 Mette Louise Mørk1
Mette Louise Mørk1 Jón Trærup Andersen
Jón Trærup Andersen Ulrik Lausten-Thomsen
Ulrik Lausten-Thomsen Christina Gade
Christina Gade
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pharmacol. , 15 February 2022
Sec. Obstetric and Pediatric Pharmacology
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.828010
This article is part of the Research Topic Insights in Obstetric and Pediatric Pharmacology: 2021 View all 17 articles
The limit for possible survival after extremely preterm birth has steadily improved and consequently, more premature neonates with increasingly lower gestational age at birth now require care. This specialized care often include intensive pharmacological treatment, yet there is currently insufficient knowledge of gestational age dependent differences in drug metabolism. This potentially puts the preterm neonates at risk of receiving sub-optimal drug doses with a subsequent increased risk of adverse or insufficient drug effects, and often pediatricians are forced to prescribe medication as off-label or even off-science. In this review, we present some of the particularities of drug disposition and metabolism in preterm neonates. We highlight the challenges in pharmacometrics studies on hepatic drug metabolism in preterm and particularly extremely (less than 28 weeks of gestation) preterm neonates by conducting a scoping review of published literature. We find that >40% of included studies failed to report a clear distinction between term and preterm children in the presentation of results making direct interpretation for preterm neonates difficult. We present summarized findings of pharmacokinetic studies done on the major CYP sub-systems, but formal meta analyses were not possible due the overall heterogeneous approaches to measuring the phase I and II pathways metabolism in preterm neonates, often with use of opportunistic sampling. We find this to be a testament to the practical and ethical challenges in measuring pharmacokinetic activity in preterm neonates. The future calls for optimized designs in pharmacometrics studies, including PK/PD modeling-methods and other sample reducing techniques. Future studies should also preferably be a collaboration between neonatologists and clinical pharmacologists.
Prematurely born children represent a very fragile subset of neonates, as they often present a complex and challenging pathophysiological condition associated with increased risk of long-term morbidity and mortality. Treatment includes various pharmaceutical agents, yet there is currently insufficient knowledge of gestational age dependent differences in drug metabolism. This potentially puts the preterm at risk of receiving suboptimal drug doses with a subsequent increased risk of adverse or insufficient drug effects (Kearns et al., 2003; O’Hara et al., 2015; van den Anker and Allegaert, 2021).
Although the need for clinical research to identify optimal drug dosing in term and preterm neonates has long been acknowledged as indispensable (Tayman et al., 2011; O’Hara et al., 2015; van den Anker and Allegaert, 2021), the progress has been slow. Recently, data on premature neonates have begun to emerge, and particularly pharmacometric modeling-approaches have added available information on this pediatric subgroup (Smits et al., 2019). However, data is still scarce, and pediatricians are often forced to prescribe medication as off-label or even off-science (Barr et al., 2002; Al-Turkait et al., 2020; Schrier et al., 2020).
The average human gestation is 40 weeks, and prematurity is defined as being born before 37 weeks of gestation (Engle et al., 2004). The global prematurity rates are approximately 10% but vary from 4 to 5% in some European countries to 15–18% in some parts of Africa and Asia (Blencowe et al., 2012; Chawanpaiboon et al., 2019). It is a complex and challenging pathophysiological condition associated with increased risk of long-term morbidity and mortality (Saigal and Doyle, 2008) and it is the leading cause of death in children under 5 years of age (Harrison and Goldenberg, 2016; Chawanpaiboon et al., 2019). Prematurity can be considered a continuum of organ immaturity with huge differences in presentation, morbidity, and need for treatment at either end of the spectrum and is often sub-categorized in moderate to late preterm (32–36 weeks of gestation), very preterm (28–32 weeks of gestation), and extremely preterm (before 28 weeks of gestation) (Engle, 2004). Neonates can equally be classified per birth weight as low birth, (LBW, <2500 g), very low birth weight (VLBW, <1500 g) and extremely low birth weight (ELBW, <1000 g) (World Health Organization, 2004, 10), but although LBW often is caused by prematurity, it cannot be used directly as a marker of the degree of prematurity as LBW can be caused by intrauterine growth restriction (IUGR).
Although there are wide variations in prematurity survival rates across regions and countries (Helenius et al., 2017), overall survival rates for premature and particularly extremely premature neonates have hugely improved since the 1980s (Glass et al., 2015). Importantly, the limit for early human viability, defined as the earliest gestational age an infant can potentially survive being born at, has steadily dropped and some babies delivered at 24, 23, and even 22 weeks of gestation are now able to survive. A recent study from Sweden reports a 20% survival rate in children born at 22 weeks (Norman et al., 2019) and a Japanese study has found a survival rate of 36% in children born at 22 weeks (Ishii et al., 2013). Case reports of children surviving being born at 21 weeks (Sung et al., 2018; Tiniest Babies Registry) or with birth weight below 250 g have emerged, but survival remains low (Brumbaugh et al., 2019). Whereas the reasons for this progress in prematurity survival certainly are multifactorial, the improvement is believed to be linked to overall improvement in neonatal intensive care, such as development of increasingly better artificial airways and breathing circuits and rational application of mechanical ventilation and airway distending pressure (Glass et al., 2015; Pierrat et al., 2021).
Another major driving factor for the improvement in premature survival rates has been pharmacological advancements, both prenatal, immediately post-natal and post-natal. Antenatally, the administering of a course of corticosteroids to women prior to anticipated preterm birth has been demonstrated to have a marked positive effect of subsequent preterm mortality and morbidity ever since the first randomized controlled trial of betamethasone for the prevention of respiratory distress syndrome in preterm neonates in 1972 (Liggins and Howie, 1972). Subsequently, many clinical trials have demonstrated the effect of antenatal corticosteroids before preterm birth, as summarized in a recent systematic Cochrane review demonstrating its effect on reducing neonatal mortality (RR 0.78, 95% CI 0.70–0.87), respiratory distress syndrome (RR 0.71, 95% CI 0.65–0.78), and cerebral intraventricular hemorrhage (RR 0.58, 95% CI 0.45–0.75) (McGoldrick et al., 2020). Antenatal corticosteroid is a pharmacological cornerstone of prophylactic treatment in preterm birth.
A huge leap in pharmacological treatment of preterm children, and possibly one of the single greatest breakthroughs in treatment of premature children, was the development of exogenous surfactant administration techniques in the 1980s and early 1990s. Since the first successful attempts in 1980 (Fujiwara et al., 1980) using the first artificial preparations, this therapy has become the definitive standard treatment for neonatal respiratory distress syndrome and is believed to be one of the most effective medicines in the health system (Hentschel et al., 2020). As respiratory distress syndrome is the single most important cause of illness and death in preterm children (Stevens et al., 2007; Sardesai et al., 2017), surfactant administration has led to a marked increase in survival and helped lower the limit for early human viability (Rojas-Reyes et al., 2012; Sweet et al., 2019; Hentschel et al., 2020).
Pharmacological treatment remains a cornerstone in postnatal care in preterm children, as demonstrated by a recent review of drug utilization studies in neonatal units that found a high mean number of drugs per infant, with eight studies reporting a very high burden (>30 drugs per infant). Drug use patterns were found to be generally uniform with antibiotics being the most frequently prescribed drug in the neonatal department (Al-Turkait et al., 2020). Naturally, trends in general drug prescription have changed over the years but off-label drug use in premature children is still very common: of the top 50 medications of extremely low birth weight premature infants, only 40% were FDA-labeled for use in infants (Stark et al., 2021). This represents a relative lack of proper pharmacokinetic (PK) studies in premature children and remedying this will likely be a long haul due to the difficulties of conducting clinical PK studies in preterm children.
Accurate dosing is essential for a safe and effective pharmacological treatment of premature neonates. An in-depth knowledge of the anatomical and physiological particularities of preterm neonates is therefore crucial for the understanding of the drug pharmacokinetics in this population. Herein, the differences in ontogeny between the extremely, the very and the late preterm neonate should be taken into consideration (Barker et al., 2018; van den Anker et al., 2018).
Also, most aspects of drug disposition are subject to change in case of co-morbidities, which unfortunately relatively often occurs in premature neonates. Sepsis, surgery, and (for moderate and late preterm neonates where such treatment is possible) advanced treatment such as whole body hypothermia (Smith et al., 2019), extracorporeal membrane oxygenation (ECMO), or hemo-dialysis may all significantly alter drug distribution and metabolism.
A summary of the most important prematurity associated characteristics of pharmacokinetics in preterm neonates is presented in Figure 1 and below.
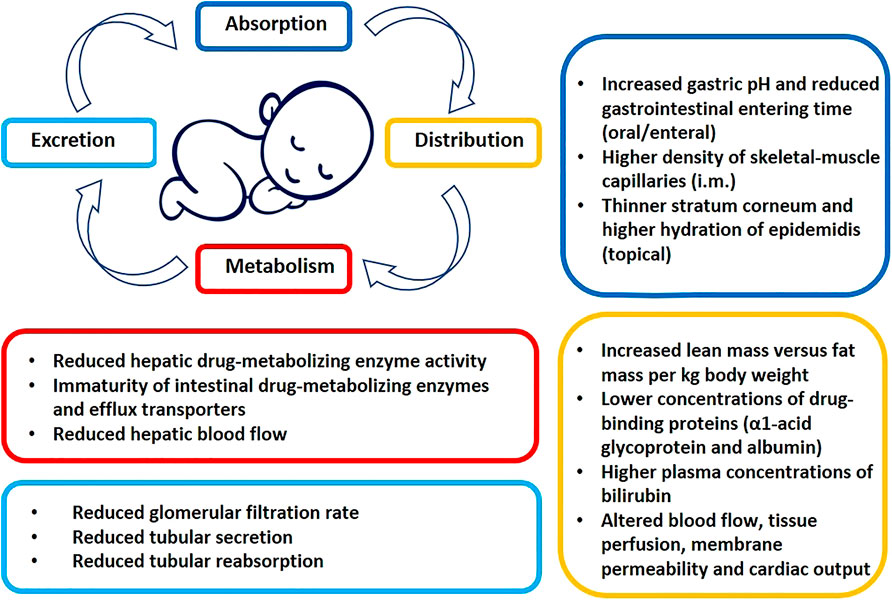
FIGURE 1. Prematurity associated pato-physiological conditions potentially altering the pharmacokinetics of drugs (see text for details).
In preterm neonates, the immaturity of absorptive surfaces may influence drug exposure (O’Hara et al., 2015). At present, there is no clear consensus describing the ontogeny of gastric pH and its impact on drug absorption, and gastric emptying time has not been found age dependent (Bonner et al., 2015). However, gastrointestinal abnormalities and dysfunctions in preterm neonates can affect transit time and enteral absorption (Johnson, 2011; van den Anker and Allegaert, 2021). Developmental differences in the activity of intestinal drug-metabolizing enzymes and efflux transporters will most likely affect the exposure of several drugs in preterm neonates, but this area is still not well understood (Kearns et al., 2003; van den Anker and Allegaert, 2021).
The exposure of drugs after rectal administration is generally increased in preterm neonates, e.g., paracetamol, most likely due to developmental immaturity of the hepatic metabolism rather than increased mucosal translocation (Kafetzis et al., 1979; Ruggiero et al., 2014). Due to the relatively higher density of skeletal-muscle capillaries in neonates, water-soluble drugs show an increased intramuscular absorption, e.g., absorption of amikacin (Kafetzis et al., 1979). Whether this is also the case for preterm neonates is unknown, but the example of intramuscular administration of vitamin E acetate in a lipophilic preparation, showed that the ester was never systematically detectable in premature neonates as opposed to E-vitamin delivered in an aqueous preparation (Italian Collaborative Group on Preterm Delivery, 1991).
The presence of a thinner stratum corneum in preterm neonates, a higher body surface area-to-weight ratio as well as higher cutaneous perfusion and hydration of the epidermis places preterm neonates at risk of adverse effects from topical exposures due to an increased absorption e.g. corticosteroids (Borzyskowski et al., 1976; Munro, 1976) and chlorhexidine (Cowen et al., 1979). Application of antiseptic solutions containing alcohols has led to severe burns in premature infants (Brayer et al., 2004). Pulmonary, sublingual, and buccal absorption are not well studied in preterm or term neonates (O’Hara et al., 2015; van den Anker and Allegaert, 2021).
In the extremely preterm neonate, total body fat content can be as low as 1% of the total body weight and total body water is decreasing from 85% in preterm neonates to 75% in term neonates (Tetelbaum et al., 2005; Ford and Calvert, 2008) (Sharma et al., 2008). Due to the lower percentage of fat and muscle mass in preterm neonates, drugs that are normally rapidly distributed into the muscle tissue, like fentanyl, will remain in the plasma compartment for a longer time (O’Hara et al., 2015). Significant changes in intra/extracellular body fluid distribution per concurrent weight occurs postnatally during the first week of life. Thus, both gestational age (GA) at birth and postnatal age (PNA) influences total body water content and distribution, and this should ideally be taken into consideration when optimizing individual drug doses (van den Anker and Allegaert, 2021).
At the time of birth, neonates have lower concentrations of the drug-binding proteins α1-acid glycoprotein and albumin when compared to older children (Ehrnebo et al., 1971; Windorfer et al., 1974; Ku and Smith, 2015). The amount of free drug available for distribution will therefore be increased for highly protein bound drugs, e.g., theophylline (Aranda et al., 1976). Effects and toxicity may therefore be obtained at lower total plasma concentrations. Also elevated plasma levels of bilirubin can increase the concentration of unbound drugs by displacing highly bound drugs from protein-binding sites, e.g., ampicillin, benzodiazepine and phenytoin (Fredholm et al., 1975; Tayman et al., 2011; Zwart et al., 2021).
Higher CNS drug concentrations may occur in preterm neonates due to reduced outward drug transport, however, this area still needs to be elaborated (Painter et al., 1981; Liu et al., 2008; Ku and Smith, 2015). Changes in the volume of distribution are also related to changes in blood flow, tissue perfusion, membrane permeability and cardiac output (Kearns et al., 2003; O’Hara et al., 2015; van den Anker and Allegaert, 2021). Furthermore, it should be noticed that pathological circulatory conditions, e.g., a hemodynamically significant persistent ductus arteriosus can also alter the volume of distribution of drugs in preterm neonates (Ku and Smith, 2015; O’Hara et al., 2015).
The major site of drug metabolism is the liver and the drug metabolizing enzymes are broadly divided into phase I and phase II enzymes. The phase I enzymes are responsible for primary oxidation, reduction and hydrolysis processes. The most important group of enzymes involved in phase I metabolism are cytochrome (CYP) P450 enzymes with a major contribution of cytochrome P450 3A4 (Hines and McCarver, 2002). However, while CYP3A4 constitutes 30–40% of the total liver CYP content in adult, CYP3A7 is found to be the major form in human embryonic, fetal and newborn liver (Gow et al., 2001; Hines and McCarver, 2002). In the period from late fetal to early neonatal life, there appears to be a peak in CYP3A7 activity, then a transition in expression and catalytic activity from predominant CYP3A7 to CYP3A4 (de Wildt et al., 1999; Gow et al., 2001).
Phase II enzymes are responsible for conjugate drug molecules to allow excretion. Phase II drug metabolizing enzymes are mostly transferases and include: UDP-glucuronosyltransferases (UGTs), sulfotransferases (SULTs), N-acetyltransferases (NATs), glutathione S-transferases (GSTs) and various methyltransferases (Xu et al., 2005; O’Hara et al., 2015).
A lack of activity of metabolizing enzymes can be responsible for extreme toxicity syndromes (O’Hara et al., 2015). Severe toxicity syndromes in premature infants have been described due to reduced capacity of their metabolic systems, e.g., grey baby syndrome, which is caused by diminished ability to conjugate chloramphenicol and to excrete the active form in the urine (Craft et al., 1974). In addition, gasping syndrome with benzyl alcohol, where benzoic acid cannot be conjugated but is accumulated, causing metabolic acidosis in premature neonates (Gershanik et al., 1982).
Similarly to many other physiological and metabolic processes in newborns, pharmacokinetics also exhibit a relative immaturity that changes postnatally, and for the CYP450 system, it is believed that some CYP450 enzymes are active in utero while others do not active until after birth (Gow et al., 2001; O’Hara et al., 2015). When corrected for weight the content of CYP enzymes in fetal livers is 30–60% of adult values and full CYP activity is usually achieved by 2 years of age. Yet, the many physiological and metabolic processes depend not only on postnatal age, but also on gestational age, i.e., degree of maturation, at the time of birth (Gow et al., 2001; Kearns et al., 2003; O’Hara et al., 2015).
Knowledge of maturation of drug metabolizing enzymes is therefore an important factor in determining drug selection in neonates. This is further complicated as various elements of the drug metabolism pathways do not mature at the same rate postnatally (Hines and McCarver, 2002). For example, use of codeine is not appropriate during the first month of life as conversion to morphine via CYP2D6 is low resulting in very limited effectiveness (O’Hara et al., 2015). Midazolam is metabolized by CYP3A4 at a slower rate causing increased duration of sedation and early exposure to opioid infusion in the first 3 days was associated with higher risk of adverse outcomes in extremely preterm infants (de Wildt et al., 2010; Shah et al., 2011; Ng et al., 2012; O’Hara et al., 2015). Contrarily, CYP1A2 is induced rapidly after birth with post-natal age rather than post-menstrual age correlating with changes in half-life and clearance (Hines and McCarver, 2002; Schmidt et al., 2006). This rapid induction fits clinically with the lack of toxicity to caffeine seen in even the most premature infants started on caffeine for the prevention or treatment of apnea of prematurity (Schmidt et al., 2006). However, the pattern and timing of post-natal CYP1A2 induction remain unclear.
Maturation rates are difficult to generalize, and enzyme-specific information needs to be determined for an accurate estimate of drug metabolism including clinical conditions such as sepsis and complex surgery, nutritional state and diet (infant formula versus breast milk), polymorphism and even antenatal exposure to cigarette smoke (Czekaj et al., 2005; Blake et al., 2006; Allegaert, 2017; Li et al., 2021).
Water soluble drugs with low molecular weight are primarily eliminated by renal excretion. The glomerular filtration rate (GFR) is highly dependent on gestational age and is ranging from 0.6–0.8 to 2–4 ml per minute per 1.73 m2 in preterm neonates and term neonates, respectively (Hayton, 2000; Ali et al., 2012). For example, gentamycin is therefore necessitating dosing intervals of 36–48 h in preterm newborns but reduced to 24 h in term newborns (Ali et al., 2012; Fuchs et al., 2014). Also, tubular secretion and reabsorption is reduced in preterm neonates. Tubular secretion has importance for the renal elimination of, e.g., penicillins, cephalosporins, and digoxin (Kearns et al., 2003).
As the anatomical and physiological characteristics of preterm neonates differ significantly from older children and adults, the process of neonatal pharmacological development becomes very complex. Furthermore, neonatology represents a small sub-field of pharmacology, and as a small target population, neonates are often overlooked.
Pharmaceutical companies largely refrain from proactively investing in the pediatric sector due to both economic and practical considerations, as reported by the EMA (European Medicines Agency and its Paediatric Committee, 2016; Van Driest and Choi, 2019). Even academia-driven research in the population of preterm neonates is limited and often focused on various other areas of clinical research than pharmacology.
The ethical principles of pediatric research are well known (Roth-Cline et al., 2011), but the challenges are even more pronounced in the preterm population. Overall, inclusion of newborns in research should comprise a minimal risk and/or have a potential for direct benefits for the trial participant to be considered ethically acceptable (Barker et al., 2018).
Due to the stressful situation of becoming a parent to a premature child, the required informed parental consent for neonates participating in research, can be difficult to obtain. The process may require repeated discussions with the families, and thus complicate recruitment for studies during the first hours/days of life (O’Hara et al., 2020).
Failure of recruitment of a sufficient number of premature neonates within the planned study period may force investigators to facilitate costly prolongations of the study or even to a premature study termination without reaching the target sample size. Failed drug trials and the general lack of pediatric clinical trials contribute to the high prevalence of off-label use in neonates.
Fortunately, relatively few children are born very or extremely preterm, but the scarcity of premature neonates makes it challenging to include this population in PK studies. Traditional PK study designs involve multiple blood samples at fixed intervals and generally require the same number of samples from all subjects taken at the same time (O’Hara et al., 2020). This approach presents practical difficulties in preterm neonates, as repeated blood sampling quickly exceeds the regulated (EMA, 2018; Barker et al., 2018) maximum of 1% at any one time, or 3% within 1 month, amounting to 400 µl or 1.2 ml respectively for a neonate weighing 500 g. Also, the sampling procedure may prove challenging, as even something as mundane as drawing blood often requires experience in the extremely preterm children. Likewise, urine sampling may prove difficult to collect in a standardized manner (Van Driest and Choi, 2019).
A PubMed search was performed on 3 January 2022 for the terms phase I and phase II metabolism in premature children using the following search string: {“Infant, Premature” (mesh) OR “Infant, Extremely Premature” (mesh) OR “Infant, Low Birth Weight” (mesh) OR “Infant, Very Low Birth Weight” (mesh) OR “Infant, Premature, Diseases” (mesh) OR [(preterm OR prematurity OR premature OR prematurely) AND (infant* OR infancy OR baby OR babies OR neonat* OR newborn*)] OR preemi* OR premi OR preterm OR “very low birth weight” OR VLBW OR “low birth weight” OR LBW OR “very low birthweight” OR “low birthweight”} AND {[“Cytochrome P-450 Enzyme System" (mesh) OR “Cytochromes” OR Cytochrome* OR “P450”] OR [“Methyltransferases” (mesh) OR “Sulfotransferases” (mesh) OR “Acetyltransferases” (mesh) OR “Acyltransferases” (mesh) OR “Glucuronosyltransferase” (mesh) OR glucuronidation* OR Methyltransferase* OR Sulfotransferase* OR Acetyltransferase*)]} AND {[humans (Filter)] AND [newborn (Filter)]}.
Manuscripts were reviewed for relevance to the topic of this review, as well as for citations related to the topic of the review by two independent reviewers (MLM and CG). In case of disagreement, a third author (ULT) would arbitrate. This review should however be considered a scoping rather than a systematic review.
Our search resulted in 1206 hits, of which a total of 70 manuscripts were found relevant to the scoping review (Aranda et al., 1976; Loughnan et al., 1977; Windorfer and Pringsheim, 1977; Pitlick et al., 1978; Onishi et al., 1979; Grygiel and Birkett, 1980; Brazier et al., 1981; Kawade and Onishi, 1981; Mulhall et al., 1983; Tserng et al., 1983; Ribon et al., 1984; Grasela and Donn, 1985; Choonara et al., 1989; RJ et al., 1990; Fujii et al., 1993; Hartley et al., 1993, 1994; Reiter and Stiles, 1993; Brammer and Coates, 1994; Vauzelle-Kervroedan et al., 1996; Sato et al., 1997; Treluyer et al., 1997; Wenzl et al., 1998; Lee et al., 1999; Touw et al., 2000; de Wildt et al., 2001, 2002, 2010; Lowry et al., 2001; Allegaert et al., 2008a, 2008b, 2015; Wade et al., 2008, 2009, 2009; Knibbe et al., 2009; Mugabo et al., 2011; George et al., 2012; Ince et al., 2013; Kim et al., 2013; Le Doare et al., 2013; Wang et al., 2013; Bekker et al., 2014; de Waal et al., 2014; Krekels et al., 2015; Mahmood, 2015, 2017; Ogawa et al., 2015; Pain et al., 2015; Auriti et al., 2016; Cook et al., 2016; Momper et al., 2016; Flint et al., 2017; Hwang et al., 2017; Sohn et al., 2017; Völler et al., 2017; JM et al., 2018, 2018; Anderson and Holford, 2018; Brussee et al., 2018; Leroux et al., 2018; Michelet et al., 2018; Neyro et al., 2018; Tsakiri et al., 2018; Gerhart et al., 2019; Gonzalez et al., 2019; Smith et al., 2019; van Groen et al., 2019).
Overall, the large heterogeneity of the studies with regards to both scope, methodology, and particularly the detail of reporting results, precludes any formal comparison, let alone meta-analyses. In particular, many studies examined neonates, but failed to distinguish between term and preterm neonates. This was the case in more than 40% of the studies. The full spectrum of prematurity was found to be explored from 22 gestational weeks and onwards. Extreme premature neonates (born before 28 GA weeks) were included in less than 55% of these studies.
Furthermore, the age of the children at the time of inclusion and/or sampling (postnatal age, PNA) was unclear in approximately 30% of the studies. In the remaining articles the PNA varied from a few hours to 1 year. The overall mean age at the time of inclusion varied from 4 days to 1.5 months. Keeping in mind that prematurity is defined as being born before 37 weeks of gestation, this logically reduces the actual number of included neonates, who were extremely, very or even late preterm at the time of sampling. These findings elucidate how most PK studies in the youngest pediatric populations are not sufficiently transparent in the presentation of data contributions.
Generally, the gestational- and postnatal ages are displayed in intervals, making an accurate estimation of the degree of prematurity impossible. Additionally, the interpretation of the strength of the contributing data becomes very difficult, as, e.g., a 2 weeks old child that was born at 26 weeks gestational age and a newborn child born at 28 weeks gestational age are not necessarily equal in terms of metabolic maturation.
Most studies (approximately 70%) focused on the phase I metabolism, and the most studied CYP subclasses were CYP3A4, CYP1A2, CYP2E1, CYP2C19, and CYP2C9 either as individual or contributing enzymes. The phase II metabolism systems were studied in approximately 35% of the articles identified [with glucuronidation (notably UDP-Glucuronosyltransferase-2B7)] and sulfation being the most studied.
In Tables 1–3 we summarize the Cytochrome P450 subclasses, we found to be the most studied in vivo in preterm neonates, i.e., 3A4, 1A2, and 2C9/2C19.
Identified studies of CYP3A4 activity are displayed in Table 1. Midazolam was predominantly reported as an in vivo probe for CYP3A4 activity, and the clearance values reported illustrated a clear tendency towards reduced CYP3A4 activity in preterm neonates as compared to full born neonates and older children (Burtin et al., 1994; Vauzelle-Kervroedan et al., 1996; Lee et al., 1999; de Wildt et al., 2001, 2002; Ogawa et al., 2015; Brussee et al., 2018; JM et al., 2018; van Groen et al., 2019). The largest study identified was a population-based study (Burtin et al., 1994) included plasma samples from 197 neonates (gestational age 26–42 weeks, postnatal age 0–10 days) on artificial ventilation. Here clearance was found to be directly proportional to birth weight and gestational age, but not postnatal age (between 0 and 10 days).
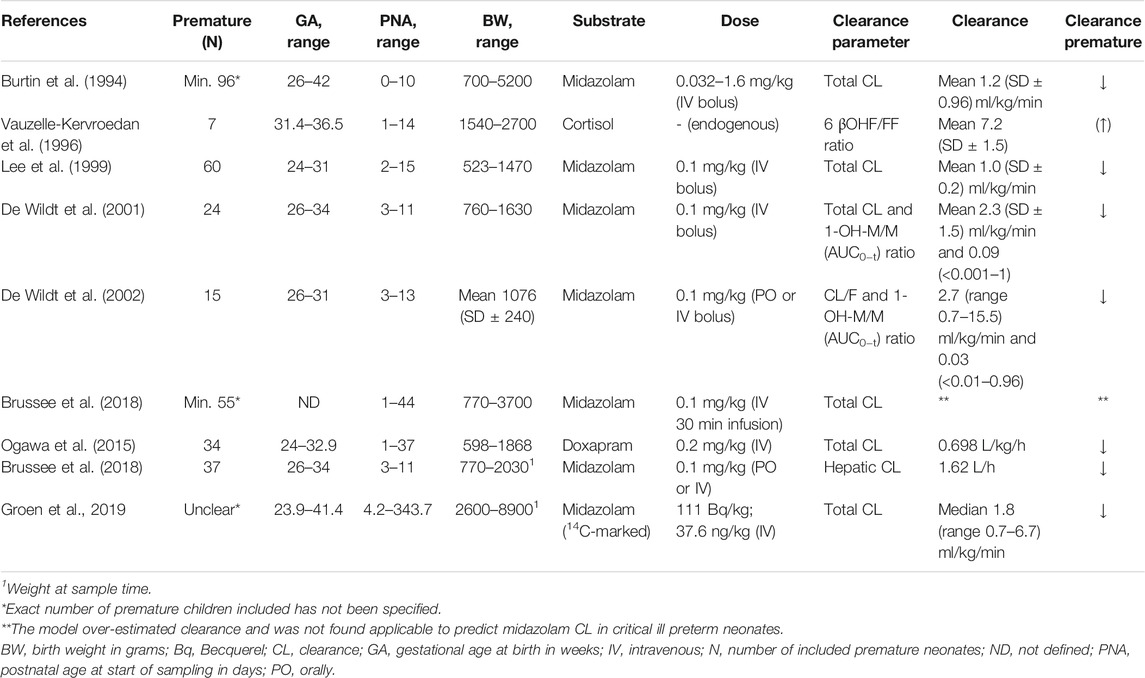
TABLE 1. Summary of studies exploring CYP3A (4/5) activity in preterm neonates.
Identified studies of CYP2C19 and CYP2C9 activity are displayed in Table 2. Only phenobarbital was found reported as an in vivo probe for CYP2C9 (Pitlick et al., 1978; Ribon et al., 1984; Grasela and Donn, 1985; MP et al., 1989; Touw et al., 2000; Völler et al., 2017), although additional minor metabolism occurs via CYP2C19 and CYP2E1 (approximately 5%). A general trend towards reduced phenobarbital clearance was observed in premature neonates. In a recent population study, a PK model was developed based on data sharing from former studies, and the maturation of clearance was predicted to be dependent on both body weight and postnatal age in preterm neonates.
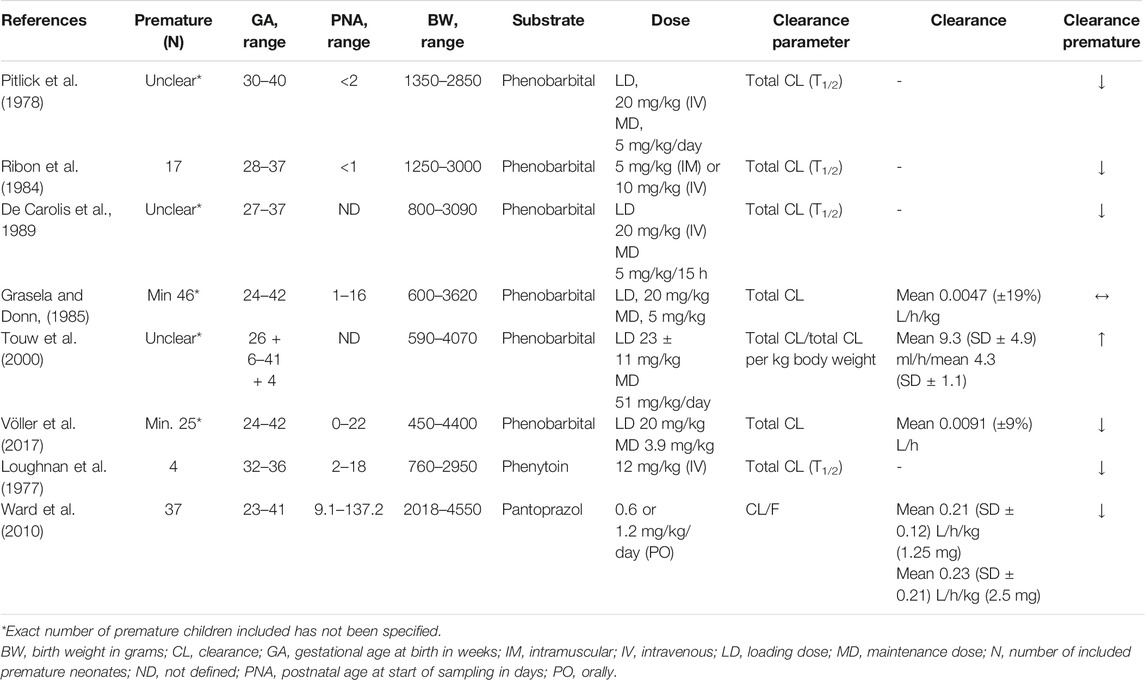
TABLE 2. Summary of studies exploring CYP2C9 (rows 1–6) and CYP2C19 (rows 7–8) activity in preterm neonates.
The activity of CYP2C19 was investigated by use of the substrate’s phenytoin and pantoprazole (Loughnan et al., 1977; Ward et al., 2010). Latest was investigated by Ward et al., in 2010, who found oral clearance of pantoprazole reduced in preterm neonates. Oral clearance increased with increased postnatal age, but no apparent trend was seen for postmenstrual age.
Primarily theophylline was used as substrate in all the identified in vivo studies investigating CYP1A2 activity in preterm neonates (Grygiel and Birkett, 1980; Brazier et al., 1981; Tserng et al., 1983; Lowry et al., 2001; Kim et al., 2013; Sohn et al., 2017; Jiang et al., 2021), which are displayed in Table 3. CYP1A2 was generally found associated to postnatal age rather than postmenstrual age and to birth weight. Furthermore, well-known genetic polymorphism-associated differences in CYP1A2 activity were not yet found expressed in the preterm population.
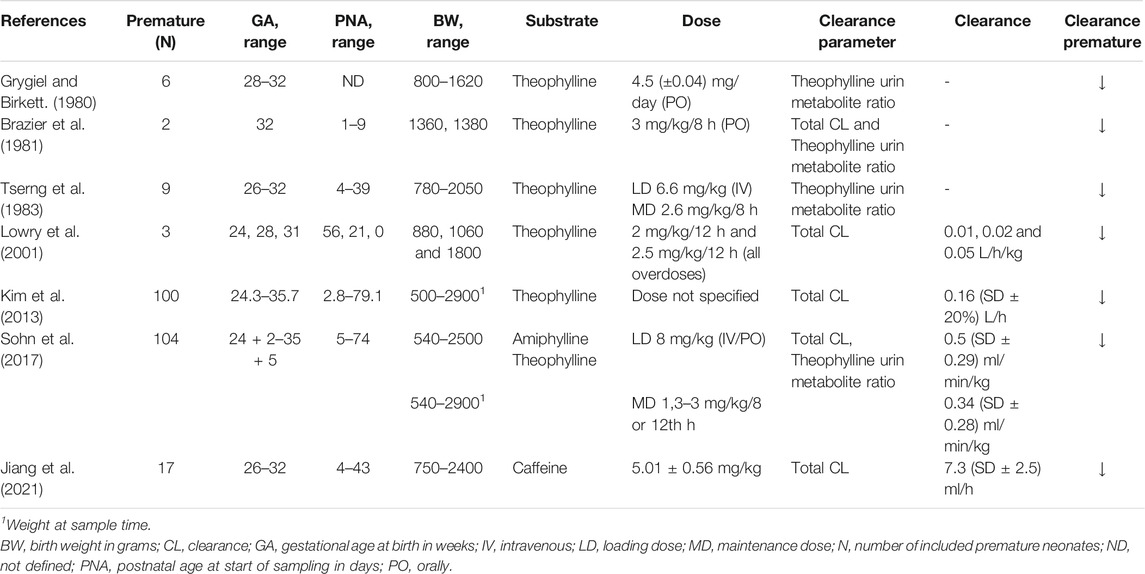
TABLE 3. Summary of studies exploring CYP1A2 activity in preterm neonates.
Three studies investigating the in vivo CYP2E1 activity were identified. Isoniazid (Bekker et al., 2014) and paracetamol (Cook et al., 2016; Flint et al., 2017) were the substrates studied. A markedly reduced isoniazid clearance was noted in neonates with low GA and LBW. None of the studies using paracetamols as substrate succeeded in defining the CYP2E1 maturity, probably because the contribution of the CYP2E1 pathway is minimal, albeit important due to formation of the toxic metabolite NAPQI, for the metabolism of paracetamol.
In vivo CYP2D6 metabolism has been investigated in premature neonates using tramadol as substrate (Allegaert et al., 2008a; 2008b). Here, PMA and CYP2D6 polymorphisms (Li et al., 2021) was found to determine the O-demethylation activity in the preterm neonates.
Twenty studies investigating the in vivo phase II metabolism were identified (Windorfer and Pringsheim, 1977; Mulhall et al., 1983a; Choonara et al., 1989; Hartley et al., 1993, 1994; H et al., 1993; Reiter and Stiles, 1993; Brammer and Coates, 1994; Sato et al., 1997; Wenzl et al., 1998; Wade et al., 2008, 2009; Knibbe et al., 2009; Krekels et al., 2015; Mahmood, 2015; Auriti et al., 2016; Cook et al., 2016; Flint et al., 2017; MF et al., 2017; Leroux et al., 2018; Gerhart et al., 2019). A large heterogenitet was found and several substrates were used and included chloramphenicol, morphine, fluconazole, lorazepam, micafungin, paracetamol, and mefenamic acid. Overall, the activity of the phase II metabolis, pathways were found reduced in preterm neonates. Herein, morphine metabolism by UGT2B7 was found closely related to body weight as opposed and post-natal age (day 1–10) (Knibbe et al., 2009), and fluconazol clearance by UGTB7was found to increase with increase with BGA, PNA and PMA (Wade et al., 2008).
The understanding of developmental pharmacology in infants and children has increased significantly since the seminal review by Kearns et al. (2003) and new data have been added in both neonates in general (Allegaert, 2017) and in premature neonates (van den Anker and Allegaert, 2021). Furthermore, pharmacometrics modelling approaches are now, despite limited data, being used to support neonatal and pediatric drug development as well as commonly used off-label drugs. The insight into ontogeny of, e.g., the phase I metabolism of extreme premature neonates has previously been based on, e.g., fetal samples (Kearns et al., 2003). However, with a limit of early human viability, that is, constantly improving, PK data on the extreme premature neonates remain unreasonable scarce.
The results from the present study illustrate the difficulties in obtaining data from the very youngest and smallest neonates. Particularly, it is challenging to explore include patients shortly after birth and consequently the early stages of xenobiotic biotransformation ontogeny remain relatively underexplored.
This is exemplified by our findings, as most studies lacked detailed information, e.g., on the number of very and extremely preterm neonates. Importantly, the post-natal age at sampling for the included patients were often not specified, making definitive interpretation of these early stages of xenobiotic biotransformation very difficult. Finally, details on the number of samples deriving from the preterm neonates was also seldom reported.
As expected, we did find an overall clear tendency of an immature, and thus reduced, drug metabolism in the preterm infants when compared to term neonates and older children. This was the case for virtually all reported enzyme-systems. However, as we also found a large heterogeneity in the studies, including methodological differences in the studies pathways and the use of both non-compartmental- and population PK methods, we cannot perform any direct comparison or formal meta-analysis of the reported findings.
Neonatology has been fortunate to experience some major leaps in pharmacology treatments for premature children but game-changing drugs like surfactant are rare. However, new therapeutic products are increasingly being studied for neonatal diseases and advances are constantly being made. These current and future advances must integrate the increased knowledge of the ontogeny of organ and enzyme systems in premature children. Thereby we can construct optimized models that takes into consideration the normal maturation of neonates (van den Anker and Allegaert, 2021).
As illustrated, there is still a lack of data from extremely premature children sampled shortly after birth, a testament to the practical and ethical challenges. Neonatal pharmacological research could benefit from increased representation of multidisciplinary neonatal clinicians on relevant committees to streamlining of ethics and governance procedures for multi-site studies. This will likely require dedicated time and support as clinician time for additional service outside of clinical care is often unfunded and burdensome. Similarly, the practicalities of inclusion of extremely premature children immediately after birth may be tackled by increased use of antenatal parental consent (Memon et al., 2020).
Obviously, the development of sparse plasma/blood sampling and analyzing techniques improve the feasibility of including the very small preterm neonates. This fact, and the use of left-over or opportunistic samples from routine sampling will yield a higher inclusion rate. Pharmacometric modeling approaches have reduced the high number of samples needed, but by combining these modern techniques with a higher inclusion rate, a high level of detailing will be possible By use of already existing modeling methods and optimal sampling design, parameter estimation with maximal precision is possible (Smits et al., 2021). However, refinement of these methods will be important for the future.
From a regulatory point of view, it would be highly desirable if continued improvements on targeted and efficient clinical trial designs in neonates became standard in pediatric drug development. Herein, PK and PD characterization in the pediatric subgroup of neonatology should be considered from the earliest drug development stages.
Furthermore, development of microdosing studies present an attractive alternative to overcome ethical and analytical challenges in phenotyping studies. Microdoses are subtherapeutic doses (typically < 100th of therapeutic dose) that are unlikely to elicit any pharmaceutical response or side effects. The microdosing approach has been validated for, e.g., midazolam in preterm neonates (van Groen et al., 2019).
The use of international multicenter studies, pediatric trial networks, diverse databases, biomarkers, and integration of Real-world Data, use of artificial intelligence and machine learning such as text mining and deep-learning models to extract relevant information from electronic patient records is likely to further advance neonatal pharmacology (Mulugeta et al., 2018; Goulooze et al., 2020; Smits et al.). However, models of any kind should be developed wisely, bearing in mind that the risk of poor performance is particularly high if certain age groups such as preterm neonates are underrepresented or absent in the data set used to develop the model (Mulugeta et al., 2018; Goulooze et al., 2020; Smits et al.).
This review highlights the insufficiencies in the current knowledge of the maturation of drug metabolizing enzymes in preterm neonates, and particularly in the very or extremely preterm neonates. We illustrate the overall heterogeneous approach to measuring and presenting the phase I and II pathways metabolism in preterm neonates, often with use of exclusively opportunistic sampling—a testament to the practical and ethical challenges in measuring pharmacokinetic activity in preterm neonates.
With the advances in overall neonatal intensive care, the limit for possible survival in extremely preterm neonates has improved. Consequently, neonates with increasingly lower gestational age at birth now require care, including intensive pharmacological treatment. This calls for optimized designs of future pharmacometrics studies, preferably as multi-site/international collaboration between neonatologists and clinical pharmacologists that will allow for integration of all available techniques, including low volume plasma/blood analysis techniques, pharmacokinetic modeling, “Big Data”, and even machine learning.
The understanding of the impact of growth, development, and organ maturation on the absorption, distribution, metabolism, and excretion of drugs in neonates, infants, children, and adolescents has progressed tremendously in recent decades, but it has mainly been driven by a few, but dedicated researchers; it is now time for the broader pharmacological scientific community to turn its gaze toward the most premature children.
MM: Project coordinator, drafted the initial manuscript, collected data, and approved the final manuscript as submitted, CG: conceptualized and designed the study, drafted the initial manuscript, designed the data collections instrument, and approved the final manuscript as submitted. UL-T: conceptualized and designed the study, drafted the initial manuscript, designed the data collection instrument, and approved the final manuscript as submitted, JA: conceptualized and designed the study, designed the data collection instrument, reviewed and revised the manuscript, and approved the final manuscript as submitted.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Al-Turkait, A., Szatkowski, L., Choonara, I., and Ojha, S. (2020). Review of Drug Utilization Studies in Neonatal Units: A Global Perspective. Int. J. Environ. Res. Public Health 17, E5669. doi:10.3390/ijerph17165669
Ali, A. S., Farouq, M. F., and Al-Faify, K. A. (2012). Pharmacokinetic Approach for Optimizing Gentamicin Use in Neonates during the First Week of Life. Indian J. Pharmacol. 44, 36–40. doi:10.4103/0253-7613.91864
Allegaert, K. (2017). Better Medicines for Neonates: Improving Medicine Development, Testing, and Prescribing. Early Hum. Dev. 114, 22–25. doi:10.1016/j.earlhumdev.2017.09.007
Allegaert, K., Holford, N., Anderson, B. J., Holford, S., Stuber, F., Rochette, A., et al. (2015). Tramadol and O-Desmethyl Tramadol Clearance Maturation and Disposition in Humans: a Pooled Pharmacokinetic Study. Clin. Pharmacokinet. 54, 167–178. doi:10.1007/s40262-014-0191-9
Allegaert, K., van den Anker, J. N., de Hoon, J. N., van Schaik, R. H. N., Debeer, A., Tibboel, D., et al. (2008a). Covariates of Tramadol Disposition in the First Months of Life. Br. J. Anaesth. 100, 525–532. doi:10.1093/bja/aen019
Allegaert, K., van Schaik, R. H. N., Vermeersch, S., Verbesselt, R., Cossey, V., Vanhole, C., et al. (2008b). Postmenstrual Age and CYP2D6 Polymorphisms Determine Tramadol O-Demethylation in Critically Ill Neonates and Infants. Pediatr. Res. 63, 674–679. doi:10.1203/PDR.0b013e31816ff712
Anderson, B. J., and Holford, N. H. G. (2018). Negligible Impact of Birth on Renal Function and Drug Metabolism. Paediatr. Anaesth. 28, 1015–1021. doi:10.1111/pan.13497
EMA, (2018). Investigation of Medicinal Products in the Term and Preterm Neonate. Eur. Med. Agency. Available at: https://www.ema.europa.eu/en/investigation-medicinal-products-term-preterm-neonate (Accessed December 1, 2021).
Aranda, J. V., Sitar, D. S., Parsons, W. D., Loughnan, P. M., and Neims, A. H. (1976). Pharmacokinetic Aspects of Theophylline in Premature Newborns. N. Engl. J. Med. 295, 413–416. doi:10.1056/NEJM197608192950803
Auriti, C., Falcone, M., Ronchetti, M. P., Goffredo, B. M., Cairoli, S., Crisafulli, R., et al. (2016). High-Dose Micafungin for Preterm Neonates and Infants with Invasive and Central Nervous System Candidiasis. Antimicrob. Agents Chemother. 60, 7333–7339. doi:10.1128/AAC.01172-16
Barker, C. I. S., Standing, J. F., Kelly, L. E., Hanly Faught, L., Needham, A. C., Rieder, M. J., et al. (2018). Pharmacokinetic Studies in Children: Recommendations for Practice and Research. Arch. Dis. Child. 103, 695–702. doi:10.1136/archdischild-2017-314506
Barr, J., Brenner-Zada, G., Heiman, E., Pareth, G., Bulkowstein, M., Greenberg, R., et al. (2002). Unlicensed and Off-Label Medication Use in a Neonatal Intensive Care Unit: a Prospective Study. Am. J. Perinatol. 19, 67–72. doi:10.1055/s-2002-23557
Bekker, A., Schaaf, H. S., Seifart, H. I., Draper, H. R., Werely, C. J., Cotton, M. F., et al. (2014). Pharmacokinetics of Isoniazid in Low-Birth-Weight and Premature Infants. Antimicrob. Agents Chemother. 58, 2229–2234. doi:10.1128/AAC.01532-13
Blake, M. J., Abdel-Rahman, S. M., Pearce, R. E., Leeder, J. S., and Kearns, G. L. (2006). Effect of Diet on the Development of Drug Metabolism by Cytochrome P-450 Enzymes in Healthy Infants. Pediatr. Res. 60, 717–723. doi:10.1203/01.pdr.0000245909.74166.00
Blencowe, H., Cousens, S., Oestergaard, M. Z., Chou, D., Moller, A.-B., Narwal, R., et al. (2012). National, Regional, and Worldwide Estimates of Preterm Birth Rates in the Year 2010 with Time Trends since 1990 for Selected Countries: a Systematic Analysis and Implications. Lancet Lond. Engl. 379, 2162–2172. doi:10.1016/S0140-6736(12)60820-4
Bonner, J. J., Vajjah, P., Abduljalil, K., Jamei, M., Rostami-Hodjegan, A., Tucker, G. T., et al. (2015). Does Age Affect Gastric Emptying Time? A Model-Based Meta-Analysis of Data from Premature Neonates through to Adults. Biopharm. Drug Dispos. 36, 245–257. doi:10.1002/bdd.1937
Borzyskowski, M., Grant, D. B., and Wells, R. S. (1976). Cushing’s Syndrome Induced by Topical Steroids Used for the Treatment of Non-bullous Ichthyosiform Erythroderma. Clin. Exp. Dermatol. 1, 337–342. doi:10.1111/j.1365-2230.1976.tb01440.x
Brammer, K. W., and Coates, P. E. (1994). Pharmacokinetics of Fluconazole in Pediatric Patients. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 13, 325–329. doi:10.1007/BF01974613
Brayer, C., Micheau, P., Bony, C., Tauzin, L., Pilorget, H., Sampériz, S., et al. (2004). Neonatal Accidental Burn by Isopropyl Alcohol. Arch. Pediatr. Organe Off. Soc. Francaise Pediatr. 11, 932–935. doi:10.1016/j.arcped.2004.04.023
Brazier, J. L., Salle, B., Ribon, B., Desage, M., and Renaud, H. (1981). In Vivo N7 Methylation of Theophylline to Caffeine in Premature Infants. Studies with Use of Stable Isotopes. Dev. Pharmacol. Ther. 2, 137–144. doi:10.1159/000481025
Brumbaugh, J. E., Hansen, N. I., Bell, E. F., Sridhar, A., Carlo, W. A., Hintz, S. R., et al. (2019). Outcomes of Extremely Preterm Infants with Birth Weight Less Than 400 G. JAMA Pediatr. 173, 434–445. doi:10.1001/jamapediatrics.2019.0180
Brussee, J. M., Yu, H., Krekels, E. H. J., de Roos, B., Brill, M. J. E., van den Anker, J. N., et al. (2018). First-Pass CYP3A-Mediated Metabolism of Midazolam in the Gut Wall and Liver in Preterm Neonates. CPT Pharmacomet. Syst. Pharmacol. 7, 374–383. doi:10.1002/psp4.12295
Burtin, P., Jacqz-Aigrain, E., Girard, P., Lenclen, R., Magny, J. F., Betremieux, P., et al. (1994). Population Pharmacokinetics of Midazolam in Neonates. Clin. Pharmacol. Ther. 56, 615–625. doi:10.1038/clpt.1994.186
Chawanpaiboon, S., Vogel, J. P., Moller, A.-B., Lumbiganon, P., Petzold, M., Hogan, D., et al. (2019). Global, Regional, and National Estimates of Levels of Preterm Birth in 2014: a Systematic Review and Modelling Analysis. Lancet Glob. Health 7, e37–e46. doi:10.1016/S2214-109X(18)30451-0
Choonara, I. A., McKay, P., Hain, R., and Rane, A. (1989). Morphine Metabolism in Children. Br. J. Clin. Pharmacol. 28, 599–604. doi:10.1111/j.1365-2125.1989.tb03548.x
Cook, S. F., Stockmann, C., Samiee-Zafarghandy, S., King, A. D., Deutsch, N., Williams, E. F., et al. (2016). Neonatal Maturation of Paracetamol (Acetaminophen) Glucuronidation, Sulfation, and Oxidation Based on a Parent-Metabolite Population Pharmacokinetic Model. Clin. Pharmacokinet. 55, 1395–1411. doi:10.1007/s40262-016-0408-1
Cowen, J., Ellis, S. H., and McAinsh, J. (1979). Absorption of Chlorhexidine from the Intact Skin of Newborn Infants. Arch. Dis. Child. 54, 379–383. doi:10.1136/adc.54.5.379
Craft, A. W., Brocklebank, J. T., Hey, E. N., and Jackson, R. H. (1974). The “Grey Toddler”. Chloramphenicol Toxicity. Arch. Dis. Child. 49, 235–237. doi:10.1136/adc.49.3.235
Czekaj, P., Wiaderkiewicz, A., Florek, E., and Wiaderkiewicz, R. (2005). Tobacco Smoke-dependent Changes in Cytochrome P450 1A1, 1A2, and 2E1 Protein Expressions in Fetuses, Newborns, Pregnant Rats, and Human Placenta. Arch. Toxicol. 79, 13–24. doi:10.1007/s00204-004-0607-7
de Waal, R., Kroon, S. M., Holgate, S. L., Horn, A. R., Tooke, L. J., Norman, J., et al. (2014). Nevirapine Concentrations in Preterm and Low Birth Weight HIV-Exposed Infants: Implications for Dosing Recommendations. Pediatr. Infect. Dis. J. 33, 1231–1233. doi:10.1097/INF.0000000000000453
de Wildt, S. N., Kearns, G. L., Hop, W. C. J., Murry, D. J., Abdel-Rahman, S. M., and van den Anker, J. N. (2002). Pharmacokinetics and Metabolism of Oral Midazolam in Preterm Infants. Br. J. Clin. Pharmacol. 53, 390–392. doi:10.1046/j.1365-2125.2002.01223.x
de Wildt, S. N., Kearns, G. L., Hop, W. C., Murry, D. J., Abdel-Rahman, S. M., and van den Anker, J. N. (2001). Pharmacokinetics and Metabolism of Intravenous Midazolam in Preterm Infants. Clin. Pharmacol. Ther. 70, 525–531. doi:10.1067/mcp.2001.120683
de Wildt, S. N., Kearns, G. L., Leeder, J. S., and van den Anker, J. N. (1999). Cytochrome P450 3A: Ontogeny and Drug Disposition. Clin. Pharmacokinet. 37, 485–505. doi:10.2165/00003088-199937060-00004
de Wildt, S. N., Kearns, G. L., Murry, D. J., Koren, G., and van den Anker, J. N. (2010). Ontogeny of Midazolam Glucuronidation in Preterm Infants. Eur. J. Clin. Pharmacol. 66, 165–170. doi:10.1007/s00228-009-0741-5
Ehrnebo, M., Agurell, S., Jalling, B., and Boréus, L. O. (1971). Age Differences in Drug Binding by Plasma Proteins: Studies on Human Foetuses, Neonates and Adults. Eur. J. Clin. Pharmacol. 3, 189–193. doi:10.1007/BF00565004
Engle, W. A. (2004). American Academy of Pediatrics Committee on Fetus and NewbornAge Terminology during the Perinatal Period. Pediatrics 114, 1362–1364. doi:10.1542/peds.2004-1915
European Medicines Agency and its Paediatric Committee (2016). 10-year Report to the European Commission - General Report on the Experience Acquired as a Result of the Application of the Paediatric Regulation. Available at: https://ec.europa.eu/health/sites/health/files/files/paediatrics/2016_pc_report_2017/ema_10_year_report_for_consultation.pdf (Accessed December 16, 2018).
Flint, R. B., Roofthooft, D. W., van Rongen, A., van Lingen, R. A., van den Anker, J. N., van Dijk, M., et al. (2017). Exposure to Acetaminophen and All its Metabolites upon 10, 15, and 20mg/kgintravenous Acetaminophen in Very -preterminfants. Pediatr. Res 82, 678–684. doi:10.1038/pr.2017.129
Ford, S., and Calvert, J. (2008). Adaptation for Life: A Review of Neonatal Physiology. Anaesth. Intensive Care Med. 12, 93–98. doi:10.1016/j.mpaic.2008.01.009
Fredholm, B. B., Rane, A., and Persson, B. (1975). Diphenylhydantoin Binding to Proteins in Plasma and its Dependence on Free Fatty Acid and Bilirubin Concentration in Dogs and Newborn Infants. Pediatr. Res. 9, 26–30. doi:10.1203/00006450-197501000-00005
Fuchs, A., Guidi, M., Giannoni, E., Werner, D., Buclin, T., Widmer, N., et al. (2014). Population Pharmacokinetic Study of Gentamicin in a Large Cohort of Premature and Term Neonates. Br. J. Clin. Pharmacol. 78, 1090–1101. doi:10.1111/bcp.12444
Fujii, R., Matsumoto, S., Sakiyama, Y., Ishikawa, Y., Takeda, T., Hatae, Y., et al. (1993). A Clinical Study of Fluconazole-Granules and -injectable in Pediatric Patients with Deep-Seated Mycoses. Jpn. J. Antibiot. 46, 654–685. doi:10.11553/antibiotics1968b.46.654
Fujiwara, T., Maeta, H., Chida, S., Morita, T., Watabe, Y., and Abe, T. (1980). Artificial Surfactant Therapy in Hyaline-Membrane Disease. Lancet Lond. Engl. 1, 55–59. doi:10.1016/s0140-6736(80)90489-4
George, M., Kitzmiller, J. P., Ewald, M. B., O’Donell, K. A., Becter, M. L., and Salhanick, S. (2012). Methadone Toxicity and Possible Induction and Enhanced Elimination in a Premature Neonate. J. Med. Toxicol. Off. J. Am. Coll. Med. Toxicol. 8, 432–435. doi:10.1007/s13181-012-0249-8
Gerhart, J. G., Watt, K. M., Edginton, A., Wade, K. C., Salerno, S. N., Benjamin, D. K., et al. (2019). Physiologically-Based Pharmacokinetic Modeling of Fluconazole Using Plasma and Cerebrospinal Fluid Samples from Preterm and Term Infants. CPT Pharmacomet. Syst. Pharmacol. 8, 500–510. doi:10.1002/psp4.12414
Gershanik, J., Boecler, B., Ensley, H., McCloskey, S., and George, W. (1982). The Gasping Syndrome and Benzyl Alcohol Poisoning. N. Engl. J. Med. 307, 1384–1388. doi:10.1056/NEJM198211253072206
Glass, H. C., Costarino, A. T., Stayer, S. A., Brett, C. M., Cladis, F., and Davis, P. J. (2015). Outcomes for Extremely Premature Infants. Anesth. Analg. 120, 1337–1351. doi:10.1213/ANE.0000000000000705
Gonzalez, D., Laughon, M. M., Smith, P. B., Ge, S., Ambalavanan, N., Atz, A., et al. (2019). Population Pharmacokinetics of Sildenafil in Extremely Premature Infants. Br. J. Clin. Pharmacol. 85, 2824–2837. doi:10.1111/bcp.14111
Goulooze, S. C., Zwep, L. B., Vogt, J. E., Krekels, E. H. J., Hankemeier, T., van den Anker, J. N., et al. (2020). Beyond the Randomized Clinical Trial: Innovative Data Science to Close the Pediatric Evidence Gap. Clin. Pharmacol. Ther. 107, 786–795. doi:10.1002/cpt.1744
Gow, P. J., Ghabrial, H., Smallwood, R. A., Morgan, D. J., and Ching, M. S. (2001). Neonatal Hepatic Drug Elimination. Pharmacol. Toxicol. 88, 3–15. doi:10.1034/j.1600-0773.2001.088001003.x
Grasela, T. H., and Donn, S. M. (1985). Neonatal Population Pharmacokinetics of Phenobarbital Derived from Routine Clinical Data. Dev. Pharmacol. Ther. 8, 374–383. doi:10.1159/000457062
Grygiel, J. J., and Birkett, D. J. (1980). Effect of Age on Patterns of Theophylline Metabolism. Clin. Pharmacol. Ther. 28, 456–462. doi:10.1038/clpt.1980.188
Saxén, H., Hoppu, K., and Pohjavuori, M., (1993). Pharmacokinetics of Fluconazole in Very Low Birth Weight Infants during the First Two Weeks of Life. Clin. Pharmacol. Ther. 54, 269–277. doi:10.1038/clpt.1993.147
Harrison, M. S., and Goldenberg, R. L. (2016). Global burden of Prematurity. Semin. Fetal Neonatal. Med. 21, 74–79. doi:10.1016/j.siny.2015.12.007
Hartley, R., Green, M., Quinn, M. W., Rushforth, J. A., and Levene, M. I. (1994). Development of Morphine Glucuronidation in Premature Neonates. Biol. Neonate 66, 1–9. doi:10.1159/000244083
Hartley, R., Quinn, M., Green, M., and Levene, M. I. (1993). Morphine Glucuronidation in Premature Neonates. Br. J. Clin. Pharmacol. 35, 314–317. doi:10.1159/000244083
Hayton, W. L. (2000). Maturation and Growth of Renal Function: Dosing Renally Cleared Drugs in Children. AAPS PharmSci 2, E3. doi:10.1208/ps020103
Helenius, K., Sjörs, G., Shah, P. S., Modi, N., Reichman, B., Morisaki, N., et al. (2017). Survival in Very Preterm Infants: An International Comparison of 10 National Neonatal Networks. Pediatrics 140, e20171264. doi:10.1542/peds.2017-1264
Hentschel, R., Bohlin, K., van Kaam, A., Fuchs, H., and Danhaive, O. (2020). Surfactant Replacement Therapy: from Biological Basis to Current Clinical Practice. Pediatr. Res. 88, 176–183. doi:10.1038/s41390-020-0750-8
Hines, R. N., and McCarver, D. G. (2002). The Ontogeny of Human Drug-Metabolizing Enzymes: Phase I Oxidative Enzymes. J. Pharmacol. Exp. Ther. 300, 355–360. doi:10.1124/jpet.300.2.355
Hwang, M. F., Beechinor, R. J., Wade, K. C., Benjamin, D. K., Smith, P. B., Hornik, C. P., et al. (2017). External Evaluation of Two Fluconazole Infant Population Pharmacokinetic Models. Antimicrob. Agents Chemother. 61, e01352–17. doi:10.1128/AAC.01352-17
Ince, I., de Wildt, S. N., Wang, C., Wang, C., Peeters, M. Y. M., Burggraaf, J., et al. (2013). A Novel Maturation Function for Clearance of the Cytochrome P450 3A Substrate Midazolam from Preterm Neonates to Adults. Clin. Pharmacokinet. 52, 555–565. doi:10.1007/s40262-013-0050-0
Ishii, N., Kono, Y., Yonemoto, N., Kusuda, S., and Fujimura, M.Neonatal Research Network, Japan (2013). Outcomes of Infants Born at 22 and 23 Weeks’ Gestation. Pediatrics 132, 62–71. doi:10.1542/peds.2012-2857
Italian Collaborative Group on Preterm Delivery (1991). Absorption of Intramuscular Vitamin E in Premature Babies. Dev. Pharmacol. Ther. 16, 13–21. doi:10.1159/000480550
Jiang, Z., Gao, X., Liang, J., and Ni, S. (2021). Simultaneous Quantitation of Serum Caffeine and its Metabolites by Ultra-high-performance Liquid Chromatography–Tandem Mass Spectrometry for CYP1A2 Activity Prediction in Premature Infants. Biomed. Chromatogr. 35, e5141. doi:10.1002/bmc.5141
Jm, B., Nj, V., Ehj, K., Aj, V., E, J.-A., Jma, van. G., et al. (2018). Predicting CYP3A-Mediated Midazolam Metabolism in Critically Ill Neonates, Infants, Children and Adults with Inflammation and Organ Failure. Br. J. Clin. Pharmacol. 84, 358–368. doi:10.1111/bcp.13459
Johnson, P. J. (2011). Neonatal Pharmacology-Ppharmacokinetics. Neonatal. Netw. NN 30, 54–61. doi:10.1891/0730-0832.30.1.54
Kafetzis, D. A., Sinaniotis, C. A., Papadatos, C. J., and Kosmidis, J. (1979). Pharmacokinetics of Amikacin in Infants and Pre-school Children. Acta Paediatr. Scand. 68, 419–422. doi:10.1111/j.1651-2227.1979.tb05030.x
Kawade, N., and Onishi, S. (1981). The Prenatal and Postnatal Development of UDP-Glucuronyltransferase Activity towards Bilirubin and the Effect of Premature Birth on This Activity in the Human Liver. Biochem. J. 196, 257–260. doi:10.1042/bj1960257
Kearns, G. L., Abdel-Rahman, S. M., Alander, S. W., Blowey, D. L., Leeder, J. S., and Kauffman, R. E. (2003). Developmental Pharmacology-Ddrug Disposition, Action, and Therapy in Infants and Children. N. Engl. J. Med. 349, 1157–1167. doi:10.1056/NEJMra035092
Kim, S. E., Kim, B.-H., Lee, S., Sohn, J. A., Kim, H.-S., Cho, J.-Y., et al. (2013). Population Pharmacokinetics of Theophylline in Premature Korean Infants. Ther. Drug Monit. 35, 338–344. doi:10.1097/FTD.0b013e3182866695
Knibbe, C. A. J., Krekels, E. H. J., van den Anker, J. N., DeJongh, J., Santen, G. W. E., van Dijk, M., et al. (2009). Morphine Glucuronidation in Preterm Neonates, Infants and Children Younger Than 3 Years. Clin. Pharmacokinet. 48, 371–385. doi:10.2165/00003088-200948060-00003
Krekels, E. H. J., van Ham, S., Allegaert, K., de Hoon, J., Tibboel, D., Danhof, M., et al. (2015). Developmental Changes rather Than Repeated Administration Drive Paracetamol Glucuronidation in Neonates and Infants. Eur. J. Clin. Pharmacol. 71, 1075–1082. doi:10.1007/s00228-015-1887-y
Ku, L. C., and Smith, P. B. (2015). Dosing in Neonates: Special Considerations in Physiology and Trial Design. Pediatr. Res. 77, 2–9. doi:10.1038/pr.2014.143
Le Doare, K., Barber, N., Doerholt, K., and Sharland, M. (20132013). Rifampicin Pharmacokinetics in Extreme Prematurity to Treat Congenital Tuberculosis. BMJ Case Rep., bcr2012008207. doi:10.1136/bcr-2012-008207
Lee, T. C., Charles, B. G., Harte, G. J., Gray, P. H., Steer, P. A., and Flenady, V. J. (1999). Population Pharmacokinetic Modeling in Very Premature Infants Receiving Midazolam during Mechanical Ventilation: Midazolam Neonatal Pharmacokinetics. Anesthesiology 90, 451–457. doi:10.1097/00000542-199902000-00020
Leroux, S., Jacqz-Aigrain, E., Elie, V., Legrand, F., Barin-Le Guellec, C., Aurich, B., et al. (2018). Pharmacokinetics and Safety of Fluconazole and Micafungin in Neonates with Systemic Candidiasis: a Randomized, Open-Label Clinical Trial. Br. J. Clin. Pharmacol. 84, 1989–1999. doi:10.1111/bcp.13628
Li, Q., Wu, Y.-E., Wang, K., Shi, H.-Y., Zhou, Y., Zheng, Y., et al. (2021). Developmental Pharmacogenetics of CYP2D6 in Chinese Children: Loratadine as a Substrate Drug. Front. Pharmacol. 12, 1396. doi:10.3389/fphar.2021.657287
Liggins, G. C., and Howie, R. N. (1972). A Controlled Trial of Antepartum Glucocorticoid Treatment for Prevention of the Respiratory Distress Syndrome in Premature Infants. Pediatrics 50, 515–525. doi:10.1542/peds.50.4.515
Liu, X., Chen, C., and Smith, B. J. (2008). Progress in Brain Penetration Evaluation in Drug Discovery and Development. J. Pharmacol. Exp. Ther. 325, 349–356. doi:10.1124/jpet.107.130294
Loughnan, P. M., Greenwald, A., Purton, W. W., Aranda, J. V., Watters, G., and Neims, A. H. (1977). Pharmacokinetic Observations of Phenytoin Disposition in the Newborn and Young Infant. Arch. Dis. Child. 52, 302–309. doi:10.1136/adc.52.4.302
Lowry, J. A., Jarrett, R. V., Wasserman, G., Pettett, G., and Kauffman, R. E. (2001). Theophylline Toxicokinetics in Premature Newborns. Arch. Pediatr. Adolesc. Med. 155, 934–939. doi:10.1001/archpedi.155.8.934
Mahmood, I. (2017). Prediction of Clearance, Volume of Distribution, and Half-Life of Drugs in Extremely Low to Low Birth Weight Neonates: An Allometric Approach. Eur. J. Drug Metab. Pharmacokinet. 42, 601–610. doi:10.1007/s13318-016-0372-z
Mahmood, I. (2015). Prediction of Glucuronidated Drug Clearance in Pediatrics (≤5 Years): An Allometric Approach. Eur. J. Drug Metab. Pharmacokinet. 40, 53–59. doi:10.1007/s13318-014-0178-9
McGoldrick, E., Stewart, F., Parker, R., and Dalziel, S. R. (2020). Antenatal Corticosteroids for Accelerating Fetal Lung Maturation for Women at Risk of Preterm Birth. Cochrane Database Syst. Rev. 12, CD004454. doi:10.1002/14651858.CD004454.pub4
Memon, N., Griffin, I. J., Lee, C. W., Herdt, A., Weinberger, B. I., Hegyi, T., et al. (2020). Developmental Regulation of the Gut-Liver (FGF19-Cyp7a1) axis in Neonates. J. Matern.-Fetal Neonatal. Med. Off. J. Eur. Assoc. Perinat. Med. Fed. Asia Ocean. Perinat. Soc. Int. Soc. Perinat. Obstet. 33, 987–992. doi:10.1080/14767058.2018.1513483
Hwang, M. F., Beechinor, R. J., Wade, K. C., Benjamin, D. K., Smith, P. B., et al. (2017). External Evaluation of Two Fluconazole Infant Population Pharmacokinetic Models. Antimicrob. Agents Chemother. 61. doi:10.1128/AAC.01352-17
Michelet, R., Van Bocxlaer, J., Allegaert, K., and Vermeulen, A. (2018). The Use of PBPK Modeling across the Pediatric Age Range Using Propofol as a Case. J. Pharmacokinet. Pharmacodyn. 45, 765–785. doi:10.1007/s10928-018-9607-8
Momper, J. D., Capparelli, E. V., Wade, K. C., Kantak, A., Dhanireddy, R., Cummings, J. J., et al. (2016). Population Pharmacokinetics of Fluconazole in Premature Infants with Birth Weights Less Than 750 Grams. Antimicrob. Agents Chemother. 60, 5539–5545. doi:10.1128/AAC.00963-16
De Carolis, M. P., Muzii, U., Romagnoli, C., Zuppa, A. A., Zecca, E., and Tortorolo, G. (1989). Phenobarbital for Treatment of Seizures in Preterm Infant: a New Administration Scheme. Dev. Pharmacol. Ther. 14, 84–89. doi:10.1159/000480923
Mugabo, P., Els, I., Smith, J., Rabie, H., Smith, P., Mirochnick, M., et al. (2011). Nevirapine Plasma Concentrations in Premature Infants Exposed to Single-Dose Nevirapine for Prevention of Mother-To-Child Transmission of HIV-1. South. Afr. Med. J. Suid-afr. Tydskr. Vir Geneeskd. 101, 655–658.
Mulhall, A., de Louvois, J., and Hurley, R. (1983a). Chloramphenicol Toxicity in Neonates: its Incidence and Prevention. Br. Med. J. Clin. Res. Ed. 287, 1424–1427. doi:10.1136/bmj.287.6403.1424
Mulugeta, L. Y., Yao, L., Mould, D., Jacobs, B., Florian, J., Smith, B., et al. (2018). Leveraging Big Data in Pediatric Development Programs: Proceedings from the 2016 American College of Clinical Pharmacology Annual Meeting Symposium. Clin. Pharmacol. Ther. 104, 81–87. doi:10.1002/cpt.975
Munro, D. D. (1976). The Effect of Percutaneously Absorbed Steroids on Hypothalamic--pituitary--adrenal function after intensive use in in-patients. Br. J. Dermatol. 94 (Suppl. 12), 67–76. doi:10.1111/j.1365-2133.1976.tb02272.x
Neyro, V., Elie, V., Médard, Y., and Jacqz-Aigrain, E. (2018). mRNA expression of drug metabolism enzymes and transporter genes at birth using human umbilical cord blood. Fundam. Clin. Pharmacol. 32, 422–435. doi:10.1111/fcp.12357
Ng, E., Taddio, A., and Ohlsson, A. (2012). Intravenous midazolam infusion for sedation of infants in the neonatal intensive care unit. Cochrane Database Syst. Rev. 13, CD002052. doi:10.1002/14651858.CD002052.pub2
Norman, M., Hallberg, B., Abrahamsson, T., Björklund, L. J., Domellöf, M., Farooqi, A., et al. (2019). Association Between Year of Birth and 1-Year Survival Among Extremely Preterm Infants in Sweden During 2004-2007 and 2014-2016. JAMA 321, 1188–1199. doi:10.1001/jama.2019.2021
Ogawa, Y., Irikura, M., Kobaru, Y., Tomiyasu, M., Kochiyama, Y., Uriu, M., et al. (2015). Population pharmacokinetics of doxapram in low-birth-weight Japanese infants with apnea. Eur. J. Pediatr. 174, 509–518. doi:10.1007/s00431-014-2416-1
O’Hara, K., Martin, J. H., and Schneider, J. J. (2020). Barriers and Challenges in Performing Pharmacokinetic Studies to Inform Dosing in the Neonatal Population. Pharm. Basel Switz. 8, E16. doi:10.3390/pharmacy8010016
O’Hara, K., Wright, I. M. R., Schneider, J. J., Jones, A. L., and Martin, J. H. (2015). Pharmacokinetics in neonatal prescribing: evidence base, paradigms and the future. Br. J. Clin. Pharmacol. 80, 1281–1288. doi:10.1111/bcp.12741
Onishi, S., Kawade, N., Itoh, S., Isobe, K., and Sugiyama, S. (1979). Postnatal development of uridine diphosphate glucuronyltransferase activity towards bilirubin and 2-aminophenol in human liver. Biochem. J. 184, 705–707. doi:10.1042/bj1840705
Pain, J. B., Lê, M. P., Caseris, M., Amiel, C., Lassel, L., Charpentier, C., et al. (2015). Pharmacokinetics of dolutegravir in a premature neonate after HIV treatment intensification during pregnancy. Antimicrob. Agents Chemother. 59, 3660–3662. doi:10.1128/AAC.00173-15
Painter, M. J., Pippenger, C., Wasterlain, C., Barmada, M., Pitlick, W., Carter, G., et al. (1981). Phenobarbital and phenytoin in neonatal seizures: metabolism and tissue distribution. Neurology 31, 1107–1112. doi:10.1212/wnl.31.9.1107
Pierrat, V., Marchand-Martin, L., Marret, S., Arnaud, C., Benhammou, V., Cambonie, G., et al. (2021). Neurodevelopmental outcomes at age 5 among children born preterm: EPIPAGE-2 cohort study. BMJ 373, n741. doi:10.1136/bmj.n741
Pitlick, W., Painter, M., and Pippenger, C. (1978). Phenobarbital pharmacokinetics in neonates. Clin. Pharmacol. Ther. 23, 346–350. doi:10.1002/cpt1978233346
Reiter, P. D., and Stiles, A. D. (1993). Lorazepam toxicity in a premature infant. Ann. Pharmacother. 27, 727–729. doi:10.1177/106002809302700611
Ribon, B., Brazier, J. L., Claris, O., Cortambert, F., Chouchane, N., Bannier, A., et al. (1984). Pharmacokinetic study in the premature newborn of a lyophilized form of phenobarbital. Dev. Pharmacol. Ther. 7 (Suppl. 1), 177–184. doi:10.1159/000457250
Rj, K., Tl, C., P, G., Jl, R., and Rl, W. (1990). Effect of phenobarbital administration on theophylline clearance in premature neonates. Ther. Drug Monit. 12, 139–143. doi:10.1097/00007691-199003000-00005
Rojas-Reyes, M. X., Morley, C. J., and Soll, R. (2012). Prophylactic versus selective use of surfactant in preventing morbidity and mortality in preterm infants. Cochrane Database Syst. Rev. 14, CD000510. doi:10.1002/14651858.CD000510.pub2
Roth-Cline, M., Gerson, J., Bright, P., Lee, C. S., and Nelson, R. M. (2011). Ethical considerations in conducting pediatric research. Handb. Exp. Pharmacol. 205, 219–244. doi:10.1007/978-3-642-20195-0_11
Ruggiero, S., Clavenna, A., Reale, L., Capuano, A., Rossi, F., and Bonati, M. (2014). Guanfacine for attention deficit and hyperactivity disorder in pediatrics: a systematic review and meta-analysis. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 24, 1578–1590. doi:10.1016/j.euroneuro.2014.08.001
Saigal, S., and Doyle, L. W. (2008). An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet Lond. Engl. 371, 261–269. doi:10.1016/S0140-6736(08)60136-1
Sardesai, S., Biniwale, M., Wertheimer, F., Garingo, A., and Ramanathan, R. (2017). Evolution of surfactant therapy for respiratory distress syndrome: past, present, and future. Pediatr. Res. 81, 240–248. doi:10.1038/pr.2016.203
Sato, J., Kudo, N., Owada, E., Ito, K., Niida, Y., Umetsu, M., et al. (1997). Urinary excretion of mefenamic acid and its metabolites including their esterglucuronides in preterm infants undergoing mefenamic acid therapy. Biol. Pharm. Bull. 20, 443–445. doi:10.1248/bpb.20.443
Schmidt, B., Roberts, R. S., Davis, P., Doyle, L. W., Barrington, K. J., Ohlsson, A., et al. (2006). Caffeine therapy for apnea of prematurity. N. Engl. J. Med. 354, 2112–2121. doi:10.1056/NEJMoa054065
Schrier, L., Hadjipanayis, A., Stiris, T., Ross-Russell, R. I., Valiulis, A., Turner, M. A., et al. (2020). Off-label use of medicines in neonates, infants, children, and adolescents: a joint policy statement by the European Academy of Paediatrics and the European society for Developmental Perinatal and Pediatric Pharmacology. Eur. J. Pediatr. 179, 839–847. doi:10.1007/s00431-019-03556-9
Shah, P. S., Dunn, M., Lee, S. K., Allen, A. C., and Singhal, N.Canadian Neonatal Network (2011). Early opioid infusion and neonatal outcomes in preterm neonates ≤28 weeks’ gestation. Am. J. Perinatol. 28, 361–366. doi:10.1055/s-0030-1270112
Sharma, A., Ford, S., and Calvert, J. (2008). Adaptation for life: a review of neonatal physiology. Anaesth. Intensive Care Med. 9 (3), 93–98. doi:10.1016/j.mpaic.2008.01.009
Smith, P. B., Cotten, C. M., Hudak, M. L., Sullivan, J. E., Poindexter, B. B., Cohen-Wolkowiez, M., et al. (2019). Rifampin Pharmacokinetics and Safety in Preterm and Term Infants. Antimicrob. Agents Chemother. 63, e00284–19. doi:10.1128/AAC.00284-19
Smits, A., Annaert, P., Cavallaro, G., De Cock, P. A. J. G., de Wildt, S. N., Kindblom, J. M., et al. (2021). Current knowledge, challenges and innovations in developmental pharmacology: A combined conect4children Expert Group and European Society for Developmental, Perinatal and Paediatric Pharmacology White Paper. Br. J. Clin. Pharmacol. N/a. Online ahead of print doi:10.1111/bcp.14958
Sohn, J. A., Kim, H.-S., Oh, J., Cho, J.-Y., Yu, K.-S., Lee, J., et al. (2017). Prediction of serum theophylline concentrations and cytochrome P450 1A2 activity by analyzing urinary metabolites in preterm infants. Br. J. Clin. Pharmacol. 83, 1279–1286. doi:10.1111/bcp.13211
Stark, A., Smith, P. B., Hornik, C. P., Zimmerman, K. O., Hornik, C. D., Pradeep, S., et al. (2021). Medication Use in the Neonatal Intensive Care Unit and Changes from 2010 to 2018. J. Pediatr. S0022-3476 (21), 00860–X. doi:10.1016/j.jpeds.2021.08.075
Stevens, T. P., Harrington, E. W., Blennow, M., and Soll, R. F. (2007). Early surfactant administration with brief ventilation vs. selective surfactant and continued mechanical ventilation for preterm infants with or at risk for respiratory distress syndrome. Cochrane Database Syst. Rev. 17, CD003063. doi:10.1002/14651858.CD003063.pub3
Sung, S. I., Ahn, S. Y., Yoo, H. S., Chang, Y. S., and Park, W. S. (2018). The Youngest Survivor with Gestational Age of 215/₇ Weeks. J. Korean Med. Sci. 33, e22. doi:10.3346/jkms.2018.33.e22
Sweet, D. G., Carnielli, V., Greisen, G., Hallman, M., Ozek, E., Te Pas, A., et al. (2019). European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2019 Update. Neonatology 115, 432–450. doi:10.1159/000499361
Tayman, C., Rayyan, M., and Allegaert, K. (2011). Neonatal pharmacology: extensive interindividual variability despite limited size. J. Pediatr. Pharmacol. Ther. JPPT Off. J. PPAG 16, 170–184. doi:10.5863/1551-6776-16.3.170
Tetelbaum, M., Finkelstein, Y., Nava-Ocampo, A. A., and Koren, G. (2005). Back to basics: understanding drugs in children: pharmacokinetic maturation. Pediatr. Rev. 26, 321–328. doi:10.1542/pir.26-9-321
Tiniest Babies Registry. University of Iowa.Available at: https://webapps1.healthcare.uiowa.edu/TiniestBabies/getInfantList.aspx (Accessed January 8, 2022).
Touw, D. J., Graafland, O., Cranendonk, A., Vermeulen, R. J., and van Weissenbruch, M. M. (2000). Clinical pharmacokinetics of phenobarbital in neonates. Eur. J. Pharm. Sci. Off. J. Eur. Fed. Pharm. Sci. 12, 111–116. doi:10.1016/s0928-0987(00)00145-7
Treluyer, J. M., Gueret, G., Cheron, G., Sonnier, M., and Cresteil, T. (1997). Developmental expression of CYP2C and CYP2C-dependent activities in the human liver: in-vivo/in-vitro correlation and inducibility. Pharmacogenetics 7, 441–452. doi:10.1097/00008571-199712000-00002
Tsakiri, S., Aneji, C., Domonoske, C., Mazur, L., Benjamin, D. K., and Wootton, S. H. (2018). Voriconazole Treatment for an Infant With Intractable Candida glabrata Meningitis. Pediatr. Infect. Dis. J. 37, 999–1001. doi:10.1097/INF.0000000000002073
Tserng, K. Y., Takieddine, F. N., and King, K. C. (1983). Developmental aspects of theophylline metabolism in premature infants. Clin. Pharmacol. Ther. 33, 522–528. doi:10.1038/clpt.1983.71
van den Anker, J., and Allegaert, K. (2021). Considerations for Drug Dosing in Premature Infants. J. Clin. Pharmacol. 61 (Suppl. 1), S141. –S151. doi:10.1002/jcph.1884
van den Anker, J., Reed, M. D., Allegaert, K., and Kearns, G. L. (2018). Developmental Changes in Pharmacokinetics and Pharmacodynamics. J. Clin. Pharmacol. 58 (Suppl. 10), S10. doi:10.1002/jcph.1284
Van Driest, S. L., and Choi, L. (2019). Real-World Data for Pediatric Pharmacometrics: Can We Upcycle Clinical Data for Research Use. Clin. Pharmacol. Ther. 106, 84–86. doi:10.1002/cpt.1416
van Groen, B. D., Vaes, W. H., Park, B. K., Krekels, E. H. J., van Duijn, E., Kõrgvee, L.-T., et al. (2019). Dose-linearity of the pharmacokinetics of an intravenous [14 C]midazolam microdose in children. Br. J. Clin. Pharmacol. 85, 2332–2340. doi:10.1111/bcp.14047
Vauzelle-Kervroedan, F., Rey, E., Pariente-Khayat, A., Bienvenu, T., Badoual, J., Olive, G., et al. (1996). Non invasive In Vivo study of the maturation of CYP IIIA in neonates and infants. Eur. J. Clin. Pharmacol. 51, 69–72. doi:10.1007/s002280050162
Völler, S., Flint, R. B., Stolk, L. M., Degraeuwe, P. L. J., Simons, S. H. P., Pokorna, P., et al. (2017). Model-based clinical dose optimization for phenobarbital in neonates: An illustration of the importance of data sharing and external validation. Eur. J. Pharm. Sci. Off. J. Eur. Fed. Pharm. Sci. 109S, S90. –S97. doi:10.1016/j.ejps.2017.05.026
Wade, K. C., Benjamin, D. K., Kaufman, D. A., Ward, R. M., Smith, P. B., Jayaraman, B., et al. (2009). Fluconazole dosing for the prevention or treatment of invasive candidiasis in young infants. Pediatr. Infect. Dis. J. 28, 717–723. doi:10.1097/INF.0b013e31819f1f50
Wade, K. C., Wu, D., Kaufman, D. A., Ward, R. M., Benjamin, D. K., Sullivan, J. E., et al. (2008). Population pharmacokinetics of fluconazole in young infants. Antimicrob. Agents Chemother. 52, 4043–4049. doi:10.1128/AAC.00569-08
Wang, C., Sadhavisvam, S., Krekels, E. H. J., Dahan, A., Tibboel, D., Danhof, M., et al. (2013). Developmental changes in morphine clearance across the entire paediatric age range are best described by a bodyweight-dependent exponent model. Clin. Drug Investig. 33, 523–534. doi:10.1007/s40261-013-0097-6
Ward, R. M., Tammara, B., Sullivan, S. E., Stewart, D. L., Rath, N., Meng, X., et al. (2010). Single-dose, multiple-dose, and population pharmacokinetics of pantoprazole in neonates and preterm infants with a clinical diagnosis of gastroesophageal reflux disease (GERD). Eur. J. Clin. Pharmacol. 66, 555–561. doi:10.1007/s00228-010-0811-8
Wenzl, T. G., Schefels, J., Hörnchen, H., and Skopnik, H. (1998). Pharmacokinetics of oral fluconazole in premature infants. Eur. J. Pediatr. 157, 661–662. doi:10.1007/s004310050906
Windorfer, A., Kuenzer, W., and Urbanek, R. (1974). The influence of age on the activity of acetylsalicylic acid-esterase and protein-salicylate binding. Eur. J. Clin. Pharmacol. 7, 227–231. doi:10.1007/BF00560385
Windorfer, A., and Pringsheim, W. (1977). Studies on the concentrations of chloramphenicol in the serum and cerebrospinal fluid of neonates, infants, and small children. Reciprocal reactions between chloramphenicol, penicillin and phenobarbitone. Eur. J. Pediatr. 124, 129–138. doi:10.1007/BF00477548
World Health Organization, (2004). ICD-10 : international statistical classification of diseases and related health problems : tenth revision. Available at: https://apps.who.int/iris/handle/10665/42980 (Accessed January 10, 2022).
Xu, C., Li, C. Y.-T., and Kong, A.-N. T. (2005). Induction of phase I, II and III drug metabolism/transport by xenobiotics. Arch. Pharm. Res. 28, 249–268. doi:10.1007/BF02977789
Zwart, L. D., Snoeys, J., Jacobs, F., Li, L. Y., Poggesi, I., Verboven, P., et al. (2021). Prediction of the drug-drug interaction potential of the alpha-acid glycoprotein bound, CYP3A4/CYP2C9 metabolized oncology drug. Erdafitinib. CPT Pharmacomet. Syst. Pharmacol. N/a. 10, 1107–1118. doi:10.1002/psp4.12682
Keywords: infant, premature, pharmacokinetics, cytochrome P-450 enzyme system, pharmaceutical preparations
Citation: Mørk ML, Andersen JT, Lausten-Thomsen U and Gade C (2022) The Blind Spot of Pharmacology: A Scoping Review of Drug Metabolism in Prematurely Born Children. Front. Pharmacol. 13:828010. doi: 10.3389/fphar.2022.828010
Received: 02 December 2021; Accepted: 25 January 2022;
Published: 15 February 2022.
Edited by:
Catherine M. T. Sherwin, Wright State University, United StatesReviewed by:
Kathleen Job, The University of Utah, United StatesCopyright © 2022 Mørk, Andersen, Lausten-Thomsen and Gade. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christina Gade, Q2hyaXN0aW5hLmdhZGVAcmVnaW9uaC5kaw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.