 Hailiang Shen
Hailiang Shen Ping Zhou2†
Ping Zhou2† Haixia Du
Haixia Du
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol., 09 January 2023
Sec. Ethnopharmacology
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.1060956
This article is part of the Research TopicPrevention and Treatment of Cardiovascular Disease with Integrated Traditional Chinese and Western MedicineView all 21 articles
Background: In view of the high morbidity and mortality of Diabetes mellitus—Coronary heart disease (DM-CHD) in diabetics, the combination therapy of traditional Chinese medicine injections (TCMIs) and conventional therapy (CT) is receiving extensive attention. Therefore, the effectiveness and security of conventional therapy with traditional Chinese medicine injections in the therapy of diabetes mellitus—coronary heart disease were compared by systematical review and network meta-analysis.
Methods: According to the preset inclusion criteria and exclusion criteria, we searched seven electronic literature databases from their inception to JAN 5,2022, to obtain the relevant RCT literature on the therapy of diabetes mellitus—coronary heart disease with traditional Chinese medicine injections. Two researchers independently reviewed the papers, two other researchers worked in extracting data and quality assessment of the included literature. The primary outcomes were total effective rate. The secondary outcomes included electrocardiogram (EGG)effective rate, the effective rate of angina pectoris, fasting blood glucose (FBG), 2-h postprandial blood glucose (PBG), hemoglobinA1c (HbA1c), total cholesterol (TC) and triglycerides (TG), high-density lipoprotein (HDL), low-density lipoprotein (LDL), frequency of angina pectoris, and duration of angina pectoris. We adopted stata16.0 software for the systematic review and network meta-analysis.
Results: A total of 53 trials involved 4,619 patients and one of the following 16 traditional Chinese medicine injections: Danhong, Danshen, Gualoupi, Gegen, Chuanxiongqin, Danshenchuanxiongqin, Shenmai, Shenqi, Xixin, Xuesaitong, Shuxuetong, Guanxinning, Kudiezi, Ciwujia, Xingding, Shuxuening. The meta-analysis revealed that Chuanxiongqin injection was superior to all other therapies in improving the total effective rate, [vs. conventional therapy odds ratio (OR): 14.52, 95% confidence interval (CI): 4.13–51.02], vs. Xuesaitong injection (odds ratio: 7.61, confidence interval: 1.25–46.40), and vs. Danshenchuanxiongqin injection (odds ratio: 3.98, confidence interval: 1.03–15.28)]. Xixin injection + conventional therapy was superior to conventional therapy only for electrocardiogram effective rate (odds ratio: 5.44, confidence interval: 1.55–19.18). Shenmai injection + conventional therapy was superior to conventional therapy in effective rate of angina (odds ratio: 11.05, confidence interval: 2.76–44.28). There was not different significantly in the comparisons of frequency of angina pectoris and duration of angina pectoris, we considered that this may be due to the lack of sufficient data. As most of the included RCTs did not monitor Adverse Events, the safety of those traditional Chinese medicine injections remains to be further explored.
Conclusion: Basing on our study, traditional Chinese medicine injections combined with conventional therapy takes important role in the treatment of diabetes mellitus—coronary heart disease, and its curative effect is better than conventional therapy. Nevertheless, properly designed RCTs are required to validate our conclusions in the future.
Systematic Review Registration: [https://inplasy.com/inplasy-2021-12-0125/], identifier [INPLASY2021120125].
Diabetes mellitus (DM) is a disease characterized by hyperglycemia caused by metabolic disorders. It is one of the most important non-communicable diseases threatening human health at present (Petersmann et al., 2019). According to the latest data from the International Diabetes Federation (IDF), there were 537 million diabetic patients worldwide in 2021. It is estimated that the number of people with diabetes will increase by 46%, reaching 780 million by 2045 (Saeedi et al., 2019). The latest epidemiology survey of diabetes in China shows that the prevalence of diabetes in people aged 18 and over is 12.4%, so it is estimated that about 150 million people with diabetes are diabetics (Wang et al., 2021a). Coronary atherosclerotic heart disease (CHD) is one of the common complications of DM, which is a kind of heart disease caused by coronary atherosclerotic plaque leading to vascular stenosis or even obstruction, myocardial ischemia, hypoxia and necrosis (Viigimaa et al., 2020). Data show that diabetic patients are 4 times more likely to suffer from cardiovascular diseases than non-diabetic patients (Lodha et al., 2018). In addition, compared with non-diabetic patients, diabetes mellitus coronary heart disease (DM-CHD) has early onset, complex condition, difficult treatment and poor prognosis (Yu and Shao, 2021).
At present, the conventional treatments of DM-CHD include angiotensin-converting enzyme inhibitors (ACEI), angiotensin receptor blockers (ARB), statins to improve blood supply, blood glucose control and reduce the risk of complications (Yang et al., 2019; Wang et al., 2021b). However, these strategies require long-term treatment and have many adverse reactions and side effects, such as hyperkalemia, arrhythmia, deterioration of renal function, etc. (Saedder et al., 2014; Yang et al., 2017). Therefore, it is urgent to explore other potential and effective interventions for the treatment of DM-CHD.
In the theory of traditional Chinese medicine (TCM), diabetes and coronary heart disease belong to the category of “chest pain” and “diabetes” (Wang et al., 2019). With thousands of years of history and practical experience, TCM has accumulated rich experience in the cognition and treatment of DM-CHD, and has created many effective therapeutic methods, and TCM has been widely used as complementary and alternative approach to the treatment and prevention of cardiovascular diseases (Hao et al., 2017). Traditional Chinese medicine injections (TCMIs), as one of the methods of TCM for the treatment of DM-CHD, has been widely used in clinical practice (Zhang et al., 2008; Wang et al., 2017; Zhou, 2017). The main TCMIs include Danhong injection, Danshen injection, Gegen injection, Shenmai injection, Gualoupi injection, Chuanxiongqin injection. This study systematically evaluated the above TCMIs.
At present, there is little literature review and systematic review on TCMIs in the treatment of DM-CHD, and point to point RCTs comparison is also lacking. Through both direct and indirect comparison, the network meta-analysis can be compared and sorted to evaluate the safety and efficacy of different TCMIs in patients with DM-CHD, so as to select the best treatment (De Laat, 2017). Therefore, we conducted pairwise comparison and meta-analysis of related randomized controlled trials (RCTs) to compare the safety and efficacy of different TCMIs in patients with DM-CHD, so as to provide better help for clinical application.
This study has been registered in the International Platform of Registered Systematic Review and Meta-Analysis Protocols (INPLASY), with the number INPLASY202120125. Our analysis was conducted based on the Preferred Reporting Item for Systematic and Meta-Analyses (PRISMA) guidelines for systematic review and meta-analysis (Hutton et al., 2015); see Supplementary material.
We searched PubMed, Web of Science, Embase, China National Knowledge Infrastructure (CNKI) Database, Chinese Biological Medicine Literature Service System Database (CBM), China Science Journal Database, China Science and Technology Journal Database (VIP), and Wan-fang database (WF) to get relevant articles that we need. The included articles were published from the establishment of each database to JAN 5, 2022. The theme search used was the combination of medical subject headings terms and free text terms. Searched terms included (“Diabetes” or “Diabetes mellitus”) and (“Coronary Diseases” or “Coronary Heart Disease”) and (“Injection”) within the restriction limit of (“randomized controlled trial”). We also manually searched journals that may publish research related to our subject.
The RCTs must meet the following requirements: 1) Participants: patients must meet the diagnostic criteria of coronary heart disease formulated by the Ministry of the health of the people’s Republic of China (Wang et al., 2018), and must meet the diagnostic criteria of diabetes published by WHO in 2019 (Kerner and Brückel, 2014). Ethnical, gender, age, and reasons for the disease are unlimited; 2) Interventions and comparisons: The control group was treated with traditional western medicine, including ACEIs or ARBs, antiplatelet drugs, hypoglycemic drugs, and statins. The treatment group was treated with one of the following 16 TCMIS based on routine western medicine treatment in the control group: Danhong injection, Danshen injection, Gualoupi injection, Gegen injection, Chuanxiongqin injection, Danshenchuanxiongqin injection, Shenmai injection, Shenqi injection, Xixin injection, Xuesaitong injection, Shuxuetong injection, Guanxinning injection, Kudiezi injection, Ciwujia injection, Xingding injection, Shuxuening injection (The details of TCMIs of all the included studies in the Supplementary Table S3); 3) Outcomes: the primary outcomes were total effective rate. The secondary outcomes included EGG effective rate, the effective rate of angina pectoris, fasting blood glucose (FBG), 2-h postprandial blood glucose (PBG), hemoglobinA1c (HbA1c), total cholesterol (TC), triglycerides (TG), high-density lipoprotein (HDL), low-density lipoprotein (LDL), frequency of angina pectoris, and duration of angina pectoris. Included trials needed to report at least one of these indicators; 4) Research design: randomized controlled trial.
Studies were excluded according to the following criteria: 1) Treatments in the control group contained other TCMIs, acupuncture, Chinese herbal medicine; 2) publications were duplicated; 3) control group was not set in the clinical study design; 4) the data was imperfect; 5) No relevant outcomes.
NoteExpress software was used for literature management, and the literature selection was independently completed by two researchers. Firstly, duplicate articles and systematic reviews of animal experiments were excluded. Articles were then preliminarily screened by reading the titles and abstracts according to the inclusion and exclusion criteria. The next step is to read the full text of the preliminarily screened articles and conduct further screening in strict accordance with the inclusion and exclusion criteria. If the results of the study are controversial at any stage, a third researcher would participate in the discussion. In addition, relevant data were extracted, including basic information (publication date, author’s name, title), detailed characteristics of included patients (sample size, gender, average age, course of treatment), intervention measures (drugs, dose), results (main results, secondary results) and RCT quality evaluation information. We also tried to contact the study authors by email, telephone or fax to obtain missing demographic information, such as the sample size, gender distribution, age, etc.
We evaluated the quality of all the included RCT literature independently by two investigators according to the Cochrane risk of bias tool (Higgins et al., 2011), mainly based on the following items: method of random assignment, concealment of allocation scheme, blinding, completeness of outcome data, selective reporting of study results, and other sources of bias. Each item was classified as low, unclear, or high risk of bias. When any disagreement arose between the two investigators, it was resolved by a third investigator.
Stata 16.0 software was used for meta-analysis of results statistics and data. For binary variables, results are shown as odds ratios (ORs) and corresponding 95% confidence intervals (95% CI). If the outcomes were continuous type variable, they would presented as mean differences (MDS) and 95% CI. In addition, if there are two or more studies for each outcome, a head-to-head pairwise meta-analysis was performed using a random-effects model. Using a frequency framework and random-effects model, different interventions were compared through network meta-analysis, and the results of the analysis were presented using the leaderboard. Surface plots under the cumulative ranking curve area (Sucra) were plotted to evaluate the ranking of each treatment measure in the systematic analysis according to the magnitude of the area under the cumulative ranking curve, which was equal to one when the treatment measure was best and equal to 0 when the treatment was worst.
In pairwise meta-analyses, clinical heterogeneity should be examined by calculating the I2statistic and taking the way of comparing data from potential effect modifiers. If I2was ≤50%, the heterogeneity was not obvious (Higgins et al., 2003). Inconsistency cannot be assessed because each network plot in our analysis was not circular. In the systematic analysis, we also assumed that the estimates of heterogeneity variance were consistent. As publication bias may occur due to the relatively large number of studies, we plotted funnel plots to determine whether there was publication bias. In addition, we also assessed the quality of included studies according to five aspects: study limitations, indirectness, inconsistency, imprecision, and publication bias.
According to the established search strategy, we initially retrieved 1,340 articles, including 156 articles from CNKI, 734 articles from Wanfang, 220 articles from CBM, 116 articles from VIP, 92 articles from Pubmed, 20 articles from WOS, and two articles from Embase. A total of 919 articles were included after deleting duplicate articles. After carefully reading of the title and abstract of each artice, we excluded 783 artices that were not related to our study. In addition, we have carefully read the full-text of the remaining articles by Picos principles. Finally, we identified 53 RCTs, all of which have been published. In addition, the patient’s conditions and treatments must meet our pre-defined necessary conditions, and the outcomes in the literature must have at least one indicator as the primary outcome. The specific flow chart of the study is shown in Figure 1.
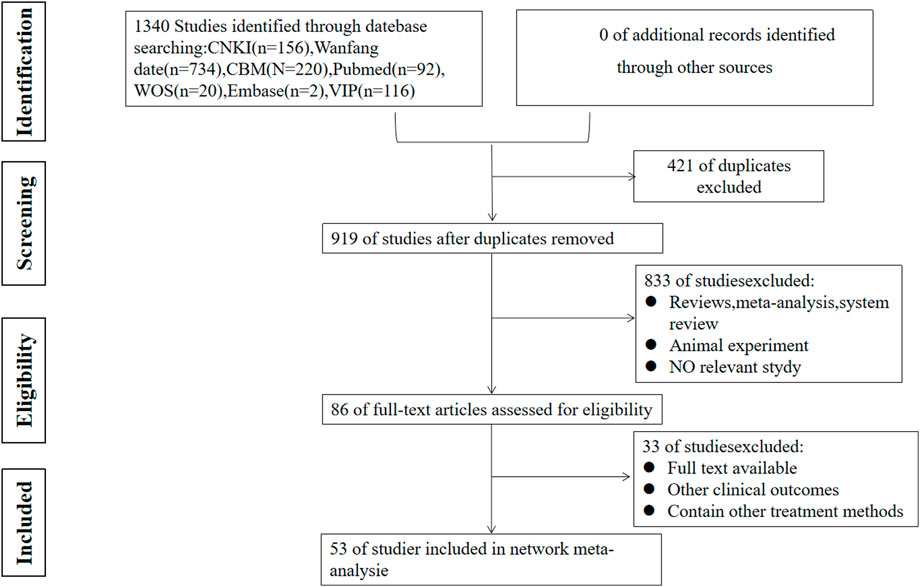
FIGURE 1. Flow chart of the study selection.
Among the 53 RCTs, a total of 4,619 patients were involved, and the patients participated in the trials were mostly middle-aged and elderly patients. All patients were treated with one of the 16 different TCMIs, as listed in the methods, in combination with conventional therapy. The main characteristics of all included studies are shown in Table 1.
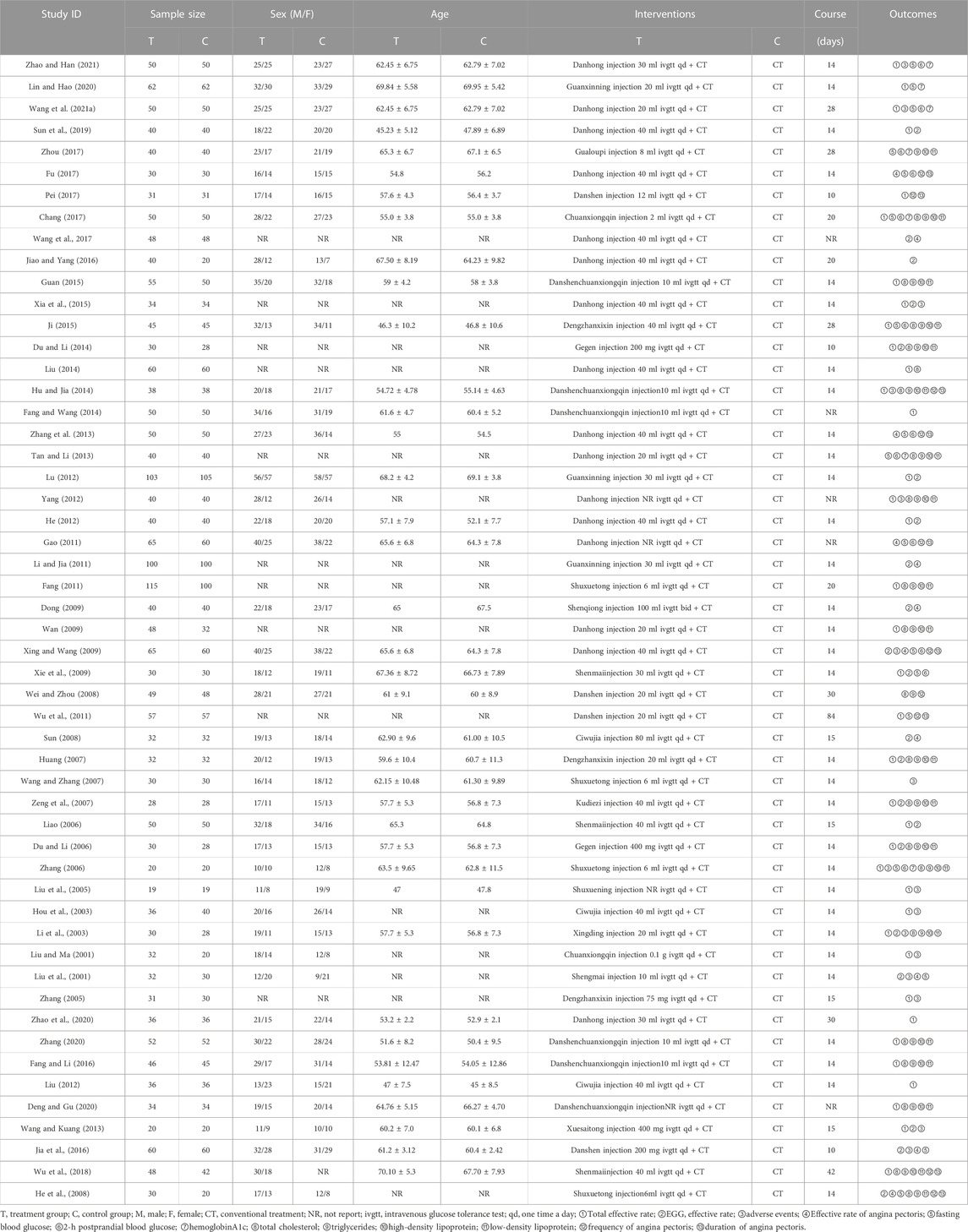
TABLE 1. Characteristic of the articles included in the network meta-analysis.
In terms of selective bias, the randomization of 11 articles was generated by a random number table, and therefore these articles were considered to be at low risk of bias. The two articles generated random sequences according to different clinical drugs, leading to higher risk of bias. The remaining RCTs used randomization only, without alternate the method of random assignment, and the risk of selection bias was considered unclear. In terms of performance bias, one study was double-blinded and five studies were all single-blinded, which were considered to be at low risk. However, three studies did not use blinding and were therefore rated as high risk. Other studies did not provide information on blinding, so performance bias was assessed as an unclear risk. Because there was incomplete information to assess the level of risk of detection bias, the risk levels were ambiguous. All articles are complete data and low risk. As the full trial protocol is not available, the risk of reporting bias was unclear. There were no other apparent biases in all studies and the risk was low. The summary of Risk of bias is shown in Figure 2, with green indicating low risk of bias, yellow indicating moderate risk of bias, and red indicating high risk of bias.
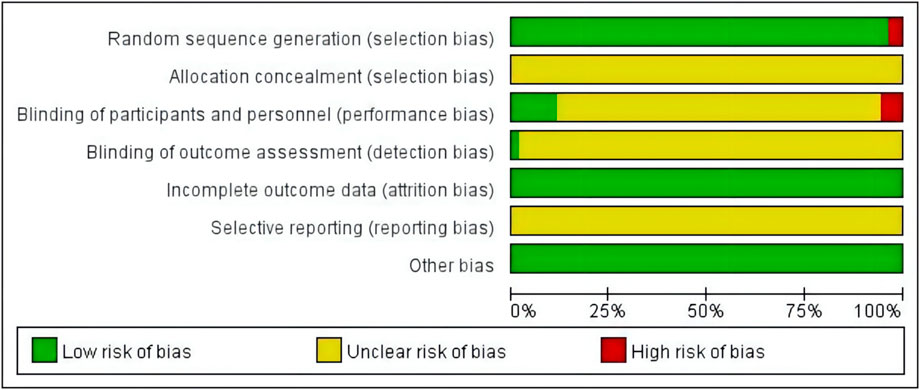
FIGURE 2. Summary of the risk of bias selection.
In total, 37 RCTs were included involving studies of 14 treatments: DH + CT vs. CT (n = 9), DSCXQ + CT vs. CT (n = 6), XX + CT vs. CT (n = 3),SM + CT vs. CT (n = 3), GXN + CT vs. CT (n = 2), DS + CT vs. CT (n = 2), CXQ + CT vs. CT (n = 2), GG + CT vs. CT (n = 2), SXT + CT vs. CT (n = 2), CWJ + CT vs. CT (n = 2), KDZ + CT vs. CT (n = 1), XST + CT vs. CT (n = 1), SXN + CT vs. CT (n = 1), XD + CT vs. CT (n = 1). We plot a network plot of the results as shown in Figure 3A, with each row representing a head-to-head comparison type. The width of the line is proportional to the number of trials comparing the connected treatments. All types of TCMI + CT were superior to CT alone, and the difference was statistically significant in outcomes. The detailed comparative information is shown in Figure 4A: CT combined with the following TCMIs performed better than CT alone: Gegen injection (OR:7.00, CI: 2.22–22.06), Xingding injection (OR:7.00, CI: 1.38–35.48), Ciwujia injection (OR:5.67, CI: 1.54–20.89), Danshen injection (OR:4.95, CI: 1.58–15.47), Xixin injection (OR:4.70, CI: 2.33–9.50), Shenmai injection (OR:4.53,CI: 2.43–8.44), Guanxining injection (OR:4.42, CI: 2.10–9.29), Danhong injection (OR:4.17, CI: 2.87–6.06), Shuxuetong injection (OR:3.73, CI: 1.71–8.13), Danshenchuanxiongqin injection (OR:3.65, CI: 2.25–5.92). Among them, Chuanxiongqin injection was superior to all other treatment methods [vs. CT (OR: 14.52, CI: 4.13–51.02), vs. Xuesaitong injection (OR: 7.61, CI: 1.25–46.40), and vs. Danshenchuanxiongqin injection (OR: 3.98, CI: 1.03–15.28)].
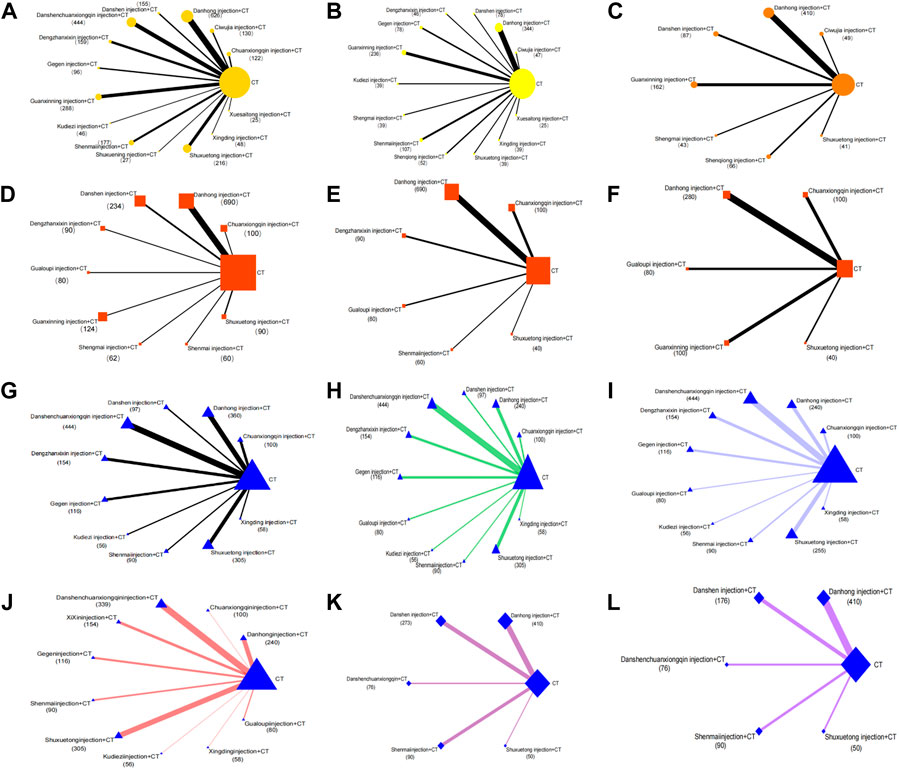
FIGURE 3. Network graphs of comparisons on different outcomes of treatments in different groups of patients with DM-CHD. (A) Total effective rate; (B) EGG effective rate; (C) Effective rate of angina pectoris; (D) FBG; (E) PBG; (F) HbA1c; (G) TC; (H) TG; (I) HDL; (J) LDL; (K) Frequency of angina pectoris; (L) Duration of angina pectoris.
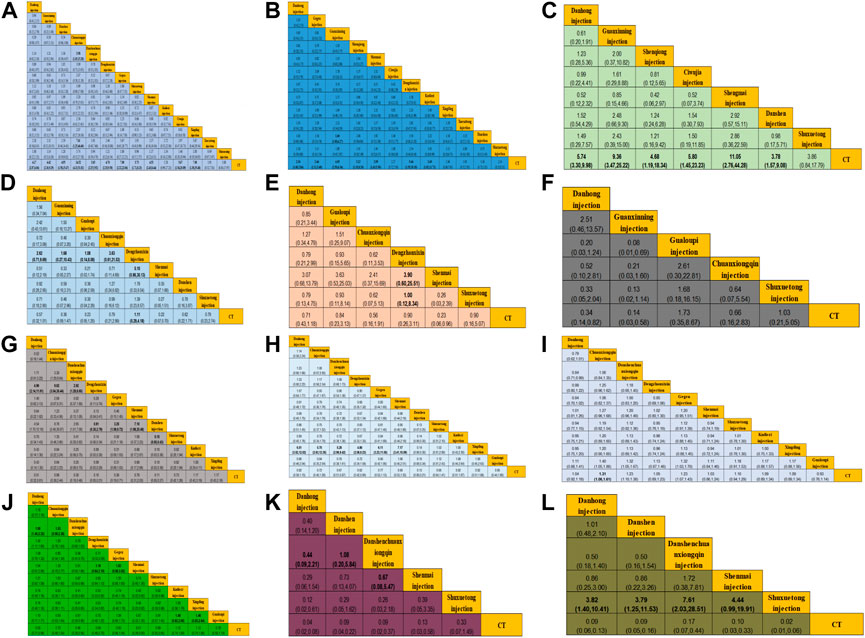
FIGURE 4. Final results of the systematic meta−analysis. (A) Total effective rate; (B) EGG effective rate; (C) Effective rate of angina pectoris; (D) FBG; (E) PBG; (F) HbA1c; (G) TC; (H) TG; (I) HDL; (J) LDL; (K) Frequency of angina pectoris; (L) Duration of angina pectoris.
For the EGG effective rate, there were a total of 21 RCTs involving 12 treatment regimens: DH + CT vs. CT (n = 6), SM + CT vs. CT (n = 3), GG + CT vs. CT (n = 2), GXN + CT vs. CT (n = 2), XX + CT vs. CT (n = 1), CWJ + CT vs. CT (n = 1), KDZ + CT vs. CT (n = 1), XD + CT vs. CT (n = 1), SXT + CT vs. CT (n = 1), XST + CT vs. CT (n = 1), DS + CT vs. CT (n = 1), SQ + CT vs. CT (n = 1). Its reticular diagram is shown in Figure 3B. In terms of ECG response rate, Xixin injection was superior to CT alone (OR:5.44, CI: 1.55–19.18), Danhong injection (OR:2.54, CI: 1.68–3.84), Gegen injection (OR:2.46, CI: 1.11–5.48), Guanxining injection (OR:4.05, CI: 2.58–6.34), Shenmai injection (OR:2.99, CI: 1.63–2.50), Kudieziinjection (OR:3.45, CI: 1.02–11.72).
There were a total of 11 RCTs on the effective rate of angina, involving seven treatment methods: DH + CT vs. CT (n = 5), GXN + CT vs. CT (n = 1), SQ + CT vs. CT (n = 1), CWJ + CT vs. CT (n = 1), SM + CT vs. CT (n = 1), DS + CT vs. CT (n = 1), SXT + CT vs. CT (n = 1). Its reticular diagram is shown in Figure 3C. Significant differences among the six treatments compared with CT alone are shown in Figure 4C: Shenmai injection + CTvs. CT (OR:11.05, CI: 2.76–44.28), Guanxining injection (OR: 9.36, CI: 3.47–25.22), Ciwujia injection (OR: 5.80, CI: 1.45–23.23), Danhong injection (OR:5.74, CI: 3.30–9.98), Shenqi injection (OR:4.68, CI:1.18–18.84), Danshen injection (OR:3.78, CI: 1.57–9.08).
For the fasting blood glucose, its net diagram is shown in Figure 3D, involving a total of 17 RCTs and eight treatments, and all treatment comparisons compared were significant. Shenmai injection + CT had the best effect among all treatments, [vs. Danhong injection (MD: 2.62, CI: .71–9.96), vs. Guanxining injection (MD: 1.68, CI: .27–10.43), vs. Gualoupi injection (MD: 1.08, CI: .14–8.08), vs. Chuanxiongqin injection (MD: 3.63, CI: .61–21.53), and vs. XiXin injection (MD: 5.10, CI: .86–30.13)]. Compared with CT alone, the effect of Xixin injection was most significant.
There were 12 RCTs with six treatments, involving 2-h postprandial blood glucose, the reticular diagram of which is shown in Figure 3E. As shown in Figure 4E, all treatments were significant compared with CT alone. Xixin injection was superior to all other treatments, [vs. CT (MD:0.90, CI:0.26-3.31), vs. Danhong injection (MD:3.07, CI:0.68-13.79), vs. Gualoupi injection (MD: 3.63, CI: .53-25.03), vs. Chuanxiongqin injection (MD: 2.41, CI: .37-15.69), vs. Shenmai injection (MD: 3.90, CI:0.60–25.51) and vs. Shuxuetong injection (MD: 1.00, CI:0.12–8.34)].
For glycated hemoglobin, a total of 7 RCTs were involved with five treatments, and their reticular diagram is shown in Figure 3F. CT combined with the following TCMIs: Danhong injection (MD:0.34, CI:0.14-.82), Guanxining injection (MD: .14, CI: .03-.58), Gualoupi injection (MD: 1.73, CI: .35–8.67), Chuanxiongqin injection (MD: .66, CI: .16–2.83), Shuxuetong injection (MD: 1.03, CI:0.21–5.05) were better than CT alone. Gualoupi injection had the best efficacy among all therapies.
A total of 21 articles and 10 treatment measures involved total cholesterol, reticular diagram of which is shown in Figure 3G. All treatment comparisons were significantly different. Xixin injection, vs. Danhong injection (MD:4.99, CI:2.14-11.61), vs. Chuanxiongqin injection (MD: 9.62, CI: 3.04-30.44), and vs. Danshenchuanxiongqin injection (MD: 2.92, CI: 1.28-6.65); Danshen injection, vs.. Xixin injection (MD: .91, CI: .30-2.79), vs. Gegen injection (MD: 3.25, CI: 1.09–9.72), and vs. Shenmai injection (MD: 7.10, CI: 1.98–25.48). All 10 interventions were significantly better than CT alone, among which Kudiezi injection had the best effect compared with CT alone, and the detailed comparison information is presented in Figure 4G.
There were a total of 21 RCTs, of which 11 treatments involved triglycerides, and their reticular diagrams are shown in Figure 3H. All TCMIs were superior to CT alone. Among them, the best effect is Xinding Injection [vs. Danhong injection (MD: 6.51, CI: 3.52–12.02), vs. Chuanxiongqin injection (MD: 5.70, CI: 2.63–12.35), vs. Danshenchuanxiongqin injection (MD: 5.28, CI: 2.96–9.42), vs. Xixin injection (MD: 4.88, CI: 2.58–9.23), vs. Gegen injection (MD: 6.11, CI:3.23–11.55) and vs. Shenmai injection (MD: 7.17, CI: 3.41–15.09)].
For HDL, a total of 19 RCTs and 10 treatments were involved, and their reticular diagrams are shown in Figure 3I. Chuanxiongqin injection was superior to CT alone (MD:1.31, CI: 1.06-1.61). Gualoupi injection was superior to other TCMIs, Gualoupi injection [vs. Chuanxiongqin injection (MD: 1.40, CI:1.05-1.88), vs. Danshenchuanxiongqin injection (MD: 1.32, CI:1.05-1.67), and vs. Gegen injection (MD: 1.32, CI:1.03–1.70)]. Additional detailed comparative information is presented in Figure 4I.
A total of 20 RCTs involving studies of 10 treatment methods, and the mesh diagram are shown in Figure 3J. There were significant differences among the treatments, Danshenchuanxiongqin vs. Danhong injection (MD: 1.80, CI: 1.40-2.32), vs. Chuanxiongqin injection (MD:1.53, CI: .99-2.36); Shenmai injection vs. Xixin injection (MD: 1.16, CI: .64-2.10), vs. Gegen injection (MD: 1.63, CI: .88-3.02). The comparison information is shown in Figure 4J.
A total of 10 articles and five treatment measures related to the frequency of angina pectoris, and the network diagram is shown in Figure 3K. In the comparison of all therapies, Shenmai injection was significantly better than other therapies. Shenmai injection, vs. Danhong injection (MD: .44, CI: .09–2.21), vs. Danshen injection (MD: 1.08, CI: .20–5.84), vs. Danshenchuanxiongqin (MD: .67, CI:0.08–5.47). However, compared with CT alone, all TCMIs interventions had no obvious advantage in reducing the frequency of angina pectoris.
For the duration of angina pectoris, a total of 9 RCTs and five treatment methods were involved, and the network diagram is shown in Figure 3L. Among the five treatment methods, the most effective ones were Shuxuetong injection [vs. Danhong injection (MD: 3.82, CI: 1.40–10.41), vs. Danshen injection (MD: 3.79, CI: 1.25-11.53), vs. Danshenchuanxiongqin injection (MD: 7.61, CI: 2.03–28.51), and vs. Shenmai injection (MD: 4.44, CI: .99–19.91)]. However, compared with CT alone, all TCMIs were less effective in shortening the duration of angina pectoris than CT alone.
Figure 5 shows the overview of Bayesian ranking of the comparison treatments, with the vertical axis representing the cumulative probability and the horizontal axis representing the sequence of processing. The detailed sorting results are summarized in Table 2. Chuanxiongqin injection is most likely to rank first in overall effective rate (cumulative probability 34.6%), Xixin injection for ECG effective rate (44.0%), Shengmai injection for an effective rate of angina pectoris (44.3%), Xixin injection for FBG effective rate (38.6%), Shuxuetong injection for PBG effective rate (30.8%), Gualoupi injection for HbA1c effective rate (56.1%), Kudiezi injection for TC effective rate (33.0%), Xingding injection for TG effective rate (19.7%), Chuanxiongqin injection for HDL effective rate (54.1%), Kudiezi injection for LDL effective rate (45.0%). Detailed SUCRA value is shown in Table 2.
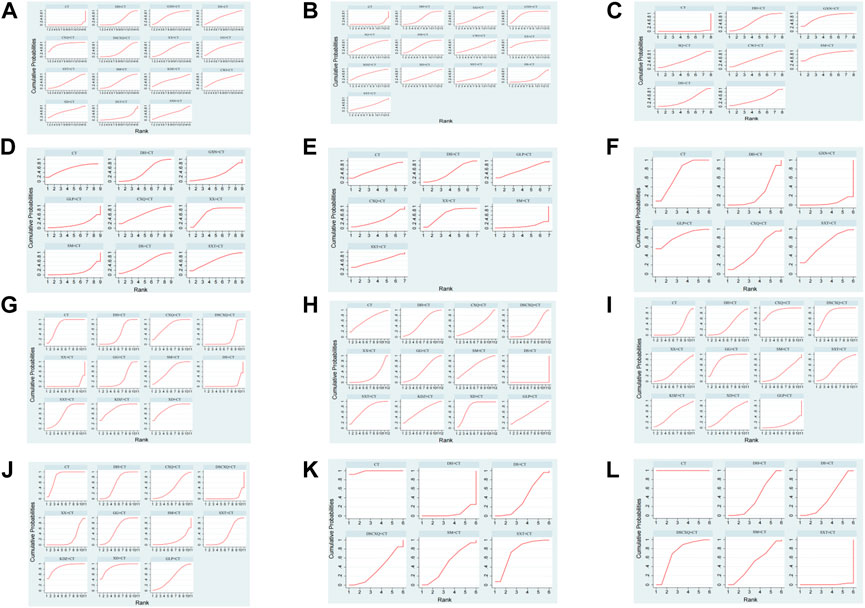
FIGURE 5. Ranking probabilities of comparable treatments. (A) Total effective rate; (B) EGG effective rate; (C) Effective rate of angina pectoris; (D) FBG; (E) PBG; (F) HbA1c; (G) TC; (H) TG; (I) HDL; (J) LDL; (K) Frequency of angina pectoris; (L) Duration of angina pectoris.
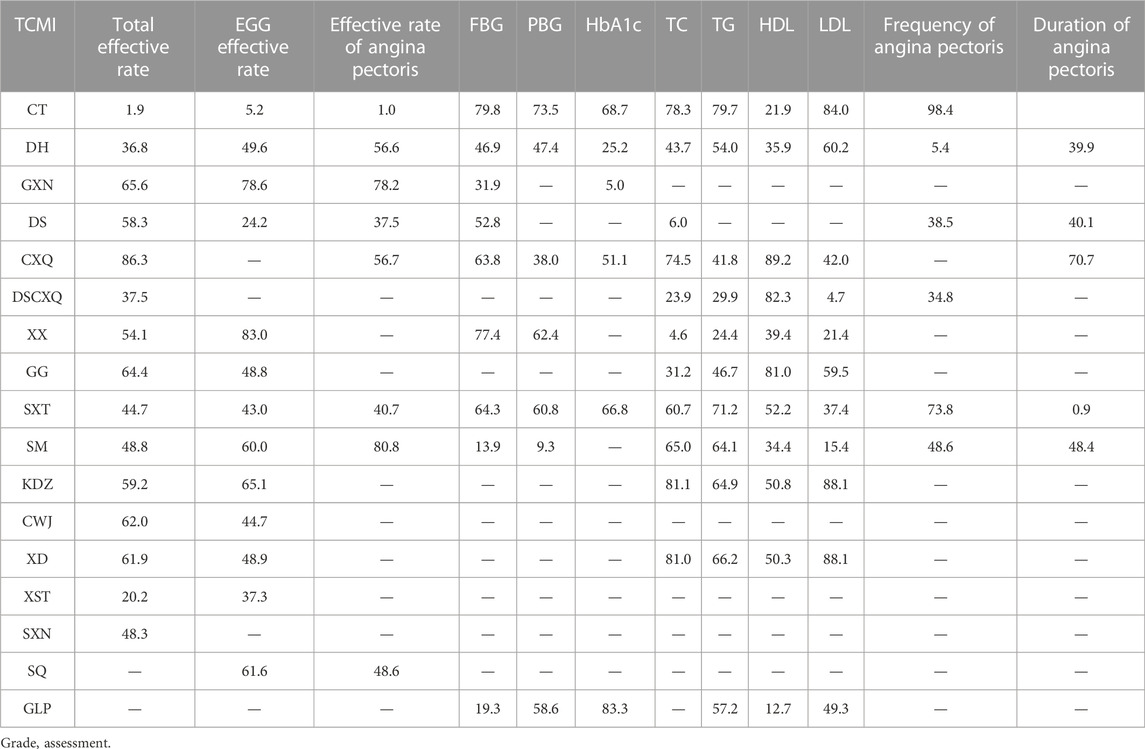
TABLE 2. SUCRA of different treatments for various outcomes.
We performed a GRADE assessment of the total effective rate using five downgrading factors: study limitations, inconsistency, indirectness, imprecision, and publication bias. The quality of evidence were graded as high, moderate,low, and very low, in which the rating of evidence quality for randomized controlled trials (RCTs) was preset as high, graded 1 as intermediate, 2 as low, and 3 as very low (Guyatt et al., 2011). Where XST + CT was downgraded by three for having a high risk of bias to be very low grade outside of this, the rest of the evidence grades were above low grade. Detailed GRADE grading is presented in Table 3.
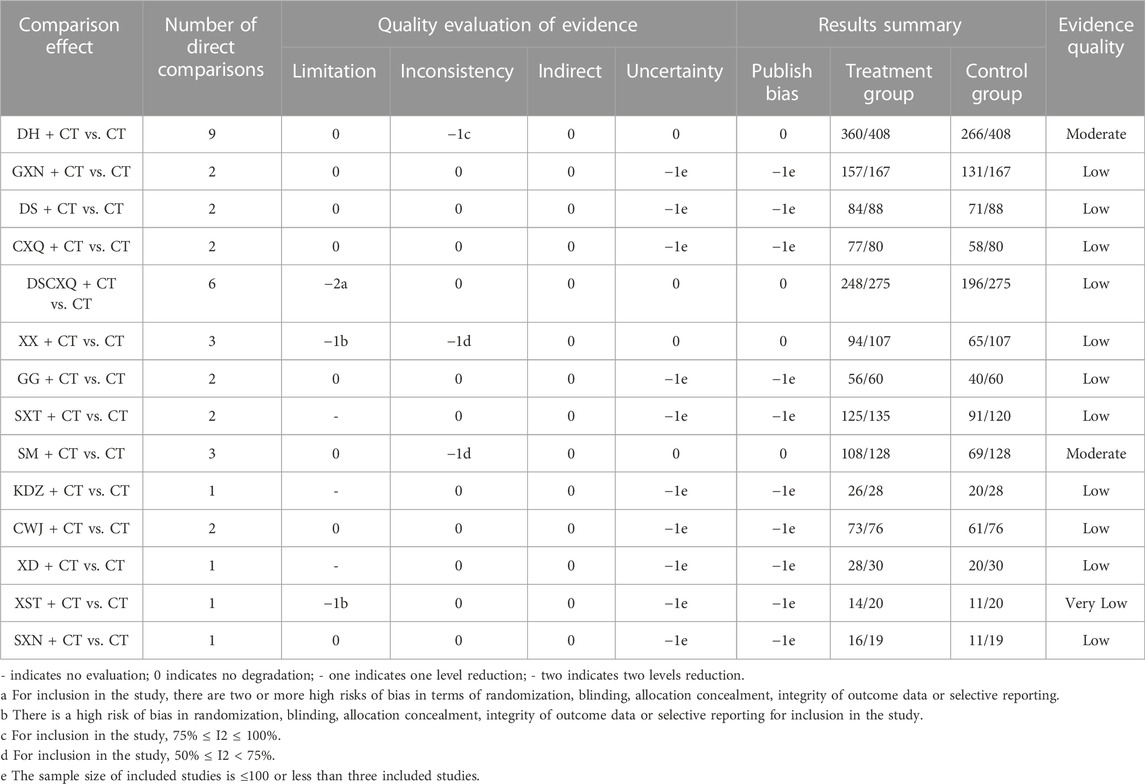
TABLE 3. GRADE assessment for the total effective rate.
We plotted a funnel plot of the overall response rate to test for publication bias. As shown in Figure 6, we found that the various interventions were symmetrical along the centerline, and the angle between the centerline and the adjusted auxiliary lines was not large, suggesting less publication bias. The results of our concurrent sensitivity analysis are shown in Figure 7; while meeting the conditions of I2 < 50%, p > .1, and the point estimates of all outcomes are within 95% CIs of the pooled effect sizes. The results indicated that there were no findings to exclude, so we did not consider each study to have any bias in the results.
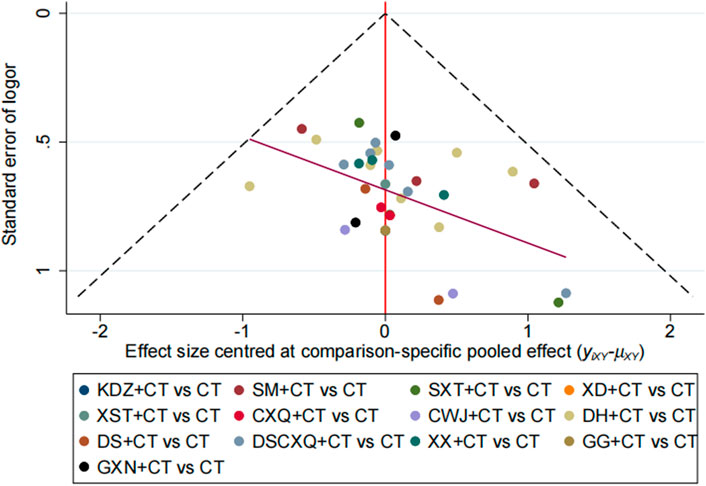
FIGURE 6. Funnel plot for total effective rate.
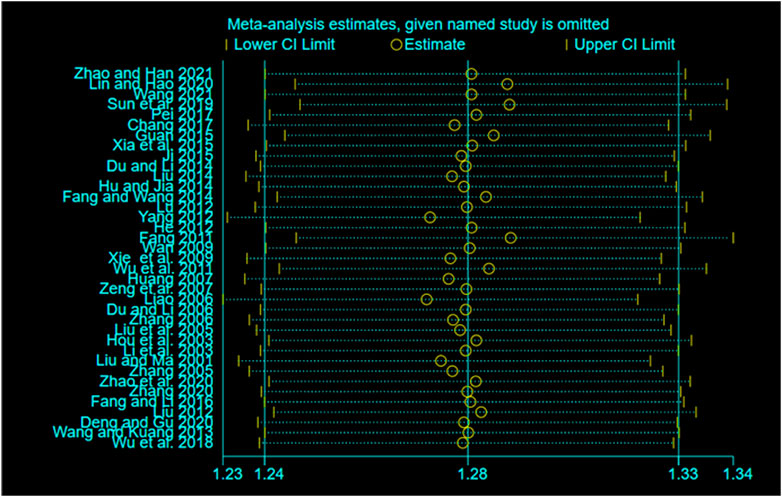
FIGURE 7. Sensitivity analysis results.
14 records considered adverse reactions, 9 records did not clearly describe adverse reactions during medication, and 5 records recorded specific adverse reactions, such as headache, nausea, somnolence, and other outcomes as shown in Table 4. The incidences of adverse reactions were 7.47%, 7.89%, and 10.85% for Danhong injection, Danshenchuanxiong injection and CT alone, respectively.

TABLE 4. Adverse reactions of TCMIs.
Abnormal glycolipid metabolism in diabetes can cause progressive damage to cardiomyocytes and activate cardiac fibroblasts, leading to myocardial interstitial fibrosis and progressive decline in cardiac function. Ang IV and its receptor AT4R overactivation in the renin-angiotensin system (RAAS) and cardiomyocyte autophagy abnormalities may be important mechanisms by which diabetes leads to myocardial injury and ventricular remodeling (Zhang et al., 2021). Meanwhile diabetes can cause pathological cardiac remodeling and heart failure by elevating the protein expression and activity of ADAM17, affecting ADRA1A regulation and AMPK signaling, and increasing myocardial fibrosis and cardiomyocyte apoptosis (Xue et al., 2022). Diabetes can aggravate coronary atherosclerosis through abnormal glycolipid metabolism, cardiomyocyte death, oxidative stress, and other pathways (Ritchie and Abel 2020), triggering coronary heart disease, which has become one of the important complications of diabetes. DM-CHD often leads to polyvascular, calcified, diffuse lesions in patients (Naito and Miyauchi, 2017), aggravates mortality of patients, and greatly affects patients’ mental health and quality of life. Despite significant progress in basic research, drugs, and interventions, the level of clinical efficacy and prognosis of DM-CHD remain unsatisfactory (Hinnen and Kruger, 2019). TCM has a long history in the treatment of the DM-CHD. In recent decades, many TCMIs with remarkable efficacy have been discovered in clinical practice, and TCMIs are playing an increasingly important role in the treatment of DM-CHD.
Danshen injection is extracted from Danshen (Salvia miltiorrhiza Bunge, Lamiaceae, Salviae miltiorrhizae radix et rhizoma), Danhong injection is extracted from Danshen and Honghua. And the main active components are danshensu, protocatechuic aldehyde, safflflower yellow A, and salvianolic acid (Jiang et al., 2015; Liu et al., 2019). Danshen injection and Danhong injection could activate blood circulation and remove stasis, widely used in the treatment of DM-CHD with blood stasis syndrome. Chuanxiongqin, Danshenchuanxiongqin, Guanxinning, Shuxuetong and Xixin injection have the same efficacy and are also used for treatment DM-CHD with the syndrome of chest pain and stuffiness, palpitations, dark purple tongue, etc (Li et al., 2022). Gegen, Shuxuening and Xingding injection play an important role in dilating coronary artery and improving myocardial ischemia (Fan et al., 2022). And there are used for treatment ischemic coronary heart disease and angina pectoris. Gualoupi and Kudiezi injection have the effect of Regulating Qi to dissipate blood stasis and phlegm, widely used in the treatment of DM-CHD with blood stasis and sputum dampness syndrome. Shenmai, Shenqi and Ciwujia injection are used for treatment DM-CHD with deficiency of vital qi.
The systematical analysis approach was taken to compare the efficacy and safety of different TCMI treatments in patients with DM-CHD. A total of 53 RCTs and 4,619 patients were included in this study, and we evaluated 16 treatment methods from 12 indicators involving total effective rate, EGG effective rate, the effective rate of angina pectoris, FBG, PBG, HbA1c, TC, TG, HDL, LDL, frequency of angina pectoris, duration of angina pectoris. The results indicated that all kinds of TCMIs + CT were more effective in the treatment of DM-CHD than CT alone.
In terms of primary outcomes included the total effective rate, EGG effective rate and effective rate of angina pectoris. The results suggested that all types of TCMIs + CT were superior to CT alone, and results were significantly different. In terms of total effective rate, Chuanxiongqin injection SUCRA had the largest area and ranked first, indicating Chuanxiongqin injection had the best effect among all therapies and was the best treatment for DM-CHD. However, Xixin injection and Shenmai injection play important roles in improving ECG and alleviating angina pectoris in DM-CHD patients respectively. Studies have found (Wang et al., 2020; Ye et al., 2021) that Xixin injection can significantly improve cardiac function by expanding coronary artery, increasing coronary flow, reducing cardiac load and myocardial gas consumption, improving ST segment and changing T wave from low to upright in patients’ ECG. Qi et al. (Qi et al., 2015) suggested that Shenmai injection can reduce the activities of serum creatine kinase (CK) and lactate dehydrogenase (LDH), resist ischemia-reperfusion injury, and protect myocardium from myocardial injury, and alleviate the symptoms of angina pectoris, which was also confirmed in our study.
The secondary outcomes included FBG, PBG, HbA1c, TC, TG, HDL, LDL, frequency of angina pectoris, and duration of angina pectoris. TCMIs were significantly better than CT alone in FBG, PBG, HbA1c, TC, TG, HDL and LDL, and SCURA ranking was higher than CT. Among them, Xixin injection ranked first in FBG and PBG, indicating that its curative effect in improving FBG and PBG indexes was significantly higher than that of other therapies. Kudiezi injection ranked first in TC and LDL as the best choice. Gualoupi injection, Xingding injection, and Chuanxiongqin injection play important roles in HbA1c, TG, and LDL, respectively, and had significant advantages compared with other therapies. Experiments showed that Danhong injection can reduce the blood lipid level, inhibit the expression of MMP9, prevent poor myocardial remodeling, reduce myocardial fibrosis and improve myocardial function (Chen et al., 2016). Danshen injection can improve the normalization of hemodynamic parameters, ventricular mass and cardiac functions (Zhang et al., 2013). Zhang (Zhang, 2016) believed that Shuxuetong injection can reduce erythrocyte aggregation, improve platelet activation function and alleviate myocardial injury. By reducing myocardial injury and protecting cardiac function, it can slow down the occurrence of angina pectoris. However, in our study, Danhong injection, Danshen injection and Shuxuetong injection had no significant advantages compared with CT alone in reducing the frequency and duration of angina pectoris, we speculated that this was caused by small sample size at that time.
The safety is crucial to TCMIs, and we also considered the safety in the test. A total 14 RCT in our study considered safety issues, 9 articles did not clearly describe adverse reactions during medication, 5 records described specific adverse reactions, and most did not report any ADRs. The specific adverse reactions were nausea, cardiopalmus, and drowsiness. Aizziness and hypoglycemia were reported occasionally. Although these ADRs could be effectively relieved by symptomatic treatments, clinicians should keep this in mind when prescribing TCMI treatments. In our comparisons, Danshenchuanxiongqin injection had the worst safety profile.
In conclusion, the efficacy of TCMIs + CT was better than that of CT alone in the treatment of DM-CHD. In combination therapy, Chuanxiongqin injection is the first choice to improve the effective rate, XiXin injection had the best curative effect when measuring by FBG and PBG, and Kudiezi injection can improve TC and LDL.
Our study had several limitations. First, no direct comparison between TCMIs were found between most treatments, and the most direct evidence was derived from one trial in the present network. Second, despite our best efforts, the quality of the included RCTs was low. Although the patients in the trials were randomized, only some of the 53 RCTs described specific randomization methods, such as random number table. And configuration concealment of some articles was unknown. Third, some trials were low sample size tests with positive findings and are particularly prone to various biases.
Due to the unsatisfactory quality of the included studies, based on our findings, we put forward the following two suggestions for further studies of TCMI-CT in the treatment of DM-CHD: 1) Prospective registration of large clinical trials in recognized clinical trial registration platform; 2) The trial protocol should be rigorously designed in terms of randomization, allocation, concealment, and blinding; 3) Design high-quality, large sample randomized controlled trial.
In our study, we revealed that TCMIs had positive effects on patients with DM-CHD, but there was no significant difference in the frequency of angina pectoris, duration of angina pectoris. In addition, XiXin injection had the best curative effect when measured by FBG and PBG, and Kudiezi injection can improve TC and LDL. At the same time, we also discovered that Danshenchuanxiongqin injection has side effects, which should be paid more attention in clinical applications.
Nevertheless, on account of some limitations, more clinical studies with well-designed, reasonable samples and good method quality are needed to test and verify our results in the future.
The original contributions presented in the study are included in the article/Supplementary Materials, further inquiries can be directed to the corresponding authors.
XQ and HD contributed conception and designed the study; HS, P Zhou and XQ extracted and analyzed the data; LS and CJ performed this systematical analysis. HS and P Zhou wrote this manuscript. All authors approved the submitted version.
This work was supported by the Construction Fund of Key Medical Disciplines of Hangzhou (grant. OO20200055), the Medical and Health Technology Project of Hangzhou (grant. A20220989) and the Research Project of Zhejiang Chinese Medical University (grant. 2021RCZXZK22).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.1060956/full#supplementary-material
Chen, J., Cao, W., Asare, P. F., Lv, M., Zhu, Y., Li, L., et al. (2016). Amelioration of cardiac dysfunction and ventricular remodeling after myocardial infarction by danhong injection are critically contributed by anti-TGF-β-mediated fibrosis and angiogenesis mechanisms. J. Ethnopharmacol. 194, 559–570. doi:10.1016/j.jep.2016.10.025
Fan, G., H., Liu, M., L., Liu, Jia., Chen, X., X., and Huang, Y., H. (2022). Systematic review of the efficacy and safety of shuxuening injection in the treatment of unstable angina. Evid. Based Complement. Altern. Med. 2022, 6650763. doi:10.1155/2022/6650763
Guyatt, G., Oxman, A. D., Akl, E. A., Kunz, R., Vist, G., Brozek, J., et al. (2011). GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 64 (4), 383–394. doi:10.1016/j.jclinepi.2010.04.026
Hao, P. P., Jiang, F., Cheng, J., Ma, L. Y., Zhang, Y., and Zhao, Y. X. (2017). Traditional Chinese medicine for cardiovascular disease: Evidence and potential mechanisms. J. Am. Coll. Cardiol. 69 (24), 2952–2966. doi:10.1016/j.jacc.2017.04.041
Higgins, J. P., Altman, D. G., Gotzsche, P. C., Moher, D., Oxman, A. D., Savovic, J., et al. (2011). The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 343, d5928. doi:10.1136/bmj.d5928
Higgins, J. P., Thompson, S. G., Deeks, J. J., and Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ 327 (7414), 557–560. doi:10.1136/bmj.327.7414.557
Hinnen, D., and Kruger, D. F. (2019). Cardiovascular risks in type 2 diabetes and the interpretation of cardiovascular outcome trials. Diabetes Metab. Syndr. Obes. 12, 447–455. doi:10.2147/DMSO.S188705
Hutton, B., Salanti, G., Caldwell, D. M., Chaimani, A., Schmid, C. H., Cameron, C., et al. (2015). The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern Med. 162 (11), 777–784. doi:10.7326/M14-2385
Jiang, X., Lv, B., Li, P., Ma, X., Wang, T., Zhou, Q., et al. (2015). Bioactivity-integrated UPLC/Q-TOF-MS of Danhong injection to identify NF-κB inhibitors and anti-inflammatory targets based on endothelial cell culture and network pharmacology. J. Ethnopharmacol. 174, 270–276. doi:10.1016/j.jep.2015.08.026
Kerner, W., and Brückel, J. (2014). Definition, classification and diagnosis of diabetes mellitus. Exp. Clin. Endocrinol. Diabetes 122 (7), 384–386. doi:10.1055/s-0034-1366278
Li, M., X., Li, H., D., Liu, H., X., Lai, X., L., and Xing, W., L. (2022). Efficacy and safety of eight types salvia miltiorrhiza injections in the treatment of unstable angina pectoris: A network meta-analysis. Front. Pharmacol. 2022, 972738. doi:10.3389/fphar.2022.972738
Liu, S., Wang, K., Duan, X., Wu, J., Zhang, D., Liu, X., et al. (2019). Efficacy of danshen class injection in the treatment of acute cerebral infarction: A bayesian network meta-analysis of randomized controlled trials. Evid. Based. Complement. Altern. Med. 2019, 5814749. doi:10.1155/2019/5814749
Lodha, S., Sharma, K. K., Bana, A., Mehta, N., and Gupta, R. (2018). Incidence of new diabetes following CABG surgery: Analysis of a single centre registry data. Indian Heart J. 70 (3), S221–s223. doi:10.1016/j.ihj.2018.11.017
Naito, R., and Miyauchi., K. (2017). Coronary artery disease and type 2 diabetes mellitus. Int. Heart J. 58 (4), 475–480. doi:10.1536/ihj.17-191
Petersmann, A., Müller-Wieland, D., Müller, U. A., Landgraf, R., Nauck, M., Freckmann, G., et al. (2019). Definition, classification and diagnosis of diabetes mellitus. Exp. Clin. Endocrinol. Diabetes 127 (01), S1–S7. doi:10.1055/a-1018-9078
Qi, Y. W., Wu, Z. R., Ma, Z. G., Feng, Z. Y., Liu, Y. X., and Liu, B. L. (2015). Mechanism of action of Shenmai injection as an adjunct to thrombolysis in acute ST segment elevation myocardial infarction. Chin. J. Exp. formulas 21 (10), 195–198. doi:10.13422/j.cnki.syfjx.2015100195
Ritchie, R. H., and Abel, E. D. (2020). Basic mechanisms of diabetic heart disease. Circ. Res. 126 (11), 1501–1525. doi:10.1161/CIRCRESAHA.120.315913
Saedder, E. A., Brock, B., Nielsen, L. P., Bonnerup, D. K., and Lisby, M. (2014). Identifying high-risk medication: A systematic literature review. Eur. J. Clin. Pharmacol. 70 (6), 637–645. doi:10.1007/s00228-014-1668-z
Saeedi, P., Petersohn, I., Salpea, P., Malanda, B., Karuranga, S., Unwin, N., et al. (2019). Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the international diabetes federation diabetes atlas, 9th edition. Diabetes Res. Clin. Pract. 9157, 107843. doi:10.1016/j.diabres.2019.107843
Viigimaa, M., Sachinidis, A., Toumpourleka, M., Koutsampasopoulos, K., Alliksoo, S., and Titma, T. (2020). Macrovascular complications of type 2 diabetes mellitus. Curr. Vasc. Pharmacol. 18 (2), 110–116. doi:10.2174/1570161117666190405165151
Wang, B., Li, Y., and Han, Y. L. (2018). Guidelines for the diagnosis and treatment of stable coronary heart disease. Chin. J. Cardiovasc. Dis. 46 (09), 680–694. doi:10.3760/cma.j.issn.0253-3758.2018.09.004
Wang, J., Xing, Y., Yao, K., Jun, L. I., Chen, G., Dong, Y., et al. (2019). Connotation and extension of the theory of phlegm-blood stasis-stagnation-deficiency in coronary heart disease. J. Traditional Chin. Med. 60 (04), 280–284. doi:10.13288/j.11-2166/r.2019.04.003
Wang, L., Peng, W., Zhao, Z., Zhang, M., Shi, Z., Song, Z., et al. (2021a). Prevalence and treatment of diabetes in China, 2013-2018. JAMA 326 (24), 2498–2506. doi:10.1001/jama.2021.22208
Wang, L., Yu, J., Fordjour, P. A., Xing, X., Gao, H., Li, Y., et al. (2017). Danshen injection prevents heart failure by attenuating post-infarct remodeling. J. Ethnopharmacol. 205, 22–32. doi:10.1016/j.jep.2017.04.027
Wang, P., Huang, H., Chen, B., Su, Y., Shi, P., and Yao, H. (2020). Systems pharmacology dissection of mechanisms of dengzhan Xixin injection against cardiovascular diseases. Chem. Pharm. Bull. 68 (9), 837–847. doi:10.1248/cpb.c20-00122
Wang, Y., Guo, Y., Lei, Y., Huang, S., Dou, L., Li, C., et al. (2021b). Design and methodology of a multicenter randomized clinical trial to evaluate the efficacy of tongmai jiangtang capsules in type 2 diabetic coronary heart disease patients. Front. Pharmacol. 12, 625785. doi:10.3389/fphar.2021.625785
Xue, F., Cheng, J., Liu, Y., Cheng, C., Zhang, M., Sui, W. H., et al. (2022). Cardiomyocyte -specific knockout of ADAM17 ameliorates left ventricular remodeling and function in diabetic cardiomyopathy of mice. Signal Transduct. Target Ther. 7 (1), 259. doi:10.1038/s41392-022-01054-3
Yang, J., Dou, G., Tesche, C., De Cecco, C. N., Jacobs, B. E., Schoepf, U. J., et al. (2019). Progression of coronary atherosclerotic plaque burden and relationship with adverse cardiovascular event in asymptomatic diabetic patients. BMC Cardiovasc Disord. 19 (1), 39. doi:10.1186/s12872-019-1016-4
Yang, Z. R., Bao, X. L., Dong, C. L., and Gong, Y. B. (2017). A review of TCM pattern correlation in type 2 diabetes and coronary heart disease. Univers. Tradit. Chin. Med. 10 (05), 631–635. doi:10.3969/j.issn.1674-1749.2017.05.037
Ye, W. F., Su, G. Z., and Zhang, D. F. (2021). Effect of Erigeron Breviscapus Injection on angina pectoris of coronary heart disease. Drugs Clin. 40 (9), 3. doi:10.16662/j.cnki.1674-0742.2021.09.086
Yu, J. B., and Shao, M. J. (2021). Clinical characteristics and biochemical indexes of patients with coronary heart disease complicated with type 2 diabetes. Chin. J. Gerontology 41 (4), 3. doi:10.3969/j.issn.1005-9202.2021.04.006
Zhang, C. H. (2016). Effects of Shuxuetong Injection on hemorheology, platelet activation function and myocardial injury after PCI in patients with unstable angina. Chin. Pat. Med. 38 (05), 992–996. doi:10.3969/j.issn.1001-1528.2016.05.006
Zhang, J. P., Zhang, Y. Y., Zhang, Y., Gao, Y. G., Ma, J. J., Wang, N., et al. (2013). Salvia miltiorrhiza (Danshen) injection ameliorates iron overload-induced cardiac damage in mice. Planta Med. 79 (9), 744–752. doi:10.1055/s-0032-1328588
Zhang, M., Sui, W. H., Xing, Y. Q., Cheng, J., Cheng, C., Xue, F., et al. (2021). Angiotensin IV attenuates diabetic cardiomyopathy via suppressing FoxO1-induced excessive autophagy, apoptosis and fibrosis. Theranostics 11 (18), 8624–8639. doi:10.7150/thno.48561
Zhang, Y. C., Lu, B. J., Zhao, M. H., Rong, Y. Z., and Chen, R. M. (2008). Effect of Shengmai injection on vascular endothelial and heart functions in patients with coronary heart disease complicated with diabetes mellitus. Chin. J. Integr. Med. 14 (4), 281–285. doi:10.1007/s11655-008-0281-3
Keywords: traditional Chinese medicine injection, diabetes mellitus, coronary heart disease, network meta-analysis, systematic review
Citation: Shen H, Zhou P, Shen L, Ju C, Du H and Qu X (2023) Effectiveness and safety of selected traditional Chinese medicine injections in patients with combined diabetes mellitus and coronary heart disease: A systematic review and network meta-analysis of randomized clinical trials. Front. Pharmacol. 13:1060956. doi: 10.3389/fphar.2022.1060956
Received: 04 October 2022; Accepted: 27 December 2022;
Published: 09 January 2023.
Edited by:
Rong-Rong He, Jinan University, ChinaReviewed by:
Panpan Hao, Shandong University, ChinaCopyright © 2023 Shen, Zhou, Shen, Ju, Du and Qu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Haixia Du, ZGh4MzExMDUxM0AxNjMuY29t; Xianguo Qu, cXV4aWFuZ3VvQDE2My5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.