 Xiao Cao
Xiao Cao Mingyao Sun
Mingyao Sun QiuYu Yang
QiuYu Yang Qi Wang
Qi Wang Liangying Hou2
Liangying Hou2 Long Ge
Long Ge
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol. , 02 September 2022
Sec. Obstetric and Pediatric Pharmacology
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.951072
Background: Hyperemesis gravidarum is a serious pregnancy complication that affects approximately 1% of pregnancies worldwide.
Objective: To determine whether the use of ondansetron during pregnancy is associated with abnormal pregnancy outcomes.
Search strategy: PubMed, Cochrane Library, CINAHL, Embase, CNKI, CBM, WANFANG, and ClinicalTrials.gov were searched for citations published in any language from inception to 15 December 2021.
Selection criteria: Eligible studies included any observational study.
Data collection and analysis: Odds ratio (OR) and 95% confidence interval (CI) were used as indicators to examine the association between ondansetron and abnormal pregnancy outcomes.
Main results: Twenty articles from 1,558 citations were included. Our preliminary analysis showed that compared with the unexposed group, the use of ondansetron during pregnancy may be associated with an increased incidence of cardiac defects (OR = 1.06, 95% CI: 1.01–1.10), neural tube defects (OR = 1.12, 95% CI: 1.05–1.18), and chest cleft (OR = 1.21, 95% CI: 1.07–1.37). Further sensitivity analysis showed no significant association between ondansetron and cardiac defects (OR = 1.15,95% CI: 0.94–1.40) or neural tube defects (OR = 0.87,95% CI: 0.46–1.66). When controversial studies were eliminated, the results for the chest defects disappeared. Simultaneously, we found that the use of ondansetron was associated with a reduced incidence of miscarriage (OR = 0.53, 95% CI: 0.31–0.89). Ondansetron was not associated with orofacial clefts (OR = 1.09,95% CI: 0.95–1.25), spinal limb defects (OR = 1.14,95% CI: 0.89–1.46), urinary tract deformities (OR = 1.06,95% CI: 0.97–1.15), any congenital malformations (OR = 1.03,95% CI: 0.98–1.09), stillbirth (OR = 0.97,95% CI: 0.83–1.15), preterm birth (OR = 1.22,95% CI: 0.80–1.85), neonatal asphyxia (OR = 1.05,95% CI: 0.72–1.54), or neonatal development (OR = 1.18,95% CI: 0.96–1.44) in our primary analysis.
Conclusion: In our analysis, using ondansetron during pregnancy was not associated with abnormal pregnancy outcomes. Although our study did not find sufficient evidence of ondansetron and adverse pregnancy outcomes, future studies including the exposure period and dose of ondansetron, as well as controlling for disease status, may be useful to truly elucidate the potential risks and benefits of ondansetron.
About 90% of pregnant women have symptoms of nausea and/or vomiting (Fejzo et al., 2019). Hyperemesis gravidarum (HG) is a severe pregnancy complication that affects about 1% of pregnancies worldwide (Einarson et al., 2013). The psychological and physical burden of pregnant women increases when suffering from HG (Fiaschi et al., 2018). Most women who experience serious nausea and vomiting in pregnancy (NVP)/HG need to use one or more drugs to control their symptoms (Lowe et al., 2020). According to clinical guidelines, ondansetron is widely used as a second-line treatment option for severe NVP (Shehmar et al., 2016; Taylor et al., 2017; Erick et al., 2018; Fiaschi et al., 2019).
Currently, ondansetron is increasingly used to treat NVP and HG worldwide. Between 2001 and 2014, the utilization rate of ondansetron increased from less than 1% to 13–25%, resulting in about 500,000 to 1 million women exposed to ondansetron in 4 million pregnancies in the US (Koren, 2014; Taylor et al., 2017; Parker et al., 2018). In Australia and New Zealand, physicians are 25% and 75% likely to use ondansetron when treating NVP and HG, respectively (Raymond, 2013). In Norway, 0.3% of pregnant women take ondansetron prescriptions, of which 76.9% are initially used in the first 3 months of pregnancy (van Gelder and Nordeng, 2021). In France, ondansetron prescriptions involved only 53 women (0.1%) between 2004 and 2017 in Haute-Garonne, contrary to other countries, like the US (Hurault-Delarue et al., 2021),
In November 2019, the European Medicines Agency (EMA) Pharmacovigilance Risk Assessment Committee (PRAC) released an updated comprehensive assessment report recommending that ondansetron should not be prescribed in the first 3 months of pregnancy (Aurobindo Pharma - Milpharm Ltd, 2022). A review about ondansetron in pregnancy revisited does not approve the epilogue of the EMA/PRAC assessment report and this part of the Summary of Product Characteristics (SmPC), and the regulators should consider eliminating this part from the SmPC (Damkier et al., 2021). Indeed, the safety of ondansetron has not concluded a decision now. Most studies have not detected that taking ondansetron in the early stages of pregnancy can lead to abnormal pregnancy outcomes in women (Lavecchia et al., 2018; Kaplan et al., 2019), but others have observed an increasing risk of hypoplastic left heart, diaphragmatic hernia, and respiratory system anomalies (Carstairs, 2016; Picot et al., 2020). The most recent meta-analysis was published in 2020, and its search ended in November 2019; therefore, this meta-analysis was not included in the five recently published studies (Huybrechts et al., 2020; Lemon et al., 2020; Dormuth et al., 2021; Sakran et al., 2021; Suarez et al., 2021). Three of these five studies were large-scale studies, which included 456, 963/33, 677/1, 880, and 594 pregnant women exposed to ondansetron. Three of the five studies focused on not only the risk of malformations but also other abnormal pregnancy outcomes (Dormuth et al., 2021; Sakran et al., 2021; Suarez et al., 2021).
Therefore, this systematic review and meta-analysis aimed to explore the association between ondansetron exposure during pregnancy and abnormal pregnancy outcomes.
PubMed, Cochrane Library, CINAHL, Embase, CNKI, CBM, WANFANG, and ClinicalTrials.gov were searched for citations published in any language from inception to 15 December 2021, including topics of ondansetron and pregnancy (for a complete retrieval strategy, Supplementary Table S1). In addition, we searched the references included in the research and related systematic reviews. There were no requirements for language or publishing forms.
Studies that met the following criteria were considered qualified: 1) population were pregnant women; 2) included the ondansetron group; 3) included healthy or disease-matched controls (gestational nausea and vomiting or gestational hyperemesis); 4) outcomes included the risk of abnormal pregnancy (such as stillbirth, preterm birth, and congenital malformations); and 5) included studies were observational studies (such as prospective cohort, nested case-control, case-control, or case-cohort designs). If an overlap was detected between the two studies, we tended to select studies with high methodological quality. Animal studies, editorials, and reviews were excluded. An inspector screened the titles and abstracts of all the retrieved studies. Studies that met the criteria were independently reviewed by another reviewer, and inconsistencies were resolved through discussion; if necessary, senior authors were consulted to reach a consensus.
Two authors (XC and MYS) separately extracted information from the selected studies including the country, study design, participant characteristics, exposure factors, result evaluation, and statistical analysis (including adjustment for confounding factors), and the differences were discussed and resolved. We chose risk estimates with the most complete adjustment for confounding factors and their 95% confidence intervals. The authors were contacted for additional data, when necessary.
Based on the selection and comparability of groups and the method of determining exposure or results, two reviewers (XC and MYS) independently assessed the risk of bias in the cohort and case-control studies using a revised version of the Newcastle–Ottawa scale (Wells et al., 2001; Stang, 2010). We judged methodological quality based on the total score: ≤5 considered low, 6–7 considered moderate, and 8–9 deemed high quality (Chaudhry et al., 2022). The reviewers were not blind to the author’s name, organization, achievements, or journals of the publication. Any differences were resolved by another author (QYY).
Odds ratio (OR) and 95% confidence interval (CI) were used to determine the correlation between ondansetron and abnormal pregnancy outcomes, although hazard ratios (HRs) and relative risks (RRs) were used in the included studies. We used the inverse variance weighting method of random effect to calculate OR and 95% CI together (Ge et al., 2019). To confirm the specific type of outcomes, we classified the abnormal pregnancy outcomes. We used Cochrane’s Q test and I2 value to test the statistical heterogeneity in the study (Higgins et al., 2003). Begg’s rank correlation test was used to evaluate publication bias at a significant level of p < 0.05 when there were at least 10 studies (Begg and Mazumdar, 1994). We also conducted a sensitivity analysis through studies that excluded a controversial or high risk of bias. All analyses were performed using Review Manager 5.4.1 (Cochrane Cooperative in Copenhagen, Denmark) and Stata V.16.1 software (Stata Corp, College Station, Texas, United States).
Literature screening and inclusion process were carried out according to PRISMA (Moher et al., 2009). Figure 1 shows the PRISMA flowchart. Our search searched 1558 records of which 39 were judged as possible studies based on the titles and abstracts (reasons and lists of references excluded from full-text filtering are presented in Supplementary Table S2) and 20 studies were eligible (Einarson et al., 2004; Asker et al., 2005; Anderka et al., 2012; Ferreira et al., 2012; Colvin et al., 2013; Pasternak et al., 2013; Danielsson et al., 2014; Werler et al., 2014; Özdemirci et al., 2014; Fejzo et al., 2016; Lemon et al., 2016; Parker et al., 2018; Bérard et al., 2019; Zambelli-Weiner et al., 2019; Couse and Syed, 2020; Huybrechts et al., 2020; Lemon et al., 2020; Dormuth et al., 2021; Sakran et al., 2021; Suarez et al., 2021). There were 11 cohort studies (Einarson et al., 2004; Asker et al., 2005; Colvin et al., 2013; Pasternak et al., 2013; Özdemirci et al., 2014; Fejzo et al., 2016; Bérard et al., 2019; Huybrechts et al., 2020; Lemon et al., 2020; Dormuth et al., 2021; Suarez et al., 2021), five case-control studies (Anderka et al., 2012; Danielsson et al., 2014; Werler et al., 2014; Parker et al., 2018; Zambelli-Weiner et al., 2019), two case reports (Lemon et al., 2016; Couse and Syed, 2020), and one study (Ferreira et al., 2012).
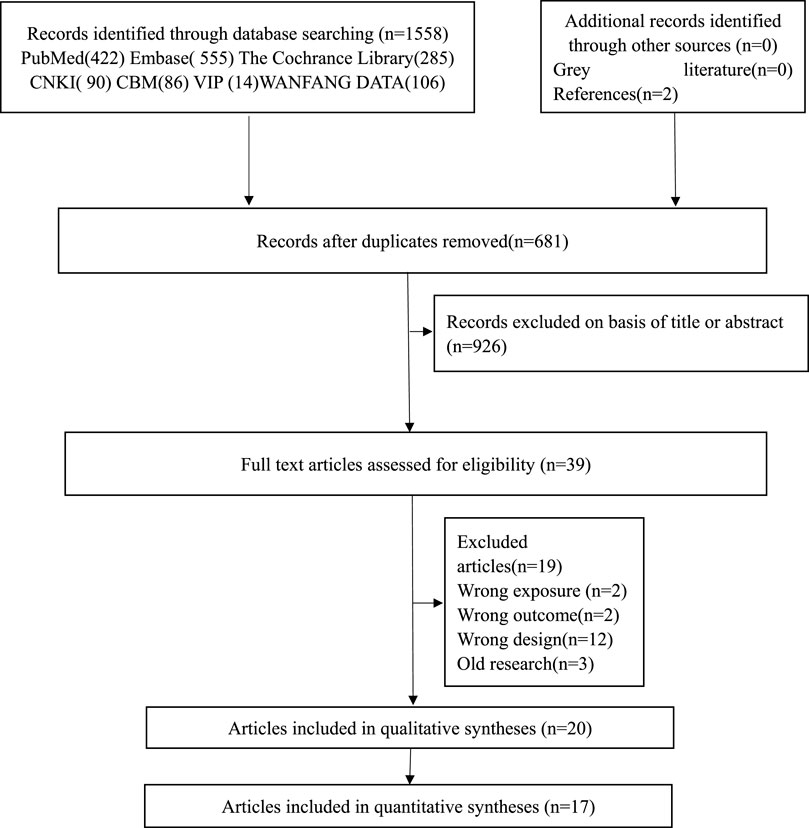
FIGURE 1. PRISMA flow diagram.
Eleven of the included studies originated from the United States, three from Canada, two from Sweden, and others apart from Turkey, Australia, Canada, Denmark, and Israel. The included studies contained a variety of controls, including chlorpromazine, unexposed, other anti-emetics, metoclopramide, non-teratogenic exposure (NTE), meclizine, and other prescription antiemetics (RxAE). Colvin et al., Berard et al., Asker et al., Dormuth et al., Lemon et al., Huybrechts et al., Suarez et al., Pasternak et al., Werler et al., Weiner et al. had one control group, unexposed, for comparison. ÖZDEMİRCİ et al. had one control group, chlorpromazine, for comparison. Fejzo et al. and Einarson et al. used two control groups for comparison, a disease matching group and an unexposed group. Parker et al. and Anderka et al. used two control groups for comparison, RxAE and unexposed. Sakran et al. observed the risk of defects in the ondansetron exposure group and the metoclopramide exposure group in the same cohort. Danielsson et al. detected the risk of the ondansetron exposure group and the meclizine exposure pregnancies. There were also two case report studies and one case series study. Table 1 presents the characteristics of the 20 studies. Supplementary Table S3 lists the adjustment variables of the included studies.
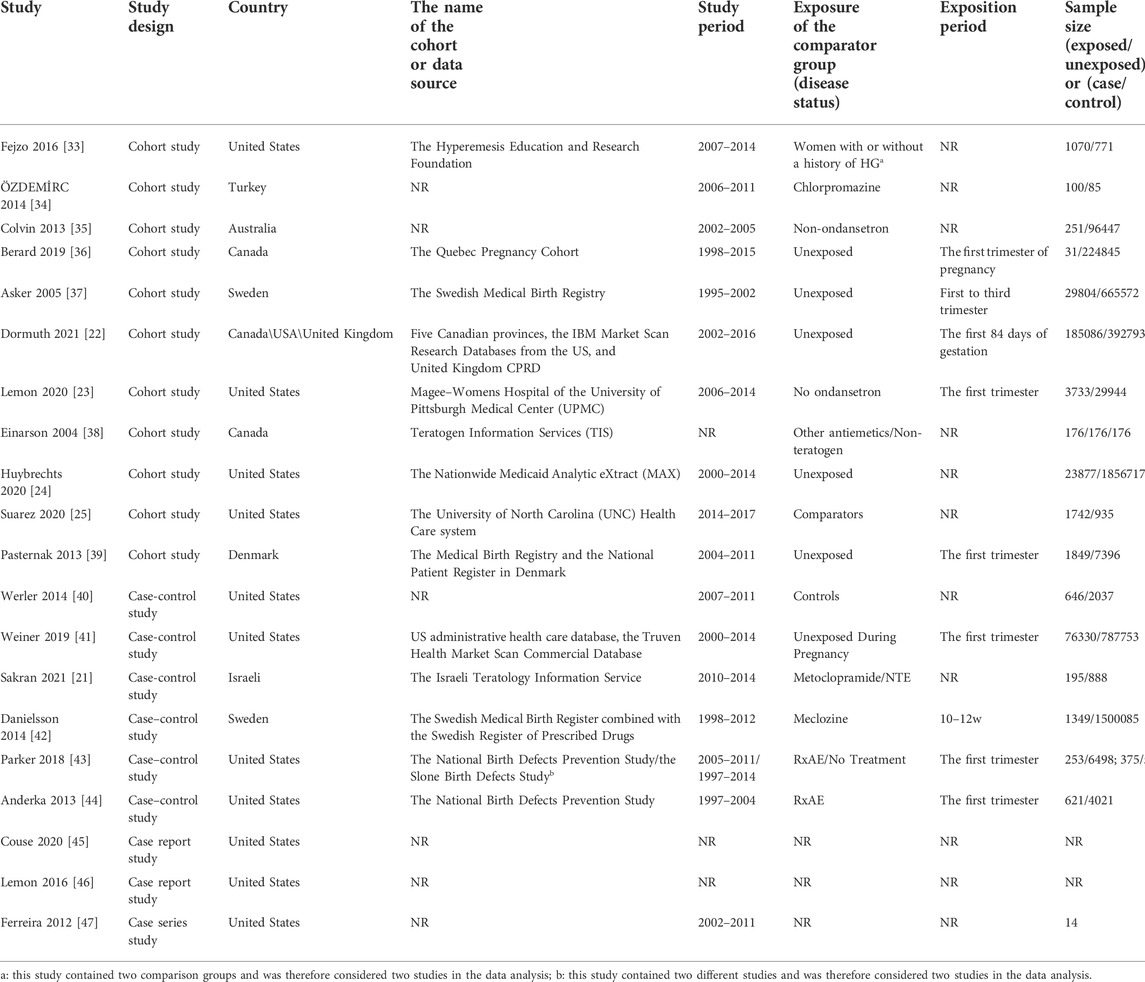
TABLE 1. Study characteristics.
Only two of the eligible studies were categorized as high methodological quality, most (13/16) of the eligible studies were categorized as moderate methodological quality, and only one (5%) low-quality study was received by Einarson et al. (Einarson et al., 2004). Three cohort studies (Einarson et al., 2004; Colvin et al., 2013; Fejzo et al., 2016) and four case-control studies (Werler et al., 2014; Parker et al., 2018; Zambelli-Weiner et al., 2019) had a high risk of bias in assessing exposure since they did not mention any information or reference about the effectiveness of ondansetron measurements or only baseline measurements. Ten cohort studies are at high risk of bias for comparability of cohorts based on the design or analysis (Einarson et al., 2004; Asker et al., 2005; Colvin et al., 2013; Pasternak et al., 2013; Özdemirci et al., 2014; Bérard et al., 2019; Huybrechts et al., 2020; Lemon et al., 2020; Dormuth et al., 2021; Suarez et al., 2021), and four case-control studies (Anderka et al., 2012; Danielsson et al., 2014; Werler et al., 2014; Parker et al., 2018) had a high risk of bias for study controls for any additional factor. Four (36.36%) cohort studies (Einarson et al., 2004; Asker et al., 2005; Özdemirci et al., 2014; Fejzo et al., 2016) were at high risk of bias for outcome assessment. One cohort study (Suarez et al., 2021) was at high risk of bias for adequacy of follow-up of cohorts. Two case-report studies and one case-series study did not assess the risk of bias. Supplementary Figure S3 showed the risk of bias in the included studies.
Although the methodological quality of the Weiner study was high according to the NOS results, the European Network of Teratology Information Services (ENTIS) Scientific Committee’s position was that the study was compromised to a certain extent methodologically and ethically and that the results could not be considered when evaluating the totality of evidence on ondansetron safety in pregnancy (Colvin et al., 2013). Therefore, our study considered Weiner's study to be a controversial study, which was dealt with in sensitivity analysis.
In this analysis, five studies detected a total of 104,763 infants exposed to ondansetron and 2687298 control infants reported cardiac defects (Parker et al., 2018; Zambelli-Weiner et al., 2019; Huybrechts et al., 2020; Lemon et al., 2020; Sakran et al., 2021). The incidence of cardiac defects increased significantly after the use of ondansetron during pregnancy (OR = 1.06,95% CI: 1.01–1.10) in our primary analysis (Figure 2). To confirm the types of cardiac defects, we conducted subgroup analyses of different types of cardiac defects. Further research showed a significant increase in the rate of cardiovascular defects (OR = 1.62, 95% CI: 1.13–2.32), septum defects (OR = 2.05, 95% CI: 1.23–3.40), and other circulatory defects (OR = 1.11, 95% CI: 1.02–1.20) was detected following ondansetron use during pregnancy. Further sensitivity analysis showed no increase in heart defects (OR = 1.15, 95% CI: 0.94–1.40, Supplementary Figure S1). The included case-report studies reported the outcomes of isolated atrial and ventricular septal defects.
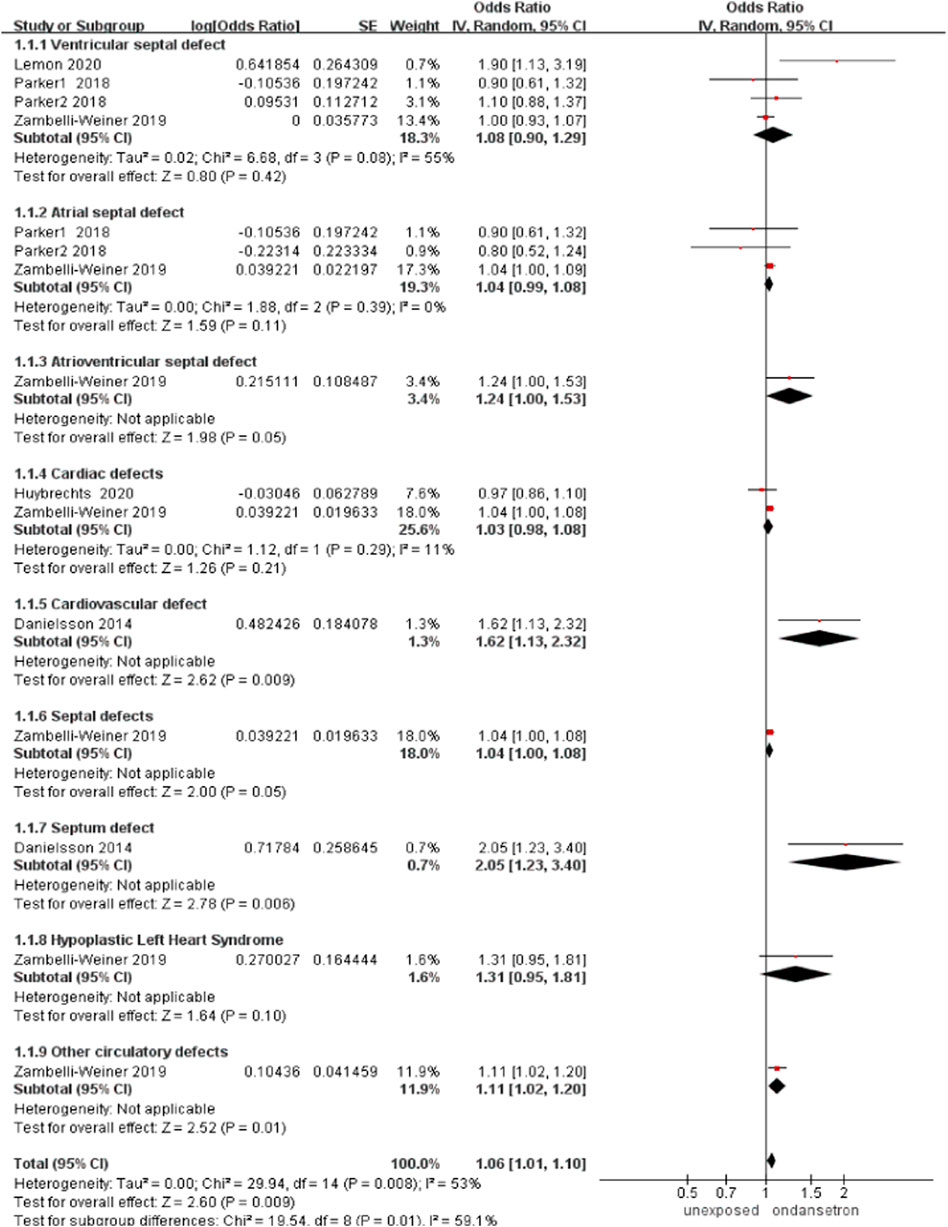
FIGURE 2. Forest plot of cardiac defects.
In this analysis, a total of 101,459 infants exposed to ondansetron and 2,660,487 control infants reported orofacial clefts in four studies (Anderka et al., 2012; Parker et al., 2018; Zambelli-Weiner et al., 2019; Huybrechts et al., 2020). The orofacial cleft rate did not increase significantly after the use of ondansetron during pregnancy (OR = 1.09, 95% CI: 0.95–1.25) in our primary analysis (Figure 3). Sensitivity analysis by excluding controversial studies showed the same result that no risk of orofacial clefts was detected (OR = 1.05, 95% CI: 0.77–1.44, Supplementary Figure S2).
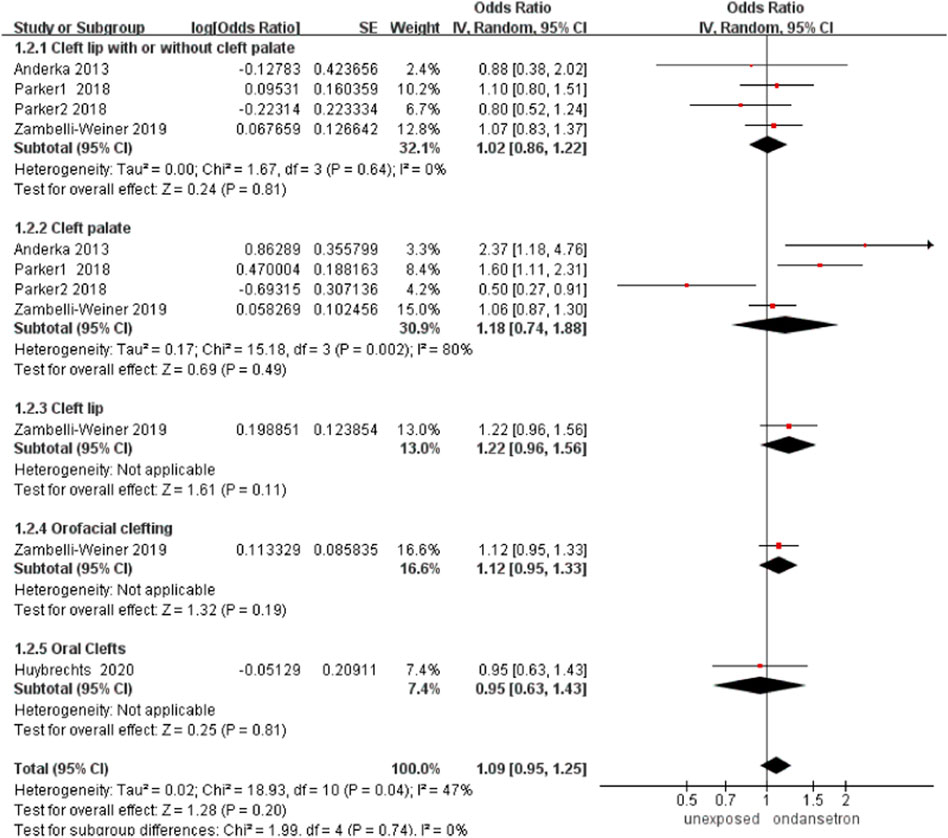
FIGURE 3. Forest plot of orofacial clefts.
In this analysis, a total of 77,604 infants exposed to ondansetron and 801,247 control infants reported spinal limb defects (Werler et al., 2014; Parker et al., 2018; Zambelli-Weiner et al., 2019). There was no obvious increase in the incidence of spinal limb defects after administration of ondansetron during pregnancy (OR = 1.14, 95% CI: 0.89–1.46) in our primary analysis (Figure 4). Sensitivity analysis by excluding controversial studies showed the same result that no risk of spinal limb defects was detected (OR = 1.34, 95% CI: 1.00–1.79, Supplementary Figure S3).
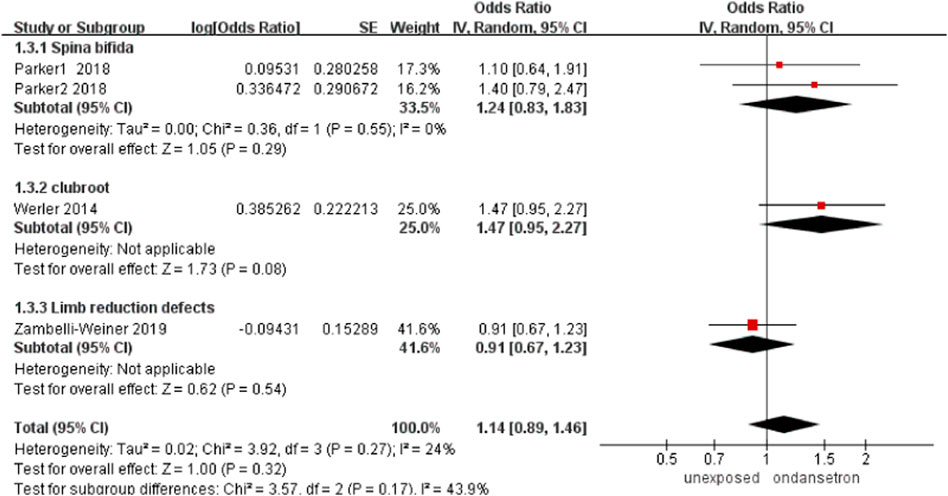
FIGURE 4. Forest plot of spinal limb defects.
In this analysis, a total of 77,579 infants exposed to ondansetron and 803,231 control infants reported neural tube defects (Anderka et al., 2012; Parker et al., 2018; Zambelli-Weiner et al., 2019). The rate of neural tube defects increased significantly after using ondansetron during pregnancy (OR = 1.12, 95% CI: 1.05–1.18) in our primary analysis (Figure 5). Sensitivity analysis by excluding controversial studies showed a different result that no risk of neural tube defects was detected (OR = 0.87, 95% CI: 0.46–1.66, Supplementary Figure S4).
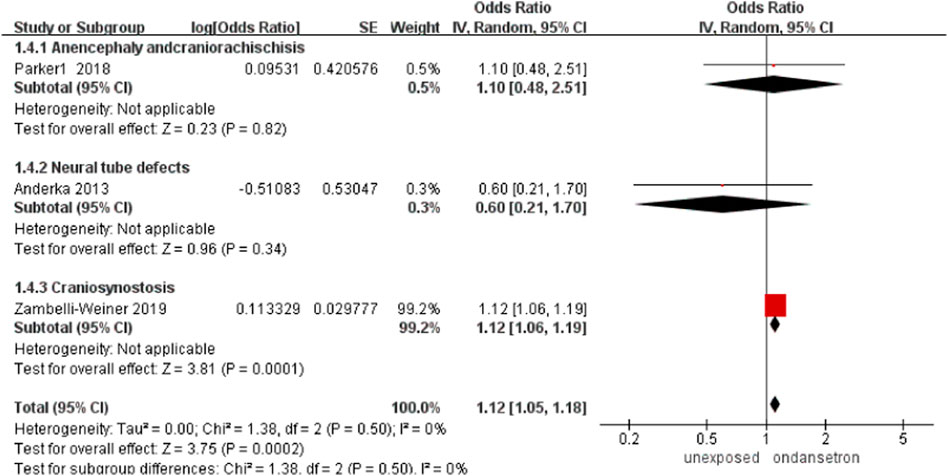
FIGURE 5. Forest plot of neural tube defects.
In this analysis, 77,579 infants exposed to ondansetron and 803,231 control infants reported urinary tract deformities (Anderka et al., 2012; Parker et al., 2018; Zambelli-Weiner et al., 2019). The incidence of urinary tract deformities did not increase significantly after ondansetron was used during pregnancy (OR = 1.06, 95% CI: 0.97–1.15) in our primary analysis (Figure 6). Sensitivity analysis by excluding controversial studies showed the same result that no risk of urinary tract deformities was detected (OR = 0.99, 95% CI: 0.77–1.26, Supplementary Figure S5).
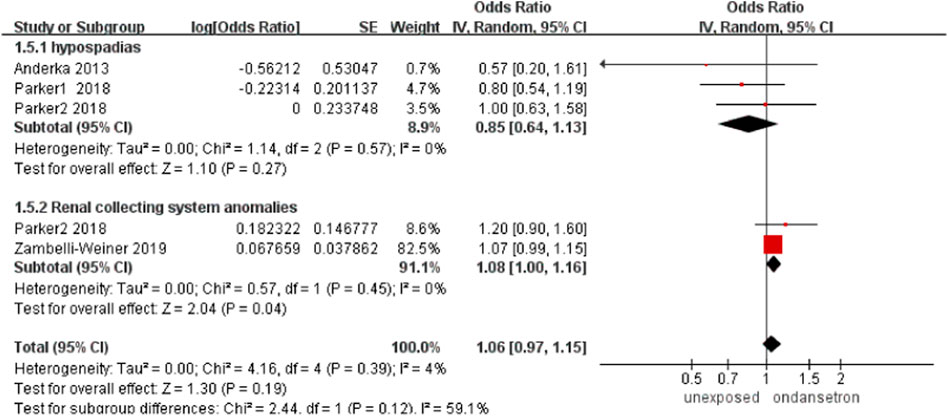
FIGURE 6. Forest plot of urinary tract deformities.
One study detected a total number of 76,330 infants exposed to ondansetron and 787,753 control infants reported chest defects in this analysis (Zambelli-Weiner et al., 2019). The incidence of chest defects increased significantly after the use of ondansetron during pregnancy (OR = 1.21, 95% CI: 1.07–1.37) in our primary analysis (Figure 7). It is important to note that the results on chest defects were obtained from Weiner’s study. If we ruled out controversial studies, then the association between ondansetron and chest defects disappeared.
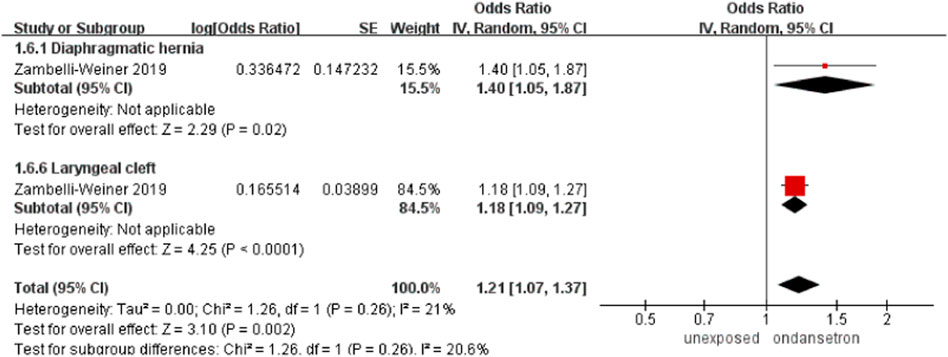
FIGURE 7. Forest plot of chest defects.
Six studies detected 212,443 infants exposed to ondansetron, and 7,613,426 control infants reported any congenital malformations in the analysis (Colvin et al., 2013; Pasternak et al., 2013; Danielsson et al., 2014; Bérard et al., 2019; Huybrechts et al., 2020; Dormuth et al., 2021). Any congenital malformation data were derived directly from the corresponding classification in the included studies. No obvious increase in congenital malformations was found after administration of ondansetron during pregnancy (OR = 1.03, 95% CI: 0.98–1.09) in our primary analysis (Figure 8). This outcome did not include any studies that required exclusion.
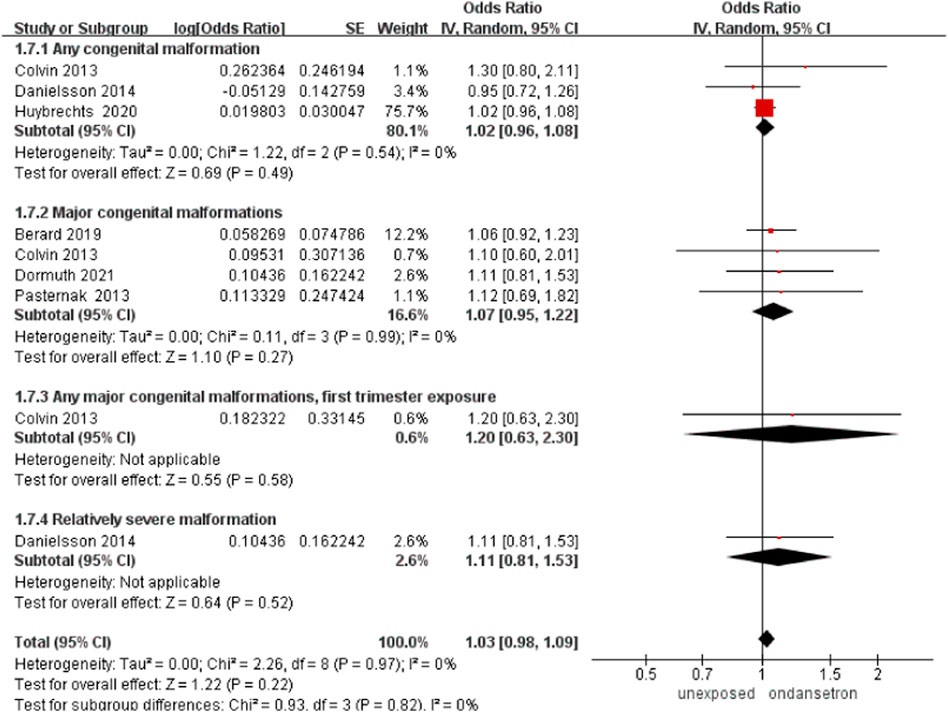
FIGURE 8. Forest plot of any congenital malformations.
One study detected 76,330 ondansetron-exposed and 787,753 control infants reported other defects (negative control) (Zambelli-Weiner et al., 2019). The rate of other defects (negative control) did not increase significantly after ondansetron was used during pregnancy (OR = 1.02, 95% CI: 1.00–1.04).
Four studies detected 188,200 ondansetron-exposed, and 3,936,991 control infants reported miscarriage (Pasternak et al., 2013; Fejzo et al., 2016; Dormuth et al., 2021; Sakran et al., 2021). Use of ondansetron during pregnancy can significantly reduce the rate of miscarriage (OR = 0.53, 95% CI: 0.31–0.89) in our primary analysis (Figure 9). This outcome did not include any studies that needed to be excluded in sensitivity analysis.
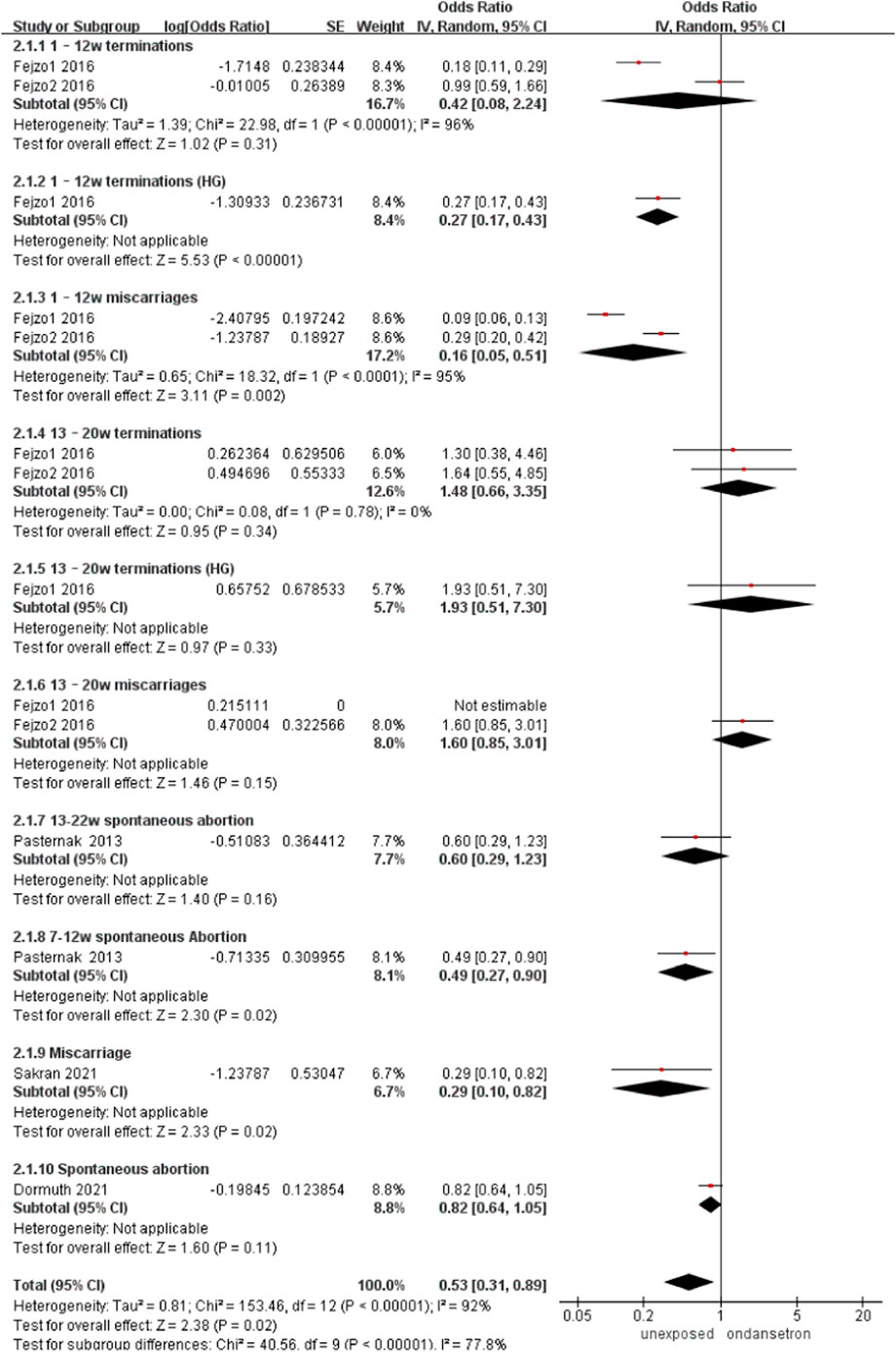
FIGURE 9. Forest plot of miscarriage.
Five studies detected 189,998 ondansetron-exposed, and 4,033,485 control infants reported stillbirth.22,25,33,35,39 There was no significant change in stillbirth rate after administration of ondansetron during pregnancy (OR = 0.97, 95% CI: 0.83–1.15) in our primary analysis (Figure 10). This outcome did not include any studies that needed to be excluded in sensitivity analysis.
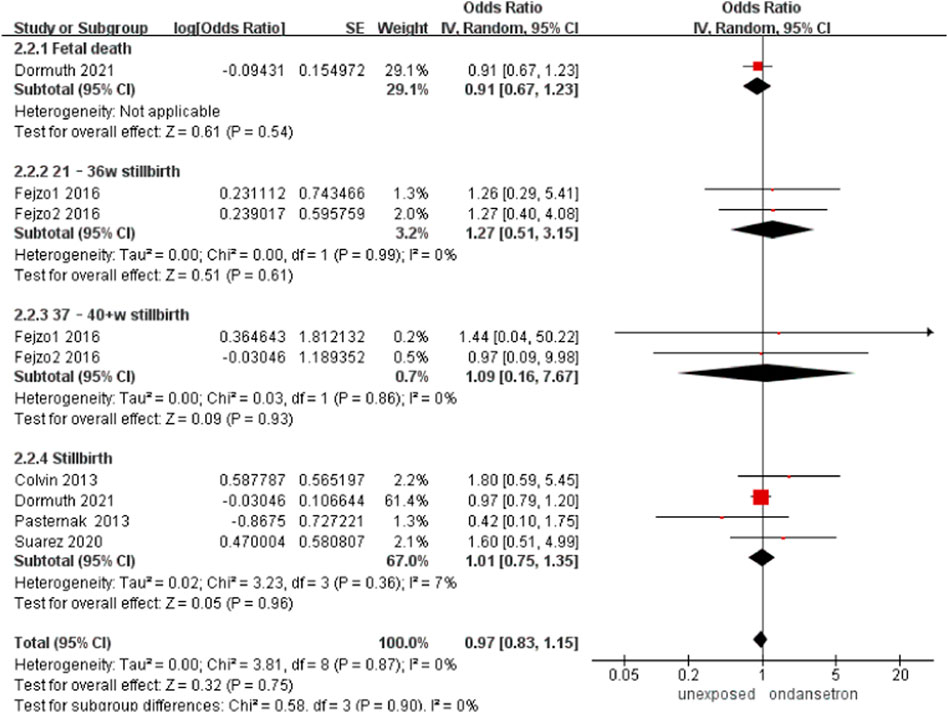
FIGURE 10. Forest plot of stillbirth.
Three studies detected 4,661 ondansetron-exposed and 9,102 control infants reported preterm birth (Pasternak et al., 2013; Fejzo et al., 2016; Suarez et al., 2021). No change in the incidence of preterm birth was found after administration of ondansetron in pregnancy (OR = 1.22, 95% CI: 0.80–1.85) in our primary analysis (Figure 11). Sensitivity analysis was not required for this part.
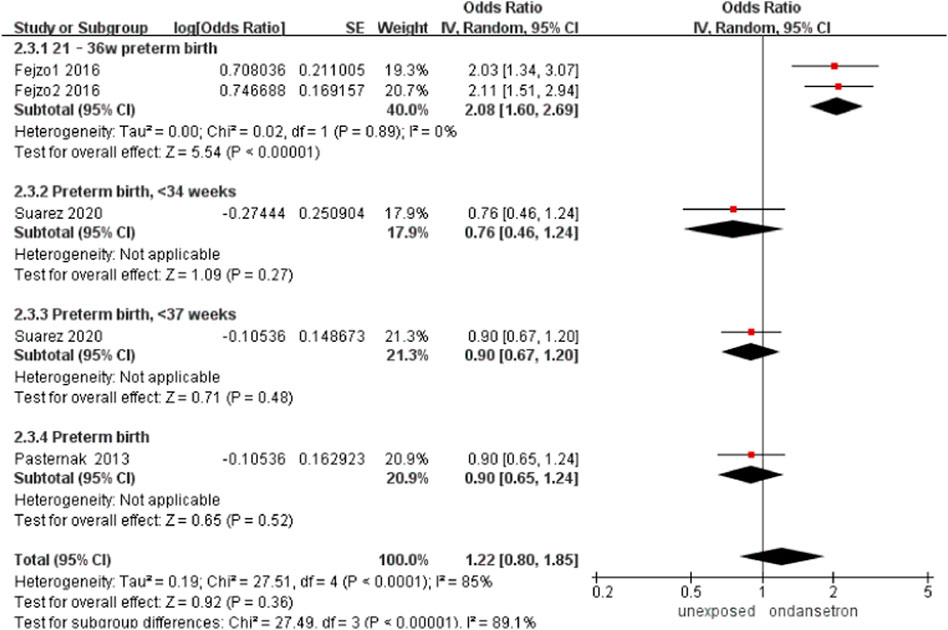
FIGURE 11. Forest plot of preterm birth.
One study detected 251 ondansetron-exposed, and 96,447 control infants reported neonatal asphyxia (Colvin et al., 2013). There was no obvious change in the incidence of neonatal asphyxia after administration of ondansetron in pregnancy (OR = 1.05, 95% CI: 0.72–1.54). (Figure 12).
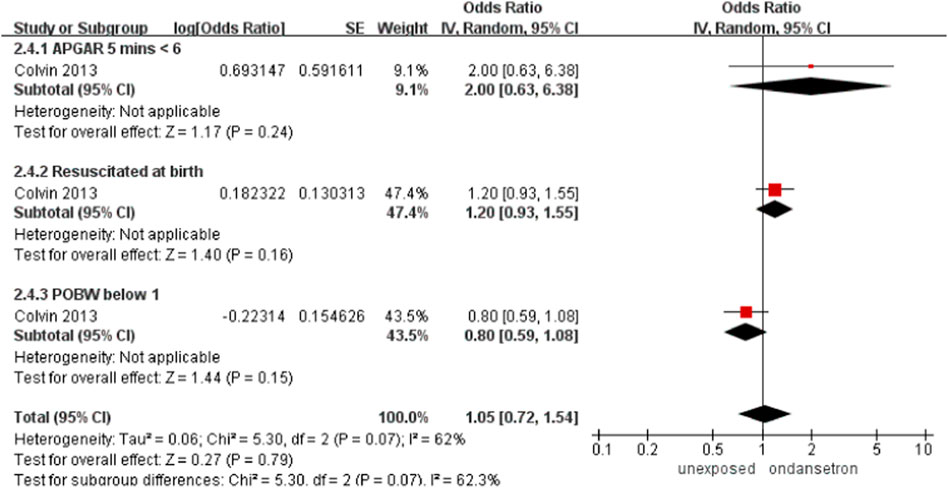
FIGURE 12. Forest plot of neonatal asphyxia.
Three studies detected 3,842 ondansetron-exposed, and 104,778 control infants reported neonatal development (Colvin et al., 2013; Pasternak et al., 2013; Suarez et al., 2021). The indicators of abnormal neonatal development included low birth weight, small gestational age, and low birth length. After the use of ondansetron during pregnancy, there was no change in the risk of abnormal neonatal development (OR = 1.18, 95% CI: 0.96–1.44) in our primary analysis (Figure 13).
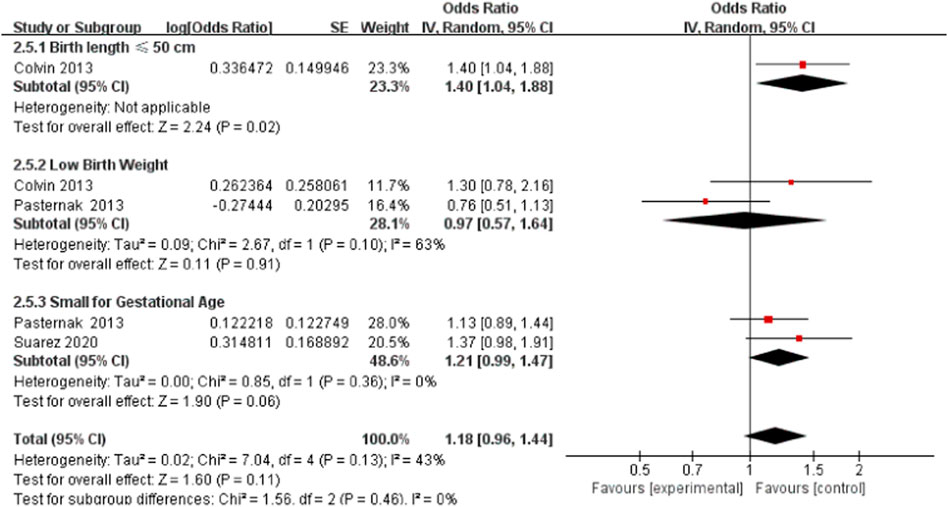
FIGURE 13. Forest plot of neonatal development.
The included case-report studies reported the outcomes included pharmacokinetic changes, intrauterine growth retardation, transient tachypnea, a mild hydrocele, and extrarenal pelvis.
Our findings enrich the previous meta-analysis to observe whether or not there is an association between ondansetron use and risk of abnormal pregnancy outcomes, which has not been fully addressed previously. This study of 20 observational studies showed that ondansetron users were at a statistically higher risk of cardiac defects, neural tube defects, and chest defects than unexposed individuals, while the risk of miscarriage was statistically lower. Based on Damkier’s comment, we excluded Weiner’s study (Damkier et al., 2021). As a result, we did not observe a correlation between the use of ondansetron and any abnormal pregnancy outcomes.
Previously published systematic reviews have focused on the association between ondansetron use and the occurrence of congenital malformations, and there are inconsistencies in their conclusions (Carstairs, 2016; Lavecchia et al., 2018; Kaplan et al., 2019; Picot et al., 2020). Kaplan et al. (2019) showed that there was no exact incidence of cardiac defects, orofacial clefts, major malformations, hypospadias, or genitourinary malformations. Picot et al. (2020) found that exposure to ondansetron in early pregnancy was associated with an increased incidence of the ventricular septal defect (OR 1.11, 95% CI 1.00–1.23) and oral clefts (OR 1.22, 95% CI 1.00–1.49). Lavecchia et al. (2018) found that the increase in the incidence of specific defects, such as cardiovascular defects and cleft palate, was contradictory. Carstairs’s analysis found that the incidence of birth defects related to ondansetron exposure appeared to be low and that the incidence of heart abnormalities in newborns exposed to ondansetron might increase Carstairs (2016). In previous studies on the use of ondansetron during pregnancy, a very major issue was the resulting risk of heart defects, cleft palate, and other malformations. Our meta-analysis of observational studies detected that those who took ondansetron during pregnancy did not have an increased risk of overall heart defect or cleft palate when compared with the control group.
The prescription of unlabeled ondansetron has increased sharply in pregnant women (Colvin et al., 2013). Hyperemesis gravidarum that does not respond to other treatments may be treated with ondansetron.
Our review included a relatively large number of studies (20) and a large number of participants from nine countries (9,445,268). This study included cohort and case-control studies, also taking into account case reports. Simultaneously, we used the adjusted effect value, and the result was closer to the real effect. Most of the results included in the studies were adjusted; therefore, there was less likelihood that confounding factors would affect the credibility of the results.
Our study had some limitations. For some outcomes, the small number of participants included in the study may have made the findings unreliable. At the same time, our systematic review did not process OR/RR/HR conversion; therefore, the aggregate values may be biased. However, most studies had unclear or wide-ranging exposure periods and doses; therefore, it was not possible to judge whether ondansetron was used in the exposure group during fetal organ development and the teratogenic dose. Moreover, most studies did not control for disease status (NVP). Ondansetron is generally prescribed for severe NVP (HG), which may be a confounding factor because it is associated with poor maternal, fetal, and child outcomes (Fejzo et al., 2019).
In conclusion, we found that there was no sufficient evidence to construct the association between ondansetron and adverse pregnancy outcomes. Our findings did not support the conclusions of the EMA/PRAC that recommended against the use of ondansetron in early pregnancy. Future studies should focus on the exposure period and dose of ondansetron, as well as controlling for disease status to truly elucidate the potential risks and benefits of ondansetron.
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding authors.
XC, YW, JW, and LG conceived the study. All authors contributed to revisions and confirmed the final version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.951072/full#supplementary-material
Anderka, M., Mitchell, A. A., Louik, C., Werler, M. M., Hernandez-Diaz, S., Rasmussen, S. A., et al. (2012). Medications used to treat nausea and vomiting of pregnancy and the risk of selected birth defects. Birth Defects Res. A Clin. Mol. Teratol. 94 (1), 22–30. doi:10.1002/bdra.22865
Asker, C., Norstedt Wikner, B., and Källén, B. (2005). Use of antiemetic drugs during pregnancy in Sweden. Eur. J. Clin. Pharmacol. 61 (12), 899–906. doi:10.1007/s00228-005-0055-1
Aurobindo Pharma - Milpharm Ltd (2022) Ondansetron 4 mg film-coated tablets - summary of product characteristics (SmPC) - (emc). Available at: https://www.medicines.org.uk/emc/medicine/32781/spc.
Begg, C. B., and Mazumdar, M. (1994). Operating characteristics of a rank correlation test for publication bias. Biometrics 50 (4), 1088. PMID: 7786990. doi:10.2307/2533446
Bérard, A., Sheehy, O., Gorgui, J., Zhao, J. P., Soares de Moura, C., and Bernatsky, S. (2019). New evidence for concern over the risk of birth defects from medications for nausea and vomitting of pregnancy. J. Clin. Epidemiol. 116, 39–48. doi:10.1016/j.jclinepi.2019.07.014
Carstairs, S. D. (2016). Ondansetron use in pregnancy and birth defects: A systematic review. Obstet. Gynecol. 127 (5), 878–883. doi:10.1097/AOG.0000000000001388
Chaudhry, D., Chaudhry, A., Peracha, J., and Sharif, A. (2022). Survival for waitlisted kidney failure patients receiving transplantation versus remaining on waiting list: Systematic review and meta-analysis. BMJ 376, e068769. doi:10.1136/bmj-2021-068769
Colvin, L., Gill, A. W., Slack-Smith, L., Stanley, F. J., and Bower, C. (2013). Off-label use of ondansetron in pregnancy in Western Australia. Biomed. Res. Int. 2013, 909860. doi:10.1155/2013/909860
Couse, M., and Syed, S. (2020). A rise in aspartate transaminase and alanine transaminase associated with ondansetron administration in a pregnant female. Cureus 12 (11), e11540. doi:10.7759/cureus.11540
Damkier, P., Kaplan, Y. C., Shechtman, S., Diav-Citrin, O., Cassina, M., and Weber-Schoendorfer, C. (2021). Ondansetron in pregnancy revisited: Assessment and pregnancy labelling by the European Medicines agency (EMA) & pharmacovigilance risk assessment committee (PRAC). Basic Clin. Pharmacol. Toxicol. 128 (4), 579–582. doi:10.1111/bcpt.13541
Danielsson, B., Wikner, B. N., and Källén, B. (2014). Use of ondansetron during pregnancy and congenital malformations in the infant. Reprod. Toxicol. 50, 134–137. doi:10.1016/j.reprotox.2014.10.017
Dormuth, C. R., Winquist, B., Fisher, A., Wu, F., Reynier, P., Suissa, S., et al. (2021). Comparison of pregnancy outcomes of patients treated with ondansetron vs alternative antiemetic medications in a multinational, population-based cohort. JAMA Netw. Open 4 (4), e215329. doi:10.1001/jamanetworkopen.2021.5329
Einarson, A., Maltepe, C., Navioz, Y., Kennedy, D., Tan, M. P., and Koren, G. (2004). The safety of ondansetron for nausea and vomiting of pregnancy: A prospective comparative study. BJOG 111 (9), 940–943. doi:10.1111/j.1471-0528.2004.00236.x
Einarson, T. R., Piwko, C., and Koren, G. (2013). Quantifying the global rates of nausea and vomiting of pregnancy: A meta analysis. J. Popul. Ther. Clin. Pharmacol. 20 (2), e171–83. PMID: 23863575.
Erick, M., Cox, J. T., and Mogensen, K. M. (2018). ACOG practice bulletin 189: Nausea and vomiting of pregnancy. Obstet. Gynecol. 131 (5), 935. doi:10.1097/AOG.0000000000002604
Fejzo, M. S., MacGibbon, K. W., and Mullin, P. M. (2016). Ondansetron in pregnancy and risk of adverse fetal outcomes in the United States. Reprod. Toxicol. 62, 87–91. doi:10.1016/j.reprotox.2016.04.027
Fejzo, M. S., Trovik, J., Grooten, I. J., Sridharan, K., Roseboom, T. J., Vikanes, A., et al. (2019). Nausea and vomiting of pregnancy and hyperemesis gravidarum. Nat. Rev. Dis. Prim. 5, 62–17. doi:10.1038/s41572-019-0110-3
Ferreira, E., Gillet, M., Lelièvre, J., and Bussieres, J. F. (2012). Ondansetron use during pregnancy: A case series. J. Popul. Ther. Clin. Pharmacol. 19 (1), e1–e10. PMID: 22267256.
Fiaschi, L., Nelson- Piercy, C., Gibson, J., Szatkowski, L., and Tata, L. J. (2018). Adverse maternal and birth outcomes in women admitted to hospital for hyperemesis gravidarum: A population- based cohort study. Paediatr. Perinat. Epidemiol. 32, 40–51. doi:10.1111/ppe.12416
Fiaschi, L., Nelson-Piercy, C., Deb, S., King, R., and Tata, L. J. (2019). Clinical management of nausea and vomiting in pregnancy and hyperemesis gravidarum across primary and secondary care: A population-based study. BJOG 126 (10), 1201–1211. doi:10.1111/1471-0528.15662
Ge, L., Guyatt, G., Tian, J., Pan, B., Chang, Y., Chen, Y., et al. (2019). Insomnia and risk of mortality from all-cause, cardiovascular disease, and cancer: Systematic review and meta-analysis of prospective cohort studies. Sleep. Med. Rev. 48, 101215. doi:10.1016/j.smrv.2019.101215
Higgins, J. P., Thompson, S. G., Deeks, J. J., and Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ 327 (7414), 557–560. doi:10.1136/bmj.327.7414.557
Hurault-Delarue, C., Araujo, M., Vabre, C., Benevent, J., Damase-Michel, C., and Lacroix, I. (2021). What changes in prescription patterns of antiemetic medications in pregnant women in France? Fundam. Clin. Pharmacol. 35 (6), 1159–1167. doi:10.1111/fcp.12681
Huybrechts, K. F., Hernandez-Diaz, S., Straub, L., Gray, K. J., Zhu, Y., Mogun, H., et al. (2020). Intravenous ondansetron in pregnancy and risk of congenital malformations. JAMA 323 (4), 372–374. doi:10.1001/jama.2019.18587
Kaplan, Y. C., Richardson, J. L., Keskin-Arslan, E., Erol-Coskun, H., and Kennedy, D. (2019). Use of ondansetron during pregnancy and the risk of major congenital malformations: A systematic review and meta-analysis. Reprod. Toxicol. 86, 1–13. doi:10.1016/j.reprotox.2019.03.001
Koren, G. (2014). Treating morning sickness in the United States—changes in prescribing are needed. Am. J. Obstet. Gynecol. 211 (6), 602–606. doi:10.1016/j.ajog.2014.08.017
Lavecchia, M., Chari, R., Campbell, S., and Ross, S. (2018). Ondansetron in pregnancy and the risk of congenital malformations: A systematic review. J. Obstet. Gynaecol. Can. 40 (7), 910–918. doi:10.1016/j.jogc.2017.10.024
Lemon, L. S., Bodnar, L. M., Garrard, W., Venkataramanan, R., Platt, R. W., Marroquin, O. C., et al. (2020). Ondansetron use in the first trimester of pregnancy and the risk of neonatal ventricular septal defect. Int. J. Epidemiol. 49 (2), 648–656. doi:10.1093/ije/dyz255
Lemon, L. S., Zhang, H., Hebert, M. F., Hankins, G. D., Haas, D. M., Caritis, S. N., et al. (2016). Ondansetron exposure changes in a pregnant woman. Pharmacotherapy 36 (9), e139–41. doi:10.1002/phar.1796
Lowe, S. A., Armstrong, G., Beech, A., Bowyer, L., Grzeskowiak, L., Marnoch, C. A., et al. (2020). SOMANZ position paper on the management of nausea and vomiting in pregnancy and hyperemesis gravidarum. Aust. N. Z. J. Obstet. Gynaecol. 60 (1), 34–43. doi:10.1111/ajo.13084
Moher, D., Liberati, A., Tetzlaff, J., and Altman, D. G.PRISMA Group (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 339, b2535. doi:10.1136/bmj.b2535
Özdemirci, Ş., Akpınar, F., Bilge, M., Ozdemirci, F., Yilmaz, S., Esinler, D., et al. (2014). The safety of ondansetron and chlorpromazine for hyperemesis gravidarum in first trimester pregnancy. Gynecol. Obstet. Reprod. Med. 20, 81–84. Corpus ID: 6404132.
Parker, S. E., Van Bennekom, C., Anderka, M., and Mitchell, A. A.National Birth Defects Prevention Study (2018). Ondansetron for treatment of nausea and vomiting of pregnancy and the risk of specific birth defects. Obstet. Gynecol. 132 (2), 385–394. doi:10.1097/AOG.0000000000002679
Pasternak, B., Svanström, H., and Hviid, A. (2013). Ondansetron in pregnancy and risk of adverse fetal outcomes. N. Engl. J. Med. 368 (9), 814–823. doi:10.1056/NEJMoa1211035
Picot, C., Berard, A., Grenet, G., Ripoche, E., Cucherat, M., and Cottin, J. (2020). Risk of malformation after ondansetron in pregnancy: An updated systematic review and meta-analysis. Birth Defects Res. 112 (13), 996–1013. doi:10.1002/bdr2.1705
Raymond, S. H. (2013). A survey of prescribing for the management of nausea and vomiting in pregnancy in Australasia. Aust. N. Z. J. Obstet. Gynaecol. 53 (4), 358–362. doi:10.1111/ajo.12045
Sakran, R., Shechtman, S., Arnon, J., and Diav-Citrin, O. (2021). Pregnancy outcome following in-utero exposure to ondansetron: A prospective comparative observational study. Reprod. Toxicol. 99, 9–14. doi:10.1016/j.reprotox.2020.11.005
Shehmar, M., Ma, M., Nelson-Piercy, C., and Gadsby, R. (2016) The management of nausea and vomiting of pregnancy and hyperemesis gravidarum (Green-top guideline No. 69). United Kingdom: Royal College of Obstetricians & Gynaecologists. Available at: https://www.rcog.org.uk/guidance/browse-all-guidance/green-top-guidelines/the-management-of-nausea-and-vomiting-of-pregnancy-and-hyperemesis-gravidarum-green-top-guideline-no-69/.
Stang, A. (2010). Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 25 (9), 603–605. doi:10.1007/s10654-010-9491-z
Suarez, E. A., Boggess, K., Engel, S. M., Sturmer, T., Lund, J. L., and Funk, M. J. (2021). Ondansetron use in early pregnancy and the risk of late pregnancy outcomes. Pharmacoepidemiol. Drug Saf. 30 (2), 114–125. doi:10.1002/pds.5151
Taylor, L. G., Bird, S. T., Sahin, L., Tassinari, M. S., Greene, P., Reichman, M. E., et al. (2017). Antiemetic use among pregnant women in the United States: The escalating use of ondansetron. Pharmacoepidemiol. Drug Saf. 26 (5), 592–596. doi:10.1002/pds.4185
van Gelder, M. M. H. J., and Nordeng, H. (2021). Antiemetic prescription fills in pregnancy: A drug utilization study among 762, 437 pregnancies in Norway. Clin. Epidemiol. 13, 161–174. doi:10.2147/CLEP.S287892
Wells, G. A., Shea, B., O'Connell, D., Peterson, J., Welch, V., Losos, M., et al. (2001). The newcastle-ottawa scale (NOS) for assessing the quality of non randomised studies in meta-analyses. Canada: The Ottawa Hospital. Available at: https://www.ohri.ca//programs/clinical_epidemiology/oxford.asp.
Werler, M. M., Yazdy, M. M., Kasser, J. R., Mahan, S. T., Meyer, R. E., Anderka, M., et al. (2014). Medication use in pregnancy in relation to the risk of isolated clubfoot in offspring. Am. J. Epidemiol. 180 (1), 86–93. doi:10.1093/aje/kwu096
Keywords: ondansetron, pregnancy, abnormal pregnancy outcomes, defects, meta-analysis
Citation: Cao X, Sun M, Yang Q, Wang Q, Hou L, Wang J, Wu Y and Ge L (2022) Risk of abnormal pregnancy outcomes after using ondansetron during pregnancy: A systematic review and meta-analysis. Front. Pharmacol. 13:951072. doi: 10.3389/fphar.2022.951072
Received: 23 May 2022; Accepted: 28 July 2022;
Published: 02 September 2022.
Edited by:
Karel Allegaert, University Hospitals Leuven, BelgiumReviewed by:
Marlena Fejzo, University of Southern California, United StatesCopyright © 2022 Cao, Sun, Yang, Wang, Hou, Wang, Wu and Ge. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yu Wu, d3kyMDExbnlkQDE2My5jb20=; Long Ge, Z2Vsb25nMjAwOUAxNjMuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.