 Lian Wang
Lian Wang Jin Fan
Jin Fan Linli Zheng
Linli Zheng Lingmin Chen
Lingmin Chen
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
METHODS article
Front. Pharmacol. , 19 July 2022
Sec. Drugs Outcomes Research and Policies
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.932688
This article is part of the Research Topic Evidence-Based Drug Treatment of Infectious Diseases - Volume II View all 8 articles
Background: Skin and soft tissue infections (SSTIs) are among the most common infections worldwide. They manifest in a variety of forms, such as erysipelas, cellulitis, and necrotizing fasciitis. Antibiotics are the significant method for clinical treatment of SSTIs. This study reported a methodology framework to determine the efficacy and safety of iclaprim in treatment of SSTIs.
Methods: We will search the PubMed, EMbase, CNKI, WanFang Data, VIP, and ClinicalTrials.gov from their inception to June 2022 for randomized controlled trials and cohort studies on iclaprim with SSTIs. Two authors will independently screen the eligible studies, assess the quality of the included papers, and extract the required information. Randomized controlled trials will be assessed using the Cochrane risk-of-bias tool. The Newcastle–Ottawa Scale will be used to evaluate observational studies. The quality of the evidence will be evaluated using the Grading of Recommendations Assessment Development and Evaluation system. RevMan 5.3 will be used for the data synthesis and quantitative analysis.
Results and Discussions: This study will provide the clinicians with more high-quality evidence to choose iclaprim for patients with SSTIs.
Ethics and Dissemination: This systematic review and meta-analysis will be based on published data, so ethical approval is not necessary. The results of this meta-analysis will be published in a peer-reviewed journal.
Skin and soft tissue infections (SSTIs) or skin and skin structure infections (SSSIs) have been a threatening challenge worldwide. They manifest in a variety of forms, such as impetigo, ecthyma, erysipelas, cellulitis, necrotizing fasciitis, and surgical site infections (Olaniyi et al., 2017). In the United States, the overall incidence of SSTIs increased by 40% from 2.4 million in 2000 to 3.3 million in 2012 (Lee et al., 2015). S. aureus is one of the most common causes of SSTIs, and it causes mild skin abscesses, superficial tissue infections, and even life-threatening diseases (Bouvet et al., 2017; Jin et al., 2021). S. aureus biofilm often exacerbates SSTIs and minimizes therapeutic drug activities and enhances colonization, leading to antibiotic resistance that limits treatment options (Kwiecinski et al., 2015; Olaniyi et al., 2017). The incidence of SSTIs has been on the rise, which is caused by methicillin-resistant S. aureus (MRSA) in hospitals and community setting (Russo et al., 2016). When the risk of exposure to MRSA is increased, the morbidity and mortality rates also increase (Miller et al., 2015). Infectious Diseases Society of America (IDSA) recommended the treatment approaches for SSTIs, which included draining, debridement, cultured and appropriate empiric antibiotic therapy (Stevens et al., 2014). The glycopeptide vancomycin has been recommended by IDSA guidelines to treat the MRSA infections. The prevalence of MRSA infection has increased dramatically in recent years (Chambers, 2001; Johnson et al., 2007), leading to the widespread use of vancomycin and the emergence of vancomycin resistance (Cosgrove et al., 2004). The emergence of MRSA and other resistant pathogens has brought a considerable challenge to its treatment. Therefore, it is of utmost importance to develop safe and effective antibiotics for the treatment of SSTIs.
Iclaprim is a diaminopyrimidine antibiotic, which potently and selectively inhibits bacterial dihydrofolate reductase and is active against Gram-positive pathogens (Schneider et al., 2003; Sader et al., 2009). Iclaprim is in the same class as trimethoprim and was designed to be more active than trimethoprim and to overcome trimethoprim resistance among Gram-positive pathogens without the need for combination with sulfonamide (Oefner et al., 2009). Previous studies have reported that iclaprim is active in vitro against major Gram-positive pathogens, including methicillin-susceptible S. aureus, MRSA, and vancomycin-resistant strains (Tenover et al., 2004; Appelbaum and Jacobs, 2005; Oefner et al., 2009). Moreover, iclaprim also shows activity against the Gram-negative respiratory pathogens Haemophilus influenzae, Moraxella catarrhalis, and Chlamydia pneumoniae (Noviello et al., 2018). In 2015, based on its potential utility, the Food and Drug Administration approved iclaprim for the treatment of acute bacterial SSSIs (Huang and Dryden, 2018). Iclaprim is a promising agent in the treatment of SSTIs. In recent years, new trials have been carried out. However, their findings were conflicted, and the efficacy and safety of iclaprim in the treatment of SSTIs remains controversial (Stevens et al., 2007; Dryden et al., 2008; Krievins et al., 2009; Huang et al., 2018a; Holland et al., 2018). Thus, we plan to conduct a meta-analysis to evaluate the efficacy and safety of iclaprim for the treatment of SSTIs.
The methodology has been prepared according to the Preferred Reporting Items for Systematic Review and Meta-analysis Protocols (PRISMA-P) (Shamseer et al., 2015). This study has been registered in PROSPERO (Registration number CRD42018107278).
The future full review will be reported according to PRISMA 2020 (Page et al., 2021) (Figure 1). The current manuscript was reported as in previous studies (Liu et al., 2022; Page et al., 2021).
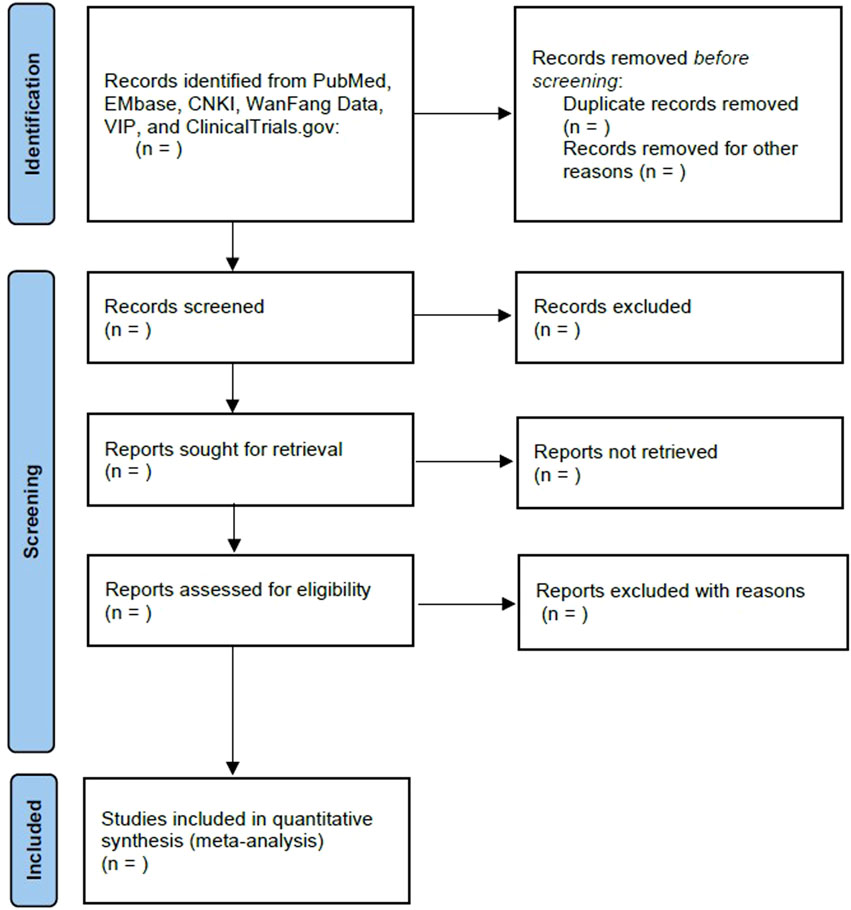
FIGURE 1. Flow diagram of the study selection process.
Relevant randomized controlled trials and cohort studies assessing the clinical efficacy and safety of lclaprim for the treatment of skin structures and soft tissue infections in patients will be included (Liu et al., 2022; Page et al., 2021). Animal studies, case reports, and case series will be excluded.
Patients aged ≥18 years with confirmed complicated SSTIs due to a Gram-positive pathogen, regardless of sex or ethnicity, will be included. SSTIs will be defined as several microbial invasions of the skin layers and of the underlying soft tissues, inducing a host response, including at least three of the following signs and symptoms: discharge, erythema, swelling and/or induration, heat and/or localized warmth, and/or pain and/or tenderness to palpation (Tognetti et al., 2012; Noviello et al., 2020). SSTIs will be sampled for microbiological culture and confirmed infections due to Gram-positive pathogens.
The intervention will be intravenous iclaprim with the purpose of anti-infection therapy compared with vancomycin or other antibiotics.
The primary outcomes will be early clinical response (ECR), clinical cure rate, and microbiologically negative rate (Krievins et al., 2009; Huang et al., 2018a; Huang and Dryden, 2018). ECR will be defined as 20% reduction in the area of the skin infection from baseline to 48–72 h after initiating antibiotics (Huang et al., 2018a). Clinical cure will be defined as the resolution of the symptoms and signs of infection and no use of any new antibiotics (Huang and Dryden, 2018). Microbiologically negative will be defined as negative culture from skin or wound at the end of the treatment (Krievins et al., 2009). The secondary outcomes will be the incidence of adverse events related to drug treatments, such as nausea, headache, diarrhea, and fatigue.
We will systematically search the PubMed, EMbase, China National Knowledge Infrastructure (CNKI), WanFang Data, Chinese Scientific Journal Database (VIP), and ClinicalTrials.gov from their inception to June 2022, without any language restrictions (Page et al., 2021; Liu et al., 2022). Table 1 lists the search strategy of PubMed, and similar strategies will be applied to the other resources.
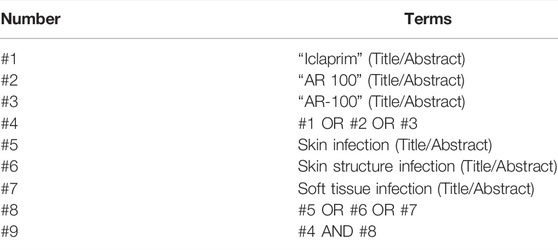
TABLE 1. PubMed search strategy.
After removing duplicates, two independent authors (Jin Fan and Lian Wang) will screen and cross-check the literature according to predefined criteria, and a third author (Lingmin Chen) will reconcile any discrepancies. The selection process will follow the PRISMA 2020 flow diagram (Figure 1) (Page et al., 2021).
The following data will be gathered by two authors independently (Jin Fan and Lian Wang): (1)) basic information of study (year of publication, the name of the first author, type of study, and sample size); (2)) participant characteristics (age, sex); (3)) interventions and controls (detailed usage of iclaprim and other antibiotics); and (4)) outcomes and adverse events. Any disagreements will be discussed and judged by a third author (Lingmin Chen or Linli Zheng). We will contact the corresponding authors via email or other methods in case of missing or incorrect data (Page et al., 2021; Liu et al., 2022). If there is no response, incomplete literature will be excluded.
Randomized controlled trials will be assessed for evidence of bias with the Cochrane risk-of-bias tool (Page et al., 2021; Liu et al., 2022). The Newcastle–Ottawa Scale will be used to assess methodological strength in observational studies (Page et al., 2021; Lemma et al., 2022). Two independent authors (Jin Fan and Lian Wang) will summarize the assessments and categorize the included studies.
This study will use RevMan 5.3 software to perform the meta-analysis (Page et al., 2021; Liu et al., 2022). Dichotomous data will be summarized using the ORs with 95% confidence intervals (CIs). Continuous outcomes will be measured using the standard mean difference or mean difference with 95% CIs. Clinical heterogeneity among studies will be assessed qualitatively, and statistical heterogeneity will be calculated using the I2 measure (Page et al., 2021; Liu et al., 2022). In instances with high levels of heterogeneity (I2 > 50%) among the studies, a random-effects model will be applied; otherwise, a fixed-effects model will be employed (Page et al., 2021; Liu et al., 2022).
Publication bias will be assessed by visual inspection of funnel plots (Page et al., 2021; Liu et al., 2022).
Subgroups analysis will be performed when meta-analysis shows significant heterogeneity and data are sufficient, such as age, treatment outcome, and type of pathogen. We plan to perform a sensitivity analysis to exclude trials of low-quality or high bias risks.
Two authors (Lian Wang and Jin Fan) will use the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) system to assess the quality of evidence associated with specific outcomes (Page et al., 2021). GRADE provides explicit criteria for rating the quality of evidence that include study design, risk of bias, imprecision, inconsistency, indirectness, and magnitude of effect (Guyatt et al., 2011). The levels of evidence will be categorized as high, moderate, low, or very low.
Ethical approval will not be necessary because this systematic review and meta-analysis only evaluated the published literature (Kim et al., 2022).
Bacterial skin and soft tissue infections (SSTIs) are one of the most common causes of infection in patients of all ages, accounting for a large proportion of hospitalizations and emergency departments (Stevens et al., 2014). Currently, SSTIs have placed an increasing burden on healthcare systems (Hersh et al., 2008). S. aureus is one of the most common causes of SSTIs, especially in wound infections, abscesses, and cellulitis (Tognetti et al., 2012). Antibiotics are generally used in the clinical treatment of SSTIs. There are many antibiotics currently approved to treat SSTIs, but almost all have safety concerns or reports of drug-resistant pathogens (Huang et al., 2019).
Iclaprim is a novel diaminopyrimidine antibiotic that inhibits bacterial dihydrofolate reductase, and it is active against Gram-positive pathogens, including emerging drug-resistant pathogens, such as MRSA and vancomycin-resistant strains (Huang et al., 2020). In two randomized, double-blind phase 3 studies (ASSIST-1 and ASSIST-2) iclaprim and linezolid were compared in patients with complicated SSSI, and the pooled clinical cure rates were 82.2% (411/500) for iclaprim and 85.3% (419/491) for linezolid (Stevens et al., 2007; Dryden et al., 2008; Huang and Dryden, 2018). Besides, two randomized, double-blind, active-controlled Phase 3 studies (REVIVE-1 and REVIVE-2) were conducted to compare iclaprim and vancomycin in patients with acute bacterial skin and skin structure infections (ABSSSI). The pooled ECR was 79.6% for iclaprim and 78.8% for vancomycin, thereby showing that iclaprim achieved noninferiority (10% margin) compared with vancomycin in the treatment of ABSSSI (Huang et al., 2018a; Huang et al., 2018b; Holland et al., 2018). In clinical trials, adverse events of iclaprim were mainly nausea, diarrhea, and headache (Sincak and Schmidt, 2009). Current research shows that the incidence of vancomycin-associated acute kidney injury (AKI) ranges from 5% to 42% (van Hal et al., 2013). Replacement of vancomycin with iclaprim for the treatment of ABSSSI may avoid vancomycin-associated AKI. Therefore, we plan to conduct a meta-analysis to evaluate the efficacy and safety of iclaprim for the treatment of SSTIs. In order to include more studies, we will include randomized control trials and cohort studies, and that will be a limitation of the future meta-analysis. In addition, we will not limit the control group. However, we will perform a subgroup analysis and discuss the clinical heterogeneity in the full review. We hope this study can provide the clinicians with more high-quality evidence to choose iclaprim for patients with skin and soft tissue infections.
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
LC and LZ conceived of the study. JF and LW will perform relevance screening, data extraction, and quality assessment of the literature. LC will resolve any disagreements in study relevancy, extraction, and quality appraisal. LW and JF drafted and revised the current manuscript. All authors will participate in data interpretation and revise the manuscript for intellectual content.
This study was supported by the Post-Doctoral Research Project of West China Hospital of Sichuan University(No. 19HXBH071).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Appelbaum, P. C., and Jacobs, M. R. (2005). Recently Approved and Investigational Antibiotics for Treatment of Severe Infections Caused by Gram-Positive Bacteria. Curr. Opin. Microbiol. 8 (5), 510–517. doi:10.1016/j.mib.2005.07.001
Bouvet, C., Gjoni, S., Zenelaj, B., Lipsky, B. A., Hakko, E., and Uçkay, I. (2017). Staphylococcus aureus Soft Tissue Infection May Increase the Risk of Subsequent Staphylococcal Soft Tissue Infections. Int. J. Infect. Dis. 60, 44–48. doi:10.1016/j.ijid.2017.05.002
Chambers, H. F. (2001). The Changing Epidemiology of Staphylococcus aureus? Emerg. Infect. Dis. 7 (2), 178–182. doi:10.3201/eid0702.010204
Cosgrove, S. E., Carroll, K. C., and Perl, T. M. (2004). Staphylococcus aureus with Reduced Susceptibility to Vancomycin. Clin. Infect. Dis. 39 (4), 539–545. doi:10.1086/422458
Dryden, M., O’Hare, M., Sidarous, E., Hadváry, P., and Islam, K. (2008). “Clinical Efficacy of Iclaprim in Complicated Skin and Skin Structure Infection (cSSSI): Preliminary Results from the ASSIST-2 Clinical Trial,” in Presented at: The 18th Annual European Congress of Clinical Microbiology and Infectious Diseases Meeting, Barcelona, Spain, April 19-22, 2008.
Guyatt, G., Oxman, A. D., Akl, E. A., Kunz, R., Vist, G., Brozek, J., et al. (2011). GRADE Guidelines: 1. Introduction-GRADE Evidence Profiles and Summary of Findings Tables. J. Clin. Epidemiol. 64 (4), 383–394. doi:10.1016/j.jclinepi.2010.04.026
Hersh, A. L., Chambers, H. F., Maselli, J. H., and Gonzales, R. (2008). National Trends in Ambulatory Visits and Antibiotic Prescribing for Skin and Soft-Tissue Infections. Arch. Intern Med. 168 (14), 1585–1591. doi:10.1001/archinte.168.14.1585
Holland, T. L., O'Riordan, W., McManus, A., Shin, E., Borghei, A., File, T. M., et al. (2018). A Phase 3, Randomized, Double-Blind, Multicenter Study to Evaluate the Safety and Efficacy of Intravenous Iclaprim versus Vancomycin for Treatment of Acute Bacterial Skin and Skin Structure Infections Suspected or Confirmed to Be Due to Gram-Positive Pathogens (REVIVE-2 Study). Antimicrob. Agents Chemother. 62 (5). doi:10.1128/AAC.02580-17
Huang, D. B., Charrier, C., and Hawser, S. (2020). Worldwide Surveillance of Iclaprim Activity: In Vitro Susceptibility of Gram-Positive Pathogens Collected from Patients with Skin and Skin Structure Infections from 2013 to 2017. Diagn Microbiol. Infect. Dis. 97 (1), 115013. doi:10.1016/j.diagmicrobio.2020.115013
Huang, D. B., Corey, G. R., Holland, T. L., Lodise, T., O'Riordan, W., Wilcox, M. H., et al. (2018). Pooled Analysis of the Phase 3 REVIVE Trials: Randomised, Double-Blind Studies to Evaluate the Safety and Efficacy of Iclaprim versus Vancomycin for Treatment of Acute Bacterial Skin and Skin-Structure Infections. Int. J. Antimicrob. Agents 52 (2), 233–240. doi:10.1016/j.ijantimicag.2018.05.012
Huang, D. B., and Dryden, M. (2018). Iclaprim, a Dihydrofolate Reductase Inhibitor Antibiotic in Phase III of Clinical Development: a Review of its Pharmacology, Microbiology and Clinical Efficacy and Safety. Future Microbiol. 13, 957–969. doi:10.2217/fmb-2018-0061
Huang, D. B., Magnet, S., De Angelis, S., Holland, T. L., File, T. M., Dryden, M., et al. (2019). Surveillance of Iclaprim Activity: In Vitro Susceptibility of Gram-Positive Skin Infection Pathogens Collected from 2015 to 2016 from North America and Europe. Diagn Microbiol. Infect. Dis. 93 (2), 154–158. doi:10.1016/j.diagmicrobio.2018.09.002
Huang, D. B., O'Riordan, W., Overcash, J. S., Heller, B., Amin, F., File, T. M., et al. (2018). A Phase 3, Randomized, Double-Blind, Multicenter Study to Evaluate the Safety and Efficacy of Intravenous Iclaprim vs Vancomycin for the Treatment of Acute Bacterial Skin and Skin Structure Infections Suspected or Confirmed to Be Due to Gram-Positive Pathogens: REVIVE-1. Clin. Infect. Dis. 66 (8), 1222–1229. doi:10.1093/cid/cix987
Jin, T., Mohammad, M., Pullerits, R., and Ali, A. (2021). Bacteria and Host Interplay in Staphylococcus aureus Septic Arthritis and Sepsis. Pathog. (Basel, Switz. 10 (2). doi:10.3390/pathogens10020158
Johnson, J. K., Khoie, T., Shurland, S., Kreisel, K., Stine, O. C., and Roghmann, M. C. (2007). Skin and Soft Tissue Infections Caused by Methicillin-Resistant Staphylococcus aureus USA300 Clone. Emerg. Infect. Dis. 13 (8), 1195–1200. doi:10.3201/eid1308.061575
Kim, E., Choi, J., and Min, S. Y. (2022). External Treatment of Herbal Medicine with Tuina in Congenital Muscular Torticollis: A Protocol for Systematic Review and Meta-Analysis. Medicine (Baltimore) 101 (10), e29035.
Krievins, D., Brandt, R., Hawser, S., Hadvary, P., and Islam, K. (2009). Multicenter, Randomized Study of the Efficacy and Safety of Intravenous Iclaprim in Complicated Skin and Skin Structure Infections. Antimicrob. Agents Chemother. 53 (7), 2834–2840. doi:10.1128/AAC.01383-08
Kwiecinski, J., Kahlmeter, G., and Jin, T. (2015). Biofilm Formation by Staphylococcus aureus Isolates from Skin and Soft Tissue Infections. Curr. Microbiol. 70 (5), 698–703. doi:10.1007/s00284-014-0770-x
Lee, G. C., Boyd, N. K., Lawson, K. A., and Frei, C. R. (2015). Incidence and Cost of Skin and Soft Tissue Infections in the united States. Value Health 18 (3), A245. doi:10.1016/j.jval.2015.03.1424
Lemma, T., Silesh, M., Taye, B. T., Desta, K., Kitaw, T. M., and Tekalign, T. (2022). HIV Serostatus Disclosure and Its Predictors Among Children Living With HIV in Ethiopia: A Systematic Review and Meta-Analysis. Front Public Health 10, 859469.
Liu, S., Cui, X., Xia, K., Duan, Y., Xiong, M., and Li, G. (2022). Efficacy and Safety of Whole-Lung Lavage for Pulmonary Alveolar Proteinosis: a Protocol for a Systematic Review and Meta-Analysis. BMJ Open 12 (4), e057671.
Miller, L. G., Eisenberg, D. F., Liu, H., Chang, C. L., Wang, Y., Luthra, R., et al. (2015). Incidence of Skin and Soft Tissue Infections in Ambulatory and Inpatient Settings, 2005-2010. BMC Infect. Dis. 15, 362. doi:10.1186/s12879-015-1071-0
Noviello, S., Corey, G. R., Holland, T. L., Lodise, T., O'Riordan, W., Wilcox, M. H., et al. (2020). A Pooled Analysis of Patients with Wound Infections in the Phase 3 REVIVE Trials: Randomized, Double-Blind Studies to Evaluate the Safety and Efficacy of Iclaprim versus Vancomycin for Treatment of Acute Bacterial Skin and Skin Structure Infections. J. Med. Microbiol. 69 (4), 625–630. doi:10.1099/jmm.0.001177
Noviello, S., Huang, D. B., and Corey, G. R. (2018). Iclaprim: a Differentiated Option for the Treatment of Skin and Skin Structure Infections. Expert Rev. Anti Infect. Ther. 16 (11), 793–803. doi:10.1080/14787210.2018.1536545
Oefner, C., Bandera, M., Haldimann, A., Laue, H., Schulz, H., Mukhija, S., et al. (2009). Increased Hydrophobic Interactions of Iclaprim with Staphylococcus aureus Dihydrofolate Reductase Are Responsible for the Increase in Affinity and Antibacterial Activity. J. Antimicrob. Chemother. 63 (4), 687–698. doi:10.1093/jac/dkp024
Olaniyi, R., Pozzi, C., Grimaldi, L., and Bagnoli, F. (2017). Staphylococcus Aureus-Associated Skin and Soft Tissue Infections: Anatomical Localization, Epidemiology, Therapy and Potential Prophylaxis. Curr. Top. Microbiol. Immunol. 409, 199–227. doi:10.1007/82_2016_32
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 Statement: an Updated Guideline for Reporting Systematic Reviews. Bmj 372, n71. doi:10.1136/bmj.n71
Russo, A., Concia, E., Cristini, F., De Rosa, F. G., Esposito, S., Menichetti, F., et al. (2016). Current and Future Trends in Antibiotic Therapy of Acute Bacterial Skin and Skin-Structure Infections. Clin. Microbiol. Infect. 22 (Suppl. 2), S27–S36. doi:10.1016/S1198-743X(16)30095-7
Sader, H. S., Fritsche, T. R., and Jones, R. N. (2009). Potency and Bactericidal Activity of Iclaprim against Recent Clinical Gram-Positive Isolates. Antimicrob. Agents Chemother. 53 (5), 2171–2175. doi:10.1128/AAC.00129-09
Schneider, P., Hawser, S., and Islam, K. (2003). Iclaprim, a Novel Diaminopyrimidine with Potent Activity on Trimethoprim Sensitive and Resistant Bacteria. Bioorg Med. Chem. Lett. 13 (23), 4217–4221. doi:10.1016/j.bmcl.2003.07.023
Shamseer, L., Moher, D., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., et al. (2015). Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015: Elaboration and Explanation. BMJ 350, g7647. doi:10.1136/bmj.g7647
Sincak, C. A., and Schmidt, J. M. (2009). Iclaprim, a Novel Diaminopyrimidine for the Treatment of Resistant Gram-Positive Infections. Ann. Pharmacother. 43 (6), 1107–1114. doi:10.1345/aph.1L167
Stevens, D., Leighton, A., Dankner, W., Islam, K., and Hadváry, P. (2007). “Efficacy of Iclaprim in Complicated Skin and Skin Structure Infections: Preliminary Results of ASSIST-1,” in Presented at: The 45th Annual Meeting of the Infectious Diseases Society of America, San Diego, CA USA, 4–7 October 2007. (Poster 1079).
Stevens, D. L., Bisno, A. L., Chambers, H. F., Dellinger, E. P., Goldstein, E. J., Gorbach, S. L., et al. (2014). Practice Guidelines for the Diagnosis and Management of Skin and Soft Tissue Infections: 2014 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 59 (2), e10–52. doi:10.1093/cid/ciu444
Tenover, F. C., Weigel, L. M., Appelbaum, P. C., McDougal, L. K., Chaitram, J., McAllister, S., et al. (2004). Vancomycin-resistant Staphylococcus aureus Isolate from a Patient in Pennsylvania. Antimicrob. Agents Chemother. 48 (1), 275–280. doi:10.1128/aac.48.1.275-280.2004
Tognetti, L., Martinelli, C., Berti, S., Hercogova, J., Lotti, T., Leoncini, F., et al. (2012). Bacterial Skin and Soft Tissue Infections: Review of the Epidemiology, Microbiology, Aetiopathogenesis and Treatment: a Collaboration between Dermatologists and Infectivologists. J. Eur. Acad. Dermatol Venereol. 26 (8), 931–941. doi:10.1111/j.1468-3083.2011.04416.x
Keywords: iclaprim, skin and skin structures infections, efficacy, safety, methodology framework
Citation: Wang L, Fan J, Zheng L and Chen L (2022) Efficacy and Safety of Iclaprim for the Treatment of Skin Structures and Soft Tissue Infections: A Methodological Framework. Front. Pharmacol. 13:932688. doi: 10.3389/fphar.2022.932688
Received: 30 April 2022; Accepted: 01 June 2022;
Published: 19 July 2022.
Edited by:
Min Yang, Anhui Medical University, ChinaReviewed by:
Yingli He, Xi’an Jiaotong University, ChinaCopyright © 2022 Wang, Fan, Zheng and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lingmin Chen, MTAxMDcwMjI4OUBxcS5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.