 Pan Hong1†
Pan Hong1† Ruikang Liu
Ruikang Liu Saroj Rai
Saroj Rai Jin Li
Jin Li
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pharmacol. , 19 May 2022
Sec. Drugs Outcomes Research and Policies
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.887386
Background: Tranexamic acid (TXA) has been applied in various types of surgery for hemostasis purposes. The efficacy and safety of TXA are still controversial in different surgeries. Guidelines for clinical application of TXA are needed.
Materials and method: We systematically searched multiple medical databases for meta-analyses examining the efficacy and safety of TXA. Types of surgery included joint replacement surgery, other orthopedic surgeries, cardiac surgery, cerebral surgery, etc. Outcomes were blood loss, blood transfusion, adverse events, re-operation rate, operative time and length of hospital stay, hemoglobin (Hb) level, and coagulation function. Assessing the methodological quality of systematic reviews 2 (AMSTAR 2) and Grading of Recommendations, Assessment, Development and Evaluation (GRADE) were used for quality assessment of the included meta-analyses. Overlapping reviews were evaluated by calculating the corrected covered area (CCA).
Result: In all, we identified 47 meta-analyses, of which 44 of them were of “high” quality. A total of 319 outcomes were evaluated, in which 58 outcomes were assessed as “high” quality. TXA demonstrates significant hemostatic effects in various surgeries, with lower rates of blood transfusion and re-operation, shorter operative time and length of stay, and higher Hb levels. Besides, TXA does not increase the risk of death and vascular adverse events, but it is a risk factor for seizure (a neurological event) in cardiac surgery.
Conclusion: Our study demonstrates that TXA has a general hemostatic effect with very few adverse events, which indicates TXA is the recommended medication to prevent excessive bleeding and reduce the blood transfusion rate. We also recommend different dosages of TXA for different types of adult surgery. However, we could not recommend a unified dosage for different surgeries due to the heterogeneity of the experimental design.
Systematic Review Registration: clinicaltrials.gov/, identifier CRD42021240303
Hemorrhage is a leading cause of death in surgery and trauma (Ferraris et al., 2011; Rossaint et al., 2016), Allogeneic blood transfusion, autologous blood donation, and acute normovolemic hemodilution are the first-line treatment for hemorrhage (Murray, 2004; Nakanishi et al., 2019; Pinto et al., 2019). However, without the potential risk of serious immune reactions and viral infections, antifibrinolytic agents seem to be a safe and affordable alternative (Etchason et al., 1995). Tranexamic acid (TXA), a synthetic lysine analogue, has been frequently used for hemostasis (Henry et al., 2011; Hunt, 2015). TXA inhibits the activation of plasminogen by blocking the lysine-binding sites of plasminogen, leading to increased clot stabilization and thus reducing blood loss (Hunt, 2015).
Investigation of TXA has been a popular topic recently where numerous meta-analyses have discussed the hemostatic efficacy and safety of TXA. Hunt et al. estimated a reduction of 120,000 deaths worldwide each year if TXA was given to all patients with severe traumatic bleeding (Hunt, 2015). TXA was also demonstrated to be a safe and effective choice in total knee arthroplasty (TKA), total hip arthroplasty (THA), cardiac surgery, and other types of surgeries (Wu et al., 2018; Zhang Y. et al., 2019; Sukeik et al., 2020). Moreover, TXA has also been reported in treating postpartum hemorrhage (Novikova et al., 2015).
So far, numerous RCTs and meta-analyses have discussed TXA in various surgery types and reported significant effects. However, the methodological and statistical qualities of these studies are heterogeneous. Besides, the risks of embolism and other complications are unclear. In order to provide a comprehensive review of existing evidence, we performed an umbrella review of meta-analyses to demonstrate the efficacy and safety of TXA in various surgeries and provide a guideline for clinical application.
Our review followed the guidelines for Meta-analyses of Observational Studies in Epidemiology and the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA), and the protocol was registered in PROSPERO (registration No CRD42021240303) (Stroup et al., 2000; Moher et al., 2009). Two independent researchers (PH and JJL) searched Medline, Embase, Web of Science, and Cochrane databases updated to 15 September for meta-analyses. The detailed search strategy is shown in Supplementary Appendix S1. We processed another search at the end of the study on 16 February 2022. We would only replace the included study when the newly published study had a different conclusion. Two researchers (RL and YD) independently screened the titles and abstracts, and articles satisfying the inclusion criteria were accessed for full-text review. They independently reviewed full-text articles for eligibility. When data were incomplete, the corresponding author was contacted by email and invited to provide additional information. Reference lists of eligible reviews and meta-analyses were searched for additional citations.
We only included meta-analyses of RCTs or meta-analyses of observational studies discussing TXA. Post hoc analyses and systematic reviews without meta-analysis were excluded. Articles were included when the exposure group was divided based on the dosage or administration method, and patients who just received the placebo or saline were included in the controlled group. We included studies with comparisons of different administration methods and dosages (high versus low dose and any versus none). Bayesian meta- and network meta-analysis were excluded unless we could extract the complete statistical data separately from a subgroup analysis. Included studies must be in accordance with the Declaration of Helsinki and approved by the respective ethics committees.
Two researchers (SR and JJL) independently extracted data from eligible articles. Our data extraction methodology was recommended and revised by the Joanna Briggs Institute (Supplementary Appendix S2) (Aromataris et al., 2014). Outcomes were classified as blood loss (total blood loss, intraoperative blood loss, and postoperative blood loss), risk of adverse effects (risk of massive hemorrhage, risk of transfusion requirement, risk of postoperative edema and ecchymosis, risk of rebleeding, and risk of significant adverse effects), and other outcomes (surgical field score, satisfaction with the surgical field, operative time, intraoperative blood pressure, hemoglobin drop, hematocrit drop, and length of hospital stay). We only compared the preoperative dose, which was more important than the maintenance dose. Considering that more variables would bring heterogeneity and that the maintenance dose was also correlated with the preoperative dose, we did not compare the maintenance dose. If an article presented separate meta-analyses for more than one health outcome, we included each of these separately. Standard mean difference (SMD) or weighted mean difference (WMD) was used for continuous variable statistics, and relative risks (RR), odds ratios (OR), or risk difference (RD) was used for discontinuous variable statistics.
We used “assessing the methodological quality of systematic reviews (AMSTAR) 2” to assess the methodological quality of the included meta-analyses (Supplementary Appendix S3) (Shea et al., 2017). We also used the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) tool to evaluate the quality of evidence for each included outcome (Supplementary Appendix S4) (Guyatt et al., 2011). The GRADE tool classifies evidence for outcomes from systematic reviews and meta-analyses into “high,” “moderate,” “low,” and “very low.” The study design of the included studies decides the baseline quality of evidence, but other factors can decrease or increase the quality level (for the detailed appraisal rule, see Supplementary Appendix S4). Two researchers (RL and JJL) rated the methodological quality of the reviews.
The heterogeneity in the results of meta-analyses was assessed by chi-square and I2 tests, followed by appropriate analysis models (fixed-effect or random-effect). Chi-squared p < 0.05 and I2 >50% indicated high heterogeneity, and random-effects models were used in these outcomes, whereas chi-squared p > 0.05 and I2<50% were considered acceptable heterogeneity, and a fixed-effects model was used instead. Most of the meta-analyses included in our review used software (Stata and RevMan) to process their statistical analyses. Publication bias was evaluated by funnel plots and further confirmed by Egger’s and Begg’s test, and p < 0.05 was considered as the statistically significant risk of bias (Sterne et al., 2000). Small-study effects that lead to potential reporting or publication bias could also be avoided by Egger’s test. However, if the data of Egger’s test were not reported, then the meta-analyses, including no more than five studies, were considered high publication bias. Sensitivity analysis was performed in the meta-analysis by excluding each study one at a time to check whether the effectiveness of the outcome was determined by individual studies. Overlapping reviews happened frequently when two or more studies evaluated the same exposure and outcome. To determine the potential overlapping, a graphical cross-tabulation was made to calculate the corrected covered area (CCA), which could quantify the degree of overlap (Pieper et al., 2014). Detailed rules and standards of calculation are explained in Supplementary Appendix S5.
Besides, Shojania et al. suggested that more than 50% of systematic reviews were outdated after 5.5 years (Shojania et al., 2007). Hence, if the gap between the year of publication of potential overlapping studies is >5 years or if meta-analysis only included studies published more than 15 years ago, the previous one would be excluded directly. Update of eligible reviews was recommended by Garner et al. (2016) and satisfied the following criterion: the review achieved a minimum rating of the Moderate AMSTAR score. We identified newly published studies that met the inclusion criteria and matched the keywords of previous studies; the outcomes from the newly published one would change the conclusion or credibility of the review.
Figure 1 (flowchart of literature search) shows the procedure for the literature search and selection of eligible studies. Overall, 736 unique records (excluded duplicates) were searched across 4 databases, and 292 full-text articles were screened in full text. After the preliminary screening, 154 meta-analyses met the inclusion criteria. Supplementary Appendix S5 describes citation matrices of CCA for reviews with overlapping associations. In all, 107 meta-analyses reported 25 overlapping topics. After removing overlapping and outdated reviews, 47 studies were included in our umbrella review with 319 unique outcomes. Supplementary Appendices S6,S7 show the characteristics of included studies and excluded studies with their reasons for exclusion. Supplementary Appendices S8,S9 show specific data of the detailed outcomes in Result and Discussion.
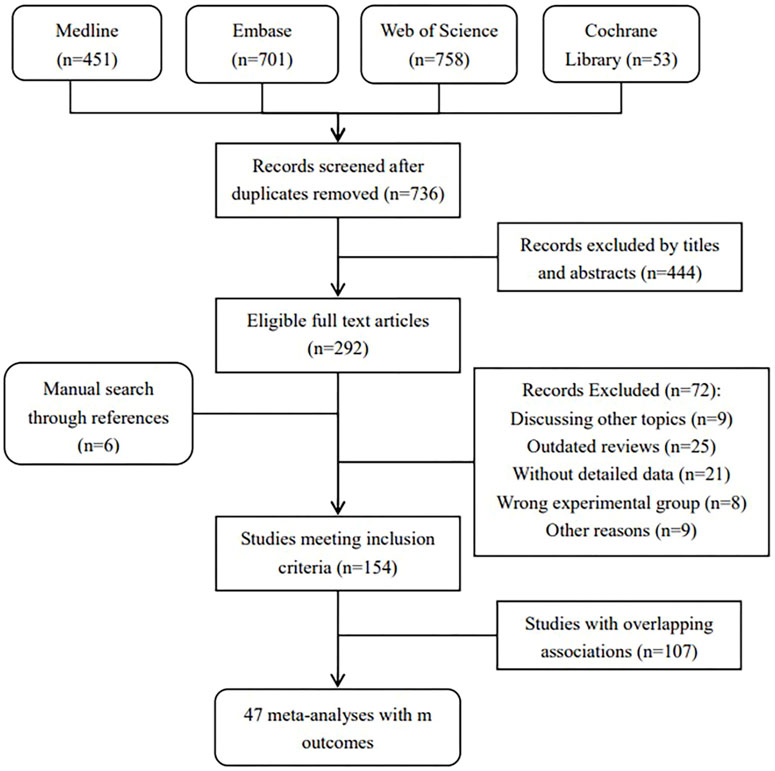
FIGURE 1. Flowchat of selection of included studies.
The included meta-analyses were divided into eight categories as per the types of surgery: joint replacement surgery, other orthopedic surgery, cerebral surgery, cardiac surgery, nasal surgery, obstetrics and gynecological surgery, other types of surgery, and complex antifibrinolytic agents. The 47 included studies were published from 2012 to 2022, and 42 of them were published within 6 years (2016 and later). A total of 45 of 47 studies were rated as High quality in AMSTAR, and the remaining two were rated as Moderate quality. All the studies of High quality were meta-analyses of RCTs. AMSTAR scores for individual studies included in the umbrella review are shown in Supplementary Appendix S10. Among 319 outcomes, there were 101 outcomes assessed as at least of Moderate quality by GRADE, and 58 of them were rated as High quality. GRADE classification of the quality of evidence is listed in Supplementary Appendix S11.
Blood loss, being the core outcome of our study, had complicated data for subgroup analysis. We divided outcomes into those of the WMD group and the SMD group. The WMD group included subgroups of total blood loss, intraoperative blood loss, and postoperative blood loss (see Table 1).
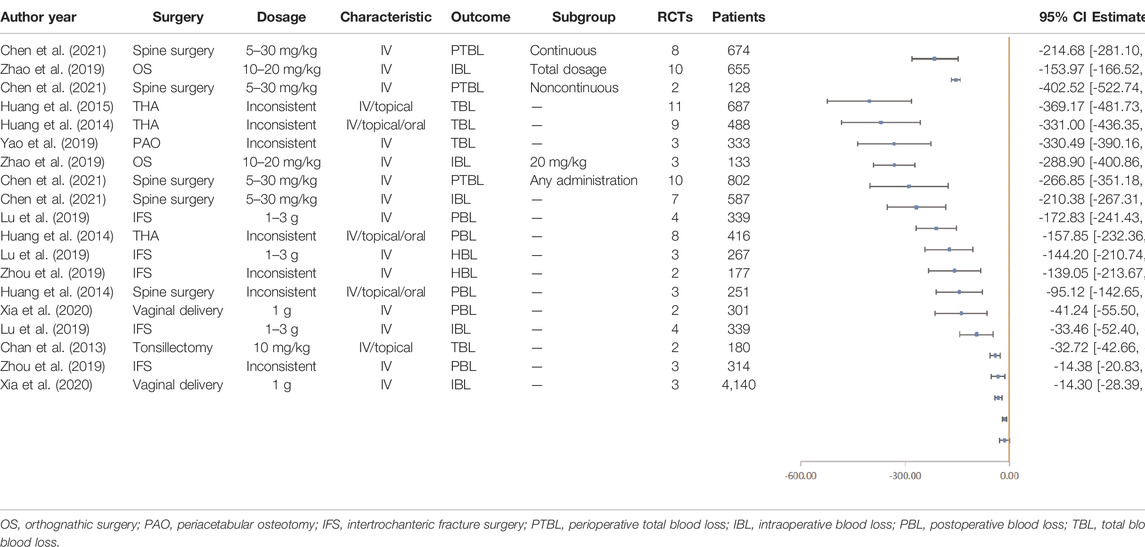
TABLE 1. High and moderate outcomes of blood loss (ml) with weighted mean difference (WMD).
Nine types of surgeries provided WMD outcomes with a relatively higher quality (at least Moderate GRADE), and two of them were High GRADE. IV TXA in spine surgery (WMD -214.68ml, 95% CI, -281.10 to -148.27) and orthognathic surgery (WMD -153.97ml, 95% CI, -166.52 to -141.41) could reduce perioperative bleeding and intraoperative bleeding, respectively (Zhao et al., 2019; Chen et al., 2021). Besides, Huang et al. (2015) reported that antifibrinolytic drugs could significantly reduce blood loss in THA (WMD -389.14, 95% CI, -483.95 to -295.23). In conclusion, TXA could effectively reduce blood loss and play a more significant role in major orthopedic surgery, including THA, TKA, and spine surgery.
As for subgroups, antifibrinolytic drugs could lead to a reduction of both intraoperative and postoperative blood loss (see Supplementary Appendix S12). A few studies that discussed SMD blood loss are shown in Supplementary Appendix S12d. IV TXA could significantly reduce intraoperative blood loss in endoscopic sinus surgery (SMD -0.66, 95% CI, –0.86 to -0.46) (Kim et al., 2019). Du and Feng concluded that IV or topical TXA could reduce intraoperative blood loss in spinal fusion surgery (SMD -0.32, 95% CI, -0.58 to -0.06) (Du and Feng, 2018).
Blood transfusion is an emergency treatment and could reflect the critical situation of the patient. In all, 14 surgeries provided outcomes with a relatively higher quality, and 16 outcomes were rated as High (see Tables 2, 3). According to 42 RCTs, Huang et al. (2014) concluded that TXA would reduce the transfusion rate in major orthopedic surgery by 49% (RR 0.51, 95% CI, 0.46–0.56). Besides, data from 31 RCTs demonstrated that IV or topical TXA in cardiac surgery could reduce the transfusion rate by 29% (RR 0.71, 95% CI, 0.65–0.78) (Guo et al., 2019). We also summarized incidences of adverse events containing seizure (a neurologic event), death, and vascular adverse events (see Table 4). Vascular adverse events included deep vein thrombosis (DVT), stroke, myocardial infarction (MI), and pulmonary embolism (PE). Five outcomes were rated as High. Zhang S. et al. (2019) reported that IV TXA could effectively reduce the rate of all adverse events in calcaneal fracture surgery (RR 0.26, 95% CI, 0.15–0.42). Li et al. indicated that IV antifibrinolytic drugs decreased the risk of DVT in spine surgery by 64%. Besides, TXA decreased the mortality of upper gastrointestinal bleeding by 41% (Twum-Barimah et al., 2020). In contrast, Guo et al. (2019) displayed that high-dose TXA increased the risk of seizure by nearly five times in cardiac surgery, and Zhang S. et al. (2019) also demonstrated an increased incidence of seizure by more than six times. Therefore, we concluded that TXA could reduce the transfusion rate and that TXA is also a protective factor from vascular adverse events and death, but it is a risk factor for seizures.
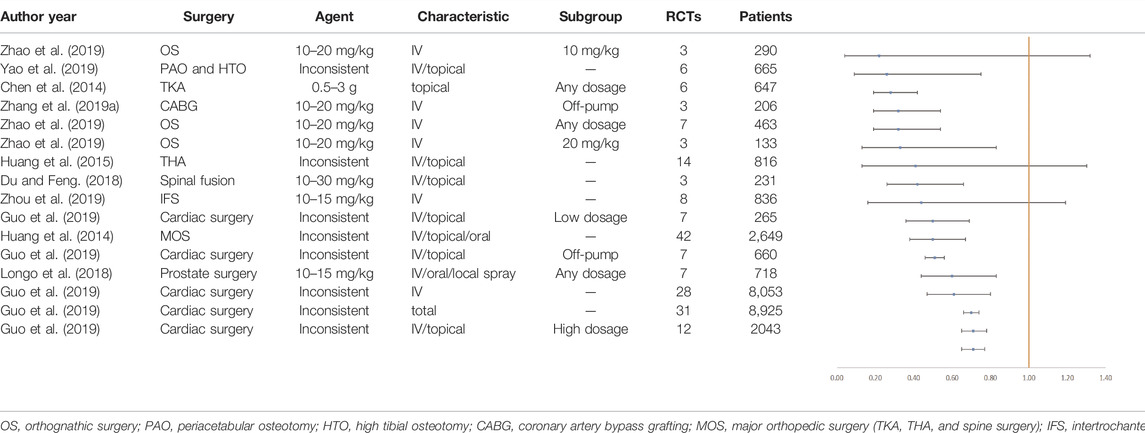
TABLE 2. Outcomes of the transfusion rate with high GRADE.
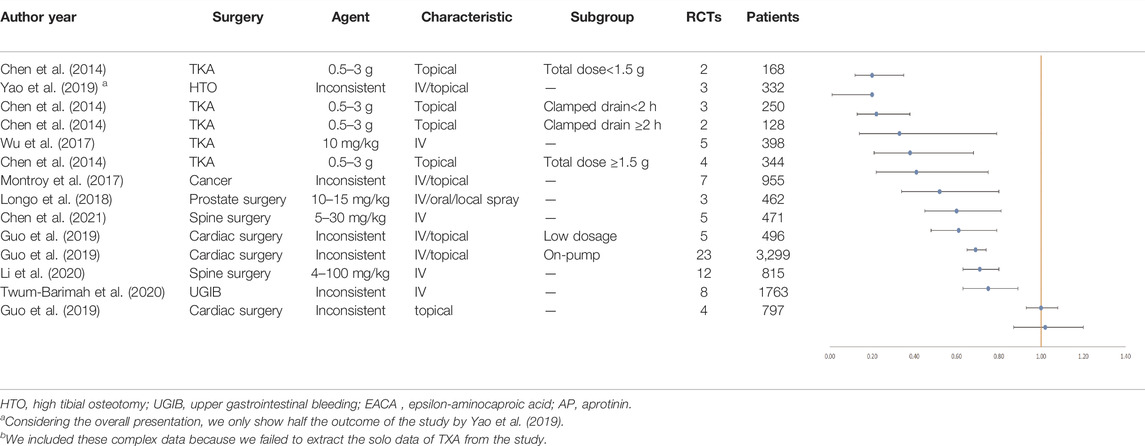
TABLE 3. Outcomes of the transfusion rate with moderate GRADE.
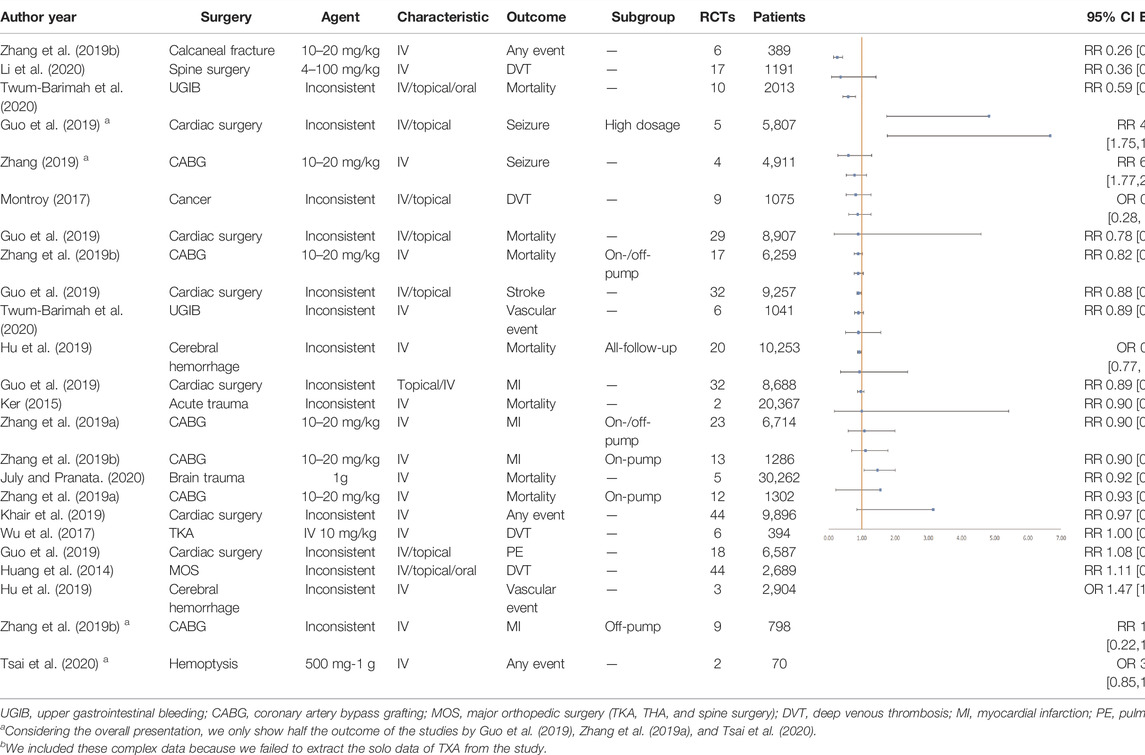
TABLE 4. Outcomes of adverse events with high or moderate GRADE.
We also evaluated outcomes of reoperation rate, operative time, length of hospital stay, and hemoglobin (Hb). Re-operation was the additional surgical intervention due to poor postoperative recovery. The reduction in the postoperative reoperation rate could avoid unnecessary pain and the economic burden on patients. As shown in Supplementary Appendix S13a, Zhang Y. et al. (2019) reported that IV TXA led to a 54% decrease in the reoperation rate in coronary artery bypass grafting (CABG) (RR 0.46, 95% CI, 0.31, 0.68). Similarly, Guo et al. (2019) showed that IV or topical TXA averts 38% of reoperation in cardiac surgery.
Besides, the operative time and length of hospital stay were also significantly shortened with TXA treatment (see Supplementary Appendix S13b,c). Zhao et al. demonstrated the decreasing operation time of orthognathic surgery with IV TXA (WMD -16.18, 95% CI, -19.60 to -12.75) (Zhao et al., 2019). Tsai et al. also reported that IV TXA could shorten the length of hospital stay for hemoptysis patients by 1.62 days (Tsai et al., 2020). These outcomes demonstrated the hemostatic effect of TXA, with faster postoperative recovery.
Furthermore, postoperative Hb outcomes have been displayed in Supplementary Appendix S14a,b. Chen et al. determined that the IV TXA group gained a higher Hb level after spine surgery (SMD 0.20, 95% CI, 0.02–0.38) (Chen et al., 2021). Yao et al. (2019) and Guo et al. (2018) also suggested that patients receiving TXA showed fewer Hb decreases. However, in terms of the coagulation function, there is no significant difference in partial thromboplastin time and prothrombin time (see Supplementary Appendix S14c).
We summarized the recommended application of TXA in different types of adult surgery after the overall data analysis. IV-combined topical TXA (1–1.5 g IV + 1–3 g topical) was recommended for joint replacement surgery, and 10–15 mg/kg IV TXA was recommended in spinal surgery. 10 mg/kg IV TXA was recommended for cardiac surgery, and 2 g IV TXA was recommended in cerebral hemorrhage. Other detailed data are presented in Table 5.
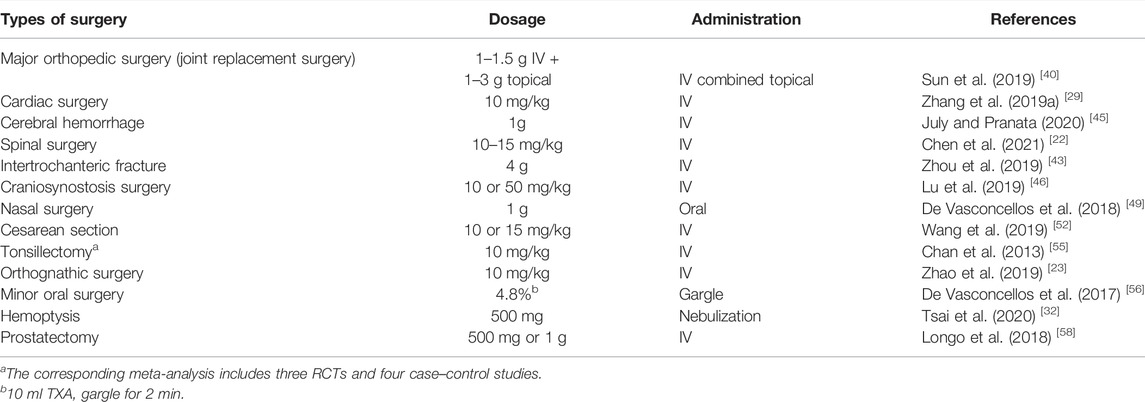
TABLE 5. Recommended dosage of TXA in different types of adult surgery.
We analyzed data from 47 meta-analyses and demonstrated that TXA effectively reduced blood loss and the transfusion rate in various surgeries. TXA resulted in a higher Hb level, shorter operative time and length of hospital stay, and a decreased rate of reoperation. Besides, TXA did not increase the risk of death and vascular adverse events, but it was a risk factor for seizure in cardiac surgery. Therefore, we believe that TXA is a safe choice for hemostasis in major surgeries, in particular with a high risk of allogeneic blood transfusion. We also recommended the dosage of TXA in different types of adult surgery.
A high dose of IV TXA and combined IV and topical TXA are recommended in joint replacement surgery. In terms of dosage, Chen et al. suggested that a high dose of IV TXA (30 mg/kg) was more effective than a low dose (15–20 mg/kg) in reducing blood loss without increasing the risk of DVT (Chen et al., 2014). However, the heterogeneity may come from selection biases: Sukeik et al. (2020), Chen et al., and Wu et al. (2017) mentioned that patients with a cardiovascular disease history and renal insufficiency were excluded, but Guo et al., Kirsch et al. (2017), and Li et al. (2020) did not. As for administration routes, detailed outcomes are displayed in Supplementary Appendix S15. Li’s research suggested topical usage: topical TXA reduced 33.38 ml more than IV TXA did on total blood loss (WMD 33.38, 95% CI, 19.24–47.51). However, Li et al. (2020) demonstrated insignificant differences in the blood transfusion rate and adverse effects. In addition, similar outcomes were found in oral and IV TXA for all aspects. However, it should be noted that combined IV and topical TXA would be better than a single route. Sun’s research showed that the combined group decreased 198.07 ml total blood loss (WMD -198.07, 95% CI, -307.67 to -88.46) and the blood transfusion rate was 60% less than that of the single route (RR 0.40, 95% CI, 0.24–0.68). Zhang H. et al. (2017) and Zhang H. et al. (2017) also reported similar outcomes preferring combined IV and topical TXA (see Supplementary Appendix S15b) (Zhang H. et al., 2017; Zhang XQ. et al., 2017).
Other types of orthopedic surgery were also included. As for spinal surgery, a starting dose of 10–15 mg/kg and a maintenance dose of 1.0–2.0 mg/(kg·h) were optimal in Chen’s study (Chen et al., 2021). Du and Feng (2018) demonstrated that intraoperative blood loss and postoperative blood loss were significantly reduced in adolescents with idiopathic scoliosis, but this could not be confirmed in lumbar pedicle subtraction osteotomy surgery. Besides, Zhou et al. (2019) concluded that 4 g TXA leads to the least amount of blood loss in femoral intertrochanteric fracture (WMD -570.8, 95% CI, -1071.04 to -70.56), which demonstrated that a larger dose corresponds to better effectiveness when under the premise of safety. Moreover, Zhang S. et al. (2019) reported that TXA could significantly reduce the incidence of postoperative incision complications in calcaneal fracture (RR 0.26, 95% CI, 0.15–0.42), which is common but inevitable.
Three meta-analyses of cerebral surgery were included. Hu et al. (2019) found that early TXA treatment (within 3 h) after cerebral hemorrhage was effective in reducing the incidence of deaths and hematoma (as well as the volume of hematoma) caused by cerebral trauma. However, delayed TXA treatment (beyond 3 h) would not benefit the patients. Therefore, they suggested that patients with acute cerebral hemorrhage should use TXA as soon as possible (<3 h). Similarly, July and Pranata (2020) also agreed that patients with acute brain injury <3 h or a mild to moderate Glasgow Coma Scale score would need early TXA treatment. In addition, the optimal dose of TXA remained controversial (50 mg/kg or 10 mg/kg) in craniosynostosis surgery, but Lu et al. (2019) demonstrated that both doses could significantly reduce blood transfusion.
In terms of cardiac surgery, we included three studies and summarized the following suggestions: low-dose IV TXA was the best choice, and it was unnecessary to exclude patients with renal impairment, coagulation dysfunction, or a history of thromboembolism. All these included studies indicated that high-dose TXA was significantly associated with the incidence of seizure (Joseph et al., 2018; Zhang S. et al., 2019; Khair et al., 2019). Guo et al. (2019) demonstrated that low-dose TXA (10 mg/kg) was sufficient to reduce blood transfusion requirements without increasing the risk of seizure, although high-dose TXA displayed less blood loss. In addition, Guo et al. (2019) found that topical TXA (whether combined with IV TXA or not) was not enough to reduce bleeding or the blood transfusion rate, and therefore, IV TXA was recommended in cardiac surgery.
According to the four included articles, different routes of administration had a similar hemostatic effect, and both oral and IV TXA were reliable in short-term surgical results and for thromboembolic complications (de Vasconcellos et al., 2018; Kim et al., 2019; Kang and Hwang, 2020). Due to the narrow scope of surgery in the nasal cavity, slight bleeding could distort the vision of the endoscope. TXA reduced intraoperative blood loss and improved the quality of the surgical field in endoscopic sinus surgery, thereby increasing the surgeon’s satisfaction and the success rate of the operation (Kim et al., 2019; Kang and Hwang, 2020). However, de Vasconcellos et al. (2018) reported that giving oral TXA (1 g) (WMD -61.70, 95% CI, –83.02 to –40.39) 2 h before rhinoplasty surgery reduced more intraoperative bleeding than IV TXA (10 mg/kg) (WMD –23.88, 95% CI, –45.19 to –2.58).
TXA has been used generally in cesarean section, vaginal delivery, and heavy menstrual bleeding (>80 ml blood loss per menstrual cycle). Wang’s study demonstrated that different doses (10 or 15 mg/kg) of TXA had similar effects in reducing blood loss and the transfusion rate in cesarean section (Wang et al., 2019). Wang also found that TXA significantly reduced the application of uterine tension agents (oxytocin and methylergometrine). In addition, according to Bryant-Smith’s study, TXA showed better efficacy than nonsteroidal anti-inflammatory drugs and progestogens (Bryant-Smith et al., 2018).
Besides, a study mainly involving orthopedics, obstetrics and gynecology, and maxillofacial and oral surgery showed the most common single preoperative dose is 15 mg/kg (Heyns et al., 2021).
We included a few operations that were difficult to be classified. Chan’s study indicated that 10 mg/kg IV TXA significantly reduced the average blood loss (−32.72 ml) and average bleeding time (−3.6 h) of tonsillectomy patients (Chan et al., 2013). Tonsils are rich in plasminogen, which may explain why anti-plasminogen TXA works well (Chan et al., 2013). In orthognathic surgery, Zhao et al. (2019) recommended 10 mg/kg IV TXA as the most effective dose for intraoperative bleeding reduction. Besides, de Vasconcellos et al. (2017) reported that flushing the surgical site with TXA (4.8%) and then gargling within 1 week after minor oral surgery could reduce the risk of bleeding in anticoagulant patients (RR 0.13, 95% CI, 0.03–0.45). However, no difference was found between TXA and the standard care group (gelatin sponge and sutures or dry gauze compression) (Engelen et al., 2018). As for prostatectomy, about 8% of patients have a blood loss of more than 2000 ml. According to Longo et al., 500 mg or 1 g TXA significantly reduced blood loss (SMD −1.93, 95% CI, −2.81 to −1.05) and the blood transfusion rate (RR 0.61, 95% CI, 0.47–0.80) (Longo et al., 2018). In addition, patients with hemoptysis were recommended for TXA (500 mg) treatment by Tsai et al. (2020). Nebulization of TXA was also helpful, which directly acts on the bleeding site and provides a beneficial hemostatic effect.
As a lysine analogue, TXA inhibits the activation of plasminogen by blocking the lysine binding site, which reduces the hydrolysis of fibrinogen and stabilizes the blood clot (Hunt, 2015). In addition to hemostasis, TXA has certain effects in other aspects. In rhinoplasty surgery, TXA reduces eyelid edema in the first week after surgery by decreasing interleukin-6 and acute-phase proteins (de Vasconcellos et al., 2018). Besides, TXA has an anti-inflammatory effect, where early use of TXA (<60min) can reduce endothelial cell apoptosis and necrosis (Diebel et al., 2017). TXA seems to reduce the incidence of incision complications, which could be seen in calcaneal fracture surgery (Zhang Y. et al., 2019).
TXA provides surgeons with new ideas for hemostasis in surgical operations and can also save blood transfusion. Attributed to its hemostatic and blood-saving effects, TXA is regarded as an excellent alternative therapy. Global demand and availability of blood products were studied by Roberts et al., and they found that 119 countries (61%) did not have enough blood supply to meet their needs. The gap between demand and supply was significant in many developing countries. They showed that the WHO target of 10–20 donations per 1,000 people was underestimated for many countries (Roberts et al., 2019). In addition, TXA is cheap enough to reduce the financial burden on patients. Kirsch et al. (2017) reported that $8,000 was saved per 100 patients undertaking TKA or THA treated with TXA. Besides, Lu et al. (2019) concluded that the cost of blood transfusion in open craniosynostosis surgery was estimated to be more than 100 pounds higher if TXA was not used. Moreover, with a half-life of 3 h, the strongest hemostatic effect appears in the first 24 h so that quick effect achieves the purpose of less medication and cost (Kirsch et al., 2017; Lu et al., 2019; Yao et al., 2019).
According to the included studies, TXA is proven as a protective factor against vascular adverse events. Furthermore, although pregnant women are in a state of hypercoagulability, no increased risk of DVT is revealed in vaginal delivery and cesarean section (Wang et al., 2019; Xia et al., 2020). In cardiac surgery, Khair et al. (2019) demonstrated that TXA could also be applied in patients with renal impairment, coagulation dysfunction, or a history of thromboembolism. Besides, a recent meta-analysis of 216 studies showed that regardless of dosage, IV TXA was not associated with an increased risk of any thromboembolic events (Taeuber et al., 2021).
Potential adverse events have limited the clinical application of TXA: high-dose TXA is a risk factor for seizure in cardiac surgery, which was shown in three studies (Zhang Y. et al., 2019; Guo et al., 2019; Khair et al., 2019). In particular, Guo’s subgroup analysis demonstrated a high risk of seizure in the high-dose TXA group (RR 4.83, 95% CI, 1.75 to 13.33) (Guo et al., 2019). Zufferey declared that low-dose TXA increased the risk of seizures by a factor of 1.2; meanwhile, the risk factor of high-dose TXA is 2 (Zufferey et al., 2021). A metaregression by Murao showed an increased risk of seizures with an increased dose of TXA (p = 0.011) (Murao et al., 2021). Another study also showed that the incidence of postoperative seizures in cardiac surgery increased from 0.5–1.0% to 6.4–7.3% after the application of high doses of TXA (Lecker et al., 2021). Stephan et al. had clearly demonstrated that TXA enhanced neuronal excitation by antagonizing inhibitory GABAergic neurotransmission via postsynaptic mechanisms (Kratzer et al., 2014). TXA, as a competitive antagonist, is structurally similar to glycine, which prevents the activation of glycine receptors and leads to the development of seizure (Lecker et al., 2012). Besides, isoflurane and the less effective propofol had been found useful in treating TXA-induced seizures, which guarantee the safety of high-dose TXA (Lecker et al., 2012).
This is the first umbrella review on the efficacy and safety of the application of TXA in surgeries. An umbrella review is a targeted compilation of evidence for various clinical-related questions on all health outcomes associated with a particular exposure. It is an ideal way of presenting a wide picture of the evidence related to an interesting question, and a higher methodological quality results in a more reliable conclusion. Precisely, in order to screen qualified results from these research studies and produce guidelines for clinical application of antifibrinolytic agents, we summarized the evidence produced to date and took a judicial, critical approach to the quality of these systematic reviews and meta-analyses. After the evaluation of AMSTAR, most of the included studies were of High quality. In addition, the studies we included are relatively updated, with 40 studies published after 2016.
However, limitations also exist: TXA may also be applied to other types of surgery, but they were not included in our umbrella review without related meta-analysis. Besides, the studies not written in English or Chinese are excluded, which provides potential bias. Furthermore, for the same outcome (such as blood loss), each meta-analysis has a different effect size, which may be a potential source of heterogeneity. However, we have tried our best to perform separate comparative studies without compromising the conclusion.
Our study demonstrates that TXA has a general hemostatic effect with very few adverse events, which indicates TXA is the recommended medication to prevent excessive bleeding and reduce the blood transfusion rate. We recommended different dosages of TXA for different types of adult surgery. However, we could not recommend a unified dosage for different surgeries due to the heterogeneity of the experimental design.
JnL was in charge of the main idea and was the guarantor of integrity of the entire clinical study. RL and YD were in charge of the study concepts, design, manuscript preparation, and editing. PH and JJL searched online databases. RL and YD independently screened the titles and abstracts. Articles satisfying the inclusion criteria were accessed for full-text review. SR and JJL independently extracted data from eligible articles. RL and JJL rated the methodological quality of the reviews. PH and SR were in charge of language polishing and grammar revision.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at https://www.frontiersin.org/articles/10.3389/fphar.2022.887386/full#supplementary-material
RCTs, randomized controlled trials; TXA, tranexamic acid; Hb, Hemoglobin; TKA, total knee arthroplasty; THA, total hip arthroplasty; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; WMD, weighted mean difference; SMD, standard mean difference; CI, confidence interval; OR, odds ratio; RR, relative risk; RD, risk difference; AMSTAR, assessing the methodological quality of systematic reviews; GRADE, Grading of Recommendations, Assessment, Development and Evaluation; CCA, corrected covered area; DVT, deep vein thrombosis; MI, myocardial infarction; PE, pulmonary embolism; CABG, coronary artery bypass grafting.
Aromataris, E., Fernandez, R. S., Godfrey, C., Holly, C., Khalil, H., and Tungpunkom, P. (2014). Methodology for JBI Umbrella Reviews. Adelaide: Joanna Briggs Inst Rev Man, 1–34. Availableat: https://ro.uow.edu.au/smhpapers/3344.
Bryant-Smith, A. C., Lethaby, A., Farquhar, C., and Hickey, M. (2018). Antifibrinolytics for Heavy Menstrual Bleeding. Cochrane Database Syst. Rev. 4 (4), CD000249. doi:10.1002/14651858.CD000249
Chan, C. C., Chan, Y. Y., and Tanweer, F. (2013). Systematic Review and Meta-Analysis of the Use of Tranexamic Acid in Tonsillectomy. Eur. Arch. Otorhinolaryngol. 270 (2), 735–748. doi:10.1007/s00405-012-2184-3
Chen, J. P., Li, K., Chen, Q., Guo, H. R., Zhang, Y. B., and Wei, B. (2021). Meta-analysis of the Efficacy and Safety of Tranexamic Acid in Open Spinal Surgery. Zhongguo Zuzhi Gongcheng Yanjiu 25 (9), 1458–1464. doi:10.3969/j.issn.2095-4344.3765
Chen, Z. Y., Gao, Y., Chen, W., Liu, Y. J., and Zhang, Y. Z. (2014). Reduced Blood Loss after Intra-articular Tranexamic Acid Injection during Total Knee Arthroplasty: a Meta-Analysis of the Literature. Knee Surg. Sports Traumatol. Arthrosc. 22 (12), 3181–3190. doi:10.1007/s00167-013-2814-3
de Vasconcellos, S. J., de Santana Santos, T., Reinheimer, D. M., Faria-E-Silva, A. L., de Melo, M. F., and Martins-Filho, P. R. (2017). Topical Application of Tranexamic Acid in Anticoagulated Patients Undergoing Minor Oral Surgery: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. J. Craniomaxillofac. Surg. 45 (1), 20–26. doi:10.1016/j.jcms.2016.10.001
de Vasconcellos, S. J. A., do Nascimento-Júnior, E. M., de Aguiar Menezes, M. V., Tavares Mendes, M. L., de Souza Dantas, R., and Martins-Filho, P. R. S. (2018). Preoperative Tranexamic Acid for Treatment of Bleeding, Edema, and Ecchymosis in Patients Undergoing Rhinoplasty: A Systematic Review and Meta-Analysis. JAMA Otolaryngol. Head Neck Surg. 144 (9), 816–823. doi:10.1001/jamaoto.2018.1381
Diebel, L. N., Martin, J. V., and Liberati, D. M. (2017). Early Tranexamic Acid Administration Ameliorates the Endotheliopathy of Trauma and Shock in an In Vitro Model. J. Trauma Acute Care Surg. 82 (6), 1080–1086. doi:10.1097/TA.0000000000001445
Du, Y., and Feng, C. (2018). The Efficacy of Tranexamic Acid on Blood Loss from Lumbar Spinal Fusion Surgery: A Meta-Analysis of Randomized Controlled Trials. World Neurosurg. 119, e228–234. doi:10.1016/j.wneu.2018.07.120
Engelen, E. T., Schutgens, R. E., Mauser-Bunschoten, E. P., van Es, R. J., and van Galen, K. P. (2018). Antifibrinolytic Therapy for Preventing Oral Bleeding in People on Anticoagulants Undergoing Minor Oral Surgery or Dental Extractions. Cochrane Database Syst. Rev. 7 (7), CD012293. doi:10.1002/14651858.CD012293
Etchason, J., Petz, L., Keeler, E., Calhoun, L., Kleinman, S., Snider, C., et al. (1995). The Cost Effectiveness of Preoperative Autologous Blood Donations. N. Engl. J. Med. 332 (11), 719–724. doi:10.1056/NEJM199503163321106
Ferraris, V. A., Ferraris, V. A., Brown, J. R., Despotis, G. J., Hammon, J. W., and Reece, T. B. (2011). Update to the Society of Thoracic Surgeons and the Society of Cardiovascular Anesthesiologists Blood Conservation Clinical Practice Guidelines. Ann. Thorac. Surg. 91 (3), 944–982. doi:10.1016/j.athoracsur.2010.11.078
Garner, P., Hopewell, S., Chandler, J., MacLehose, H., Schünemann, H., Akl, E., et al. (2016). Panel for Updating Guidance for Systematic Reviews (PUGs). When and How to Update Systematic Reviews: Consensus and Checklist. BMJ 354, i3507. doi:10.1136/bmj.i3507
Guo, J., Gao, X., Ma, Y., Lv, H., Hu, W., Zhang, S., et al. (2019). Different Dose Regimes and Administration Methods of Tranexamic Acid in Cardiac Surgery: a Meta-Analysis of Randomized Trials. BMC Anesthesiol 19 (1), 129. doi:10.1186/s12871-019-0772-0
Guo, P., He, Z., Wang, Y., Gao, F., Sun, W., Guo, W., et al. (2018). Efficacy and Safety of Oral Tranexamic Acid in Total Knee Arthroplasty: A Systematic Review and Meta-Analysis. Medicine (Baltimore) 97 (18), e0587. doi:10.1097/MD.0000000000010587
Guyatt, G., Oxman, A. D., Akl, E. A., Kunz, R., Vist, G., Brozek, J., et al. (2011). GRADE Guidelines: 1. Introduction GRADE Evidence Profiles and Summary of Findings Tables. J. Clin. Epidemiol. 64, 383–394. doi:10.1016/j.jclinepi.2010.04.026
Henry, D. A., Carless, P. A., Moxey, A. J., O'Connell, D., Stokes, B. J., McClelland, B., et al. (2011). Anti-fibrinolytic Use for Minimising Perioperative Allogeneic Blood Transfusion. Cochrane Database Syst. Rev. 2011 (3), CD001886. doi:10.1002/14651858.CD001886
Heyns, M., Knight, P., Steve, A. K., and Yeung, J. K. (2021). A Single Preoperative Dose of Tranexamic Acid Reduces Perioperative Blood Loss: A Meta-Analysis. Ann. Surg. 273 (1), 75–81. doi:10.1097/SLA.0000000000003793
Hu, W., Xin, Y., Chen, X., Song, Z., He, Z., and Zhao, Y. (2019). Tranexamic Acid in Cerebral Hemorrhage: A Meta-Analysis and Systematic Review. CNS Drugs 33 (4), 327–336. doi:10.1007/s40263-019-00608-4
Huang, F., Wu, D., Ma, G., Yin, Z., and Wang, Q. (2014). The Use of Tranexamic Acid to Reduce Blood Loss and Transfusion in Major Orthopedic Surgery: a Meta-Analysis. J. Surg. Res. 186 (1), 318–327. doi:10.1016/j.jss.2013.08.020
Huang, F., Wu, Y., Yin, Z., Ma, G., and Chang, J. (2015). A Systematic Review and Meta-Analysis of the Use of Antifibrinolytic Agents in Total Hip Arthroplasty. Hip Int. 25 (6), 502–509. doi:10.5301/hipint.5000285
Hunt, B. J. (2015). The Current Place of Tranexamic Acid in the Management of Bleeding. Anaesthesia 70 (1), 50–53. doi:10.1111/anae.12910
Joseph, J., Martinez-Devesa, P., Bellorini, J., and urton, M. J. (2018). Tranexamic Acid for Patients with Nasal Haemorrhage (Epistaxis). Cochrane Database Syst. Rev. 12 (12), CD004328. doi:10.1002/14651858.CD004328
July, J., and Pranata, R. (2020). Tranexamic Acid Is Associated with Reduced Mortality, Hemorrhagic Expansion, and Vascular Occlusive Events in Traumatic Brain Injury - Meta-Analysis of Randomized Controlled Trials. BMC Neurol. 20 (1), 119. doi:10.1186/s12883-020-01694-4
Kang, H., and Hwang, S. H. (2020). Does Topical Application of Tranexamic Acid Reduce Intraoperative Bleeding in Sinus Surgery during General Anesthesia? Braz. J. Otorhinolaryngol. 86 (1), 111–118. doi:10.1016/j.bjorl.2019.08.006
Khair, S., Perelman, I., Yates, J., Taylor, J., Lampron, J., Tinmouth, A., et al. (2019). Exclusion Criteria and Adverse Events in Perioperative Trials of Tranexamic Acid in Cardiac Surgery: a Systematic Review and Meta-Analysis. Can. J. Anaesth. 66 (10), 1240–1250. doi:10.1007/s12630-019-01393-w
Kim, D. H., Kim, S., Kang, H., Jin, H. J., and Hwang, S. H. (2019). Efficacy of Tranexamic Acid on Operative Bleeding in Endoscopic Sinus Surgery: A Meta-Analysis and Systematic Review. Laryngoscope 129 (4), 800–807. doi:10.1002/lary.27766
Kirsch, J. M., Bedi, A., Horner, N., Wiater, J. M., Pauzenberger, L., Koueiter, D. M., et al. (2017). Tranexamic Acid in Shoulder Arthroplasty: A Systematic Review and Meta-Analysis. JBJS Rev. 5 (9), e3. doi:10.2106/JBJS.RVW.17.00021
Kratzer, S., Irl, H., Mattusch, C., Bürge, M., Kurz, J., Kochs, E., et al. (2014). Tranexamic Acid Impairs γ-aminobutyric Acid Receptor Type A-Mediated Synaptic Transmission in the Murine Amygdala: a Potential Mechanism for Drug-Induced Seizures? Anesthesiology 120 (3), 639–649. doi:10.1097/ALN.0000000000000103
Lecker, I., Wang, D. S., Romaschin, A. D., Peterson, M., Mazer, C. D., and Orser, B. A. (2012). Tranexamic Acid Concentrations Associated with Human Seizures Inhibit glycine Receptors. J. Clin. Invest. Dec. 122 (12), 4654–4666. doi:10.1172/JCI63375
Lecker, I., Wang, D. S., Whissell, P. D., Avramescu, S., Mazer, C. D., and Orser, B. A. (2021). Tranexamic Acid-Associated Seizures: Causes and Treatment. Ann. Neurol. 79 (1), 18–26. doi:10.1002/ana.24558
Li, J., Liu, R., Rai, S., Ze, R., Tang, X., and Hong, P. (2020). Intra-articular vs. Intravenous Administration: a Meta-Analysis of Tranexamic Acid in Primary Total Knee Arthroplasty. J. Orthop. Surg. Res. 215 (1), 581. doi:10.1186/s13018-020-02119-1
Longo, M. A., Cavalheiro, B. T., and de Oliveira Filho, G. R. (2018). Systematic Review and Meta-Analyses of Tranexamic Acid Use for Bleeding Reduction in Prostate Surgery. J. Clin. Anesth. 48, 32–38. doi:10.1016/j.jclinane.2018.04.014
Lu, V. M., Goyal, A., and Daniels, D. J. (2019). Tranexamic Acid Decreases Blood Transfusion Burden in Open Craniosynostosis Surgery without Operative Compromise. J. Craniofac. Surg. 30 (1), 120–126. doi:10.1097/SCS.0000000000004875
Moher, D., Liberati, A., Tetzlaff, J., and Altman, D. G.PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA Statement. J. Clin. Epidemiol. 62, 1006–1012. doi:10.1371/journal.pmed.1000097
Murao, S., Nakata, H., Roberts, I., and Yamakawa, K. (2021). Effect of Tranexamic Acid on Thrombotic Events and Seizures in Bleeding Patients: a Systematic Review and Meta-Analysis. Crit. Care 25 (1), 380. doi:10.1186/s13054-021-03799-9
Murray, D. (2004). Acute Normovolemic Hemodilution. Eur. Spine J. 13 (1), S72–S75. doi:10.1007/s00586-004-0755-8
Nakanishi, K., Kanda, M., and Kodera, Y. (2019). Long-lasting Discussion: Adverse Effects of Intraoperative Blood Loss and Allogeneic Transfusion on Prognosis of Patients with Gastric Cancer. World J. Gastroenterol. 25 (22), 2743–2751. doi:10.3748/wjg.v25.i22.2743
Novikova, N., Hofmeyr, G. J., and Cluver, C. (2015). Tranexamic Acid for Preventing Postpartum Haemorrhage. Cochrane Database Syst. Rev. (6), CD007872. doi:10.1186/s12884-019-2718-4
Pieper, D., Antoine, S-L., Mathes, T., Neugebauer, E. A., and Eikermann, M. (2014). Systematic Review Finds Overlapping Reviews Were Not Mentioned in Every Other Overview. J. Clin. Epidemiol. 67, 368–375. doi:10.1016/j.jclinepi.2013.11.007
Pinto, M. A., Chedid, M. F., Sekine, L., Schmidt, A. P., Capra, R. P., Prediger, C., et al. (2019). Intraoperative Cell Salvage with Autologous Transfusion in Liver Transplantation. World J. Gastrointest. Surg. 11 (1), 11–18. doi:10.4240/wjgs.v11.i1.11
Roberts, N., James, S., Delaney, M., and Fitzmaurice, C. (2019). The Global Need and Availability of Blood Products: a Modelling Study. Lancet Haematol. 6 (12), e606–615. doi:10.1016/S2352-3026(19)30200-5
Rossaint, R., Bouillon, B., Cerny, V., Coats, T. J., Duranteau, J., Fernández-Mondéjar, E., et al. (2016). The European Guideline on Management of Major Bleeding and Coagulopathy Following Trauma: Fourth Edition. Crit. Care 20, 100. doi:10.1186/s13054-016-1265-x
Shea, B. J., Reeves, B. C., Wells, G., Thuku, M., Hamel, C., Moran, J., et al. (2017). AMSTAR 2: a Critical Appraisal Tool for Systematic Reviews that Include Randomised or Non-randomised Studies of Healthcare Interventions, or Both. BMJ 358, j4008. doi:10.1136/bmj.j4008
Shojania, K. G., Sampson, M., Ansari, M. T., Ji, J., Doucette, S., and Moher, D. (2007). How Quickly Do Systematic Reviews Go Out of Date? A Survival Analysis. Ann. Intern. Med. 147, 224–233. doi:10.7326/0003-4819-147-4-200708210-00179
Sterne, J. A., Gavaghan, D., and Egger, M. (2000). Publication and Related Bias in Meta-Analysis: Power of Statistical Tests and Prevalence in the Literature. J. Clin. Epidemiol. 53, 1119–1129. doi:10.1016/S0895-4356(00)00242-0
Stroup, D. F., Berlin, J. A., Morton, S. C., Olkin, I., Williamson, G. D., Rennie, D., et al. (2000). Meta-analysis of Observational Studies in Epidemiology - a Proposal for Reporting. JAMA 283, 2008–2012. doi:10.1001/jama.283.15.2008
Sukeik, M., Alshryda, S., Powell, J., and Haddad, F. S. (2020). The Effect of Tranexamic Acid on Wound Complications in Primary Total Hip Arthroplasty: A Meta-Analysis. Surgeon 18 (1), 53–61. doi:10.1016/j.surge.2019.05.003
Sun, Q., Li, J., Chen, J., Zheng, C., Liu, C., and Jia, Y. (2019). Comparison of Intravenous, Topical or Combined Routes of Tranexamic Acid Administration in Patients Undergoing Total Knee and Hip Arthroplasty: a Meta-Analysis of Randomised Controlled Trials. BMJ Open 9 (1), e024350. doi:10.1136/bmjopen-2018-024350
Taeuber, I., Weibel, S., Herrmann, E., Neef, V., Schlesinger, T., Kranke, P., et al. (2021). Association of Intravenous Tranexamic Acid with Thromboembolic Events and Mortality: A Systematic Review, Meta-Analysis, and Meta-Regression. JAMA Surg. 156 (6), e210884. doi:10.1001/jamasurg.2021.0884
Tsai, Y. S., Hsu, L. W., Wu, M. S., Chen, K. H., and Kang, Y. N. (2020). Effects of Tranexamic Acid on Hemoptysis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin. Drug Investig. 40 (9), 789–797. doi:10.1007/s40261-020-00946-y
Twum-Barimah, E., Abdelgadir, I., Gordon, M., and Akobeng, A. K. (2020). Systematic Review with Meta-Analysis: the Efficacy of Tranexamic Acid in Upper Gastrointestinal Bleeding. Aliment. Pharmacol. Ther. 51 (11), 1004–1013. doi:10.1111/apt.15761
Wang, Y., Liu, S., and He, L. (2019). Prophylactic Use of Tranexamic Acid Reduces Blood Loss and Transfusion Requirements in Patients Undergoing Cesarean Section: A Meta-Analysis. J. Obstet. Gynaecol. Res. 45 (8), 1562–1575. doi:10.1111/jog.14013
Wu, Y., Yang, T., Zeng, Y., Si, H., Cao, F., and Shen, B. (2017). Tranexamic Acid Reduces Blood Loss and Transfusion Requirements in Primary Simultaneous Bilateral Total Knee Arthroplasty: a Meta-Analysis of Randomized Controlled Trials. Blood Coagul. Fibrinolysis 28 (7), 501–508. doi:10.1097/MBC.0000000000000637
Wu, Y. G., Zeng, Y., Hu, Q. S., Bao, X. C., Xiong, H. Z., and Shen, B. (2018). Tranexamic Acid Plus Low-Dose Epinephrine Reduces Blood Loss in Total Knee Arthroplasty: A Systematic Review and Meta-Analysis. Orthop. Surg. 10 (4), 287–295. doi:10.1111/os.12404
Xia, Y., Griffiths, B. B., and Xue, Q. (2020). Tranexamic Acid for Postpartum Hemorrhage Prevention in Vaginal Delivery: A Meta-Analysis. Medicine (Baltimore) 99 (3), e18792. doi:10.1097/MD.0000000000018792
Yao, R. Z., Gao, W. Q., Wang, B. W., Wang, G. L., Wu, C. X., and A-Mu Yd, (2019). Efficacy and Safety of Tranexamic Acid in Reducing Blood Loss of Lower Extremity Osteotomy in Peri-Acetabulum and High Tibia: A Systematic Review and Meta-Analysis. Orthop. Surg. 11 (4), 545–551. doi:10.1111/os.12515
Zhang, H., He, G., Zhang, C., Xu, B., Wang, X., and Zhang, C. (2017a). Is Combined Topical and Intravenous Tranexamic Acid superior to Intravenous Tranexamic Acid Alone for Controlling Blood Loss after Total Hip Arthroplasty?: A Meta-Analysis. Medicine (Baltimore) 96 (21), e6916. doi:10.1097/MD.0000000000006916
Zhang, S., Ge, W. L., Li, C., Han, S. C., Wang, G., and en, W. J. (2019b). Efficacy and Safety of Intravenous Tranexamic Acid in the Operative Treatment of Calcaneal Fractures: a Meta-Analysis. Zhongguo Zuzhi Gongcheng Yanjiu 23 (20), 3268–3274. doi:10.3969/j.issn.2095-4344.3765
Zhang, X. Q., Ni, J., and Ge, W. H. (2017b). Combined Use of Intravenous and Topical versus Intravenous Tranexamic Acid in Primary Total Joint Arthroplasty: A Meta-Analysis of Randomized Controlled Trials. Int. J. Surg. 38, 15–20. doi:10.1016/j.ijsu.2016.11.136
Zhang, Y., Bai, Y., Chen, M., Zhou, Y., Yu, X., Zhou, H., et al. (2019a). The Safety and Efficiency of Intravenous Administration of Tranexamic Acid in Coronary Artery Bypass Grafting (CABG): a Meta-Analysis of 28 Randomized Controlled Trials. BMC Anesthesiol 19 (1), 104. doi:10.1186/s12871-019-0761-3
Zhao, H., Liu, S., Wu, Z., Zhao, H., and Ma, C. (2019). Comprehensive Assessment of Tranexamic Acid during Orthognathic Surgery: A Systematic Review and Meta-Analysis of Randomized, Controlled Trials. J. Craniomaxillofac. Surg. 47 (4), 592–601. doi:10.1016/j.jcms.2019.01.021
Zhou, X. D., Li, J., Fan, G. M., Huang, Y., and Xu, N. W. (2019). Efficacy and Safety of Tranexamic Acid in Elderly Patients with Intertrochanteric Fracture: An Updated Meta-Analysis. World J. Clin. Cases 7 (11), 1302–1314. doi:10.12998/wjcc.v7.i11.1302
Keywords: umbrella review, meta-analysis, antifibrinolytic agent, tranexamic acid, blood transfusion, hemostasis
Citation: Hong P, Liu R, Rai S, Liu J, Ding Y and Li J (2022) Does Tranexamic Acid Reduce the Blood Loss in Various Surgeries? An Umbrella Review of State-of-the-Art Meta-Analysis. Front. Pharmacol. 13:887386. doi: 10.3389/fphar.2022.887386
Received: 01 March 2022; Accepted: 14 April 2022;
Published: 19 May 2022.
Edited by:
Daniela Calina, University of Medicine and Pharmacy of Craiova, RomaniaReviewed by:
Kurt Neumann, Independent Researcher, Kerékteleki, HungaryCopyright © 2022 Hong, Liu, Rai, Liu, Ding and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuhong Ding, ZGluZ3loMDBAZm94bWFpbC5jb20=; Jin Li, bGlqaW4yMDAzd2h4aEBmb3htYWlsLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.