{kind=link}

94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol., 17 November 2022
Sec. Drugs Outcomes Research and Policies
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.1042418
This article is part of the Research TopicEvidence for Assessing Drug Safety and Drug Use in Older People - Volume IIView all 11 articles
 Ikhwan Yuda Kusuma1,2
Ikhwan Yuda Kusuma1,2 Maria Matuz1,3
Maria Matuz1,3 Réka Bordás1Maria Juhasz Haverinen4Muh. Akbar Bahar1,5
Réka Bordás1Maria Juhasz Haverinen4Muh. Akbar Bahar1,5 Edit Hajdu6Ádám Visnyovszki6Roxána Ruzsa1Péter Doró1Zsófi Engi1Dezső Csupor1,7
Edit Hajdu6Ádám Visnyovszki6Roxána Ruzsa1Péter Doró1Zsófi Engi1Dezső Csupor1,7 Ria Benko1,3,8*
Ria Benko1,3,8*Background: The elderly use antibiotics frequently due to their increasing infection susceptibility. Given the high and increasing proportion of elderly in the population, their antibiotic use is substantial. Objective: This study aimed to compare antibiotic use in the elderly in the ambulatory care sector between Hungary and Sweden.
Methods: This retrospective, descriptive, cross-national, comparative study included antibacterial use data from the Hungarian National Health Insurance Fund and the Swedish eHealth Agency. Antibiotic use (anatomical therapeutical chemical: J01) was expressed as the number of prescriptions/1000 inhabitants/year or month and was further stratified by age and sex.
Results: Antibiotic exposure was higher in the Hungarian elderly population (649.8 prescriptions/1000 inhabitants/year) compared to its Swedish counterparts (545.0 prescriptions/1000 inhabitants/year). Hungary had a similar scale of antibacterial exposure across all elderly age subgroups, with different trends in males and females, while Sweden had a stepwise increase in antibiotic exposure by age in both sexes. The seasonal fluctuation was high in Hungary and reached a peak of 80.7 prescriptions/1000 inhabitants/month in January 2017, while even antibiotic use was detected throughout the year in Sweden. The pattern of antibiotic use in the elderly considerably differed between the two countries. Penicillin and beta-lactamase combinations, such as co-amoxiclav, were more frequently used in Hungary than in Sweden (19.08% vs 1.83% of corresponding total ambulatory antibiotic use). Likewise, quinolones were more commonly used in Hungary than in Sweden (34.53% vs. 9.98). The elderly in Sweden were mostly prescribed narrow spectra penicillins (26.71% vs. 0.29% in Hungary).
Conclusion: This cross-national comparison revealed important differences in all aspects of antibiotic use in the elderly between the two countries. The identical scale and pattern of antibiotic use cannot be anticipated due to the poorer health status of the Hungarian elderly population. However, the substantial differences indicate some room for improvement in the antibiotic prescription for the Hungarian elderly.
Antimicrobial resistance (AMR) implies a threat to global human health. Contributing factors of AMR include antibiotic overuse and misuse in hospital and ambulatory care settings (Ventola, 2015). Current demographic projections show an increasing elderly population in Europe. In 2019, proportion of the elderly population (≥65 years) proportion in Europe, Hungary, and Sweden was 31.4%, 29.3%, and 31.9%, respectively, of the total adult active (15–64 years) population, which is projected as 39.1%, 33.7%, and 34.4% by 2030, respectively (Eurostat, 2019).
The elderly population is at increased risk of many infectious diseases due to progressive functional decline of the immune system, commonly referred to as immunosenescence (Feehan et al., 2021). Age-related immune system changes affect innate and adaptive immune responses (Feehan et al., 2021). Research data on outpatient antibiotic use in the elderly remained scarce despite the growing population size of the elderly in Europe, and most studies focus on long-term care facilities (Raban et al., 2021). Comprehensive country-wide data on antibiotic use in the elderly in ambulatory care have only been published for a limited number of countries, including Denmark (Jensen et al., 2021), Norway (Blix et al., 2007), and the United States (Kabbani et al., 2018). Moreover, no cross-national comparison research has compared antibiotic use for the elderly in ambulatory care between European countries. Therefore, this study aimed to compare antibiotic use in the elderly in the ambulatory care sector in Hungary and Sweden.
This retrospective and descriptive cross-national comparative study collected data on antibacterial prescriptions dispensed at community pharmacies in Hungary and Sweden in 2017. Antibacterials were classified according to the anatomical therapeutical chemical (ATC) classification system defined by the World Health Organization (WHO), version 2022 (WHO, 2020). The use of systemic antibacterials (ATC: J01) was measured as prescriptions/1000 inhabitants/year or month. The elderly population (aged >65 years) of Hungary and Sweden in 2017 served as study populations for this study, including 1,828,226 elderly in Hungary and 1,976,857 elderly in Sweden (data derived from Eurostat). The two populations were further stratified into subgroups according to age (65–69 years, 70–74 years, 75–79 years, 80–85 years, and >85 years) and sex. Seasonal variation of antibiotic consumption was also assessed.
Data on antibacterial use was obtained from the Hungarian National Health Insurance Fund and the Swedish eHealth Agency. Both the Hungarian and the Swedish national health insurance systems cover almost 100% of the population of each country. The database in Hungary contains records of all dispensed and reimbursed ambulatory care prescriptions issued by general practitioners (GPs), specialists, and dentists to ambulatory care patients, nursing home residents, and patients visiting private practices (e.g., gynecologists, dentists). The drug coverage is approximately 95% because non-reimbursed antibiotics are not included in the database.
The Swedish database contains data on all dispensed antibiotic prescriptions providing 100% drug coverage. All medications prescribed to outpatients (irrespective of reimbursement status) that are issued by GPs, specialists, dentists, patients visiting private practices, or nursing homes are included in this database.
Excel was used for the statistical analyses, and visualization was done by the R package (version 4.1.2).
Ethical approval was not needed because aggregated data were collected for both countries.
The entire Hungarian population (approximately 9.8 million people) was dispensed 6,792,714 prescriptions of antibiotics in 2017, 17.5% of which were dispensed to the elderly. Concurrently, the entire Swedish population (approximately 10 million people) was dispensed 3,204,838 prescriptions of antibiotics, 33.6% of which were dispensed to the elderly. The antibiotic exposure was 649.8 prescriptions/1000 inhabitants/year in Hungarian and 545.0 prescriptions/1000 inhabitants/year in the Swedish elderly population.
Figure 1 presents the level of antibiotic exposure across the elderly age subgroups. The antibacterial exposure of the Hungarian elderly population was similar across all age subgroups, while a stepwise increase was observed in antibacterial exposure by age subgroups (an increase from 398 [65–69 years old] to 852 (>85 years old) prescriptions/1000 inhabitants/year) in the Swedish elderly population.
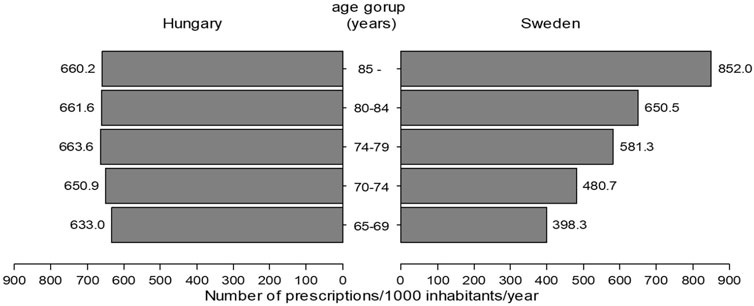
FIGURE 1. Antibacterial use in different elderly age subgroups in Hungary and Sweden (2017).
Table 1 shows the absolute and relative use of different antibacterial subgroups. Concerning the beta-lactam antibacterials, the penicillin group in Hungary was responsible for one-fifth of total ambulatory care antibiotic use in the elderly, and cephalosporins also had considerable use and share. In contrast, the penicillin group in Sweden was responsible for almost half of antibiotic use in the elderly, and marginal cephalosporin use was observed. The absolute and relative use of macrolides and fluoroquinolones were considerably higher in the Hungarian elderly population than in the Swedish counterparts, with an opposite pattern for tetracyclines and other antibacterials because their use was higher in the Swedish elderly (Table 1).
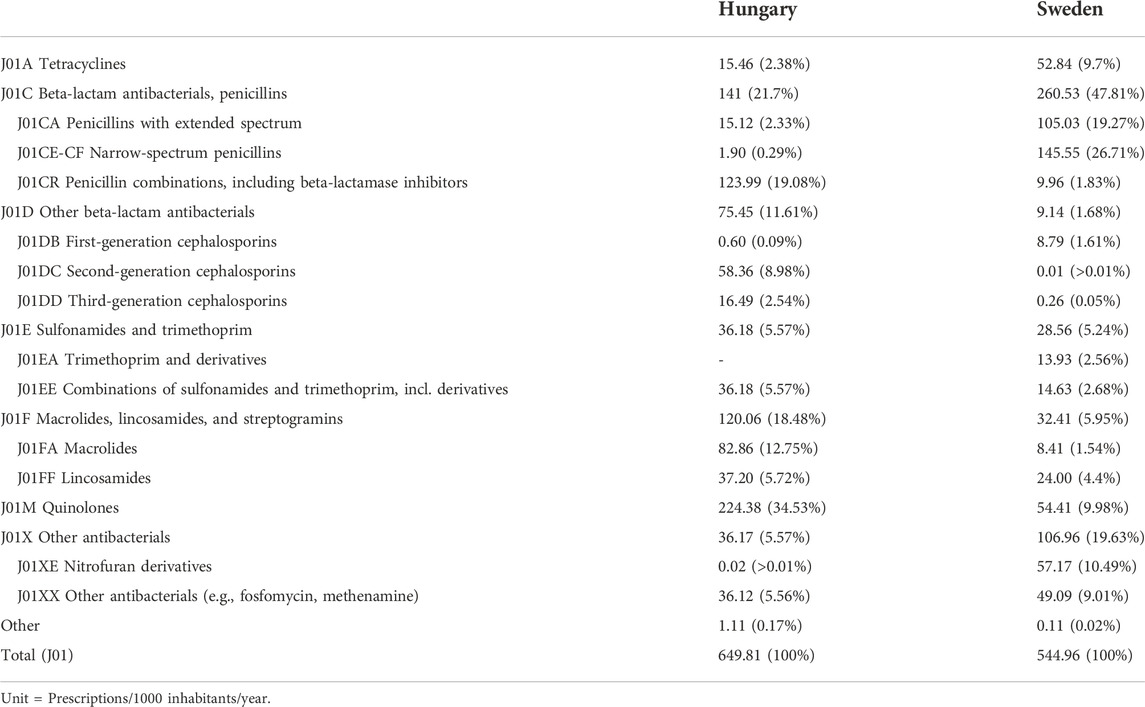
TABLE 1. Absolute and relative use of different antibiotic subgroups in the elderly population in Hungary and Sweden.
Table 2 shows the top ten list of antibacterials. Amoxicillin and clavulanic acid (co-amoxiclav) and two fluoroquinolones (levofloxacin and ciprofloxacin) covered almost half (46.6%) of the antibiotic use of the Hungarian elderly population in ambulatory care (Table 2), whereas 40% of all antibiotics used by the elderly population in ambulatory care constituted of the narrow-spectrum penicillin V, flucloxacillin, or pivmecillinam in Sweden. Nitrofurantoin use was almost absent in Hungary but constituted approximately 10.5% of the elderly antibiotic use in Sweden.
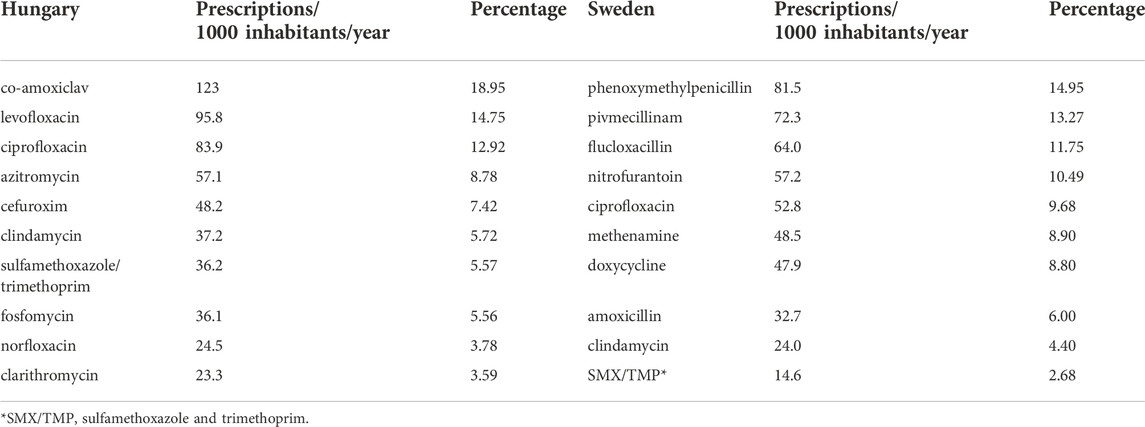
TABLE 2. The top ten list of antibacterials used in the elderly population in Hungary and Sweden (2017).
Overall, elderly females used more antibiotics than elderly males in Hungary and Sweden. Elderly females have been exposed to antibiotics at 668 prescriptions/1000 elderly females/year in Hungary, while elderly males at 620 prescriptions/1000 elderly males/year. Swedish elderly females were exposed to antibiotics at 618 prescriptions/1000 females/year, while elderly males at 460 prescriptions/1000 males/year in ambulatory care.
However, the antibiotic exposure of the two sexes of the elderly population showed opposite trends in the age subgroup analysis in Hungary (Figure 2). Antibiotic use decreased from 685 prescriptions/1000 females/year (60–65 years old) to 631 prescriptions/1000 females/year (>85 years old) in Hungary. Conversely, the scale of antibiotic use in the Hungarian elderly male increased by age [from 563 prescriptions/1000 males/year (65–69 years old) to 739 prescriptions/1000 males/year (>85 years old)]. Both elderly females and males in Sweden were exposed to increasing amounts of antibiotics by increasing age (Figures 1, 2) and in all elderly subgroups Swedish females were exposed to more antibiotics than Swedish males).
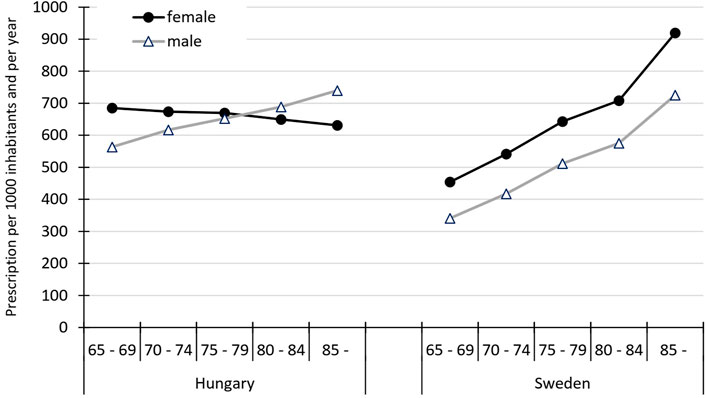
FIGURE 2. Sex-specific use of antibiotics in ambulatory care presented by age subgroups in the elderly population in Hungary and Sweden (2017).
Figure 3 shows the seasonal variation in antibiotic use in the elderly in Hungary and Sweden. The seasonal fluctuation was high in Hungary, reaching a peak of 80.7 prescriptions/1000 inhabitants/month in January. The lowest value in Hungary was 39.2 prescriptions/1000 inhabitants/month in July. Antibacterial use in the elderly population in Sweden was more equally distributed over the entire year, with a peak consumption of 49 prescriptions/1000 inhabitants/month in March and a nadir of 42 prescriptions/1000 inhabitants/month in April.
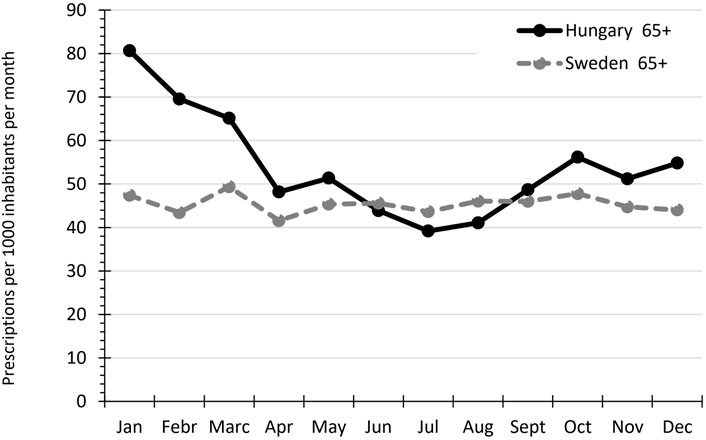
FIGURE 3. Seasonal variation of antibiotic use among the elderly population in Hungary and Sweden in 2017.
To the best of our knowledge, this is the first study to report on Hungarian data on antibiotic use in the elderly and the first age-specific comparison of antibiotic use between two countries. Our results showed that antibiotic exposure was higher in the Hungarian elderly population than in their Swedish counterparts. Several factors might explain the higher antibiotic exposure in the Hungarian elderly than in Sweden.
Life expectancy is one of the most commonly used measures of the overall health of a population. The average life expectancy in 2017 for those aged 65 years was higher in Sweden than in Hungary (20.40 years vs 16.70 years), meaning that the Hungarian elderly has poorer health status (Eurostat, 2022).
Data on acute infection incidences are unavailable in the national statistics, but data on chronic disease prevalence, which can increase infection risk compared to the healthy population, is retrievable and can partly explain the observed differences between Hungary and Sweden. Two-thirds of Hungarians and nearly half of Swedish elderly (aged ≥65) reported at least one chronic disease (OECD, 2020). An epidemiological research revealed that patients with diabetes suffer infections more frequently than those without diabetes with consequent higher antibiotic use (Alves et al., 2012). The prevalence of diabetes in the elderly was higher in 2014 in Hungary than in Sweden (18.6% vs 12.6%) (Eurostat, 2014c). Obesity has also been an independent risk factor for infections in retrospective and prospective studies (Harpsøe et al., 2016). It increases the risk of pneumococcal respiratory tract infections (RTI), skin, gastrointestinal tract, and urinary tract infections (UTI) in elderly individuals (Frasca and McElhaney, 2019; Ghilotti et al., 2019). The prevalence of obesity in the elderly was much higher in 2014 in Hungary than in Sweden (26.5% vs 14.5%) (Eurostat, 2014a).
Smoking is one of the main risk factors for RTI, and the rate of daily smokers among the elderly was higher in Hungary (10.8%) than in Sweden (7.2 %), however this difference is much higher in the overall population (28 % vs. 7%, in 2020). In addition, smoking increases infection risk for digestive, reproductive, and other systems, which could lead to slightly higher antibiotic use in Hungarian elderly than in Swedish (Jiang et al., 2020). The annual number of hospital discharges due to malignant neoplasm of the respiratory tract (trachea, bronchus, and lung) in 2017 was also higher in Hungarian elderly (13,115 patients) than in its Swedish counterparts (4,966 patients) (Eurostat, 2017a). Prescribers may have a lower threshold for initiating antibiotic use in patients with cancer because antibiotics have positive side effects, such as cancer apoptosis promotion, cancer growth inhibition, and cancer metastasis prevention, e.g., lung cancer (Gao et al., 2020).
The population’s low health literacy and health-related knowledge can contribute to patients’ attitudes, beliefs, perceptions, and behaviors related to antibiotic use and can result in higher overall antibiotic use (Salm et al., 2018). The Eurobarometer public survey from 2018 revealed that the Hungarian public’s knowledge of antibiotics was worse than Swedish because only 37% of respondents gave entirely correct answers for all four antibiotic knowledge-related questions in Hungary, while 74% in Sweden (WHO, 2018).
The Eurostat statistics from 2017 revealed that the proportion of Hungarian elderly with >10 GP visits per year was 20.0% (65–74 years) and 29.5% (≥75 years), while this rate was only 3.7% (65–74 years) and 5.8% (≥75 years or more) in Sweden, suggesting that GP visits have a lower threshold in the Hungarian elderly population, which can contribute to higher antibiotic use (Tyrstrup et al., 2017). In addition, of the surveyed people in Hungary in the Eurobarometer study, 25% stated antibiotic prescription for sore throat and 17% for fever, while 9% for sore throat and 2% for fever in Sweden (European Commission, 2016). Data suggests that initiating antibiotic treatment is less judicious among Hungarian doctors although this data is based on patient recalls. Misleading advertising can be partly responsible for this. Over-the-counter dorithricin-containing lozenges, a local antibiotic, were heavily advertised on TV as a “throat saver antibiotic” in earlier years in Hungary, sending the incorrect message both to patients and doctors that antibiotics are required to relieve sore throats.
Physicians are primarily responsible for the decision to use antibiotics; thus, ensuring the optimal attitudes and knowledge that underlie their prescribing habits is a prerequisite for improving prescription quality (Gonzalez et al., 2015). A recent study revealed a 20% proportion of final-year medical students who want more education on prudent antibiotic use in Sweden, while >71% in Hungary. This means that medical students in Sweden feel prepared for prudent antibiotic prescription in much higher percentages than final-year students in Hungary (Dyar et al., 2018).
Moreover, antibiotic use is influenced by the existence of a national antibiotic policy (WHO, 2011). Sweden implemented the WHO recommendations for antibiotic stewardship in the form of a national strategic program to combat antibiotic resistance (Medical Products Agency and Strama, 2008), which is a continuously evolving collaboration that has been in place since 1995 (Mölstad et al., 2017). In contrast, a national antibiotic policy is not implemented with clear targets, responsibilities, and dedicated funding in Hungary (WHO, 2018).
Market forces and manufacturers’ marketing activity can also largely influence prescription practices in Hungary (WHO, 2018). The number of generics is very high in Hungary because they aim to reduce the price as much as possible (MacKenzie et al., 2006; Wouters et al., 2017), which might promote higher antibiotic use.
Overall, our study revealed that elderly females were prescribed more antibiotics than males in both countries. This can be partly explained by the sex differences in GPs visiting rates, wherein the rate of Hungarian elderly with >10 GP visits per year was 17.7% and 28.6% for males aged 65–74 years and >75 years, respectively, while 21.5% and 30.0% in the same age groups for females.
The sex gap in antibiotic prescription can partly be explained by consultation behavior differences (Smith et al., 2018). Males and females communicate differently with healthcare professionals, and prescribers may have gender biases that affect their willingness to prescribe antibiotics, resulting in higher antibiotic use in females (Smith et al., 2018). Males in the oldest two age groups were prescribed more antibiotics in Hungary due to the higher prevalence of risk factors among males, such as smoking and excessive alcohol consumption (WHO, 2018). The number of elderly male smokers is double compared to elderly female smokers aged 65–74 years and is five times higher in >75 years old in Hungary. Meanwhile, both sexes are equally smokers in each age subgroup in Sweden (Eurostat, 2014).
We found that the absolute and relative ambulatory care use of different antibacterial subgroups differed greatly in the elderly population between Hungary and Sweden. In Hungary, penicillin beta-lactamase combinations, such as co-amoxiclav were preferred, compared to Sweden where it was marginally used (19.08% vs 1.83%). The high use of co-amoxiclav has been estabilished in previous research as a drug of choice for RTI in Hungary (Matuz et al., 2013). Swedish policy recommends prescribing narrow-spectrum penicillins in ambulatory care for RTI (Aspevall et al., 2020) and our data indirectly indicate good adherence to this guideline. Surveillance report from the European Antimicrobial Resistance Surveillance Network (EARS-Net) showed that percentages of penicillin-resistant pneumococci (PRP) were similar in Hungary (6.9%) and Sweden (6.1%) (ECDC, 2017). Clavulanic acid use is not necessary for PRP because the resistance mechanism is not connected to the bacteria’s capability to produce beta-lactamase enzymes; hence, the addition of clavulanic acid to aminopenicillin will not help to overcome this resistance (Huttner et al., 2020). Co-amoxiclav is dominantly used compared to amoxicillin alone in Hungary because co-amoxiclav was placed on the market earlier than amoxicillin alone; thus, doctors became used to it (Benko, 2016). The use of broad-spectrum antibiotics, such as co-amoxiclav can compromise the host microbiome. Even short-term antibiotic exposure alters the gut microbiota and bacterial diversity recover after weeks or months after (Elvers et al., 2020). Disruption of the human microbiom by antibiotic use can lead to AMR infections and several diseases such as allergia, asthma, obesity or vitamin K deficiency (Langdon et al., 2016).
Quinolone was also more frequently used in Hungary than in Sweden (34.53% vs. 9.98% of total ambulatory use in the elderly, respectively). Previous research showed that fluoroquinolones were commonly used in ambulatory care to treat urinary tract infections and also RTIs in Hungary (Juhasz et al., 2013; Matuz et al., 2015; Benkő et al., 2020). Contrarily, pivmecillinam and nitrofurantoin were proved to be the first-line antibiotics to treat community-acquired UTIs in Sweden (Kornfält et al., 2019). The consequences of high fluoroquinolone use can be various. The Food and Drug Administration has placed a boxed warning on fluoroquinolone antibiotics which highlights older adults as being at an elevated risk of serious side effects, including tendon rupture, delirium, peripheral neuropathy, blood sugar disturbances, and aortic dissection (U.S. Food and Drug Administration, 2018). Fluoroquinolones also increase the risk of CDI (Clostridioides difficile infection) (Kabbani et al., 2018). Fluoroquinolone can cause QT interval prolongation and subsequently increase the risk of torsades de pointes (TdP) type arrhythmias. Given that heart failure and other risk factors such as uncorrected hypokalaemia, hypomagnesaemia might be present more frequently in the elderly, they are more vulnerable to potentially fatal cardiac arrhythmias such as TdP (Stahlmann & Lode, 2010). The 2017 annual report of the EARS-Net showed a difference in the percentage of fluoroquinolone-resistant Escherichia coli between Hungary and Sweden (30.6% vs 15.8%, respectively) that could be due to differences in the quinolone use in the two countries (ECDC, 2017).
The results of this comparison between the two countries are essential for Hungary since they need to optimize antibiotic use in the elderly to prevent serious adverse effects, more rapid resistance development, and higher costs (WHO, 2018). The availability of therapeutic guidelines might contribute to the observed pattern of antibiotic use in both countries. Up-to-date diagnostic and treatment guidelines have been unavailable for most community-associated infections for several years in Hungary, but Sweden continuously updates the guidelines every 3 years (Government Offices of Sweden, 2020).
The Hungarian antibiotic use in the elderly was very similar to Sweden in the summer months, but we detected substantially higher antibiotic use in the Hungarian elderly in the winter months. Seasonal fluctuation of outpatient antibiotic use in the general population across European countries has been previously described (Elseviers et al., 2007) and linked to an increased prevalence of RTI during the winter months, resulting in higher antibiotic prescription rates during this time (Elseviers et al., 2007).
Viral RTI and influenza-like syndromes were the most frequent infections in winter in both countries (Folkhälsomyndigheten, 2017; Kovács and Pakot, 2020); thus, antibiotics were possibly prescribed for self-limiting viral infections. The close correlation between viral respiratory infections, such as influenza and antibiotic prescriptions (Ryu et al., 2018), suggests that reducing the incidence of influenza through vaccination efforts in elderly people (Smetana et al., 2018) could help decrease the overprescription of antibiotics. The Eurostat in 2017 reported that Sweden has a higher vaccination rate against influenza in the population aged ≥65 years (49.8%) than in Hungary (26.8%) (Eurostat, 2017b), which might result in lower influenza illness rates in Sweden.
The strength of this study is the nearly 100% population and drug coverage in both countries. However, some limitations need to be acknowledged. Firstly, this research only uses 1-year data from the two countries, which precludes analysis of annual trends in antibiotic use. Secondly, data is not stratified by specific indications. However, these limitations do not affect our aims and conclusions. Finally, we have to highlight, that systemic antibiotic use (WHO: J01) includes methenamine (urinary disinfectant) with considerable use in Sweden (sixth place on the top list). Excluding methenamine would result in even higher differences in the antibiotic utilization of the two countries.
The scale and pattern of elderly ambulatory antibiotic use differed between Hungary and Sweden. Some of the observed differences could be explained by the different health statuses between the two populations; however, data suggest that interventions are needed to optimize antibiotic use in the elderly in Hungary.
The data analyzed in this study is subject to the following licenses/restrictions: Aggregated datasets (without age, gender) is publicly available, while more detailed should be requested from the National Health Fund (NEAK). Requests to access these datasets should be directed to www.neak.gov.hu.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Conceptualization: MM, RB, MH, IK, RB; methodology, formal analysis, software, RB and MM; investigation, RB and MM, data curation, validation, MH, EH, and AV; writing—original draft preparation, IK; writing—review and editing, IK, MM, RB, and MB; and funding acquisition, DC. writing: RB, RR, IK, writing, review, editing: MM, RB, EH, ÁV, PD, MB, EZ, DC. All authors have read and approved the final version of the manuscript.
This work has been implemented with the support provided by the Ministry of Innovation and Technology of Hungary from the National Research, Development and Innovation Fund, financed supported by ITM NKFIA TKP2021-EGA-32. RB was supported by The János Bolyai Research Scholarship of the Hungarian Academy of Science.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Alves, C., Casqueiro, J., and Casqueiro, J. (2012). Infections in patients with diabetes mellitus: A review of pathogenesis. Indian J. Endocrinol. Metab. 16 (7), 27–S36. doi:10.4103/2230-8210.94253
Aspevall, O., Bergfeldt, V., Nilsson, O., and Pringle, M. (2020). Swedres | svarm 2017. Public Health Agency of Sweden and National Veterinary Institute. Shewa, Ethiopia 9 (9), 624. http://files/1182/Unknown - 2017 - 2017 Swedres Svarm.pdf%0Ahttp://files/522/Unknown - 2017 - 2017 Swedres Svarm.pdf.
Benkő, R., Gajdács, M., Matuz, M., Bodó, G., Lázár, A., Hajdú, E., et al. (2020). Prevalence and antibiotic resistance of eskape pathogens isolated in the emergency department of a tertiary care teaching hospital in Hungary: A 5-year retrospective survey. Antibiotics 9 (9), 6244–E717. doi:10.3390/antibiotics9090624
Benko, R., Matuz, M., Doro, P., Hajdu, E., Nagy, G., Nagy, E., et al. (2016). [Antibiotic consumption between 1996 and 2003: National survey and international comparison] Orv. Hetil. 157, 1215–1222.
Blix, H. S., Engeland, A., Litleskare, I., and Rønning, M. (2007). Age- and gender-specific antibacterial prescribing in Norway. J. Antimicrob. Chemother. 59 (5), 971–976. doi:10.1093/jac/dkm032
Dyar, O. J., Nathwani, D., Monnet, D. L., Gyssens, I. C., Lundborg, C. S., Pulcini, C., et al. (2018). Do medical students feel prepared to prescribe antibiotics responsibly? Results from a cross-sectional survey in 29 European countries. J. Antimicrob. Chemother. 73 (8), 2236–2242. doi:10.1093/jac/dky150
ECDC (2017). “Ecdc: SURVEILLANCE REPORT. Annual report of the European antimicrobial resistance surveillance Network (EARS-Net) 2017,” in Surveillance of antimicrobial resistance in Europe. https://ecdc.europa.eu/en/publications-data/antimicrobial-resistance-surveillance-europe-2016.
Elseviers, M. M., Ferech, M., Vander Stichele, R. H., Goossens, H., Mittermayer, H., Metz, S., et al. (2007). Antibiotic use in ambulatory care in Europe (ESAC data 1997-2002): Trends, regional differences and seasonal fluctuations. Pharmacoepidemiol. Drug Saf. 16 (1), 115–123. doi:10.1002/pds.1244
Elvers, K. T., Wilson, V. J., Hammond, A., Duncan, L., Huntley, A. L., Hay, A. D., et al. (2020). Antibiotic-induced changes in the human gut microbiota for the most commonly prescribed antibiotics in primary care in the UK: A systematic review. BMJ Open 10 (9), doi:e035677doi:10.1136/bmjopen-2019-035677
European Commission (2016). “Special eurobarometer 445 report antimicrobial resistance,” in Antimicrobial resistance (issue April). http://ec.europa.eu/COMMFrontOffice/PublicOpinion.
European Union O,, and OECD (2020). Health at a glance: Europe 2020: State of health in the EU cycle. PublishingOECD Publishing. Paris, France. doi:10.1787/9789264105133-ko
Eurostat, (2014b). Data-Eurostat. Daily smokers of cigarettes by sex, age and educational attainment level. Eurostat https://ec.europa.eu/eurostat/databrowser/view/HLTH_EHIS_SK3E__custom_3202364/default/table?lang=en.
Eurostat, (2017a). Data-Eurostat. Hospital discharges by diagnosis and NUTS 2 regions, in-patients, per 100 000 inhabitants. Eurostat https://ec.europa.eu/eurostat/databrowser/view/HLTH_CO_DISCH2T__custom_3202411/default/table?lang=en.
Eurostat, (2017b). Data-Eurostat. Vaccination against influenza of population aged 65 and over[hlth_ps_immu]. Eurostat https://appsso.eurostat.ec.europa.eu/nui/submitViewTableAction.do.
Eurostat, (2022). Data-Eurostat. Life Expectancy at 65. Eurostat https://ec.europa.eu/eurostat/statistics-explained/index.php?title=File:Table2_Life_expectancy_at_65.png.
Eurostat, (2019). “Data - Eurostat,” in Eurostat. https://ec.europa.eu/eurostat/web.
Eurostat, (2014d). Data-eurostat. https://ec.europa.eu/eurostat/web/.
Eurostat, (2014a). Data-Eurostat. Body mass index (BMI) by sex, age and educational attainment level. Eurostat https://ec.europa.eu/eurostat/databrowser/view/HLTH_EHIS_BM1E__custom_3202342/default/table?lang=en.
Eurostat, (2014c). Eurostat. http://appsso.eurostat.ec.europa.eu/nui/submitViewTableAction.do.Data-Eurostat. Persons reporting a chronic disease, by disease, sex, age and educational attainment level
Feehan, J., Tripodi, N., and Apostolopoulos, V. (2021). The twilight of the immune system: The impact of immunosenescence in aging. Maturitas 147, 7–13. doi:10.1016/j.maturitas.2021.02.006
Folkhälsomyndigheten, (2017). Influenza in Sweden 2016-2017 season. http://www.folkhalsomyndigheten.se/publicerat-material/publikationer/.
Frasca, D., and McElhaney, J. (2019). Influence of obesity on pneumococcus infection risk in the elderly. Front. Endocrinol. 10 (FEB), 71–78. doi:10.3389/fendo.2019.00071
Gao, Y., Shang, Q., Li, W., Guo, W., Stojadinovic, A., Mannion, C., et al. (2020). Antibiotics for cancer treatment: A double-edged sword. J. Cancer 11 (17), 5135–5149. doi:10.7150/jca.47470
Ghilotti, F., Bellocco, R., Ye, W., Adami, H. O., and Trolle Lagerros, Y. (2019). Obesity and risk of infections: Results from men and women in the Swedish national March cohort. Int. J. Epidemiol. 48 (6), 1783–1794. doi:10.1093/ije/dyz129
Gonzalez-Gonzalez, C., López-Vázquez, P., Vázquez-Lago, J. M., Piñeiro-Lamas, M., Herdeiro, M. T., Arzamendi, P. C., et al. (2015). Effect of physicians’ attitudes and knowledge on the quality of antibiotic prescription: A cohort study. PLoS ONE 10 (10), e0141820. doi:10.1371/journal.pone.0141820
Government Offices of Sweden, (2020). Swedish strategy to combat antibiotic resistance 2020-2023. https://www.government.se/499178/globalassets/government/dokument/socialdepartementet/amr_strategi_eng_web.pdf.
Harpsøe, M. C., Nielsen, N. M., Friis-Møller, N., Andersson, M., Wohlfahrt, J., Linneberg, A., et al. (2016). Body mass index and risk of infections among women in the Danish national birth cohort. Am. J. Epidemiol. 183 (11), 1008–1017. doi:10.1093/aje/kwv300
Huttner, A., Bielicki, J., Clements, M. N., Frimodt-Møller, N., Muller, A. E., Paccaud, J. P., et al. (2020). Oral amoxicillin and amoxicillin–clavulanic acid: Properties, indications and usage. Clin. Microbiol. Infect. 26 (7), 871–879. doi:10.1016/j.cmi.2019.11.028
Jensen, M. L. V., Aabenhus, R. M., Holzknecht, B. J., Bjerrum, L., Jensen, J. N., Siersma, V., et al. (2021). Antibiotic prescribing in Danish general practice in the elderly population from 2010 to 2017. Scand. J. Prim. Health Care 39 (4), 498–505. doi:10.1080/02813432.2021.2004754
Jiang, C., Chen, Q., and Xie, M. (2020). Smoking increases the risk of infectious diseases: A narrative review. Tob. Induc. Dis. 18 (July), 60. doi:10.18332/tid/123845
Juhasz, Z., Benko, R., Matuz, M., Viola, R., Soos, G., and Hajdu, E. (2013). Treatment of acute cystitis in Hungary: Comparison with national guidelines and with disease-specific quality indicators. Scand. J. Infect. Dis. 45 (8), 612–615. doi:10.3109/00365548.2013.777157
Kabbani, S., Palms, D., Bartoces, M., Stone, N., and Hicks, L. A. (2018). Outpatient Antibiotic prescribing for older adults in the United States: 2011 to 2014. J. Am. Geriatr. Soc. 66 (10), 1998–2002. doi:10.1111/jgs.15518
Kornfält Isberg, H., Melander, E., Hedin, K., Mölstad, S., and Beckman, A. (2019). Uncomplicated urinary tract infections in Swedish primary care; Etiology, resistance and treatment. BMC Infect. Dis. 19 (1), 155–158. doi:10.1186/s12879-019-3785-x
Kovács, K., and Pakot, L. (2020). [Influenza-associated mortality in Hungary between 2009/2010 and 2016/2017]. Orv. Hetil. 161 (23), 962–970. doi:10.1556/650.2020.31725
Langdon, A., Crook, N., and Dantas, G. (2016). The effects of antibiotics on the microbiome throughout development and alternative approaches for therapeutic modulation. Genome Med. 8 (1), 39. doi:10.1186/s13073-016-0294-z
MacKenzie, F. M., Monnet, D. L., and Gould, I. M. (2006). Relationship between the number of different antibiotics used and the total use of antibiotics in European hospitals. J. Antimicrob. Chemother. 58 (3), 657–660. doi:10.1093/jac/dkl286
Matuz, M., Benkő, R., Hajdú, E., Viola, R., and Soós, G. (2013). [Evaluation of ambulatory antibiotic use in Hungary using drug-specific quality indicators]. Orv. Hetil. 154 (24), 947–956. doi:10.1556/OH.2013.29632
Matuz, Maria, Bognar, J., Hajdu, E., Doro, P., Bor, A., Viola, R., et al. (2015). Treatment of community-acquired pneumonia in adults: Analysis of the national dispensing database. Basic Clin. Pharmacol. Toxicol. 117 (5), 330–334. doi:10.1111/bcpt.12426
Medical Products Agency and Strama, (2008). Management of Respiratory Tract Infections. Sweden. [In Swedish] https://www.lakemedelsverket.se/sv/behandling-och-forskrivning/behandlingsrekommendationer/sok-behandlingsrekommendationer/antibiotika-vid-nedre-luftvagsinfektioner-i-oppenvard---behandlingsrekommendation#hmainbody1.
Mölstad, S., Löfmark, S., Carlin, K., Erntell, M., Aspevall, O., Blad, L., et al. (2017). Lessons learnt during 20 years of the Swedish strategic programme against antibiotic resistance. Bull. World Health Organ. 95 (11), 764–773. doi:10.2471/BLT.16.184374
Raban, M. Z., Gates, P. J., Gasparini, C., and Westbrook, J. I. (2021). Temporal and regional trends of antibiotic use in long-term aged care facilities across 39 countries, 1985-2019: Systematic review and meta-analysis. PloS One 16 (8). doi:10.1371/journal.pone.0256501doi:e0256501
Ryu, S., Kim, S., Kim, B. I., Klein, E. Y., Yoon, Y. K., and Chun, B. C. (2018). Temporal relationship between antibiotic use and respiratory virus activities in the republic of Korea: A time-series analysis. Antimicrob. Resist. Infect. Control 7, 56. doi:10.1186/s13756-018-0347-8
Salm, F., Ernsting, C., Kuhlmey, A., Kanzler, M., Gastmeier, P., and Gellert, P. (2018). Antibiotic use, knowledge and health literacy among the general population in Berlin, Germany and its surrounding rural areas. PLoS One 13 (2). doi:10.1371/journal.pone.0193336doi:e0193336
Smetana, J., Chlibek, R., Shaw, J., Splino, M., and Prymula, R. (2018). Influenza vaccination in the elderly. Hum. Vaccin. Immunother. 14 (3), 540–549. doi:10.1080/21645515.2017.1343226
Smith, D. R. M., Dolk, F. C. K., Smieszek, T., Robotham, J. V., and Pouwels, K. B. (2018). Understanding the gender gap in antibiotic prescribing: A cross-sectional analysis of English primary care. BMJ Open 8 (2), e020203–e020207. doi:10.1136/bmjopen-2017-020203
Stahlmann, R., and Lode, H. (2010). Safety considerations of fluoroquinolones in the elderly: An update. Drugs Aging 27 (3), 193–209. doi:10.2165/11531490-000000000-00000
Tyrstrup, M., van der Velden, A., Engstrom, S., Goderis, G., Molstad, S., Verheij, T., et al. (2017). Antibiotic prescribing in relation to diagnoses and consultation rates in Belgium, The Netherlands and Sweden: Use of European quality indicators. Scand. J. Prim. Health Care 35 (1), 10–18. doi:10.1080/02813432.2017.1288680
U.S. Food and Drug Administration (2018). Drug safety communication: FDA warns about increased risk of ruptures or tears in the aorta blood vessel with fluoroquinolone antibiotics in certain patients. U.S. Food and Drug Administration https://www.jwatch.org/na48248/2019/02/13/adverse-effects-fluoroquinolones-where-do-we-stand.
Ventola, C. L. (2015) The antibiotic resistance crisis: Part 1: Causes and threats P Trans. 40 (40), 277–283. doi:10.1016/B978-1-4831-9711-1.50022-3
Who, (2018). Evidence brief for policy: promoting the appropriate use of antibiotics to contain antibiotic resistance in human medicine in Hungary, 2. Evidence Informed Policy Network (EVIPNet) Europe.
Who, (2020). ATC/DDD index 2022. WHO Publications. https://www.whocc.no/atc_ddd_index/.
Who, (2011). European strategic action plan on antibiotic resistance. http://www.euro.who.int/__data/assets/pdf_file/0008/147734/wd14E_AntibioticResistance_111380.pdf.6September12–15.
Keywords: drug utilization study, ambulatory care, antibacterials, elderly, cross national comparison, prescrptions/1000 inhabitants/year, public health, antibiotic stewardship
Citation: Kusuma IY, Matuz M, Bordás R, Juhasz Haverinen M, Bahar MA, Hajdu E, Visnyovszki Á, Ruzsa R, Doró P, Engi Z, Csupor D and Benko R (2022) Antibiotic use in elderly patients in ambulatory care: A comparison between Hungary and Sweden. Front. Pharmacol. 13:1042418. doi: 10.3389/fphar.2022.1042418
Received: 12 September 2022; Accepted: 27 October 2022;
Published: 17 November 2022.
Edited by:
Domenico Criscuolo, Italian Society of Pharmaceutical Medicine, ItalyReviewed by:
Sandor Kerpel-Fronius, Semmelweis University, HungaryCopyright © 2022 Kusuma, Matuz, Bordás, Juhasz Haverinen, Bahar, Hajdu, Visnyovszki, Ruzsa, Doró, Engi, Csupor and Benko. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ria Benko, YmVua29yaWFAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.