
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol., 17 May 2022
Sec. Drugs Outcomes Research and Policies
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.876955
This article is part of the Research TopicMedication Safety and Interventions to Reduce Patient Harm in Low- and Middle-Income CountriesView all 20 articles
 Farman Ullah Khan1,2,3,4,5
Farman Ullah Khan1,2,3,4,5 Amjad Khan5
Amjad Khan5 Faiz Ullah Khan1,2,3,4
Faiz Ullah Khan1,2,3,4 Khezar Hayat1,2,3,4,6
Khezar Hayat1,2,3,4,6 Asim ur. Rehman5
Asim ur. Rehman5 Jie Chang1,2,3,4
Jie Chang1,2,3,4 Waseem Khalid7Sidra Noor7
Waseem Khalid7Sidra Noor7 Asad Khan8
Asad Khan8 Yu Fang1,2,3,4*
Yu Fang1,2,3,4*Background: Multidrug-resistant tuberculosis (MDR-TB) is a growing public health problem. Treatment regimens used against MDR-TB are costly, prolonged, and associated with more side effects as compared with the drug-susceptible tuberculosis. This study was framed to determine the incidence of adverse drug events, risk factors, and their management in MDR-TB patients.
Methods: This prospective follow-up cohort study was conducted at the site of programmatic management of drug-resistant TB located at the Pakistan Institute of Medical Sciences, Islamabad. All patients, irrespective of their age, gender, and ethnicity, were included in the study. Adverse drug events were observed in patients at different time points during the study. Patients enrolled for the treatment from January 2018 were prospectively followed till December 2020 up to their end treatment outcomes.
Results: Out of 126 MDR-TB patients enrolled for treatment, 116 met the inclusion criteria and were included in the final analysis. Most patients (50.9%) were between 18 and 45 years of age. A minimum of one adverse event was experienced by (50.9%) patients. Of all the adverse events, gastrointestinal disorders were more frequent (47.4%), followed by arthralgia (28.4%) and psychiatric disturbance (20.6%). Furthermore, multivariate analysis showed a significant association with the incidence of adverse events in patients with age group above 60 years (odds ratio (OR) 4.50; 95% CI 1.05-19.2), active smokers (OR 4.20; 95% CI 1.31-13.4), delayed reporting to the TB center (OR 4.03; 95% CI 1.34-12.1), and treatment without bedaquiline regime (OR 3.54; 95% CI 1.23-10.1). Most of the patients (94.6%), counseled by the pharmacist, were found to be satisfied with the information provided and looked for more pharmacist counseling opportunities in the management of MDR-TB.
Conclusion: Current findings recommend that ADEs might be well managed by timely identification and reporting. Bedaquiline coupled with other active medications lowered the chance of ADEs in MDR-TB patients. Elderly patients, active smoking behavior, and those who have a delay in the treatment initiation are more prone to ADEs. Clinical pharmacist’s contribution to TB control programs may help caregivers and patients concerning the rational use of medication, early detection, and management of ADEs.
The emergence and spread of multidrug-resistant tuberculosis (MDR-TB) poses significant challenges to the control and successful eradication of TB, particularly in developing countries (Iradukunda et al., 2021). Despite all the efforts made throughout the world by the WHO, the treatment success rate for MDR-TB is still low. The WHO targets a success rate of at least 75% for MDR-TB patients; however, the most recent statistics on treatment outcomes indicate a success rate of 56% (Baluku et al., 2021; Yang et al., 2017). This is mainly because the MDR-TB therapy is costly, has low efficacy, and has more adverse drug events when compared to drug-susceptible TB (Baluku et al., 2021). One of the factors causing MDR-TB is non-compliance to the anti-MDR-TB treatment regimen. The most important independent factor underlying non-compliance to treatment is adverse events of medications (Resende and Santos-Neto, 2015; Merid et al., 2019; Sankar et al., 2021). The overall incidence of ADEs caused by anti-TB medications ranges from 5.1% to 83.5% in different populations (Kefale et al., 2020). ADEs increase patient suffering and increase substantial additional costs because of added outpatient visits, laboratory investigations, and hospitalizations, in more serious instances (Resende and Santos-Neto, 2015). Despite these difficulties, up to 80% of the treatment results can be achieved by effectively treating MDR-TB patients. Most ADEs can be controlled with over-the-counter and commonly prescribed medications. If the ADEs are mild, then proceeding with supplementary medications may be helpful (Trubnikov et al., 2021). In some cases, ADEs disappear over time and patients should be encouraged to tolerate them until the effects subside. Studies have shown that multidrug regimens can cause numerous ADEs such as nausea, vomiting, diarrhea, skin reaction, ototoxicity, peripheral neuropathy, psychiatric symptoms, nephrotoxicity, impaired vision, and hypothyroidism (Bezu et al., 2014; Merid et al., 2019).
Pakistan ranked the highest for MDR-TB burden in EMRO (Eastern Mediterranean Region of the WHO) and fourth highest country in the world (WHO, 2018; NTP, 2020). Drug-resistant tuberculosis is becoming more common in Pakistan, which highlights the need for efficient treatment regimens for MDR/XDR-TB (Javaid et al., 2018). Despite being the country with the highest burden of MDR-TB in EMRO, there is little information available about the management of adverse effects and treatment outcomes of patients with MDR-TB in Pakistan. To attain the 2025 goal of complete elimination of TB, a better understanding of the ADE of all drugs used to treat MDR-TB is an important and much-needed step in improving patient management and treatment outcomes. Therefore, close monitoring of patients is important to ensure that the ADEs are timely reported and managed. Clinical pharmacists providing pharmaceutical care services have been shown to improve adherence to therapy and reduce potential ADEs. More data on their characteristics and management are very valuable for clinicians and pharmacists. Therefore, this study was framed to determine the incidence, risk factors, and management of adverse events encountered in clinical practice.
This prospective case series analysis was carried out at the unit for programmatic management of drug-resistant TB (PMDT) located in the Pakistan Institute of Medical Sciences, Islamabad. Doctors, nurses, data operators, coordinators, pharmacists, psychologists, and other support personnel work at the research site to help MDR-TB patients achieve a treatment success rate of 75%.
Patients enrolled for the treatment from January 2018 were followed from the baseline visit. Those registered before 2018 and still on treatment were retrospectively followed till January 2018. Afterward, all the enrolled patients were prospectively followed till December 2020 up to their end treatment outcomes. All MDR-TB patients, irrespective of their age, gender, and ethnicity, were included in the study, while the multidrug-resistant cases those were transferred out from the study center or were still on the treatment medications during the final day of analysis were excluded.
Based on WHO guidelines for the treatment of MDR-TB and previous research, a standardized data-collecting form was developed. The supervisory committee and healthcare personnel at the study site also provided input. The patients were first assessed for symptoms at baseline and then reviewed and evaluated on a monthly basis by the doctor. Once the screening tests at baseline were completed, the MDR-TB patients were enrolled to be treated with the treatment regimen according to the NTP guidelines. All the drugs were provided at their maximum prescribed dosage, which were determined by the patient body weight. The treatment of all the patients after sputum culture conversion was continued for a minimum of 18 months. The patients were closely monitored during the follow-up visits to assess the ADEs Table 1. Specialist clinicians, pharmacists, and data coordinators reviewed every patient once a month to make sure their treatment was as effective as possible. All the patients were being assessed on a monthly basis and were treated as outpatients. To ensure adherence to the treatment, the patients were monitored by trained treatment supporters.
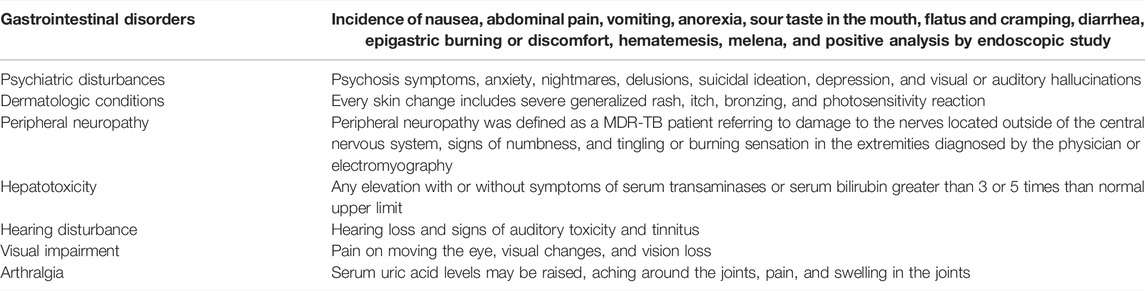
TABLE 1. Definition of side effects.
Patients found resistant in the Xpert MTB/RIF diagnostic test were registered as MDR-TB cases and treated with a regimen proposed by the WHO and National TB guidelines (WHO, 2012; WHO, 2014). Baseline laboratory tests, such as complete blood count, hepatitis, HIV, blood sugar level, kidney and liver function tests, urine routine test, and thyroid function test were conducted prior to the start of the treatment. AEs were recorded after laboratory test confirmation, and only those AEs that had at least one abnormal value were considered significant. As a requirement of PMDT, on each visit, ADEs were documented based on laboratory results, self-recorded by patients, or monitored by doctors and pharmacists. All patients were assessed for scheduled follow-up visits. Moreover, free laboratory tests and medications were provided, and both patients and treatment supporters were provided with nutritional and transport allowance support.
During corona virus infectious disease (COVID-19) pandemic, protocol of the National TB Control Program (NTP) for the protection from COVID-19 was strictly followed for both patients and healthcare professionals (NTP, 2020). According to the instruction of the NTP, an isolated triage area was assigned for all patients to separate them from suspected and non-suspected COVID-19 patients. Appropriate digital and telecommunication support were provided to the patients to ensure communication if they want any consultation for the management of ADEs caused by anti-MDR-TB treatment.
According to WHO guidelines, treatment outcomes are classified as successful when the TB patient finalizes the treatment medication to indicate cure and completion, while unsuccessful treatment outcomes are classified as treatment failure, treatment defaulters, and died patients (WHO, 2021). This study assessed patients’ satisfaction with pharmacist counseling services. A novel tool known as the patient satisfaction feedback on counseling (PSF) questionnaire in English and Urdu languages was used to document the satisfaction of patients following pharmacist counseling sessions (Naqvi et al., 2019).
Distributions of participants’ characteristics and the cumulative incidences of adverse events were studied using descriptive statistics. Variables having significant association in the chi-square test were further analyzed through a univariate and then a multivariate logistic regression model. Variables with a p-value of <0.15 in the univariate regression analysis were analyzed in the final multivariate regression model. The occurrence of substantial intercorrelations between two or more independent variables in a regression model is referred to as multicollinearity. We examined the collinearity and tolerance value for each variable while creating the multivariate binary logistic regression. If the variables have a strong correlation (variance inflation factor = 10 and tolerance value > 0.1), one of them was excluded from the concluding model (Pallant, 2020). The final multivariate binary logistic regression model was adjusted using the Hosmer–Lemeshow test. The odds ratios with 95% confidence intervals were considered to measure the significant (p ≤ 0.05) relationship between variables and adverse events. We used the Statistical Package for the Social Sciences, version 26 (SPSS) in all statistical analyses.
Overall, 126 MDR-TB patients signed up for the treatment at the site during data collection for this study. A total of ten patients were omitted from the trial because they did not match the study’s eligibility requirements. A total of 116 MDR-TB patients were included and followed for their therapeutic outcomes. Baseline clinical and sociodemographic characteristics of the patients are given in Table 2.
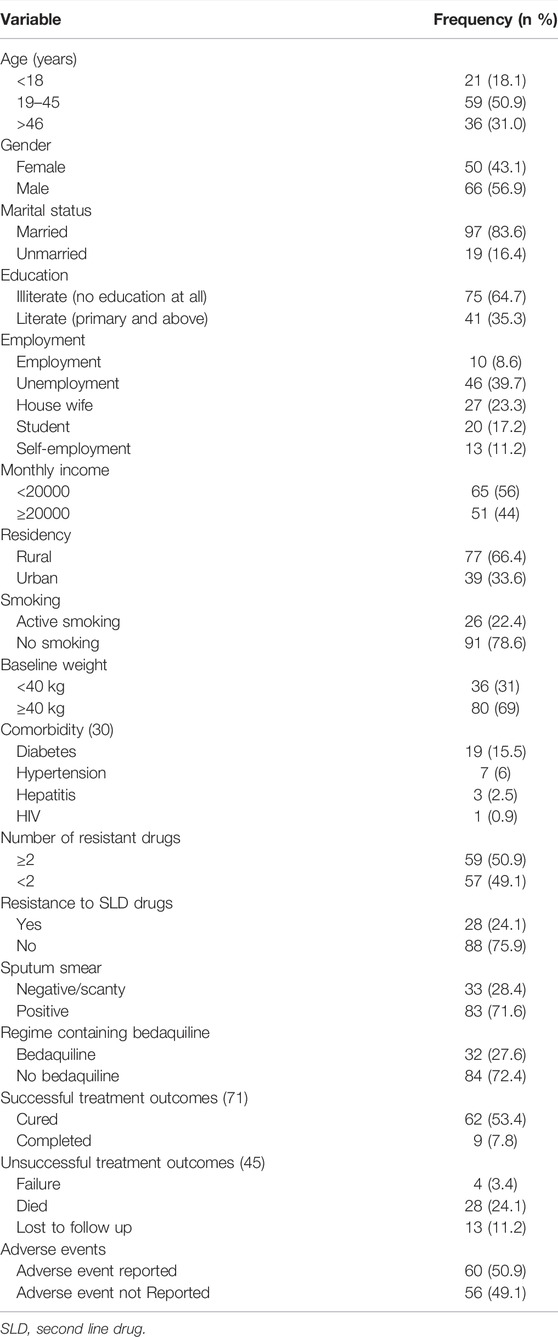
TABLE 2. Baseline demographic and clinical characteristics of the participants (n, 116).
Most patients (50.9%) were between 18 and 45 years of age. Male and female were 80 (56.9%) and 56 (43.1%), respectively. Nearly 66% of the patients resided in rural areas, 64.7% have no formal level of education, and 83.6% patients were married. Active smokers were 21.6%, and 25.8% had one or more comorbidities, and 27.6% were those with regime containing bedaquiline. Most of the patients (69%) had a baseline body weight of above 40 kg.
A statistically significant association was found between the incidence of ADEs and age, comorbidities, smoking, baseline weight, delayed reporting to the TB center, and regime plan containing bedaquiline. No statistically significant association was identified between gender, marital status, education, employment status, residency, and number of drug resistance (Table 3).
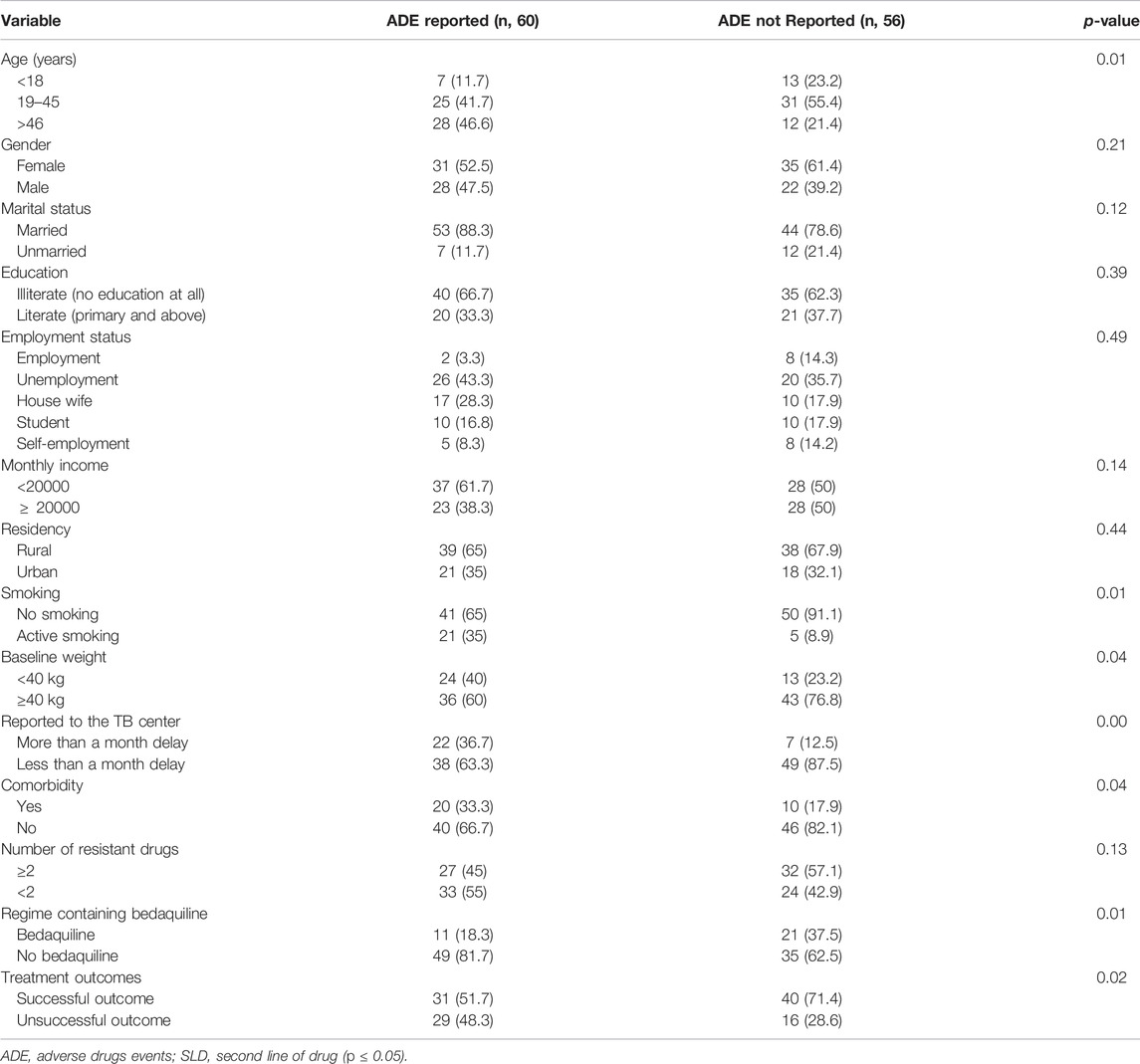
TABLE 3. Association between patients’ characteristics and incidence of ADEs (n, 116).
Furthermore, during multivariate analysis, the variables that had a significant association with the occurrence of AEs were patients with age group above 60 years (odds ratio (OR) 4.50; 95% CI 1.05-19.2), active smokers (OR 4.20; 95% CI 1.31-13.4), and delayed reporting to the TB center (OR 4.03; 95% CI 1.34-12.1). Similarly, bedaquiline regime had the lowest incidence of ADEs among amino salicylic acid, linezolid, and injectable drugs (OR 3.54; 95% CI 1.23-10.1). Exploring the impact of ADEs on TB treatment outcomes through univariate analysis, the occurrence of ADEs had a significant risk of positive association with unsuccessful treatment outcomes (OR 2.33; 95% CI 1.08-5.05). However, in multivariate analysis, no level of significance was found Table 4.
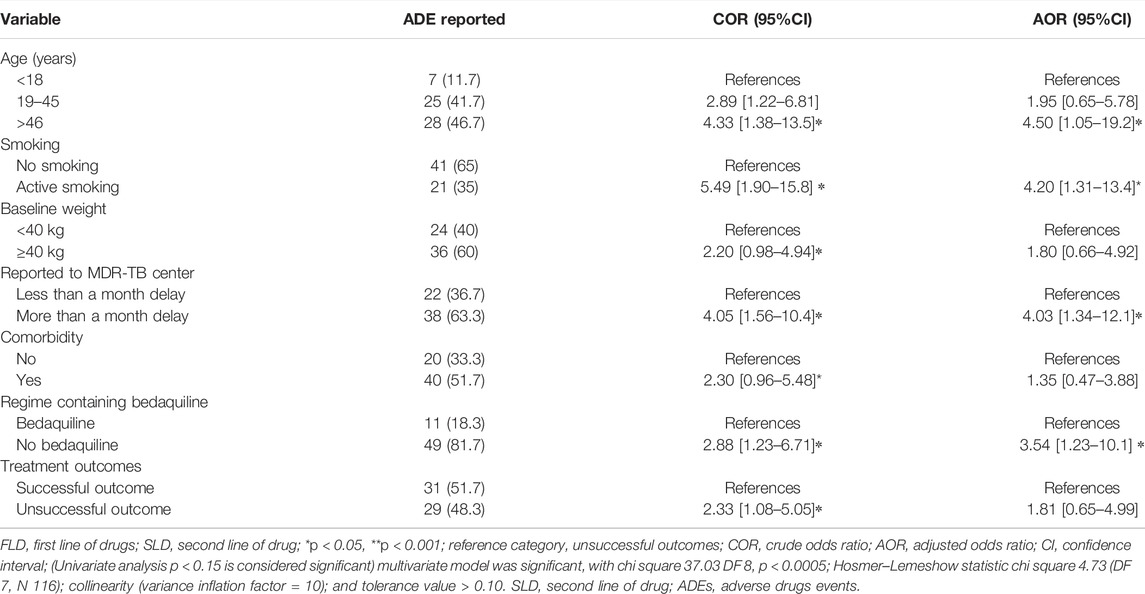
TABLE 4. Risk factors associated with adverse drugs events.
Out of 116 patients, 59 (50.8%) experienced at least one ADE. Most ADEs occurred during the 6-month interim period of MDR-TB treatment. Among all types of ADEs, nausea and vomiting (33%), arthralgia (28.4%), psychiatric disturbance (20.6%), and gastritis (10.3%) were mostly reported by patients during clinical follow-up assessment. Similarly, hearing disturbance (11.2%), gastritis (10.3%), skin rashes (6%), headache (4.3%), peripheral neuropathy (3.4%), and visual disturbance (1.7%) were also observed (Table 5).
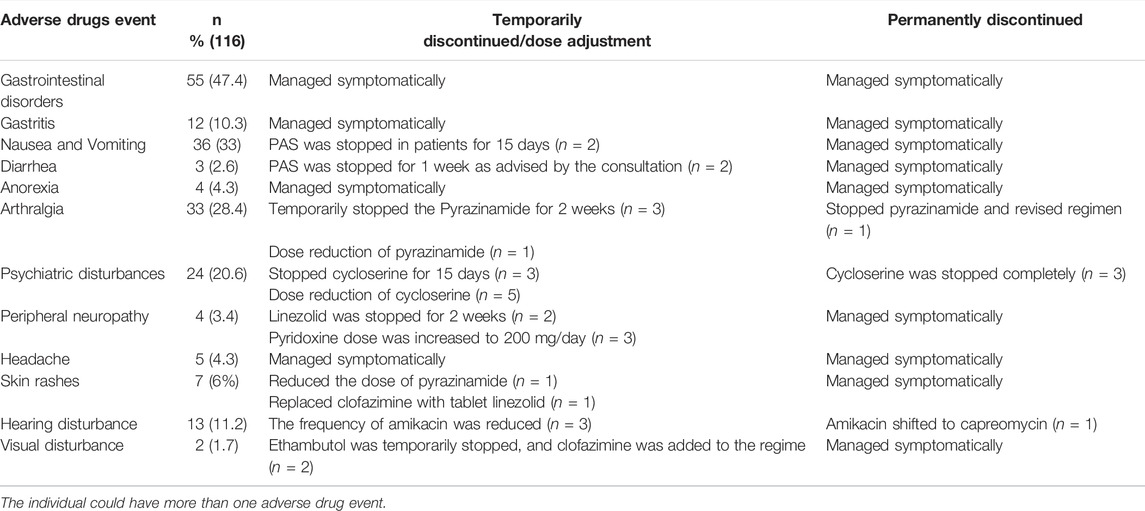
TABLE 5. Prevalence and management of adverse events in patients with MDR-TB treatment.
All the adverse events were managed by pharmacological, psychological, and supportive therapies. In addition, education was provided during each follow-up visit to patients regarding ADEs and their management. ADEs were thoroughly evaluated, and it was found that no drug(s) should be permanently discontinued unless they pose a life-threatening situation or causing a lasting injury to the patient. But in a worse condition, all the required changes were made according to the WHO guidelines. Among 11 (9.48%) MDR-TB patients, temporary medications were stopped, and drugs were successfully reintroduced within 4 weeks after the problem resolution. For 6 (5.1%) drug-resistant TB patients, permanent changes were made in the regimen, and for 14 (12.0%) patients dose adjustment was suggested during the study time. All of the problematic medicines that had been temporarily discontinued over the course of therapy were restarted after the ADRs had abated.
Symptomatic management was carried out for all the patients who had the gastrointestinal disorder until the problem was resolved. In case of persistent diarrhea, temporary discontinuation of para-amino salicylic acid for 1 week (n = 2) was advised by the consultant.
In case of no improvement or worsening of arthralgia, consultation with a physician withheld the suspected agent temporarily (n = 3) or dose of the offending drug (pyrazinamide) was reduced (n = 1) or permanently stopped (n = 1). In these four patients, pyrazinamide and clofazimine were replaced with ethambutol and ethionamide, respectively.
Psychiatric problems reported by drug-resistant TB patients compelled the healthcare team for modification in the treatment regimen. Cycloserine was temporary stopped in three patients, and for five patients, the dosage was reduced for 15 days, while in three patients cycloserine was completely stopped after proper consultation with a physician.
Similarly, in case of peripheral neuropathy, linezolid was stopped for 2 weeks (n = 2). In three patients with ototoxicity, frequency of amikacin was reduced, and in one patient, the regime was switched from amikacin daily to alternate day’s capreomycin, with physician’s consultation. In case of skin rash, the physician advised to reduce the dose of pyrazinamide and replace clofazimine with tablet linezolid for 15 days (1) Table 5.
Out of 116 MDR-TB patients, 75 patients were available for patient satisfaction feedback regarding pharmacist-counseling assessment, and the majority (94.6%) of the respondents agreed that they were able to receive consultation without having any trouble with a pharmacist. A total of 81.3% agreed that they developed the knowledge related to MDR-TB according to their needs. However, 82.7% assured that the pharmacist helped resolve their medication-related queries during the treatment session. The majority (97.3%) appeared promising to recommend counseling from a pharmacist to others and recommended that this facility should be accessible in community pharmacies in the district. More than half of the patients (65.3%) were willing to pay for this counseling service. Moreover, 73.3% of the patients appeared satisfied with the counseling Table 6.
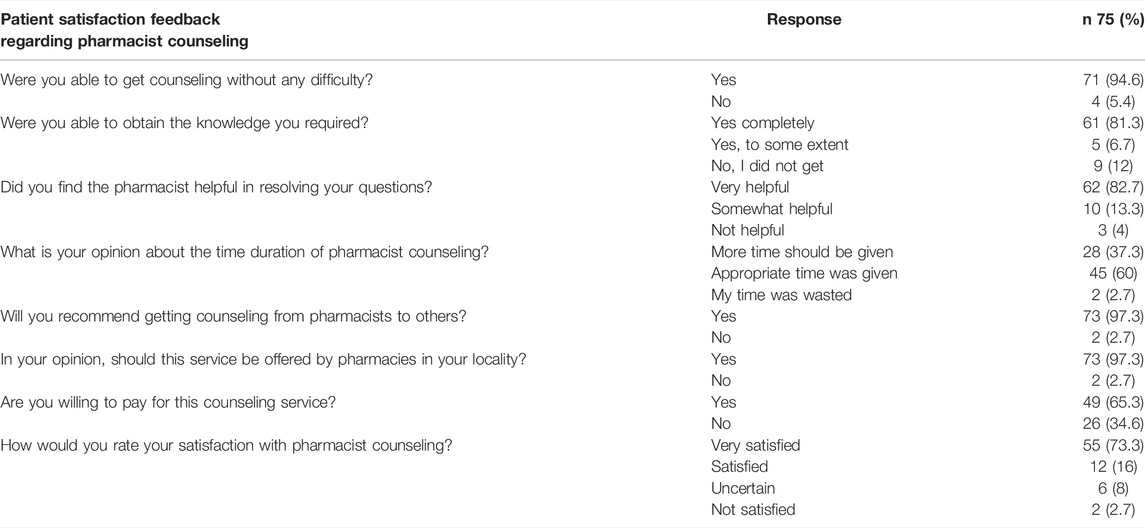
TABLE 6. Patient satisfaction feedback regarding pharmacist counseling.
Multidrug TB treatment has long therapy duration (18 months to 2 years), and the number of drugs used for the treatment is comparatively more complex than that for drug-susceptible TB (Khan et al., 2022). Numerous side effects are identified that result in patients’ non-compliance and predictably poor outcomes (Tahaoğlu et al., 2001; Mukherjee et al., 2004). Therefore, monitoring and appropriate administration of drugs are of utmost significance for the successful treatment of MDR-TB patients (Zhang et al., 2017; Ahmad et al., 2018). In this current study, gastrointestinal disorders were the most common type of adverse events observed in patients (50.9%). The results of the present study are parallel to previously reported studies (Farazi et al., 2014; Javadi et al., 2007; Laghari et al., 2020). However, a study reported higher (71.3%) incidence of ADEs in MDR-TB patients. These differences between studies are likely due to the differences in patient characteristics, treatment regimens, and AE-monitoring approaches. In this study, ADEs were monitored prospectively following the patient-centered care approach delivered by the pharmacist. In our study, 50.9% of the patients developed ADEs of various severities during treatment, of whom 21.5% required minimal modification of the TB treatment regimen and symptomatic treatment in managing ADEs, and these results are consistent with previous studies (Javadi et al., 2007; Baghaei et al., 2011). While maximal modification in treatment was reported in few studies as compared with the current study, i.e., 55.2% from Turkey, 29% from Namibia, and 84% from Latvia (Sagwa et al., 2014; Shin et al., 2007; Törün et al., 2005). These findings point out the promising and important role of the pharmacist to manage all adverse events. All the adverse events in the study were managed by pharmacological, psychological, and supportive therapy. Those who developed gastrointestinal disorders were reassured and symptomatically managed by adding secondary drugs. Patients with adverse events such as nausea and vomiting were advised to perform liver function tests and take anti-TB medication after a light meal. To stop vomiting symptomatically, an antiemetic was added to their regimen. In the case of persistent diarrhea, para-amino salicylic acid was stopped for 1 week or until the adverse event was not resolved. Metronidazole was also prescribed by the physician for the relief of abdominal pain and diarrhea. In the current study, modification in patient’s regimes due to gastrointestinal disorders was according to the previously reported studies (Merid et al., 2019; Ahmad et al., 2018). In the current study, one of the reasons for the adverse events due to gastrointestinal disorders could be that 39.7% of patients were underweight, and they might not have tolerated the multidrug regimen. Previous studies also reported that underweight patients were more prone to ADEs (Laghari et al., 2020; Zhang et al., 2017). Therefore, appetite-stimulating agents and nutritional supplements were added to increase body weight in patients who were underweight.
A significant percentage of the patients (28.4%) experienced arthralgia, inconsistent with the results from India (Qureshi et al., 2007), Japan (Inoue et al., 1999), and Namibia (Sagwa et al., 2013). However, slightly less arthralgia is reported from China (Zhang et al., 2017). In the current study, both pyrazinamide and clofazimine were reported to be the leading cause of arthralgia. The findings of this study are in line with previous studies that reported pyrazinamide as a renowned cause of arthralgia in MDR-TB treatment (Farazi et al., 2014; Abraham et al., 2006). Symptoms of arthralgia were reduced by supportive and pharmacological treatment. The approach of treatment modification applied in our study was similar to the approach used by previous studies (Gülbay et al., 2006; Yang et al., 2017; Ahmad et al., 2018). Another adverse event, the psychiatric disturbance (20.6%), was almost parallel to the previous studies conducted in Turkey (21.3%) and Russia (20.5%) (Törün et al., 2005; Shin et al., 2007). The previous study also mentioned that the leading cause of the MDR-TB treatment modification was a psychiatric disturbance among patients. Cycloserine and ethionamide were recognized as the foremost drugs associated with psychiatric disorders (Leston et al., 1970; Yang et al., 2017; Zhang et al., 2017). Ototoxicity reported in our study (11.2%) was several times lower than that reported in the previous studies, viz., 55% reported in the United Kingdom (Arnold et al., 2017), and 14.5% reported in Iran (Baghaei et al., 2011)), while the cases of ototoxicity in the current study was more than that in the study conducted in Ethiopia (4.8%) (Shibeshi et al., 2019). The variability in the results might be due to the unavailability of proper audiometric assessments at regular intervals at the study site. This might have caused the under-reporting of the actual ototoxicity frequency in our study. Audiometric assessment with consistent intervals of follow-up visits must be considered in patients’ AE detection. The ototoxicity signs were recognized through assessment of hearing loss, imbalance, and visual disturbance. The prevalence of skin adverse reactions was comparatively lower than that reported in previous studies (Schaberg et al., 1996; Yee et al., 2003). We also observed 3.4% of neurologic side effects, much lower than that in a study conducted in Peru (36.7%) (Furin et al., 2001). Linezolid, which was temporarily discontinued, was reintroduced once symptoms resolved, and the dose of vitamin B6 was increased. Elderly patients are predominantly susceptible to ADRs. According to our results, the age group of above 46 years was more significantly associated with ADRs (OR 4.50; 95% CI 1.05-19.2 p < 0.05). The result of this study is entirely consistent with previous study reports (Laghari et al., 2020; Bezu et al., 2014). Geriatrics patients’ liver is less able to metabolize many drugs, and the kidneys are less able to eliminate the drug from the body (Merid et al., 2019). Most reported ADEs were also associated with the smokers’ group as compared with nonsmokers (OR 4.20; 95% CI 1.31-13.4). This result was supported by experimental and clinical studies that smoking increases the chance of ADEs (Bezu et al., 2014; Chung-Delgado et al., 2011). Bedaquiline is a novel drug approved by the WHO, for the treatment of MDR TB. This study investigated the safety of bedaquiline; patients who were without a bedaquiline regime have a higher chance of adverse events (OR 3.54; 95% CI 1.23-10.1) than the other group. The results of this study are consistent with previous studies (Gao et al., 2021; Mbuagbaw et al., 2019; Lan et al., 2020). This indicates that bedaquiline added to a background regimen can improve the rate of successful outcomes and quality of life.
Most patients looked for counseling with no trouble, discovered the pharmacists being helpful, seemed happy with the information they acquired, and looked for more pharmacist counseling opportunities. The findings of our study are consistent with other studies (Alqarni et al., 2019; Naqvi et al., 2019). A higher percentage of patients were willing to pay for the service, and the satisfaction score finding is in line with studies conducted in the United States and Saudi (Poulos et al., 2008; Alshayban et al., 2020). Pharmacists need to provide appropriate, clear, and relevant information to patients about their medications. The results of this study suggest the role of the pharmacist’s services in the Pakistan’s TB health sector. Therefore, efforts to emphasize pharmacists’ role, as a health promoter, will help attain safe and effective pharmaceutical care services.
There are several limitations in our study. First, we only evaluated patients from a single TB referral hospital that may have introduced selection bias; as a single-centered study, its results cannot be generalized. Second, the laboratory tests, especially audiometry, were not performed at the baseline level due to limited resources provided at the study site.
Despite these limitations, we believe that our study provides important information regarding the side effects of second-line anti-TB drugs in resource-poor settings.
In conclusion, we believe that adverse drug events have implications not only for the patient but also for the entire healthcare system. In the present study, ADEs were highly prevalent with second-line anti-TB therapy, but neither led to permanent discontinuation of the regime nor significantly conceited the treatment outcomes. Current findings recommend that ADEs might be well managed by sympathetic, emotional, and pharmaceutical therapy and may be provided without disturbing anti-DR-TB regime. Bedaquiline coupled with other active medications reduce ADEs in MDR-TB patients. As a result, bedaquiline usage in DR-TB patients should be promoted. The elderly patients with active smoking behavior and those who have a delay in treatment initiation are more prone to ADEs. The contribution of clinical pharmacists in TB control programs may help caregivers and patients in the rational use of medication, early identification, and management of ADEs.
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the study protocol that was approved by the Ethics Committee of the Pakistan Institute of Medical Sciences Hospital, Islamabad, and Shaheed Zulfiqar Ali Medical University, Islamabad (F.1-1/2015/ERB/SZABMU/359), and ethically approved after scientific review. The study was also approved by Xian Jiaotong University’s Health Science Center Biology Scientific and Research Ethics Committe (2019-1257). Both a written and oral consent form was obtained from every enrolled patient in this study. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
FK is the principal investigator in the project and drafted the manuscript. WK, SN, JC, and AR have contributed in training and clinical supervision. AK, FK, and KH analyzed and review the final data. YF led the principal developer of the project and ongoing management of the study. All authors have read and approved the drafts of the final manuscript.
This work was funded by the National Natural Science Fund (71974156), the “Young Talent Support 522 Plan,” the “High Achiever Plan” of the Health Science Center, Xi’an Jiaotong University, and the Central 523 University Basic Research Fund (2015qngz05).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor FS declared a past collaboration with the authors AK, YF.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank the MDR TB control center staff for their expertise and assistance throughout all aspects of our study.
Abraham, S., Mitchell, A., and Cope, A. (2006). Anti-Tuberculous Therapy-Induced Crystal Arthropathy. Rheumatology (Oxford) 45, 1173–1174. doi:10.1093/Rheumatology/Kel209
Ahmad, N., Javaid, A., Sulaiman, S. A. S., Afridi, A. K., and Khan, A. H. (2018). Occurrence, Management, and Risk Factors for Adverse Drug Reactions in Multidrug Resistant Tuberculosis Patients. Am. J. Ther. 25, 1–8. doi:10.1097/Mjt.0000000000000421
Alqarni, K., Alqarni, E. A., Naqvi, A. A., Alshayban, D. M., Ghori, S. A., Haseeb, A., et al. (2019). Assessment of Medication Adherence in Saudi Patients with Type II Diabetes Mellitus in Khobar City, Saudi Arabia. Front. Pharmacol. 10, 1306. doi:10.3389/Fphar.2019.01306
Alshayban, D. M., Naqvi, A. A., Islam, M. A., Almaskeen, M., Almulla, A., Alali, M., et al. (2020). Patient Satisfaction and Their Willingness to Pay for A Pharmacist Counseling Session in Hospital and Community Pharmacies in Saudi Healthcare Settings. Front. Pharmacol. 11, 138. doi:10.3389/Fphar.2020.00138
Arnold, A., Cooke, G. S., Kon, O. M., Dedicoat, M., Lipman, M., Loyse, A., et al. (2017). Adverse Effects and Choice between the Injectable Agents Amikacin and Capreomycin in Multidrug-Resistant Tuberculosis. Antimicrob. Agents Chemother. 61, 1–29. doi:10.1128/AAC.02586-16
Baghaei, P., Tabarsi, P., Dorriz, D., Marjani, M., Shamaei, M., Pooramiri, M. V., et al. (2011). Adverse Effects of Multidrug-Resistant Tuberculosis Treatment with A Standardized Regimen: A Report from Iran. Am. J. Ther. 18, E29–E34. doi:10.1097/MJT.0b013e3181c0806d
Baluku, J. B., Nakazibwe, B., Naloka, J., Nabwana, M., Mwanja, S., Mulwana, R., et al. (2021). Treatment Outcomes of Drug Resistant Tuberculosis Patients with Multiple Poor Prognostic Indicators in Uganda: A Countrywide 5-Year Retrospective Study. J. Clin. Tuberc. Other Mycobact Dis. 23, 100221–100228. doi:10.1016/J.Jctube.2021.100221
Bezu, H., Seifu, D., Yimer, G., and Mebrhatu, T. (20142014). Prevalence and Risk Factors of Adverse Drug Reactions Associated Multidrug Resistant Tuberculosis Treatments in Selected Treatment Centers in Addis Ababa Ethiopia. Jtr 02, 144–154. doi:10.4236/Jtr.2014.23018
Chung-Delgado, K., Revilla-Montag, A., Guillen-Bravo, S., Velez-Segovia, E., Soria-Montoya, A., Nuñez-Garbin, A., et al. (2011). Factors Associated with Anti-tuberculosis Medication Adverse Effects: A Case-Control Study in Lima, Peru. Plos One 6, E27610–E27615. doi:10.1371/Journal.Pone.0027610
Farazi, A., Sofian, M., Jabbariasl, M., and Keshavarz, S. (20142014). Adverse Reactions to Antituberculosis Drugs in Iranian Tuberculosis Patients. Tuberc. Res. Treat 2014, 412893–412896. doi:10.1155/2014/412893
Furin, J. J., Mitnick, C. D., Shin, S. S., Bayona, J., Becerra, M. C., Singler, J. M., et al. (2001). Occurrence of Serious Adverse Effects in Patients Receiving Community-Based Therapy for Multidrug-Resistant Tuberculosis. Int. J. Tuberc. Lung Dis. 5, 648–655.
Gao, J. T., Du, J., Wu, G. H., Pei, Y., Gao, M. Q., Martinez, L., et al. (2021). Bedaquiline-Containing Regimens in Patients with Pulmonary Multidrug-Resistant Tuberculosis in China: Focus on the Safety. Infect. Dis. Poverty 10, 32–10. doi:10.1186/S40249-021-00819-2
Gülbay, B. E., Gürkan, Ö. U., Yıldız, Ö. A., Önen, Z. P., Erkekol, F. Ö., Baççıoğlu, A., et al. (2006). Side Effects Due to Primary Antituberculosis Drugs during the Initial Phase of Therapy in 1149 Hospitalized Patients for Tuberculosis. Respir. Med. 100, 1834–1842.
Inoue, T., Ikeda, N., Kurasawa, T., Sato, A., Nakatani, K., Ikeda, T., et al. (1999). Hyperuricemia and Arthralgia during Pyrazinamide Treatment. Nihon Kokyuki Gakkai Zasshi 37, 115–118.
Iradukunda, A., Ndayishimiye, G. P., Sinarinzi, D., Odjidja, E. N., Ntakaburimvo, N., Nshimirimana, I., et al. (2021). Key Factors Influencing Multidrug-Resistant Tuberculosis in Patients under Anti-tuberculosis Treatment in Two Centres in Burundi: A Mixed Effect Modelling Study. BMC Public Health 21, 2142–2149. doi:10.1186/S12889-021-12233-2
Javadi, M. R., Shalviri, G., Gholami, K., Salamzadeh, J., Maghooli, G., and Mirsaeedi, S. M. (2007). Adverse Reactions of Anti-tuberculosis Drugs in Hospitalized Patients: Incidence, Severity and Risk Factors. Pharmacoepidemiol. Drug Saf. 16, 1104–1110. doi:10.1002/Pds.1468
Javaid, A., Khan, M. A., Jan, F., Rauf, M., Khan, M. A., Basit, A., et al. (2018). Occurrence of Adverse Events in Patient Receiving Community-Based Therapy for Multidrug-Resistant Tuberculosis in Pakistan. Tuberk Toraks 66, 16–25. doi:10.5578/Tt.64054
Kefale, B., Degu, A., and Tegegne, G. T. (2020). Medication-Related Problems and Adverse Drug Reactions in Ethiopia: A Systematic Review. Pharmacol. Res. Perspect. 8, 006411–E711. doi:10.1002/Prp2.641
Khan, F. U., Rehman, A. U., Khan, F. U., Hayat, K., Khan, A., Ahmad, N., et al. (2022). Assessment of Factors Associated with Unfavorable Outcomes Among Drug-Resistant TB Patients: A 6-Year Retrospective Study from Pakistan. Ijerph 19, 1574. doi:10.3390/Ijerph19031574
Laghari, M., Talpur, B. A., Syed Sulaiman, S. A., Khan, A. H., and Bhatti, Z. (2020). Adverse Drug Reactions of Anti-tuberculosis Treatment Among Children with Tuberculosis. Int. J. Mycobacteriol 9, 281–288. doi:10.4103/Ijmy.Ijmy_75_20
Lan, Z., Ahmad, N., Baghaei, P., Barkane, L., Benedetti, A., Brode, S. K., et al. (2020). Drug-Associated Adverse Events in the Treatment of Multidrug-Resistant Tuberculosis: An Individual Patient Data Meta-Analysis. Lancet Respir. Med. 8, 383–394. doi:10.1016/S2213-2600(20)30047-3
Leston, J. M., Rey, J. C., Gonzalez Montaner, L. J., Grondona, A., and Zavalla, P. N. (1970). Psychosomatic Reactions to Cycloserine in the Treatment of Tuberculosis. Scand. J. Respir. Dis. Suppl. 71, 231–234.
Mbuagbaw, L., Guglielmetti, L., Hewison, C., Bakare, N., Bastard, M., Caumes, E., et al. (2019). Outcomes of Bedaquiline Treatment in Patients with Multidrug-Resistant Tuberculosis. Emerg. Infect. Dis. 25, 936–943. doi:10.3201/Eid2505.181823
Merid, M. W., Gezie, L. D., Kassa, G. M., Muluneh, A. G., Akalu, T. Y., and Yenit, M. K. (2019). Incidence and Predictors of Major Adverse Drug Events Among Drug-Resistant Tuberculosis Patients on Second-Line Anti-tuberculosis Treatment in Amhara Regional State Public Hospitals; Ethiopia: A Retrospective Cohort Study. BMC Infect. Dis. 19, 286–312. doi:10.1186/S12879-019-3919-1
Mukherjee, J. S., Rich, Ml., Socci, A. R., Joseph, J. K., Virú, F. A., Shin, S. S., et al. (2004). Programmes and Principles in Treatment of Multidrug-Resistant Tuberculosis. Lancet 363, 474–481. doi:10.1016/S0140-6736(04)15496-2
Naqvi, A. A., Hassali, M. A., Naqvi, S. B. S., Aftab, M. T., Zehra, F., Nadir, M. N., et al. (2019). Assessment of Patient Satisfaction Following Pharmacist Counselling Session by A Novel Patient Satisfaction Feedback on Counselling Questionnaire. J. Pharm. Health Serv. Res. 10, 243–254. doi:10.1111/Jphs.12294
NTP (2020). COVID-19 AND TB CARE IN OPD SETTINGS OPERATIONAL GUIDE 2020. [Online]. NATIONAL TB CONTROL PROGRAM ISLAMABAD. Available: Https://Ntp.Gov.Pk/Wp-Content (Accessed July 9, 2020).
Pallant, J. (2020). SPSS Survival Manual: A Step by Step Guide to Data Analysis Using IBM SPSS. Routledge.
Poulos, G. A., Brodell, R. T., and Mostow, E. N. (2008). Improving Quality and Patient Satisfaction in Dermatology Office Practice. Arch. Dermatol. 144, 263–265. doi:10.1001/Archdermatol.2007.58
Qureshi, W., Hassan, G., Kadri, S. M., Khan, G. Q., Samuel, B., and Arshad, A. (2007). Hyperuricemia and Arthralgias during Pyrazinamide Therapy in Patients with Pulmonary Tuberculosis. Lab. Med. 38, 495–497. doi:10.1309/7gbyqty62pfehdp1
Resende, L. S., and Santos-Neto, E. T. (2015). Risk Factors Associated with Adverse Reactions to Antituberculosis Drugs. J. Bras Pneumol 41, 77–89. doi:10.1590/S1806-37132015000100010
Sagwa, E. L., Mantel-Teeuwisse, A. K., and Ruswa, N. C. (2014). Occurrence and Clinical Management of Moderate-To-Severe Adverse Events during Drug-Resistant Tuberculosis Treatment: A Retrospective Cohort Study. J. Pharm. Policy Pract 7, 14–18. doi:10.1186/2052-3211-7-14
Sagwa, E., Ruswa, N., Musasa, Jp., and Mantel-Teeuwisse, A. K. (2013). Adverse Events during Treatment of Drug-Resistant Tuberculosis: A Comparison between Patients with or without Human Immunodeficiency Virus Co-infection. Drug Saf. 36, 1087–1096. doi:10.1007/S40264-013-0091-1
Sankar, K. H., Roch, K., Jom, D., Palappallil, D. S., Panattil, P., and Sankaranarayanan, R. K. (2021). Adverse Drug Reaction Profile of Daily Regimen Antituberculosis Treatment.
Schaberg, T., Rebhan, K., and Lode, H. (1996). Risk Factors for Side-Effects of Isoniazid, Rifampin and Pyrazinamide in Patients Hospitalized for Pulmonary Tuberculosis. Eur. Respir. J. 9, 2026–2030. doi:10.1183/09031936.96.09102026
Shibeshi, W., Sheth, A. N., Admasu, A., Berha, A. B., Negash, Z., and Yimer, G. (2019). Nephrotoxicity and Ototoxic Symptoms of Injectable Second-Line Anti-tubercular Drugs Among Patients Treated for MDR-TB in Ethiopia: A Retrospective Cohort Study. BMC Pharmacol. Toxicol. 20, 31–10. doi:10.1186/S40360-019-0313-Y
Shin, S. S., Pasechnikov, A. D., Gelmanova, I. Y., Peremitin, G. G., Strelis, A. K., Mishustin, S., et al. (2007). Adverse Reactions Among Patients Being Treated for MDR-TB in Tomsk, Russia. Int. J. Tuberc. Lung Dis. 11, 1314–1320.
Tahaoğlu, K., Törün, T., Sevim, T., Ataç, G., Kir, A., Karasulu, L., et al. (2001). The Treatment of Multidrug-Resistant Tuberculosis in Turkey. New Engl. J. Med. 345, 170–174.
Törün, T., Güngör, G., Özmen, I., Bölükbaşı, Y., Maden, E., Bıçakçı, B., et al. (2005). Side Effects Associated with the Treatment of Multidrug-Resistant Tuberculosis. Int. J. Tuberculosis Lung Dis. 9, 1373–1377.
Trubnikov, A., Hovhannesyan, A., Akopyan, K., Ciobanu, A., Sadirova, D., Kalandarova, L., et al. (2021). Effectiveness and Safety of A Shorter Treatment Regimen in A Setting with A High Burden of Multidrug-Resistant Tuberculosis. Int. J. Environ. Res. Public Health 18, 1–16. doi:10.3390/Ijerph18084121
WHO (2014). Companion Handbook to the WHO Guidelines for the Programmatic Management of Drug-Resistant Tuberculosis 2014. World Health Organization. Available: Https://Apps.Who.Int/Iris/Bitstream/Handle/10665/130918 (Accessed March 2, 2021).
WHO (2021). Meeting Report of the WHO Expert Consultation on Drug-Resistant Tuberculosis Treatment Outcome Definitions, 17-19 November 2020. Available: Https://Www.Who.Int/Publications/I/Item/9789240022195 (Accessed December 5, 2021).
WHO (2012). National Guidelines for Programmatic Man-Agement of Drug-Resistant Tuberculosis (PMDT) 2012. Islamabad, Pakistan NTP. [Online]. Available: Http://Ntp.Gov.Pk/Uploads/Ntp1368669324 (Accessed November 4, 2020).
WHO (2018). WHO EMRO Tuberculosis 2018. WHO. Available: Http://Www.Emro.Who.Int/Pak/Programmes/Stop-Tuberculosis.Html (Accessed May 2, 2021).
Yang, T. W., Park, H. O., Jang, H. N., Yang, J. H., Kim, S. H., Moon, S. H., et al. (2017). Side Effects Associated with the Treatment of Multidrug-Resistant Tuberculosis at A Tuberculosis Referral Hospital in South Korea: A Retrospective Study. Medicine (Baltimore) 96, E7482–E7486. doi:10.1097/MD.0000000000007482
Yee, D., Valiquette, C., Pelletier, M., Parisien, I., Rocher, I., and Menzies, D. (2003). Incidence of Serious Side Effects from First-Line Antituberculosis Drugs Among Patients Treated for Active Tuberculosis. Am. J. Respir. Crit. Care Med. 167, 1472–1477. doi:10.1164/Rccm.200206-626OC
Keywords: multidrug-resistant tuberculosis, adverse drug event, management, pharmacist, patient satisfaction
Citation: Khan FU, Khan A, Khan FU, Hayat K, Rehman Au, Chang J, Khalid W, Noor S, Khan A and Fang Y (2022) Assessment of Adverse Drug Events, Their Risk Factors, and Management Among Patients Treated for Multidrug-Resistant TB: A Prospective Cohort Study From Pakistan. Front. Pharmacol. 13:876955. doi: 10.3389/fphar.2022.876955
Received: 16 February 2022; Accepted: 25 March 2022;
Published: 17 May 2022.
Edited by:
Fahad Saleem, University of Balochistan, PakistanReviewed by:
Mohammad Bashaar, Universiti Sains Malaysia, AfghanistanCopyright © 2022 Khan, Khan, Khan, Hayat, Rehman, Chang, Khalid, Noor, Khan and Fang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yu Fang, eXVmYW5nQG1haWwueGp0dS5lZHUuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.