
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol., 24 November 2022
Sec. Drugs Outcomes Research and Policies
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.1054603
This article is part of the Research TopicEffective Methods to Promote Appropriate Use of MedicinesView all 16 articles
 Wenjing Cao1,2
Wenjing Cao1,2 Azidah Abdul Kadir3
Azidah Abdul Kadir3 Juan Wang4Lin Hu2Linlan Wen5Mei Yu6Liqun Peng7Lanying Chen7Na Luo2
Juan Wang4Lin Hu2Linlan Wen5Mei Yu6Liqun Peng7Lanying Chen7Na Luo2 Intan Idiana Hassan1*
Intan Idiana Hassan1*Aim: Medication non-adherence has remained a common and costly global health issue of growing importance among older adults. This study aims to determine the prevalence and associated factors related to medication non-adherence among older adult stroke survivors in China.
Methods and results: In this cross-sectional study, a total of 402 older adult stroke survivors were recruited from three tertiary hospitals in China. The results of the survey showed that 61.4% exhibited medication non-adherence. The chances of medication non-adherence among older adult stroke survivors who had primary school or less educational levels were higher than those who had senior secondary and junior college educational levels [OR (95% CI) = 0.440(0.249, 0.778)] as well as those who had a bachelor’s degree or above educational levels [OR (95%CI) = 0.367(0.202, 0.667)]. Moreover, the probability of medication non-adherence with 4–5 and ≥6 types of total prescription medications per day increased by 1.993 times [OR (95% CI) = 1.993(1.190, 3.339))] and 2.233 times [OR (95%CI) = 2.233(1.159, 4.300)], respectively, as compared to when there were ≤3 types. Furthermore, medication non-adherence decreased with the increase in health literacy scores (β = −0.641 (95% CI; (0.913, 0.965)) and BMQ specific-necessity scores (β = −0.131 (95% CI; 0.806, 0.995)). On the other hand, when the BMQ specific-concerns score increased by one unit, medication non-adherence increased by 11.1% [OR (95% CI) = 1.111(1.044, 1.182)].
Conclusion: The present study found that patient medication adherence among older adult stroke survivors in China is problematic and associated with educational levels, total prescribed drugs per day, beliefs about medication, and health literacy scores. This indicates that measures should be taken to enhance medication adherence among such higher-risk populations.
Globally, stroke remains the second leading cause of death and the third leading cause of disability in adults (Zhang et al., 2021; Feigin et al., 2022). In 2019, stroke was responsible for 143 million disability-adjusted life-years and 6·55 millions of deaths (Feigin et al., 2022). In this context, many published studies have concluded that multiple modifiable or non-modifiable factors may increase the risk of stroke occurrences. Here, it is worth mentioning that approximately three-quarters of all strokes occur in persons older than 65 years (Yousufuddin and Young, 2019). Additionally, Gorelick (2019) suggested that to relieve the future global burden of strokes, prevention among older adults would be an important objective.
Stroke survivors are at an elevated risk of having recurrences (Del et al., 2019), which make up 25–30% of all strokes (Hankey, 2014). As recurrent strokes are associated with high mortality and more disabling (Wu et al., 2019), prescribed medications are recommended for secondary prevention of stroke by guidelines (Coutts et al., 2015; Ahmed et al., 2019). Moreover, several sources of evidence indicate that secondary prevention medications tend to reduce the risk of stroke recurrence (Bushnell et al., 2014; Flach et al., 2020; Yeo et al., 2020). For example, it has been conclusively shown that higher adherence to antithrombotic or statin treatments is associated with a decreased risk of stroke recurrence and mortality (Yeo et al., 2020; Rodriguez-Bernal et al., 2021). In the same vein, Toyoda et al. (2019) reported that the combination of cilostazol with aspirin or clopidogrel resulted in a reduced recurrence of ischemic strokes. In addition, a review conducted by Katsanos and Hart (2020) indicated that an important protection against recurrent strokes is provided by the current triad of pharmacologic mainstays for secondary stroke prevention: blood-pressure lowering drugs, statin drugs, and antiplatelet agents. Meanwhile, there is consensus among scientists that non-medication adherence is a potential modifiable risk factor for poor BP control (Boima et al., 2015; Burnier and Egan, 2019), which is itself a well-established and modifiable risk factor for strokes.
However, patient adherence to medication is largely accounted for the effect of medical management to prevent recurrent strokes and other adverse outcomes (Zhang et al., 2021). Medication adherence is generally defined as the extent to which patients take their medication in line with the recommendations of their healthcare provider (Sabaté, 2003). A large and growing body of literature has reported that post-stroke medication adherence and persistence rates are low in stroke survivors (Kim et al., 2020; Ruksakulpiwat et al., 2020; Zhang et al., 2021). These results, therefore, suggest that improving medication adherence among survivors of stroke should be a growing concern to clinicians, healthcare systems, and other stakeholders (e.g., payers).
There is no doubt that a key step in the creation of an appropriate strategy to improve medication adherence is first understanding stroke survivors’ non-medication adherence and its associated factors. Although several studies have shown the prevalence and factors associated with medication adherence among stroke survivors (Pan et al., 2017; Wei et al., 2017; Ruksakulpiwat et al., 2020), they are not specific to older adults. Furthermore, it is important to note that medication adherence is of a particular concern in older persons. A recent systematic review indicated factors negatively associated with adherence in this population: complex regimens with multiple prescribing physicians; problems with medication storage and formulation; and multimorbidity and cognitive impairment (Smaje et al., 2018). On the other hand, non-medication adherence rates among older adults in other chronic diseases (e.g., diabetes mellitus and hypertension patients) have been found to be alarmingly high (Saqlain et al., 2019; Xu et al., 2020). Meanwhile, older adult stroke survivors are likelier to have other chronic medical conditions (e.g., hypertension, history of cardiac-related comorbidities, diabetes, etc.) (Gruneir et al., 2016; Maresova et al., 2019), which means they have to take more medications to meet their broader health needs, thus further challenging their adherence to medications and an increase in the possibilities of worse health-related risks when non-adherence occurs. However, little is known about the prevalence of non-medication adherence and the factors associated with it among older adult stroke survivors, which this study aims to examine among older adult stroke survivors in Chenzou, Hunan, China.
We conducted a cross-sectional study from June 2022 to August 2022. The study was approved by the ethics committee of three tertiary hospitals (Affiliated Hospital of Xiangnan University, Chenzhou No. 1 People’s Hospital, and Chenzhou Third People’s Hospital) before the initiation of this study.
Participants were recruited using a systematic sampling method from three tertiary hospitals in Chenzhou, Hunan Province, China. They were eligible for inclusion based on the following criteria: if they were aged 60 years or older; had a history of strokes confirmed by neuroimaging at the time of the episode; taken at least one medication in the previous month such as (but not limited to) anti-platelets, statins, and anti-hypertensives to control risk factors for strokes; it had been more than a month since the last stroke episode; were able to read Chinese and communicate in Mandarin Chinese or the local Chenzhou dialect. We excluded the following patients who: had psychiatric illness or deafness, aphasia, or other language barriers; had cognitive impairment (Mini-Mental State Examination score ≤17 [for illiterate] or ≤20 [individuals with 1–6 years of education] or ≤24 [individuals with 7 or more years of education]).
Sample size calculations were conducted to determine the prevalence of medication non-adherence using a single proportion formula and the associated factors using PS Power and Sample Size software version 3.1.6 for a dichotomous two-proportion formula. Based on the calculations, the highest sample size of 416 was chosen. This sample size was based on a precision of 0.05 and power of 80%; the proportion of permanent employment being 0.448 was based on the study by Kim et al. (2020). However, after considering the non-response level of 10%, the calculated sample size is 458.
The study protocol included one set of demographic questions and three validated instruments—the General Medication Adherence Scale (GMAS-C), Beliefs about Medicines Questionnaire (BMQ), and Health Literacy Scale for Stroke Patients.
Demographic data were self-reported by the participants and included gender, age, marital status, educational level, duration of disease, living conditions, membership in ethnic groups, payment method for medical expenses, per-capita monthly household income, occupation status, number of prescribed medicines, frequency of daily doses, types of strokes, residence, and existence of comorbidities.
The GMAS-C is a self-report tool containing 11 items that measure medication adherence among patients with chronic diseases, including strokes. It consists of three dimensions: 1) patient behavior-related non-adherence (five items), 2) additional disease and pill burden (four items), and 3) cost-related non-adherence (two items). All items are answered on a four-point Likert scale: responses of “always,” “mostly,” “sometimes,” and “never” are scored as 0, 1, 2, and 3, respectively. The total GMAS-C score is the summation of the scores for the 11 items and ranges from 0 to 33: high adherence (30–33), good adherence (27–29), partial adherence (17–26), low adherence (11–16), and poor adherence (0–10). Patients with a total score of 26 and below are considered medication non-adherent, while a score of 27 and above indicates adherence (Naqvi et al., 2019).
Moreover, Wang et al. (2021) undertook validity and reliability studies of the Chinese version of the GMAS-C in 2021 and found that the exploratory factor analysis extracted three factors with eigenvalues >1 and that 60% of the total variance was explained by a three-factor solution. Next, confirmatory factor analysis showed acceptable fit indices (χ2/df = 1.58, IFI = 0.96, TLI = 0.94, CFI = 0.96, and RMSEA = 0.05). Thus, it was concluded that the scale was a valid and reliable instrument for the assessment of medication adherence.
The BMQ was developed to assess personal beliefs and worries about taking medications for diseases (Horne and Weinman, 1999a). It consists of two domains—the BMQ-Specific and BMQ General—that are independently validated and can be used in combination or separately. In this study, we used only the BMQ-Specific because Horne and Weinman (1999a) reported that it is a flexible instrument that can be adapted to assess beliefs about all medicines for a particular condition or individual components of a regimen. The Chinese version of the BMQ-Specific has been proved to be a good instrument with acceptable reliability and validity. The Cronbach’s α coefficients of the necessary and concerns dimensions were 0.813 and 0.706, respectively, and the test–retest reliability coefficients were 0.743 and 0.786, respectively (Yang, et al., 2014). The BMQ-Specific has two subscales (specific-necessity and the specific-concerns) with five questions each, which aim to assess beliefs about the necessity of prescribed medication and concerns about them based on beliefs about the danger of dependence, long-term toxicity, and the disruptive effects of medication (Verhagen, 2018).
The Chinese version of the Health Literacy Scale for Stroke Patients has been used to assess the health literacy of patients who have had a stroke and proved to be a good instrument with acceptable reliability and validity (Jiru, et al., 2020). It has three subscales and a total of 20 items. The first subscale is basic knowledge of strokes, which consists of six items. A five-point Likert scale is used, and responses are assigned to a score of 5 for “strongly agree,” 4 for “agree,” 3 for “neutral,” 2 for “disagree,” and 1 for “strongly disagree.” For two items (4,5), reverse scoring is applied. The second subscale with nine items evaluates the healthy lifestyles and behaviors of stroke survivors: it is responded to as follows: 1—“never”; 2—“rarely”; 3—“sometimes”; 4—“often”; and 5—“always.” Reverse coding was carried out for item 2 because it is a negative statement. The third subscale is related to the basic skills of stroke survivors and consists of five items, for which a five-point Likert score method is used. The response options are “never,” “rarely,” “sometimes,” “often,” and “always,” which corresponds to the scores of 1, 2, 3, 4, and 5 points, respectively. A higher score indicates better health literacy.
Data were collected using a questionnaire-guided interview method. Written informed consent was received prior to the respondents answering the questionnaire. This study was conducted in full accordance with the principles of the Declaration of Helsinki. The participants were informed that their participation was voluntary and that they had the right to withdraw from the study at any time without any influence, coercion, or persuasion. Questionnaires were distributed and completed by participants (it took approximately 20 min to complete the questionnaires) who were in rehabilitation settings, at the departments of neurology, or at the out-patient clinics during the investigation period. A total of 458 stroke survivors who were admitted to hospitals were approached. Five trained health professionals who speak the local language and did not work at the study hospital were recruited to distribute and collect questionnaires. In order to familiarize data collectors the data collection tool, we conducted training prior to the study. Regarding illiterate participants or those with eye problems, the question items were read word by word exactly as they appeared on the questionnaires by the researchers. Responses were then recorded on the questionnaire. Upon completion, the questionnaires were collected immediately and checked for any missing information, after which follow-ups were undertaken with the participants if needed.
All statistical analyses were performed using the Statistical Program for the Social Sciences (SPSS version 26). The data were checked, explored, and cleaned. Descriptive statistics was used to calculate the frequency and percentage (categorical data) or the mean and standard deviations (continuous data). The prevalence of medication adherence was calculated using the aforementioned cutoff scores and reported as the percentage of cases in different populations. The 95% CIs were produced using exact binomial methods. The chi-squared test method was used for univariate analysis. To explore factors that are potentially associated with medication non-adherence, binary logistic regression analyses were performed, and odds ratios (ORs) and 95% CIs were presented. p-values less than 0.05 were considered statistically significant throughout the analysis.
A total of 458 older adult stroke survivors were approached, with 402 giving consent and being enrolled in the study (response rate of 87.8%). Most participants were male (243 [60.4%]), were married (293 [72.9%]), were of Han nationality (350 [87.5%]), and had comorbidities (334 [83.1%]). Of the 402 responding participants, 341 (84.8%) had ischemic strokes, while 61 (15.2%) had hemorrhagic strokes. Meanwhile, 43.5% resided in city areas, and 42.0% took medicine only one time a day. Almost half the participants (211 [52.5%]) were unemployed. Approximately one-third (39.2%) only had a primary school education or less. Those living with spouses represented 51.0% of the sample, and 43.5% used rural cooperative medical insurance. A total of 184 participants (45.8%) had a monthly per-capita income between 1,001 and 3,000 ¥. The mean age of participants was 72.16 ± 7.43 SD, the mean (SD) duration of stroke disease was 49.37 (51.99) months, and the mean total types of prescription medications per day was 3.96 (1.68). The characteristics of the study participants are shown in Table 1.
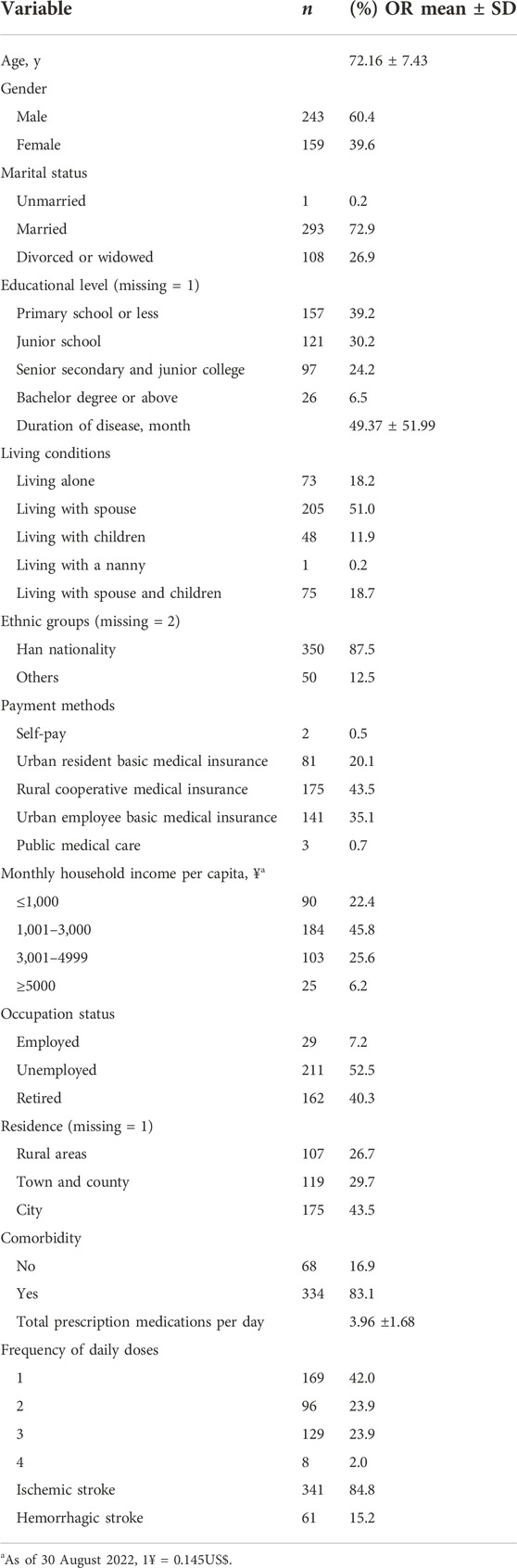
TABLE 1. Demographic characteristics of total participants (N = 402).
Of the 402 responding participants, 247 (61.4%) exhibited medication non-adherence. In total, 22.6% of the participants had high adherence, approximately 64 (15.9%) of the participants had good adherence, and 149 (37.1%) had partial adherence. Meanwhile, low adherence and poor adherence were 13.7% and 10.7%, respectively. The participants’ medication adherence is detailed in Table 2.
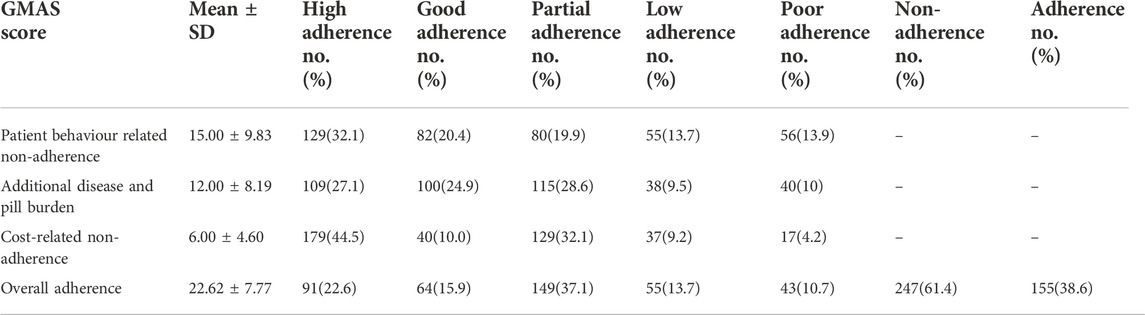
TABLE 2. Medication adherence among patients.
Table 3 shows the univariate analysis of the factors associated with medication non-adherence, which are as follows: educational level (p < 0.001), payment methods (p < 0.001), total prescription medications per day (p = 0.002), monthly income per capita (p < 0.001), occupation status (p < 0.001), residence (p < 0.001), BMQ specific-necessity score (p < 0.001), BMQ specific-concerns score (p = 0.002), and health literacy score (p < 0.001).
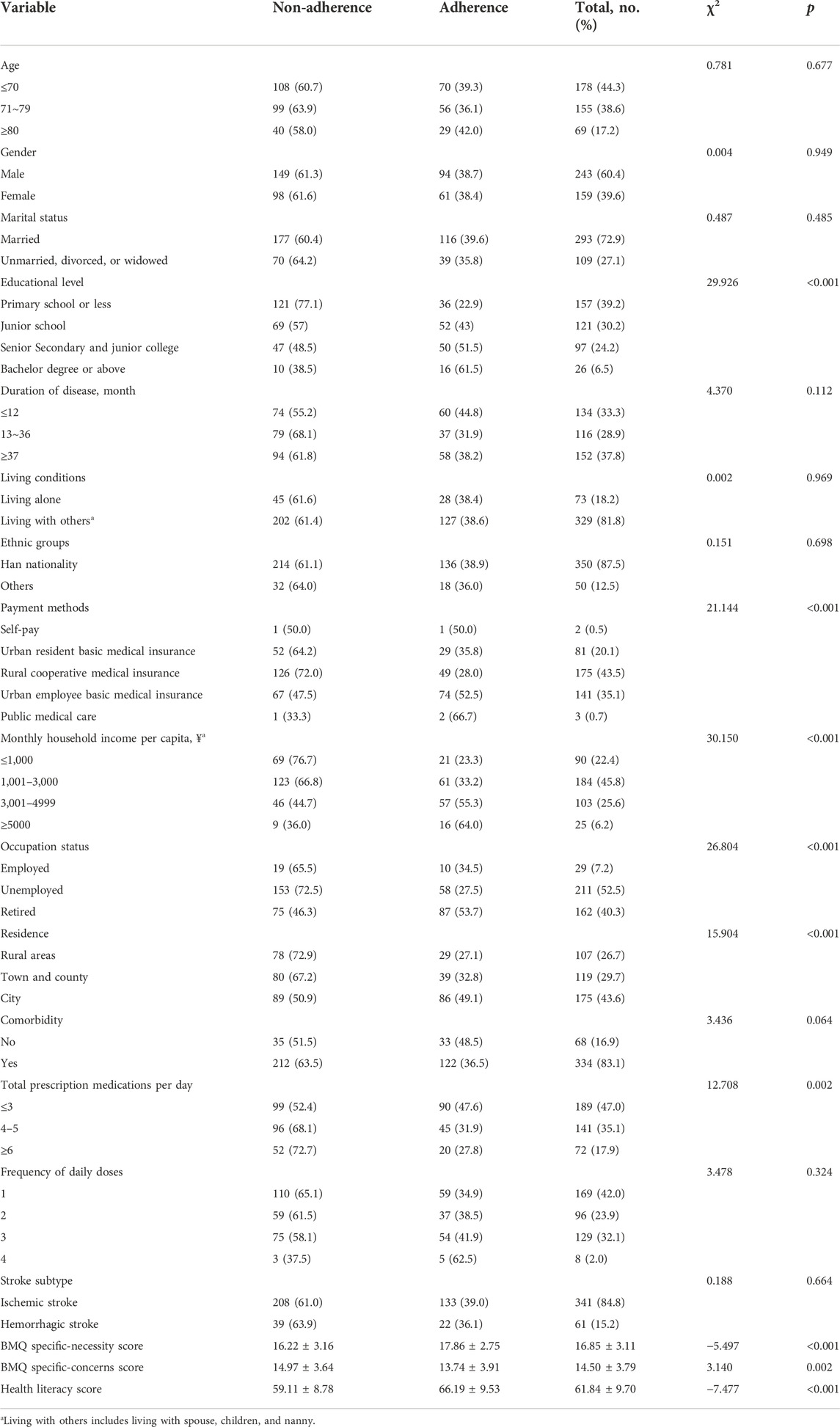
TABLE 3. Relationship of non-adherence with related factors.
All variables with a p-value < 0.05 in the univariate analysis were included in the logistic regression analysis. Table 4 shows the results of the multivariable analyses. Results from logistic regression suggest that educational level and total prescription medications per day as well as the BMQ specific-necessity, BMQ specific-concerns, and health literacy scores were associated with medication non-adherence.
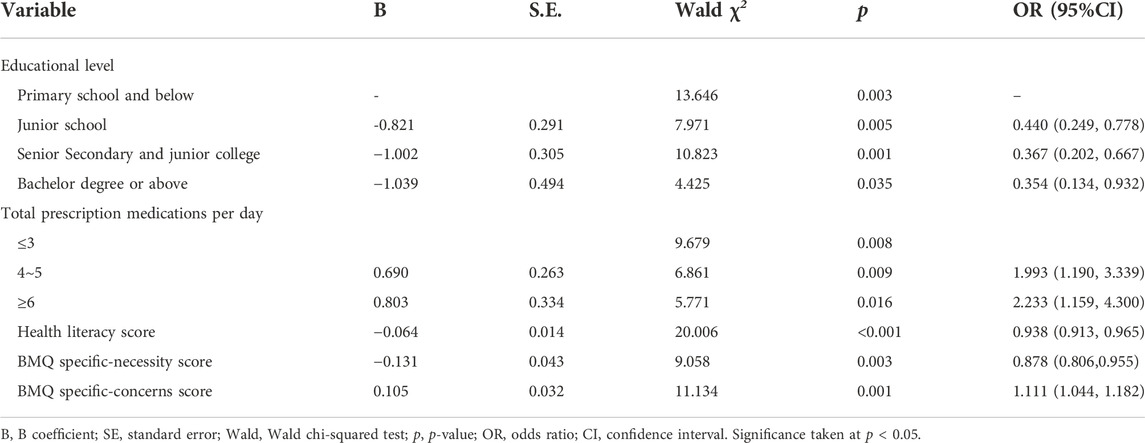
TABLE 4. Factors associated with medication non-adherence using logistic regression.
Compared to stroke survivors who had primary school or less educational levels, those with senior secondary and junior college educational levels [OR (95% CI) = 0.440(0.249, 0.778)] as well as those who had bachelor’s degree or above [OR (95% CI) = 0.367(0.202, 0.667)] had significantly decreased risks of medication non-adherence. Those with 4–5 types of total prescription medications per day had 1.993 times the risk of medication non-adherence as compared to those with ≤3 types [OR (95% CI) = 1.993(1.190, 3.339)]. On the other hand, those with ≥6 types of total prescription medications per day were 2.233 times likelier to be medication non-adherent as compared to those with ≤3 types [OR (95% CI) = 2.233(1.159, 4.300)]. Furthermore, when the BMQ specific-concerns score increased by one unit, the medication non-adherence increased by 11.1% [OR (95% CI) = 1.111(1.044, 1.182)]. Meanwhile, for every one-unit increase in the Health Literacy Scale for Stroke Patients score, there will be a 0.938 times decrease in the GMAS-C score (β = −0.641 (95% CI; (0.913, 0.965)). Lastly, for every one-unit increase in the BMQ specific-necessity score, there will be a 0.878 times decrease in the GMAS-C score (β = −0.131, (95% CI; 0.806, 0.995)).
To the best of our knowledge, this cross-sectional study is the first to evaluate medication non-adherence among older adult stroke survivors in China. Our findings showed that medication non-adherence was observed in 61.4% of the 402 sampled patients. Specifically, partial adherence, low adherence, and poor adherence were found to be 37.1%, 13.7%, and 10.7%, respectively. Moreover, the findings in terms of the non-adherence rates in the current study were much higher than those previously published in a meta-analysis of observational studies regarding post-stroke patients. The latter indicated that the overall non-adherence rate to secondary preventative medication among stroke survivors was 30.9%–35.9% (Al et al., 2016; Zhang et al., 2021). A possible explanation for this is that the aforementioned studies included all stroke patients aged over 18 years, while the present study focused on patients over 60 years of age. In this context, Yuvaraj et al. (2019) found that being part of the elderly age group is a determinant of non-adherence to medications after adjusting for possible confounding variables. Older adults are prone to multiple comorbidities and use more medications than their younger counterparts and may therefore present with a higher risk of medication non-adherence (Chiang-Hanisko et al., 2014). Taken together, our findings present concerns about the alarming rate of non-medication adherence among older adult stroke survivors in Chenzhou, Hunan Province, China, which requires further attention. This finding, while preliminary, suggests that strategies to promote medication adherence among this group are urgently needed.
Meanwhile, the educational level was found to be a predictor of medication non-adherence among older adult stroke survivors. According to our findings, patients who had higher educational levels were less likely to be non-adherent as compared to those who had attended only primary school or less. These results are consistent with those of other studies and suggest that higher education levels are associated with adherence (Kirkman et al., 2015; Jin et al., 2016; Bandi et al., 2017). This could be explained by the fact that those with higher educational levels may be less likely to have negative beliefs about medications (Lemay et al., 2018), which would promote medication adherence. Therefore, when seeking strategies to improve medication adherence among stroke survivors, educational-level factors must be considered. Meanwhile, it is worth noting that the average duration of education for stroke patients was significantly lower in patients aged ≥65 years than in patients aged <65 years (Lu et al., 2018). Such findings help shed light on the educational level as an important challenge for medication adherence interventions among older adult stroke survivors.
Among the common concerns, we found that the medication non-adherence of stroke survivors increased with that of total prescription medications per day. These results are congruent with the findings of earlier studies that indicate older adults are more adherent to a simplified medication regime (Jin et al., 2016). A possible explanation of this result is that patients may be less likely to forget to take medicine if the number of pills is low (Napolitano et al., 2016). However, Kim et al. (2020) reported that optimal medication adherence was associated with more prescribed medicines. This rather contradictory result could be attributed to the study including chronic diseases, while our study only considered elderly stroke patients.
Another important finding was that low needs or high concern regarding medication were associated with medication non-adherence. This finding is in agreement with previous studies on medication adherence among elderly people with chronic diseases (Lemay et al., 2018; Park et al., 2018), which revealed that as compared to patients with high needs and low concerns about medication, those with low needs and high concerns had significantly high medication non-adherence. Our results corroborated that of Horne and Weinman (1999b) who suggested that beliefs in medication may offer accurate predictability about adherence. Additionally, concerns about prescribed medications and unawareness of the rationale for treatments were expressed as primary reasons for non-adherence by stroke survivors (Bauler et al., 2014). Hence, for medical professionals, it is of great importance to outline and educate patients on the necessity of treatments rather than simply providing information about medication, while also managing patients’ concerns by sharing the known side effects of prescribed drugs and helping them recognize and cope with side effects to improve their confidence.
Overall, the most important clinically relevant finding was that health literacy is significantly associated with medication non-adherence. Here, health literacy refers to the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to understand and use information to promote, maintain, or improve their health (Ratzan, 2001). According to this finding, lower health literacy has a greater likelihood of being associated with non-medication adherence. This result matches those observed in earlier studies (Lee et al., 2017; Mayo-Gamble and Mouton, 2018). This may be attributable to the fact that low health literacy is associated with less understanding of prescribed medication instructions (Mayo-Gamble and Mouton, 2018) and problems in using preventive services (Stormacq et al., 2019). As health literacy is considered the most important modifiable risk factor of socioeconomic differences in health (šedová et al., 2021), future work should investigate tailored interventions considering health literacy among older adult stroke survivors.
The most important strength of this study is that to the best of our knowledge, it provides invaluable information on the prevalence and factors associated with medication non-adherence by using standardized rating scales among older adult stroke survivors in Chenzhou, Hunan Province, China. Furthermore, our findings may provide a comprehensive picture of medication non-adherence among stroke survivors, which may lay the groundwork for interventions aimed at increasing adherence among this population. Here, it should be noted that our participant population was older adult stroke survivors, who have been frequently left out of studies. Hence, our study addresses an understudied group.
However, this study has limitations that are worth considering. First, information on medication adherence was collected for the previous months prior to the survey, so some degree of recall bias cannot be ruled out. This could lead to inaccurate estimations of the prevalence of medication non-adherence. Additionally, the data relied on self-reported practices of medication adherence, which might have been over- or under-reported by participants. Second, it was limited in scope. Participants were from three tertiary hospitals in Chenzhou, Hunan Province, China, which limits its generalizability to the broader regions in China. Third, this was a cross-sectional study. Therefore, associations between medication non-adherence and risk factors cannot necessarily be considered causal relationships.
Our findings emphasize that medication adherence among older adult stroke survivors is problematic in this sample of study participants from Chenzhou, Hunan Province, China. Specifically, we found that medication non-adherence was significantly associated with educational levels, number of prescription medications to be taken per day, low needs or high concerns for medication, and health literacy. Building on this, we have offered specific recommendations for proposing population-specific medication adherence interventions among older adult stroke survivors. Our findings also suggest that efforts are needed to explore the prevalence and associated factors of medication non-adherence among older adult stroke survivors in other countries.
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the ethical committees of the Affiliated hospital of Xiangnan University (Linyan K2022—003—01), Chenzhou No. 1 People’s Hospital (Yu2022033)and Third People’s Hospital (Lunshen 2022—10). All participants gave written consent.
IIH and AAK conceived and proposed the idea. JW and WC designed the work. WC, LC, LP, and NL contributed to the data collection. WC and LH contributed to data analysis and the interpretation of data for the work. WC wrote the first draft of the manuscript. IIH, AAK, and JW helped revise the manuscript. All authors read and approved the submitted version.
This work was supported by a special fund for young key teachers in Hunan Province, China (Xiangjiaotong (2021) 29) and the Hunan University Students’ Innovation and Entrepreneurship Training Project (Xiangjiaotong (2022) 174 -4315).
The authors would like to thank the physicians and nurses of the departments of neurology at the three hospitals visited for this study for their valuable support and cooperation in conducting this study. The authors are also particularly grateful to the contributions of the patients who participated in this research. Finally, the authors would like to thank Scribendi for their professional proofreading of this manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Ahmed, N., Audebert, H., Turc, G., Cordonnier, C., Christensen, H., Sacco, S., et al. (2019). Consensus statements and recommendations from the ESO-karolinska stroke update conference, stockholm 11-13 november 2018. Eur. Stroke J. 4 (4), 307–317. doi:10.1177/2396987319863606
Al, A. S., Quinn, T., Dunn, W., Walters, M., and Dawson, J. (2016). Predictive factors of non-adherence to secondary preventative medication after stroke or transient ischaemic attack: A systematic review and meta-analyses. Eur. Stroke J. 1 (2), 65–75. doi:10.1177/2396987316647187
Bandi, P., Goldmann, E., Parikh, N. S., Farsi, P., and Boden-Albala, B. (2017). Age-related differences in antihypertensive medication adherence in hispanics: A cross-sectional community-based survey in New York city, 2011-2012. Prev. Chronic Dis. 14, E57. doi:10.5888/pcd14.160512
Bauler, S., Jacquin-Courtois, S., Haesebaert, J., Luaute, J., Coudeyre, E., Feutrier, C., et al. (2014). Barriers and facilitators for medication adherence in stroke patients: A qualitative study conducted in French neurological rehabilitation units. Eur. Neurol. 72 (5-6), 262–270. doi:10.1159/000362718
Boima, V., Ademola, A. D., Odusola, A. O., Agyekum, F., Nwafor, C. E., Cole, H., et al. (2015). Factors associated with medication nonadherence among hypertensives in Ghana and Nigeria. Int. J. Hypertens. 2015, 205716. doi:10.1155/2015/205716
Burnier, M., and Egan, B. M. (2019). Adherence in hypertension. Circ. Res. 124 (7), 1124–1140. doi:10.1161/CIRCRESAHA.118.313220
Bushnell, C., Arnan, M., and Han, S. (2014). A new model for secondary prevention of stroke: Transition coaching for stroke. Front. Neurol. 5, 219. doi:10.3389/fneur.2014.00219
Chiang-Hanisko, L., Tan, J. Y., and Chiang, L. C. (2014). Polypharmacy issues in older adults. Hu Li Za Zhi 61 (3), 97–104. doi:10.6224/JN.61.3.97
Coutts, S. B., Wein, T. H., Lindsay, M. P., Buck, B., Cote, R., Ellis, P., et al. (2015). Canadian stroke best practice recommendations: Secondary prevention of stroke guidelines, update 2014. Int. J. Stroke. 10 (3), 282–291. doi:10.1111/ijs.12439
Del, B. V., Chaturvedi, S., Diener, H. C., Romano, J. G., and Sacco, R. L. (2019). Antithrombotic therapy to prevent recurrent strokes in ischemic cerebrovascular disease: JACC scientific expert panel. J. Am. Coll. Cardiol. 74 (6), 786–803. doi:10.1016/j.jacc.2019.06.039
Feigin, V. L., Brainin, M., Norrving, B., Martins, S., Sacco, R. L., Hacke, W., et al. (2022). World stroke organization (WSO): Global stroke fact sheet 2022. Int. J. Stroke. 17 (1), 18–29. doi:10.1177/17474930211065917
Flach, C., Muruet, W., Wolfe, C., Bhalla, A., and Douiri, A. (2020). Risk and secondary prevention of stroke recurrence: A population-base cohort study. Stroke 51 (8), 2435–2444. doi:10.1161/STROKEAHA.120.028992
Gorelick, P. B. (2019). The global burden of stroke: Persistent and disabling. Lancet. Neurol. 18 (5), 417–418. doi:10.1016/S1474-4422(19)30030-4
Gruneir, A., Griffith, L. E., Fisher, K., Panjwani, D., Gandhi, S., Sheng, L., et al. (2016). Increasing comorbidity and health services utilization in older adults with prior stroke. Neurology 87 (20), 2091–2098. doi:10.1212/WNL.0000000000003329
Hankey, G. J. (2014). Secondary stroke prevention. Lancet. Neurol. 13 (2), 178–194. doi:10.1016/S1474-4422(13)70255-2
Horne, R., and Weinman, J. (1999a). Patients' beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J. Psychosom. Res. 47 (6), 555–567. doi:10.1016/s0022-3999(99)00057-4
Horne, R., and Weinman, J. (1999b). Patients' beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J. Psychosom. Res. 47 (6), 555–567. doi:10.1016/s0022-3999(99)00057-4
Jin, H., Kim, Y., and Rhie, S. J. (2016). Factors affecting medication adherence in elderly people. Patient prefer. Adherence 10, 2117–2125. doi:10.2147/PPA.S118121
Jiru, L., Juan, L., and Fang, T.(2020). Development and reliability and validity test of the health literacy scale for stroke patients. 34(18), 3220–3225.doi: doi:10.12102/j.issn.1009-6493.2020.18.007
Katsanos, A. H., and Hart, R. G. (2020). New horizons in pharmacologic therapy for secondary stroke prevention. JAMA Neurol. 77 (10), 1308–1317. doi:10.1001/jamaneurol.2020.2494
Kim, G. G., Chae, D. H., Park, M. S., and Yoo, S. H. (2020). Factors influencing 1-year medication adherence of Korean ischemic stroke survivors. Int. J. Behav. Med. 27 (2), 225–234. doi:10.1007/s12529-020-09854-z
Kirkman, M. S., Rowan-Martin, M. T., Levin, R., Fonseca, V. A., Schmittdiel, J. A., Herman, W. H., et al. (2015). Determinants of adherence to diabetes medications: Findings from a large pharmacy claims database. Diabetes Care 38 (4), 604–609. doi:10.2337/dc14-2098
Lee, Y. M., Yu, H. Y., You, M. A., and Son, Y. J. (2017). Impact of health literacy on medication adherence in older people with chronic diseases. Collegian 24 (1), 11–18. doi:10.1016/j.colegn.2015.08.003
Lemay, J., Waheedi, M., Al-Sharqawi, S., and Bayoud, T. (2018). Medication adherence in chronic illness: Do beliefs about medications play a role? Patient prefer. Adherence 12, 1687–1698. doi:10.2147/PPA.S169236
Lu, H., Guo, Z., Liu, J., Zhang, H., Zhao, W., Wu, Y., et al. (2018). Trends in stroke incidence among elderly low-income residents of rural China: A population-based study from 1992 to 2016. Aging (Albany NY) 10 (11), 3438–3449. doi:10.18632/aging.101657
Maresova, P., Javanmardi, E., Barakovic, S., Barakovic, H. J., Tomsone, S., Krejcar, O., et al. (2019). Consequences of chronic diseases and other limitations associated with old age - a scoping review. BMC Public Health 19 (1), 1431. doi:10.1186/s12889-019-7762-5
Mayo-Gamble, T. L., and Mouton, C. (2018). Examining the association between health literacy and medication adherence among older adults. Health Commun. 33 (9), 1124–1130. doi:10.1080/10410236.2017.1331311
Napolitano, F., Napolitano, P., and Angelillo, I. F. (2016). Medication adherence among patients with chronic conditions in Italy. Eur. J. Public Health. 26 (1), 48–52. doi:10.1093/eurpub/ckv147
Naqvi, A. A., Hassali, M. A., Jahangir, A., Nadir, M. N., and Kachela, B. (2019). Translation and validation of the English version of the general medication adherence scale (GMAS) in patients with chronic illnesses. J. Drug Assess. 8 (1), 36–42. doi:10.1080/21556660.2019.1579729
Pan, J., Lei, T., Hu, B., and Li, Q. (2017). Post-discharge evaluation of medication adherence and knowledge of hypertension among hypertensive stroke patients in northwestern China. Patient prefer. Adherence 11, 1915–1922. doi:10.2147/PPA.S147605
Park, H. Y., Seo, S. A., Yoo, H., and Lee, K. (2018). Medication adherence and beliefs about medication in elderly patients living alone with chronic diseases. Patient prefer. Adherence 12, 175–181. doi:10.2147/PPA.S151263
Ratzan, S. C. (2001). Health literacy: Communication for the public good. Health promot. Int. 16 (2), 207–214. doi:10.1093/heapro/16.2.207
Rodriguez-Bernal, C. L., Sanchez-Saez, F., Bejarano-Quisoboni, D., Riera-Arnau, J., Sanfelix-Gimeno, G., and Hurtado, I. (2021). Real-world management and clinical outcomes of stroke survivors with atrial fibrillation: A population-based cohort in Spain. Front. Pharmacol. 12, 789783. doi:10.3389/fphar.2021.789783
Ruksakulpiwat, S., Liu, Z., Yue, S., and Fan, Y. (2020). The association among medication beliefs, perception of illness and medication adherence in ischemic stroke patients: A cross-sectional study in China. Patient prefer. Adherence 14, 235–247. doi:10.2147/PPA.S235107
Sabaté, E. (2003). Adherence to long-term therapies :evidence for action. Geneva: World Health Organization, 198.
Saqlain, M., Riaz, A., Malik, M. N., Khan, S., Ahmed, A., Kamran, S., et al. (2019). Medication adherence and its association with health literacy and performance in activities of daily livings among elderly hypertensive patients in islamabad, Pakistan. Med. Kaunas. 55 (5), E163. doi:10.3390/medicina55050163
šedová, L., Bártlová, S., Hudáčková, A., Havierniková, L., Dolák, F., and Ostrý, S. (2021). Health literacy and modifiable risk factors of a stroke. Kontakt 23 (3), 149–156. doi:10.32725/kont.2021.024
Smaje, A., Weston-Clark, M., Raj, R., Orlu, M., Davis, D., and Rawle, M. (2018). Factors associated with medication adherence in older patients: A systematic review. Aging Med. 1 (3), 254–266. doi:10.1002/agm2.12045
Stormacq, C., Van den Broucke, S., and Wosinski, J. (2019). Does health literacy mediate the relationship between socioeconomic status and health disparities? Integrative review. Health promot. Int. 34 (5), e1–e17. doi:10.1093/heapro/day062
Toyoda, K., Uchiyama, S., Yamaguchi, T., Easton, J. D., Kimura, K., Hoshino, H., et al. (2019). Dual antiplatelet therapy using cilostazol for secondary prevention in patients with high-risk ischaemic stroke in Japan: A multicentre, open-label, randomised controlled trial. Lancet. Neurol. 18 (6), 539–548. doi:10.1016/S1474-4422(19)30148-6
Verhagen, A. P. (2018). Beliefs about medicine questionnaire. J. Physiother. 64 (1), 60. doi:10.1016/j.jphys.2017.04.006
Wang, Y., Wang, X., Wang, X., Naqvi, A. A., Zhang, Q., and Zang, X. (2021). Translation and validation of the Chinese version of the general medication adherence scale (GMAS) in patients with chronic illness. Curr. Med. Res. Opin. 37 (5), 829–837. doi:10.1080/03007995.2021.1901680
Wei, L., Champman, S., Li, X., Li, X., Li, S., Chen, R., et al. (2017). Beliefs about medicines and non-adherence in patients with stroke, diabetes mellitus and rheumatoid arthritis: A cross-sectional study in China. BMJ Open 7 (10), e017293. doi:10.1136/bmjopen-2017-017293
Wu, Q. E., Zhou, A. M., Han, Y. P., Liu, Y. M., Yang, Y., Wang, X. M., et al. (2019). Poststroke depression and risk of recurrent stroke: A meta-analysis of prospective studies. Med. Baltim. 98 (42), e17235. doi:10.1097/MD.0000000000017235
Xu, N., Xie, S., Chen, Y., Li, J., and Sun, L. (2020). Factors influencing medication non-adherence among Chinese older adults with diabetes mellitus. Int. J. Environ. Res. Public Health 17 (17), E6012. doi:10.3390/ijerph17176012
Yang, L., Zheng, L., Meiying, H., Xianhui, M., Liang, C., and Fengrong, A. (2014). The reliability and validity of the Chinese version of Beliefs about Medical Questionnaire among elderly patients with depressive disorder. Chin. J. Nurs. 49 (5), 389–393. doi:10.3761/j.issn.0254-1769.2014.04.001
Yeo, S. H., Toh, M., Lee, S. H., Seet, R., Wong, L. Y., and Yau, W. P. (2020). Impact of medication nonadherence on stroke recurrence and mortality in patients after first-ever ischemic stroke: Insights from registry data in Singapore. Pharmacoepidemiol. Drug Saf. 29 (5), 538–549. doi:10.1002/pds.4981
Yousufuddin, M., and Young, N. (2019). Aging and ischemic stroke. Aging (Albany NY) 11 (9), 2542–2544. doi:10.18632/aging.101931
Yuvaraj, K., Gokul, S., Sivaranjini, K., Manikandanesan, S., Murali, S., Surendran, G., et al. (2019). Prevalence of medication adherence and its associated factors among patients with noncommunicable disease in rural Puducherry, South India - a facility-based cross-sectional study. J. Fam. Med. Prim. Care 8 (2), 701–705. doi:10.4103/jfmpc.jfmpc_350_18
Keywords: medication, non-adherence, older adults, stroke survivors, associated factors
Citation: Cao W, Kadir AA, Wang J, Hu L, Wen L, Yu M, Peng L, Chen L, Luo N and Hassan II (2022) Medication non-adherence and associated factors among older adult stroke survivors in China. Front. Pharmacol. 13:1054603. doi: 10.3389/fphar.2022.1054603
Received: 27 September 2022; Accepted: 02 November 2022;
Published: 24 November 2022.
Edited by:
Tomoya Tachi, Gifu Pharmaceutical University, JapanReviewed by:
Bradi B. Granger, Duke University, United StatesCopyright © 2022 Cao, Kadir, Wang, Hu, Wen, Yu, Peng, Chen, Luo and Hassan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Intan Idiana Hassan, aW50YW5pZGlhbmFAdXNtLm15, aW50YW5pZGlhbmFAeWFob28uY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.