
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol., 04 May 2023
Sec. Pharmacoepidemiology
Volume 14 - 2023 | https://doi.org/10.3389/fphar.2023.1056192
This article is part of the Research TopicLong Term Effects of Prenatal Exposure to Medications and VaccinesView all 7 articles
 Ingvild Odsbu1,2*
Ingvild Odsbu1,2* Marte Handal3,4
Marte Handal3,4 Vidar Hjellvik3
Vidar Hjellvik3 Sonia Hernandez-Diaz5
Sonia Hernandez-Diaz5 Helle Kieler2,6Mette Nørgaard7Svetlana Skurtveit1,4
Helle Kieler2,6Mette Nørgaard7Svetlana Skurtveit1,4 Buket Öztürk Esen7Milada Mahic1
Buket Öztürk Esen7Milada Mahic1Background: Opioids may modulate the immune function through opioid receptors on immune cells. Long-term consequences of prenatal opioid exposure on the immune system, such as childhood asthma, are unknown.
Objectives: To investigate whether prenatal opioid exposure is associated with the risk of childhood asthma.
Methods: Cohort study using linked nationwide registers in Denmark (1996–2015), Norway (2005–2015), and Sweden (2006–2013). Children born by mothers who were chronic opioid analgesics users before pregnancy (n = 14,764) or who were receiving opioid maintenance therapy (OMT) before or during pregnancy (n = 1,595) were identified based on information from each of the medical birth registers and prescription registers. Long-term opioid analgesics exposed children were compared to short-term exposed or unexposed, whereas OMT exposed children were compared to OMT unexposed. Asthma among children ≥1 years of age was defined as two or more filled prescriptions of antiasthmatic medication within 365 days, or a diagnosis of asthma. Hazard ratios (HRs) were calculated using Cox proportional hazards regression with attained age as the time scale. Inverse probability of treatment weights based on propensity scores were applied to adjust for measured confounders. Individual level data from Norway and Sweden were pooled, whereas individual level data from Denmark were analyzed separately. For the opioid analgesics comparisons, adjusted HRs (aHR) from the combined Norwegian/Swedish data and the Danish data were pooled in a fixed-effects meta-analysis.
Results: For the opioid analgesics cohort, no increased risk of asthma was observed in long-term exposed children neither compared with unexposed [aHR = 0.99 (95% CI 0.87-1.12)], nor compared with short-term exposed [aHR = 0.97 (0.86-1.10)]. No increased risk of asthma was observed in OMT exposed compared with OMT unexposed children [Norway/Sweden: aHR = 1.07 (0.60-1.92), Denmark: aHR = 1.25 (0.87-1.81)]. Results from sensitivity analyses, where potential misclassification of the outcome and misclassification of OMT exposure were assessed, as well as starting follow-up at 6 years of age, showed that the estimates of association were generally robust.
Conclusion: We found no association between prenatal exposure to opioids and risk of childhood asthma. Results were consistent across two different opioid exposure groups with different confounder distributions.
Asthma is one of the most common chronic diseases among children with high burden for affected individuals as well as for the health care system (Lai et al., 2009; Serebrisky and Wiznia, 2019). If not diagnosed and controlled properly, children with asthma are at higher risk of future morbidity and mortality (Serebrisky and Wiznia, 2019; Caffrey Osvald et al., 2020). The mechanisms behind the development of childhood asthma are largely unknown. Prenatal exposures might affect immune programming during fetal development and trigger immune-mediated diseases, including asthma, later in life (Olin et al., 2018). Asthma is characterized by imbalance of the immune system, overactive Th2 immune response and a downregulated Th1 immune response, and exposures with the ability to skew the immune response towards a Th2 phenotype could potentially increase the risk of asthma development (Holtzman, 2012; Douros et al., 2017). Opioids are found to modulate the immune system through opioid receptors on immune cells and affect the balance of the immune response (Vallejo et al., 2004; Al-Hashimi et al., 2013; Plein and Rittner, 2018). Since opioids pass the placenta (Malek and Mattison, 2011), prenatal exposure to opioids might modulate the immune function of the developing fetus.
Pregnant women use opioid analgesics for pain treatment and the prevalence of use during pregnancy has been reported to be from 2.9% to 5.1% in the Nordic countries (Handal et al., 2011; Stephansson et al., 2011; Faltmarch et al., 2019), and as high as 14.4%–21.6% in the US (Bateman et al., 2014; Desai et al., 2014). Clinical guidelines in the Nordic countries recommend using opioid analgesics for the shortest possible time and at the lowest effective dose if such treatment is indicated during pregnancy (Läkemedelsboken, 2015; Dansk Selskab for Obstetrik og Gynækologi, 2016; Norsk legemiddelbok, 2019). In addition to treatment of pain, pregnant women receive opioids (methadone or buprenorphine) for treatment of opioid use disorder [opioid maintenance treatment (OMT)]. Clinical guidelines recommend that pregnant women already receiving OMT continue their treatment throughout pregnancy, or that OMT is initiated in pregnant women not already receiving such treatment (Handal et al., 2020). Most women receiving OMT are of childbearing age (Gyarmathy et al., 2009). Since 1997 in Denmark, 2005 in Norway and 2006 in Sweden, approximately 800 women were reported to have received OMT drugs during pregnancy (Handal et al., 2020). Over the past decades, an increasing use of opioid analgesics was observed, not only in the general population, but also in the pregnant population (Bjorn et al., 2011; Desai et al., 2014; Muller et al., 2019). The increased use of opioid analgesics could potentially put more individuals at risk of developing opioid use disorder.
For children exposed prenatally to opioids, there seems to be increased risk of adverse birth outcomes and neonatal outcomes such as neonatal abstinence syndrome (Desai et al., 2015; Nørgaard et al., 2015; Wurst et al., 2016; Sujan et al., 2019). In contrast, evidence on long-term consequences of prenatal opioid exposure on immune reactions is scarce. A recent study found no evidence for an association between prenatal opioid exposure and risk of infections in the offspring (Mahic et al., 2020). Some epidemiological studies have investigated the association between prenatal exposure to analgesics and risk of childhood asthma with conflicting results (Källén et al., 2013; Cheelo et al., 2015; Magnus et al., 2016; Fan et al., 2017; Shaheen et al., 2019).
As an increasing number of pregnant women use opioids, more knowledge is needed about the long-term consequences of proposed opioid-induced immunomodulation in the fetus. In this population-based cohort study, we examined the association between prenatal opioid exposure and childhood asthma in live-born children from Denmark, Norway, and Sweden. To minimize any background differences between the groups, we compared children whose mothers had similar indications for opioid use, either long-term opioid use for pain or opioid use disorders. A potential dose-response relationship was also assessed.
Data were retrieved from the national health- and population registers in Denmark, Norway, and Sweden. The Nordic countries have comparable public healthcare systems and population-based registers, and all citizens have unique personal identification numbers which makes it possible to link data sources within a country (Laugesen et al., 2021). The medical birth registers contain information on all deliveries from week 12 (Norway) and week 22 (Denmark and Sweden) of gestation (Langhoff-Roos et al., 2014). The personal identity numbers of the live-born infant and parents are recorded. The prescription registers contain information on all filled prescriptions to patients in ambulatory care (Furu et al., 2010). Data on drugs administered in hospitals are not captured in the prescription registers. Drugs are classified according to the Anatomic Therapeutic Chemical (ATC) classification system (WHO, 2021a). The national patient registers capture hospitalizations and visits in outpatient specialist care (the latter not captured in Denmark). Diagnoses are recorded according to the International Classification of Diseases, 10th revision (ICD-10) (WHO, 1992). The patient registers do not capture visits in primary care. In Norway, data on diagnosis from primary care [ICPC-2, International Classification of Primary Care, 2nd edition (WONCA, 1998)] were retrieved from the Control and Payment of Health Reimbursement (KUHR) database (The Norwegian Directorate of Health, 2022). Data on cause of death (ICD-10) were retrieved from the cause of death registers, and information on emigration (not Sweden) was retrieved from the population registers. Individual level data from Norway and Sweden were pooled, whereas individual level data from Denmark were analyzed separately due to legal restrictions on data sharing between countries.
A cohort of children born in Denmark 1997–2015, Norway 2005–2015, or Sweden July 1 2006–2013, and whose mothers used opioids pre-pregnancy (opioid analgesics, illicit opioids or OMT), was identified from the medical birth registers and prescription registers. A total of 1,471,406 children born in Norway/Sweden and 1,207,989 children born in Denmark were eligible for inclusion in the study. There were 14,764 children in the opioid analgesics cohort and 1,595 children in the OMT cohort.
Opioids included in the study were opioid analgesics (ATC code N02A) and opioids used for OMT. OMT drugs included methadone oral solution (ATC code N07BC02) and high-dose buprenorphine tablets (≥2 mg sublingual tablets, ATC codes N07BC01 or N07BC51) which, in Scandinavia, are almost solely prescribed for the treatment of opioid use disorder. Pre-pregnancy opioid use was defined as either having filled at least three prescriptions of opioid analgesics and 30 or more days of supply in the period of up to 12 months prior to pregnancy start (chronic opioid analgesics users) or having filled at least one prescription of any OMT drug in the period of up to 12 months prior to pregnancy or using illicit opioids before pregnancy (i.e., mothers filling prescriptions of OMT drugs during pregnancy, but not in the 12 months period before pregnancy) (Supplementary Figure S1). Information on illicit opioid use was not available, but since only mothers who had used illicit opioids before pregnancy would be initiated on OMT during pregnancy, we assumed that mothers receiving OMT during pregnancy were exposed to illicit opioids in the year before pregnancy. Pregnancy start was defined as the first day of the last menstrual period (LMP) and was ascertained using date of delivery and gestational age mainly based on prenatal ultrasound. Days’ supply was defined as the number of defined daily doses (DDDs) dispensed. The DDD is the assumed average maintenance dose per day for a drug used for its main indication in adults (WHO, 2021b).
For children born to mothers with chronic opioid analgesics use before pregnancy, we made three mutually exclusive comparison groups based on exposure to opioid analgesics during pregnancy, i.e., from pregnancy start until delivery (Supplementary Figure S1). Long-term maternal opioid analgesics use during pregnancy (i.e., long-term exposed children) was defined as being dispensed 30 or more days of supply during pregnancy, whereas short-term opioid analgesic use during pregnancy (i.e., short-term exposed children) was defined as being dispensed less than 30 days of supply. Opioid analgesics discontinuation (i.e., unexposed children) was defined as no filled prescriptions of opioids during pregnancy.
For children born to mothers with opioid use disorder (OMT cohort), we made two mutually exclusive comparison groups (Supplementary Figure S1). OMT exposed children were defined as children whose mothers filled at least one prescription of any OMT drug during pregnancy and who either filled OMT prescriptions before pregnancy or had illicit drug use before pregnancy. OMT unexposed children were defined as children whose mothers filled at least one prescription of any OMT drug in the 12 months prior to pregnancy and who did not fill any prescriptions of OMT drugs during pregnancy.
Asthma was defined based on filled prescriptions of asthma drugs from the prescription registers and/or asthma diagnoses from the patient registers. In children 1 year of age or older, asthma was defined as two or more dispensed inhaled corticosteroids (ATC code R03BA), leukotriene receptor antagonists (R03DC), or fixed combinations of β2-agonists and corticosteroids (R03AK) within 365 days (and not on the same day) during follow-up time, or an asthma diagnosis (ICD-10 J45 or J46) as a primary or secondary diagnosis from specialist healthcare. The date of onset was set as the date when the child was defined as having asthma, i.e., the day of the first filled prescription within a 365-day period of any of the drugs or first date of diagnosis, whichever came first.
Information on maternal age, parity, smoking during pregnancy, cohabitation/marital status, sex of the child, year of birth and birth season was retrieved from the medical birth registers. Information on selected maternal diseases (asthma, reoccurring urinary tract infection, and hepatitis B and C) was retrieved from the medical birth registers, patient registers, and prescription registers (filled prescriptions of asthma drugs). Total number of any filled prescriptions, total number of pharmacological subgroups (ATC 3rd level) dispensed, total number of filled prescriptions for systemic treatment of infections (ATC group J), and dispensations (yes/no) of non-opioid analgesics (ATC groups N02B, N02C or M01), corticosteroids (ATC group H02A) and treatments for chronic obstructive pulmonary disease (ATC group R03) during pregnancy were retrieved from the prescription registers. All variables were assessed from pregnancy start until delivery, except for information on maternal chronic diseases from the patient registers that were assessed from 12 months before pregnancy start. Definitions of the covariates are shown in Supplementary Table S1.
We included only women with complete information on all covariates (complete case analysis).
Characteristics of the mothers and newborns were summarized and described according to drug exposure. Crude cumulative incidence of asthma by age 4 years was calculated using the cumulative incidence function (CIF) to account for competing events. Cumulative incidence curves are presented in Supplementary Figure S2. The association between exposure and risk of childhood asthma was analyzed in children 1 year of age or older using Cox proportional hazard regression, with attained age as the time scale. We studied childhood asthma in children 1 year of age or older to avoid misclassification of the outcome in the youngest children as symptoms from respiratory infections can be misinterpreted as asthma, and also, antiasthmatic medication can be used to relieve such symptoms in young children. Individuals were censored at first study outcome, emigration (in Norway and Denmark), death, or end of study period, whichever occurred first. Hazard ratios (HRs) were calculated for long-term opioid analgesics exposed children versus short-term exposed, and long-term exposed versus unexposed, as well as OMT exposed children versus OMT unexposed. For the OMT comparison, restricted follow-up (730 days, i.e., 1–3 years of age) was applied for the pooled Norwegian/Swedish data due to few observations beyond 3 years of age (Supplementary Figures S3, S4). No restriction was applied for the OMT comparison for the Danish data.
Propensity scores were calculated to address imbalances in baseline confounder distributions. In logistic regression models, the probability of receiving treatment was estimated conditional on a set of identified confounders and risk factors for the outcome. A directed acyclic graph (DAG) showing the covariates included in the propensity score is shown in Supplementary Figure S5. We used the inverse probability of treatment weighting (IPTW) approach based on the propensity score to estimate hazard rate ratios associated with opioid use. Balance of baseline characteristics in the weighted population was assessed using the standardized mean difference. The standardized mean differences before and after applying the IPTW are included in the supplementary material (Supplementary Tables S3–S5). Normalized IPTW weights were included in adjusted Cox regression. Clustered robust variance estimators for 95% confidence intervals were used to account for clustering among mothers with multiple pregnancies.
For the opioid analgesics comparisons, adjusted HRs from Norway/Sweden and Denmark were pooled in a fixed-effects meta-analysis using the inverse variance method, that is weighting the country-specific log-hazard ratios (HRs) by the inverse of the within-countries’ variances. Meta-analysis was not performed for the OMT comparison since restricted follow-up was applied for the pooled Norwegian/Swedish data.
Statistical analyses were conducted using R (R Core Team, 2020). and SAS 9.4 (SAS Institute Inc., Cary, United States).
Two sensitivity analyses were performed to evaluate potential misclassification of the outcome. In the first (sensitivity 1), the outcome was defined as two or more dispensed inhaled corticosteroids (R03BA), leukotriene receptor antagonists (R03DC), or fixed combinations of β2-agonists and corticosteroids (R03AK) within 365 days (and not on the same day) during follow-up time, and an asthma primary or secondary diagnosis (J45 or J46) (i.e., both filled prescriptions and diagnosis required). In the second (sensitivity 2), the outcome was defined as two or more dispensed inhaled corticosteroids (R03BA), leukotriene receptor antagonists (R03DC), or fixed combinations of β2-agonists and corticosteroids (R03AK) (not on the same day), or three or more dispensed selective β2-agonists (R03AC) within 365 days (on three different days) during follow-up time, or an asthma primary or secondary diagnosis (J45 or J46) (i.e., including short-acting β2-agonists). As an asthma diagnosis generally is more reliable, when set at a later age, we also performed a sensitivity analysis (sensitivity 3) where follow-up started at 6 years of age. To evaluate potential misclassification of OMT exposure we performed two additional analyses where OMT unexposed children with neonatal abstinence syndrome (NAS) were removed from the analysis (sensitivity 4) and where OMT unexposed children with NAS were defined as OMT exposed (sensitivity 5).
Use of data was approved by the Regional Ethical Research Board in Norway (2014/358/REK sør-øst D) and the Regional Ethical Review Board in Stockholm, Sweden (2009/775-31/4, 2016/152-32, and 2017/1159-32), and the Norwegian (16/01326-2/SBO) and the Danish Data Protection Agency (J.nr. 2013-41-1789). The national parliaments have on behalf of their populations given informed consent to be included in the registers. According to Danish legislation, no ethical permission is needed for registry-based research in Denmark.
Baseline characteristics of mothers and newborns are presented in Table 1. Among mothers who were chronic opioid analgesics users before pregnancy in the pooled Norwegian and Swedish cohort, those who were long-term exposed to opioids during pregnancy seemed to have a higher burden of health problems compared to those discontinuing use (unexposed) during pregnancy as shown by a higher number of pharmacological subgroups dispensed (64.2% vs. 32.9% were dispensed five or more subgroups) as well as more frequent use of other prescription drugs. In addition, long-term exposed mothers had higher parity (71.3% vs. 57.4% with 2 or more births) and higher prevalence of asthma (24.0% vs. 18.9%). Long-term opioid analgesics exposed mothers were more frequently smoking during pregnancy compared to those discontinuing use during pregnancy (30.2% vs. 21.2%). Mothers who were short-term exposed to opioids during pregnancy were found to be slightly healthier than the long-term exposed mothers. The observed patterns were similar in the Danish cohort. Neonatal abstinence syndrome (NAS) was more frequently reported for children long-term exposed to opioid analgesics (1.9% in Norway/Sweden and 8.2% in Denmark) compared to unexposed children (0.2% in Norway/Sweden and 0.8% in Denmark).
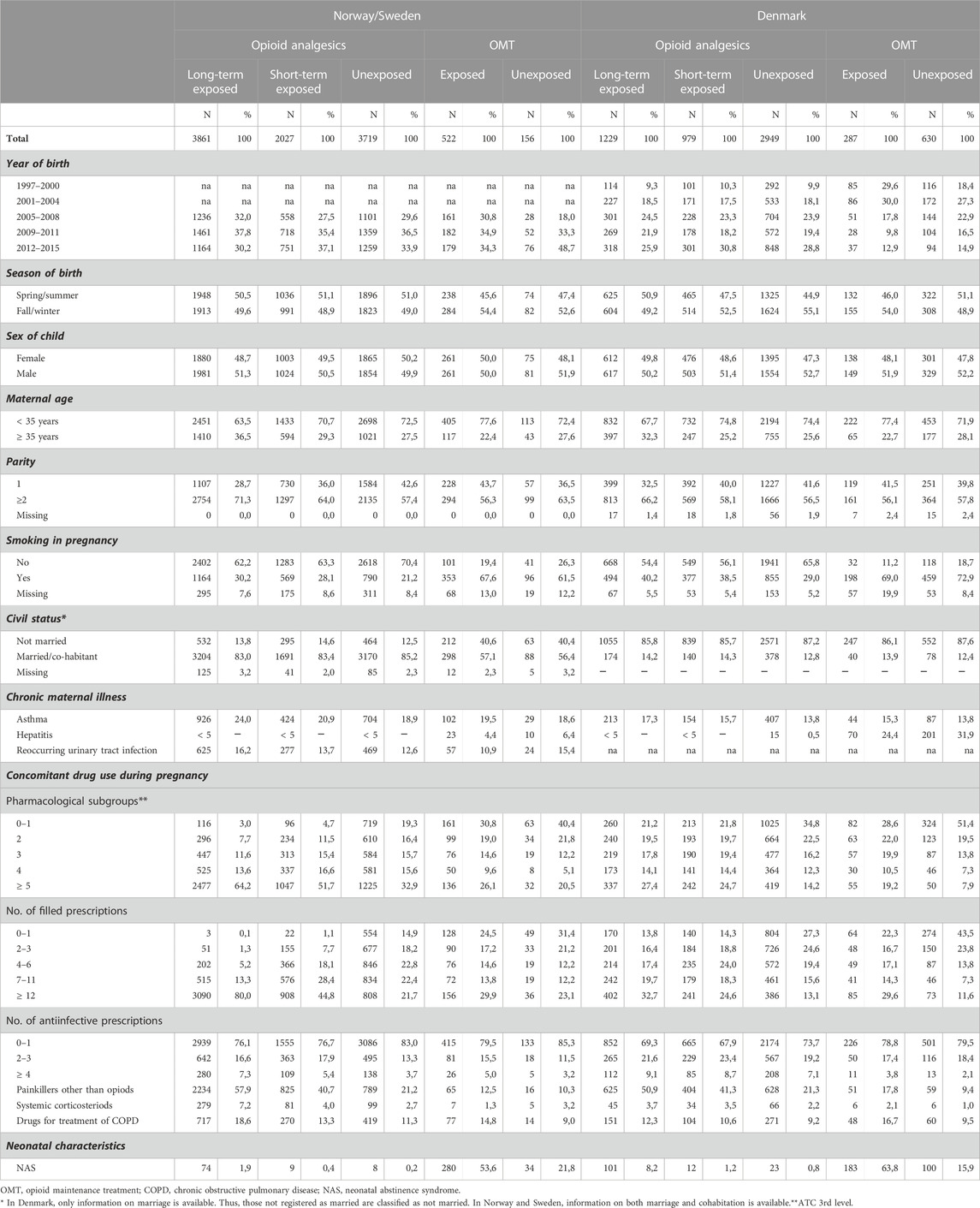
TABLE 1. Baseline characteristics of mothers and newborns stratified by comparison group.
A large proportion of OMT exposed mothers and OMT discontinuers were smokers (OMT exposed: 67.6% in Norway/Sweden and 69.0% in Denmark). A higher proportion of the OMT exposed mothers were prescribed drugs belonging to five or more pharmacological subgroups and had a higher total number of any filled prescriptions during pregnancy compared with OMT discontinuers. The prevalence of hepatitis B and C virus infection was higher among OMT discontinuers (6.4% in Norway/Sweden and 31.9% in Denmark) compared to OMT exposed mothers. NAS was reported for more than half of the children in the OMT exposed cohort compared to 16% (Norway/Sweden) and 22% (Denmark) in the OMT unexposed cohort.
Supplementary Figure S2 shows the unadjusted cumulative incidence curves for all exposure groups in Norway/Sweden and Denmark. Also, the 4-year cumulative incidence of asthma for all exposure groups is presented in Table 2.
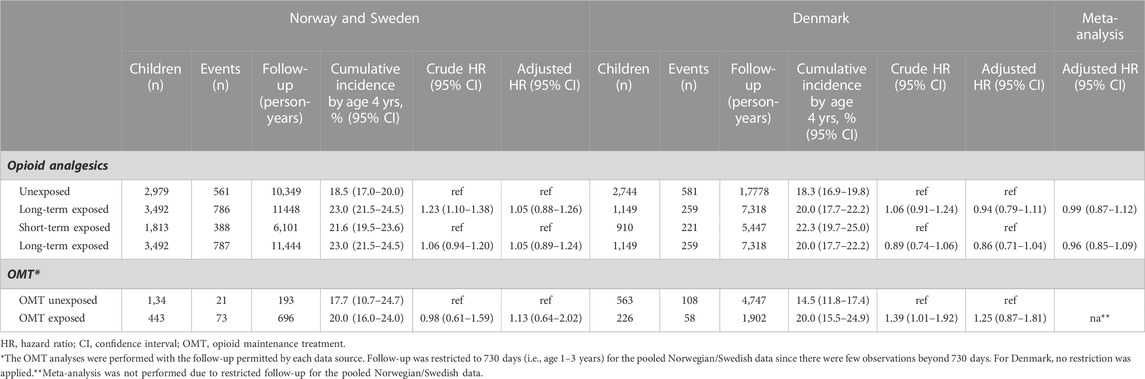
TABLE 2. Cumulative incidence and propensity-score (PS) adjusted hazard ratios (HRs) for the association between prenatal opioid exposure and risk of childhood asthma.
In the opioid analgesics cohort, the adjusted HR from the fixed-effects meta-analysis was 0.99 [95% CI 0.87-1.12] when long-term exposed children were compared with unexposed (Table 2). Similarly, when comparison was made between long- and short-term opioid analgesics exposed children, the adjusted HR was 0.96 (0.85–1.09). Details on country-specific estimates are presented in Table 2. In the Norwegian/Swedish OMT cohort the adjusted HR at 3 years of age was 1.13 (0.64–2.02) when OMT exposed children were compared with OMT unexposed children (Table 2). For the Danish OMT cohort, where no restriction of follow-up time was applied, the adjusted HR was 1.25 (0.87–1.81).
For the opioid analgesic cohort, the estimates from the sensitivity analyses were in the same range as the main analysis (Figure 1). The point estimate was increased when follow-up started from 6 years of age (sensitivity 3), especially for the long-term exposed versus short-term exposed comparison. However, the estimate was imprecise [1.25 (0.85–1.83)]. For the OMT cohort the estimates were also in the same range as the main analysis, but with wider confidence intervals when we applied a stricter outcome definition (sensitivity 1), especially in the pooled data from Norway and Sweden [1.90 (0.66–5.44)] (Figure 2). When follow-up started from 6 years of age in the Danish data, the estimate also became less precise [0.94 (0.32–2.80)]. Details on country-specific estimates are presented in Supplementary Table S2.
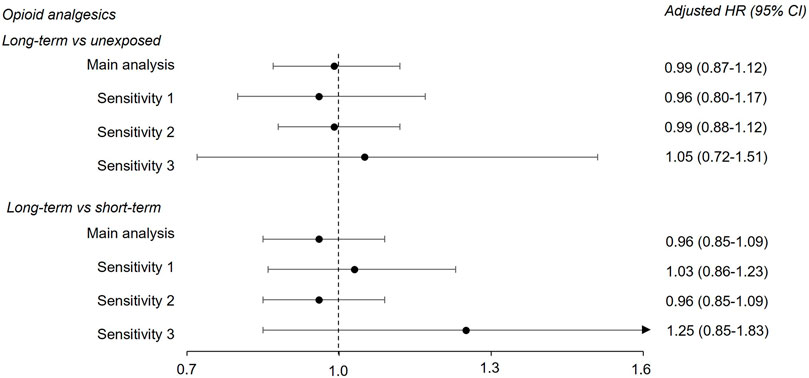
FIGURE 1. Adjusted hazard ratios (HR) and corresponding 95% confidence intervals (CI) from fixed-effects meta-analysis for the long-term opioid analgesics versus unexposed comparison and the long-term opioid analgesics versus short-term comparison. Results from main and sensitivity analyses are shown. See Table 2 and Supplementary Table S2 for country-specific estimates, as well as sensitivity analyses definitions.
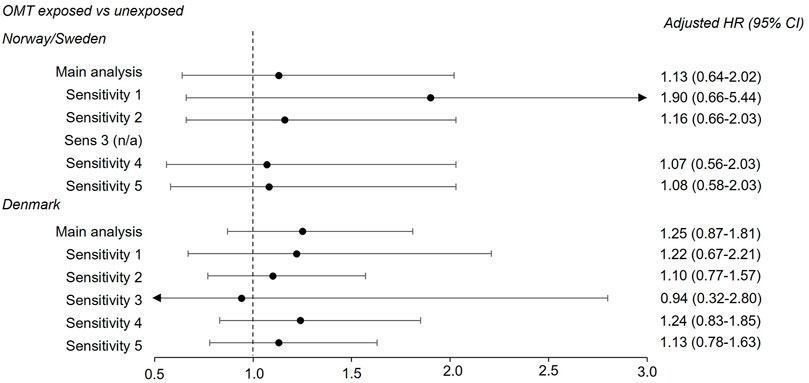
FIGURE 2. Adjusted hazard ratios (HR) and corresponding 95% confidence intervals (CI) from country-specific main and sensitivity analyses for the OMT exposed versus unexposed comparison. See footnote in Supplementary Table S2 for sensitivity analyses definitions. As follow-up was restricted at 3 years of age in the pooled data from Norway and Sweden, sensitivity analysis 3 (follow-up from 6 years of age) was not performed. OMT, opioid maintenance treatment.
In this Scandinavian cohort study with a total follow-up of up to 10 years in pooled data from Norway and Sweden and 19 years in Denmark, we report no significant increased risk of childhood asthma when comparing children born to mothers who were chronic opioid analgesic users before pregnancy and who either continued or discontinued use of opioids during pregnancy. No dose-response relationship was observed when comparing children long-term exposed to opioid analgesics with short-term exposed children. Results from the sensitivity analyses showed that the estimates of association were generally robust.
When comparing OMT exposed children with OMT unexposed, a non-significant increased risk of 25% was observed in Denmark. A non-significant increased risk of 13% was observed in children up to 3 years of age in the pooled data from Norway and Sweden. However, the upper bound of the confidence intervals ruled out more than a doubling of the risk. In the sensitivity analysis where we applied a stricter outcome definition, the estimates became imprecise especially in the pooled data from Norway and Sweden. When children with NAS, who were considered unexposed to OMT were reclassified as exposed, the estimates moved towards the null further supporting no association.
If there was a causal relationship between prenatal exposure to opioids and childhood asthma, we would have expected it to be reflected as a dose-response relationship when comparing children short-term or long-term exposed to opioid analgesics, unless there is a low threshold dose that triggers the effect. No such dose-response relationship was observed in our study. Also, no association was observed among children exposed to OMT, and thereby much higher opioid doses than for pain treatment, further supporting no dose-response relationship.
The Nordic countries have similar health systems and health- and population registers which makes it possible to perform large multi-database studies which is an advantage when studying rare exposures and rare outcomes (Selmer et al., 2016). Although the health systems and registers share many similarities, different treatment traditions and coding practices could lead to some variables being recorded differently or more accurately in one country than in the other countries. For the opioid analgesics cohorts, the prevalence of NAS was consistently higher in the Danish cohort. One possible explanation could be different opioid use patterns during pregnancy in the different countries. During the study period there were higher use of tramadol, oxycodone, and morphine among pregnant women in Denmark compared to Norway and Sweden where use of codeine-paracetamol was more common (Milada Mahic, personal communication). It has previously been shown that the risk of NAS is high for the opioids used in Denmark (Esposito et al., 2022). In our study we found that the prevalence of hepatitis was much higher in the OMT cohort in Denmark compared to the OMT cohort in Norway/Sweden. One possible explanation could be that the Danish cohort was comprised of women giving birth from the mid-1990s, while the Norwegian/Swedish cohort included births from mid-2000s. The introduction of direct-acting antivirals agents (DAAs) for treatment of hepatitis C infection were introduced from 2011 and has revolutionized treatment of hepatitis (Pecoraro et al., 2019). Thus, in the Danish cohort more women did not have access to such treatment.
Two previous population-based studies from Sweden have investigated the association between prenatal exposure to opioids and risk of childhood asthma. Källen et al found a positive association when adjusting for potential confounders, but the association was attenuated after restricting to women without asthma [OR = 1.56 (1.05-2.34)] showing that maternal asthma is an important confounder (Källén et al., 2013). Confounding by indication was not taken into consideration as children born to mothers exposed to opioids during pregnancy was compared with unexposed mothers with no requirement of pre-pregnancy opioid use. A recent population-based study from Sweden reported a positive association between prenatal opioid exposure and asthma/wheeze in children at the age of 4 years after adjusting for potential confounders [OR = 1.39 (1.30–1.49)]. However, when adjusting for intrinsic maternal factors, such as chronic pain and anxiety, in a sibling analysis, no association was observed [OR = 0.91 (0.62–1.31)] (Shaheen et al., 2019). The authors also investigated paracetamol and antimigraine drugs with similar results and concluded that the observed positive associations between prenatal exposure to analgesics and childhood asthma likely is confounded by maternal factors. Likewise, in a study from Norway an association between maternal pain in pregnancy and risk of childhood asthma was observed, further supporting maternal pain as an important confounder (Magnus et al., 2016).
To avoid confounding by indication it is important to choose relevant comparison groups. In our study we included women who were chronic opioid users before pregnancy, both women using opioid analgesics and women receiving OMT. The baseline characteristics of the various exposure groups indicated that the burden of health problems among these women correlated with the reason for use and treatment intensity. By applying propensity scores and a weighted approach, the observed differences in background characteristics were balanced and no associations were observed, further supporting the findings by Shaheen et al. (2019).
The study had several strengths. All live births in Denmark, Norway, and Sweden in the study period were included. Drug exposure was based on prospectively collected data on filled prescriptions from the nationwide prescription registers eliminating the possibility for recall bias and primary non-compliance (Furu et al., 2010). Confounding by indication was controlled for by only including women with chronic opioid analgesics use or use of OMT drugs or illicit opioid use before pregnancy. For the opioid analgesics comparisons, it was important to exclude women using opioids to treat acute pain since they might have a different health status than women using opioid analgesics long-term. Opioid use with two different indications were explored, namely, pain and opioid use disorder, representing women with different confounder distributions and different treatment intensity. Women receiving OMT were studied separately since opioid use disorder is associated with worse health outcomes and more unstable living conditions that could potentially lead to bias of the result if this population was compared with women not receiving OMT. By using propensity scores, the comparison groups were balanced across several potential important confounders making it possible to come closer to unbiased associations.
The study had some limitations. Since exposure is based on filled prescriptions, we do not know whether the women used the drugs. However, by only including chronic opioid analgesics users, the women had filled several prescriptions or been dispensed a large amount of opioids before pregnancy, increasing the probability that they were consuming the drugs. Timing of exposure in pregnancy, which may be important particularly for exposure during early development when the immune system is developing, could not be assessed due to small sample size. We also did not assess exposure to individual opioids so any drug specific effects could be masked. Further, regarding OMT exposure, some women might receive OMT drugs from specialized addiction outpatient clinics within specialist care. As the prescription registers only contain information about filled prescriptions from pharmacies this might lead to selection bias since some OMT exposed children might not be captured. It could also lead to misclassification of exposure as some women retrieving OMT drugs from pharmacies before pregnancy might have a closer follow-up in specialized outpatient clinics during pregnancy and their OMT drug use during pregnancy would not be captured. We tried to overcome this limitation by performing sensitivity analyses to address potential misclassification of OMT exposure. We did not have information about illicit opioid use which could be an issue particularly for the OMT analyses.
Identifying asthma in children is challenging since, particularly in small children, symptoms of respiratory infections could be misinterpreted as asthma and antiasthmatic medications could be used to relieve such symptoms. We performed a range of sensitivity analyses to address potential misclassification of the outcome.
Even though we tried to identify women with chronic pain via chronic opioid analgesics use, we did not have information about the severity of pain that could have an impact on the observed associations. Also, we had no information about whether the women had planned to become pregnant, but it is estimated that 38% of pregnancies in Northern Europe are unintended (Sedgh et al., 2014). A planned pregnancy might indicate a healthier lifestyle, and this could also be the reason for discontinuing drug use. We tried to overcome this by using propensity scores to balance the measured covariates, but there could still be differences in unmeasured covariates.
We found no association between prenatal exposure to opioids and risk of childhood asthma. Also, we did not observe any dose-response relationship for opioid exposure. The results were consistent across two different opioid exposure groups with different confounder distributions. Our findings are reassuring for women who need to use opioids in pregnancy. The study shows the importance of choosing relevant comparison groups and applying appropriate statistical methods to control for confounding by indication.
The data analyzed in this study is subject to the following licenses/restrictions: The register-based cohorts are based on individual-level data from national health and population registers. The authors are not allowed, by law, to publicly share this data. Therefore, the authors cannot make this data fully available to the public. The authors may share statistical code. Requests to access these datasets should be directed to the register holders in each country.
The studies involving human participants were reviewed and approved by the Regional Ethical Research Board in Norway (2014/358/REK sør-øst D) and the Regional Ethical Review Board in Stockholm, Sweden (2009/775-31/4, 2016/152-32, and 2017/1159-32), and the Norwegian (16/01326-2/SBO) and the Danish Data Protection Agency (J.nr. 2013-41-1789). The national parliaments have on behalf of their populations given informed consent to be included in the registers. According to Danish legislation, no ethical permission is needed for registry-based research in Denmark. Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
All authors contributed to conception and design of the study. VH, BE, and MM performed the statistical analysis. IO wrote the first draft of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
The Scandinavian cohort study has received grants from the Research Council of Norway, Grant no 240197/H10. IO, VH, and SS were also partly funded by the Research Council of Norway Grant no 320360.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer NT declared a shared affiliation with the author(s) MH and SS to the handling editor at the time of review.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2023.1056192/full#supplementary-material
Al-Hashimi, M., Scott, S. W., Thompson, J. P., and Lambert, D. G. (2013). Opioids and immune modulation: More questions than answers. Br. J. Anaesth. 111 (1), 80–88. doi:10.1093/bja/aet153
Bateman, B. T., Hernandez-Diaz, S., Rathmell, J. P., Seeger, J. D., Doherty, M., Fischer, M. A., et al. (2014). Patterns of opioid utilization in pregnancy in a large cohort of commercial insurance beneficiaries in the United States. Anesthesiology 120 (5), 1216–1224. doi:10.1097/aln.0000000000000172
Bjorn, A. M., Norgaard, M., Hundborg, H. H., Nohr, E. A., and Ehrenstein, V. (2011). Use of prescribed drugs among primiparous women: An 11-year population-based study in Denmark. Clin. Epidemiol. 3, 149–156. doi:10.2147/clep.s17747
Caffrey Osvald, E., Bower, H., Lundholm, C., Larsson, H., Brew, B. K., and Almqvist, C. (2020). Asthma and all-cause mortality in children and young adults: A population-based study. Thorax 75 (12), 1040–1046. doi:10.1136/thoraxjnl-2020-214655
Cheelo, M., Lodge, C. J., Dharmage, S. C., Simpson, J. A., Matheson, M., Heinrich, J., et al. (2015). Paracetamol exposure in pregnancy and early childhood and development of childhood asthma: A systematic review and meta-analysis. Arch. Dis. Child. 100 (1), 81–89. doi:10.1136/archdischild-2012-303043
Dansk Selskab for Obstetrik og Gynækologi (2016). Behandling af akutte og kroniske smerter hos gravide. Available from: https://static1.squarespace.com/static/5467abcce4b056d72594db79/t/579a3aa320099e24a49bb68f/1469725350260/160211+Behandling+af+akutte+og+kroniske+smerter+hos+gravide.pdf [accessed 02 01 2023].
Desai, R. J., Hernandez-Diaz, S., Bateman, B. T., and Huybrechts, K. F. (2014). Increase in prescription opioid use during pregnancy among Medicaid-enrolled women. Obstet. Gynecol. 123 (5), 997–1002. doi:10.1097/aog.0000000000000208
Desai, R. J., Huybrechts, K. F., Hernandez-Diaz, S., Mogun, H., Patorno, E., Kaltenbach, K., et al. (2015). Exposure to prescription opioid analgesics in utero and risk of neonatal abstinence syndrome: Population based cohort study. Bmj 350, h2102. doi:10.1136/bmj.h2102
Douros, K., Moustaki, M., Tsabouri, S., Papadopoulou, A., Papadopoulos, M., and Priftis, K. N. (2017). Prenatal maternal stress and the risk of asthma in children. Front. Pediatr. 5, 202. doi:10.3389/fped.2017.00202
Esposito, D. B., Huybrechts, K. F., Werler, M. M., Straub, L., Hernández-Díaz, S., Mogun, H., et al. (2022). Characteristics of prescription opioid analgesics in pregnancy and risk of neonatal opioid withdrawal syndrome in newborns. JAMA Netw. Open 5 (8), e2228588. doi:10.1001/jamanetworkopen.2022.28588
Faltmarch, S., Perttila, I., Tuomi, U., Kautiainen, H., Gissler, M., Pennanen, P., et al. (2019). Use of opioids during pregnancy and effects of pregnancy outcomes. Pharmacoepidemiol Drug Saf. 28 (9), 1239–1245. doi:10.1002/pds.4848
Fan, G., Wang, B., Liu, C., and Li, D. (2017). Prenatal paracetamol use and asthma in childhood: A systematic review and meta-analysis. Allergol. Immunopathol. Madr. 45 (6), 528–533. doi:10.1016/j.aller.2016.10.014
Furu, K., Wettermark, B., Andersen, M., Martikainen, J. E., Almarsdottir, A. B., and Sorensen, H. T. (2010). The Nordic countries as a cohort for pharmacoepidemiological research. Basic Clin. Pharmacol. Toxicol. 106 (2), 86–94. doi:10.1111/j.1742-7843.2009.00494.x
Gyarmathy, V. A., Giraudon, I., Hedrich, D., Montanari, L., Guarita, B., and Wiessing, L. (2009). Drug use and pregnancy - challenges for public health. Euro Surveill. 14 (9), 33–36. doi:10.2807/ese.14.09.19142-en
Handal, M., Engeland, A., Ronning, M., Skurtveit, S., and Furu, K. (2011). Use of prescribed opioid analgesics and co-medication with benzodiazepines in women before, during, and after pregnancy: A population-based cohort study. Eur. J. Clin. Pharmacol. 67 (9), 953–960. doi:10.1007/s00228-011-1030-7
Handal, M., Skurtveit, S., Mahic, M., Öhman, I., Wikner, B. N., Tjagvad, C., et al. (2020). Opioid maintenance treatment of pregnant women in the Scandinavian countries. Nordic Stud. Alcohol Drugs 37 (3), 298–312. doi:10.1177/1455072520914114
Holtzman, M. J. (2012). Asthma as a chronic disease of the innate and adaptive immune systems responding to viruses and allergens. J. Clin. Invest. 122 (8), 2741–2748. doi:10.1172/jci60325
Källén, B., Finnström, O., Nygren, K. G., and Otterblad Olausson, P. (2013). Maternal drug use during pregnancy and asthma risk among children. Pediatr. Allergy Immunol. 24 (1), 28–32. doi:10.1111/pai.12034
Lai, C. K., Beasley, R., Crane, J., Foliaki, S., Shah, J., Weiland, S., et al. (2009). Global variation in the prevalence and severity of asthma symptoms: Phase three of the international study of asthma and allergies in childhood (ISAAC). Thorax 64 (6), 476–483. doi:10.1136/thx.2008.106609
Läkemedelsboken (2015). Sjukdomar och läkemedel under graviditet och amning. Available from: https://lakemedelsboken.se/kapitel/gynekologi/sjukdomar_och_lakemedel_under_graviditet_och_amning.html#i1-2_24 [accessed 02 01 2023].
Langhoff-Roos, J., Krebs, L., Klungsoyr, K., Bjarnadottir, R. I., Kallen, K., Tapper, A. M., et al. (2014). The Nordic medical birth registers--a potential goldmine for clinical research. Acta Obstet. Gynecol. Scand. 93 (2), 132–137. doi:10.1111/aogs.12302
Laugesen, K., Ludvigsson, J. F., Schmidt, M., Gissler, M., Valdimarsdottir, U. A., Lunde, A., et al. (2021). Nordic health registry-based research: A review of health care systems and key registries. Clin. Epidemiol. 13, 533–554. doi:10.2147/clep.S314959
Magnus, M. C., Karlstad, O., Haberg, S. E., Nafstad, P., Davey Smith, G., and Nystad, W. (2016). Prenatal and infant paracetamol exposure and development of asthma: The Norwegian mother and child cohort study. Int. J. Epidemiol. 45 (2), 512–522. doi:10.1093/ije/dyv366
Mahic, M., Hernandez-Diaz, S., Wood, M., Kieler, H., Odsbu, I., Nørgaard, M., et al. (2020). In utero opioid exposure and risk of infections in childhood: A multinational nordic cohort study. Pharmacoepidemiol Drug Saf. 29, 1596–1604. doi:10.1002/pds.5088
Malek, A., and Mattison, D. R. (2011). Drugs and medicines in pregnancy: The placental disposition of opioids. Curr. Pharm. Biotechnol. 12 (5), 797–803. doi:10.2174/138920111795470859
Muller, A. E., Clausen, T., Sjogren, P., Odsbu, I., and Skurtveit, S. (2019). Prescribed opioid analgesic use developments in three Nordic countries, 2006-2017. Scand. J. Pain 19 (2), 345–353. doi:10.1515/sjpain-2018-0307
Nørgaard, M., Nielsson, M. S., and Heide-Jørgensen, U. (2015). Birth and neonatal outcomes following opioid use in pregnancy: A Danish population-based study. Subst. Abuse 9 (2), 5–11. doi:10.4137/sart.S23547
Norsk legemiddelbok (2019). Graviditet og legemidler. Available from: https://www.legemiddelhandboka.no/G7/Graviditet_og_legemidler [accessed 02.01.2023].
Olin, A., Henckel, E., Chen, Y., Lakshmikanth, T., Pou, C., Mikes, J., et al. (2018). Stereotypic immune system development in newborn children. Cell 174 (5), 1277–1292. doi:10.1016/j.cell.2018.06.045
Pecoraro, V., Banzi, R., Cariani, E., Chester, J., Villa, E., D'Amico, R., et al. (2019). New direct-acting antivirals for the treatment of patients with hepatitis C virus infection: A systematic review of randomized controlled trials. J. Clin. Exp. Hepatol. 9 (4), 522–538. doi:10.1016/j.jceh.2018.07.004
Plein, L. M., and Rittner, H. L. (2018). Opioids and the immune system - friend or foe. Br. J. Pharmacol. 175 (14), 2717–2725. doi:10.1111/bph.13750
R Core Team (2020). R: A language and environment for statistical computing. R foundation for statistical computing, Available at: https://www.R-project.org/
Sedgh, G., Singh, S., and Hussain, R. (2014). Intended and unintended pregnancies worldwide in 2012 and recent trends. Stud. Fam. Plann 45 (3), 301–314. doi:10.1111/j.1728-4465.2014.00393.x
Selmer, R., Haglund, B., Furu, K., Andersen, M., Norgaard, M., Zoega, H., et al. (2016). Individual-based versus aggregate meta-analysis in multi-database studies of pregnancy outcomes: The nordic example of selective serotonin reuptake inhibitors and venlafaxine in pregnancy. Pharmacoepidemiol Drug Saf. 25 (10), 1160–1169. doi:10.1002/pds.4033
Serebrisky, D., and Wiznia, A. (2019). Pediatric asthma: A global epidemic. Ann. Glob. Health 85 (1), 6. doi:10.5334/aogh.2416
Shaheen, S. O., Lundholm, C., Brew, B. K., and Almqvist, C. (2019). Prescribed analgesics in pregnancy and risk of childhood asthma. Eur. Respir. J. 53 (5), 1801090. doi:10.1183/13993003.01090-2018
Stephansson, O., Granath, F., Svensson, T., Haglund, B., Ekbom, A., and Kieler, H. (2011). Drug use during pregnancy in Sweden - assessed by the prescribed drug register and the medical birth register. Clin. Epidemiol. 3, 43–50. doi:10.2147/clep.s16305
Sujan, A. C., Quinn, P. D., Rickert, M. E., Wiggs, K. K., Lichtenstein, P., Larsson, H., et al. (2019). Maternal prescribed opioid analgesic use during pregnancy and associations with adverse birth outcomes: A population-based study. PLoS Med. 16 (12), e1002980. doi:10.1371/journal.pmed.1002980
The Norwegian Directorate of Health (2022). Description of the Norwegian control and payment of health reimbursements database (KUHR). Available from: https://helsedata.no/en/forvaltere/norwegian-directorate-of-health/norwegian-control-and-payment-of-health-reimbursements-database-kuhr/ [accessed 16.09.2022].
Vallejo, R., de Leon-Casasola, O., and Benyamin, R. (2004). Opioid therapy and immunosuppression: A review. Am. J. Ther. 11 (5), 354–365. doi:10.1097/01.mjt.0000132250.95650.85
WHO (2021a). ATC classification index with DDDs 2022. WHO collaborating centre for drug statistics methodology, Oslo, Norway. Available from: https://www.whocc.no/atc_ddd_index_and_guidelines/atc_ddd_index/ [accessed 10.02.2022].
WHO (2021b). Guidelines for ATC classification and DDD assignment. Oslo, Norway: WHO Collaborating Centre for Drug Statistics Methodology.
WHO (1992 ). International statistical classification of diseases and related health problems (ICD-10), 10th revision. Geneva, Switzerland. Available from: https://icd.who.int/browse10/2019/en [accessed 10.02.2022].
WONCA (1998). International classification of primary care (ICPC-2). 2nd edition. Oxford: Oxford University Press.
Keywords: opioids, childhood asthma, pregnancy, prenatal exposure, observational study
Citation: Odsbu I, Handal M, Hjellvik V, Hernandez-Diaz S, Kieler H, Nørgaard M, Skurtveit S, Esen BÖ and Mahic M (2023) Prenatal opioid exposure and risk of asthma in childhood: a population-based study from Denmark, Norway, and Sweden. Front. Pharmacol. 14:1056192. doi: 10.3389/fphar.2023.1056192
Received: 28 September 2022; Accepted: 18 April 2023;
Published: 04 May 2023.
Edited by:
Anick Bérard, Montreal University, CanadaReviewed by:
Nhung Trinh, University of Oslo, NorwayCopyright © 2023 Odsbu, Handal, Hjellvik, Hernandez-Diaz, Kieler, Nørgaard, Skurtveit, Esen and Mahic. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ingvild Odsbu, aW5ndmlsZC5vZHNidUBmaGkubm8=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.