 Linrui Xu1,2,3
Linrui Xu1,2,3 Fengming Luo
Fengming Luo
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol. , 28 October 2022
Sec. Drugs Outcomes Research and Policies
Volume 13 - 2022 | https://doi.org/10.3389/fphar.2022.1019915
Background: Interstitial lung disease (ILD) is a common pulmonary disease often associated with significant morbidity and mortality in patients with connective tissue diseases (CTD). Currently, no gold-standard therapies are available for CTD-ILD. Recently, several studies have proposed that rituximab (RTX) may be effective for the treatment of CTD-ILD.
Objectives: This study aimed to systematically evaluate the efficacy and safety of RTX for the treatment of CTD-ILD.
Methods: Studies were selected from PubMed, Embase, and Cochrane Library, up to 20 July 2022. Improvement and stable rates were extracted as the main outcomes and pooled using the weighted mean proportion with fixed or random-effects models, in case of significant heterogeneity (I2 > 50%). Safety analysis was performed based on the adverse events reported in all of the studies.
Results: Thirteen studies (312 patients) were included in the meta-analysis. The follow-up durations ranged from 6 to 36 months. The pooled improvement rate was 35.0% (95% CI: 0.277–0.442), while the pooled stable rate was 59.2% (95% CI: 0.534–0.656). Anti-synthetase syndrome associated with ILD [ASS-ILD, 48.1% (95% CI, 0.373–0.620)] and idiopathic inflammatory myopathies associated with ILD [IIM-ILD, non-ASS, 47.4% (95% CI, 0.266–0.846)] had higher improvement rates than the other types. A total of 106 adverse events associated with RTX or progressive ILD were reported among the 318 patients, 55.7% of which were mild. Among 19 deaths, 17 were due to ILD progression, one to severe pulmonary arterial hypertension, and one to Pneumocystis jirovecii infection.
Conclusion: RTX, which exhibits a satisfactory safety profile, is an effective treatment option for CTD-ILD, even in patients who fail to respond to other therapies. Further randomized trials are needed to assess the efficacy of rituximab compared to other treatments for CTD-ILD.
Systematic review registration: PROSPERO, identifier (CRD42022363403).
Connective tissue diseases (CTDs) are a group of disorders characterized by diverse symptoms and autoantibodies that circulate throughout the body and damage internal organs (Koo et al., 2019). Interstitial lung disease (ILD) is a common pulmonary disease that is associated with significant morbidity and mortality in patients with CTDs. The prevalence of CTD-ILD varies, depending on the underlying CTD (Marigliano et al., 2013). A high prevalence of ILD in systemic sclerosis (SSc), idiopathic inflammatory myopathies (IIM), rheumatoid arthritis (RA), and mixed CTD (MCTD), of up to 50%–60%, has been reported in previous studies. Furthermore, ILD has been reported in 25% of patients with primary Sjögren’s syndrome (pSS) and 2%–8% of patients with lupus (Lynch, 2009; Castelino and Varga, 2010; Solomon and Fischer, 2015; Mathai and Danoff, 2016). It is very important to identify ILD in CTD in the early stages and develop a proper treatment plan, which may improve prognosis.
The pathogenesis of CTD-ILD is complex and not fully understood; however, it is generally accepted that underlying immune system dysfunction, immune-mediated pulmonary inflammation, and subsequent fibrosis are crucial steps. Therefore, corticosteroids and immunosuppressive drugs are considered crucial for the treatment of CTD-ILD (Mathai and Danoff, 2016). Evidence from clinical trials suggests that immunosuppressant therapies, such as cyclophosphamide (CYC), mycophenolate mofetil (MMF), and tacrolimus, are associated with lung function improvement and ILD regression (Tashkin et al., 2006; Ge et al., 2015; Tashkin et al., 2016; Karampitsakos et al., 2022). In recent years, nintedanib, an anti-fibrotic tyrosine kinase inhibitor, has revolutionized the treatment of connective tissue diseases (Distler et al., 2019; Flaherty et al., 2019) and was approved by the United States Food and Drug Administration and the European Medicines Agency. In contrast, evidence for the efficacy of pirfenidone (another antifibrotic drug) in CTD-ILD is not equally compelling (Li et al., 2016; Acharya et al., 2020). For severe progressive CTD-ILD, intravenous CYC is considered the standard treatment (Hoyles et al., 2006). However, disease progression was observed in some patients, even with intensive therapy. Patients with SSc-ILD have a median survival duration of less than five years, and a similar poor prognosis has been observed in patients with IIM-ILD and MCTD-ILD (Goh et al., 2008). Alternative therapies may be required for patients with poor response to conventional treatment.
Biological treatments [TNF-α inhibitors (Wang et al., 2011), B-cell-targeted therapies (Sharp et al., 2016), T cell co-stimulatory molecule blockers (Fernández-Díaz et al., 2018), and immune checkpoint inhibitors (Akiyama et al., 2016)] may achieve beneficial outcomes in a proportion of patients with refractory CTD-ILD. Among them, rituximab (RTX) and TNF-α inhibitors are the most widely used biological treatments for patients with CTD-ILD (Karampitsakos et al., 2019). An observational cohort study reported better long-term survival in patients receiving rituximab than in those receiving a TNF-α inhibitor (Druce et al., 2017). RTX is a chimeric monoclonal antibody that targets CD20 expressed on pre-B and B lymphocytes, which depletes B cells from peripheral circulation for six to nine months (Leandro et al., 2006; Perosa et al., 2010). RTX has gained popularity for the management of a variety of systemic autoimmune diseases and is now approved for the treatment of RA (Smolen et al., 2017), antineutrophil cytoplasmic antibody-associated vasculitis (ANCA-associated vasculitis) (Yates et al., 2016), and immune thrombocytopenic purpura (Arnold et al., 2007). Several small studies have suggested that RTX may also be effective in CTD-ILD, with favorable responses in the treatment of patients refractory to conventional immunosuppression. RTX can be considered an effective “rescue therapy” for progressive CTD-ILD (Keir et al., 2012; Keir et al., 2014; Fitzgerald et al., 2015; Sharp et al., 2016). Most of the data supporting RTX for CTD-ILD comes from retrospective studies and small case series. To our knowledge, no systematic review has evaluated the outcomes of RTX in a population of patients with CTD-ILD. As no randomized clinical trials are available for RTX in CTD-ILD, such data are important to weigh the benefits of individual patient decision-making. However, RTX may contribute to the development and progression of pulmonary disease (Naqibullah et al., 2015). To understand and clarify the available evidence, we conducted a systematic review and meta-analysis to evaluate the efficacy and safety of RTX in patients with CTD-ILD.
We followed the Meta-Analysis of Observational Studies in Epidemiology guidelines during all stages of design, implementation, and reporting of this meta-analysis (Stroup et al., 2000). This study was registered at PROSPERO under registration number CRD42022363403.
An exhaustive literature search, both computer-assisted and manual, was performed. A systematic literature search of the PubMed, Embase and Cochrane Library was conducted, using the keywords “Rituximab”, “CD20 Antibody”, “Interstitial Lung Disease”, “Interstitial Pneumonia”, “systemic sclerosis”, “idiopathic inflammatory myopathies”, “rheumatoid arthritis”, “primary Sjögren’s syndrome”, “systemic lupus erythematosus”, and “connective tissue disease”. The last date of the search was 20 July 2022 (Supplementary Table S1).
We included the studies if relevant information on patients’ characteristics, treatment interventions, and outcomes were available. The research was limited to articles published in English language. There was no restriction in study design. The inclusion criteria were: 1) the diagnosis of CTD met the accepted international criteria and the patients presented with ILD based on chest high-resolution computed tomography (HRCT) and/or lung biopsy (Bohan and Peter, 1975; Author anonymous, 1980; Arnett et al., 1988; Alarcón-Segovia and Cardiel, 1989; Hochberg, 1997; Mosca et al., 1999); 2) patients were treated with RTX were included; 3) outcomes assessed improvement rate and stable rate based on pulmonary function test (PFT). The response criteria were based on the guidance provided by American Thoracic Society/European Respiratory Society guidelines (Raghu et al., 2011). This lung response was classified into improving [increases of ≥ 10% in forced vital capacity (FVC) and/or ≥ 15% in diffusing capacity of carbon monoxide (DLCO)], worsening (decrease of ≥ 10% in FVC and/or ≥15% in DLCO, or death from progressive ILD) and stable (others that did not meet criteria for either worsening/improving). Studies with patients less than 10 were excluded. Reports only in abstract were also excluded. Adverse drug reactions and adverse events related to ILD progression were reported together in most original studies, so all reported adverse events associated with RTX treatment or progressive ILD were included for safety assessment.
Two reviewers carried out the searches, study selection and data extraction, independently. In Case of discrepancy, a consensus was reached by two reviewers. Two reviewers independently screened the titles and abstracts from the data sources based on eligibility criteria mentioned above. Then, the full texts of the potentially relevant articles were reviewed thoroughly to guarantee its eligibility criteria. We recorded the following information from the original literature (Koo et al., 2019): the first author; (Marigliano et al., 2013) year of publication; (Castelino and Varga, 2010) study design (prospective or retrospective); (Solomon and Fischer, 2015) baseline data of patients, including the number of patients that meet the inclusion criteria, type of CTD, gender, age; (Mathai and Danoff, 2016) dose and schedule of RTX; (Lynch, 2009) follow-up period; (Tashkin et al., 2006) lung response outcome; (Tashkin et al., 2016) adverse events.
We used the modified Newcastle–Ottawa scale to make the quality assessment of observational studies (Lo et al., 2014). This scale included three parts mainly: Patient selection, comparability between study groups through design or analysis, and outcome assessment. Every study allocated a score (0–9) and a study was considered to be of high quality if it was with a score of five or more.
Patients’ baseline characteristics and lung responses were analyzed from those studies enrolling ten or more patients only to avoid the extreme risk of selection and reporting biased data. The assessment criteria were the improvement and stable rate of CTD-ILD, expressed as their mean rates, together with their 95% confidence interval (95% CI). We performed subgroup analysis based on different types of CTD. The Chi-square test (Q statistic) and I2 statistic were performed to assess heterogeneity (Higgins et al., 2003). If p ≥ 0.10 and/or I2 ≤ 50%, the heterogeneity was recognized to be low and we would select a fixed effect model. If not, we would choose random effects. The risk of publication bias was determined by funnel plot and the Egger’s test (Egger et al., 1997). A p-value below 0.05 was considered statistically significant. Adverse events were extracted from all studies to provide a thorough description of safety. We used the logit transformation for meta-analyzing raw proportions with a continuity correction of 0.5 in studies with zero cell frequencies. All analyses were performed using the R programming language (package meta, version 3.6.1).
A flow chart of the screening process is shown in Figure 1. A total of 368 articles were identified through the database search. Of the selected studies, 70 duplicate articles were excluded using Endnote Software. After exclusion based on the titles and abstracts, 36 full-text articles were reviewed. After full-text screening, 13 publications (312 patients) were included in this systematic review. The classifications and features of the included studies are presented in Table 1. All studies were non-randomized, three (Allenbach et al., 2015; Bosello et al., 2015; Sircar et al., 2018) were prospective, and 10 (Sem et al., 2009; Keir et al., 2014; Lepri et al., 2016; Sharp et al., 2016; Md Yusof MYKabia et al., 2017; Sari et al., 2017; Doyle et al., 2018; Duarte et al., 2019; Narváez et al., 2020a; Narváez et al., 2020b) were retrospective. In total, 312 patients were diagnosed with CTD-ILD, including RA, SSc, IIM, SLE, pSS, UCTD, and MCTD. Among the 13 included studies (Sem et al., 2009; Keir et al., 2014; Allenbach et al., 2015; Bosello et al., 2015; Lepri et al., 2016; Sharp et al., 2016; Md Yusof MYKabia et al., 2017; Sari et al., 2017; Doyle et al., 2018; Sircar et al., 2018; Duarte et al., 2019; Narváez et al., 2020a; Narváez et al., 2020b), 157 patients with CTD-ILD (212/312, 67.9%) were refractory to conventional treatments. The studies were performed in the United Kindom (n = 4) (Keir et al., 2014; Sharp et al., 2016; Md Yusof MYKabia et al., 2017; Duarte et al., 2019), Spain (n = 2) (Narváez et al., 2020a; Narváez et al., 2020b), French (n = 1) (Allenbach et al., 2015), United States (n = 1) (Doyle et al., 2018), Turkey (n = 1) (Sari et al., 2017), Norway (n = 1) (Sem et al., 2009), India (n = 1) (Sircar et al., 2018), and Italy (n = 1) (Bosello et al., 2015), and there was only one multicenter study (Lepri et al., 2016). There were 208 (208/312, 66.7%) patients treated with RTX (1,000 mg on day 0 and day 14/day 15), one (1/312, 0.3%) patient treated with RTX (700 mg on day 0 and day 14) and one (1/312, 0.3%) patient treated with RTX (1,000 mg on day 0, day 15, and month 6), while the treatment plans were not available in other studies. Treatments before RTX varied among the studies. CYC, MMF, azathioprine (AZA), and steroids were the most commonly used treatments, while less common treatments included intravenous immunoglobulin (IVIg), TNFi, and tacrolimus. The follow-up period was 6–36 months (Table 1). Quality assessment using the Newcastle–Ottawa scale is shown in Table 2.
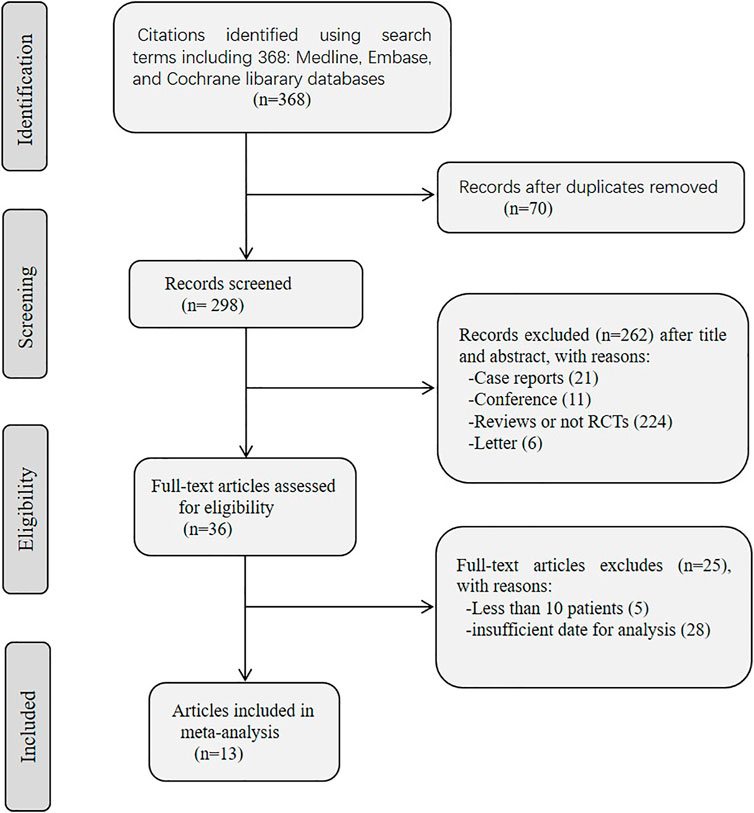
FIGURE 1. Flow diagram of study selection process for this systematic review and meta-analysis.

TABLE 1. Baseline clinical characteristics of included studies.
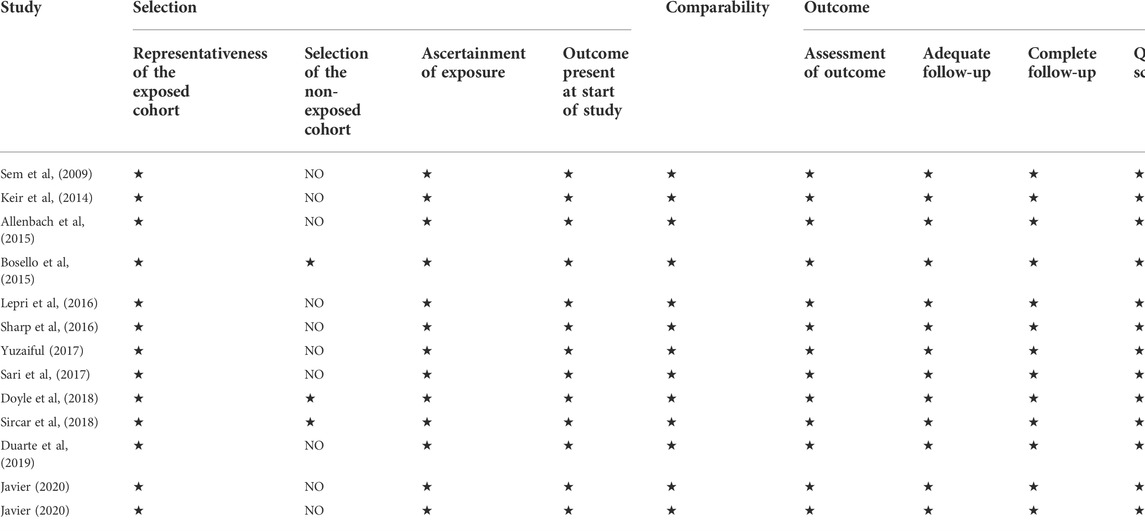
TABLE 2. Quality assessment of included studies by Newcastle–Ottawa scale (score).
The pooled improvement rate was evaluated in 13 studies that included 312 patients with CTD-ILD. A total of 101 patients (101/312, 32.4%) reported improved lung function after RTX in all studies. The improvement rate ranged from 16% to 64%, and the pooled rate was 35.0% (95% CI, 0.277–0.442), with high heterogeneity (I2 = 54%, p = 0.01) (Figure 2A).
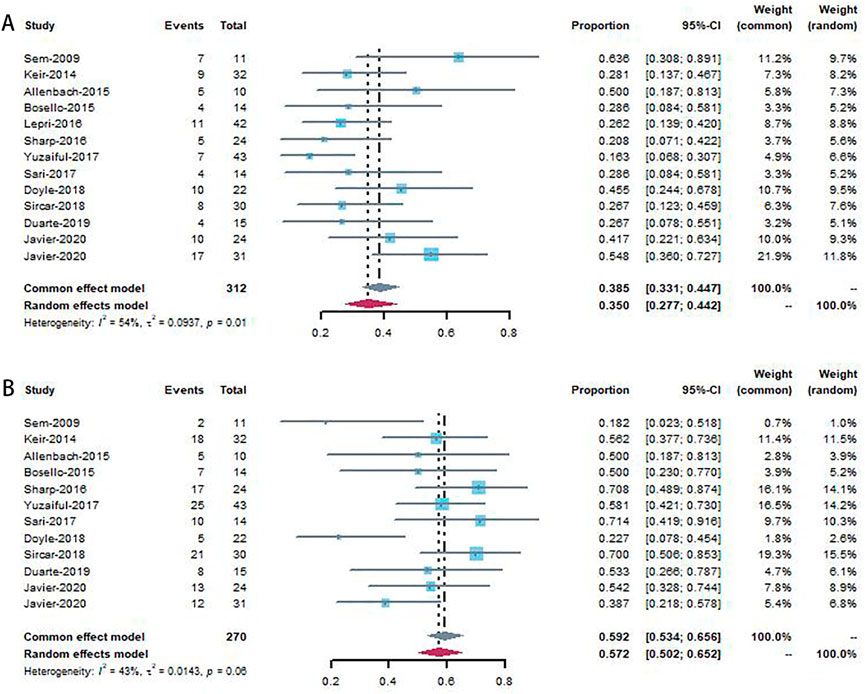
FIGURE 2. Forest plot showing improvement rate (A) and stable rate (B) to patients using rituximab.
Forest plots for the subgroup analyses of studies involving anti-synthetase syndrome (ASS)-ILD, IIM (non-ASS)-ILD, MCTD-ILD, RA-ILD, SSc-ILD, and UCTD-ILD are shown in Figure 3A. ASS-ILD, IIM (non-ASS)-ILD, MCTD-ILD, SSc-ILD and UCTD-ILD were associated with improvement rates of 48.1% (95% CI, 0.373–0.620), 47.4% (95% CI, 0.266–0.845), 33.1% (95% CI, 0.111–0.991), 32.9% (95% CI, 0.252–0.430) and 25.7% (95% CI, 0.098–0.677) respectively, without heterogeneity, except for RA (17% (95% CI, 0.04–0.48), I2 = 74%, p<0.01).
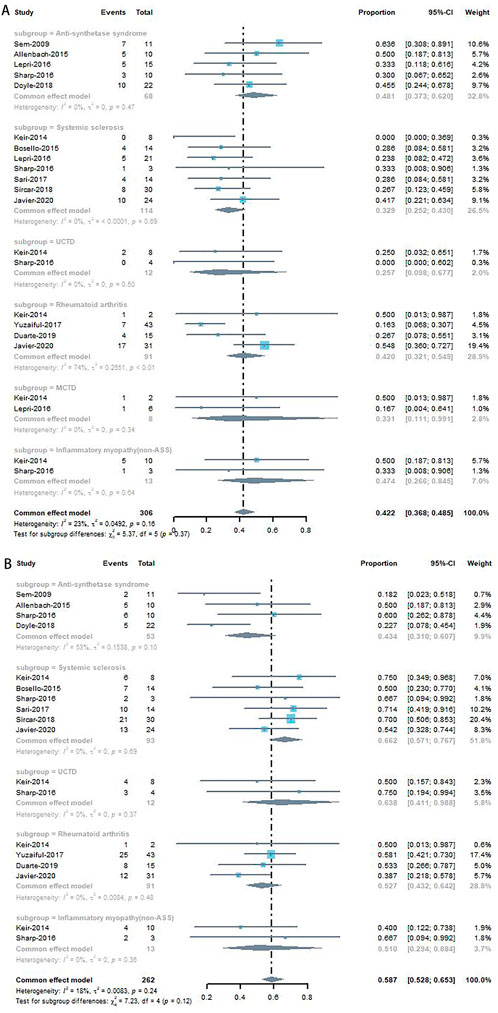
FIGURE 3. Subgroup analyses of improvement rate (A) and stable rate (B) in CTD-ILD studies.
Twelve studies were included in the analysis of lung function stability (Figure 2B). The stability rates ranged from 18% to 71%, and the pooled rate was 59.2% (95% CI, 0.534–0.656) with low heterogeneity (I2 = 43%, p = 0.06).
The forest plot for the subgroup analyses is shown in Figure 3B. IIM (non-ASS)-ILD, RA-ILD, SSc-ILD, and UCTD-ILD were associated with stable rates of 51.0% (95% CI, 0.294–0.884), 52.7% (95% CI, 0.432–0.642), 66.2% (95% CI, 0.571–0.767), and 63.8% (95% CI, 0.411–0.988), respectively, without heterogeneity, except for ASS-ILD [43.4% (95% CI, 0.310–0.607), I2 = 53%, p = 0.10].
All patients treated with RTX were evaluated, some of whom were not included in the pooled analysis of lung response outcomes because lung function data and survival conditions were unavailable. Twelve (Sem et al., 2009; Keir et al., 2014; Allenbach et al., 2015; Bosello et al., 2015; Lepri et al., 2016; Sharp et al., 2016; Sari et al., 2017; Doyle et al., 2018; Sircar et al., 2018; Narváez et al., 2020a; Narváez et al., 2020b) studies reported adverse events. Among them, one study (Keir et al., 2014) reported three deaths due to respiratory failure secondary to ILD progression, but did not report other adverse events. One study (Duarte et al., 2019) did not provide any relevant information. We evaluated adverse events related to RTX treatment or progressive ILD according to the Common Terminology Criteria for Adverse Events (CTCAE), which are shown in Table 3. A total of 318 patients from 12 studies were included. A total of 55.7% of the adverse events were mild-to-moderate (grade 1–2), including a mild infection that was treated with oral antibiotics without hospitalization (n = 44), fever (n = 6), infusion reactions (n = 5), fatigue (n = 3), and cardiac involvement with arrhythmia (n = 1). Among grade 3–4 events, 28 adverse events occurred, including infection requiring hospitalization (n = 23), serum sickness (n = 2), gastrointestinal complications requiring surgery (n = 2), and anaphylaxis (n = 1). Nineteen deaths were reported in 318 patients: 17 due to respiratory failure secondary to ILD progression, one with severe pulmonary arterial hypertension, and one with Pneumocystis jirovecii infection.
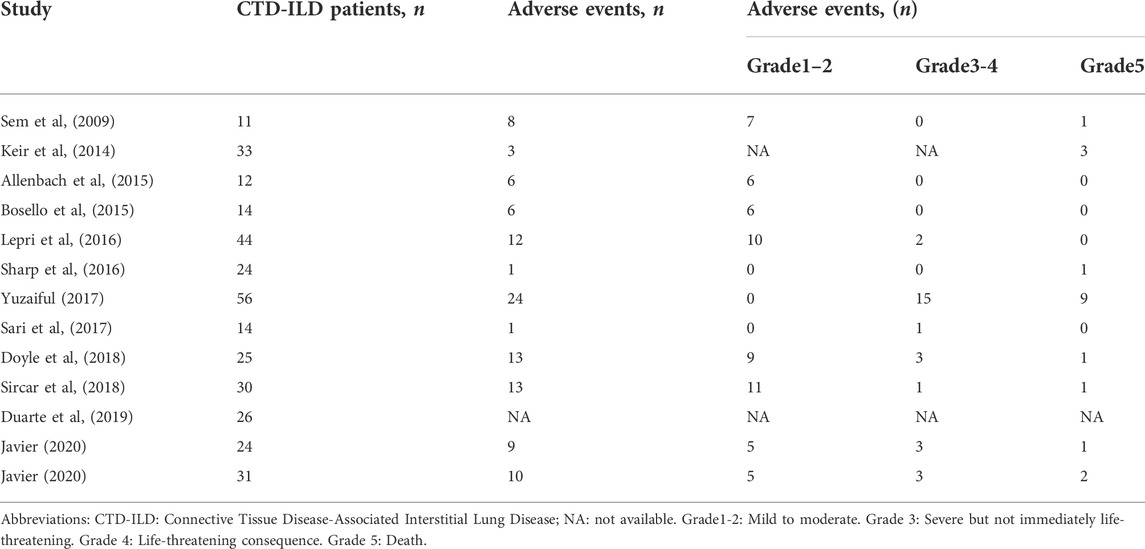
TABLE 3. Adverse events observed after rituximab infusion in CTD-ILD patients.
Sensitivity analysis was performed by removing individual studies one by one from the pooled results with high heterogeneity. The pooled analysis of improvement rate and stable rate did not change significantly when studies were omitted, indicating that our combined results are reliable (Figure 4).
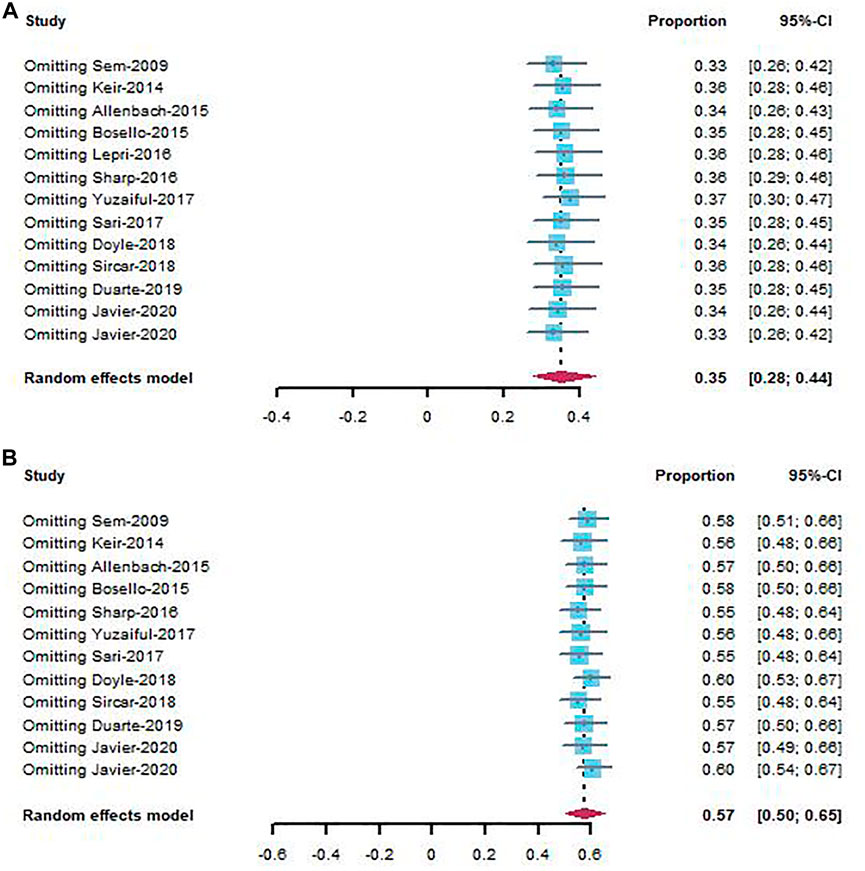
FIGURE 4. Sensitivity analysis of improvement rate (A) and stable rate (B) in CTD-ILD studies.
We used the Egger’s test and funnel plots to evaluate the publication bias in studies included. The results of the Egger’s test showed no evidence of publication bias in the studies on improvement rate (p = 0.17) (Figure 5A) and stable rate (p = 0.21) (Figure 5B). This was consistent with the shape of funnel plots which had a good symmetry.
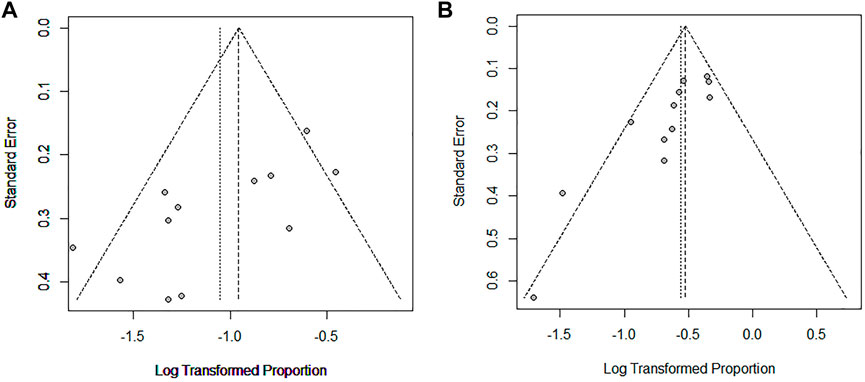
FIGURE 5. Egger funnel plot of improvement rate (A) and stable rate (B) in CTD-ILD studies.
To the best of our knowledge, this is the first meta-analysis of observational studies on the efficacy and safety of RTX in CTD-ILD. Considering that most of the involved patients were refractory to conventional treatments and had progressive ILD, improving or stabilizing lung function was regarded as an effective response. In our results, the improvement rate was estimated to be 35.0% in 312 patients with CTD-ILD, while the stable rate was 59.2%. This result indicates that RTX was an effective treatment option for patients with CTD-ILD based on the lung function test, even in those who failed to respond to other conventional therapies, such as CYC. A total of 106 adverse events associated with rituximab treatment or progressive ILD were reported among the 318 patients. Most were mild, indicating that RTX was tolerated in most patients.
An optimal management for CTD-ILD has not been established because of the relative rarity of the disease and the high variability in disease presentation. Currently, corticosteroids are widely used to manage CTD-ILD (Kowal-Bielecka et al., 2009; Maher, 2014). Other immunosuppressants, including alkylating agent CYC, purine analog azathioprine, antifolate drug methotrexate, inosine monophosphate dehydrogenase inhibitor mycophenolate mofetil, and calcineurin inhibitors ciclosporin and tacrolimus, are also used in the management of CTD-ILD. Among these, CYC is the most well studied for CTD-ILD. Two multicenter randomized studies reported that CYC treatment is associated with an improved FVC trend (Hoyles et al., 2006; Tashkin et al., 2006). A recent open-label, randomized, controlled trial for SSc-ILD that compared the efficacy of RTX and CYC found that RTX improved FVC% while CYC did not after six months of treatment (Sircar et al., 2018). Stone et al. found that rituximab therapy was inferior to daily cyclophosphamide treatment in inducing remission of relapsing disease in severe ANCA-associated vasculitis (Stone et al., 2010). The efficacy and safety reported in these trials suggest that RTX may be considered a first-line therapy (Roofeh et al., 2019). In our meta-analysis, most patients were treated with other immunosuppressants before RTX treatment; however, the efficacy was limited. Stability or improvement of PFT was seen in the majority of patients after RTX therapy in our study, which indicates RTX as a choice in the management of refractory CTD-ILD. However, due to the absence of controlled studies, the present meta-analysis was unable to draw firm conclusions about the difference in efficacy between RTX therapies and other drugs.
Nowadays the treatment of CTD-ILD has a more extended measure with the presence of antifibrotic treatments. The main antifibrotic drugs, pirfenidone (King et al., 2014) and nintedanib (Richeldi et al., 2011), have been proved efficacious for the management of IPF by phase II and III clinical trials. Given the fact that CTD-ILD share many imaging and histopathological characters with IPF (61), of particular interest for rheumatologists are the effectiveness of antifibrotic treatments in CTD-ILD. Nintedanib proved efficacious in reducing the annual rate of decline in FVC in patients with SSc-ILD (12) in the phase III SENSCIS trial, and in treating patients who have fibrosing ILDs with a progressive phenotype (including CTD-ILDs) in the phase III INBUILD study (Flaherty et al., 2019). Pirfenidone showed a modest effectiveness in the decline of FVC in progressive fibrotic CTD-ILD based on a small sample size (Guenther et al., 2019). However, no clinical trials are performed to compare the efficacy between RTX therapies and antifibrotic treatments. Patients involved in our meta-analysis are not received antifibrotic treatment. Further studies are needed to explore the efficacy between RTX therapies and antifibrotic treatments in patients with CTD-ILD who failed to respond to other conventional therapy.
No consensus criteria for assessing the treatment efficacy of CTD-ILD are currently available. Some studies were excluded from our pool analysis because of different assessment methods that focused on the efficacy of RTX. These excluded studies assessed efficacy by comparing mean/median FVC and/or DLCO pre- and post-RTX treatment using the Student t-test or Wilcoxon’s rank sum test. Daoussis et al. (2012) found a significant increase of FVC and DLCO at two years after RTX treatment, compared to baseline (FVC 77.13 ± 7.13 vs. 68.13 ± 6.96; DLCO 63.13 ± 7.65 vs. 52.25 ± 7.32) for SSc-ILD (Daoussis et al., 2012). Two studies focusing on ASS revealed that FVC increased from 66% to 74% and 58%–72%, while DLCO increased from 39% to 59% and 41%–48% after RTX therapy, respectively (Marie et al., 2012; Andersson et al., 2015). A study by Fui found that FVC and DLCO percentages stabilized after RTX treatment (Fui et al., 2019). Our analysis supported these positive findings. In addition, Doyle et al. (2018) found that corticosteroids were stable or decreased in 88% of patients with CTD-ILD one year after RTX treatment, with an average drop of 6 mg, which could be helpful for decreasing the side effects of corticosteroids.
There was medium heterogeneity in the improvement rate (I2 = 54%) and stability rate (I2 = 43%). Subgroup analysis revealed that IIM-ILD (non-ASS) (improvement rate, 47.4%) and ASS-ILD (improvement rate, 48.1%) had higher improvement rates than the others. This adds to the weight of the evidence regarding the heterogeneity of CTD-ILD. However, the pathogenesis of CTD-ILD is not fully understood, and the mechanism by which IIM-CTD responds better to RTX therapy than the other types of CTD-ILD is uncertain. Further research that investigates on the pathogenic mechanisms of CTD-ILD is required.
RTX is a drug that leads to the depletion of B-cells, the mechanism of which remains unknown, but some evidence supports the possibility that B cell function may contribute to the pathogenesis of CTD-ILD. B cell infiltration was found in lung biopsies of 11 patients with SSc-associated ILD (Lafyatis et al., 2007). A study that focused on bronchoalveolar lavage (BAL) fluid found that ILD progression was associated with a higher B-cell percentage in BAL fluid in 73 patients with SSc-ILD (De Santis et al., 2012). It is well known that B cells are a source of autoantibodies, some of which may contribute to the pathogenesis of CTD (Baroni et al., 2006). In addition, RTX can indirectly affect other immune cells, such as T cells, to ““normalizeˮ auto-reactive T cells (Sfikakis et al., 2005; Sfikakis et al., 2007). The repopulation of the B-cell line following RTX tends to be antigenically inexperienced, which suggests that the degree of immune system resetting may contribute to the therapeutic effect (Anolik et al., 2007).
A study conducted by Gagiannis et al. (2020) found overlapping serological, clinical, radiologic, and histopathological features of severe COVID-19 and lung manifestations of autoimmune disease (CTD-ILD). Another study (Narváez et al., 2020a) included patients between January 2010 and December 2019; some of whom may have had COVID disease, as the initial COVID-19 outbreak was reported in 2019. In addition, rituximab use was significantly associated with a higher risk of COVID-19 in CTD-ILD (de Oliveira et al., 2022) included patients between January 2010 and December 2019; some of whom may have had COVID disease, as the initial COVID-19 outbreak was reported in 2019. In addition, rituximab use was significantly associated with a higher risk of COVID-19 in CTD-ILD.
RTX is well-tolerated and safe for CTD-ILD. The adverse events were mainly infectious, most of which were mild and resolved soon after antibiotic treatment. Although there were 19 deaths reported in our analysis, most were due to progressive ILD. Among them, nine deaths with a median DLCO of 41% predicted pre-RTX were reported [36], which indicates severely impaired lung function. However, the safety of RTX warrants further investigation.
This meta-analysis has several limitations. First, the number of patients included was small, and all studies were observational. The small sample size may have influenced the strength of our study. Second, the sex ratio discrepancy among the studies varied due to the small number of included patients, and the female predominant phenomenon may affect the result of the treatment effect analysis in males. Third, all studies failed to compare the efficacy of RTX with other drugs, so we could not provide an unbiased head-to-head comparison of the treatment effects. Fourth, HRCT was not analyzed as an evaluation index, which can be considered another assessment of the efficacy of RTX. It is difficult to pool these data because the criteria for the assessment of HRCT varied among the eligible studies.
In this systematic review and meta-analysis, RTX was found to be an effective treatment option for CTD-ILD according to the assessment of improvement and stability rates based on PFT, even in those who failed to respond to other conventional therapies. Our study revealed that patients with IIM-CTD (non-ASS) or ASS-ILD responded better to rituximab than those with other CTD-ILDs. Regarding side effects, most patients showed good tolerance to RTX. Considering these limitations, prospective randomized trials are needed to assess the efficacy of rituximab compared to other drugs in CTD-ILD. Consensual criteria based on PFT and HRCT for the assessment of CTD-ILD treatment efficacy should be established in the future.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Conception and design: FL, and LX. Acquisition of data: LX, and FW. Critical revision of the manuscript for important intellectual content: FL, LX, and FW. Statistical analysis: LX, and FW. Obtain funding: FW.
This work was supported by Sichuan Science and Technology Program (No.2021YFQ0030); Tibet Science and Technology Program (XZ202201ZY0002G); 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (ZYJC18021); Post-Doctor Research Project, West China Hospital (2021HXBH074) and the National Natural Science Foundation of China (No. 82100075).
The authors thank Lichun Zhong (Laboratory of Pulmonary Immunology and Inflammation, Frontiers Science Center for Disease-related Molecular Network, West China Hospital, Sichuan University) for advising on the data collection.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.1019915/full#supplementary-material
Acharya, N., Sharma, S. K., Mishra, D., Dhooria, S., Dhir, V., and Jain, S. (2020). Efficacy and safety of pirfenidone in systemic sclerosis-related interstitial lung disease-a randomised controlled trial. Rheumatol. Int. 40 (5), 703–710. doi:10.1007/s00296-020-04565-w
Akiyama, M., Kaneko, Y., Yamaoka, K., Kondo, H., and Takeuchi, T. (2016). Association of disease activity with acute exacerbation of interstitial lung disease during tocilizumab treatment in patients with rheumatoid arthritis: A retrospective, case-control study. Rheumatol. Int. 36 (6), 881–889. doi:10.1007/s00296-016-3478-3
Alarcón-Segovia, D., and Cardiel, M. H. (1989). Comparison between 3 diagnostic criteria for mixed connective tissue disease. Study of 593 patients. J. Rheumatol. 16 (3), 328–334.
Allenbach, Y., Guiguet, M., Rigolet, A., Marie, I., Hachulla, E., Drouot, L., et al. (2015). Efficacy of rituximab in refractory inflammatory myopathies associated with anti- synthetase auto-antibodies: An open-label, phase II trial. PloS one 10 (11), e0133702. doi:10.1371/journal.pone.0133702
Andersson, H., Sem, M., Lund, M. B., Aalokken, T. M., Gunther, A., Walle-Hansen, R., et al. (2015). Long-term experience with rituximab in anti-synthetase syndrome-related interstitial lung disease. Rheumatol. Oxf. Engl. 54 (8), 1420–1428. doi:10.1093/rheumatology/kev004
Anolik, J. H., Barnard, J., Owen, T., Zheng, B., Kemshetti, S., Looney, R. J., et al. (2007). Delayed memory B cell recovery in peripheral blood and lymphoid tissue in systemic lupus erythematosus after B cell depletion therapy. Arthritis Rheum. 56 (9), 3044–3056. doi:10.1002/art.22810
Arnett, F. C., Edworthy, S. M., Bloch, D. A., McShane, D. J., Fries, J. F., Cooper, N. S., et al. (1988). The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 31 (3), 315–324. doi:10.1002/art.1780310302
Arnold, D. M., Dentali, F., Crowther, M. A., Meyer, R. M., Cook, R. J., Sigouin, C., et al. (2007). Systematic review: Efficacy and safety of rituximab for adults with idiopathic thrombocytopenic purpura. Ann. Intern. Med. 146 (1), 25–33. doi:10.7326/0003-4819-146-1-200701020-00006
Author anonymous, Preliminary criteria for the classification of systemic sclerosis (scleroderma). Subcommittee for scleroderma criteria of the American Rheumatism Association Diagnostic and Therapeutic Criteria Committee. Arthritis Rheum. 1980;23(5), 581–590. doi:10.1002/art.1780230510
Baroni, S. S., Santillo, M., Bevilacqua, F., Luchetti, M., Spadoni, T., Mancini, M., et al. (2006). Stimulatory autoantibodies to the PDGF receptor in systemic sclerosis. N. Engl. J. Med. 354 (25), 2667–2676. doi:10.1056/NEJMoa052955
Bohan, A., and Peter, J. B. (1975). Polymyositis and dermatomyositis (first of two parts). N. Engl. J. Med. 292 (7), 344–347. doi:10.1056/NEJM197502132920706
Bosello, S. L., De Luca, G., Rucco, M., Berardi, G., Falcione, M., Danza, F. M., et al. (2015). Long-term efficacy of B cell depletion therapy on lung and skin involvement in diffuse systemic sclerosis. Semin. Arthritis Rheum. 44 (4), 428–436. doi:10.1016/j.semarthrit.2014.09.002
Castelino, F. V., and Varga, J. (2010). Interstitial lung disease in connective tissue diseases: Evolving concepts of pathogenesis and management. Arthritis Res. Ther. 12 (4), 213. doi:10.1186/ar3097
Daoussis, D., Liossis, S. N., Tsamandas, A. C., Kalogeropoulou, C., Paliogianni, F., Sirinian, C., et al. (2012). Effect of long-term treatment with rituximab on pulmonary function and skin fibrosis in patients with diffuse systemic sclerosis. Clin. Exp. Rheumatol. 30, S17–S22.
de Oliveira, S. M., Martins, L. V. O., Lupino-Assad, A. P., Medeiros-Ribeiro, A. C., de Moraes, D. A., Del-Rio, A. P. T., et al. (2022). Severity and mortality of COVID-19 in patients with systemic sclerosis: A Brazilian multicenter study. Semin. Arthritis Rheum. 55, 151987. doi:10.1016/j.semarthrit.2022.151987
De Santis, M., Bosello, S. L., Peluso, G., Pinnelli, M., Alivernini, S., Zizzo, G., et al. (2012). Bronchoalveolar lavage fluid and progression of scleroderma interstitial lung disease. Clin. Respir. J. 6 (1), 9–17. doi:10.1111/j.1752-699X.2010.00228.x
Distler, O., Highland, K. B., Gahlemann, M., Azuma, A., Fischer, A., Mayes, M. D., et al. (2019). Nintedanib for systemic sclerosis-associated interstitial lung disease. N. Engl. J. Med. 380 (26), 2518–2528. doi:10.1056/NEJMoa1903076
Doyle, T. J., Dhillon, N., Madan, R., Cabral, F., Fletcher, E. A., Koontz, D. C., et al. (2018). Rituximab in the treatment of interstitial lung disease associated with antisynthetase syndrome: A multicenter retrospective case review. J. Rheumatol. 45 (6), 841–850. doi:10.3899/jrheum.170541
Druce, K. L., Iqbal, K., Watson, K. D., Symmons, D. P. M., Hyrich, K. L., and Kelly, C. (2017). Mortality in patients with interstitial lung disease treated with rituximab or TNFi as a first biologic. RMD open 3 (1), e000473. doi:10.1136/rmdopen-2017-000473
Duarte, A. C., Porter, J. C., and Leandro, M. J. (2019). The lung in a cohort of rheumatoid arthritis patients-an overview of different types of involvement and treatment. Oxford, England): Rheumatology.
Egger, M., Davey Smith, G., Schneider, M., and Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test. BMJ Clin. Res. ed) 315 (7109), 629–634. doi:10.1136/bmj.315.7109.629
Fernández-Díaz, C., Loricera, J., Castañeda, S., López-Mejías, R., Ojeda-García, C., Olivé, A., et al. (2018). Abatacept in patients with rheumatoid arthritis and interstitial lung disease: A national multicenter study of 63 patients. Semin. Arthritis Rheum. 48 (1), 22–27. doi:10.1016/j.semarthrit.2017.12.012
Fitzgerald, D. B., Moloney, F., Twomey, M., O'Connell, J. O., Cronin, O., Harty, L., et al. (2015). Efficacy and safety of rituximab in connective tissue disease related interstitial lung disease. Sarcoidosis Vasc. Diffuse Lung Dis. 32 (3), 215–221.
Flaherty, K. R., Wells, A. U., Cottin, V., Devaraj, A., Walsh, S. L. F., Inoue, Y., et al. (2019). Nintedanib in progressive fibrosing interstitial lung diseases. N. Engl. J. Med. 381 (18), 1718–1727. doi:10.1056/NEJMoa1908681
Fui, A., Bergantini, L., Selvi, E., Mazzei, M. A., Bennett, D., Pieroni, M. G., et al. (2019). Rituximab therapy in interstitial lung disease associated with rheumatoid arthritis. Intern. Med. J. 50, 330–336. doi:10.1111/imj.14306
Gagiannis, D., Steinestel, J., Hackenbroch, C., Schreiner, B., Hannemann, M., Bloch, W., et al. (2020). Clinical, serological, and histopathological similarities between severe COVID-19 and acute exacerbation of connective tissue disease-associated interstitial lung disease (CTD-ILD). Front. Immunol. 11, 587517. doi:10.3389/fimmu.2020.587517
Ge, Y., Zhou, H., Shi, J., Ye, B., Peng, Q., Lu, X., et al. (2015). The efficacy of tacrolimus in patients with refractory dermatomyositis/polymyositis: A systematic review. Clin. Rheumatol. 34 (12), 2097–2103. doi:10.1007/s10067-015-3065-0
Goh, N. S., Desai, S. R., Veeraraghavan, S., Hansell, D. M., Copley, S. J., Maher, T. M., et al. (2008). Interstitial lung disease in systemic sclerosis: A simple staging system. Am. J. Respir. Crit. Care Med. 177 (11), 1248–1254. doi:10.1164/rccm.200706-877OC
Guenther, A., Prasse, A., Kreuter, M., Neuser, P., Rabe, K., Bonella, F., et al. (2019). Late breaking abstract - exploring efficacy and safety of oral pirfenidone for progressive, non-IPF lung fibrosis (RELIEF). Eur. Respir. J. 54, RCT1879, doi:10.1183/13993003.congress-2019.RCT1879
Higgins, J. P., Thompson, S. G., Deeks, J. J., and Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ Clin. Res. ed). 327 (7414), 557–560. doi:10.1136/bmj.327.7414.557
Hochberg, M. C. (1997). Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 40 (9), 1725. doi:10.1002/art.1780400928
Hoyles, R. K., Ellis, R. W., Wellsbury, J., Lees, B., Newlands, P., Goh, N. S., et al. (2006). A multicenter, prospective, randomized, double-blind, placebo-controlled trial of corticosteroids and intravenous cyclophosphamide followed by oral azathioprine for the treatment of pulmonary fibrosis in scleroderma. Arthritis Rheum. 54 (12), 3962–3970. doi:10.1002/art.22204
Jee, A. S., Sheehy, R., Hopkins, P., Corte, T. J., Grainge, C., Troy, L. K., et al. (2021). Diagnosis and management of connective tissue disease-associated interstitial lung disease in Australia and New Zealand: A position statement from the thoracic society of Australia and New Zealand. Respirology 26 (1), 23–51. doi:10.1111/resp.13977
Karampitsakos, T., Kalogeropoulou, C., Tzilas, V., Papaioannou, O., Kazantzi, A., Koukaki, E., et al. (2022). Safety and effectiveness of mycophenolate mofetil in interstitial lung diseases: Insights from a machine learning radiographic model. Respiration. 101 (3), 262–271. doi:10.1159/000519215
Karampitsakos, T., Vraka, A., Bouros, D., Liossis, S. N., and Tzouvelekis, A. (2019). Biologic treatments in interstitial lung diseases. Front. Med. 6, 41. doi:10.3389/fmed.2019.00041
Keir, G. J., Maher, T. M., Hansell, D. M., Denton, C. P., Ong, V. H., Singh, S., et al. (2012). Severe interstitial lung disease in connective tissue disease: Rituximab as rescue therapy. Eur. Respir. J. 40 (3), 641–648. doi:10.1183/09031936.00163911
Keir, G. J., Maher, T. M., Ming, D., Abdullah, R., de Lauretis, A., Wickremasinghe, M., et al. (2014). Rituximab in severe, treatment-refractory interstitial lung disease. Respirology 19 (3), 353–359. doi:10.1111/resp.12214
King, T. E., Bradford, W. Z., Castro-Bernardini, S., Fagan, E. A., Glaspole, I., Glassberg, M. K., et al. (2014). A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N. Engl. J. Med. 370 (22), 2083–2092. doi:10.1056/NEJMoa1402582
Koo, S. M., Kim, S. Y., Choi, S. M., and Lee, H. K. (2019). Korean guidelines for diagnosis and management of interstitial lung diseases: Part 5. Connective tissue disease associated interstitial lung disease. Tuberc. Respir. Dis. 82, 285–297. doi:10.4046/trd.2019.0009
Kowal-Bielecka, O., Landewe, R., Avouac, J., Chwiesko, S., Miniati, I., Czirjak, L., et al. (2009). EULAR recommendations for the treatment of systemic sclerosis: A report from the EULAR scleroderma trials and research group (EUSTAR). Ann. Rheum. Dis. 68 (5), 620–628. doi:10.1136/ard.2008.096677
Lafyatis, R., O'Hara, C., Feghali-Bostwick, C. A., and Matteson, E. (2007). B cell infiltration in systemic sclerosis-associated interstitial lung disease. Arthritis Rheum. 56 (9), 3167–3168. doi:10.1002/art.22847
Leandro, M. J., Cambridge, G., Ehrenstein, M. R., and Edwards, J. C. (2006). Reconstitution of peripheral blood B cells after depletion with rituximab in patients with rheumatoid arthritis. Arthritis Rheum. 54 (2), 613–620. doi:10.1002/art.21617
Lepri, G., Avouac, J., Airo, P., Anguita Santos, F., Bellando-Randone, S., Blagojevic, J., et al. (2016). Effects of rituximab in connective tissue disorders related interstitial lung disease. Clin. Exp. Rheumatol. 34, 181–185.
Li, T., Guo, L., Chen, Z., Gu, L., Sun, F., Tan, X., et al. (2016). Pirfenidone in patients with rapidly progressive interstitial lung disease associated with clinically amyopathic dermatomyositis. Sci. Rep. 6, 33226. doi:10.1038/srep33226
Lo, C. K., Mertz, D., and Loeb, M. (2014). Newcastle-Ottawa scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 14, 45. doi:10.1186/1471-2288-14-45
Lynch, D. A. (2009). Lung disease related to collagen vascular disease. J. Thorac. Imaging 24 (4), 299–309. doi:10.1097/RTI.0b013e3181c1acec
Maher, T. M. (2014). Immunosuppression for connective tissue disease-related pulmonary disease. Semin. Respir. Crit. Care Med. 35 (2), 265–273. doi:10.1055/s-0034-1371531
Marie, I., Dominique, S., Janvresse, A., Levesque, H., and Menard, J. F. (2012). Rituximab therapy for refractory interstitial lung disease related to antisynthetase syndrome. Respir. Med. 106 (4), 581–587. doi:10.1016/j.rmed.2012.01.001
Marigliano, B., Soriano, A., Margiotta, D., Vadacca, M., and Afeltra, A. (2013). Lung involvement in connective tissue diseases: A comprehensive review and a focus on rheumatoid arthritis. Autoimmun. Rev. 12 (11), 1076–1084. doi:10.1016/j.autrev.2013.05.001
Mathai, S. C., and Danoff, S. K. (2016). Management of interstitial lung disease associated with connective tissue disease. BMJ Clin. Res. ed) 352, h6819. doi:10.1136/bmj.h6819
Md Yusof My, , Kabia, A., Darby, M., Lettieri, G., Beirne, P., Vital, E. M., et al. (2017). Effect of rituximab on the progression of rheumatoid arthritis-related interstitial lung disease: 10 years' experience at a single centre. Rheumatol. Oxf. Engl. 56 (8), 1348–1357. doi:10.1093/rheumatology/kex072
Mosca, M., Neri, R., and Bombardieri, S. (1999). Undifferentiated connective tissue diseases (UCTD): A review of the literature and a proposal for preliminary classification criteria. Clin. Exp. Rheumatol. 17 (5), 615–620.
Naqibullah, M., Shaker, S. B., Bach, K. S., and Bendstrup, E. (2015). Rituximab-induced interstitial lung disease: Five case reports. Eur. Clin. Respir. J. 2, 27178. doi:10.3402/ecrj.v2.27178
Narváez, J., Luch, J, L., Molina-Molina, M., Vicens-Zygmunt, V., Luburich, P., Yañez, M. A., et al. (2020). Rituximab as a rescue treatment added on mycophenolate mofetil background therapy in progressive systemic sclerosis associated interstitial lung disease unresponsive to conventional immunosuppression. Semin. Arthritis Rheum. 50 (5), 977–987. doi:10.1016/j.semarthrit.2020.08.004
Narváez, J., Robles-Pérez, A., Molina-Molina, M., Vicens-Zygmunt, V., Luburich, P., Yañez, M. A., et al. (2020). Real-world clinical effectiveness of rituximab rescue therapy in patients with progressive rheumatoid arthritis-related interstitial lung disease. Semin. Arthritis Rheum. 50 (5), 902–910. doi:10.1016/j.semarthrit.2020.08.008
Perosa, F., Prete, M., Racanelli, V., and Dammacco, F. (2010). CD20-depleting therapy in autoimmune diseases: From basic research to the clinic. J. Intern. Med. 267 (3), 260–277. doi:10.1111/j.1365-2796.2009.02207.x
Raghu, G., Collard, H. R., Egan, J. J., Martinez, F. J., Behr, J., Brown, K. K., et al. (2011). An official ATS/ERS/JRS/ALAT statement: Idiopathic pulmonary fibrosis: Evidence-based guidelines for diagnosis and management. Am. J. Respir. Crit. Care Med. 183 (6), 788–824. doi:10.1164/rccm.2009-040GL
Richeldi, L., Costabel, U., Selman, M., Kim, D. S., Hansell, D. M., Nicholson, A. G., et al. (2011). Efficacy of a tyrosine kinase inhibitor in idiopathic pulmonary fibrosis. N. Engl. J. Med. 365 (12), 1079–1087. doi:10.1056/NEJMoa1103690
Roofeh, D., Jaafar, S., Vummidi, D., and Khanna, D. (2019). Management of systemic sclerosis-associated interstitial lung disease. Curr. Opin. Rheumatol. 31 (3), 241–249. doi:10.1097/BOR.0000000000000592
Sari, A., Guven, D., Armagan, B., Erden, A., Kalyoncu, U., Karadag, O., et al. (2017). Rituximab experience in patients with long-standing systemic sclerosis-associated interstitial lung disease: A series of 14 patients. J. Clin. Rheumatol. 23 (8), 411–415. doi:10.1097/RHU.0000000000000584
Sem, M., Molberg, O., Lund, M. B., and Gran, J. T. (2009). Rituximab treatment of the anti-synthetase syndrome: A retrospective case series. Rheumatol. Oxf. Engl. 48 (8), 968–971. doi:10.1093/rheumatology/kep157
Sfikakis, P. P., Boletis, J. N., Lionaki, S., Vigklis, V., Fragiadaki, K. G., Iniotaki, A., et al. (2005). Remission of proliferative lupus nephritis following B cell depletion therapy is preceded by down-regulation of the T cell costimulatory molecule CD40 ligand: An open-label trial. Arthritis Rheum. 52 (2), 501–513. doi:10.1002/art.20858
Sfikakis, P. P., Souliotis, V. L., Fragiadaki, K. G., Moutsopoulos, H. M., Boletis, J. N., and Theofilopoulos, A. N. (2007). Increased expression of the FoxP3 functional marker of regulatory T cells following B cell depletion with rituximab in patients with lupus nephritis. Clin. Immunol. 123 (1), 66–73. doi:10.1016/j.clim.2006.12.006
Sharp, C., McCabe, M., Dodds, N., Edey, A., Mayers, L., Adamali, H., et al. (2016). Rituximab in autoimmune connective tissue disease-associated interstitial lung disease. Rheumatol. Oxf. Engl. 55 (7), 1318–1324. doi:10.1093/rheumatology/kew195
Sircar, G., Goswami, R. P., Sircar, D., Ghosh, A., and Ghosh, P. (2018). Intravenous cyclophosphamide vs rituximab for the treatment of early diffuse scleroderma lung disease: Open label, randomized, controlled trial. Rheumatol. Oxf. Engl. 57 (12), 2106–2113. doi:10.1093/rheumatology/key213
Smolen, J. S., Landewe, R., Bijlsma, J., Burmester, G., Chatzidionysiou, K., Dougados, M., et al. (2017). EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2016 update. Ann. Rheum. Dis. 76 (6), 960–977. doi:10.1136/annrheumdis-2016-210715
Solomon, J. J., and Fischer, A. (2015). Connective tissue disease-associated interstitial lung disease: A focused review. J. Intensive Care Med. 30 (7), 392–400. doi:10.1177/0885066613516579
Stone, J. H., Merkel, P. A., Spiera, R., Seo, P., Langford, C. A., Hoffman, G. S., et al. (2010). Rituximab versus cyclophosphamide for ANCA-associated vasculitis. N. Engl. J. Med. 363 (3), 221–232. doi:10.1056/NEJMoa0909905
Stroup, D. F., Berlin, J. A., Morton, S. C., Olkin, I., Williamson, G. D., Rennie, D., et al. (2000). Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-Analysis of observational studies in Epidemiology (MOOSE) group. Jama 283 (15), 2008–2012. doi:10.1001/jama.283.15.2008
Tashkin, D. P., Elashoff, R., Clements, P. J., Goldin, J., Roth, M. D., Furst, D. E., et al. (2006). Cyclophosphamide versus placebo in scleroderma lung disease. N. Engl. J. Med. 354 (25), 2655–2666. doi:10.1056/NEJMoa055120
Tashkin, D. P., Roth, M. D., Clements, P. J., Furst, D. E., Khanna, D., Kleerup, E. C., et al. (2016). Mycophenolate mofetil versus oral cyclophosphamide in scleroderma-related interstitial lung disease (SLS II): A randomised controlled, double-blind, parallel group trial. Lancet. Respir. Med. 4 (9), 708–719. doi:10.1016/S2213-2600(16)30152-7
Wang, Y., Xu, S. Q., Xu, J. H., and Ding, C. (2011). Treatment with etanercept in a patient with rheumatoid arthritis-associated interstitial lung disease. Clin. Med. Insights. Case Rep. 4, 49–52. doi:10.4137/CCRep.S8150
Keywords: connective tissue disease-associated interstitial lung disease, rituximab, efficacy, safety, meta-analysis
Citation: Xu L, Wang F and Luo F (2022) Rituximab for the treatment of connective tissue disease–associated interstitial lung disease: A systematic review and meta-analysis. Front. Pharmacol. 13:1019915. doi: 10.3389/fphar.2022.1019915
Received: 15 August 2022; Accepted: 17 October 2022;
Published: 28 October 2022.
Edited by:
Ariela Hoxha, University Hospital of Padua, ItalyReviewed by:
Theodoros Karampitsakos, General University Hospital of Patras, GreeceCopyright © 2022 Xu, Wang and Luo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Faping Wang, d2FuZ2Zwc2N1QGdtYWlsLmNvbQ==; Fengming Luo, ZmVuZ21pbmdsdW9Ab3V0bG9vay5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.