 Qian Zhao
Qian Zhao Wen-jia Wang1
Wen-jia Wang1 Jing-bo Zhai
Jing-bo Zhai Yun-hui Hu
Yun-hui Hu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol. , 26 September 2022
Sec. Ethnopharmacology
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.959184
Background: Helicobacter pylori (H. pylori) infection is one of the most common chronic bacterial infections worldwide. The resistance of H. pylori to antibiotics may increase the risk of treatment failure. Complementary and alternative regimens are still needed. This study aimed to critically assess the efficacy and safety of Jinghua Weikang capsule (JWC) for H. pylori eradication.
Materials and methods: PubMed, Embase, Web of Science, Cochrane library, China National Knowledge Infrastructure, Wanfang Digital Periodicals, and Chinese Science and Technology Periodicals database were searched from inception to April 2022. Randomized controlled trials (RCTs) comparing a combination of JWC and conventional treatments with conventional treatments alone or combined with a placebo for H. pylori eradication were considered for inclusion. The primary outcome was H. pylori eradication rate. The meta-analysis and trial sequential analysis (TSA) were conducted where possible.
Results: A total of 34 studies were included in the statistical analysis. A pooled result showed that JWC with the duration of 2 weeks combined with the triple/quadruple therapy could significantly increase the H. pylori eradication rate compared with the triple/quadruple therapy alone (RR: 1.13, 95% CI: 1.05 to 1.21, p = 0.0008). However, the evidence of benefit was not confirmed by TSA. Another pooled result showed that JWC with the duration of 4 weeks combined with the triple/quadruple therapy could significantly increase the H. pylori eradication rate compared with the triple/quadruple therapy alone (RR: 1.21, 95% CI: 1.15 to 1.27, p < 0.00001). The evidence of benefit was confirmed by TSA. There were no statistically significant differences in the incidence of adverse reactions between the two groups.
Conclusion: The present study suggests that JWC with the duration of 4 weeks can significantly improve the H. pylori eradication rate and should be considered as a complementary treatment to conventional regimens for H. pylori eradication. However, more high-quality RCTs are still needed to confirm these findings.
Helicobacter pylori (H. pylori) belongs to gram-negative bacteria (IARC Working Group on the Evaluation of Carcinogenic Risks to Humans, 2012). H. pylori infection is one of the most common chronic bacterial infections worldwide (Randel, 2018). More than 50% of the population is infected by H. pylori in the world. However, the prevalence of H. pylori infection varies across regions and countries (Hooi et al., 2017). H. pylori infection may be associated with multiple factors, such as socioeconomic status and health care resources (Hooi et al., 2017). It may contribute to some gastrointestinal diseases, such as gastritis and peptic ulcer (Malfertheiner et al., 2007; Malfertheiner et al., 2017). H. pylori has been classified as carcinogenic to humans by the International Agency for Research on Cancer (IARC Working Group on the Evaluation of Carcinogenic Risks to Humans, 2012). It can increase the risk of gastric cancer (Torre et al., 2015; Machlowska et al., 2020). However, a systematic review has shown that the incidence of gastric cancer can be significantly reduced by eradicating H. pylori (Lee et al., 2016).
Many drugs can be used for H. pylori eradication, such as proton pump inhibitors (PPIs), clarithromycin, amoxicillin, and metronidazole. Multiple combinations of these drugs, such as clarithromycin triple therapy and bismuth quadruple therapy, have been recommended for eradicating H. pylori according to practice guidelines from the American College of Gastroenterology (Chey et al., 2017). A recent systematic review showed that the pooled prevalence rate of H. pylori resistance to clarithromycin, metronidazole, or levofloxacin was more than 15% (Savoldi et al., 2018). It is noteworthy that the resistance of H. pylori to antibiotics may increase the risk of treatment failure (Chey et al., 2017; Shiotani et al., 2017). However, the development of new antibiotics has not met the needs for gram-negative organism eradication at present (Laxminarayan et al., 2020). Therefore, complementary and alternative regimens are still needed (Savoldi et al., 2018).
Traditional Chinese medicine (TCM) has been attracting attention for H. pylori eradication (Li et al., 2021a; Li et al., 2021b; Zhong et al., 2022). Jinghua Weikang capsule (JWC) as a specific TCM is composed of Dysphania ambrosioides (L.) Mosyakin & Clemants and Adina pilulifera (Lam.) Franch. ex Drake described in Table 1 (Chen, 2005; Zhu et al., 2012; Shi et al., 2018). Some randomized controlled trials (RCTs) have investigated the efficacy of JWC for H. pylori eradication (Zhou, 2008; Zhang, 2012a; Bai, 2012; Zhang, 2012b; Zhang Y., 2013a). The results showed that JWC might be beneficial for H. pylori eradication. However, these trials have a relatively small sample size and have been not comprehensively searched and combined to increase the power and improve the precision of the estimated intervention effects due to the lack of a high-quality systematic review on this topic. Therefore, this systematic review was conducted to critically assess the efficacy and safety of JWC for H. pylori eradication.
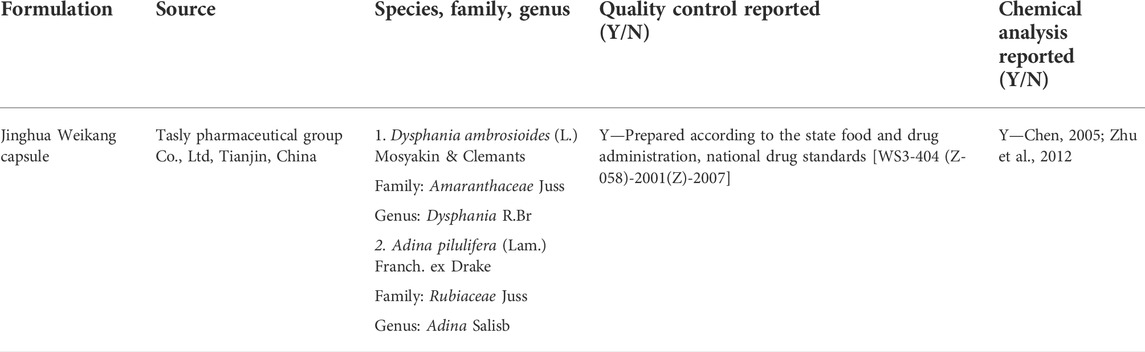
TABLE 1. Main components of the Jinghua Weikang capsule.
This study was registered on PROSPERO (No. CRD42022315488) available from: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022315488. It was conducted following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement (Page et al., 2021).
RCTs were considered for inclusion, regardless of publication date and language. Abstracts, letters, and comments were deleted.
H. pylori-infected patients were included, regardless of age, gender, race, or nationality. Gastrointestinal diseases, such as gastritis and peptic ulcer, were unlimited because they may be associated with H. pylori infection. H. pylori infection should be tested by internationally recognized methods, such as endoscopic biopsy and a urea breath test (Randel, 2018).
A combination of JWC and conventional treatments was used in the experimental group. Comparator interventions included conventional treatments alone or combined with a placebo. Dosage, frequency, and duration were unlimited. Conventional treatments refer to regimens recommended for H. pylori eradication by clinical guidelines, such as clarithromycin triple therapy and bismuth quadruple therapy (Randel, 2018).
The primary outcome was H. pylori eradication rate. The secondary outcomes included H. pylori recurrence rate, cure rate, response rate, and incidence of adverse reactions (such as nausea, diarrhea, dizziness, and constipation). The cure rate was expressed as a percentage of the number of well-healed patients with gastritis or peptic ulcer divided by the total number of patients in a certain group. The cure was defined as the disappearance of clinical symptoms associated with gastritis or peptic ulcer. The response rate was expressed as a percentage of the number of patients meeting the “response” standard divided by the total number of patients in a certain group. The response was defined as more than 50% reduction of peptic ulcer area.
PubMed, Embase, Web of Science, Cochrane library, China National Knowledge Infrastructure, Wanfang Digital Periodicals, and Chinese Science and Technology Periodicals database were searched from inception to April 2022 independently by two reviewers (J. Zhai and Q. Zhao). The search terms included (“Helicobacter pylori” OR “H. pylori” OR “Helicobacter infection” OR Hp) AND (Jinghuaweikang OR “Jinghua weikang” OR “Jing Hua Wei Kang”). The detailed search strategies are available in Supplementary Material. Some clinical trial registry platforms (e.g., ClinicalTrials.gov, World Health Organization International Clinical Trials Registry platform, and Chinese Clinical Trial Registry) and references of eligible studies were also searched. Publication date and language were unlimited.
Potentially eligible studies were collected from the comprehensive literature search and imported into EndNote software to remove duplicate studies. Then, two reviewers (J. Zhai and Q. Zhao) independently deleted ineligible studies by checking titles and abstracts according to the inclusion and exclusion criteria. Full texts of the remaining studies were read to identify included studies. The process of screening eligible studies was presented by the PRISMA flow diagram. Disagreements were handled in consultation with a third reviewer (Y. Hu).
The important data were extracted and imported into Excel software by two authors (J. Zhai and Q. Zhao) independently. They included characteristics of included studies (first author, publication year, country, sample size, design), patients (age, gender, race, nationality), interventions (type, dosage, frequency, duration), and outcomes (primary and secondary outcomes). The information on the risk of bias assessment (randomization, allocation, blinding, loss to follow-up) was also extracted synchronously.
The risk of bias was assessed using the Cochrane “risk of bias” tool (Higgins et al., 2022). It can be used to investigate some important biases in clinical trials, such as selection bias, performance bias, detection bias, attrition bias, and reporting bias. The risk of bias was judged to be low, high, or unclear against the judgment of two reviewers (J. Zhai and Q. Zhao) independently. The quality of evidence was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system. Disagreements were resolved by consensus or consultation with a third author (Y. Hu).
A risk ratio (RR) with 95% confidence intervals (CIs) was used to estimate the effect of the dichotomous variables. The meta-analysis with the random-effect model was conducted by Review Manager 5.4 software. p < 0.05 indicated a statistically significant difference between the two groups. Subgroup analyses were conducted based on control interventions (triple and quadruple therapy) and types of diseases (gastritis and peptic ulcer), if possible. Traditional meta-analysis may lead to the falsely positive or falsely negative conclusions because of sparse data and repeated testing of significance (Wetterslev et al., 2017). Trial sequential analysis (TSA) can be used to evaluate if the evidence from the meta-analysis is sufficiently reliable based on some important parameters (Wetterslev et al., 2008; Thorlund et al., 2009). For the primary outcome, TSA was conducted with a relative risk reduction (RRR) of 10%, type I error of 5% (two-sided), and type II error of 20% (a power of 80%) according to previous studies (Zhang et al., 2015; Zhou et al., 2019). Firm evidence is reached when the cumulative Z-curve crosses the trial sequential monitoring boundary or the futility boundary. Otherwise, it is insufficient to draw any firm conclusion. The publication bias was assessed for the primary outcome by Stata 16 software if the meta-analysis included more than 10 studies.
A total of 479 potentially eligible studies were identified from the initial search. Two hundred and thirty-three duplicate studies were removed using EndNote software. One hundred and ninety-eight irrelevant studies were deleted by checking the titles and abstracts. After reading full texts of the remaining records, 34 studies were included in the statistical analysis (Zhou, 2008; Zhang, 2012a; Bai, 2012; Zhang, 2012b; Zhang, 2013a; Zhang., 2013b; Shi and Sun, 2014; Lin, 2015; Wang and Han, 2015; Zhao, 2015; Chai, 2016; Deng, 2016; Lin, 2016; Xu et al., 2016; Su and Wu, 2017; Tao et al., 2017; Wang, 2018a; Wang, 2018b; Chen, 2018; Zhang et al., 2018; Zhi and Jiao, 2018; Dai and Cheng, 2019; Liu, 2019; Niu, 2019; Xu and Yu, 2019; Zhu, 2019; Cheng et al., 2020; Hang, 2020; Yao et al., 2020; Zheng, 2020; Cen, 2021; Wang et al., 2021; Xiong et al., 2021; Zhu, 2021). The process of screening eligible studies is presented in Figure 1.
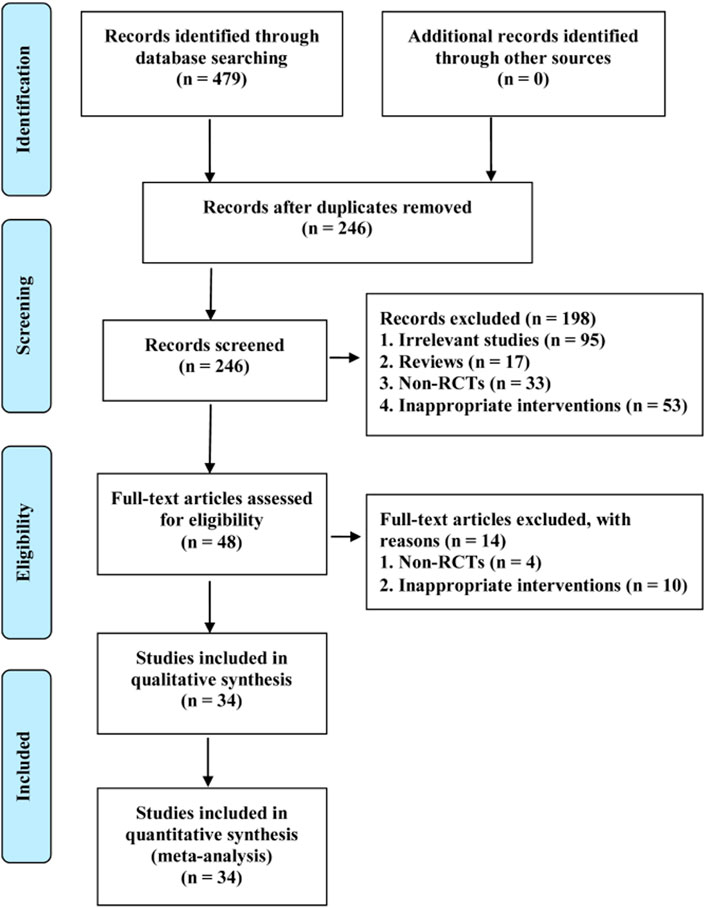
FIGURE 1. PRISMA flow diagram of study retrieval and selection.
The characteristics of the included studies are summarized in Table 2. The included studies involving 3920 patients were published between 2008 and 2021. The sample size ranged from 30 to 138 in the experimental group and 30 to 142 in the control group. JWC plus the triple therapy was compared with the triple therapy alone in 24 trials (Zhou, 2008; Zhang, 2012a; Bai, 2012; Zhang, 2012b; Zhang, 2013a; Zhang, 2013b; Shi and Sun, 2014; Lin, 2015; Wang and Han, 2015; Zhao, 2015; Chai, 2016; Deng, 2016; Lin, 2016; Xu et al., 2016; Su and Wu, 2017; Tao et al., 2017; Wang, 2018a; Wang, 2018b; Zhi and Jiao, 2018; Liu, 2019; Niu, 2019; Cheng et al., 2020; Cen, 2021; Xiong et al., 2021). One trial compared JWC plus the triple therapy with the triple therapy plus placebo (Dai and Cheng, 2019). JWC plus the quadruple therapy was compared with the quadruple therapy alone in nine studies (Chen, 2018; Zhang et al., 2018; Xu and Yu, 2019; Zhu, 2019; Hang, 2020; Yao et al., 2020; Zheng, 2020; Wang et al., 2021; Zhu, 2021). The duration of JWC treatment ranged from 10 days to 8 weeks. Patients with gastritis were enrolled in 14 trials (Bai, 2012; Lin, 2015; Deng, 2016; Xu et al., 2016; Tao et al., 2017; Wang, 2018b; Chen, 2018; Zhang et al., 2018; Dai and Cheng, 2019; Liu, 2019; Hang, 2020; Zheng, 2020; Wang et al., 2021; Zhu, 2021). Patients with peptic ulcer were included in 19 trials (Zhou, 2008; Zhang, 2012a; Zhang, 2012b; Zhang, 2013a; Zhang, 2013b; Shi and Sun, 2014; Wang and Han, 2015; Zhao, 2015; Chai, 2016; Su and Wu, 2017; Wang, 2018a; Chen, 2018; Zhi and Jiao, 2018; Niu, 2019; Xu and Yu, 2019; Zhu, 2019; Cheng et al., 2020; Cen, 2021; Xiong et al., 2021). Two trials recruited patients with gastritis or peptic ulcer (Lin, 2016; Yao et al., 2020). Thirteen studies reported adverse reactions (Bai, 2012; Shi and Sun, 2014; Wang and Han, 2015; Chai, 2016; Wang, 2018b; Liu, 2019; Xu and Yu, 2019; Cheng et al., 2020; Yao et al., 2020; Zheng, 2020; Wang et al., 2021; Xiong et al., 2021; Zhu, 2021).
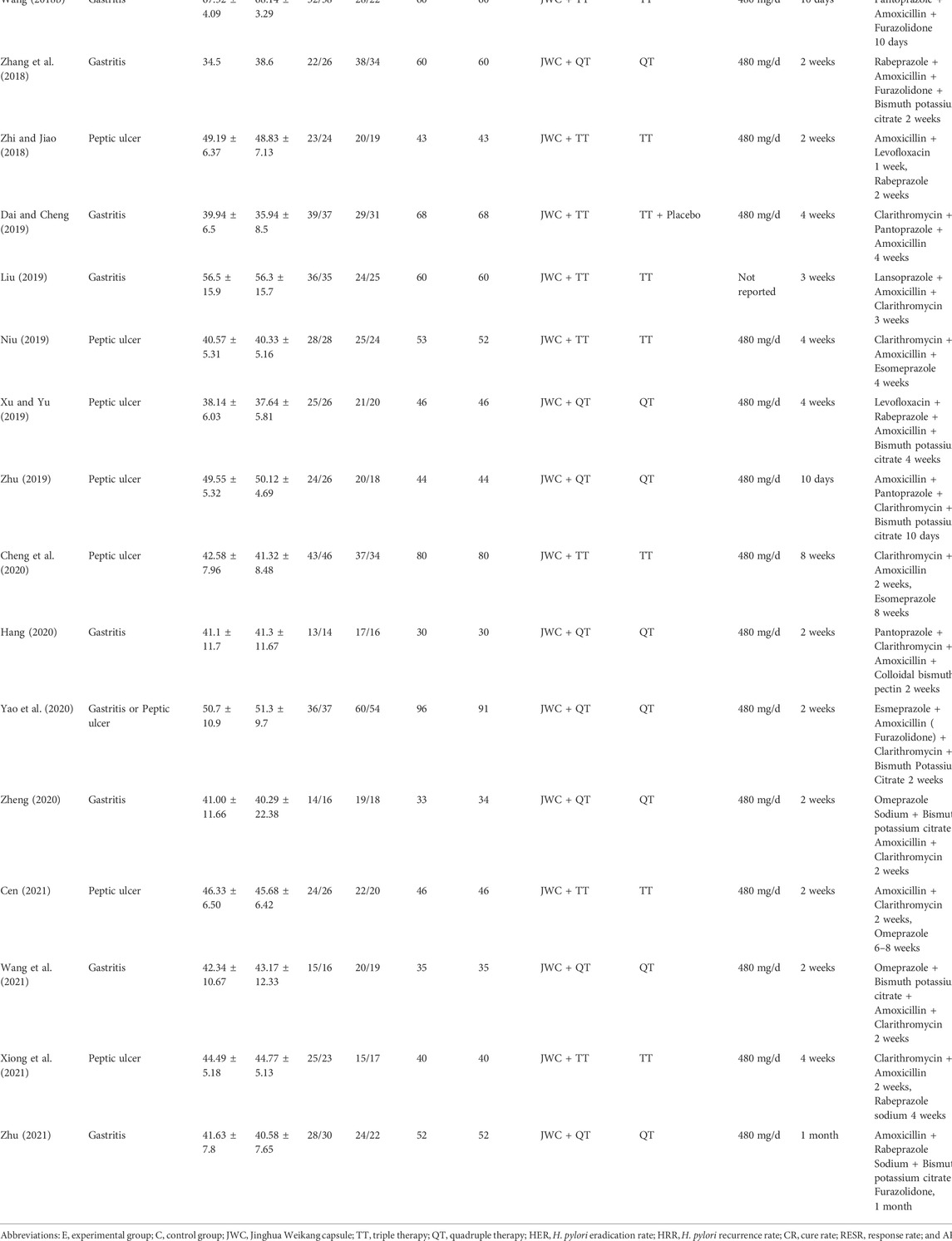
TABLE 2. Characteristics of included studies.
The results of the risk of bias assessment are presented in Figure 2 and Figure 3. Eleven studies had a low risk of bias for random sequence generation items because they reported specific methods of random sequence generation. Attrition bias was classified as a low level for all included studies because of complete outcome data. The risk of bias for allocation concealment items, performance bias, and detection bias for all included studies was graded as unclear levels due to the lack of sufficient information.
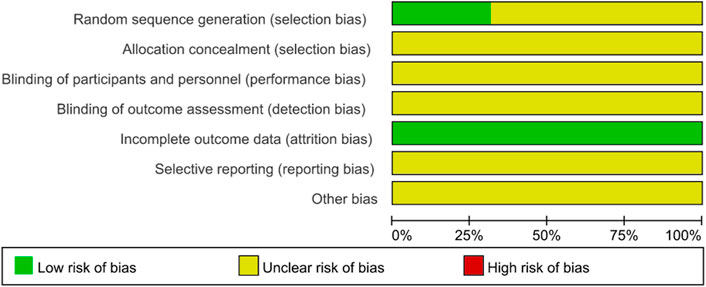
FIGURE 2. Risk of bias graph.
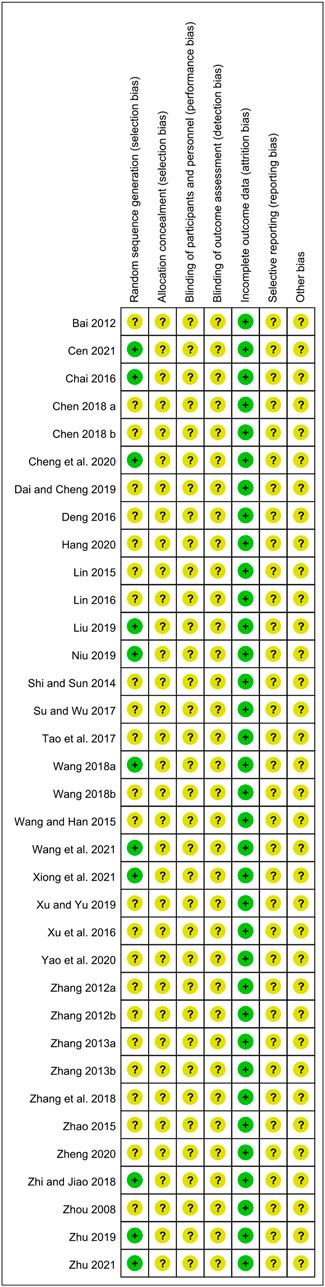
FIGURE 3. Risk of bias summary.
A total of 12 RCTs evaluated the H. pylori eradication rate after JWC treatment with the duration of 2 weeks combined with the triple or quadruple therapy (Lin, 2015; Zhao, 2015; Chai, 2016; Chen, 2018; Zhang et al., 2018; Zhi and Jiao, 2018; Hang, 2020; Yao et al., 2020; Zheng, 2020; Cen, 2021; Wang et al., 2021). A pooled result showed that the H. pylori eradication rate in JWC combined with the triple or quadruple therapy group was statistically higher than that in the triple or quadruple therapy alone group (N = 12, RR: 1.13, 95% CI: 1.05 to 1.21, p = 0.0008, Figure 4). The result from TSA showed that the cumulative Z-curve crossed the conventional boundary for benefit in Figure 5. However, it did not cross the trial sequential monitoring boundary for benefit. This means that firm evidence is not reached and larger-scale trials are still needed. The publication bias might be found because the Z value is equal to 4.26 and p-value is less than 0.0001 based on the Harbord test.
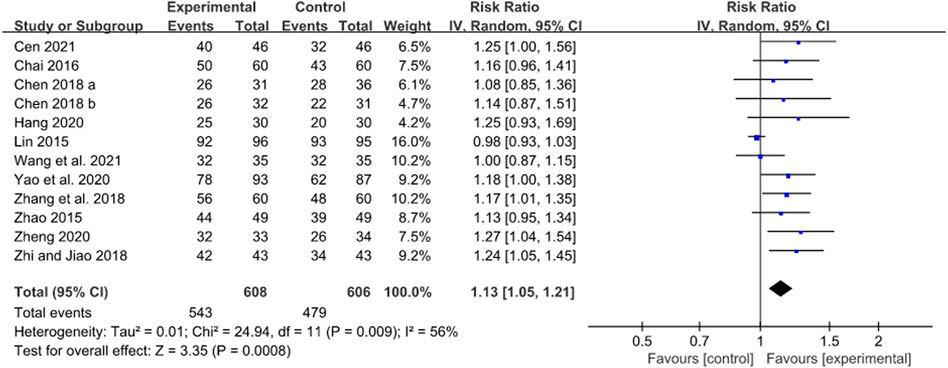
FIGURE 4. Forest plot of H. pylori eradication rate after JWC with the duration of 2 weeks.
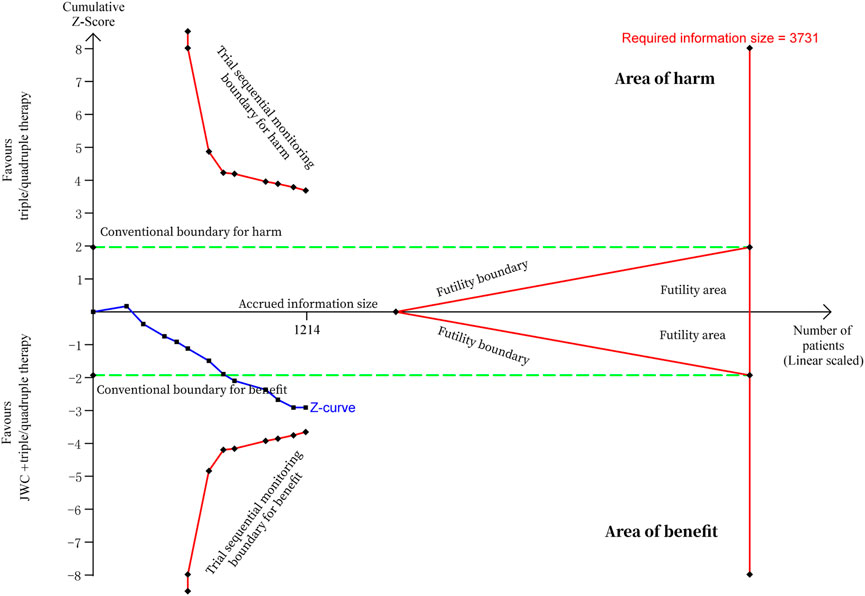
FIGURE 5. Trial sequential analysis of H. pylori eradication rate after JWC with the duration of 2 weeks.
Subgroup analyses were conducted based on control interventions (triple and quadruple therapy) and types of diseases (gastritis and peptic ulcer). There was no statistically significant difference in H. pylori eradication rate between JWC combined with the triple therapy group and the triple therapy alone group (N = 5, RR: 1.13, 95% CI: 1.00 to 1.27, p = 0.06). Furthermore, a RCT enrolling patients with gastritis reported a similar result (RR: 0.98, 95% CI: 0.93 to 1.03, p = 0.41) (Lin, 2015). However, in patients with peptic ulcer, H. pylori eradication rate was statistically higher after JWC combined with the triple therapy compared with the triple therapy alone (N = 4, RR: 1.19, 95% CI: 1.09 to 1.30, p = 0.0002). A pooled result showed that JWC combined with the quadruple therapy significantly increased the H. pylori eradication rate compared with the quadruple therapy alone (N = 7, RR: 1.13, 95% CI: 1.06 to 1.22, p = 0.0004). A similar result was found in patients with gastritis (N = 5, RR: 1.13, 95% CI: 1.03 to 1.24, p = 0.008) and not in patients with peptic ulcer (N = 1, RR: 1.08, 95% CI: 0.85 to 1.36, p = 0.53).
Two RCTs reported the H. pylori eradication rate, in which patients took JWC for 3 weeks (Wang, 2018a; Liu, 2019). A pooled result showed that H. pylori eradication rate was significantly increased after JWC combined with the triple therapy compared with the triple therapy alone (N = 2, RR: 1.21, 95% CI: 1.08 to 1.36, p = 0.001). Similar findings were also identified in patients with gastritis (N = 1, RR: 1.22, 95% CI: 1.04 to 1.42, p = 0.01) and peptic ulcer (N = 1, RR: 1.20, 95% CI: 1.01 to 1.43, p = 0.04).
Thirteen RCTs with the JWC treatment for 4 weeks reported the H. pylori eradication rate (Zhou, 2008; Zhang, 2012a; Bai, 2012; Zhang, 2012b; Zhang, 2013a; Zhang, 2013b; Shi and Sun, 2014; Lin, 2016; Su and Wu, 2017; Tao et al., 2017; Niu, 2019; Xu and Yu, 2019; Xiong et al., 2021). A pooled result showed that JWC combined with the triple or quadruple therapy could significantly improve the H. pylori eradication rate compared with the triple or quadruple therapy alone (N = 13, RR: 1.21, 95% CI: 1.15 to 1.27, p < 0.00001, Figure 6). The result from TSA showed that the cumulative Z-curve crossed both the conventional boundary for the benefit and the trial sequential monitoring boundary for the benefit in Figure 7. This means that firm evidence is reached and no larger-scale trials are needed. However, the publication bias might be found because the Z value is equal to 2.07 and the p value is equal to 0.0382 based on the Harbord test.
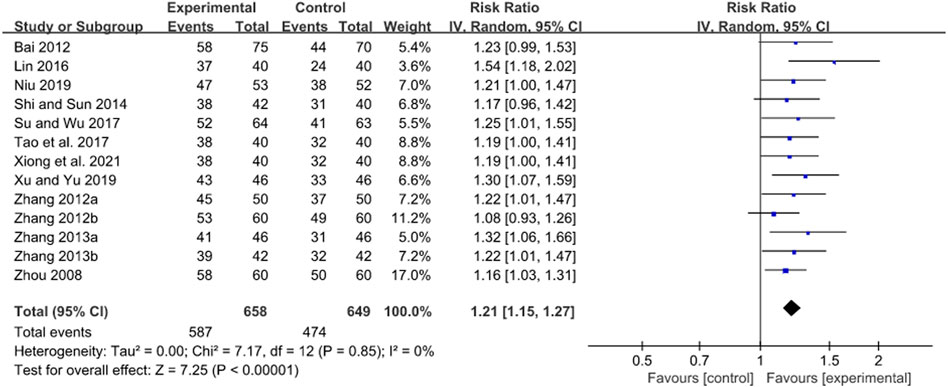
FIGURE 6. Forest plot of H. pylori eradication rate after JWC with the duration of 4 weeks.
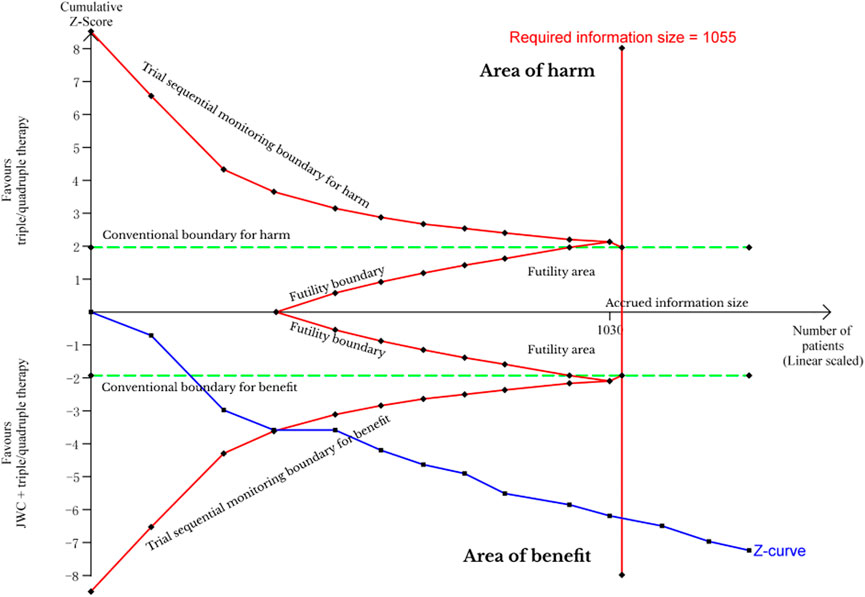
FIGURE 7. Trial sequential analysis of H. pylori eradication rate after JWC with the duration of 4 weeks.
Subgroup analyses were conducted based on control interventions (triple and quadruple therapy) and types of diseases (gastritis and peptic ulcer). A pooled result showed a greater increase in H. pylori eradication rate after JWC combined with the triple therapy compared with the triple therapy alone (N = 12, RR: 1.20, 95% CI: 1.14 to 1.26, p < 0.00001). Similar results were also found in patients with gastritis (N = 2, RR: 1.20, 95% CI: 1.05 to 1.38, p = 0.007) and peptic ulcer (N = 9, RR: 1.18, 95% CI: 1.12 to 1.25, p < 0.00001). Xu and Yu (2019) reported that JWC combined with the quadruple therapy could significantly increase the H. pylori eradication rate compared with the quadruple therapy alone in patients with peptic ulcer (RR: 1.30, 95% CI: 1.07 to 1.59, p = 0.008). Dai and Cheng (2019) reported that JWC combined with the triple therapy significantly increased the H. pylori eradication rate compared with placebo combined with the triple therapy in patients with gastritis (RR: 1.29, 95% CI: 1.09 to 1.51, p = 0.002).
Two studies reported that the H. pylori eradication rate was significantly increased after JWC combined with the triple therapy compared with the triple therapy alone in patients with gastritis, respectively (N = 1, RR: 1.29, 95% CI: 1.06 to 1.57, p = 0.010, duration of 10 days; N = 1, RR: 1.56, 95% CI: 1.23 to 1.98, p = 0.0003, duration of 15 days) (Xu et al., 2016; Wang, 2018b). Two studies showed a greater increase in H. pylori eradication rate after JWC combined with the triple therapy compared with the triple therapy alone in patients with peptic ulcer, respectively (N = 1, RR: 1.19, 95% CI: 1.09 to 1.29, p < 0.0001, duration of 6 weeks; N = 1, RR: 1.21, 95% CI: 1.02 to 1.44, p = 0.03, duration of 8 weeks) (Wang and Han, 2015; Cheng et al., 2020). Zhu (2019) found that JWC combined with the quadruple therapy could significantly increase the H. pylori eradication rate compared with the quadruple therapy alone in patients with peptic ulcer (RR: 1.30, 95% CI: 1.04 to 1.63, p = 0.02, duration of 10 days). Zhu (2021) reported that the H. pylori eradication rate was significantly increased after JWC combined with the quadruple therapy compared with the quadruple therapy alone in patients with gastritis (RR: 1.23, 95% CI: 1.04 to 1.44, p = 0.01, duration of 1 month).
Liu (2019) reported a lower H. pylori recurrence rate at 6 months after JWC treatment with the duration of 3 weeks combined with the triple therapy compared with the triple therapy alone in patients with gastritis (RR: 0.36, 95% CI: 0.14 to 0.93, p = 0.03).
The cure rate of gastritis or peptic ulcer was reported in eight trials, in which patients took JWC for 2 weeks (Lin, 2015; Zhao, 2015; Chai, 2016; Chen, 2018; Zhang et al., 2018; Hang, 2020; Cen, 2021; Wang et al., 2021). A pooled result showed that the cure rate in JWC combined with the triple or quadruple therapy group was statistically higher than that in the triple or quadruple therapy alone group (N = 8, RR: 1.34, 95% CI: 1.21 to 1.49, p < 0.00001, Figure 8).
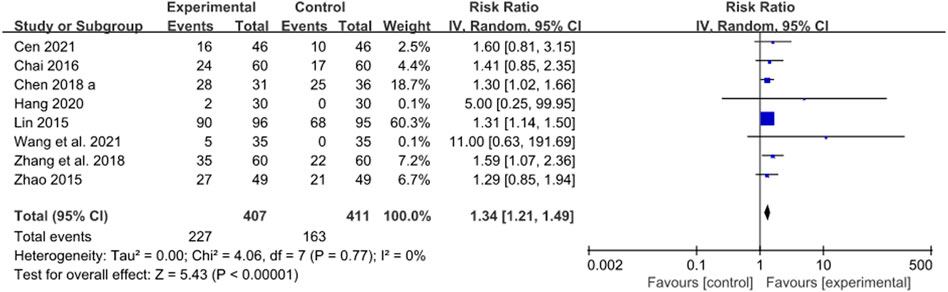
FIGURE 8. Forest plot of cure rate after JWC with the duration of 2 weeks.
Subgroup analyses were conducted based on control interventions (triple and quadruple therapy) and types of diseases (gastritis and peptic ulcer). Compared with the triple therapy alone, JWC combined with the triple therapy could significantly increase the cure rate (N = 4, RR: 1.32, 95% CI: 1.17 to 1.50, p < 0.00001). Similar results were also found in patients with gastritis (N = 1, RR: 1.31, 95% CI: 1.14 to 1.50, p = 0.0001) and peptic ulcer (N = 3, RR: 1.38, 95% CI: 1.03 to 1.84, p = 0.03). Compared with the quadruple therapy alone, JWC combined with the quadruple therapy showed a greater cure rate (N = 4, RR: 1.43, 95% CI: 1.10 to 1.86, p = 0.007). A similar result was also found in patients with peptic ulcer (N = 1, RR: 1.30, 95% CI: 1.02 to 1.66, p = 0.04) but not in patients with gastritis (N = 3, RR: 1.95, 95% CI: 0.90 to 4.24, p = 0.09).
Two studies reported a statistically significant increase in the cure rate in JWC combined with the triple therapy group compared with the triple therapy alone group in patients with gastritis (N = 2, RR: 1.28, 95% CI: 1.01 to 1.61, p = 0.04) (Deng, 2016; Liu, 2019).
Nine trials compared the cure rate of a combination of JWC with the duration of 4 weeks and the triple/quadruple therapy with the triple/quadruple therapy alone (Zhou, 2008; Zhang, 2012b; Zhang 2013a; Zhang, 2013b; Shi and Sun, 2014; Lin, 2016; Niu, 2019; Xu and Yu, 2019; Xiong et al., 2021). A pooled result showed that the cure rate was statistically higher in the JWC combined with the triple/quadruple therapy group than that in the triple/quadruple therapy alone group (N = 9, RR: 1.16, 95% CI: 1.06 to 1.27, p = 0.001, Figure 9).
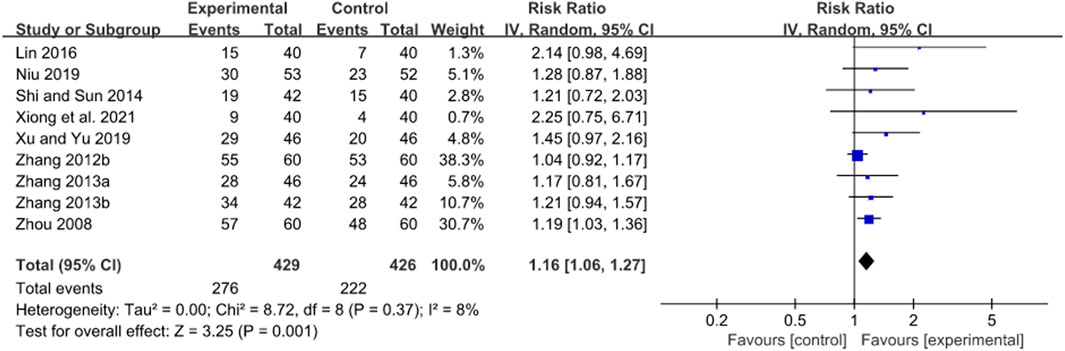
FIGURE 9. Forest plot of cure rate after JWC with the duration of 4 weeks.
Subgroup analyses were conducted based on control interventions (triple and quadruple therapy) and types of diseases (gastritis and peptic ulcer). Compared with the triple therapy alone, JWC combined with the triple therapy could significantly increase the cure rate (N = 8, RR: 1.16, 95% CI: 1.06 to 1.27, p = 0.0002). Moreover, JWC combined with the triple therapy could significantly increase the cure rate compared with the triple therapy alone in patients with peptic ulcer (N = 7, RR: 1.13, 95% CI: 1.04 to 1.22, p = 0.004). Xu and Yu (2019) reported that the cure rate in JWC combined with the quadruple therapy group was higher than that in the quadruple therapy alone group with no statistical significance in patients with peptic ulcer (RR: 1.45, 95% CI: 0.97 to 2.16, p = 0.07).
Two studies reported that the cure rate in JWC with the duration of 10 days or 15 days combined with the triple therapy group was statistically higher than that in the triple therapy alone group in patients with gastritis, respectively (N = 1, RR: 1.25, 95% CI: 1.01 to 1.54, p = 0.04, duration of 10 days; N = 1, RR: 1.58, 95% CI: 1.20 to 2.08, p = 0.0010, duration of 15 days) (Xu et al., 2016; Wang, 2018b). Another study showed that JWC combined with the triple therapy induced a greater cure rate compared with the triple therapy alone in patients with peptic ulcer (RR: 1.62, 95% CI: 1.04 to 2.53, p = 0.03, duration of 8 weeks) (Cheng et al., 2020).
A pooled result of 4 RCTs showed that JWC with the duration of 2 weeks combined with the triple therapy could significantly increase the response rate compared with the triple therapy alone in patients with peptic ulcer (RR: 1.21, 95% CI: 1.12 to 1.32, p < 0.00001, Figure 10) (Zhao, 2015; Chai, 2016; Zhi and Jiao, 2018; Cen, 2021).
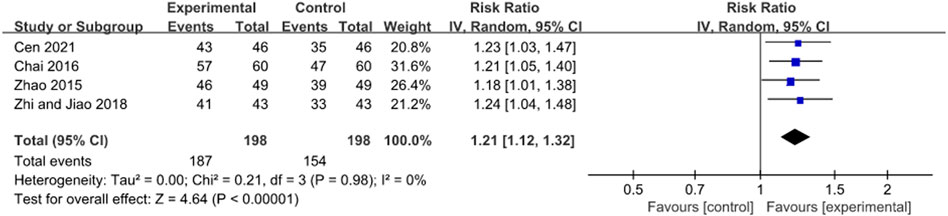
FIGURE 10. Forest plot of response rate after JWC with the duration of 2 weeks.
A pooled result of nine trials showed that the response rate in JWC combined with the triple or quadruple therapy group was statistically higher than that in the triple or quadruple therapy alone group (RR: 1.10, 95% CI: 1.03 to 1.18, p = 0.003, Figure 11) (Zhou, 2008; Zhang, 2012b; Zhang, 2013a; Zhang, 2013b; Shi and Sun, 2014; Lin, 2016; Niu, 2019; Xu and Yu, 2019; Xiong et al., 2021).
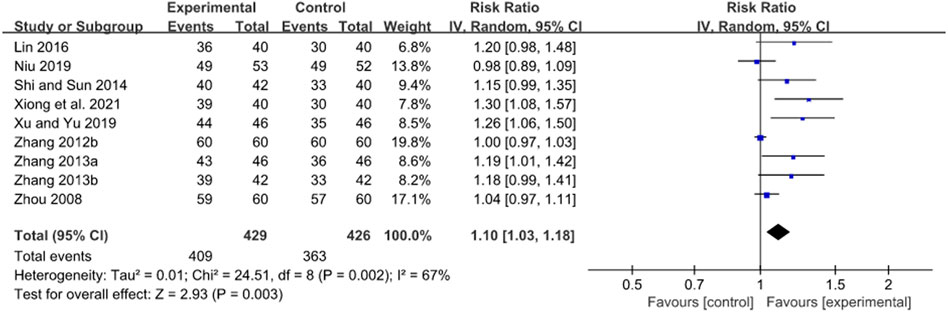
FIGURE 11. Forest plot of response rate after JWC with the duration of 4 weeks.
A subgroup analysis found that JWC combined with the triple therapy could significantly increase the response rate compared with the triple therapy alone (N = 8, RR: 1.08, 95% CI: 1.02 to 1.16, p = 0.01). Moreover, JWC combined with the triple therapy could significantly increase the response rate compared with the triple therapy alone in patients with peptic ulcer (N = 7, RR: 1.11, 95% CI: 1.02 to 1.21, p = 0.02). Xu and Yu (2019) found a greater response rate in JWC combined with the quadruple therapy group compared with the quadruple therapy alone group in patients with peptic ulcer (RR: 1.26, 95% CI: 1.06 to 1.50, p = 0.010).
Cheng et al. (2020) reported that the response rate in JWC with the duration of 8 weeks combined with the triple therapy group was statistically higher than that in the triple therapy alone group in patients with peptic ulcer (RR: 1.23, 95% CI: 1.07 to 1.42, p = 0.004).
Thirteen studies reported adverse reactions (Bai, 2012; Shi and Sun, 2014; Wang and Han, 2015; Chai, 2016; Wang, 2018b; Liu, 2019; Xu and Yu, 2019; Cheng et al., 2020; Yao et al., 2020; Zheng, 2020; Wang et al., 2021; Xiong et al., 2021; Zhu, 2021). The results of the meta-analyses showed no statistically significant differences in the incidence of nausea, diarrhea, dizziness, constipation, vomiting, and bitter taste in the mouth between the two groups in Figure 12.
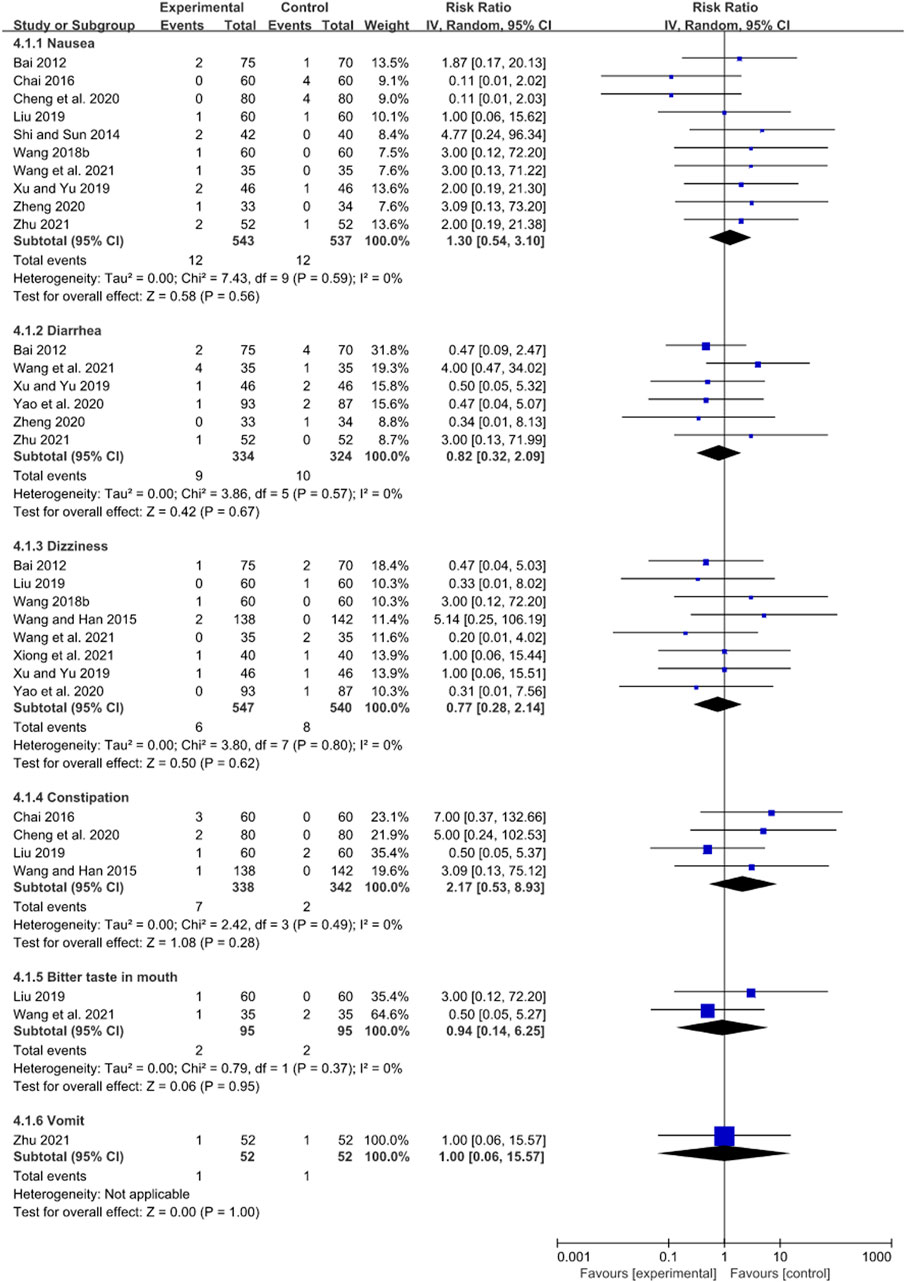
FIGURE 12. Forest plots of adverse reactions.
The quality of evidence is presented in Table 3. The quality of evidence on H. pylori eradication rate after JWC treatment with the duration of 2 and 4 weeks was graded as very low and low, respectively.
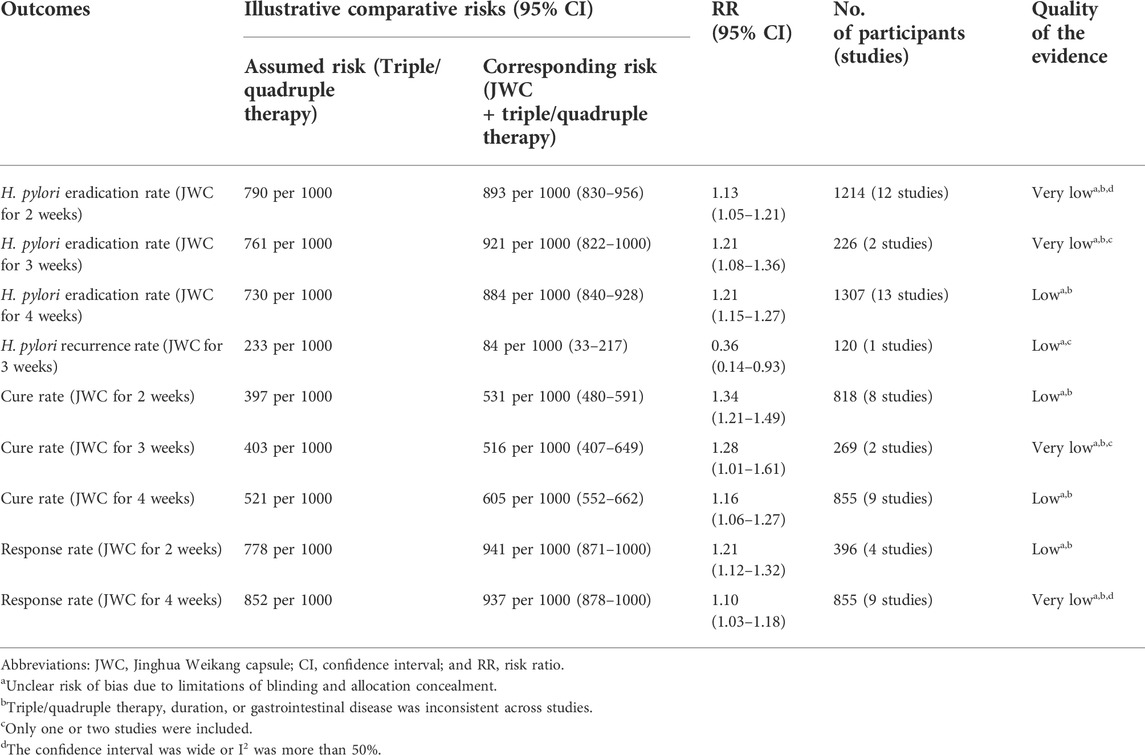
TABLE 3. GRADE quality of evidence summary table.
This systematic review critically assessed the efficacy and safety of JWC for H. pylori eradication. The main findings are summarized as follows. A pooled result showed that JWC with the duration of 2 weeks combined with the triple/quadruple therapy could significantly increase the H. pylori eradication rate compared with the triple/quadruple therapy alone. However, the evidence of benefit was not confirmed by TSA. Subgroup analyses found no statistically significant differences in H. pylori eradication rate between JWC combined with the triple therapy and the triple therapy alone in patients with gastritis and between JWC combined with the quadruple therapy and the quadruple therapy alone in patients with peptic ulcer. Another pooled result showed that JWC with the duration of 4 weeks combined with the triple/quadruple therapy could significantly increase the H. pylori eradication rate compared with the triple/quadruple therapy alone. The evidence of benefit was confirmed by TSA. Moreover, subgroup analyses also found statistically significant differences in H. pylori eradication rate between JWC combined with the triple therapy and the triple therapy alone in patients with gastritis or peptic ulcer, and between JWC combined with the quadruple therapy and the quadruple therapy alone in patients with peptic ulcer. Moreover, one study reported a statistically lower H. pylori recurrence rate at 6 months after JWC combined with the triple therapy compared with the triple therapy alone in patients with gastritis. Other results showed that JWC combined with the triple/quadruple therapy could significantly increase the cure rate of gastritis or peptic ulcer and promote peptic ulcer healing compared with the triple/quadruple therapy alone. There were no statistically significant differences in the incidence of adverse reactions between the two groups.
A combination of PPI and antibiotics is typically used for H. pylori eradication. For example, clarithromycin triple therapy and bismuth quadruple therapy are recommended according to clinical guidelines (Chey et al., 2017). However, a recent study reported an increased H. pylori resistance to antibiotics in most World Health Organization regions (Savoldi et al., 2018). The prevalence of H. pylori resistance was also high among children according to a study from Iran (Yousefi-Avarvand et al., 2018). A review reported the reduction of H. pylori eradication rate after clarithromycin triple therapy and bismuth quadruple therapy associated with antibiotic resistance (Kim et al., 2015). It poses a great challenge to the selection of treatments for H. pylori eradication. A common effort is to seek alternative antibiotics with no H. pylori resistance. However, H. pylori resistance to many conventional antibiotics has been reported (Kuo et al., 2017; Savoldi et al., 2018). There has been an increased interest in the development of new antibiotics in recent years (Tacconelli et al., 2018). However, few antibiotics have been developed successfully (Tacconelli et al., 2018). Antimicrobial susceptibility testing for H. pylori is rarely performed partly due to the lack of standardized testing methods and consensus on antibiotic resistance breakpoints (Li et al., 2022). The salvage therapy may be selected empirically after first-line therapy fails (Chey et al., 2017).
In recent years, some novel therapies have brought benefits to patients with H. pylori. Some studies reported the potential of nanotechnology for H. pylori eradication (de Souza et al., 2021; Khan et al., 2022). Nonetheless, clinical trials on this topic are still needed. Some systematic reviews showed that probiotics could be considered an adjuvant therapy for H. pylori eradication (Yu et al., 2019; Zhou et al., 2019). However, a study reported that probiotics were recommended only for patients with poor compliance to treatments (Shiotani et al., 2017). A recent review suggested that TCM herbs and their active ingredients combined with antibiotics could be considered a novel antibacterial treatment (Su et al., 2020). A systematic review showed that TCM-based therapy could be used as rescue therapy for H. pylori eradication (Zhong et al., 2022). Berberine belongs to the isoquinoline alkaloid extracted from Chinese herbal medicine. A systematic review showed that berberine combined with the standard triple therapy could significantly increase the H. pylori eradication rate (Hu et al., 2019). The main components of JWC are also extracted from Chinese herbal medicine (Shi et al., 2018). The efficacy of JWC with the duration of 4 weeks for eradicating H. pylori is confirmed by both conventional meta-analysis and TSA in the present study.
The efficacy of triple/quadruple therapy for H. pylori eradication may be dependent on the intragastric potential of hydrogen (pH) (Shiotani et al., 2017). For example, the instability of clarithromycin was reported at low pH (Erah et al., 1997). An experiment showed that JWC could significantly inhibit the secretion of gastric acid in rats (Xie and Huang, 2001). H. pylori are tolerant to multiple antibiotics possibly by forming a biofilm (Yonezawa et al., 2019; Hathroubi et al., 2020). An in vitro experiment found that volatile oil extracted from Dysphania ambrosioides (L.) Mosyakin & Clemants as the main ingredient of JWC could inhibit the formation of H. pylori biofilm (Zhang et al., 2020). A study reported that Adina pilulifera (Lam.) Franch. ex Drake as the main ingredient of JWC might prevent H. pylori from sticking to the stomach wall by competitively inhibiting the blood group antigen-binding adhesion (BabA) (Hong et al., 2021). Some experiments found that JWC could accelerate peptic ulcer healing by stimulating the secretion of nitric oxide and epidermal growth factor and reducing the endothelin level (Cao et al., 2006; Liang, 2007). Another experiment reported that JWC could inhibit H. pylori-induced inflammatory responses by regulating the nuclear factor-kappa B signaling pathway (Shi et al., 2018). The mechanisms of JWC for eradicating H. pylori and treating gastritis and peptic ulcer may be explained partly by the abovementioned evidence. Overall, the present study provides new insight into the management of H. pylori eradication. JWC can be considered a new complementary treatment to conventional regimens for H. pylori eradication.
This systematic review has some minor limitations. Due to the lack of relevant data, the long-term effect of JWC for H. pylori eradication is poorly investigated, and the efficacy of JWC versus some novel therapies for H. pylori eradication is not compared directly. The unclear risk of bias was identified in the blinding and allocation concealment item. The same triple/quadruple therapies are used between two groups in each included study. However, the specific drugs and durations of triple/quadruple therapies may be different across included studies. The heterogeneity of the meta-analyses may be partly explained by the abovementioned factors.
The present study suggests that JWC with the duration of 4 weeks can significantly improve H. pylori eradication rate and should be considered as a complementary treatment to conventional regimens for H. pylori eradication. However, more high-quality RCTs are still needed to confirm these findings.
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding authors.
J-bZ and Y-hH conceived the study. J-bZ and QZ searched databases, screened the studies, extracted the data, assessed the methodological quality, and performed the statistical analysis. All authors drafted, reviewed, and revised the manuscript. All authors have read and approved the final version of the manuscript.
QZ, W-jW, and Y-hH were employed by Cloudphar Pharmaceuticals Co., Ltd.
S-pZ and HS were as employed by The State Key Laboratory of Core Technology in Innovative Chinese Medicine, Tasly Academy, Tasly Holding Group Co., Ltd.
JS and HS were employed by Tasly Pharmaceutical Group Co., Ltd.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.959184/full#supplementary-material
Bai, M. (2012). Effects of Jinghua weikang capsules combined with the standard triple therapy in the treatment of chronic gastritis. J. Drug Eval. 9 (20), 23–25. doi:10.3969/j.issn.1672-2809.2012.20.005
Cao, M. B., Chang, X. M., Dong, L., and Ren, L. (2006). Effect of Jinghua weikang Capsule on concrescence of gastric mucosa in rats with gastric ulcer. Chin. J. New Drugs 1 (16), 1357–1359. doi:10.3321/j.issn:1003-3734.2006.16.011
Cen, Y. H. (2021). Proton pump inhibitor triple therapy combined with Jinghua Weikang Capsule in the treatment of Helicobacter pylori-positive patients with chronic peptic ulcer. Int. Med. Health Guid. News 27 (15), 2359–2362. doi:10.3760/cma.j.issn.1007-1245.2021.15.037
Chai, Y. P. (2016). Observation on the curative effect of Jinghua weikang capsule combined with triple therapy containing proton pump inhibitor in the treatment of peptic ulcer. China Med. Eng. 24 (04), 110–111. doi:10.19338/j.issn.1672-2019.2016.04.050
Chen, Q. (2005). Study on GC fingerprint of Jinghua weikang capsule. Fuzhou, China: Strait Pharmaceutical Journal 17 (1), 58–60. doi:10.3969/j.issn.1006-3765.2005.01.034
Chen, X. (2018). Clinical study on the treatment of chronic gastritis and duodenal bulb ulcer of helicobacter pylori by Jinghua weikang combined with quadruple therapy. China: Bengbu Medical College. [Master’s thesis].
Cheng, J., Yu, K. T., and Tan, H. (2020). Efficacy and safety of Jinghua weikang capsule combined with proton pump inhibitor and antibiotic in the treatment of peptic ulcer. Chin. J. Mod. Drug Appl. 14 (09), 150–151. doi:10.14164/j.cnki.cn11-5581/r.2020.09.069
Chey, W. D., Leontiadis, G. I., Howden, C. W., and Moss, S. F. (2017). ACG clinical guideline: Treatment of Helicobacter pylori infection. Am. J. Gastroenterol. 112 (2), 212–239. doi:10.1038/ajg.2016.563
Dai, M. S., and Cheng, X. H. (2019). Clinical study on Jinghua weikang soft capsules for chronic gastritis caused by Helicobacter pylori. J. New Chin. Med. 51 (11), 110–112. doi:10.13457/j.cnki.jncm.2019.11.032
de Souza, M. P. C., de Camargo, B. A. F., Spósito, L., Fortunato, G. C., Carvalho, G. C., Marena, G. D., et al. (2021). Highlighting the use of micro and nanoparticles based-drug delivery systems for the treatment of Helicobacter pylori infections. Crit. Rev. Microbiol. 47 (4), 435–460. doi:10.1080/1040841x.2021.1895721
Deng, H. H. (2016). Therapeutic effect of integrated traditional Chinese and Western Medicine for Helicobacter pylori-infected patients with atrophic gastritis. Cardiovasc. Dis. J. Integr. traditional Chin. West. Med. 4 (26), 181. doi:10.16282/j.cnki.cn11-9336/r.2016.26.140
Erah, P. O., Goddard, A. F., Barrett, D. A., Shaw, P. N., and Spiller, R. C. (1997). The stability of amoxycillin, clarithromycin and metronidazole in gastric juice: Relevance to the treatment of Helicobacter pylori infection. J. Antimicrob. Chemother. 39 (1), 5–12. doi:10.1093/jac/39.1.5
Hang, L. (2020). Clinical research on the treatment of chronic non-atrophic gastritis by Helicobacter pylori with Jinghua weikang capsule combined with cuadruple combination therapy. China: Nanjing University of Chinese Medicine. [Master’s thesis].
Hathroubi, S., Zerebinski, J., Clarke, A., and Ottemann, K. M. (2020). Helicobacter pylori biofilm confers antibiotic tolerance in part via A protein-dependent mechanism. Antibiot. (Basel) 9 (6), E355. doi:10.3390/antibiotics9060355
Higgins, J. P. T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M. J., et al. (2022). Cochrane handbook for systematic reviews of interventions version 6.3 (updated february 2022). Cochrane, 2022. Available from www.training.cochrane.org/handbook (Accessed March 15, 2022).
Hong, S. W., Yang, Y., Xu, D. L., Cao, Q. Q., Yin, H. L., Xia, Z. Y., et al. (2021). Systematic pharmacological methodology-based investigation on interventional mechanism of Jinghua weikang capsule protecting against Helicobacter pylori-induced inflammatory responses. J. Anhui Sci. Technol. Univ. 35 (02), 57–66. doi:10.19608/j.cnki.1673-8772.2017.0899
Hooi, J. K. Y., Lai, W. Y., Ng, W. K., Suen, M. M. Y., Underwood, F. E., Tanyingoh, D., et al. (2017). Global prevalence of Helicobacter pylori infection: Systematic review and meta-analysis. Gastroenterology 153 (2), 420–429. doi:10.1053/j.gastro.2017.04.022
Hu, Q., Peng, Z., Li, L., Zou, X., Xu, L., Gong, J., et al. (2019). The efficacy of berberine-containing quadruple therapy on Helicobacter pylori eradication in China: A systematic review and meta-analysis of randomized clinical trials. Front. Pharmacol. 10, 1694. doi:10.3389/fphar.2019.01694
IARC Working Group on the Evaluation of Carcinogenic Risks to Humans (2012). Biological agents. Volume 100 B. A review of human carcinogens. Switzerland: World Health Organization Press.
Khan, S., Sharaf, M., Ahmed, I., Khan, T. U., Shabana, S., Arif, M., et al. (2022). Potential utility of nano-based treatment approaches to address the risk of Helicobacter pylori. Expert Rev. anti. Infect. Ther. 20 (3), 407–424. doi:10.1080/14787210.2022.1990041
Kim, S. Y., Choi, D. J., and Chung, J. W. (2015). Antibiotic treatment for Helicobacter pylori: Is the end coming? World J. Gastrointest. Pharmacol. Ther. 6 (4), 183–198. doi:10.4292/wjgpt.v6.i4.183
Kuo, Y. T., Liou, J. M., El-Omar, E. M., Wu, J. Y., Leow, A. H. R., Goh, K. L., et al. (2017). Primary antibiotic resistance in Helicobacter pylori in the asia-pacific region: A systematic review and meta-analysis. Lancet. Gastroenterol. Hepatol. 2 (10), 707–715. doi:10.1016/s2468-1253(17)30219-4
Laxminarayan, R., Van Boeckel, T., Frost, I., Kariuki, S., Khan, E. A., Limmathurotsakul, D., et al. (2020). The lancet infectious diseases commission on antimicrobial resistance: 6 years later. Lancet. Infect. Dis. 20 (4), e51–e60. doi:10.1016/s1473-3099(20)30003-7
Lee, Y. C., Chiang, T. H., Chou, C. K., Tu, Y. K., Liao, W. C., Wu, M. S., et al. (2016). Association between Helicobacter pylori eradication and gastric cancer incidence: A systematic review and meta-analysis. Gastroenterology 150 (5), 1113–1124. e1115. doi:10.1053/j.gastro.2016.01.028
Li, H., Shen, Y., Song, X., Tang, X., Hu, R., Marshall, B. J., et al. (2022). Need for standardization and harmonization of Helicobacter pylori antimicrobial susceptibility testing. Helicobacter 27 (2), e12873. doi:10.1111/hel.12873
Li, R. J., Dai, Y. Y., Qin, C., Huang, G. R., Qin, Y. C., Huang, Y. Y., et al. (2021b). Application of traditional Chinese medicine in treatment of Helicobacter pylori infection. World J. Clin. Cases 9 (35), 10781–10791. doi:10.12998/wjcc.v9.i35.10781
Li, Y., Li, X., and Tan, Z. (2021a). An overview of traditional Chinese medicine therapy for Helicobacter pylori-related gastritis. Helicobacter 26 (3), e12799. doi:10.1111/hel.12799
Liang, W. Y. (2007). Effect of Jinghuaweikang Capsule on the levels of NO, NOS and ET in the gastric mucous of rats with gastric ulcer. China: Beijing University of Chinese Medicine. [Master’s thesis].
Lin, R. F. (2016). Clinical observation on treating 40 Helicobacter pylori-infected cases with Jinghua weikang capsule combined with Western medicine. Clin. J. Chin. Med. 8 (01), 81–83. doi:10.3969/j.issn.1674-7860.2016.01.041
Lin, S. Q. (2015). Clinical study of Jinghuaweikang capsule in the adjuvant treatment of Helicobacter pylori-positive patients with chronic gastritis. J. New Chin. Med. 47 (08), 73–74. doi:10.13457/j.cnki.jncm.2015.08.033
Liu, L. (2019). Effects of Jinghua Weikang capsule combined with triple therapy in the treatment of Helicobacter pylori-positive patients with verrucous gastritis. Chin. J. Prim. Med. Pharm. 26 (06), 641–645. doi:10.3760/cma.j.issn.1008-6706.2019.06.001
Machlowska, J., Baj, J., Sitarz, M., Maciejewski, R., and Sitarz, R. (2020). Gastric cancer: Epidemiology, risk factors, classification, genomic characteristics and treatment strategies. Int. J. Mol. Sci. 21 (11), E4012. doi:10.3390/ijms21114012
Malfertheiner, P., Megraud, F., O'Morain, C. A., Gisbert, J. P., Kuipers, E. J., Axon, A. T., et al. (2017). Management of Helicobacter pylori infection-the maastricht V/florence consensus report. Gut 66 (1), 6–30. doi:10.1136/gutjnl-2016-312288
Malfertheiner, P., Megraud, F., O'Morain, C., Bazzoli, F., El-Omar, E., Graham, D., et al. (2007). Current concepts in the management of Helicobacter pylori infection: The maastricht III consensus report. Gut 56 (6), 772–781. doi:10.1136/gut.2006.101634
Niu, L. P. (2019). Jinghua weikang capsule combined with esomeprazole triple therapy in the treatment of Helicobacter pylori-positive patients with gastric ulcer. Henan Med. Res. 28 (12), 2249–2251. CNKI:SUN:HNYX.0.2019-12-066.
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Bmj 372, n71. doi:10.1136/bmj.n71
Randel, A. (2018). H. pylori infection: ACG updates treatment Recommendations. Am. Fam. Physician 97 (2), 135–137.
Savoldi, A., Carrara, E., Graham, D. Y., Conti, M., and Tacconelli, E. (2018). Prevalence of antibiotic resistance in Helicobacter pylori: A systematic review and meta-analysis in world health organization regions. Gastroenterology 155 (5), 1372–1382. e1317. doi:10.1053/j.gastro.2018.07.007
Shi, Y. Y., and Sun, J. (2014). Clinical observation of Jinghua weikang capsule for peptic ulcerCNKI:SUN:YCGC. China Med. Eng. 22 (12), 114. 10.2014-12-093.
Shi, Z. M., Ye, H., Yu, J., Zhang, X., Cheng, H., and Li, J. (2018). Jinghua Weikang capsule protects against Helicobacter pylori-induced inflammatory responses via the nuclear factor-kappa B signaling pathway. J. Traditional Chin. Med. 38 (3), 366–372. doi:10.1016/j.jtcm.2018.03.001
Shiotani, A., Lu, H., Dore, M. P., and Graham, D. Y. (2017). Treating Helicobacter pylori effectively while minimizing misuse of antibiotics. Cleve. Clin. J. Med. 84 (4), 310–318. doi:10.3949/ccjm.84a.14110
Su, T., Qiu, Y., Hua, X., Ye, B., Luo, H., Liu, D., et al. (2020). Novel opportunity to reverse antibiotic resistance: To explore traditional Chinese medicine with potential activity against antibiotics-resistance bacteria. Front. Microbiol. 11, 610070. doi:10.3389/fmicb.2020.610070
Su, Y. S., and Wu, F. (2017). Efficacy of Jinghua weikang combined with triple therapy on Helicobacter pylori-positive patients with peptic ulcer. China Med. Pharm. 7 (21), 215–217. doi:10.3969/j.issn.2095-0616.2017.21.064
Tacconelli, E., Carrara, E., Savoldi, A., Harbarth, S., Mendelson, M., Monnet, D. L., et al. (2018). Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet. Infect. Dis. 18 (3), 318–327. doi:10.1016/s1473-3099(17)30753-3
Tao, H. Y., Lu, Y., and Huang, X. Y. (2017). Clinical observation of Jinghuaweikang capsule in the treatment of Helicobacter pylori-positive patients with chronic gastritis. Shanxi J. Traditional Chin. Med. 38 (02), 159–160. doi:10.3969/j.issn.1000-7369.2017.02.009
Thorlund, K., Devereaux, P. J., Wetterslev, J., Guyatt, G., Ioannidis, J. P., Thabane, L., et al. (2009). Can trial sequential monitoring boundaries reduce spurious inferences from meta-analyses? Int. J. Epidemiol. 38 (1), 276–286. doi:10.1093/ije/dyn179
Torre, L. A., Bray, F., Siegel, R. L., Ferlay, J., Lortet-Tieulent, J., and Jemal, A. (2015). Global cancer statistics, 2012. Ca. Cancer J. Clin. 65 (2), 87–108. doi:10.3322/caac.21262
Wang, H. J. (2018a). Effect of triple therapy combined with Jinghua Weikang Capsule on improvement of duodenal ulcer symptoms and Helicobacter pylori eradication rate. Inn. Mong. Med. J. 50 (05), 596–598. doi:10.16096/J.cnki.nmgyxzz.2018.50.05.040
Wang, J. H., and Han, Y. C. (2015). Clinical analysis of Jinghua weikang capsule in the treatment of 138 patients with peptic ulcer. J. North Pharm. 12 (08), 168–169. CNKI: SUN:BFYX.0.2015-08-132.
Wang, R. X., Zhang, S. S., and Zhou, Q. (2021). The research of curative effect of patients with chronic gastritis associated with Helicobacter pylori treated by Jinghua Weikang Capsule combined with standard quadruple therapy. Chin. J. Integr. Traditional West. Med. Dig. 29 (09), 610–614. doi:10.3969/j.issn.1671-038X.2021.09.03
Wang, Y. G. (2018b). To observe the clinical efficacy of Jinghua weikang capsule combined with triple therapy in the treatment of Helicobacter pylori-infected chronic gastritis. Qinghai Med. J. 48 (12), 59–60. CNKI:SUN:QHYZ.0.2018-12-026.
Wetterslev, J., Jakobsen, J. C., and Gluud, C. (2017). Trial Sequential Analysis in systematic reviews with meta-analysis. BMC Med. Res. Methodol. 17 (1), 39. doi:10.1186/s12874-017-0315-7
Wetterslev, J., Thorlund, K., Brok, J., and Gluud, C. (2008). Trial sequential analysis may establish when firm evidence is reached in cumulative meta-analysis. J. Clin. Epidemiol. 61 (1), 64–75. doi:10.1016/j.jclinepi.2007.03.013
Xie, Z. J., and Huang, M. X. (2001). Inhibitory effect of Jinghua weikang Capsule on experimental gastric ulcer and Helicobacter pylori. Chin. J. New Drugs 1 (03), 221–223. doi:10.3321/j.issn:1003-3734.2001.03.024
Xiong, Y. F., Yuan, S. H., and Zhang, Q. H. (2021). Clinical observation of Jinghua Weikang capsules combined with Rabeprazole triple therapy in the treatment of Helicobacter pylori-related gastric ulcer. Med. Forum 25 (35), 5050–5052. doi:10.19435/j.1672-1721.2021.35.006
Xu, L. P., and Yu, H. S. (2019). Efficacy of Jinghua weikang capsule in the treatment of Helicobacter pylori-positive patients with gastric ulcer. J. Shanxi Med. Coll. Continuing Educ. 29 (04), 74–76.
Xu, Y. M., Lin, J. H., Liang, X. H., Xie, Y. H., and Cheng, W. H. (2016). Observation on the efficacy of Jinghua weikang capsule in the treatment of chronic gastritis and eradication of Helicobacter pylori. J. Intern. Intensive Med. 22 (01), 41–42. doi:10.11768/nkjwzzzz20160115
Yao, G. P., Li, Q. X., Duan, X. H., and Yin, H. K. (2020). A randomized controlled study of Jinghua weikang capsule combined with quadruple therapy in the treatment of Helicobacter pylori infection. Mod. Dig. Intervention 25 (07), 922–925. doi:10.3969/j.issn.1672-2159.2020.07.020
Yonezawa, H., Osaki, T., Hojo, F., and Kamiya, S. (2019). Effect of Helicobacter pylori biofilm formation on susceptibility to amoxicillin, metronidazole and clarithromycin. Microb. Pathog. 132, 100–108. doi:10.1016/j.micpath.2019.04.030
Yousefi-Avarvand, A., Vaez, H., Tafaghodi, M., Sahebkar, A. H., Arzanlou, M., and Khademi, F. (2018). Antibiotic resistance of Helicobacter pylori in Iranian children: A systematic review and meta-analysis. Microb. Drug Resist. 24 (7), 980–986. doi:10.1089/mdr.2017.0292
Yu, M., Zhang, R., Ni, P., Chen, S., and Duan, G. (2019). Efficacy of lactobacillus-supplemented triple therapy for H. pylori eradication: A meta-analysis of randomized controlled trials. PLoS One 14 (10), e0223309. doi:10.1371/journal.pone.0223309
Zhang, E. E., Ye, H., Jia, X. F., Huang, Q. Y., Zhang, X. Z., and Liu, Y. (2020). Effect of Chenopodium ambrosioides L. On biofilm formation of Helicobacter pylori in vitro. Chin. J. Integr. Traditional West. Med. 40 (10), 1241–1245. doi:10.7661/j.cjim.20200904.334
Zhang, H. Y. (2013a). Jinghua weikang capsule combined with triple therapy in the treatment of 46 Helicobacter pylori-positive patients with peptic ulcer. China Pharm. 22 (16), 109. doi:10.3969/j.issn.1006-4931.2013.16.062
Zhang, H. Y., Liu, J., Liu, W. P., Liu, Y., Lin, H. Y., Li, X. L., et al. (2018). Clinical observation of 60 patients with Verrucous Gastritis Treated with traditional Chinese medicine via Helicobacter pylori eradication. Mil. Med. J. Southeast China 20 (01), 70–72. doi:10.3969/j.issn.1672-271X.2018.01.016
Zhang, L. L. (2013b). Observation on the curative effect of Jinghua weikang capsule plus quadruple therapy in the treatment of peptic ulcer. Med. J. Chin. People's Health 25 (09), 11–12. doi:10.3969/j.issn.1672-0369.2013.09.001
Zhang, M. M., Qian, W., Qin, Y. Y., He, J., and Zhou, Y. H. (2015). Probiotics in Helicobacter pylori eradication therapy: A systematic review and meta-analysis. World J. Gastroenterol. 21 (14), 4345–4357. doi:10.3748/wjg.v21.i14.4345
Zhang, W. M. (2012a). Jinghua Weikang Capsule Combined with triple therapy to eradicate Helicobacter pylori in patients with gastroduodenal ulcer. Chin. J. Mod. Drug Appl. 6 (03), 65–67. doi:10.14164/j.cnki.cn11-5581/r.2012.03.070
Zhang, Y., Zhang, J., Huang, X., Zhou, X., Wu, H., and Guo, S. (2012b). Observation on the curative effect of Jinghua weikang capsule combined with triple therapy for Helicobacter pylori-positive patients with duodenal ulcer. Small 9 (16), 154–159. doi:10.1002/smll.201101695
Zhao, D., Fan, Y., Gao, F., and Yang, T. m. (2015). Curative effect of Triple therapy combined Jinghua Weikang capsule for Helicobacter pylori eradication in patients with gastric ulcer. Anal. Chim. Acta 34 (01), 131–137. doi:10.1016/j.aca.2015.06.053
Zheng, L. (2020). Clinical observation of Jinghua weikang capsule combined with bismuth agent in the treatment of Helicobacter prlori-associated aastritis. China: Hubei University of Chinese Medicine. [Master’s thesis].
Zhi, H., and Jiao, K. F. (2018). Effect of Jinghua Weikang Capsule Combined with rabeprazole triple therapy in the treatment of Helicobacter pylori positive-patients with duodenal ulcer. Henan Med. Res. 27 (19), 3523–3524. doi:10.3969/j.issn.1004-437X.2018.19.030
Zhong, M. F., Li, J., Liu, X. L., Gong, P., and Zhang, X. T. (2022). TCM-based therapy as a rescue therapy for Re-eradication of Helicobacter pylori infection: A systematic review and meta-analysis. Evid. Based. Complement. Altern. Med. 2022, 5626235. doi:10.1155/2022/5626235
Zhou, B. G., Chen, L. X., Li, B., Wan, L. Y., and Ai, Y. W. (2019). Saccharomyces boulardii as an adjuvant therapy for Helicobacter pylori eradication: A systematic review and meta-analysis with trial sequential analysis. Helicobacter 24 (5), e12651. doi:10.1111/hel.12651
Zhou, Y. (2008). Observation on the curative effect of Jinghua weikang capsule combined with triple therapy for peptic ulcer. Mod. J. Integr. Traditional Chin. West. Med. 17 (28), 4426–4427. doi:10.3969/j.issn.1008-8849.2008.28.041
Zhu, G. L. (2019). Efficacy of Jinghua weikang capsule combined with pantoprazole quadruple therapy for 44 Helicobacter pylori-positive patients with duodenal ulcer. J. North Pharm. 16 (01), 106–107. CNKI:SUN:BFYX.0.2019-01-083.
Zhu, Y. C. (2021). Efficacy of Jinghua Weikang capsule combined with rabeprazole quadruple therapy in the treatment of Helicobacter pylori-infected patients with Verrucous Gastritis. Pract. Clin. J. Integr. Traditional Chin. West. Med. 21 (06), 73–74. doi:10.13638/j.issn.1671-4040.2021.06.036
Keywords: Jinghua Weikang capsule, Helicobacter pylori eradication, triple therapy, quadruple therapy, systematic review
Citation: Zhao Q, Wang W-j, Zhou S-p, Su J, Sun H, Zhai J-b and Hu Y-h (2022) Jinghua Weikang capsule for helicobacter pylori eradication: A systematic review and meta-analysis with trial sequential analysis. Front. Pharmacol. 13:959184. doi: 10.3389/fphar.2022.959184
Received: 07 June 2022; Accepted: 01 September 2022;
Published: 26 September 2022.
Edited by:
Abhay Prakash Mishra, University of the Free State, South AfricaReviewed by:
Ling Li, West China Hospital, ChinaCopyright © 2022 Zhao, Wang, Zhou, Su, Sun, Zhai and Hu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jing-bo Zhai, emhhaWppbmdib0Bmb3htYWlsLmNvbQ==; Yun-hui Hu, dHNsLWh1eXVuaHVpQHRhc2x5LmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.