 Jason B. Giles
Jason B. Giles Elise C. Miller
Elise C. Miller Heidi E. Steiner
Heidi E. Steiner Jason H. Karnes
Jason H. Karnes
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pharmacol., 21 January 2022
Sec. Pharmacogenetics and Pharmacogenomics
Volume 12 - 2021 | https://doi.org/10.3389/fphar.2021.812830
This article is part of the Research TopicInsights in Pharmacogenetics and Pharmacogenomics: 2021View all 11 articles
Heparin-induced thrombocytopenia (HIT) is an unpredictable, complex, immune-mediated adverse drug reaction associated with a high mortality. Despite decades of research into HIT, fundamental knowledge gaps persist regarding HIT likely due to the complex and unusual nature of the HIT immune response. Such knowledge gaps include the identity of a HIT immunogen, the intrinsic roles of various cell types and their interactions, and the molecular basis that distinguishes pathogenic and non-pathogenic PF4/heparin antibodies. While a key feature of HIT, thrombocytopenia, implicates platelets as a seminal cell fragment in HIT pathogenesis, strong evidence exists for critical roles of multiple cell types. The rise in omic technologies over the last decade has resulted in a number of agnostic, whole system approaches for biological research that may be especially informative for complex phenotypes. Applying multi-omics techniques to HIT has the potential to bring new insights into HIT pathophysiology and identify biomarkers with clinical utility. In this review, we review the clinical, immunological, and molecular features of HIT with emphasis on key cell types and their roles. We then address the applicability of several omic techniques underutilized in HIT, which have the potential to fill knowledge gaps related to HIT biology.
Heparin is a widely used anticoagulant indicated for a broad range of diseases and procedures. Approximately one third of all hospitalized patients in the United States receive heparin therapy (Campbell et al., 2000). This frequency of administration is due in part to multiple pharmacologic benefits of heparin, including immediate onset of action, rapid reversibility, and relative ease of titration (Bauer et al., 1997). However, these advantages are potentially offset by the immune-mediated complication, heparin-induced thrombocytopenia (HIT). HIT occurs in 0.2–2.7% of patients exposed to heparin anticoagulants and this risk increases in patients undergoing cardiac surgery (Warkentin et al., 1995; Warkentin et al., 2000; Girolami et al., 2003; Martel et al., 2005; Smythe et al., 2007). Despite the high prevalence and potentially life-threatening prognosis of this immune-mediated adverse drug reaction (ADR), the pathophysiology of HIT is still poorly understood making it difficult to predict and prevent.
HIT pathogenesis is initiated when heparin molecules, bound to circulating Platelet Factor 4 (PF4) proteins, are recognized by immunoglobulin G (IgG) antibodies (Kelton et al., 1994). These PF4/heparin antibodies then engage with platelets, leading to platelet activation and ultimately thrombocytopenia. Despite extensive research efforts towards understanding the immunopathology of HIT, fundamental knowledge gaps persist regarding HIT etiology (Cuker 2011; Greinacher et al., 2011; Karnes 2018). The HIT immunogen, the roles of antigen presenting cells and T-cells, and the B cell subtypes that produce the antibody remain unknown (Arepally 2017). The contributing role of non-platelet cell types in HIT, the interactions between cell types (platelets, monocytes, neutrophils, T-cells, etc.), and the heterogeneity of cell types intrinsic to HIT have yet to be fully resolved. Furthermore, the clinical significance of non-pathogenic PF4/heparin antibodies and the molecular basis that distinguishes them from pathogenic PF4/heparin antibodies remain unclear (Khandelwal and Arepally 2016). Transgenic mouse models (Zheng et al., 2015; Tutwiler et al., 2016; Perdomo et al., 2019), microfluidics devices (Tutwiler et al., 2016), and in vitro work on isolated cells (Kasthuri et al., 2012; Zhou et al., 2016) including platelets, peripheral blood mononuclear cells (PBMCs) (Kasthuri et al., 2012), and neutrophils (Duarte et al., 2019; Lelliott et al., 2020) have previously been employed to understand the pathophysiology of HIT. Although informative, prior targeted molecular approaches have not fully identified the mechanisms of HIT, likely due to the complicated and unusual nature of the HIT immune response. The rise in omics and “Big Data” over the last decade has resulted in a number of agnostic, whole system approaches for biological research that are especially informative for complex phenotypes. The common omics disciplines including genomics, transcriptomics, proteomics, metabolomics, and metagenomics, all have made great strides to answer questions in a wide range of biological topics. In the HIT field, however, these techniques have been under-utilized with studies employing only genome-wide association (Karnes et al., 2015; Karnes et al., 2017a; Witten et al., 2018) and array-based transcriptomic (Haile et al., 2017) approaches. This review will outline the current understanding of HIT pathogenesis within the context of specific cell types. This review will then evaluate omics techniques which might answer many unresolved questions related to HIT pathogenesis.
In contrast to most immune-mediated ADRs, the immune response in HIT is atypical and transient (Karnes et al., 2019). HIT is characterized by a fall in platelets (thrombocytes), 5–14 days after exposure to heparin (Prince and Wenham 2018). Mortality associated with HIT can reach 30% (Franchini 2005; Martel et al., 2005). PF4/heparin antibodies are necessary but not sufficient for HIT to occur, and these antibodies are typically produced 5–10 days after heparin exposure (Reilly et al., 2001; Staibano et al., 2017). IgG antibodies bind to PF4/heparin complexes to form ultra-large complexes (ULCs). These PF4/heparin antibodies are rarely detected in healthy individuals, with one study identifying ∼3% (Khandelwal and Arepally 2016) of the general population had detectable antibodies, using an optical density (OD) threshold of 0.4. A second study corroborated these findings and observed that 4.4% of healthy patients had antibodies against PF4/heparin (OD threshold = 0.5) (Krauel et al., 2011). In patients taking heparin, PF4/heparin antibodies are seen in 8–50% of patients (Arepally, 2017).
Up to half of patients with confirmed HIT experience thromboembolic complication including limb-threatening and life-threatening venous or arterial thrombosis (Prince and Wenham 2018). When thromboembolic events occur, the condition is sometimes referred to as HIT-associated thrombosis or HIT with thrombosis (HITT). In many patients, thromboembolic complications occur before a decrease in platelet count is observed (Prince and Wenham 2018). Less common presentations can also occur, such as skin necrosis and venous limb gangrene (Arepally 2017). Female sex, intravenous route of administration, and major surgery increase the risk of HIT (Arepally and Ortel 2010; Linkins et al., 2012). Patients receiving heparin within the last 90 days may experience rapid onset HIT within 24 h (Greinacher 2015). Patients receiving unfractionated heparin (UFH) are at higher risk of HIT compared to those receiving low molecular-weight heparin (LMWH) (Stein et al., 2009). One meta-analysis showed an absolute HIT risk of 0.2% with LMWH and 2.6% with UFH (Martel et al., 2005). Fondaparinux, a synthetic pentasaccharide fragment of heparin, shows almost no cross-reactivity with PF4/heparin antibodies and HIT is rare during fondaparinux treatment (Greinacher et al., 2017). Fondaparinux-associated HIT cases may be due to autoimmune HIT rather than fondaparinux. Autoimmune HIT occurs even in the absence of heparin but exhibits many clinical features of HIT (Greinacher et al., 2017). Proposed mechanisms of autoimmune HIT include endogenous polyanions, such as non-heparin glycosaminoglycans (GAGs), binding to PF4 complexes and exposing a neoepitope similar to heparin, which is subsequently recognized by IgG antibodies.
Confirmation of HIT requires both clinical and experimental confirmation. Clinically, a key indicator of HIT is an absolute drop in platelet count of 30–50% or a drop in platelet count of 40,000 to 80,000 per cubic mL (Greinacher 2015; Warkentin and Greinacher 2016). Platelet count along with other clinical indicators such as timing of onset of thrombocytopenia, presence of thrombosis or other sequelae, and alternative causes of thrombocytopenia collectively comprise the 4T scoring system (Warkentin and Greinacher 2016). Laboratory testing is also frequently used to confirm diagnosis of HIT. These laboratory tests include enzyme-linked immunosorbent assay (ELISA), which is used to test for PF4/heparin antibodies, and washed platelet activation assays such as the serotonin-release assay (SRA) and the heparin-induced platelet activation assay (HIPA) (Warkentin and Greinacher 2016), which quantify platelet activation in suspected patients’ serum. The SRA and HIPA assays are the “gold-standard” for detecting HIT but vary slightly in their assay endpoints. The SRA assay measures the release of radiolabel C14–serotonin from activated platelets while the HIPA test measures formation of platelet aggregation (Bakchoul et al., 2014). These functional assays are time-intensive and technically challenging, resulting in few laboratories having the regulatory and safety measures in place to perform these assays (Bakchoul et al., 2014). This limits their timeliness in clinical decision making and in confirming HIT cases.
HIT is initiated by ULCs cross-linking with the Fc domain of PF4/heparin antibodies via the low affinity IgG Fc region receptor II-a (FcγRIIa) on the surface of platelets. This initiates platelet activation and release of procoagulant microparticles (Warkentin et al., 1994), culminating in thrombocytopenia and/or thrombotic complications (Rollin et al., 2015). ULCs have been shown to interact with monocytes (Arepally and Mayer 2001; Pouplard 2001; Kasthuri et al., 2012; Tutwiler et al., 2016), endothelial cells (Arepally and Mayer 2001; Arepally 2002; Arepally 2017), neutrophils (Perdomo et al., 2019), and platelets (Figure 1).
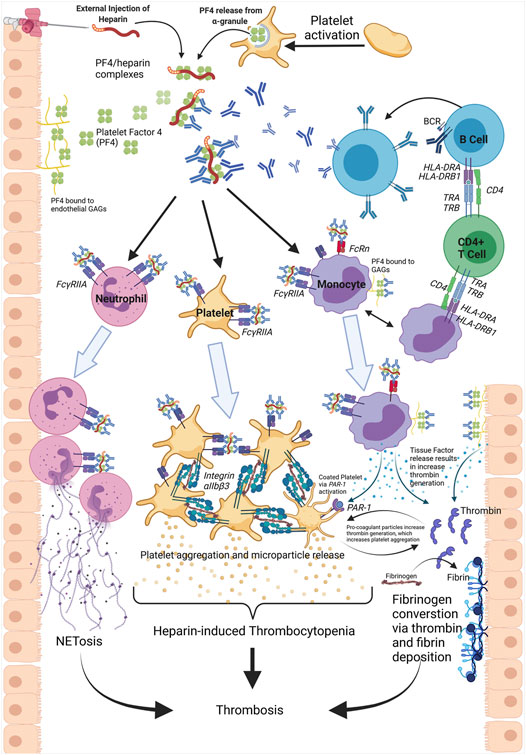
FIGURE 1. Heparin-induced thrombocytopenia (HIT) is initiated by the binding of heparin to platelet factor 4 (PF4), released from platelet α-granules. This binding results in a conformational change and exposure of a neo-epitope. PF4/heparin IgG antibodies generated from B cells bind to the neo-epitope, forming PF4/heparin/IgG ultra-large complexes (ULCs). The Fc region of the antibodies engage with FcγRIIa receptors on platelets, neutrophils, and monocytes. In platelets, this ULC binding results in intracellular activation, release of pro-coagulant microparticles, and subsequent platelet-platelet aggregation via Integrin αIIb/β3 engagement. The consumption of platelets into thrombi and platelet disintegration via microvesiculation causes thrombocytopenia. Neutrophil activation via ULC binding results in neutrophil recruitment to the endothelium and release of Neutrophil extracellular traps (NETs). The process of NETosis is a driver of thrombus formation and thrombosis. Monocyte activation leads to tissue factor (TF) expression and an increase in thrombin generation. Conversion of fibrinogen to fibrin via thrombin also contributes to an increased risk of thrombosis. TF released from monocytes additionally transactivates platelets via PAR-1 receptors, leaded to highly thrombotic, coated platelets. Furthermore, GAGs expressed on the endothelium act as binding partners for PF4 and subsequent antibody recognition. This antibody deposition results in increased TF release, thrombosis risk and serves as a site for activation of cells containing FcγRIIa receptors.
The immunopathogenesis of HIT is atypical and has characteristics of both innate and adaptive immunity (Greinacher 2015; Arepally 2017). Rapid production of PF4/heparin IgG antibodies, typical of a secondary adaptive immune or anamnestic response, is seen as early as 5 days after an initial heparin exposure. This response may be due to prior expose of PF4 bound to heparin-like GAGs or polyanions (Krauel et al., 2011; Staibano et al., 2017). However, PF4/heparin antibodies are transient, disappearing after approximately 90 days, characteristic of a non-anamnestic response (Warkentin and Kelton 2001). Heparin re-exposure after this 90 day period also does not reliably induce HIT, and patients with a previous HIT episode may be rechallenged with heparin (Warkentin and Sheppard 2014). PF4/heparin complexes activate complement, characteristic of an innate immune response. Binding of ULCs to B cells is mediated through the interaction between C3/C4 complement and complement receptor 2 (CR2 [CD21]). (Khandelwal et al., 2016). Polyreactive immunoglobulin M (IgM) antibodies initiate complement activation by binding to PF4/heparin complexes. IgM binding generates ULCs, facilitates the deposition of complement components, and promotes ULC binding to B cells (Khandelwal et al., 2018).
Heparin is a naturally occurring, endogenous GAG, and it has been extensively studied in both the context of HIT and in its pharmacologic action. In HIT, heparin molecules bind to complexes of circulating PF4, a chemokine (chemokine C-X-C motif 4 [CXCL4]) that is stored in α-granules of platelets (Delcea and Greinacher 2016). Polyanionic heparin binds to positively charged PF4, but this must occur in specific molar ratios or charge imbalances and complex instability will prevent ULC formation (Suvarna et al., 2007). Studies have identified structural (Cai et al., 2016) and thermodynamic (Brandt et al., 2014; Kreimann et al., 2014) features necessary for formation of ULCs. While PF4 exists in monomer, dimer, and tetramer states, PF4 must exist in a tetrameric configuration for ULCs to form and HIT to occur (Mayo and Chen 1989; Cai et al., 2015). The tetrameric structure of PF4 displays a pseudosymmetry exhibiting an “open” and “closed” end characterized by distances between two salt bridge forming amino acids, glutamic acid 28 and lysine 50. In PF4 monomers A and C, amino acids E28 and K50 are ∼3 angstroms (Å) apart and form stable salt bridges. The same amino acids in monomers B and D are too far apart to form a salt bridge (∼8 Å) without a bond mediator (Cai et al., 2015). Heparin binds in the “closed” end of the tetramer and stabilizes the self-association of the PF4 tetramer (Cai et al., 2016). Binding of heparin results in a conformational change in the PF4 tetramer complex and stabilizes the “open” end of the tetramer, exposing the epitope recognized by PF4/heparin IgG antibodies (Cai et al., 2016).
Circulating PF4 interacts with other polyanions, including nucleic acids, liposaccharides on bacteria (Greinacher 2015), and cellular GAGs, but PF4 has a greater affinity for heparin than for other GAGs (Arepally 2017). The atomic weight and structure of GAGs dictates the binding strength to PF4. UFH is more likely to stabilize the intramolecular interactions within the PF4 tetramer compared to LMWHs (Cai et al., 2016). Fondaparinux, shows an even greater loss of stabilizing potential for the PF4 tetramer.
Platelets are a primary driver of HIT and platelet activation contributes to HIT’s thromboembolic consequences. While the role of platelets and megakaryocytes have been extensively studied, other cells play critical roles in HIT pathogenesis, including T-cells, monocytes, endothelial cells, and neutrophils (Table 1) (Arepally and Mayer 2001; Pouplard 2001; Xia and Kao 2002; Tutwiler et al., 2016) (Cines et al., 1987; Arepally 2002) (Zheng et al., 2015) (Perdomo et al., 2019).
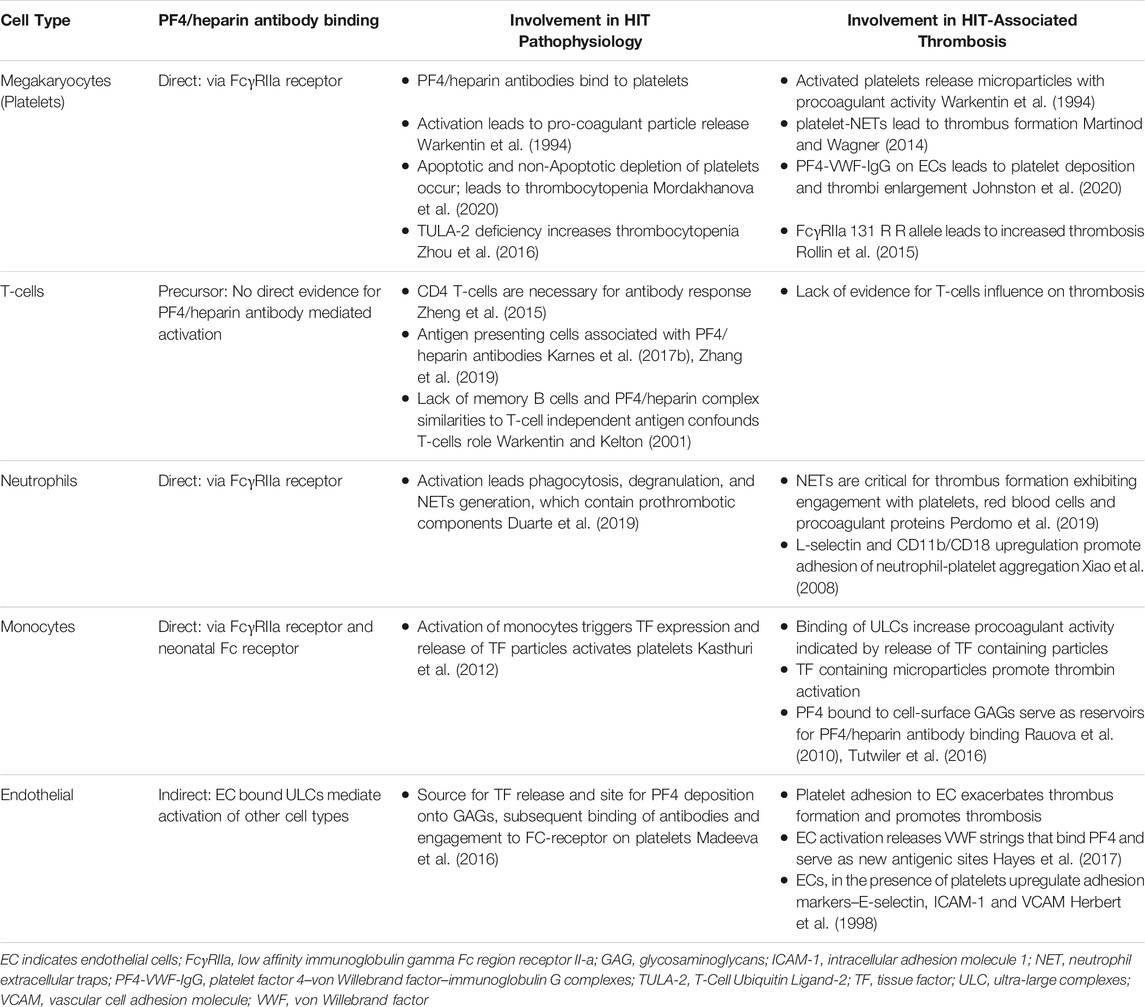
TABLE 1. Mechanisms of PF4/heparin antibody binding, involvement in pathogenesis of heparin-induced thrombocytopenia, and involvement in HIT-associated thrombosis of various cell types.
Platelets, the circulating anuclear fragments derived from megakaryocytes, express a single class of Fcγ receptors, FcγRIIa (Gratacap et al., 1998). Binding of ULCs to the FcγRIIa receptor triggers intracellular signaling involving the spleen tyrosine kinase 50 (SYK50) (Arepally 2017). SYK is phosphorylated when bound to FcγRIIa, activating SYK and triggering downstream signaling through calcium mobilization and PI3-kinase activation (Zhou et al., 2016). This leads to integrin αIIb/β3 activation and release of procoagulant microparticles from platelet granules. Two types of granules are released from activated platelets: dense granules, containing serotonin, calcium, adenosine triphosphate, and adenosine diphosphate and α-granules containing PF4, P-selectin, and fibrinogen (Fitch-Tewfik and Flaumenhaft 2013; Arepally and Padmanabhan 2020; Tardy et al., 2020). As shown in Figure 1, this signaling cascade leads to platelet activation and aggregation upon fibrinogen binding to the integrin receptor (Gratacap et al., 1998), resulting in a positive feedback loop facilitating a hypercoagulant state.
While the mechanisms of platelet activation via the FcγRIIa receptor are well understood, the mechanism of thrombocytopenia in HIT is not fully resolved. Clearance of antibody-coated platelets in the spleen (Prince and Wenham 2018), the consumption of platelets by thrombi, and platelet disintegration through platelet-derived microvesicles are proposed mechanisms for thrombocytopenia in HIT (Liu et al., 2013; Liu et al., 2016). A recent study showed that platelet activation was accompanied by cell death through complex apoptotic and non-apoptotic pathways, which may contribute to thrombocytopenia (Mordakhanova et al., 2020). Platelet activation and aggregation into thrombi reduce platelet count (Greinacher 2015). More recently, von Willebrand factor (VWF) and complexes of PF4-VWF-IgG antibodies were shown to bind extensively to platelets (Chen and Chung 2018) (Johnston et al., 2020).
Mutations in the FcγRIIa receptor have been shown to be associated with both HIT and HITT (Karnes 2018). The polymorphism H131R in the IgG binding region of FcγRIIa receptor has been associated with HIT in several populations, but a meta-analysis showed no difference in HIT between the wild-type and 131R variant (Trikalinos et al., 2001). However, individuals homozygous for the 131-RR genotype were at higher risk of HITT, likely due to the inability of endogenous IgG2 antibodies to bind to the RR genotype receptor. IgG2 antibodies compete with PF4/heparin antibodies (IgG1) for binding to FcγRIIa (Rollin et al., 2015). Decreased IgG2 affinity allows increased engagement of the IgG1 antibody, further stimulating the intracellular pathway involving FcγRIIa, SYK50 and platelet activation.
After maturation, selection, and transport out of the thymus, subsets of T-cells including regulatory T-cells (Treg), naïve T-cells, and memory T-cells are critically important for the maintenance of immune response and immunological memory. T-cells, particularly those subsets involved in antigen presentation, have been implicated in the immune response seen in HIT patients. HIT exhibits T-cell dependent characteristics (Xia and Kao 2002, Xia and Kao 2003; Chudasama et al., 2010; Joglekar et al., 2015), such as the requirement of CD4 and CD40 ligands on T-cells for PF4/heparin IgG production (Zheng et al., 2015). Observed associations between Human Leukocyte Antigen (HLA-DR) alleles and HIT suggest T-cell dependent mechanisms (Karnes et al., 2015; Karnes et al., 2017b; Zhang et al., 2019). However, HIT also presents T-cell independent characteristics. PF4/heparin complexes have similar characteristics to T-cell independent antigens, including similar molecular weight, repetitive epitopes, and spacing between elements (Vos et al., 2000; Staibano et al., 2017). The lack of memory B cells after heparin exposure (Selleng et al., 2010), and the role for marginal B cells in PF4/heparin IgG production in mouse models (Jouni et al., 2016) point to T-cell independent mechanisms.
Neutrophils are phagocytes and the most abundant type of white blood cell in the body (Van Rees et al., 2016). They migrate through blood vessels and perform a variety of function such as recruitment to sites of inflammation, phagocytosis of pathogens, degranulation, and generation of neutrophil extracellular traps (NETs). Activation of neutrophils via FcγRIIa receptor promotes phagocytosis, degranulation, and production of reactive oxygen species (ROS) (Gollomp et al., 2018). Neutrophils exposed to PF4 and PF4/heparin antibodies show enhanced adhesion to venous endothelium. In a microfluidics model, enhanced neutrophil involvement within venular thrombi was observed after induction of PF4 and PF4/heparin antibodies (Gollomp et al., 2018). Changes in absolute neutrophil counts have also been observed in HIT patients (Hui et al., 2019).
Neutrophils may play a role in HIT through generation of neutrophil extracellular traps (NETs). NETs are complexes of intracellular components including histones, myeloperoxidase, and elastase. NETs, when released from neutrophils, bind to pathogens and have anti-microbial activity (Van Rees et al., 2016). NETs have also been shown to contain prothrombotic components, such as tissue factor (TF), factor XII, VWF, and fibrinogen (Perdomo et al., 2019). Increased levels of cell-free DNA (cf-DNA), myeloperoxidase (MPO), elastase, VWF, and citrullinated histone H3 (CitH3), which are all markers of NETosis, have been reported in HIT patient plasma (Perdomo et al., 2019). In one study, whole blood from HIT patients included a second population of neutrophils that were not present in healthy controls, classified as activated neutrophils or low-density granulocytes (LDGs) (Perdomo et al., 2019). Using microfluidics models, complexes of NET and PF4 were shown to be recognized by KKO antibodies, which are synthetic antibodies that mimic PF4/heparin antibodies, and IgG from the plasma of HIT patients (Gollomp et al., 2018). Recently, murine HIT models (FcγRIIa+/hPF4+) recapitulated ex vivo results, in which NETosis was required for thrombus formation. Inhibition of NET formation by the NET inhibitor, GSK484, caused a marked reduction in thrombus deposition and neutralization of FcγRIIa completely abolished thrombi. However, blocking of platelet-neutrophil interactions via anti-CD62p did not inhibit thrombus formation (Perdomo et al., 2019).
More recent studies show neutrophils and the release of NETs do not initiate thrombosis in HIT mouse models, but play a role in thrombus growth and stabilization. Loss of peptidyl arginine deiminase type IV (PAD4) abolishes neutrophils’ ability to release NETs. Pad4 −/− HIT mice following KKO injection had thrombocytopenia comparable to Pad4 +/+ HIT mice. However, loss of PAD4 led to smaller venular thrombi following injury but did not abrogate thrombosis all together (Gollomp et al., 2018). Other studies have shown that heparin-induced NETs display two markedly different phenotypes. The first NETs (described above) are from neutrophils where cell nuclear membranes are disrupted, and the second subset are from neutrophils where small amounts of extracellular DNA were released but those neutrophils maintained their structural integrity (Lelliott et al., 2020). One study showed neutrophil activation induced by ULCs varied among individuals. In fact, an individual’s neutrophil response to ULCs remained fixed over a longitudinal 1-year period (Duarte et al., 2019), suggesting that susceptibility to neutrophil activation by ULCs is specific to the host and may be genetic in nature. These studies indicate that NETosis is a driver of thrombosis in HIT, but inter-individual variability in neutrophil count and heterogeneity, including polymorphism in cell surface receptors, are potential modifiers of HITT risk.
Monocytes, the immature precursor to macrophages and dendritic cells, serve as vehicles for antigen presentation, cytokine production, tissue remodeling, and phagocytosis (Guilliams et al., 2018). Monocytes express GAGs that react with PF4 to generate structural changes in PF4, which allows binding of PF4/heparin antibodies (Rauova et al., 2009). Monocytes primarily express two GAGs, heparin sulfate (HS) and dermatan sulfate (DS) (Madeeva et al., 2016). These GAGs may be the preferred target for PF4 binding and formation of ULCs, compared to platelets, as platelets express a low affinity GAG, chondroitin sulfate (Rauova et al., 2010). The binding of PF4/heparin antibodies to these PF4/GAG complexes on monocytes results in activation of Fc-receptors on monocytes.
Binding of PF4/heparin antibodies to FcγRIIa receptors trigger monocyte TF expression and release of TF particles (Kasthuri et al., 2012). TF binds to Factor VII (FVII)/FVIIa complexes and initiates coagulation by activating FX and FIX. The conversion of FX to FXa in complex with FVa activates prothrombin to thrombin (Mackman, 2004) (Tutwiler et al., 2016). The removal of monocytes from whole blood decreases platelet accretion and fibrin deposition. When levels of monocytes are brought back to normal physiological levels, the ability of KKO antibodies to stimulate platelet accretion and fibrin deposition is restored (Madeeva et al., 2016). Recent work has shown that in HIT patients, absolute monocyte levels decrease over a 7-days span post-HIT (Hui et al., 2019). However, overall counts of monocytes did not vary between patients with HIT and HITT (Hui et al., 2019).
The activation of monocytes and release of TF has recently been shown to involve the neonatal Fc receptor (FcRn) (Cines et al., 2020). Dual receptor engagement of ULCs (FcγRIIa and FcRn) on monocytes may explain why KKO antibodies have higher binding affinity to monocytes compared to platelets (Rauova et al., 2010). Thrombin generated by stimulated monocytes can trans-activate platelets via protease-activated receptor 1 (PAR-1), a subfamily of G protein-coupled receptors (Tutwiler et al., 2016). Coactivation of platelets via PAR and FcγRIIa leads to the formation of highly prothrombotic, coated platelets (Figure 1) (Tutwiler et al., 2016). Following whole blood exposure to KKO and PF4, a population of platelets exist with increase expression of P-selectin and other markers of coated platelets (Tutwiler et al., 2016). Expression of coated platelet markers was considerably reduced in the absence of monocytes in mouse platelet-rich plasma and in monocyte-depleted whole blood (Tutwiler et al., 2016). The amount of PF4 deposition onto monocytes is likely correlated with the extent of platelet transactivation (Madeeva et al., 2016). This amplification loop where activated platelets release PF4, this PF4 binds to monocytes, resulting in release of TF particles, which then further activates platelets and generates coated platelets, illustrates the complex interplay of cells in HIT.
Endothelial cells line blood vessels and play a critical role in regulating blood flow, vascular homeostasis, vascular tone, and platelet function (Jain et al., 2016; Madeeva et al., 2016; Sturtzel 2017). Signaling between vascular endothelial cells and platelets is vital for regulation of thrombosis (Jain et al., 2016). The basal state of endothelium is anticoagulant in nature, but at the onset of tissue trauma the endothelium facilitates coagulation (Sturtzel 2017). The endothelium expresses a mosaic sheath of glycoproteins, proteoglycans, and GAGs, known as the glycocalyx, under normal physiological conditions (Madeeva et al., 2016). Endothelial cells may bind PF4 with a greater affinity than platelets or monocytes given the predominant GAG on endothelial cells is heparin sulfate (Madeeva et al., 2016).
As shown in Figure 1, platelet activation at the site of injured endothelium releases PF4, which is deposited onto the endothelium due to a high affinity for GAGs. The PF4/GAG complex then becomes a target for PF4/heparin antibody binding. This binding contributes to increased endothelial activation and recruitment of platelets in a feed forward loop resulting in fibrin deposition and thrombosis (Madeeva et al., 2016). PF4 release was associated with binding of ULCs on thrombi following laser injury of endothelial cells (Hayes et al., 2017). Complexes of PF4 and VWF, released from endothelium following injury, may also be an antigenic site for PF4/heparin antibodies (Johnston et al., 2020). Microfluidics injury models also support that endothelial cells are the main initial harbor for PF4 released from activated platelets and a target for PF4/heparin antibodies (Hayes et al., 2017). The higher affinity of endothelial GAGs for PF4 may help to explain why antiplatelet therapy is not efficacious in HIT (Madeeva et al., 2016) and why thrombotic conditions may persist after heparin is no longer present. As approaches to date have yet to resolve these questions, applying multi-omics techniques to HIT has the potential to bring new insights and fundamentally improve our understanding.
Application and integration of omics disciplines, such as genomics, transcriptomics, metagenomics, proteomics, and metabolomics, has the potential to probe cellular roles discussed above and reveal previously unknown aspects of HIT biology. The complex, immune-mediated nature of HIT makes it well-suited for multi-omics approaches to solve questions surrounding the pathogenesis of HIT.
The majority of genetic studies related to HIT have been candidate gene studies. (Arepally et al., 1997; Pouplard et al., 2012; Rollin et al., 2012; Rollin et al., 2013; Rollin et al., 2015; Karnes et al., 2017b; Zhang et al., 2019). These studies focus on genes or single nucleotide polymorphisms (SNPs) with suspected biological relevance to the disease (Tabor et al., 2002). Genomic association studies for HIT and HITT are summarized in Table 2. Such studies have identified multiple associations with HIT and HITT (Brandt et al., 1995; Arepally et al., 1997; Rollin et al., 2015). Candidate gene/SNP studies can be cost effective, but these approaches have multiple limitations. They include the need for a priori information on gene function and a historical inability to replicate observed associations (Tabor et al., 2002; Patnala et al., 2013). Genome-wide association studies (GWAS) are an “agnostic” approach, in contrast to the hypothesis-driven candidate gene studies, and have become a powerful tool in discovering the genetic influence of complex disease. GWAS investigates the association between millions of genetic variants and a phenotype of interest. Despite clear successes in GWAS in identifying genetic polymorphisms associated with other phenotypes/diseases, very few GWAS studies have been performed for HIT (Karnes et al., 2015; Witten et al., 2018). One study identified a SNP in chromosome 5 in AC106799.2 as a risk allele for HIT (Witten et al., 2018). This GWAS only contained 96 suspected HIT cases and a replication cohort of 86 suspected HIT cases. Another GWAS observed a significant association with HIT near TDAG8 (or GPR65) (Karnes et al., 2015). Low sample sizes, particularly in HIT cases, were a limitation in both studies and reduce the impact of these findings. Furthermore, many of the HIT cases in both studies were determined through antibody testing and 4Ts scores and HIT was not confirmed with functional assays. Additionally, discovery cohorts in both studies did not include differentiation between antibody positive patients who develop HIT and antibody positive patients who did not develop HIT. This creates ambiguity in these results as the associations seen may be with PF4/heparin antibody levels and not HIT itself.
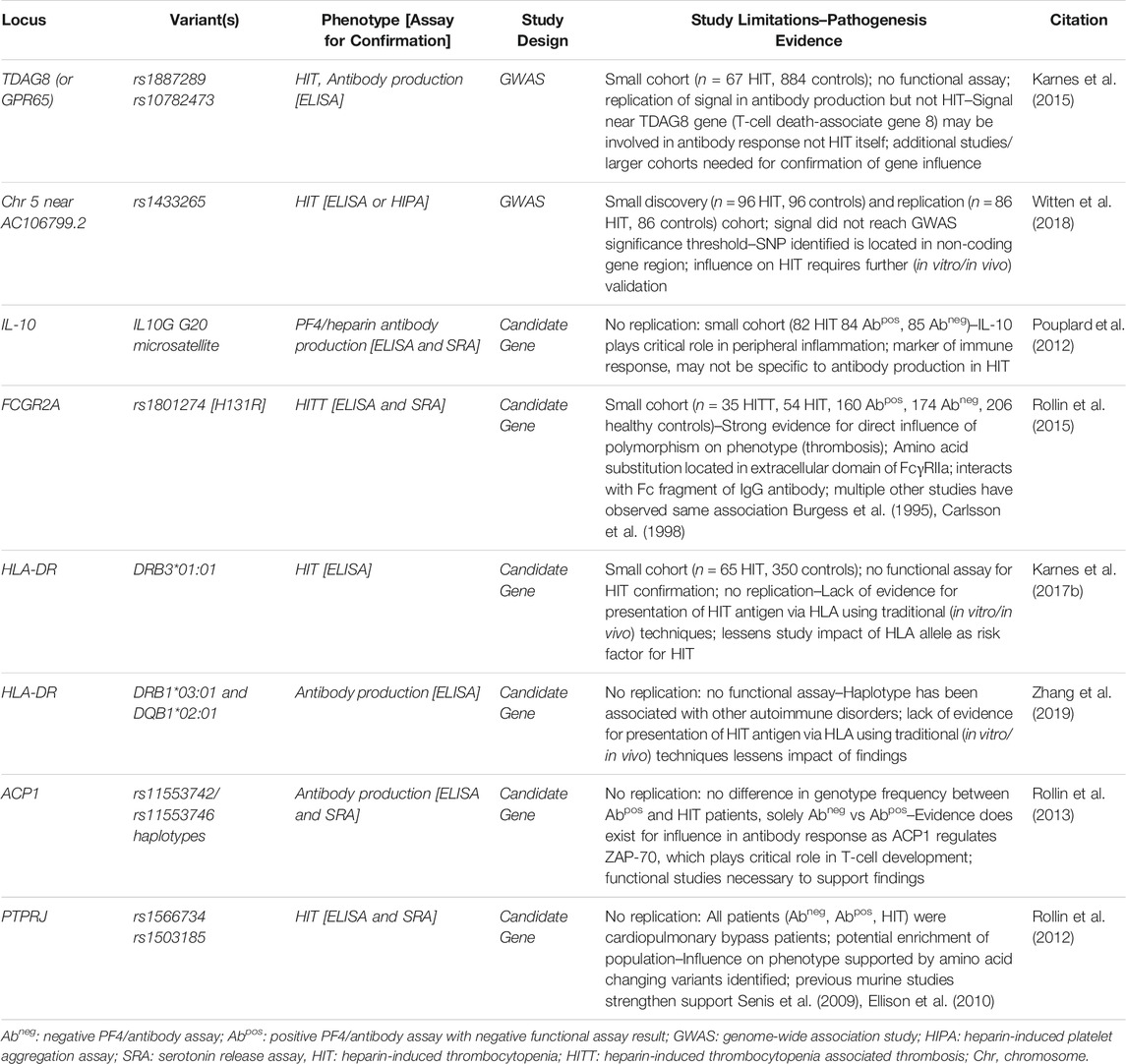
TABLE 2. Genomic studies identifying associations with Heparin-Induced Thrombocytopenia.
Within the HIT field, there is a need for a well-powered GWAS study which can overcome the limitations of the previous literature. Applying GWAS strategies to HIT research could have its largest impact in 1) identifying novel variants associated with HIT and 2) corroborating previous findings of variants which alter HIT risk. Large GWAS could provide valuable information on additional polymorphisms that alter thrombosis risk in HIT. GWAS could be used to identify genetic variants associated with antibody production independent of HIT and bring new insights into why only a subset of antibody positive patients develop HIT. However, the acquisition of enough HIT cases to create a sufficiently powered GWAS for HIT is a challenge. Whole-genome sequencing (WGS) might also be used to discover new polymorphisms with an influence on HIT. Declining sequencing costs will permit large scale interrogation of entire genomes, including rare variants, in the near future (Tam et al., 2019). However, WGS approaches will likely require even greater sample sizes for statistical power and additional resources for data storage, processing, and analysis.
Microorganisms, present throughout the human body, including bacteria, viruses, and fungi, collectively defined as the human microbiota, may have more biological influence that previously expected. Metagenomics, or the surveying of all (“Meta-”) microbial genomes (genomics), is typically performed via shotgun or 16s rRNA sequencing. Briefly, 16s rRNA sequencing is a cost-effective solution to surveying the communities of a bacterial microbiome via a single gene, the 16S ribosomal gene. Whereas shotgun sequencing surveys the entire genome of all organism present in a sample, including human, viral and fungal DNA (Ranjan et al., 2016). Recent evidence suggests that HIT is a misguided immune response, involving a prior bacterial exposure serving as a “priming” event. PF4/polyanion antibodies are produced and later recognize heparin as a “foreign” entity. PF4 has been shown to interact with both gram-positive and gram-negative bacteria and antibodies obtained from HIT patients recognize PF4 bound to bacteria (Krauel et al., 2011). Additional studies show PF4/heparin antibodies present in a cohort of subjects with periodontal disease (Greinacher et al., 2011) as well as inpatients with bacteremia. Patients with gram-negative bacteria showed higher levels of PF4/heparin antibodies relative to healthy controls (Pongas et al., 2013). Mice with polymicrobial sepsis produced PF4/heparin antibodies which followed the expected seroconversion from IgM to IgG (Jouni et al., 2016). The rapid antibody class switching observed in HIT, may in fact be due to a prior exposure of PF4 bound to polyanions expressed on bacteria or those with ongoing infections (Pongas et al., 2013). This evidence suggests the response against PF4/heparin complexes may be a misguided immune reaction, in that the epitope generated by PF4/heparin “mimics” the epitope of PF4 when bound to bacteria cell wall components. As this theory of a misguided immune response in HIT has yet to identify specific classes or even phyla of bacteria, sequencing the microbiome may provide powerful insights into HIT pathogenesis.
Sequencing of microbiomes from antibody positive patients compared with that of antibody negative controls could elucidate if the presence of particular microorganisms is associated with detectable PF4/heparin antibodies. Patients with specific bacterial exposure, identified through presence of bacteria or relevant antibodies, could alert clinicians to the increased risk of HIT prior to heparin exposure. Studies have already observed that gut microbiota alter the risk of cardiovascular disease (Witkowski et al., 2020; Jin et al., 2021). Gut microbiota-derived metabolites may increase the risk of venous thromboembolisms (Zhu et al., 2016; Hasan et al., 2020; Lichota et al., 2020). However, the influence of gut microbiota-derived metabolites has not been evaluated in the context of HIT or HITT. Given the number of patients prescribe heparin relative to the few who develop HIT, there are methodological difficulties in the assessment of all heparin-exposed patients prior heparin administration.
Transcriptomics, the comprehensive study of all RNA transcripts within an organism, is a powerful approach to explore cellular functions. The dominant techniques employed today are microarrays and RNA-sequencing (RNA-seq). Microarrays measure the abundance of a predefined set of transcripts and can allow the assay of thousands of transcripts simultaneously. Conversely, RNA-seq quantifies the entire transcriptome of cells via the sequencing of cDNA transcripts. Numerous HIT studies have looked at targeted mRNA levels using quantitative real-time PCR. Often these studies focus on a specific gene of interest (Lhermusier et al., 2011; Kasthuri et al., 2012; Rollin et al., 2015) as opposed to the broader scope that microarrays provide. Microarray studies could identify new roles of mRNA transcripts and their genes involved in HIT. This information could be used to delineate individuals who may produce higher antibody quantities and increased monitoring of those patients could be implemented to help minimize the progression to thromboembolic complications of HIT. Microarrays require a priori information on specific transcripts, but RNA-Seq provides a more agnostic approach for surveying the transcriptome. RNA-seq, most often utilized for differential gene expression (DGE), allows users to determine quantitative changes in expression levels between experiments, cases/controls studies, different disease states, etc.
Transcriptomics work could help identify specific transcriptional activity present in HIT cases compared to non-HIT controls in cross sectional studies. Also informative may be longitudinal studies on patients during HIT and post-HIT after antibodies have waned to interrogate the transcriptional differences where patients can serve as their own controls. Despite the clear applicability of RNA-seq in investigating HIT cases/controls, or even antibody cases/controls, RNA-seq has not yet been applied to HIT research. The most common RNA-sequencing technology, short read cDNA sequencing for DGE, is a robust and highly reproducible across and between platforms (Stark et al., 2019). Applying RNA-seq to HIT research might have a large impact in determining novel biological pathways involved in HIT pathogenesis. This application might also identify differentially expressed genes responsible for the subset of PF4/heparin antibody positive patients who go on to develop full-blown HIT. RNA-seq has the potential to discovery if difference in transcript levels amplify, or suppress, the antibody signally cascade initiated by IgG-platelet binding.
RNA-seq from bulk heterogeneous cells, as described in the previous paragraph, fails to resolve the role of specific cell types in the biological system being studied. As HIT pathogenesis is complex and involves multiple cell types, single-cell RNA sequencing (scRNA-seq) may reveal specific roles individual cells play in HIT, and potentially identify cell types that were previously not known to be involved in HIT. ScRNA-seq has been successful in discovering previously unknown cells types and mechanisms involved in phenotypes such as cystic fibrosis and myocardial infarction (Montoro et al., 2018) (Li et al., 2019) (Paik et al., 2020). ScRNA-seq could help answer questions surrounding the individual pathogenic roles of distinct cell types, in the case of monocytes and neutrophils, and the role of cell subtypes, in the case of T-cells and B-cells.
Proteomic analysis characterizes the proteome, including expression, structure, function, interaction, and modification of proteins (Aslam et al., 2017). While proteomic analysis has brought new insights into HIT, these studies have been limited in scope thus far (Khandelwal et al., 2018). Probing the proteome has the potential to identify a broader range of proteins and post-translational modifications of proteins involved in HIT. Proteomic approaches might be used to determine how glycosylation or post-translational modifications of proteins alters binding affinities and results in differential antibody response. A recent GWAS identified five novel loci associated with IgG antibody glycosylation (Shen et al., 2017).
Although not specific to HIT, proteomic approaches have been used successfully in cohorts of patients treated with heparin and other anticoagulants. One study identified 25 proteins displaying changes in concentration following heparin administration, with 14 proteins replicating in a validation cohort (Beck et al., 2018). In another study of heparin-treated pregnant women, multiplex protein screening identified increased levels of chemokines CXCL10, CLCL11 and CCL20 when compared to untreated pregnant controls (Rasmark Roepke et al., 2019). Another recent study showed substantive changes to expression of focal adhesion and cytoskeletal proteins in podocytes following chronic heparin exposure (Delézay et al., 2021). In a cohort of 4,200 oral anticoagulant patients with atrial fibrillation, one recent study identified seven novel proteins associated with increased risk of bleeding (Siegbahn et al., 2021). A number of other targeted proteomic studies have reported additional biomarkers associated with risk of bleeding in patients with acute coronary syndromes (Hagström et al., 2016; Hijazi et al., 2016). In a study comparing treatment with warfarin and rivaroxaban, nine metaproteins were shown to be differentially expressed (Mueck et al., 2014; Harter et al., 2015; Kaye et al., 2017; Reçber et al., 2020).
Proteomic profiling still suffers from shortcomings, such as the large samples required to achieve an accurate measurement and difficulty accounting for heterogeneity within a sample. Single-cell proteomics is an emerging technique that is applicable to HIT research. Still in its infancy, initial reports of profiling hundreds of proteins from a single, or small number of mammalian cells were first published in 2018 (Budnik et al., 2018; Zhu et al., 2018). As the transcriptome is not a direct reflection of the proteome, and that post-translational modifications of proteins are unattainable from RNA transcripts, the use of proteomics should be strongly considered to probe unanswered questions within the field. Furthermore, proteomics can be a powerful complement to genomic and transcriptomic studies, by offering systems-level insights into HIT pathogenesis.
The comprehensive set of small molecules within the body, the metabolome, is another avenue of research for further understanding of HIT pathogenesis. The metabolome can affect biological pathways through the modulation of the genome, transcriptome, and proteome (Rinschen et al., 2019). Metabolites serve as enzyme cofactors and substrates in biochemical processes. Activity of transmembrane receptors and transcription factors can be modulated by metabolites via allosteric regulation and metabolites can influence RNA metabolism by acting on riboswitches (Rinschen et al., 2019).
Metabolites such as physiologically relevant metal cations induce conformational changes in heparin (Seo et al., 2011; Zhang 2014). Neutralization of heparin via metal ion binding could influence the binding of PF4 to heparin since the electrostatic interaction between heparin and PF4 is critical for complex formation. Calcium (Ca2+) also induces substantive conformational changes in heparin (Seo et al., 2011) and is a critical cofactor in the binding of heparin to particular proteins such as Annexin A2 (Shao et al., 2006). Changes in concentrations of Ca2+ and Zinc (Zn2+), alters the binding affinity of heparin to other proteins including fibroblast growth factor-1 and interleukin 7 (Zhang 2014). Zinc (Zn2+) is present in high concentrations in α-granules, is a critical cofactor in non-HIT thrombosis (Vu et al., 2013), and is known to mediate binding of heparin to proteins including fibrinogen, high molecular weight kininogen, and histidine-rich glycoprotein (Fredenburgh et al., 2013; Sobczak et al., 2018). Substantive changes in the concentrations of these physiologically relevant metal cations could be a risk factor for HITT. Profiling of metal cation concentrations in the serum of HIT cases and heparin-treated controls could identify novel biomarkers in HITT. Metabolites, including acetate, citric acid, 3-hydroxybutarate, glucose, and some mono- and polyunsaturated fatty acids have been shown to be altered in arterial and deep venous thrombosis (Quintero et al., 2020). Metabolomics work could be applied to determine differences in metabolite levels affecting differential antibody responses and differences in HIT risk. The identification of metabolites that are risk factors for HIT could be invaluable within the clinic. Patients with metabolic alterations could alert clinicians to prescribe alternative therapies or increase monitoring of these at-risk patients.
Heparin-induced thrombocytopenia is a complex, unpredictable, immune-mediated adverse drug reaction involving multiple cell types. While platelets appear to be primarily involved in HIT, strong evidence exists for a critical role of several cell types in HIT pathogenesis. Neutrophils and monocytes have strong evidence for their role in HIT, particularly in HITT. HIT exhibits both T-cell dependent and independent features and genomic studies have observed associations between variation in antigen presentation pathways and HIT. Endothelial cells serve as a deposition site for PF4, likely playing a role in PF4/heparin antibody binding and signal transduction. Despite our understanding of these cell types and their roles in HIT, multiple gaps in our knowledge of HIT pathogenesis remain. Applying multi-omics techniques to HIT has the potential to bring new insights. Larger and functional assay-confirmed HIT cohorts are necessary to overcome the limitations of published HIT genomic studies. Other omics techniques, such as transcriptomics and proteomics, have been underutilized in HIT research. As technologies become more established and less cost prohibitive, single cell transcriptomics and proteomics are particularly well-suited to address for the gaps in our knowledge of HIT pathogenesis. Such omics approaches have great promise to elucidate biological pathways, profile patient samples and discover valuable clinical biomarkers, which could reduce the risk of HIT and improve patient outcomes in the clinic.
JG and JK conceived of project; JG and JK drafted the manuscript; JG, EM, HS, and JK performed literature review and critically revised manuscript. All authors reviewed and approved the final version of the manuscript.
JG is funded by the National Institutes of Health’s Environmental Health Sciences (NIEHS) T32 Training Grant-T32 ES007091. JK is funded by the National Institutes of Health’s (NIH) National Heart, Lung, and Blood Institute (NHLBI) under award K01HL143137 and R01HL158686.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Arepally, G., and Cines, D. B. (2002). Pathogenesis of Heparin-Induced Thrombocytopenia and Thrombosis. Autoimmun. Rev. 1, 125–132. doi:10.1016/s1568-9972(02)00031-9
Arepally, G., Mckenzie, S. E., Jiang, X. M., Poncz, M., and Cines, D. B. (1997). Fc Gamma RIIA H/R 131 Polymorphism, Subclass-specific IgG Anti-heparin/platelet Factor 4 Antibodies and Clinical Course in Patients with Heparin-Induced Thrombocytopenia and Thrombosis. Blood 89, 370–375. doi:10.1182/blood.v89.2.370
Arepally, G. M. (2017). Heparin-induced Thrombocytopenia. Blood 129, 2864–2872. doi:10.1182/blood-2016-11-709873
Arepally, G. M., and Mayer, I. M. (2001). Antibodies from Patients with Heparin-Induced Thrombocytopenia Stimulate Monocytic Cells to Express Tissue Factor and Secrete Interleukin-8. Blood 98, 1252–1254. doi:10.1182/blood.v98.4.1252
Arepally, G. M., and Ortel, T. L. (2010). Heparin-induced Thrombocytopenia. Annu. Rev. Med. 61, 77–90. doi:10.1146/annurev.med.042808.171814
Arepally, G. M., and Padmanabhan, A. (2020). Heparin-Induced Thrombocytopenia: A Focus on Thrombosis. Arteriosclerosis, Thromb. Vasc. Biol. 41, 141–152. doi:10.1161/atvbaha.120.315445
Aslam, B., Basit, M., Nisar, M. A., Khurshid, M., and Rasool, M. H. (2017). Proteomics: Technologies and Their Applications. J. Chromatogr. Sci. 55, 182–196. doi:10.1093/chromsci/bmw167
Bakchoul, T., Zöllner, H., and Greinacher, A. (2014). Current Insights into the Laboratory Diagnosis of HIT. Int. J. Lab. Hematol. 36, 296–305. doi:10.1111/ijlh.12236
Bauer, T. L., Arepally, G., Konkle, B. A., Mestichelli, B., Shapiro, S. S., Cines, D. B., et al. (1997). Prevalence of Heparin-Associated Antibodies without Thrombosis in Patients Undergoing Cardiopulmonary Bypass Surgery. Circulation 95, 1242–1246. doi:10.1161/01.cir.95.5.1242
Beck, H. C., Jensen, L. O., Gils, C., Ilondo, A. M. M., Frydland, M., Hassager, C., et al. (2018). Proteomic Discovery and Validation of the Confounding Effect of Heparin Administration on the Analysis of Candidate Cardiovascular Biomarkers. Clin. Chem. 64, 1474–1484. doi:10.1373/clinchem.2017.282665
Brandt, J. T., Isenhart, C. E., Osborne, J. M., Ahmed, A., and Anderson, C. L. (1995). On the Role of Platelet Fc Gamma RIIa Phenotype in Heparin-Induced Thrombocytopenia. Thromb. Haemost. 74, 1564–1572. doi:10.1055/s-0038-1649983
Brandt, S., Krauel, K., Gottschalk, K. E., Renné, T., Helm, C. A., Greinacher, A., et al. (2014). Characterisation of the Conformational Changes in Platelet Factor 4 Induced by Polyanions: towards in vitro Prediction of Antigenicity. Thromb. Haemost. 112, 53–64. doi:10.1160/TH13-08-0634
Budnik, B., Levy, E., Harmange, G., and Slavov, N. (2018). SCoPE-MS: Mass Spectrometry of Single Mammalian Cells Quantifies Proteome Heterogeneity during Cell Differentiation. Genome Biol. 19, 161. doi:10.1186/s13059-018-1547-5
Burgess, J. K., Lindeman, R., Chesterman, C. N., and Chong, B. H. (1995). Single Amino Acid Mutation of Fc Gamma Receptor Is Associated with the Development of Heparin-Induced Thrombocytopenia. Br. J. Haematol. 91, 761–766. doi:10.1111/j.1365-2141.1995.tb05383.x
Cai, Z., Yarovoi, S. V., Zhu, Z., Rauova, L., Hayes, V., Lebedeva, T., et al. (2015). Atomic Description of the Immune Complex Involved in Heparin-Induced Thrombocytopenia. Nat. Commun. 6, 8277. doi:10.1038/ncomms9277
Cai, Z., Zhu, Z., Greene, M. I., and Cines, D. B. (2016). Atomic Features of an Autoantigen in Heparin-Induced Thrombocytopenia (HIT). Autoimmun. Rev. 15, 752–755. doi:10.1016/j.autrev.2016.03.011
Campbell, K. R., Mahaffey, K. W., Lewis, B. E., Weitz, J. I., Berkowitz, S. D., Ohman, E. M., et al. (2000). Bivalirudin in Patients with Heparin-Induced Thrombocytopenia Undergoing Percutaneous Coronary Intervention. J. Invasive Cardiol. 12, 14f–9.
Carlsson, L. E., Santoso, S., Baurichter, G., Kroll, H., Papenberg, S., Eichler, P., et al. (1998). Heparin-induced Thrombocytopenia: New Insights into the Impact of the FcgammaRIIa-R-H131 Polymorphism. Blood 92, 1526–1531. doi:10.1182/blood.v92.5.1526
Chen, J., and Chung, D. W. (2018). Inflammation, von Willebrand factor, and ADAMTS13. Blood 132, 141–147. doi:10.1182/blood-2018-02-769000
Chudasama, S. L., Espinasse, B., Hwang, F., Qi, R., Joglekar, M., Afonina, G., et al. (2010). Heparin Modifies the Immunogenicity of Positively Charged Proteins. Blood 116, 6046–6053. doi:10.1182/blood-2010-06-292938
Cines, D. B., Tomaski, A., and Tannenbaum, S. (1987). Immune Endothelial-Cell Injury in Heparin-Associated Thrombocytopenia. N. Engl. J. Med. 316, 581–589. doi:10.1056/NEJM198703053161004
Cines, D. B., Zaitsev, S., Rauova, L., Rux, A. H., Stepanova, V., Krishnaswamy, S., et al. (2020). FcRn Augments Induction of Tissue Factor Activity by IgG-Containing Immune Complexes. Blood 135, 2085–2093. doi:10.1182/blood.2019001133
Cuker, A. (2011). Heparin-induced Thrombocytopenia: Present and Future. J. Thromb. Thrombolysis 31, 353–366. doi:10.1007/s11239-011-0569-6
Delcea, M., and Greinacher, A. (2016). Biophysical Tools to Assess the Interaction of PF4 with Polyanions. Thromb. Haemost. 116, 783–791. doi:10.1160/TH16-04-0258
Delézay, O., Hodin, S., Hé, Z., Ollier, E., and Delavenne, X. (2021). Functional, Proteomic and Phenotypic in vitro Studies Evidence Podocyte Injury after Chronic Exposure to Heparin. Toxicol. Appl. Pharmacol. 429, 115683. doi:10.1016/j.taap.2021.115683
Duarte, M., Kuchibhatla, M., Khandelwal, S., Arepally, G. M., and Lee, G. M. (2019). Heterogeneity in Neutrophil Responses to Immune Complexes. Blood Adv. 3, 2778–2789. doi:10.1182/bloodadvances.2019000235
Ellison, S., Mori, J., Barr, A. J., and Senis, Y. A. (2010). CD148 Enhances Platelet Responsiveness to Collagen by Maintaining a Pool of Active Src Family Kinases. J. Thromb. Haemost. 8, 1575–1583. doi:10.1111/j.1538-7836.2010.03865.x
Fitch-Tewfik, J. L., and Flaumenhaft, R. (2013). Platelet Granule Exocytosis: A Comparison with Chromaffin Cells. Front. Endocrinol. (Lausanne) 4, 77. doi:10.3389/fendo.2013.00077
Franchini, M., and Veneri, D. (2005). Heparin-induced Thrombocytopenia. Recenti Prog. Med. 96, 433–435. doi:10.1186/1477-9560-3-14
Fredenburgh, J. C., Leslie, B. A., Stafford, A. R., Lim, T., Chan, H. H., and Weitz, J. I. (2013). Zn2+ Mediates High Affinity Binding of Heparin to the αC Domain of Fibrinogen. J. Biol. Chem. 288, 29394–29402. doi:10.1074/jbc.M113.469916
Girolami, B., Prandoni, P., Stefani, P. M., Tanduo, C., Sabbion, P., Eichler, P., et al. (2003). The Incidence of Heparin-Induced Thrombocytopenia in Hospitalized Medical Patients Treated with Subcutaneous Unfractionated Heparin: a Prospective Cohort Study. Blood 101, 2955–2959. doi:10.1182/blood-2002-07-2201
Gollomp, K., Kim, M., Johnston, I., Hayes, V., Welsh, J., Arepally, G. M., et al. (2018). Neutrophil Accumulation and NET Release Contribute to Thrombosis in HIT. JCI Insight 3. doi:10.1172/jci.insight.99445
Gratacap, M. P., Payrastre, B., Viala, C., Mauco, G., Plantavid, M., and Chap, H. (1998). Phosphatidylinositol 3,4,5-trisphosphate-dependent Stimulation of Phospholipase C-Gamma2 Is an Early Key Event in FcgammaRIIA-Mediated Activation of Human Platelets. J. Biol. Chem. 273, 24314–24321. doi:10.1074/jbc.273.38.24314
Greinacher, A. (2015). CLINICAL PRACTICE. Heparin-Induced Thrombocytopenia. N. Engl. J. Med. 373, 252–261. doi:10.1056/NEJMcp1411910
Greinacher, A., Holtfreter, B., Krauel, K., Gätke, D., Weber, C., Ittermann, T., et al. (2011). Association of Natural Anti-platelet Factor 4/heparin Antibodies with Periodontal Disease. Blood 118, 1395–1401. doi:10.1182/blood-2011-03-342857
Greinacher, A., Selleng, K., and Warkentin, T. E. (2017). Autoimmune Heparin-Induced Thrombocytopenia. J. Thromb. Haemost. 15, 2099–2114. doi:10.1111/jth.13813
Guilliams, M., Mildner, A., and Yona, S. (2018). Developmental and Functional Heterogeneity of Monocytes. Immunity 49, 595–613. doi:10.1016/j.immuni.2018.10.005
Hagström, E., James, S. K., Bertilsson, M., Becker, R. C., Himmelmann, A., Husted, S., et al. (2016). Growth Differentiation Factor-15 Level Predicts Major Bleeding and Cardiovascular Events in Patients with Acute Coronary Syndromes: Results from the PLATO Study. Eur. Heart J. 37, 1325–1333. doi:10.1093/eurheartj/ehv491
Haile, L. A., Rao, R., Polumuri, S. K., Arepally, G. M., Keire, D. A., Verthelyi, D., et al. (2017). PF4-HIT Antibody (KKO) Complexes Activate Broad Innate Immune and Inflammatory Responses. Thromb. Res. 159, 39–47. doi:10.1016/j.thromres.2017.09.018
Harter, K., Levine, M., and Henderson, S. O. (2015). Anticoagulation Drug Therapy: A Review. West. J. Emerg. Med. 16, 11–17. doi:10.5811/westjem.2014.12.22933
Hasan, R. A., Koh, A. Y., and Zia, A. (2020). The Gut Microbiome and Thromboembolism. Thromb. Res. 189, 77–87. doi:10.1016/j.thromres.2020.03.003
Hayes, V., Johnston, I., Arepally, G. M., Mckenzie, S. E., Cines, D. B., Rauova, L., et al. (2017). Endothelial Antigen Assembly Leads to Thrombotic Complications in Heparin-Induced Thrombocytopenia. J. Clin. Invest. 127, 1090–1098. doi:10.1172/JCI90958
Herbert, J. M., Savi, P., Jeske, W. P., and Walenga, J. M. (1998). Effect of SR121566A, a Potent GP IIb-IIIa Antagonist, on the HIT Serum/heparin-Induced Platelet Mediated Activation of Human Endothelial Cells. Thromb. Haemost. 80, 326–331.
Hijazi, Z., Oldgren, J., Lindbäck, J., Alexander, J. H., Connolly, S. J., Eikelboom, J. W., et al. (2016). The Novel Biomarker-Based ABC (Age, Biomarkers, Clinical History)-Bleeding Risk Score for Patients with Atrial Fibrillation: a Derivation and Validation Study. Lancet 387, 2302–2311. doi:10.1016/S0140-6736(16)00741-8
Hui, M., Sheppard, J. I., Li, N., and Warkentin, T. E. (2019). Neutrophil and Monocyte Counts in Heparin-Induced Thrombocytopenia. Thromb. Haemost. 119, 941–951. doi:10.1055/s-0039-1683913
Jain, A., Van Der Meer, A. D., Papa, A. L., Barrile, R., Lai, A., Schlechter, B. L., et al. (2016). Assessment of Whole Blood Thrombosis in a Microfluidic Device Lined by Fixed Human Endothelium. Biomed. Microdevices 18, 73. doi:10.1007/s10544-016-0095-6
Jin, L., Shi, X., Yang, J., Zhao, Y., Xue, L., Xu, L., et al. (2021). Gut Microbes in Cardiovascular Diseases and Their Potential Therapeutic Applications. Protein Cell 12, 346–359. doi:10.1007/s13238-020-00785-9
Joglekar, M., Khandelwal, S., Cines, D. B., Poncz, M., Rauova, L., and Arepally, G. M. (2015). Heparin Enhances Uptake of Platelet Factor 4/heparin Complexes by Monocytes and Macrophages. J. Thromb. Haemost. 13, 1416–1427. doi:10.1111/jth.13003
Johnston, I., Sarkar, A., Hayes, V., Koma, G. T., Arepally, G. M., Chen, J., et al. (2020). Recognition of PF4-VWF Complexes by Heparin-Induced Thrombocytopenia Antibodies Contributes to Thrombus Propagation. Blood 135, 1270–1280. doi:10.1182/blood.2018881607
Karnes, J. H., Bastarache, L., Shaffer, C. M., Gaudieri, S., Xu, Y., Glazer, A. M., et al. (2017a). Phenome-wide Scanning Identifies Multiple Diseases and Disease Severity Phenotypes Associated with HLA Variants. Sci. Transl Med. 9, eaai8708. doi:10.1126/scitranslmed.aai8708
Karnes, J. H., Cronin, R. M., Rollin, J., Teumer, A., Pouplard, C., Shaffer, C. M., et al. (2015). A Genome-wide Association Study of Heparin-Induced Thrombocytopenia Using an Electronic Medical Record. Thromb. Haemost. 113, 772–781. doi:10.1160/TH14-08-0670
Karnes, J. H., Miller, M. A., White, K. D., Konvinse, K. C., Pavlos, R. K., Redwood, A. J., et al. (2019). Applications of Immunopharmacogenomics: Predicting, Preventing, and Understanding Immune-Mediated Adverse Drug Reactions. Annu. Rev. Pharmacol. Toxicol. 59, 463–486. doi:10.1146/annurev-pharmtox-010818-021818
Karnes, J. H. (2018). Pharmacogenetics to Prevent Heparin-Induced Thrombocytopenia: what Do We Know? Pharmacogenomics 19, 1413–1422. doi:10.2217/pgs-2018-0147
Karnes, J. H., Shaffer, C. M., Cronin, R., Bastarache, L., Gaudieri, S., James, I., et al. (2017b). Influence of Human Leukocyte Antigen (HLA) Alleles and Killer Cell Immunoglobulin-like Receptors (KIR) Types on Heparin-Induced Thrombocytopenia (HIT). Pharmacotherapy 37, 1164–1171. doi:10.1002/phar.1983
Kasthuri, R. S., Glover, S. L., Jonas, W., Mceachron, T., Pawlinski, R., Arepally, G. M., et al. (2012). PF4/heparin-antibody Complex Induces Monocyte Tissue Factor Expression and Release of Tissue Factor Positive Microparticles by Activation of FcγRI. Blood 119, 5285–5293. doi:10.1182/blood-2011-06-359430
Kaye, J. B., Schultz, L. E., Steiner, H. E., Kittles, R. A., Cavallari, L. H., and Karnes, J. H. (2017). Warfarin Pharmacogenomics in Diverse Populations. Pharmacotherapy 37, 1150–1163. doi:10.1002/phar.1982
Kelton, J. G., Smith, J. W., Warkentin, T. E., Hayward, C. P., Denomme, G. A., and Horsewood, P. (1994). Immunoglobulin G from Patients with Heparin-Induced Thrombocytopenia Binds to a Complex of Heparin and Platelet Factor 4. Blood 83, 3232–3239. doi:10.1182/blood.v83.11.3232.bloodjournal83113232
Khandelwal, S., and Arepally, G. M. (2016). Immune Pathogenesis of Heparin-Induced Thrombocytopenia. Thromb. Haemost. 116, 792–798. doi:10.1160/TH16-01-0074
Khandelwal, S., Lee, G. M., Hester, C. G., Poncz, M., Mckenzie, S. E., Sachais, B. S., et al. (2016). The Antigenic Complex in HIT Binds to B Cells via Complement and Complement Receptor 2 (CD21). Blood 128, 1789–1799. doi:10.1182/blood-2016-04-709634
Khandelwal, S., Ravi, J., Rauova, L., Johnson, A., Lee, G. M., Gilner, J. B., et al. (2018). Polyreactive IgM Initiates Complement Activation by PF4/heparin Complexes through the Classical Pathway. Blood 132, 2431–2440. doi:10.1182/blood-2018-03-834598
Krauel, K., Pötschke, C., Weber, C., Kessler, W., Fürll, B., Ittermann, T., et al. (2011). Platelet Factor 4 Binds to Bacteria, [corrected] Inducing Antibodies Cross-Reacting with the Major Antigen in Heparin-Induced Thrombocytopenia. Blood 117, 1370–1378. doi:10.1182/blood-2010-08-301424
Krauel, K., Schulze, A., Jouni, R., Hackbarth, C., Hietkamp, B., Selleng, S., et al. (2016). Further Insights into the Anti-PF4/heparin IgM Immune Response. Thromb. Haemost. 115, 752–761. doi:10.1160/TH15-08-0654
Kreimann, M., Brandt, S., Krauel, K., Block, S., Helm, C. A., Weitschies, W., et al. (2014). Binding of Anti-platelet Factor 4/heparin Antibodies Depends on the Thermodynamics of Conformational Changes in Platelet Factor 4. Blood 124, 2442–2449. doi:10.1182/blood-2014-03-559518
Lelliott, P. M., Momota, M., Shibahara, T., Lee, M. S. J., Smith, N. I., Ishii, K. J., et al. (2020). Heparin Induces Neutrophil Elastase-dependent Vital and Lytic NET Formation. Int. Immunol. 32, 359–368. doi:10.1093/intimm/dxz084
Lhermusier, T., Van Rottem, J., Garcia, C., Xuereb, J. M., Ragab, A., Martin, V., et al. (2011). The Syk-Kinase Inhibitor R406 Impairs Platelet Activation and Monocyte Tissue Factor Expression Triggered by Heparin-PF4 Complex Directed Antibodies. J. Thromb. Haemost. 9, 2067–2076. doi:10.1111/j.1538-7836.2011.04470.x
Li, Z., Solomonidis, E. G., Meloni, M., Taylor, R. S., Duffin, R., Dobie, R., et al. (2019). Single-cell Transcriptome Analyses Reveal Novel Targets Modulating Cardiac Neovascularization by Resident Endothelial Cells Following Myocardial Infarction. Eur. Heart J. 40, 2507–2520. doi:10.1093/eurheartj/ehz305
Lichota, A., Gwozdzinski, K., and Szewczyk, E. M. (2020). Microbial Modulation of Coagulation Disorders in Venous Thromboembolism. J. Inflamm. Res. 13, 387–400. doi:10.2147/JIR.S258839
Linkins, L.-A., Dans, A. L., Moores, L. K., Bona, R., Davidson, B. L., Schulman, S., et al. (2012). Treatment and Prevention of Heparin-Induced Thrombocytopenia, 9th Ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 141, e495S–e530S. doi:10.1378/chest.11-2303
Liu, M. L., Williams, K. J., and Werth, V. P. (2016). Microvesicles in Autoimmune Diseases. Adv. Clin. Chem. 77, 125–175. doi:10.1016/bs.acc.2016.06.005
Mackman, N. (2004). Role of Tissue Factor in Hemostasis, Thrombosis, and Vascular Development. Atvb 24, 1015–1022. doi:10.1161/01.atv.0000130465.23430.74
Madeeva, D., Cines, D. B., Poncz, M., and Rauova, L. (2016). Role of Monocytes and Endothelial Cells in Heparin-Induced Thrombocytopenia. Thromb. Haemost. 116, 806–812. doi:10.1160/TH16-02-0162
Martel, N., Lee, J., and Wells, P. S. (2005). Risk for Heparin-Induced Thrombocytopenia with Unfractionated and Low-Molecular-Weight Heparin Thromboprophylaxis: a Meta-Analysis. Blood 106, 2710–2715. doi:10.1182/blood-2005-04-1546
Martinod, K., and Wagner, D. D. (2014). Thrombosis: Tangled up in NETs. Blood 123, 2768–2776. doi:10.1182/blood-2013-10-463646
Mayo, K. H., and Chen, M. J. (1989). Human Platelet Factor 4 Monomer-Dimer-Tetramer Equilibria Investigated by 1H NMR Spectroscopy. Biochemistry 28, 9469–9478. doi:10.1021/bi00450a034
Montoro, D. T., Haber, A. L., Biton, M., Vinarsky, V., Lin, B., Birket, S. E., et al. (2018). A Revised Airway Epithelial Hierarchy Includes CFTR-Expressing Ionocytes. Nature 560, 319–324. doi:10.1038/s41586-018-0393-7
Mordakhanova, E. R., Nevzorova, T. A., Synbulatova, G. E., Rauova, L., Weisel, J. W., and Litvinov, R. I. (2020). Platelet Activation in Heparin-Induced Thrombocytopenia Is Followed by Platelet Death via Complex Apoptotic and Non-apoptotic Pathways. Int. J. Mol. Sci. 21, 2556. doi:10.3390/ijms21072556
Mueck, W., Stampfuss, J., Kubitza, D., and Becka, M. (2014). Clinical Pharmacokinetic and Pharmacodynamic Profile of Rivaroxaban. Clin. Pharmacokinet. 53, 1–16. doi:10.1007/s40262-013-0100-7
Paik, D. T., Cho, S., Tian, L., Chang, H. Y., and Wu, J. C. (2020). Single-cell RNA Sequencing in Cardiovascular Development, Disease and Medicine. Nat. Rev. Cardiol. 17, 457–473. doi:10.1038/s41569-020-0359-y
Patnala, R., Clements, J., and Batra, J. (2013). Candidate Gene Association Studies: a Comprehensive Guide to Useful In Silico Tools. BMC Genet. 14, 39. doi:10.1186/1471-2156-14-39
Perdomo, J., Leung, H. H. L., Ahmadi, Z., Yan, F., Chong, J. J. H., Passam, F. H., et al. (2019). Neutrophil Activation and NETosis Are the Major Drivers of Thrombosis in Heparin-Induced Thrombocytopenia. Nat. Commun. 10, 1322. doi:10.1038/s41467-019-09160-7
Pongas, G., Dasgupta, S. K., and Thiagarajan, P. (2013). Antiplatelet Factor 4/heparin Antibodies in Patients with Gram Negative Bacteremia. Thromb. Res. 132, 217–220. doi:10.1016/j.thromres.2013.06.013
Pouplard, C., Cornillet-Lefebvre, P., Attaoua, R., Leroux, D., Lecocq-Lafon, C., Rollin, J., et al. (2012). Interleukin-10 Promoter Microsatellite Polymorphisms Influence the Immune Response to Heparin and the Risk of Heparin-Induced Thrombocytopenia. Thromb. Res. 129, 465–469. doi:10.1016/j.thromres.2011.09.033
Pouplard, C., Iochmann, S., Renard, B., Herault, O., Colombat, P., Amiral, J., et al. (2001). Induction of Monocyte Tissue Factor Expression by Antibodies to Heparin-Platelet Factor 4 Complexes Developed in Heparin-Induced Thrombocytopenia. Blood 97, 3300–3302. doi:10.1182/blood.v97.10.3300
Prince, M., and Wenham, T. (2018). Heparin-induced Thrombocytopaenia. Postgrad. Med. J. 94, 453–457. doi:10.1136/postgradmedj-2018-135702
Quintero, M., Tasic, L., and Annichino-Bizzacchi, J. M. (2020). Thrombosis: Current Knowledge Based on Metabolomics by Nuclear Magnetic Resonance (NMR) Spectroscopy and Mass Spectrometry (MS). Thromb. Update 1, 100011. doi:10.1016/j.tru.2020.100011
Ranjan, R., Rani, A., Metwally, A., Mcgee, H. S., and Perkins, D. L. (2016). Analysis of the Microbiome: Advantages of Whole Genome Shotgun versus 16S Amplicon Sequencing. Biochem. Biophys. Res. Commun. 469, 967–977. doi:10.1016/j.bbrc.2015.12.083
Rasmark Roepke, E., Bruno, V., Nedstrand, E., Boij, R., Strid, C. P., Piccione, E., et al. (2019). Low-molecular-weight-heparin Increases Th1- and Th17-Associated Chemokine Levels during Pregnancy in Women with Unexplained Recurrent Pregnancy Loss: a Randomised Controlled Trial. Sci. Rep. 9, 12314. doi:10.1038/s41598-019-48799-6
Rauova, L., Arepally, G., Mckenzie, S. E., Konkle, B. A., Cines, D. B., and Poncz, M. (2009). Platelet and Monocyte Antigenic Complexes in the Pathogenesis of Heparin-Induced Thrombocytopenia (HIT). J. Thromb. Haemost. 7, 249–252. doi:10.1111/j.1538-7836.2009.03373.x
Rauova, L., Hirsch, J. D., Greene, T. K., Zhai, L., Hayes, V. M., Kowalska, M. A., et al. (2010). Monocyte-bound PF4 in the Pathogenesis of Heparin-Induced Thrombocytopenia. Blood 116, 5021–5031. doi:10.1182/blood-2010-03-276964
Reilly, M. P., Taylor, S. M., Hartman, N. K., Arepally, G. M., Sachais, B. S., Cines, D. B., et al. (2001). Heparin-induced Thrombocytopenia/thrombosis in a Transgenic Mouse Model Requires Human Platelet Factor 4 and Platelet Activation through FcgammaRIIA. Blood 98, 2442–2447. doi:10.1182/blood.v98.8.2442
Reçber, T., Haznedaroğlu, İ. C., and Çelebier, M. (2020). Review on Characteristics and Analytical Methods of Rivaroxaban. Crit. Rev. Anal. Chem., 1–13. doi:10.1080/10408347.2020.1839735
Rinschen, M. M., Ivanisevic, J., Giera, M., and Siuzdak, G. (2019). Identification of Bioactive Metabolites Using Activity Metabolomics. Nat. Rev. Mol. Cell Biol 20, 353–367. doi:10.1038/s41580-019-0108-4
Rollin, J., Pouplard, C., Gratacap, M. P., Leroux, D., May, M. A., Aupart, M., et al. (2012). Polymorphisms of Protein Tyrosine Phosphatase CD148 Influence FcγRIIA-dependent Platelet Activation and the Risk of Heparin-Induced Thrombocytopenia. Blood 120, 1309–1316. doi:10.1182/blood-2012-04-424044
Rollin, J., Pouplard, C., Leroux, D., May, M. A., and Gruel, Y. (2013). Impact of Polymorphisms Affecting the ACP1 Gene on Levels of Antibodies against Platelet Factor 4-Heparin Complexes. J. Thromb. Haemost. 11, 1609–1611. doi:10.1111/jth.12278
Rollin, J., Pouplard, C., Sung, H. C., Leroux, D., Saada, A., Gouilleux-Gruart, V., et al. (2015). Increased Risk of Thrombosis in FcγRIIA 131RR Patients with HIT Due to Defective Control of Platelet Activation by Plasma IgG2. Blood 125, 2397–2404. doi:10.1182/blood-2014-09-594515
Selleng, K., Schütt, A., Selleng, S., Warkentin, T. E., and Greinacher, A. (2010). Studies of the Anti-platelet Factor 4/heparin Immune Response: Adapting the Enzyme-Linked Immunosorbent Spot Assay for Detection of Memory B Cells against Complex Antigens. Transfusion 50, 32–39. doi:10.1111/j.1537-2995.2009.02360.x
Senis, Y. A., Tomlinson, M. G., Ellison, S., Mazharian, A., Lim, J., Zhao, Y., et al. (2009). The Tyrosine Phosphatase CD148 Is an Essential Positive Regulator of Platelet Activation and Thrombosis. Blood 113, 4942–4954. doi:10.1182/blood-2008-08-174318
Seo, Y., Schenauer, M. R., and Leary, J. A. (2011). Biologically Relevant Metal-Cation Binding Induces Conformational Changes in Heparin Oligosaccharides as Measured by Ion Mobility Mass Spectrometry. Int. J. Mass. Spectrom. 303, 191–198. doi:10.1016/j.ijms.2011.02.003
Shao, C., Zhang, F., Kemp, M. M., Linhardt, R. J., Waisman, D. M., Head, J. F., et al. (2006). Crystallographic Analysis of Calcium-dependent Heparin Binding to Annexin A2. J. Biol. Chem. 281, 31689–31695. doi:10.1074/jbc.M604502200
Shen, X., Klarić, L., Sharapov, S., Mangino, M., Ning, Z., Wu, D., et al. (2017). Multivariate Discovery and Replication of Five Novel Loci Associated with Immunoglobulin G N-Glycosylation. Nat. Commun. 8, 447. doi:10.1038/s41467-017-00453-3
Siegbahn, A., Lindbäck, J., Hijazi, Z., Åberg, M., Alexander, J. H., Eikelboom, J. W., et al. (2021). Multiplex Protein Screening of Biomarkers Associated with Major Bleeding in Patients with Atrial Fibrillation Treated with Oral Anticoagulation. J. Thromb. Haemost. 19, 2726–2737. doi:10.1111/jth.15498
Smythe, M. A., Koerber, J. M., and Mattson, J. C. (2007). The Incidence of Recognized Heparin-Induced Thrombocytopenia in a Large, Tertiary Care Teaching Hospital. Chest 131, 1644–1649. doi:10.1378/chest.06-2109
Sobczak, A. I. S., Pitt, S. J., and Stewart, A. J. (2018). Influence of Zinc on Glycosaminoglycan Neutralisation during Coagulation. Metallomics 10, 1180–1190. doi:10.1039/c8mt00159f
Staibano, P., Arnold, D. M., Bowdish, D. M., and Nazy, I. (2017). The Unique Immunological Features of Heparin-Induced Thrombocytopenia. Br. J. Haematol. 177, 198–207. doi:10.1111/bjh.14603
Stark, R., Grzelak, M., and Hadfield, J. (2019). RNA Sequencing: the Teenage Years. Nat. Rev. Genet. 20, 631–656. doi:10.1038/s41576-019-0150-2
Stein, P. D., Hull, R. D., Matta, F., Yaekoub, A. Y., and Liang, J. (2009). Incidence of Thrombocytopenia in Hospitalized Patients with Venous Thromboembolism. Am. J. Med. 122, 919–930. doi:10.1016/j.amjmed.2009.03.026
Sturtzel, C. (2017). Endothelial Cells. Adv. Exp. Med. Biol. 1003, 71–91. doi:10.1007/978-3-319-57613-8_4
Suvarna, S., Espinasse, B., Qi, R., Lubica, R., Poncz, M., Cines, D. B., et al. (2007). Determinants of PF4/heparin Immunogenicity. Blood 110, 4253–4260. doi:10.1182/blood-2007-08-105098
Tabor, H. K., Risch, N. J., and Myers, R. M. (2002). Candidate-gene Approaches for Studying Complex Genetic Traits: Practical Considerations. Nat. Rev. Genet. 3, 391–397. doi:10.1038/nrg796
Tam, V., Patel, N., Turcotte, M., Bossé, Y., Paré, G., and Meyre, D. (2019). Benefits and Limitations of Genome-wide Association Studies. Nat. Rev. Genet. 20, 467–484. doi:10.1038/s41576-019-0127-1
Tardy, B., Lecompte, T., Mullier, F., Vayne, C., and Pouplard, C. (2020). Detection of Platelet-Activating Antibodies Associated with Heparin-Induced Thrombocytopenia. J. Clin. Med. 9, 1226. doi:10.3390/jcm9041226
Trikalinos, T. A., Karassa, F. B., and Ioannidis, J. P. (2001). Meta-analysis of the Association between Low-Affinity Fcgamma Receptor Gene Polymorphisms and Hematologic and Autoimmune Disease. Blood 98, 1634–1635. doi:10.1182/blood.v98.5.1634
Tutwiler, V., Madeeva, D., Ahn, H. S., Andrianova, I., Hayes, V., Zheng, X. L., et al. (2016). Platelet Transactivation by Monocytes Promotes Thrombosis in Heparin-Induced Thrombocytopenia. Blood 127, 464–472. doi:10.1182/blood-2013-11-539262
Van Rees, D. J., Szilagyi, K., Kuijpers, T. W., Matlung, H. L., and Van Den Berg, T. K. (2016). Immunoreceptors on Neutrophils. Semin. Immunol. 28, 94–108. doi:10.1016/j.smim.2016.02.004
Vos, Q., Lees, A., Wu, Z. Q., Snapper, C. M., and Mond, J. J. (2000). B-cell Activation by T-cell-independent Type 2 Antigens as an Integral Part of the Humoral Immune Response to Pathogenic Microorganisms. Immunological Rev. 176, 154–170. doi:10.1034/j.1600-065x.2000.00607.x
Vu, T. T., Fredenburgh, J. C., and Weitz, J. I. (2013). Zinc: An Important Cofactor in Haemostasis and Thrombosis. Thromb. Haemost. 109, 421–430. doi:10.1160/TH12-07-0465
Warkentin, T. E., and Greinacher, A. (2016). Management of Heparin-Induced Thrombocytopenia. Curr. Opin. Hematol. 23, 462–470. doi:10.1097/MOH.0000000000000273
Warkentin, T. E., Hayward, C. P., Boshkov, L. K., Santos, A. V., Sheppard, J. A., Bode, A. P., et al. (1994). Sera from Patients with Heparin-Induced Thrombocytopenia Generate Platelet-Derived Microparticles with Procoagulant Activity: an Explanation for the Thrombotic Complications of Heparin-Induced Thrombocytopenia. Blood 84, 3691–3699. doi:10.1182/blood.v84.11.3691.bloodjournal84113691
Warkentin, T. E., Levine, M. N., Hirsh, J., Horsewood, P., Roberts, R. S., Gent, M., et al. (1995). Heparin-induced Thrombocytopenia in Patients Treated with Low-Molecular-Weight Heparin or Unfractionated Heparin. N. Engl. J. Med. 332, 1330–1335. doi:10.1056/NEJM199505183322003
Warkentin, T. E., Sheppard, J. A., Horsewood, P., Simpson, P. J., Moore, J. C., and Kelton, J. G. (2000). Impact of the Patient Population on the Risk for Heparin-Induced Thrombocytopenia. Blood 96, 1703–1708. doi:10.1182/blood.v96.5.1703.h8001703_1703_1708
Warkentin, T. E., and Sheppard, J. A. (2014). Serological Investigation of Patients with a Previous History of Heparin-Induced Thrombocytopenia Who Are Reexposed to Heparin. Blood 123, 2485–2493. doi:10.1182/blood-2013-10-533083
Warkentin, T. E., and Kelton, J. G. (2001). Temporal Aspects of Heparin-Induced Thrombocytopenia. N. Engl. J. Med. 344, 1286–1292. doi:10.1056/nejm200104263441704
Witkowski, M., Weeks, T. L., and Hazen, S. L. (2020). Gut Microbiota and Cardiovascular Disease. Circ. Res. 127, 553–570. doi:10.1161/CIRCRESAHA.120.316242
Witten, A., Bolbrinker, J., Barysenka, A., Huber, M., Rühle, F., Nowak-Göttl, U., et al. (2018). Targeted Resequencing of a Locus for Heparin-Induced Thrombocytopenia on Chromosome 5 Identified in a Genome-wide Association Study. J. Mol. Med. (Berl) 96, 765–775. doi:10.1007/s00109-018-1661-6
Xia, C. Q., and Kao, K. J. (2003). Effect of CXC Chemokine Platelet Factor 4 on Differentiation and Function of Monocyte-Derived Dendritic Cells. Int. Immunol. 15, 1007–1015. doi:10.1093/intimm/dxg100
Xia, C. Q., and Kao, K. J. (2002). Heparin Induces Differentiation of CD1a+ Dendritic Cells from Monocytes: Phenotypic and Functional Characterization. J. Immunol. 168, 1131–1138. doi:10.4049/jimmunol.168.3.1131
Xiao, Z., Visentin, G. P., Dayananda, K. M., and Neelamegham, S. (2008). Immune Complexes Formed Following the Binding of Anti-platelet Factor 4 (CXCL4) Antibodies to CXCL4 Stimulate Human Neutrophil Activation and Cell Adhesion. Blood 112, 1091–1100. doi:10.1182/blood-2008-04-153288
Zhang, F., Liang, X., Beaudet, J. M., Lee, Y., and Linhardt, R. J. (2014). The Effects of Metal Ions on Heparin/heparin Sulfate-Protein Interactions. J. Biomed. Technol. Res. 1. doi:10.19104/jbtr.2014.101
Zhang, R., Duffy, B. F., Lange, V., Eby, C. S., and Liu, C. (2019). Association between the HLA-Drb1*03:01-Dqb1*02:01 Haplotype and PF4/heparin Antibodies. Blood Adv. 3, 3136–3142. doi:10.1182/bloodadvances.2019000311
Zhang, Y., Liu, X., Liu, L., Zaske, A. M., Zhou, Z., Fu, Y., et al. (2013). Contact- and Agonist-Regulated Microvesiculation of Human Platelets. Thromb. Haemost. 110, 331–339. doi:10.1160/TH12-11-0853
Zheng, Y., Yu, M., Padmanabhan, A., Aster, R. H., Yuan, L., Wen, R., et al. (2015). Critical Role of CD4 T Cells in PF4/heparin Antibody Production in Mice. Blood 125, 1826–1829. doi:10.1182/blood-2014-09-603464
Zhou, Y., Abraham, S., Renna, S., Edelstein, L. C., Dangelmaier, C. A., Tsygankov, A. Y., et al. (2016). TULA-2 (T-Cell Ubiquitin Ligand-2) Inhibits the Platelet Fc Receptor for IgG IIA (FcγRIIA) Signaling Pathway and Heparin-Induced Thrombocytopenia in Mice. Arterioscler Thromb. Vasc. Biol. 36, 2315–2323. doi:10.1161/ATVBAHA.116.307979
Zhu, W., Gregory, J. C., Org, E., Buffa, J. A., Gupta, N., Wang, Z., et al. (2016). Gut Microbial Metabolite TMAO Enhances Platelet Hyperreactivity and Thrombosis Risk. Cell 165, 111–124. doi:10.1016/j.cell.2016.02.011
Keywords: heparin-induced thrombocytopenia, adverse drug reaction, t-cell, neutrophil, genomics, transcriptomics, metagenomic, proteomic
Citation: Giles JB, Miller EC, Steiner HE and Karnes JH (2022) Elucidation of Cellular Contributions to Heparin-Induced Thrombocytopenia Using Omic Approaches. Front. Pharmacol. 12:812830. doi: 10.3389/fphar.2021.812830
Received: 10 November 2021; Accepted: 31 December 2021;
Published: 21 January 2022.
Edited by:
Elena García-Martín, University of Extremadura, SpainReviewed by:
Christina Lamers, University of Basel, SwitzerlandCopyright © 2022 Giles, Miller, Steiner and Karnes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jason H. Karnes, a2FybmVzQHBoYXJtYWN5LmFyaXpvbmEuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.