
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CORRECTION article
Front. Pharmacol. , 24 November 2022
Sec. Pharmacoepidemiology
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.1088973
 Martijn J. Schuemie1,2,3*
Martijn J. Schuemie1,2,3* Faaizah Arshad1,3
Faaizah Arshad1,3 Nicole Pratt4
Nicole Pratt4 Fredrik Nyberg5
Fredrik Nyberg5 Thamir M Alshammari6
Thamir M Alshammari6 George Hripcsak1,7
George Hripcsak1,7 Patrick Ryan1,2,7
Patrick Ryan1,2,7 Daniel Prieto-Alhambra8,9
Daniel Prieto-Alhambra8,9 Lana Y. H. Lai10
Lana Y. H. Lai10 Xintong Li11
Xintong Li11 Stephen Fortin2
Stephen Fortin2 Evan Minty10
Evan Minty10 Marc A. Suchard1,3,12
Marc A. Suchard1,3,12A Corrigendum on
Vaccine safety surveillance using routinely collected healthcare data—An empirical evaluation of epidemiological designs
by Schuemie MJ, Arshad F, Pratt N, Nyberg F, Alshammari TM, Hripcsak G, Ryan P, Prieto-Alhambra D, Lai LYH, Li X, Fortin S, Minty E and Suchard MA (2022). Front. Pharmacol. 13:893484. doi: 10.3389/fphar.2022.893484
In the published article, there was an error in Figure 4 and Figure 5 as published. After publication, the authors found that the positive control imputation multiplication was accidentally applied twice, meaning the intended multiplication of 1.25, 2, and 4 actually were 1.252 = 1.5625, 22 = 4, and 42 = 16, respectively. This means the type 2 error in Figure 4 and the time to 50% sensitivity in Figure 5 were underestimated. The corrected Figure 4 and Figure 5 appear below.
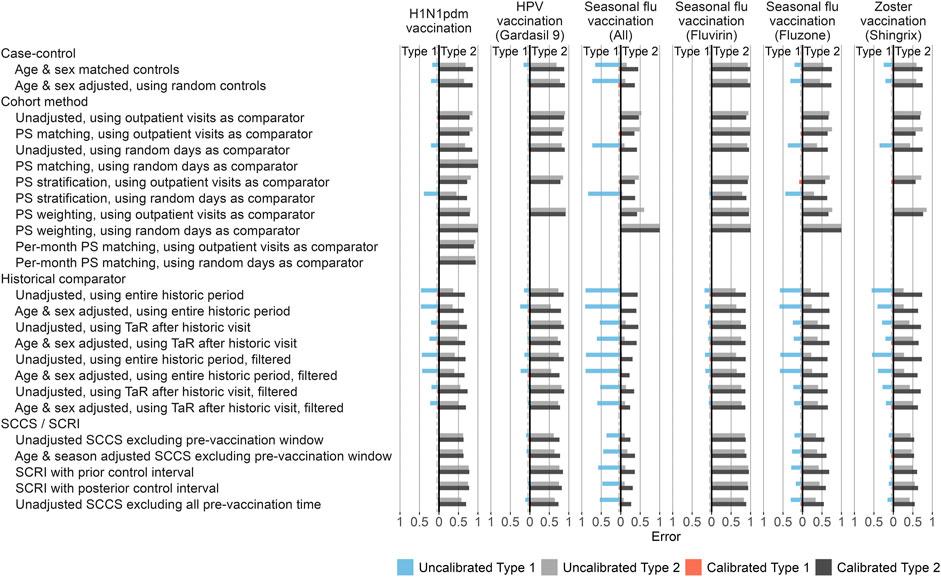
FIGURE 4. Type 1 and 2 error before and after empirical calibration. For each method variation and vaccine group, the type 1 and 2 error before and after empirical calibration in the Optum EHR database are shown. The x-axis indicates the type 1 error (higher values to the left) and type 2 error (higher values to the right), based on the (calibrated) one-sided p-value. The dashed line indicates nominal type 1 error of 5%. HPV = Human papillomavirus, PS = Propensity Score, SCCS = Self-Controlled Case Series, SCRI = Self-Controlled Risk Interval, TaR = Time-at-Risk.
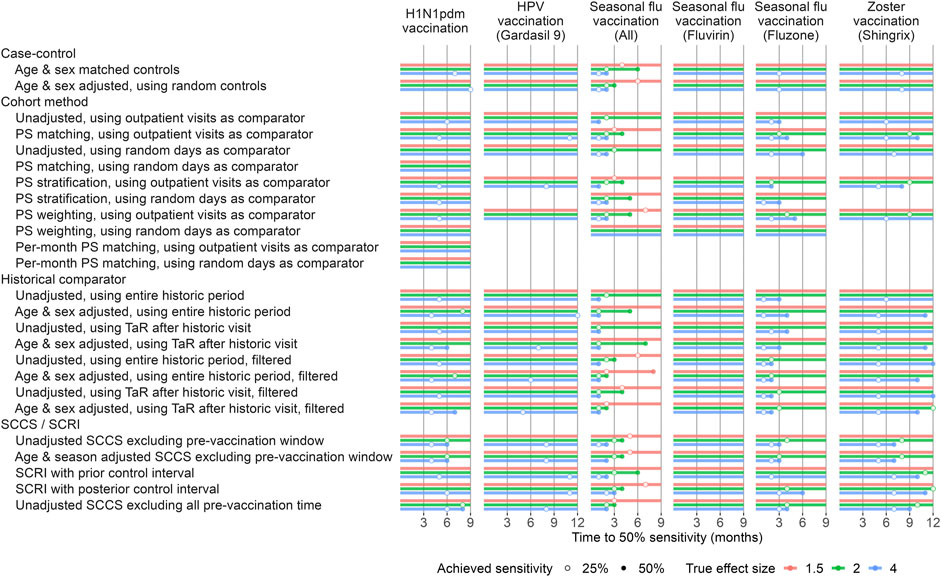
FIGURE 5. Time to 50% sensitivity after calibration. For each method variation and vaccine group, the number of months of data needed to achieve 50% sensitivity based on the calibrated MaxSPRT in the Optum EHR database are shown, stratified by true effect size of the positive controls. HPV = Human papillomavirus, PS = Propensity Score, SCCS = Self-Controlled Case Series, SCRI = Self-Controlled Risk Interval, TaR = Time-at-Risk.
In the published article the same error was present in the Supplementary Material. This means the type 2 error and the time to 50% sensitivity were underestimated. The correct Supplementary Data Sheet S1 can be found in the Supplementary Materials.
The authors apologize for these errors and state that they does not change the scientific conclusions of the article in any way. The original article has been updated.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.1088973/full#supplementary-material
Keywords: vaccine safely, routinely collected data, adverse event, surveillance, methods
Citation: Schuemie MJ, Arshad F, Pratt N, Nyberg F, Alshammari TM, Hripcsak G, Ryan P, Prieto-Alhambra D, Lai LYH, Li X, Fortin S, Minty E and Suchard MA (2022) Corrigendum: Vaccine safety surveillance using routinely collected healthcare data—An empirical evaluation of epidemiological designs. Front. Pharmacol. 13:1088973. doi: 10.3389/fphar.2022.1088973
Received: 03 November 2022; Accepted: 04 November 2022;
Published: 24 November 2022.
Edited and reviewed by:
Carlos Alves, University of Coimbra, PortugalCopyright © 2022 Schuemie, Arshad, Pratt, Nyberg, Alshammari, Hripcsak, Ryan, Prieto-Alhambra, Lai, Li, Fortin, Minty and Suchard. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martijn J. Schuemie, c2NodWVtaWVAb2hkc2kub3Jn
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.