 L. Yesenia Rodríguez-Tanta1*Héctor Garavito Farro2Lisiane Freitas Leal3Maribel Salas4,5Monique M. Elseviers6Luciane Cruz Lopes7*
L. Yesenia Rodríguez-Tanta1*Héctor Garavito Farro2Lisiane Freitas Leal3Maribel Salas4,5Monique M. Elseviers6Luciane Cruz Lopes7*- 1Institute for the Evaluation of Health Technologies and Research, Social Security of Health, Lima, Peru
- 2Ministry of Health of Peru, Lima, Peru
- 3Department of Epidemiology, Biostatistics and Occupational Health, McGill University, Montreal, QC, Canada
- 4Daiichi Sankyo (United States), Parsippany, NJ, United States
- 5Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, United States
- 6Department of Clinical Pharmacology, Ghent University, Ghent, Belgium
- 7Pharmaceutical Science Graduate Course, University of Sorocaba, São Paulo, Brazil
Background: Drug utilization research (DUR) is used to provide evidence-based data to inform policies and make decisions. The aim of this study was to map and describe available data sources for drug utilization research in Peru.
Methods: We performed a search of data sources providing information on medication use on the website of governmental organizations. We also conducted a literature review using PubMed, LILACs, and BVS. Independently, researchers screened eligible data sources. Data characterization included accessibility, coverage data provider, type of data sources, and setting. We performed a descriptive analysis.
Results: We identified seven data sources, CENAFyT, ICI, IDI (SISMED), and ENSUSALUD from MINSA, and CRI-ESSALUD, SGSS/ESSI, and ENSSA from ESSALUD. These presented information on adverse drug reactions (n = 2), drug consumption, and distribution (n = 2), prescription and drug dispensing (n = 1), and surveys addressed to medication users (n = 2). ENSUSALUD was the only data source publicly available. VIGIFLOW and ENSUSALUD have a national granularity from the public and private sectors. The setting of the data sources was both hospital and ambulatory care. Two data sources have individual-level data on adverse drug reactions and one on prescriptions. Four studies on drug utilization research in Peru were derived from ENSUSALUD.
Conclusion: In Peru, few data sources are available for drug utilization research. There is an increased need to monitor medications for decision-making purposes. Local and international initiatives and partnerships of the government with academic institutions and the private sector might be a good strategy to increase the transparency of health data and for supporting decision-making using drug utilization research.
Introduction
Medications are essential to improve individual patient care and public health worldwide. However, inappropriate drug use, particularly, overmedication and self-medication might lead to adverse drug reactions (ADR) (Ahmed et al., 2014; Berreni et al., 2015; Rajan et al., 2019), resulting in non-adherence problems, increase morbidity, mortality, and negative socio-economic consequences (Formica et al., 2018). For these reasons, the evaluation of the process of prescribing, dispensing, and consumption of medicines through Drug Utilization Research (DUR), particularly in low- and middle-income countries, is fundamental to informing policies and make informed decisions from health, economic and social perspectives (Massele et al., 2015).
DUR began in the 1960s and, since then, it has been progressively demanded by health authorities, consumers, and payers. Many countries have developed DUR and are taking advantage of its usefulness to improve access to medicines and to evaluate their impact on the benefit-risk in the real-world setting (Bergman, 2006; Linnér et al., 2020; Monica, 2020; Ontario Ministry of Health, 2020). European countries pioneered DUR with important results in clinical and regulatory settings. In the United States, DUR has contributed to improving the quality of patient care through effective drug management (Sabaté et al., 2014; Wettermark et al., 2016). DUR may also guide healthcare providers (HCP) on the rational use of drugs and promote their cost-effectiveness. However, DUR progress has not been the same across the globe due to multiple factors (World Health Organization, 2003). Indeed, a study that compiled information on drug data sources in Latin American (LA) found 124 potential data sources for DUR from nine countries, being Brazil and Argentine the countries with the major number of data sources. Unfortunately, accessibility to those databases is limited and only aggregate-level data was available, given this situation, the DUR implementation is scarce in LA (Lopes et al., 2022).
Additionally, in many LA countries, the lack of identification of data sources with information about medicines use and the decentralized healthcare systems are the main barriers to conduct DUR (Sales et al., 2020). Peru has a significantly fragmented healthcare system divided into five entities: the Ministry of Health (MINSA) which covers almost the majority of the population (60%), the Social Security of Health (ESSALUD) covering 30%, and the Armed Forces (FFAA), Peruvian National Police (PNP), and the private sector that cover the remaining part of the population (Arroyo et al., 2011) (Figure 1). Each entity has, therefore, its own information, making it difficult to implement DUR at a national level. Consequently, the General Directorate of Medicines Supplies and Drugs (DIGEMID) of the MINSA, which is responsible for national drug policy, has no access to data concerning drug utilization which limits the improvement of making decisions based on real-world evidence.
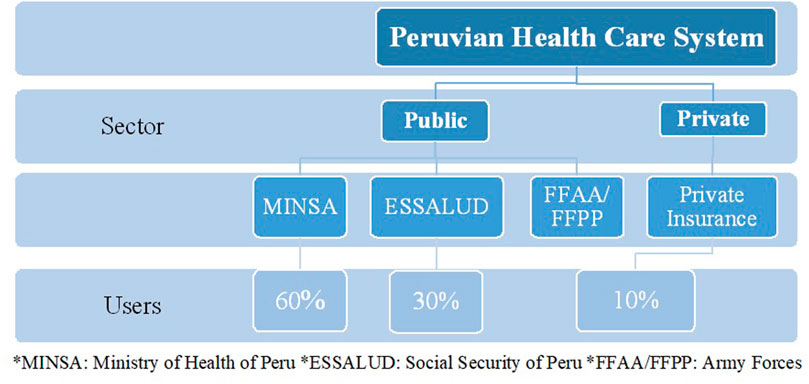
FIGURE 1. Peruvian Healthcare System Structure. *MINSA, Ministry of Health of Peru; *ESSALUD, Social Security of Peru; *FFAA/FFPP, Army Forces.
In Peru, pharmaceutical products and medical devices are regulated by the DIGEMID based on technical information on efficacy, safety, and quality. Once products are in the market, purchases of medicines are centralized and distributed at the national level and also can be acquired locally by regional authorities (Coronado and Espinoza, 2014). The government assures price regulation for medicines only in the public sector. In addition, Peru, as part of the National Drug Policy, has its own National List of Essential Drugs (PNUME) based on the model list provided by the World Health Organization (WHO). PNUME is managed by MINSA with the aiming to cover the priority healthcare needs of the population (Petitorio, 2020). Recently, the introduction of health technology assessment (HTA) and the development of evidence-based clinical guidelines in the Peruvian public sector are improving drug policies and access to medicines. Ever since ESSALUD deployed a decision-making process based on HTA to cover new medications or medical devices, the efficient use of resources and the transparency of the approval process have been enhanced. Indeed, the average of money invested to better the patient’s access to new technologies has decreased from S/133, 270.00 in 2011 to S/. 47,779.00 in 2019 per capita (Peralta et al., 2022). However, the increase in pharmaceutical expenditure and the knowledge on how medicines are prescribed and used across insurance schemes through DUR are limited.
Identifying drug data sources is relevant to perform DUR which in turn, may contribute to public health from medical, social, and economic perspectives (Sacristán and Soto, 1994; Wettermark et al., 2016; Peralta et al., 2022). Some initiatives to map drug databases have been developed, especially in Europe, to help stakeholders make informed decisions to promote the rational use of medicines (Eriksson and Ibáñez, 2016; ENCePP, 2022). To our knowledge, no mapping has been conducted until now to describe the existence of data sources for DUR in Peru, where the demand for medications is increasing. Therefore, the aim of this study is to map and describe data sources accessible for Drug Utilization Research in Peru by conducting a review of public Peruvian Health Institutions and scientific databases. We believe this manuscript might help inform Peruvian healthcare policy and enhance drug policies worldwide.
Methods
The methods were based on the DASDUR-LATAM Study which was sponsored by ISPE (Lopes et al., 2022). DASDUR-LATAM is a cross-sectional comparison study that aimed to compile an inventory of available national drug data sources from nine countries.
Design
This was a cross-sectional study in which an expert network of health national data providers and academic specialists on DUR created an inventory of data sources for DUR in Peru.
Type of data sources (eligibility criteria)
We defined a data source for DUR as a database with information on medicines including volume, price, dose, or safety information (for example, notification of adverse drug reactions). Included drug data sources of large jurisdictions or from organizations multi-sited that serve a large population, supported by governmental organizations. Considered jurisdictions were at the national and/or regional level. We did not include in this inventory data sources from health insurance companies, sickness funds, and private organizations (e.g., IQVIA) because payment to access them is required. Data sources containing a mix of data from the public and private health sectors were included.
Search strategy
First, we carried out a search of data sources providing information on access, use, and safety of drugs on the websites of Peruvian institutions such as the General Directorate of Medicines Supplies and Drugs (DIGEMID) and the National Superintendence of Health of Peru (SUSALUD) both from the Ministry of Health of Peru (MINSA) and Peruvian Social Security (ESSALUD), as well as academic institutional repositories from the main Peruvian universities.
Second, we performed a scientific literature review on PubMed, SciELO, and BVS to identify studies that used such data sources in Peru. We also searched for gray literature (thesis, unpublished studies, abstracts from conferences and meetings), and used a citation manager to import references (see Supplementary Appendix SA). We used the following combined keywords “drug data sources,” “drug utilization,” “pharmacovigilance,” and “Peru.” There was no limitation either by type of study or language. Both searches were conducted in July 2019 and updated in February 2020.
Screening process
Working in pairs and independently two researchers (YR, HG), conducted a screening and reviewed the potentially eligible data sources. The divergences in the usefulness of each database for DUR were discussed during the monthly meeting with the coordinator of the project (LCL) for consensus.
Data extraction and analysis
Once eligible data sources were selected from Peruvian health institutions’ websites and studies using data sources were retrieved, two reviewers independently extracted the following information:
i. Data provider custodian, steward;
ii. Accessibility (publicly available and convenient; restricted pre-authorized protocol only access; access limited to or dependent on country-specific legislation; available only to researchers working at each institution; the process for obtaining data is not clear without general regulation; not accessible anyway) at which level the data was generated (whole-sellers, pharmacy, physician, others);
iii. Healthcare setting (hospital, ambulatory care, both);
iv. Years coverage;
v. Geographic granularity (national, regional, municipal, organization multi-sited, other);
vi. Type of data (aggregate or individual level);
vii. Sector data source (public, private, or both).
In some cases, we contacted data sources to ensure accuracy and improve completeness. We analyzed data collected descriptively and summarized it in tables. In case of disagreement, the coordinating team (LCL, ME, MS) was consulted for consensus.
Results
Drug database selection
We identified a total of seven drug data sources from Peruvian Health institutions for the qualitative analysis (Figure 2).
- Pharmacovigilance data base of the National Center of Pharmacovigilance and Technovigilance (CENAFyT)
- Data Base of ADR of the Reference Center of Pharmacovigilance and Technovigilance of EsSalud (CRI-ESSALUD);
- Hospital Management System of EsSalud (SGSS/ESSI);
- National Socioeconomic Survey of Access to Health (ENSSA)
- National Survey on User Satisfaction of Health Services (ENSUSALUD) (Su perintendencia Nacional de Salud, 2016);
- Consumption of Medications and Medical Devices (ICI) (Ministerio de Salud, 2022)
- Distribution of Medications and Medical Devices (IDI) (Ministerio de Salud, 2022)
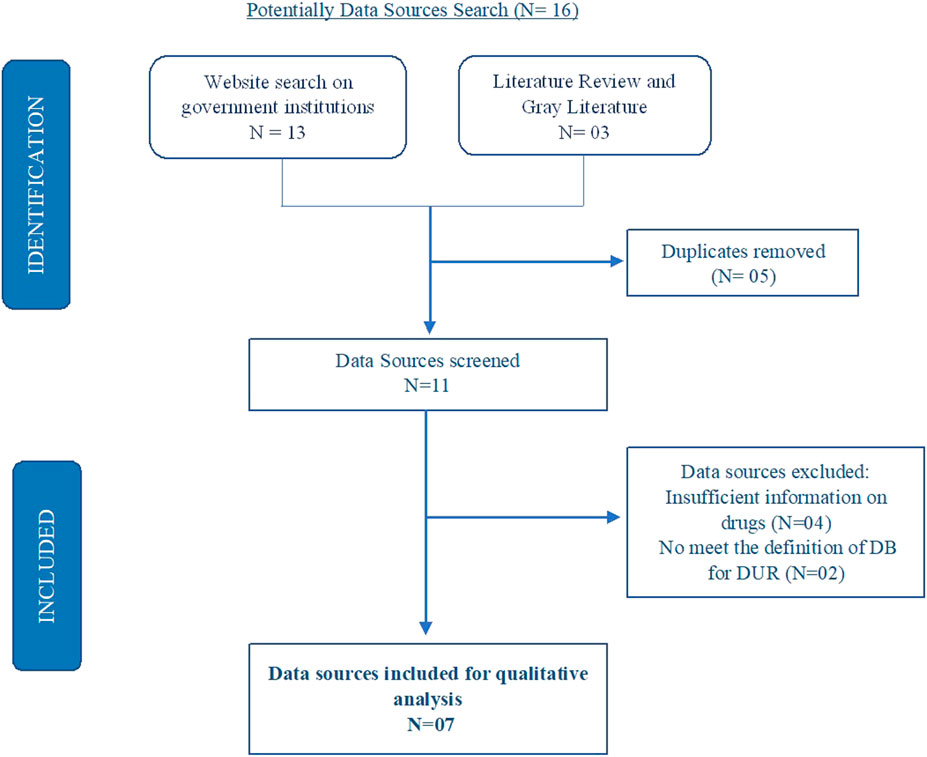
FIGURE 2. Drug data sources search flowchart. Potentially Data Sources Search (N = 16).
From the systematic search performed in PubMed, SciELO and BVS, we initially identified a total of 305 studies and after screening the full text manually, we found five studies, four used the National Survey on User Satisfaction of Health Services (ENSUSALUD 2015–2017) and the other the Drug Integrated System (SISMED) of the Ministry of Health of Peru (Supplementary Figure S1).
The drug data sources identified from the literature review on PubMed, SciELO, and BVS were ENSUSALUD and ICI. Five studies were conducted using these databases (Hodgkin et al., 2014; Urrunaga-Pastor et al., 2015; Mezones-Holguín et al., 2016; Hernández-Vásquez et al., 2018; Rojas-Adrianzén et al., 2018). From the gray literature search, we found CENAFyT. This data source was used in a bachelor thesis that aimed to assess the quality of ADR reporting from marketing authorization holders (MAH) using VIGIGRADE (Condori Quito and Hernandez Loli DM de los, 2018).
Drug data sources characteristics
CENAFyT and CRI-ESSALUD contained information on ADR at the individual level. SGSS/ESSI has data on prescriptions and pharmacy dispensation from medical centers, ENSSA and ENSUSALUD provide data from surveys addressed to users at the aggregate level. Finally, ICI and IDI, drug data sources that comprised the Integrated Supply System for Medicines and Medical-Surgical (SISMED), display data on drug consumption and distribution (see Tables 1, 2).
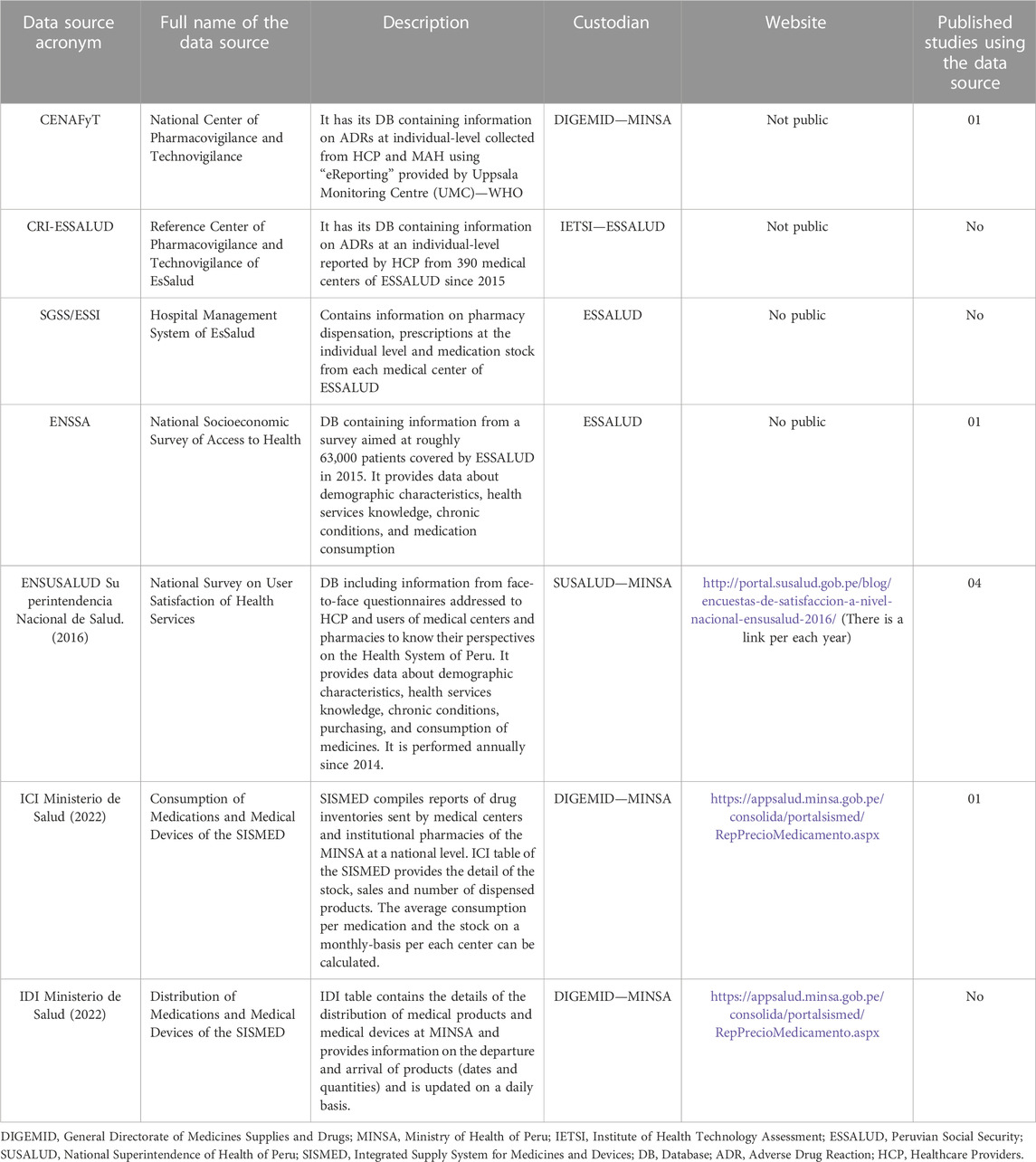
TABLE 1. General description of data sources for DUR in Peru.
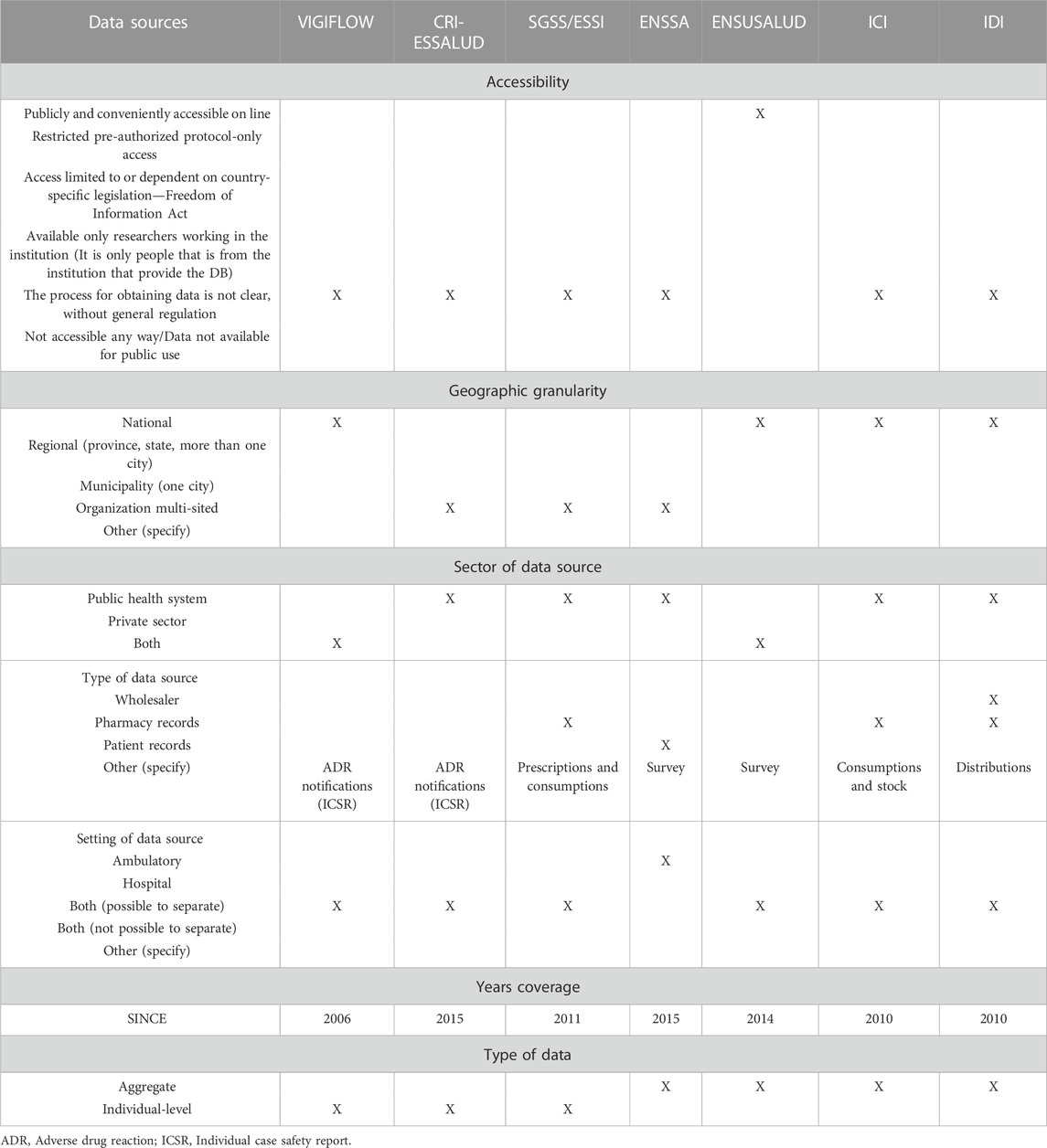
TABLE 2. Characteristics of data sources identified for DUR in Peru.
Regarding the institutional origin, CENAFyT, ENSUSALUD, ICI, and IDI were found on the MINSA websites. It is important to highlight that CENAFyT is a division of the DIGEMID of the MINSA. On the other hand, SGSS/ESSI, ENSSA, and CRI-ESSALUD drug data sources belong to ESSALUD.
In terms of accessibility, ENSUSALUD was the only data source publicly available. The MINSA through SUSALUD has included questionnaires denominated ENSUSALUD from 2014. These surveys are applied annually to health services users (healthcare providers and patients) to assess the level of satisfaction. The process for obtaining data from these data sources was not clear for the other drug data sources.
CENAFyT of the DIGEMID and ENSUSALUD were the only data sources with national information from the public and private sectors. DIGEMID as a regulatory agency is responsible to conduct the Peruvian System of Pharmacovigilance through the collection of ADRs notification not only from MINSA, ESSALUD, FFAA, and PNP, but also from the pharmaceutical industry. Likewise, ENSUSALUD is conducted annually to collect information on private sector users also (pharmaceutical companies and private pharmacies and drugstores).
CRI-ESSALUD, SGSS/ESSI, and ENSSA were multi-sited organizations. CRI-ESSALUD has national granularity but it only collects individual case safety reports from healthcare providers (medical doctors, pharmacists, nurses, and dentists) working at 400 medical centers of ESSALUD. Furthermore, both data sources, ICI and IDI, included important drug information at the national level but only from healthcare institutions of the MINSA.
Regarding the setting, CENAFyT, CRI-ESSALUD, SGSS/ESSI, ENSSA, ICI, and IDI incorporate information on hospital and ambulatory care. Most of the drug data sources had less than 10 years of coverage with exception of CENAFyT.
Discussion
In this study, we identified seven data sources that potentially might be useful to perform DUR. To our knowledge, this is the first mapping to identify data sources for DUR in Peru. These data sources included institutions under the control of the Government (MINSA and ESSALUD) and constitute information on ADR, prescription, dispensing, consumption, and distribution of medication. However, they have limited available data for DUR and many restrictions to access. The National Survey on User Satisfaction of Health Services (ENSUSALUD) was the only data source publicly available. ENSUSALUD is carried out annually by SUSALUD of MINSA since 2014 to assess the performance of the Healthcare System in Peru. This survey targets healthcare providers and users (e.g., patients), and data is freely available on the website of SUSALUD. This data source was the most frequently used for DUR purposes. As a result of the review, we found four studies that aimed to evaluate factors associated with self-medication and the purchase of medications without prescription (Urrunaga-Pastor et al., 2015; Mezones-Holguín et al., 2016; Hernández-Vásquez et al., 2018; Rojas-Adrianzén et al., 2018).
Regarding the existing drug data sources in Peru, four were at population-level information. Aggregate-level data, such as sales data, can play an important role to evaluate the impact of the pharmaceutical policies and interventions, however, individual-level data might enhance the insight of DUR because it is possible for researchers to visualize drug distribution (incidence, prevalence, drug duration and patterns of drug use over the time), assess temporal sequences, identify problems related to prescription (cascade prescriptions due to adverse drug reactions), etc. (Sacristán and Soto, 1994; Hallas, 2005). Unfortunately, we only identified three drug data sources at an individual-level with limited information on drug and patient characteristics. Since research on DUR is relevant to help inform healthcare policy, we believe that the government should deploy activities to increase the collection of drug utilization and clinical outcomes information at a patient-level, particularly in important settings such as hospitals, physician practices, pharmacies, and drugstores.
Few studies have been conducted to identify data sources available for DUR in LA. Justo et al. (2019) recently published an analysis to characterize and evaluate data sources and their uses in Argentina, Brazil, Colombia, and Chile. The authors identified a total of 407 unique databases, but the fragmentation of the healthcare system and the lack of resources and infrastructure are the major limitations to collecting interoperable data from many institutions and organizations (e.g., the government, providers, insurers, etc.). In addition, the authors describe that real-world evidence (RWE) is not used for health technology assessment (HTA) purposes, but mostly for pharmacovigilance (Justo et al., 2019). In 2014, Gregory (2014) performed a systematic review of the literature to examine administrative and clinical data for 10 major LA countries. They found Brazil, Mexico, Argentina, and Chile as having contributory information on data sources for RWE. However, given the low quality of databases, well-designed prospective studies should be conducted to improve RWE (Gregory, 2014).
The scarce number of drug data sources in Peru might be due to several factors. First, Peru currently has one of the lowest public spendings on health at 2.2% of Gross Domestic Product (GDP) among LA countries, and it is estimated that the public sector accounts for only 30% of the expenditure on medications. Second, the Healthcare System is fragmented which represents a limitation on the collection of data on access, distribution, and use of medicines. Third, administrative and care patient data coming from the four public health institutions (MINSA, ESSALUD, FFAA, and PNP) are not systematically recorded and the little information available is not integrated. Fourth, nearly 31% of patients have limited access to medicines although the Peruvian Government has deployed strategies to improve universal health coverage (Velásquez et al., 2016). Finally, decision-makers in Peru, as in many LA countries, maybe not be acquainted with the importance of DUR (Moscou et al., 2016). In consequence, Peruvian authorities are limited to making evidence-based decisions based on the real use, safety, effectiveness of pharmaceutical products already marketed which can have a negative impact on the cost of technology acquisition, reimbursement, efficient use of resources and the transparency of processes in clinical settings.
Using one or a few drug data sources may be weaker and hence is not actually representative of the real-world setting of drug use. Addressing a limited number of drug data sources in Peru requires the involvement of different institutions and organizations, mainly the MINSA and ESSALUD, and to be more economically resourced. Although public institutions like DIGEMID of the MINSA play key roles in collecting population-level drug data (distribution, consumption, and individual case safety reports); the major disadvantage is the fact that those data are not linked. Record linkage enables researchers to have more extensive prescriber and patient information to study drug utilization (Sacristán and Soto, 1994). In consequence, the main challenges are to integrate data across entities to obtain a robust data system and to have a standard process to extract information to best answer any DUR research. In addition, more work is needed to improve the quality, accessibility, and transparency of drug data sources particularly, for research purposes. Collaboration among academia, stakeholders, government and the private sector might be a good strategy to improve drug data sources and research.
There is an increased need to develop DUR in Peru due to the increased demand for medications (UgarteUbilluz, 2019). Currently, there is limited and incomplete information on drug use due to various factors, such as inadequate drug information, HCP with basic training on drugs, prescribing and dispensing activities influenced by socio-cultural patient demands and drug promotion, and the weakness of Peruvian drug policies (Paredes et al., 1996; Maldonado et al., 2002; Bustamante Robles et al., 2012; Florián-Castro, 2018). This situation derives from issues, such as over-prescription (Bustamante Robles et al., 2012), medication non-adherence, drug misuse in vulnerable populations [e.g., polypharmacy in the elderly, off-label use of medications in pregnancy, overuse of antibiotics in children (Ecker et al., 2011; Ecker et al., 2013; Fernandez-Arias et al., 2014; BojórquezGiraldo et al., 2017; Leyva-Moral et al., 2019; Rueda et al., 2019), self-medication (Hernández-Vásquez et al., 2018), purchasing medications without medical prescription, especially in poor regions with bounded access to public healthcare services in Peru (Urrunaga-Pastor et al., 2015; Hernández-Vásquez et al., 2018)], which lead to negative outcomes in patient’s health. Ideally, these issues should be characterized and quantified through DUR.
It is important to consider that developing DUR might provide essential information on the use of medications among Peruvians from social, cultural, and economic perspectives. Furthermore, DUR might be the gateway to better-informed decisions and provides an excellent opportunity to set priorities for healthcare budgets (Sales et al., 2020). These priorities might complement HTA through the improvement of the rational use of medications and promoting pharmaceutical policies for the wellbeing of patients.
Our study has some limitations. To begin with, details on special data sources description (e.g., number of variables and observations) could be missing since we did not access to the data sources themselves because special permission is required. In addition, we could not validate the quality of information described in each drug data source identified since we were only focused on the identification of their characteristics and their convenience for DUR in Peru. Finally, since the literature review performed in this study is not a systematic review, it is possible that our search did not identify all available evidence.
When it comes to the strengths, the major asset is that the description of the characteristics of most data sources was based on information provided directly by database owners and workers of the MINSA and ESSALUD. In addition, in spite of the limitations of the literature review performed besides the electronic searching on websites of Peruvian health institutions, we consider that this process enabled us to identify data sources used for secondary analysis in some studies.
Conclusion
Few data sources are available for DUR in Peru. There is an increased need to develop DUR in Peru due to the high demand for medications. The main challenges are to increase the collection of drug utilization and clinical outcomes information at a patient-level, integrate data across institutions, and to have a standard process to extract information. In addition, more work needs to be done to improve the accessibility, quality, and transparency of drug data sources particularly, for research purposes. Collaboration between academia, the private sector, the government, international institutions, and other stakeholders might be a good strategy to improve drug utilization research in Peru. DUR results might be important not only to implement strategies to deliver rational drug policy but also to provide information on the efficiency of drug use, which may be useful to set priorities for financial healthcare budgets. In addition, the availability of robust drug data sources enables researchers to use data to perform cross-national comparative drug utilization research and to enhance drug policies worldwide.
Data availability statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Author contributions
LL and LR-T conceived the study. LR-T and HG carried out the data collection, analysis, and interpretation. LR-T, HG, MS, and LL participated in drafting the manuscript. LL, MS, ME, and LFL did a critical revision of the article. All authors read and approved the final manuscript.
Funding
International Society for Pharmacoepidemiology (ISPE) board has fully funded the publication of this manuscript through the strategic initiative “Making pharmacoepidemiology LATAM data accessible to all” which includes this research paper.
Conflict of interest
MS was employed by Daiichi Sankyo.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.1047946/full#supplementary-material
References
Ahmed, B., Nanji, K., Mujeeb, R., and Patel, M. J. (2014). Effects of polypharmacy on adverse drug reactions among geriatric outpatients at a tertiary care hospital in karachi: A prospective cohort study. PLOS ONE. 17 noviembre 9 (11), e112133. doi:10.1371/journal.pone.0112133
Arroyo, J., Hartz, J., and Lau, M. (2011). “Recursos humanos en salud al 2011: Evidencias para la toma de decisiones,” in Recur hum en Salud Al 2011 evid para toma decis (Brazil, BR, USA: Pesquisa), 116.
Bergman, U. (2006). The history of the drug utilization research group in Europe. Pharmacoepidemiol Drug Saf. febrero15 (2), 95–98. doi:10.1002/pds.1171
Berreni, A., Montastruc, F., Bondon-Guitton, E., Rousseau, V., Abadie, D., Durrieu, G., et al. (2015). Adverse drug reactions to self-medication: A study in a pharmacovigilance database. Fundam Clin Pharmacol. Oct. 29 (5), 517–520. doi:10.1111/fcp.12140
Bojórquez Giraldo, E., Arévalo Alván, A., Castro Cisneros, K., Ludowieg Casinelli, L., and Orihuela Fernández, S. (2017). Patrones de prescripción de psicofármacos en pacientes con esquizofrenia y trastornos relacionados internados en el Hospital Víctor Larco Herrera. An Fac Med. octubre de 78 (4), 386–392. doi:10.15381/anales.v78i4.14258
Bustamante Robles, K. Y., Ticse Aguirre, R., Cánepa Rondo, I. F., Costta Herrera, C. G., Vasquez Kunze, S., Soto Arquiñigo, L., et al. (2012). Frequency of proton pump inhibitor prescription based in clinical practice guidelines in hospitalized patients in two academic hospitals in Lima, Peru. marzo 32 (1), 44–49.
Condori Quito, Y. C., and Hernandez Loli Dm de los, A. (2018). Calidad de las notificaciones de sospechas de RAMs reportadas por empresas farmacéuticas al Centro Nacional de Farmacovigilancia y Tecnovigilancia de la DIGEMID. Lima, Peru: Universidad Nacional Mayor de San Marcos.
Coronado, J., and Espinoza, J. (2014). Competitions issues in the distribution of pharmaceutical. http://www.oecd.org/officialdocuments/publicdisplaydocumentpdf/?cote=DAF/COMP/GF/WD%282014%2922&docLanguage=En.
Ecker, L., Ochoa, T. J., Vargas, M., Del Valle, L. J., and Ruiz, J. (2013). Preferences of antibiotic use in children less than five in physicians working health centers of primary level in peri-urban areas of Lima, Peru. Rev Peru Exp Salud Publica. abril30 (2), 181–189.
Ecker, L., Olarte, L., Vilchez, G., Ochoa, T. J., Amemiya, I., Gil, A. I., et al. (2011). Physicians’ responsibility for antibiotic use in infants from periurban Lima, Peru. Rev Panam Salud Publica Pan Am Publicealth. diciembre30 (6), 574–579.
EncePP, (2022). European network of centres for pharmacoepidemiology and pharmacovigilance. http://www.encepp.eu/.
Eriksson, I., and Ibáñez, L. (2016). “Secondary data sources for drug utilization research,” in Drug utilization research (Hoboken, NJ, USA: John Wiley & Sons), 39–48. doi:10.1002/9781118949740.ch4
Fernandez-Arias, M., Acuna-Villaorduna, A., Miranda, J. J., Diez-Canseco, F., and Malaga, G. (2014). Adherence to pharmacotherapy and medication-related beliefs in patients with hypertension in Lima, Peru. PloS One 9 (12), e112875. doi:10.1371/journal.pone.0112875
Florián-Castro, R. O. (2018). Perceptions on pharmaceutical promotion and medicine prescription of physicians in Lima, Peru 2016. Rev Peru Exp Salud Publica. diciembre35 (4), 710–711. doi:10.17843/rpmesp.2018.354.3718
Formica, D., Sultana, J., Cutroneo, P. M., Lucchesi, S., Angelica, R., Crisafulli, S., et al. (2018). The economic burden of preventable adverse drug reactions: A systematic review of observational studies. Expert Opin Drug Saf. 3 julio17 (7), 681–695. doi:10.1080/14740338.2018.1491547
Gregory, V. (2014). Real world research in Latin America: Opportunities sources and barriers (PRM 43). Value Health 17 (3).
Hallas, J. (2005). Drug utilization statistics for individual-level pharmacy dispensing data. Pharmacoepidemiol Drug Saf. julio14 (7), 455–463. doi:10.1002/pds.1063
Hernández-Vásquez, A., Alarcon-Ruiz, C. A., Díaz-Seijas, D., Magallanes-Quevedo, L., and Rosselli, D. (2018). Purchase of medications without prescription in Peru: A cross-sectional population-based study. F1000Research 7.
Hodgkin, D., Piazza, M., Crisante, M., Gallo, C., and Fiestas, F. (2014). Availability of psychotropic medications in health care facilities of the Ministry of Health of Peru, 2011. Oct.31 (4), 660–668.
Justo, N., Espinoza, M. A., Ratto, B., Nicholson, M., Rosselli, D., Ovcinnikova, O., et al. (2019). Real-world evidence in healthcare decision making: Global trends and case studies from Latin America. Value Health J. Int. Soc. Pharmacoeconomics Outcomes Res. 22 (6), 739–749. doi:10.1016/j.jval.2019.01.014
Leyva-Moral, J. M., Loayza-Enriquez, B. K., Palmieri, P. A., Guevara-Vasquez, G. M., Elias-Bravo, U. E., Edwards, J. E., et al. (2019). Adherence to antiretroviral therapy and the associated factors among people living with HIV/AIDS in northern Peru: A cross-sectional study. AIDS Res. Ther. 2816 (1), 22. doi:10.1186/s12981-019-0238-y de
Linnér, L., Eriksson, I., Persson, M., and Wettermark, B. (2020). Forecasting drug utilization and expenditure: Ten years of experience in stockholm. BMC Health Serv Res. 11 mayo 20 (1), 410. doi:10.1186/s12913-020-05170-0
Lopes, L. C., Salas, M., Osorio-de-Castro, C. G. S., Leal, L. F., Doubova, S. V., Cañás, M., et al. (2022). Data sources for drug utilization research in Latin American countries – a cross-national study: DASDUR-LATAM study. Pharmacoepidemiol. Drug Saf.31 3 doi:10.1002/pds.5404
Maldonado, C. F., Llanos-Zavalaga, F., and Mayca, P. J. (2002). Uso y Prescripción de Medicamentos Antimicrobianos en el Hospital de Apoyo de la Merced - perú. Rev Peru Exp Salud Publica. Oct.19 (4), 181–185.
Massele, A., Godman, B., Adorka, M., Fadare, J., Gray, A., Lubbe, M., et al. (2015). Initiative to progress research on medicine utilization in africa: Formation of the medicines utilization research in africa group. Expert Rev Pharmacoecon Outcomes Res. 4 julio 15 (4), 607–610. doi:10.1586/14737167.2015.1065735
Mezones-Holguín, E., Solis-Cóndor, R., Benites-Zapata, V. A., Garnica-Pinazo, G., Marquez-Bobadilla, E., Tantaleán-Del-Águila, M., et al. (2016). Diferencias institucionales en el insuficiente acceso efectivo a medicamentos prescritos en instituciones prestadoras de servicios de salud en Perú: Análisis de la Encuesta Nacional de Satisfacción de Usuarios de los Servicios de Salud (ENSUSALUD 2014). Rev Peru Exp Salud Publica. junio 33 (2), 205–214. doi:10.17843/rpmesp.2016.332.2197
Ministerio de Salud (2022). MINSA-Consulta sobre disponibilidad de Medicamentos. https://appsalud.minsa.gob.pe/consolida/portalsismed/RepPrecioMedicamento.aspx.
Monica (2020). RAND drug policy research center. https://www.rand.org/well-being/justice-policy/centers/dprc.html.
Moscou, K., Kohler, J. C., and MaGahan, A. (2016). Governance and pharmacovigilance in Brazil: A scoping review. J. Pharm. Policy Pract. 9, 3. doi:10.1186/s40545-016-0053-y
Ontario Ministry of Health (2020). Drug policy & research in Ontario. https://odprn.ca/.
Paredes, P., de la Peña, M., Flores-Guerra, E., Diaz, J., and Trostle, J. (1996). Factors influencing physicians’ prescribing behaviour in the treatment of childhood diarrhoea: Knowledge may not be the clue. Soc. Sci. Med. 42 (8), 1141–1153. doi:10.1016/0277-9536(95)00387-8
Peralta, V., Castro-Reyes, M. M., Pimentel-Álvarez, P., Fiestas, F., and Dongo, V. (2022). Incorporación de la evaluación de tecnologías sanitarias en la toma de decisiones en el sistema de servicios de salud del seguro social del perú: La experiencia del IETSI. Rev. Cuerpo Méd Hosp. Nac. Almanzor Aguinaga Asenjo 15 (1).
Petitorio, D. (2020). Nacional único de Medicamentos esenciales. http://www.digemid.minsa.gob.pe/Main.asp?Seccion=686.
Rajan, R., Peter, S. M., Kurian, V. M., Ansari, R., Pawar, S., and Kalrao, V. (2019). The practice of off label prescribing and associated adverse drug reactions in pediatric inpatients in a tertiary care hospital in India. J. Pharm. Health Serv. Res. 10 (1), 29–34. doi:10.1111/jphs.12286
Rojas-Adrianzén, C., Pereyra-Elías, R., and Mayta-Tristán, P. (2018). [Prevalence and factors associated with over-the-counter antimicrobial purchases, Peru 2016]. Rev Peru med exp salud publica. septiembre 35 (3), 400–408.
Rueda, M. S., Calderon-Anyosa, R., Gonzales, J., Turin, C. G., Zea-Vera, A., Zegarra, J., et al. (2019). Antibiotic overuse in premature low birth weight infants in a developing country. Pediatr. Infect. Dis. J. 38 (3), 302–307. doi:10.1097/INF.0000000000002055
Sabaté, M., Pacheco, J. F., Ballarín, E., Ferrer, P., Petri, H., Hasford, J., et al. (2014). A compilation of research working groups on drug utilisation across Europe. BMC Res Notes. 13 marzo 7 (1), 143. doi:10.1186/1756-0500-7-143
Sacristán, J. A., and Soto, J. (1994). Drug utilisation studies as tools in health economics. PharmacoEconomics. abril 5 (4), 299–312. doi:10.2165/00019053-199405040-00005
Sales, M., Lopes, L. C., Godman, B., Truter, I., Hartzema, A. G., Wettermark, B., et al. (2020). Challenges facing drug utilization research in the Latin American region. https://pureportal.strath.ac.uk/en/publications/challenges-facing-drug-utilization-research-in-the-latin-american.
Superintendencia Nacional de Salud (2016). MINSA-Encuestas de satisfacción a nivel nacional (ENSUSALUD 2016). http://portal.susalud.gob.pe/blog/encuestas-de-satisfaccion-a-nivel-nacional-ensusalud-2016/.
Ugarte Ubilluz, O. (2019). Estrategias para mejorar el acceso a medicamentos en el Perú. An Fac Med. enero de 80 (1), 104–108. doi:10.15381/anales.v80i1.15878
Urrunaga-Pastor, D., Benites-Zapata, V. A., and Mezones-Holguín, E. (2015). Factors associated with self-medication in users of drugstores and pharmacies in Peru: An analysis of the national survey on user satisfaction of health services, ENSUSALUD 2015. ENSUSALUDF1000Research 8, 23. doi:10.12688/f1000research.17578.2
Velásquez, A., Suarez, D., and Nepo-Linares, E. (2016). Health sector reform in Peru: Law, governance, universal coverage, and responses to health risks. Rev Peru Exp Salud Publica. septiembre 33 (3), 546–555. doi:10.17843/rpmesp.2016.333.2338
Wettermark, B., Elseviers, M., Almarsdottir, A. B., Andersen, M., Benko, R., Bennie, M., et al. (2016). Introduction to drug utilization research. Drug Util. Res. methods Appl., 1–12.
Keywords: Peru (fuente), drug utilisation research, data sources, Pharmacoepidemiology, Latin America
Citation: Rodríguez-Tanta LY, Garavito Farro H, Freitas Leal L, Salas M, Elseviers MM and Lopes LC (2023) Drug utilization research in Peru: Is real-world data available?. Front. Pharmacol. 13:1047946. doi: 10.3389/fphar.2022.1047946
Received: 19 September 2022; Accepted: 28 December 2022;
Published: 17 January 2023.
Edited by:
Elisabetta Poluzzi, University of Bologna, ItalyReviewed by:
Luis Eduardo Pino, Fundación Santa Fe de Bogotá, ColombiaIppazio Cosimo Antonazzo, University of Milan-Bicocca, Italy
Copyright © 2023 Rodríguez-Tanta, Garavito Farro, Freitas Leal, Salas, Elseviers and Lopes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: L. Yesenia Rodríguez-Tanta, yesi.psb26@gmail.com; Luciane Cruz Lopes, luslopesbr@gmail.com