 Carlen Reyes1
Carlen Reyes1 Luz M León-Muñoz2Andrea Pistillo1Sigrún Alba Jóhannesdóttir Schmidt3,4Kasper Bruun Kristensen5Diana Puente1,6Ana LLorente-García7Consuelo Huerta-Álvarez8Anton Pottegård3
Luz M León-Muñoz2Andrea Pistillo1Sigrún Alba Jóhannesdóttir Schmidt3,4Kasper Bruun Kristensen5Diana Puente1,6Ana LLorente-García7Consuelo Huerta-Álvarez8Anton Pottegård3 Talita Duarte-Salles1*
Talita Duarte-Salles1*- 1Fundació Institut Universitari per a la Recerca a L'Atenció Primària de Salut Jordi Gol i Gurina (IDIAPJGol), Barcelona, Spain
- 2Delegation for the National Plan on Drugs, Ministry of Health, Madrid, Spain
- 3Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark
- 4Department of Dermatology, Aarhus University Hospital, Aarhus, Denmark
- 5Clinical Pharmacology, Pharmacy, and Environmental Medicine, Institute of Public Health, University of Southern Denmark, Odense, Denmark
- 6Universitat Autònoma de Barcelona, Bellaterra, Spain
- 7Pharmacoepiemiology and Pharmacovigilance Division, Spanish Agency for Medicines and Clinical Devices-AEMPS, Madrid, Spain
- 8Department of Public Health & Maternal and Child Health, Faculty of Medicine. Complutense University of Madrid-UCM, Madrid, Spain
Background: A previous study in Denmark suggested an increased melanoma risk associated with the use of flecainide.
Objective: To study the association between flecainide use and the risk of melanoma and non-melanoma skin cancer in Spain and Denmark.
Methods: We conducted a multi-database case–control study in (database/study period) Spain (SIDIAP/2005–2017 and BIFAP/2007–2017) and Denmark (Danish registries/2001–2018). We included incident cases of melanoma or non-melanoma skin cancer (NMSC) aged ≥18 with ≥2 years of previous data (≥10 years for Denmark) before the skin cancer and matched them to controls (10:1 by age and sex). We excluded persons with immunosuppression or previous cancer. We defined ever-use as any prescription fill and high-use as a cumulative dose of at least 200 g (reference: never-use). We categorized a cumulative dose for a dose–response assessment. We used conditional logistic regression to compute ORs (95% CI) adjusted for photosensitizing, anti-neoplastic, disease-specific drugs and comorbidities.
Results: The total numbers of melanoma/NMSC cases included were 7,809/64,230 in SIDIAP, 4,661/31,063 in BIFAP, and 27,978/152,821 in Denmark. In Denmark, high-use of flecainide was associated with increased adjusted ORs of skin cancer compared with never-use [melanoma: OR 1.97 (1.38–2.81); NMSC: OR 1.34 (1.15–1.56)]. In Spain, an association between high-use of flecainide and NMSC was also observed [BIFAP: OR 1.42 (1.04–1.93); SIDIAP: OR 1.19 (0.95–1.48)]. There was a non-significant dose–response pattern for melanoma in Denmark and no apparent dose–response pattern for NMSC in any of the three databases. We found similar results for ever-use of flecainide.
Conclusion: Flecainide use was associated with an increased risk of melanoma (Denmark only) and NMSC (Denmark and Spain) but without substantial evidence of dose–response patterns. Further studies are needed to assess for possible unmeasured confounders.
Introduction
The burden of skin cancer, comprising both melanoma and non-melanoma skin cancer (NMSC), has increased in the past decades (Saginala et al., 2021). In 2020, estimates from the global statistics (GLOBOCAN) identified 325,000 new cases of melanoma (1.7% of all cancer diagnoses) and positioned melanoma as the most lethal form of skin cancer in the world (Saginala et al., 2021). In Europe, the skin cancer incidence is marked by a latitudinal north–south gradient. For example, the annual rate of melanoma decreases from 50 per 100,000 in Denmark to 12 per 100,000 in Spain (ECIS, 2022).
The main risk factor for skin cancer is ultraviolet (UV) light exposure, which may explain the increased skin cancer risk and severity found among users of certain photosensitizing drugs (Gonçalo et al., 2011; de Vries et al., 2012; Dika et al., 2021). Among these are certain medications used for cardiovascular diseases such as antihypertensives (Schmidt et al., 2015a; Drucker et al., 2021) and antiarrhythmics (Monk, 1995; Hall et al., 2004; Maoz et al., 2009). In a hypothesis-generating screening study carried out in Denmark, the use of the classic antiarrhythmic flecainide was associated with a 2-fold increased risk of melanoma (Pottegård et al., 2016), with some evidence of a dose–response pattern.
Detailed and up-to-date data on the use of flecainide and its relation with skin cancer risk, including both melanoma and NMSC, are not available from Denmark nor from populations in South Europe. Framing skin cancer as a possible adverse effect of flecainide would allow prescribers to reinforce the preventive measures to treated patients. Therefore, the aim of this study was to assess the association between the use of flecainide and the incidence of melanoma and NMSC in adults from Denmark and Spain.
Materials and methods
Design
We conducted a nested case–control study, in three databases of two countries, namely the Danish nationwide health registries in Denmark and the SIDIAP and the BIFAP databases in Spain.
Data sources
In Denmark, we analyzed data gathered from five nationwide registries: the Danish Cancer Registry (Gjerstorff, 2011), the National Prescription Registry (Pottegård et al., 2017), the National Patient Registry (Schmidt et al., 2015), registries on educational level from Statistics Denmark (Jensen and Rasmussen, 2011), and the Civil Registration System (Schmidt et al., 2014). Linkage was achieved using the personal identification number, which is a unique identifier assigned to all Danish residents since 1968 (Pedersen, 2011). Virtually, all medical care in Denmark is supplied by the national health authorities, allowing true population-based register linkage studies covering all legal residents of Denmark.
In Spain, two databases were used: The SIDIAP (Sistema d’Informació per al Desenvolupament de la Investigació en Atenció Primària) and the BIFAP databases (Base de Datos para la Investigación Farmacoepidemiológica en Atención Primaria).
The SIDIAP is a large population-based database that gathers routinely collected anonymized healthcare records from nearly six million people (∼75% of the Catalan population) since 2005 (Recalde et al., 2022). Data include sociodemographic, lifestyle and anthropometric information, clinical diagnosis [International Classification of Diseases 10th revision (ICD-10)], laboratory test results, prescribed and dispensed medications, and hospital referrals, among others.
The BIFAP is a longitudinal population-based database that gathers electronic healthcare anonymized information recorded by general practitioners (GPs) and pediatricians belonging to the National Health System throughout Spain (http://bifap.aemps.es/) since 2001. Nine autonomous regions of Spain currently collaborate in this database providing information on lifestyle factors, clinical events, laboratory test results, specialist referrals, electronic prescriptions, and their dispensations in pharmacies. The BIFAP population is representative of the Spanish population in terms of age and sex. At the time of the study, the database covered a total of 7.8 million patients which represents 49 million person-years of follow-up. The mean follow-up of patients in the database was 6.3 years. The BIFAP database has been extensively described elsewhere (Maciá-Martínez et al., 2020).
Study population, selection of skin cancer cases, and population control
We included all individuals aged between 18 and 85 years old with an incident diagnosis of melanoma or NMSC between 1 January 2001 and 31 of December 2018, in the Danish Cancer Registry database, between the 1 January 2007 and the 31 December 2017 in the BIFAP database, and between 1 January 2006 and the 31 December 2017 in the SIDIAP database. To ensure sufficient follow-up, we required individuals to be registered for at least two consecutive years in the Spanish databases or to be alive at least 10 years prior to the index data for the Danish registries. Given that immunosuppression may increase the risk of skin cancer (International Agency for Research on Cancer (IARC), 2012), we excluded patients with an HIV diagnosis, an organ transplant (Danish population), and dispensation of azathioprine, cyclosporin, or mycophenolate mofetil. We excluded cases and controls with any previous cancer, except for those with previous NMSC in analyses of melanoma as an outcome (only in Denmark).
In Denmark, we included cases with a histologically verified skin cancer diagnosis in the Danish Cancer Registry using the ICD-10 codes. In SIDIAP, we identified cases through ICD-10-Clinical Modification codes linked to two regional population cancer registries available in Catalonia. In BIFAP, all skin cancer diagnoses were validated using an independent validation process which used a specific algorithm and a natural language processing procedure taking into account comments in the free text to validate the potential cases. All the ATC and ICD codes used to identify the variables are listed in Supplementary Table 1.
We selected controls with risk-set sampling in each database. For each case, we matched to up to 10 controls with the same sex and birth year (± 1 for the Spanish databases). We assigned controls on the same index date as the case to whom they were matched. Subjects were eligible for sampling as controls more than one time before possibly becoming cases. Thereby, the calculated odds ratios (ORs) are direct estimates of the incidence rate ratios (IRRs) that would have emerged from a cohort study in the source population.
Definition of the exposure to flecainide
We defined ever-use of flecainide as having filled at least one dispensation of flecainide (in BIFAP, we used dispensations unless these were not available in which case prescriptions were selected) before the index date. High-use of flecainide was defined as a cumulative dose of at least 200 g of flecainide (1,000 DDD (WHO, 2022)). For the dose–response analyses, we used the following pre-specified categories: ≤19 g, 20–99 g, 100–199 g, 200–399 g, and ≥400 g. In all exposure calculations, we discarded dispensations redeemed during the 2 years before the index date, as recent exposure to flecainide is unlikely to affect skin cancer development and in order to avoid reverse causation (Pottegård and Hallas, 2017).
Other variables and potential confounders
The list of confounders included comorbid conditions such as diabetes, chronic obstructive pulmonary disease, myocardial infarction (BIFAP and the Danish registries), chronic kidney disease, and alcohol-related disorders (Danish registries), the Charlson Comorbidity Index derived from the prevalence of 14 chronic conditions (SIDIAP and the Danish registries) and related disease-specific drugs, as well as those drugs identified as having photosensitizing properties [retinoids, photosensitizing antibiotics including tetracycline, macrolides, and aminoquinolines, hydrochlorothiazide (Danish registries), amiodarone, and methoxypsoralen/PUVA therapy (Robinson et al., 2013; Schmidt et al., 2015a; Gallelli et al., 2022)] or anti-neoplastic effects [aspirin, NSAIDs, oral corticosteroids, and statins (Friis et al., 2015)]. We defined drug exposure as at least two prescriptions on separate dates, and the comorbid conditions were selected if registered as primary or secondary discharge or outpatient diagnoses. Other confounders gathered included smoking habits (never, current, and former smokers; only available in SIDIAP and BIFAP) and socioeconomic status defined as the highest education level achieved [basic (10 years), medium (11–13 years), higher (>13 years), or unknown] in the Danish registries or the MEDEA deprivation index in SIDIAP (categorized in quintiles U1 for the least deprived and U5 for the most deprived) (Domínguez-Berjón et al., 2008). For drugs and comorbid conditions, information within 2 years prior to the index date was disregarded.
Statistical analysis
All analyses followed a conventional matched case–control approach. We computed the frequency and proportion of cases and controls within categories of both flecainide exposure and covariates. We used conditional logistic regression analysis to compute odds ratios (ORs) with 95% confidence intervals (CIs) for the association of NMSC or melanoma with flecainide use adjusted for the predefined potential confounders. In addition to the predefined categories of cumulative use, we carried out a formal dose–response test by restricting to flecainide ever-users and estimating the incremental OR for each 100 g of flecainide using logistic regression while also adjusting for sex, age, and index year. In all analyses, we analyzed NMSC and melanoma separately and never-use of flecainide was the reference group unless stated otherwise. We also calculated adjusted OR according to age (<50, 50–59, 60–74, and 75 +) and sex categories with ever-use as exposure for the Spanish databases and with high-use as exposure for the Danish databases. We performed all the analyses locally and for each database separately. We performed analyses in Stata Release 14.2 (StataCorp, College Station, TX, United States) for the BIFAP database, Stata Release 17.0 (StataCorp, College Station, TX, United States) for the Danish registries, and R version 4.0.3 for SIDIAP.
The study was approved by the Danish Data Protection Agency. According to the Danish law, studies based solely on registered data do not require approval from an ethics review board (Thygesen et al., 2011). We obtained approval for all observational research using SIDIAP data from a local ethics committee (Clinical Research Ethics Committee of the IDIAP Jordi Gol) and for the study in BIFAP from the BIFAP Scientific Committee (Ref #01-2018).
Results
The final population included in the study is reported in the Supplementary Figures S1 and S2 (for the Danish and Spanish population, respectively). Baseline characteristics of the cases and controls with and without melanoma and NMSC are reported in Table 1. A total of 4,661, 7,809, and 27,978 cases of melanoma and 31,063, 64,230, and 152,821 cases of NMSC and their matched controls were included in the BIFAP, SIDIAP, and Danish registries, respectively. Compared with patients with melanoma, those with NMSC were on average 8–12 years older, were more likely to be men (48% vs. 44%–45%), and had a higher comorbidity burden. The vast majority of patients analyzed had never used flecainide (∼99% of cases); however, among those who did, flecainide was more frequently prescribed among NMSC than melanoma in BIFAP (0.84% vs. 0.60%) and SIDIAP (0.79% vs. 0.50%) and at higher cumulative dosages.
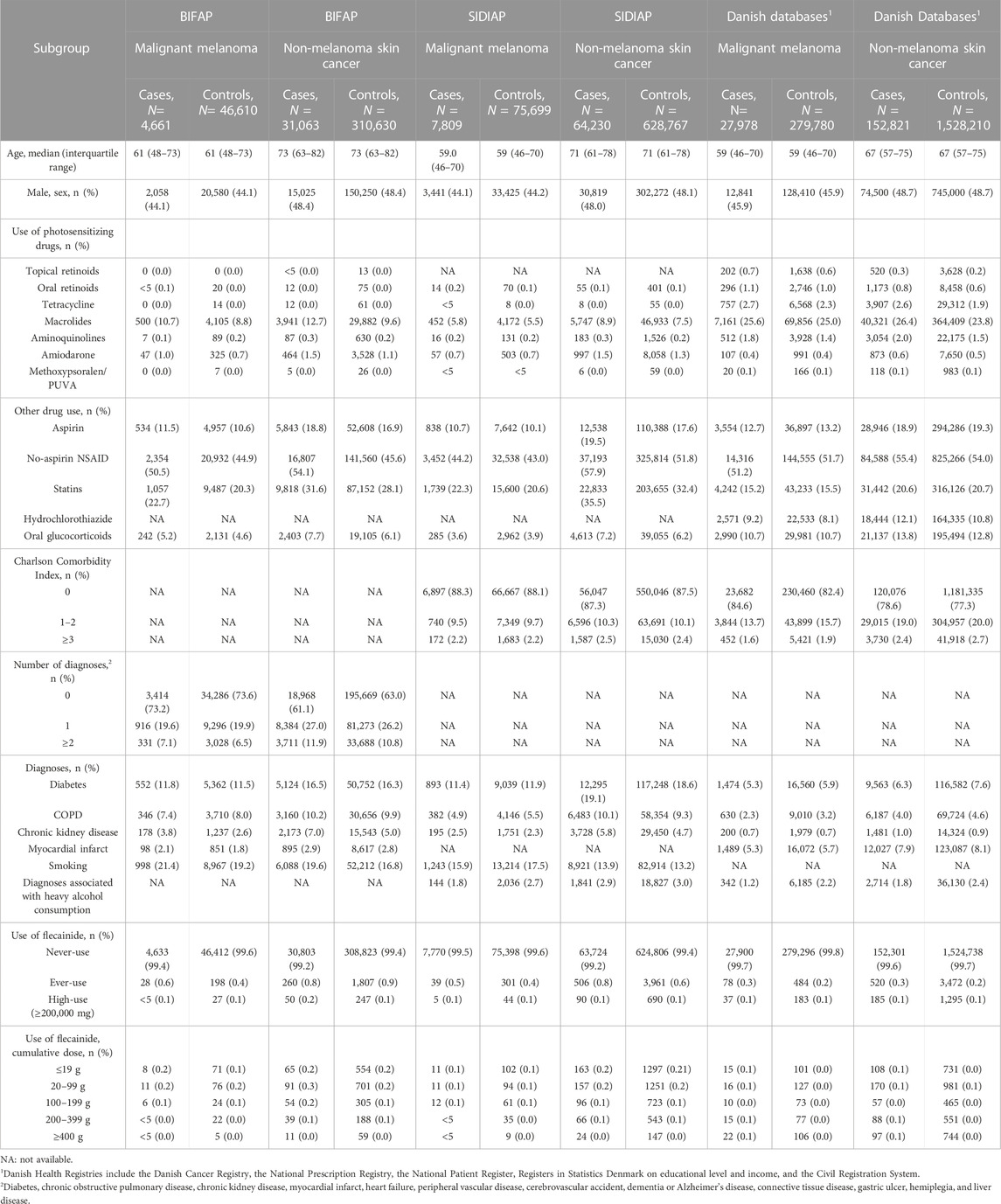
TABLE 1. Characteristics of melanoma and non-melanoma skin cancer cases and matched controls in BIFAP, SIDIAP, and Danish databases.
The association between the use of flecainide and the risk of melanoma and NMSC is reported in Table 2. Ever- and high-use of flecainide was associated with an increased risk of melanoma only in the Danish registries (adjusted OR of 1.58 (1.24–2.01) for ever-use; OR 1.97 (1.38–2.81) for high-use); however, there was no substantial variation in risk in analyses with cumulative flecainide dose as a categorical variable. Also, when restricting the analyses to ever-users of flecainide, the adjusted ORs for each 100 g increment in cumulative flecainide dose were inconclusive in all three databases [ORs of 1.04 (0.97–1.13) in Denmark, 0.96 (0.63–1.46) in BIFAP, and 1.05 (0.74–1.41) in SIDIAP].
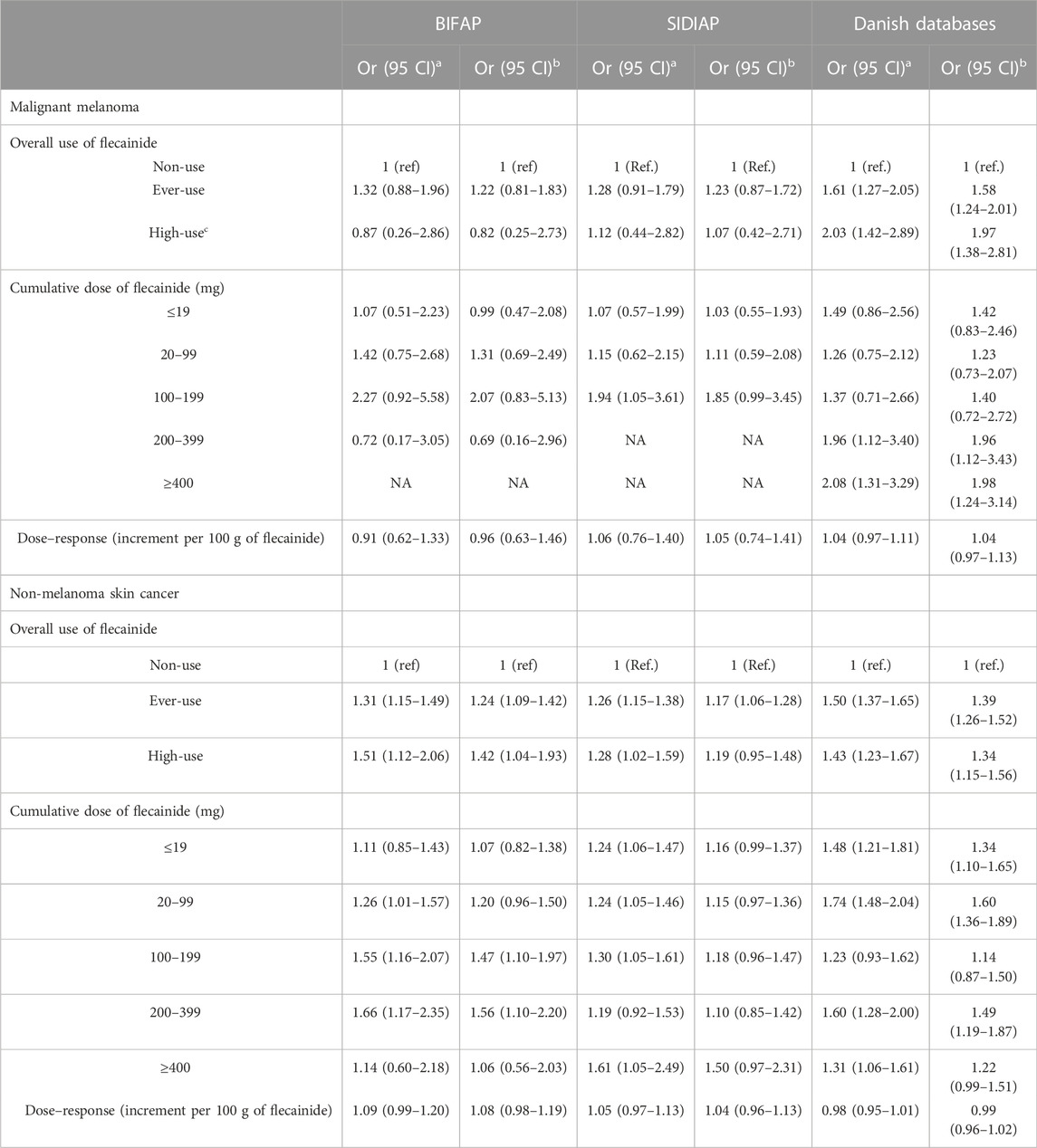
TABLE 2. Association between exposure to flecainide and risk of skin cancer, according to cumulative amount of flecainide use.
Compared with non-users, users of flecainide (ever- and high-use) were found to have a moderate increased risk of NMSC in all databases with adjusted ORs between 1.17 and 1.39 for ever-use and 1.19 and 1.42 for high-use. However, analyses by cumulative dose in the different databases showed no consistent dose–response patterns in associations. When restricting the analyses to ever-use of flecainide, the dose–response association was also not conclusive with ORs for each incremental cumulative dose increase of 100 g of flecainide were 0.99 (0.96–1.02) in Denmark, 1.08 (0.98–1.19) in BIFAP, and 1.04 (0.96–1.13) in SIDIAP.
The association between the use of flecainide and the risk of melanoma and NMSC stratified by age and sex was carried out with ever-use as exposure for the Spanish databases (Table 3) and with high-use as exposure for the Danish databases (Table 4). In general, the results stratified by age showed the highest estimates in the youngest age groups, but the precision was limited as reflected in the overlapping confidence intervals. When stratified by sex, all databases showed inconsistent results for both melanoma and NMSC; a higher risk of NMSC was found in male patients in the Danish databases, OR of 1.41 (1.16–1.70), and in female patients in the SIDIAP database, OR of 1.19 (1.05–1.36). In Spain, no association was observed between the ever-use of flecainide and the risk of melanoma stratified by sex, and a similar increased risk of melanoma was found in both male and female patients in Denmark.
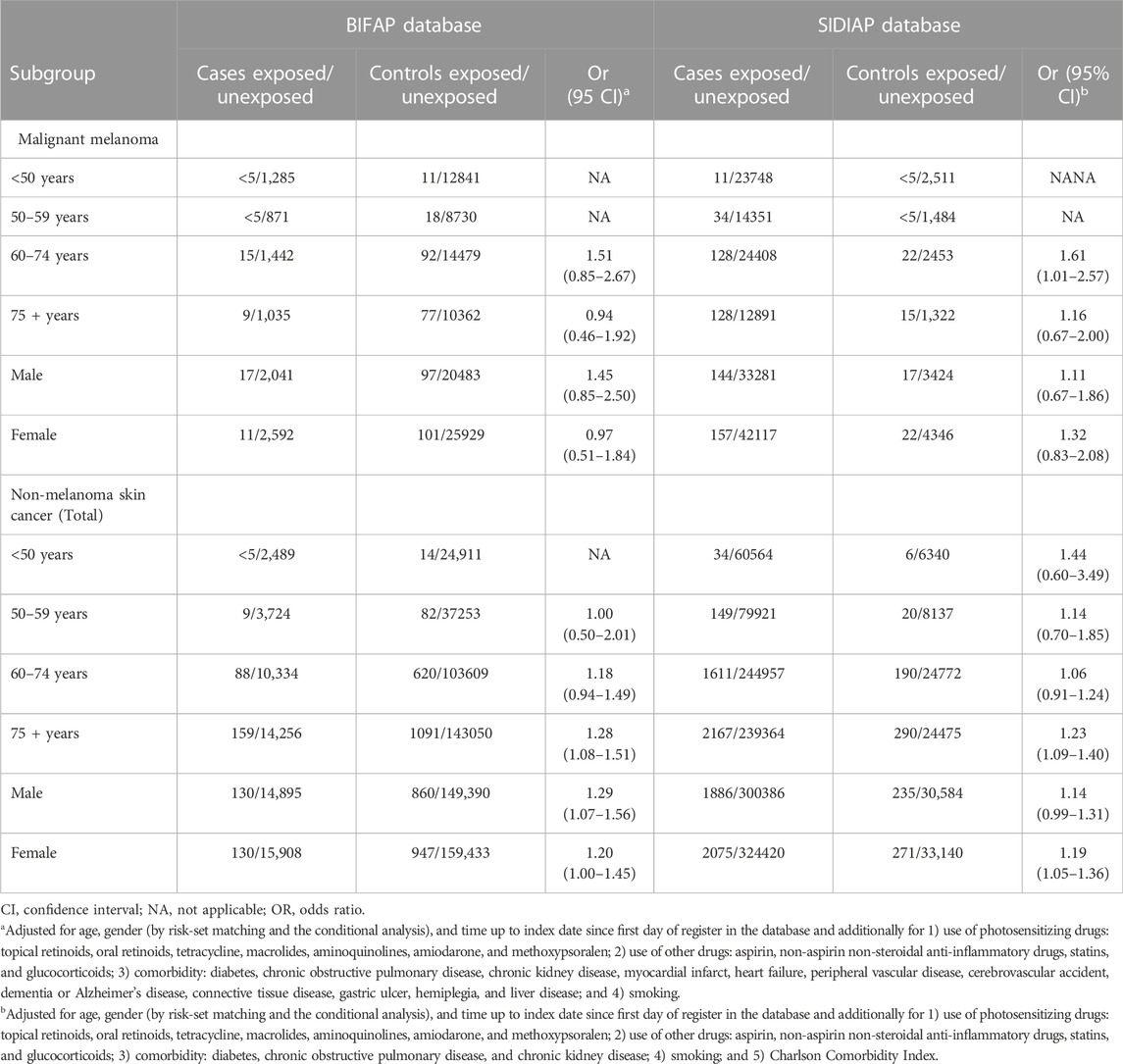
TABLE 3. Association between ever-use of flecainide and risk of skin cancer, according to patient subgroups in the Spanish databases (SIDIAP and BIFAP). Reference: Never-users of flecainide in each subgroup (unexposed).
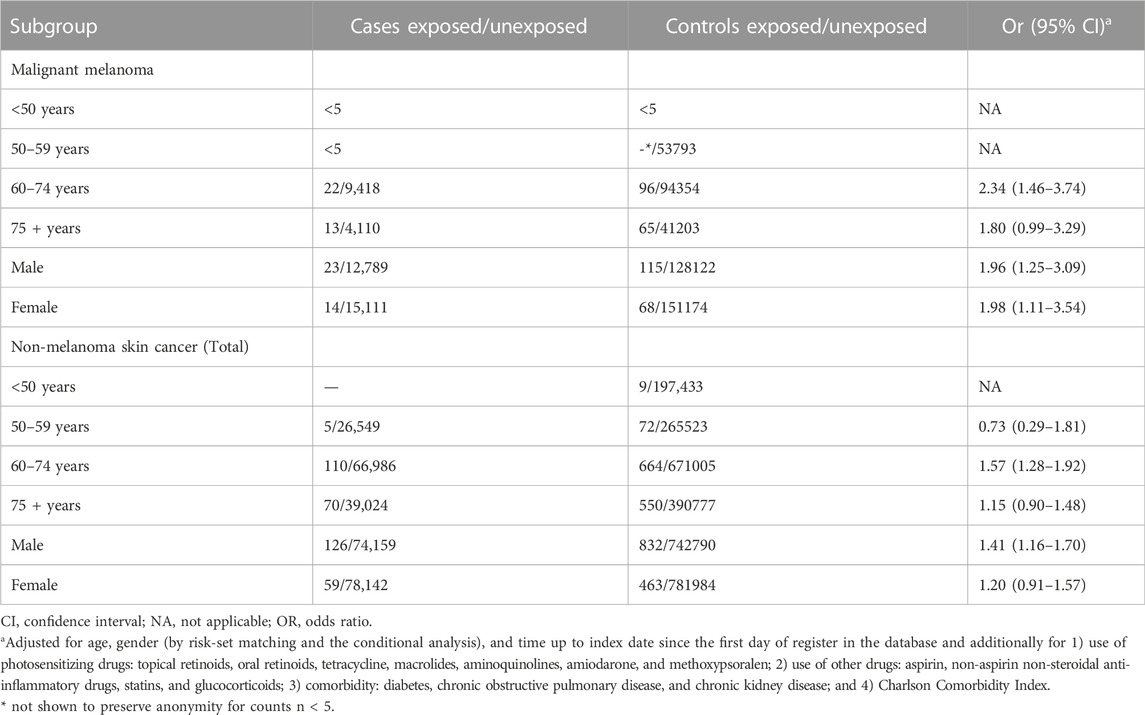
TABLE 4. Association between high-use of flecainide and risk of skin cancer, according to patient subgroups in the Danish databases. Reference: Never-users of flecainide in each subgroup (unexposed).
Discussion
In this multi-database population-based case–control study, we found an association between the use of flecainide and risk of melanoma (Denmark only) and NMSC (Denmark and Spain), but with no clear dose–response pattern in any of the analyses.
Although many antiarrhythmics are known to have photosensitizing properties and photosensitivity has been related to an increased risk of skin cancers (Robinson et al., 2013), the few studies that have assessed the associated risk of skin cancer with the intake of these drugs found conflictive results; while case reports support an increased risk of NMSC associated with amiodarone (Monk, 1995; Hall et al., 2004; Maoz et al., 2009), two large observational studies from Taiwan and Denmark found no association between the use of amiodarone and the overall risk of skin cancer (Su et al., 2013; Rasmussen et al., 2020). No previous study has analyzed the risk of melanoma and NMSC associated with the intake of other antiarrhythmics, such as flecainide, nor has it analyzed the risk according to the cumulative exposure of the drug.
The increased melanoma risk found in Denmark (up to 2-fold among high-users of flecainide), but not in Spain; in the current study, it could be explained by differences in environmental factors (i.e., UV exposure) and genetic and phenotypic differences (e.g., skin pigmentation) as such factors would modify the proposed photosensitizing effects of flecainide (ECIS, 2021). Thus, the skin pigmentation difference, with the Danish having fairer skin compared with the Spanish, could make them more prone to sunburn at lower sunlight exposure levels, increasing the risk of melanoma (Tuohimaa et al., 2007). This increased risk could be further accentuated with the use of a photosensitizing drug such as flecainide, partly explaining our results. Conversely, it has been suggested that NMSC is more related to the cumulative sunlight exposure, rather than to episodic sunburns, which could be increased by the use of flecainide and could explain the overall risk found in both countries.
When analyzing the cumulative exposure of flecainide, an association was observed between doses ≥200 mg and melanoma in Denmark. Although the association found was statistically significant, the clinical implications of it are not clear; there is no consistent pattern with increasing cumulative doses of flecainide. Similarly, the dose–response patterns were not apparent for NMSC which may indicate the existence of unmeasured confounders. One of these could be the socioeconomic status (SES); high SES has been associated both with a higher risk of being diagnosed with skin cancer (Doherty et al., 2010) and a greater likelihood of being prescribed an antiarrhythmic drug (Eberly et al., 2021). In this study, although the information related to SES was available for SIDIAP (through the MEDEA deprivation index) and the Danish registries (through the level of education) (data not shown), the lack of uniformity in the data prevented us to adjust for it. In SIDIAP, a higher proportion of skin cancer (19.3% of melanoma and 16.2% of NMSC) was observed among the least deprived compared with the most deprived (9.9% of melanoma and 8.0% of NMSC). Similarly, in Denmark, a higher proportion of skin cancer (74.5% of melanoma and 68.6% of NMSC) was observed among those who had achieved a medium/higher education compared with those who had achieved a short education (24.1% for melanoma and 29.3% for NMSC). This suggests that socioeconomic status could have influenced our results.
The main advantage of the study is the multinational approach, investigating the association between the use of flecainide and non-melanoma and melanoma skin cancer in two countries in which different ethnicities/skin types and different UV exposure patterns can be assumed, and with potential different utilization patterns of flecainide. Furthermore, data from the nationwide Danish health registries, SIDIAP, and BIFAP are generally considered to be of high validity and well suited for epidemiological research. The main limitation of the study is the lack of direct or indirect measures of UV exposure, as well as the lack of uniformity gathering the socioeconomic status which prevented us to adjust to it. There is no reason to suspect that users of flecainide will differ substantially from the background population regarding sun exposure habits and the likely impact of this factor is thus expected to be limited within each database. Underestimation of the incidence of skin cancer in primary care databases is also possible which could have contributed to the underestimation of the cases. Other potential limitation in BIFAP is the use of prescription information for drug exposure when drug dispensation was not available which could have overestimated our intake of flecainide. However, given that we found similar results compared with the other Spanish database (SIDIAP) in where only dispensations were collected, the effect of this overestimation is likely to be minimal. At last, information on histology or localization was not examined.
Conclusion
Flecainide use was associated with an increased risk of melanoma (Denmark only) and NMSC, but without substantial evidence of dose–response patterns. In Spain, flecainide use was associated with an increased risk of NMSC with no dose–response pattern. Further studies are needed assessing for possible unmeasured confounders.
Data availability statement
Data partners contributing to this study remain custodians of their individual patient-level health information. Due to data protection regulations, individual level data from this study and administrative registries cannot be shared by the authors. Data access can be granted to Danish scientific and university-based organizations after application to Statistics Denmark (www.sundhedsdatastyrelsen.dk). According to the Spanish law and the IDIAP JGol Ethical Review Board, it is prohibited to publicly share data with personal information. Requests to access the Spanish datasets should be directed to https://www.sidiap.org/index.php/solicituds for the SIDIAP database and to www.bifap.org for the BIFAP database.
Ethics statement
The study was approved by the Danish Data Protection Agency. According to Danish law, studies based solely on registered data do not require approval from an ethics review board (Thygesen et al., 2011). We obtained approval for all observational research using SIDIAP data from a local ethics committee (Clinical Research Ethics Committee of the IDIAP Jordi Gol) and for the study in BIFAP from the BIFAP Scientific Committee (Ref #01-2018).
Author contributions
CR, TD-S, LL-M, APi, DP, ALL-G, CH-A, KK, APo, and SJ provided substantial contributions to the conception or design, analysis, and interpretation of data for the work. CR, KK, LL-M, CH-A, APi, and DP drafted the initial manuscript, and SJ, APo, and the rest of the authors revised the manuscript critically for important intellectual content. All authors approved the final version of the manuscript and TD-S, CH-A, and KK agreed to be accountable for all aspects of the work regarding their respective databases and ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Acknowledgments
The authors would like to acknowledge the excellent collaboration of the primary care practitioners and pediatricians and also the support of the regional authorities participating in the BIFAP database. BIFAP is a database fully funded by the AEMPS. LL-M and CH-A were employees of the AEMPS when this study started and the first part of the study was performed there. They no longer work for the AEMPS. TDS acknowledges receiving financial support from the Instituto de Salud Carlos III (ISCIII; Miguel Servet 2021: CP21/00023) which is cofunded by the European Union.
Conflict of interest
SJ reports speaker’s honoraria from GlaxoSmithKline Pharma. AP reports participation in research projects funded by Alcon, Almirall, Astellas, AstraZeneca, Boehringer Ingelheim, Novo Nordisk, Servier and LEO Pharma, all regulator-mandated phase IV studies, and all with funds paid to the institution where he was employed (no personal fees) and with no relation to the work reported in this paper.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2022.1002451/full#supplementary-material
References
de Vries, E., Trakatelli, M., Kalabalikis, D., Ferrandiz, L., Ruiz-de-Casas, A., Moreno-Ramirez, D., et al. (2012). Known and potential new risk factors for skin cancer in European populations: A multicentre case-control study. Br. J. Dermatol. 167, 1–13. doi:10.1111/j.1365-2133.2012.11081.x
Dika, E., Maestroeni, S., Lambertini, M., Scarfi, F., Patrizi, A., Veronesi, G., et al. (2021). The chronic use of multiple photosensitizing drugs is associated with breslow thickness in female melanoma patients: A bicentric retrospective study. J. Am. Acad. Dermatol. 84, 1762–1764. doi:10.1016/j.jaad.2020.11.050
Doherty, V. R., Brewster, D. H., Jensen, S., and Gorman, D. (2010). Trends in skin cancer incidence by socioeconomic position in Scotland, 1978-2004. Br. J. Cancer 102, 1661–1664. doi:10.1038/sj.bjc.6605678
Domínguez-Berjón, M. F., Borrell, C., Cano-Serral, G., Esnaola, S., Nolasco, A., Pasarin, M. I., et al. (2008). Constructing a deprivation index based on census data in large Spanish cities (the MEDEA project). Gac. Sanit. 22, 179–187. doi:10.1157/13123961
Drucker, A. M., Hollestein, L., Na, Y., Weinstock, M. A., Li, W. Q., Abdel-Qadir, H., et al. (2021). Association between antihypertensive medications and risk of skin cancer in people older than 65 years: A population-based study. CMAJ 193, E508–E516. doi:10.1503/cmaj.201971
Eberly, L. A., Garg, L., Yang, L., Markman, T. M., Nathan, A. S., Eneanya, N. D., et al. (2021). Racial/ethnic and socioeconomic disparities in management of incident paroxysmal atrial fibrillation. JAMA Netw. Open 4, e210247. doi:10.1001/jamanetworkopen.2021.0247
ECIS (2022). Ecis - European cancer information System. © European Comission. last Available at: https://ecis.jrc.ec.europa.eu (Accessed 01 14, 2022).
ECIS (2021). “Ecis – European cancer information System,” in Skin melanoma burden in EU-27. Available at: https://ecis.jrc.ec.europa.eu (Accessed May 15, 2021).
Friis, S., Kesminiene, A., Espina, C., Auvinen, A., Straif, K., and Schuz, J. (2015). European Code against Cancer 4th Edition: Medical exposures, including hormone therapy, and cancer. Cancer Epidemiol. 39, S107–S119. doi:10.1016/j.canep.2015.08.003
Gallelli, L., Cione, E., Siniscalchi, A., Vasta, G., Guerra, A., Scaramuzzino, A., et al. (2022). Is there a link between non melanoma skin cancer and hydrochlorothiazide? Curr. Drug Saf. 17, 211–216. doi:10.2174/1574886316666211103164412
Gjerstorff, M. L. (2011). The Danish cancer Registry. Scand. J. Public Health 39, 42–45. doi:10.1177/1403494810393562
Gonçalo, M. (2011). “Phototoxic and photoallergic reactions,” in Contact dermatitis. Editors J. Johansen, P. Frosch, and J. P. Lepoittevin (Berlin, Heidelberg: Springer). doi:10.1007/978-3-642-03827-3_18
Hall, M. A., Annas, A., Nyman, K., Talme, T., and Emtestam, L. (2004). Basalioma after amiodarone therapy-not only in Britain. Br. J. Dermatol. 151, 932–933. doi:10.1111/j.1365-2133.2004.06193.x
International Agency for Research on Cancer (IARC) (2012). Pharmaceuticals. IARC Monographs on the evaluation of carcinogenic risks to humans, 100A. Lyon: International Agency for Research Cancer.
Jensen, V. M., and Rasmussen, A. W. (2011). Danish education registers. Scand. J. Public Health 39, 91–94. doi:10.1177/1403494810394715
Maciá-Martínez, M. A., Gil, M., Huerta, C., Martín-Merino, E., Álvarez, A., Bryant, V., et al. (2020). Base de Datos para la Investigación Farmacoepidemiológica en Atención Primaria (BIFAP): A data resource for pharmacoepidemiology in Spain. Pharmacoepidemiol. Drug Saf. 29, 1236–1245. doi:10.1002/pds.5006
Maoz, K. B., Dvash, S., Brenner, S., and Brenner, S. (2009). Amiodarone-induced skin pigmentation and multiple basal-cell carcinomas. Int. J. Dermatol. 48, 1398–1400. doi:10.1111/j.1365-4632.2008.03819.x
Monk, B. E. (1995). Basal cell carcinoma following amiodarone therapy. Br. J. Dermatol. 133, 148–149. doi:10.1111/j.1365-2133.1995.tb02515.x
Pedersen, C. B. (2011). The Danish Civil registration System. Scand. J. Public Health 39, 22–25. doi:10.1177/1403494810387965
Pottegård, A., Friis, S., Christensen, R. D., Habel, L. A., Gagne, J. J., and Hallas, J. (2016). Identification of associations between prescribed medications and cancer: A nationwide screening study. EBioMedicine 7, 73–79. doi:10.1016/j.ebiom.2016.03.018
Pottegård, A., and Hallas, J. (2017). New use of prescription drugs prior to a cancer diagnosis. Pharmacoepidemiol. Drug Saf. 26, 223–227. doi:10.1002/pds.4145
Pottegård, A., Schmidt, S. A. J., Wallach-Kildemoes, H., Sørensen, H. T., Hallas, J., and Schmidt, M. (2017). Data resource profile: The Danish national prescription Registry. Int. J. Epidemiol. 46, 798–798f. doi:10.1093/ije/dyw213
Rasmussen, P. V., Dalgaard, F., Gislason, G. H., Torp-Pedersen, C., Piccini, J., Martin, H. R., et al. (2020). Amiodarone treatment in atrial fibrillation and the risk of incident cancers: A nationwide observational study heart. Rhythm 17, 560–566. doi:10.1016/j.hrthm.2019.11.025
Recalde, M., Rodríguez, C., Burn, E., Far, M., García, D., Carrere-Molina, J., et al. (2022). Data resource profile: The information System for research in primary care (SIDIAP). Int. J. Epidemiol. Online ahead of print, dyac068. doi:10.1093/ije/dyac068
Robinson, S. N., Zens, M. S., Perry, A. E., Spencer, S. K., Duell, E. J., and Karagas, M. R. (2013). Photosensitizing agents and the risk of non-melanoma skin cancer: A population-based case-control study. J. Invest. Dermatol. 133, 1950–1955. doi:10.1038/jid.2013.33
Saginala, K., Barsouk, A., Aluru, J. S., Rawla, P., and Barsouk, A. (2021). Epidemiology of bladder cancer. Med. Sci. 9, 15. doi:10.3390/medsci8010015
Schmidt, M., Pedersen, L., and Sørensen, H. T. (2014). The Danish Civil registration System as a tool in epidemiology. Eur. J. Epidemiol. 29, 541–549. doi:10.1007/s10654-014-9930-3
Schmidt, M., Schmidt, S. A., Sandegaard, J. L., Ehrenstein, V., Pedersen, L., and Sorensen, H. T. (2015). The Danish national patient Registry: A review of content, data quality, and research potential. Clin. Epidemiol. 7, 449–490. doi:10.2147/CLEP.S91125
Schmidt, S. A., Schmidt, M., Mehnert, F., Lemeshow, S., and Sørensen, H. T. (2015). Use of antihypertensive drugs and risk of skin cancer. J. Eur. Acad. Dermatol. Venereol. 29, 1545–1554. doi:10.1111/jdv.12921
Su, V. Y., Hu, Y. W., Chou, K. T., Ou, S. M., Lee, Y. C., Lin, E. Y. H., et al. (2013). Amiodarone and the risk of cancer: A nationwide population-based study. Cancer 119, 1699–1705. doi:10.1002/cncr.27881
Thygesen, L. C., Daasnes, C., Thaulow, I., and Brønnum-Hansen, H. (2011). Introduction to Danish (nationwide) registers on health and social issues: Structure, access, legislation, and archiving. Scand. J. Public Health 39, 12–16. doi:10.1177/1403494811399956
Tuohimaa, P., Pukkala, E., Scélo, G., Olsen, J. H., Brewster, D. H., Hemminki, K., et al. (2007). Does solar exposure, as indicated by the non-melanoma skin cancers, protect from solid cancers: vitamin D as a possible explanation. Eur. J. Cancer 43, 1701–1712. doi:10.1016/j.ejca.2007.04.018
Keywords: case-control studies, flecainide, skin neoplasm, database, melanoma
Citation: Reyes C, León-Muñoz LM, Pistillo A, Jóhannesdóttir Schmidt SA, Kristensen KB, Puente D, LLorente-García A, Huerta-Álvarez C, Pottegård A and Duarte-Salles T (2022) Flecainide and risk of skin neoplasms: Results of a large nested case–control study in Spain and Denmark. Front. Pharmacol. 13:1002451. doi: 10.3389/fphar.2022.1002451
Received: 25 July 2022; Accepted: 29 November 2022;
Published: 22 December 2022.
Edited by:
Elisabetta Poluzzi, University of Bologna, ItalyReviewed by:
Emi Dika, University of Bologna, ItalyTanja Mueller, University of Strathclyde, United Kingdom
Copyright © 2022 Reyes, León-Muñoz, Pistillo, Jóhannesdóttir Schmidt, Kristensen, Puente, LLorente-García, Huerta-Álvarez, Pottegård and Duarte-Salles. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Talita Duarte-Salles, dGR1YXJ0ZUBpZGlhcGpnb2wub3Jn