2 periodontitis. BMC Oral Health 21 (1), 239. doi:10.1186/s12903-021-01588-y
Thomas, A., and Deshmukh, R. (2019). Tea tree oil market by application (cosmetics & toiletries application, therapeutics application, and industrial application), end user (FMCG manufacturer, cosmetics companies, pharmaceutical companies, and others), and grade (Pharma/Cosmetic grade and therapeutic grade): Global opportunity analysis and industry forecast, 2018–2025. Allied Market Research.)
Tisserand, R., and Young, R. (2014). Essential oil safety: A guide for health care professionals. Edinburgh: Churchill Livingstone.
Toholka, R., Wang, Y. S., Tate, B., Tam, M., Cahill, J., Palmer, A., et al. (2015). The first Australian Baseline Series: Recommendations for patch testing in suspected contact dermatitis. Australas. J. Dermatol 56 (2), 107–115. doi:10.1111/ajd.12186
Tong, M. M., Altman, P. M., and Barnetson, R. S. (1992). Tea tree oil in the treatment of tinea pedis. Australas. J. Dermatol 33 (3), 145–149. doi:10.1111/j.1440-0960.1992.tb00103.x
Wong, K., Flanagan, J., Jalbert, I., and Tan, J. (2019). The effect of Blephadex Eyelid Wipes on Demodex mites, ocular microbiota, bacterial lipase and comfort: a pilot study. Cont. Lens Anterior Eye 42 (6), 652–657. doi:10.1016/j.clae.2019.06.001
World Health Organization, (1999). WHO consultation on selected medicinal plants (2nd: 1999: Ravello-salerno, Italy). WHO monographs on selected medicinal plants. Geneva: World Health Organization.
Youn, B. H., Kim, Y. S., Yoo, S., and Hur, M. H. (2021). Antimicrobial and hand hygiene effects of Tea Tree Essential Oil disinfectant: A randomised control trial. Int. J. Clin. Pract. 75 (8), e14206. doi:10.1111/ijcp.14206
Keywords: tea tree oil, Melaleuca alternifolia oil, essential oils, phytotherapy, systematic review, randomized controlled trials, anti-infective agents, human trial
Citation: Kairey L, Agnew T, Bowles EJ, Barkla BJ, Wardle J and Lauche R (2023) Efficacy and safety of Melaleuca alternifolia (tea tree) oil for human health—A systematic review of randomized controlled trials. Front. Pharmacol. 14:1116077. doi: 10.3389/fphar.2023.1116077
Received: 08 December 2022; Accepted: 04 January 2023;
Published: 24 March 2023.
Edited by:
Diana Simona Antal, Victor Babes University of Medicine and Pharmacy, RomaniaReviewed by:
Hans Wohlmuth, The University of Queensland, AustraliaCopyright © 2023 Kairey, Agnew, Bowles, Barkla, Wardle and Lauche. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Romy Lauche, cm9teS5sYXVjaGVAc2N1LmVkdS5hdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.