
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 13 December 2021
Sec. Pharmacoepidemiology
Volume 12 - 2021 | https://doi.org/10.3389/fphar.2021.789783
 Clara L. Rodríguez-Bernal1,2*
Clara L. Rodríguez-Bernal1,2* Francisco Sanchez-Saez1,2
Francisco Sanchez-Saez1,2 Daniel Bejarano-Quisoboni1
Daniel Bejarano-Quisoboni1 Judit Riera-Arnau3
Judit Riera-Arnau3 Gabriel Sanfélix-Gimeno1,2†
Gabriel Sanfélix-Gimeno1,2† Isabel Hurtado1,2†
Isabel Hurtado1,2†Objective: Despite the continuous update of clinical guidelines, little is known about the real-world management of patients with atrial fibrillation (AF) who survived a stroke. We aimed to assess patterns of therapeutic management of stroke survivors with AF and clinical outcomes using data from routine practice in a large population-based cohort.
Methods: A population-based retrospective cohort study of all patients with AF who survived a stroke, from January 2010 to December 2017 in the Valencia region, Spain (n = 10,986), was carried out. Treatment strategies and mean time to treatment initiation are described. Temporal trends are shown by the management pattern during the study period. Factors associated with each pattern (including no treatment) vs. oral anticoagulant (OAC) treatment were identified using logistic multivariate regression models. Incidence rates of clinical outcomes (mortality, stroke/TIA, GI bleeding, and ACS) were also estimated by the management pattern.
Results: Among stroke survivors with AF, 6% were non-treated, 23% were prescribed antiplatelets (APT), 54% were prescribed OAC, and 17% received OAC + APT at discharge. Time to treatment was 8.0 days (CI 7.6–8.4) for APT, 9.86 (CI 9.52–10.19) for OAC, and 16.47 (CI 15.86–17.09) for OAC + APT. Regarding temporal trends, management with OAC increased by 20%, with a decrease of 50% for APT during the study period. No treatment and OAC + APT remained relatively stable. The strongest predictor of no treatment and APT treatment was having the same management strategy pre-stroke. Those treated with APT had the highest rates of GI bleeding and recurrent stroke/TIA, and untreated patients showed the highest rates of mortality.
Conclusion: In this large population-based cohort using real-world data, nearly 30% of AF patients who suffered a stroke were untreated or treated with APT, which overall is not recommended. Treatment was started within 2 weeks as recommended, except for OAC + APT, which was started later. The strong association of APT treatment or non-treatment with the same treatment strategy before stroke occurrence suggests a strong therapeutic inertia and opposes recommendations. Patients under these two strategies had the highest rates of adverse outcomes. An inadequate prescription poses a great risk on patients with AF and stroke; thus monitoring their management is necessary and should be setting-specific.
Stroke is currently the second leading cause of death and an important contributor to disability-adjusted life years worldwide (Lozano et al., 2012; Murray et al., 2012). Patients who have survived a stroke are at an increased risk of a recurrent event, and recurrent strokes constitute an important proportion (25–30%) of all preventable strokes (Rothwell et al., 2004; Hata et al., 2005; Mohan et al., 2009; Sun et al., 2013; Flach et al., 2020). Atrial Fibrillation (AF), the most common cardiac arrhythmia (Steinberg and Piccini, 2014), increases the risk of stroke and is one of the leading causes of cerebrovascular mortality and morbidity (Jørgensen et al., 1996; Lin et al., 1996).
These figures offer a clear picture of the importance of secondary prevention of stroke in patients with AF. Data on routine management of patients with AF (for primary prevention of stroke) indicate that treatment is poor (Kakkar et al., 2013; Sabouret et al., 2015; Carnero Montoro et al., 2017). However, the occurrence of an adverse event (i.e., a stroke) is likely to compel physicians to modify the therapeutic management of these patients. Furthermore, relatively recent changes, such as the introduction of non-VKA oral anticoagulants (NOAC) into the market, and the development of new thromboembolic and bleeding risk scales (Lane and Lip, 2012) might have changed the management of patients with AF who have survived a stroke. Physicians have to weigh the risk/benefit of preventing the recurrence of stroke while avoiding hemorrhagic events. Additionally, timing of initiation of drug therapy is still an unresolved challenge (Klijn et al., 2019; Seiffge et al., 2019). All these factors make decision making a complex issue for physicians treating these patients. Current recommendations on secondary prevention of stroke in patients with AF suggest antiplatelet therapy in the first 48 h after ischemic stroke and to start anticoagulation therapy at day 3 or 4 from the index stroke in patients with mild stroke and small infarcts (<1.5 cm) and at day 7 for moderate infarcts. In the case of large infarcts, the recommendation is to start OAC therapy at day 14 after the index stroke (Klijn et al., 2019; Seiffge et al., 2019). Antiplatelets are not indicated beyond this initial time (Klijn et al., 2019; Seiffge et al., 2019). However, studies on the real-world management of these patients including the whole picture of all possible treatments (including no treatment) are lacking, and it is unknown if the real world meets guidelines’ recommendations.
Knowledge on patterns of management in the real world, predictors for these treatment patterns and their evolution over time, and clinical outcomes will help the design of strategies to improve the secondary prevention of stroke in these patients.
We aimed to assess patterns of management of stroke survivors with atrial fibrillation and clinical outcomes using data from routine practice in a large population-based cohort.
A population-based retrospective cohort of all patients with a diagnosis of AF, discharged alive following an ischemic stroke or transient ischemic attack (TIA) from any Valencia Health System (VHS) hospital from January 1, 2010, to December 31, 2017, was constructed. Patients were followed for a minimum of 365 days from the date of hospital discharge (index date).
The study was set in the Valencia region and, specifically, in the population covered by the VHS, the public health system serving about 97% of the region’s population (≈5 million inhabitants) providing universal free healthcare services (except drug copayment). We identified all patients aged 18 years and over with AF (diagnosis code of International Classification of Diseases, ninth Revision, Clinical Modification [ICD-9-CM] 427.3x and 10th Revision, Clinical Modification [ICD-10-CM] I48.x), discharged alive from VHS hospitals (index date) with a main diagnosis of acute ischemic stroke or TIA ([ICD-9-CM]/[ICD-10-CM] 433.x1, 434.x1, 436.xx/I63.x, I67.81, I67.82, I67.89 for stroke and 435.x/G45.x, I67.848 for TIA) between 2010 and 2017. One year of look-back period was used to define the baseline characteristics of the population. Patients who died within 30 days after the index date were excluded due to the short timeframe to assess treatment initiation. Also, people without pharmaceutical/health coverage by VHA, mainly some government employees whose prescriptions are reimbursed by civil service mutual insurance companies and thus not included in the pharmacy databases of the VHA, and patients not registered in the municipal census (non-residents or temporary residents) were excluded because of limitations on the follow-up.
Data were obtained from the Valencia Health System Integrated Database (VID), which combines data sources linking them at an individual level through a single anonymized patient identifier. The main source of data was the VHS ambulatory Electronic Medical Record (EMR), which includes information on diagnoses, personal medical history, laboratory test results, lifestyle factors, and information on both physician prescriptions and dispensations from community pharmacies. The information on hospitalizations was based on the minimum basic dataset (MBDS) at hospital discharge, a synopsis of clinical and administrative information on all hospital discharges, including diagnoses and procedures. The population information system (SIP) provides information on the population covered by the VHS and registers certain demographic characteristics, including the geographical location of each person and the dates and causes of VHS discharge, including deaths. A detailed description of the sources of data can be found elsewhere (García-Sempere et al., 2020).
The study was approved by the Institutional Review Board of the Public Health General Directorate of the Valencia Health Authority and the Center for Public Health Research (September 29, 2017) and by the Ethics Committee for Drug Research of the “Hospital Clínico-Universitario de Valencia” (September 5, 2018). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements. All patient data were transferred to the research team anonymized and de-identified prior to analysis. The Regulatory Commission of Access to Ambulatory Care Information of the Valencia Health Authority approved the cession of this anonymized data.
Based on electronic pharmacy data, we assessed therapeutic management, examining the presence (or not) of a prescription (filled or not from the pharmacy) for the drug classes of interest (i.e., antiplatelets and oral anticoagulants). Exposure to three different strategies of antithrombotic therapy (ATT) was considered: antiplatelets (APT), oral anticoagulants (OAC), or both (OAC + APT). Medications included were as follows: 1) For antiplatelets: acetylsalicylic acid, clopidogrel, prasugrel, ticagrelor, triflusal, cilostazol, ticlopidine, and dipyridamole; and 2) For oral anticoagulants: acenocoumarol, warfarin, apixaban, dabigatran, rivaroxaban, or edoxaban. The initial treatment of the patients is assigned considering the start of 20 consecutive days of ATT (or 20 overlapping consecutive days for considering treatment with OAC + APT) within 60 days after hospital discharge from ischemic stroke (IS) or TIA.
We established four clinical outcomes, measured during a follow-up (any time after the index date) as follows: 1) Mortality, 2) Hospitalizations for IS and TIA 3) Hospitalizations for gastrointestinal (GI) bleeding, and 4) Acute coronary syndrome (ACS). Only principal discharge diagnoses based on ICD9CM and ICD10CM (see Supplementary Table S1 for coding on clinical outcomes) were used to define endpoints. Out-of-hospital mortality was collected from the SIP system that, in turn, obtains this information from the mortality register. All outcomes were analyzed separately, and only the first event was considered. Patients were followed from the index date and until the relevant event, health system disenrollment, death, or end of study, whichever came first.
Covariates included relevant socio-demographic and clinical characteristics and measures of health service use at the time of discharge. We identified the following variables: age, gender, and country of origin; Clinical factors included the following: baseline diagnosis (AF or flutter), main diagnosis at admission (stroke or TIA), and several comorbidities including congestive heart failure, hypertension, diabetes mellitus, liver and renal disease, dementia, depression, cancer, coronary heart disease, venous thromboembolism (VTE), intracranial hemorrhage, gastrointestinal bleeding and other bleeding previous to the current admission (see Supplementary Table S1 for codes), and risk scores (CHADS2, CHA2DS2-VASC, and HAS-BLED scores). Health service use variables included preventive medication use in the last 3 months and length of stay.
The study population baseline characteristics are presented as means for continuous variables and frequencies for categorical variables according to each treatment strategy. Temporal trends of treatment initiation (patients starting treatment per month during the study period) were plotted according to the therapeutic strategy. The time to start of treatment was also assessed, as mean number of days from discharge.
Logistic multinomial regression models were used to assess the independent associations between treatment strategies and baseline covariates; then, we estimated the incidence of clinical outcomes and presented unadjusted event rates per 1,000 person-year along with 95% CIs separately for each outcome and for each treatment cohort.
All statistical analyses were conducted using STATA 14® (StataCorp, College Station, TX, United States) and R software, and the 5% level of significance was considered.
The cohort was composed of 10,986 patients with AF, discharged alive after an ischemic stroke or TIA, from which 643 (5.9%) did not receive ATT at discharge, 2,530 (23.0%) were prescribed antiplatelets (APT), 5,900 (53.7%) were prescribed OAC, and 1,913 (17.4%) received both (OAC + APT) (Figure 1).
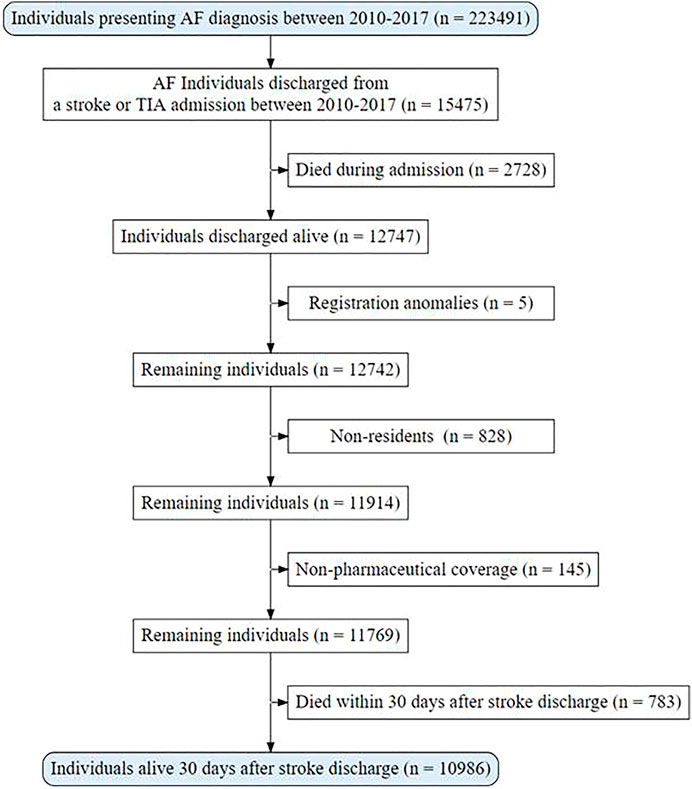
FIGURE 1. Population flowchart.
Overall cohort characteristics and by treatment at discharge are presented in Table 1. The mean age was 78.8 years, 53% of patients were female, and 17% were foreigners. Regarding previous medication use (3 months before suffering the stroke), 34% of patients were not receiving therapy, and similar rates were observed for antiplatelet and anticoagulant use (at around 30% each) before suffering the index stroke. The more prevalent comorbidities were hypertension (75%) and diabetes (32%). The cohort had a mean CHA2DS2-VASC score of 5.58 and a mean HAS BLED score of 3.70.
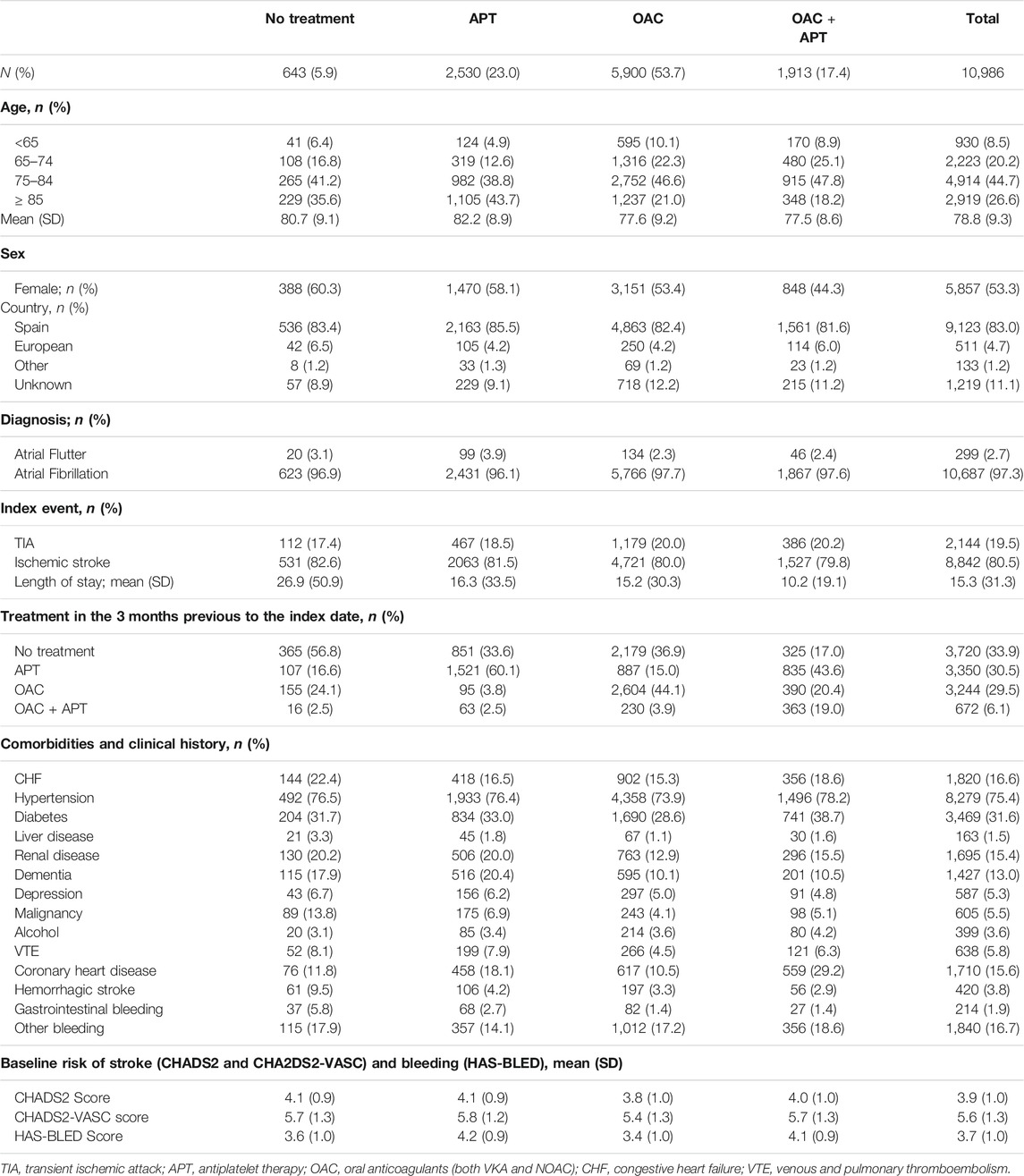
TABLE 1. Characteristics of patients with atrial fibrillation who survived a stroke, by treatment strategy (secondary prevention).
Patients not treated at discharge were mainly women (60%), more likely to be non-treated previously and had more prevalence of hemorrhagic stroke and GI bleeding. Patients prescribed antiplatelets were the eldest (mean age 82.2 years old) and were less likely to be on previous OAC treatment but had higher proportions of comorbidities such as hypertension, dementia, coronary heart disease, and had higher risk scores. Those treated with OAC were more likely to be treated with OAC previously, had a lower prevalence of comorbidities, and had the lowest mean risk scores. Patients prescribed OAC + APT were less likely to be female; their most common previous prescription was antiplatelets and were less likely to have depression, dementia, VTE, and any bleeding. They also had the shortest mean in-hospital stay. Both, patients prescribed OAC and those prescribed OAC + APT were younger, as compared to the other subgroups (mean age 77.6 and 77.5 years old, respectively) (Table 1).
Figure 2 shows treatment patterns over time for the study period (2010–2018).
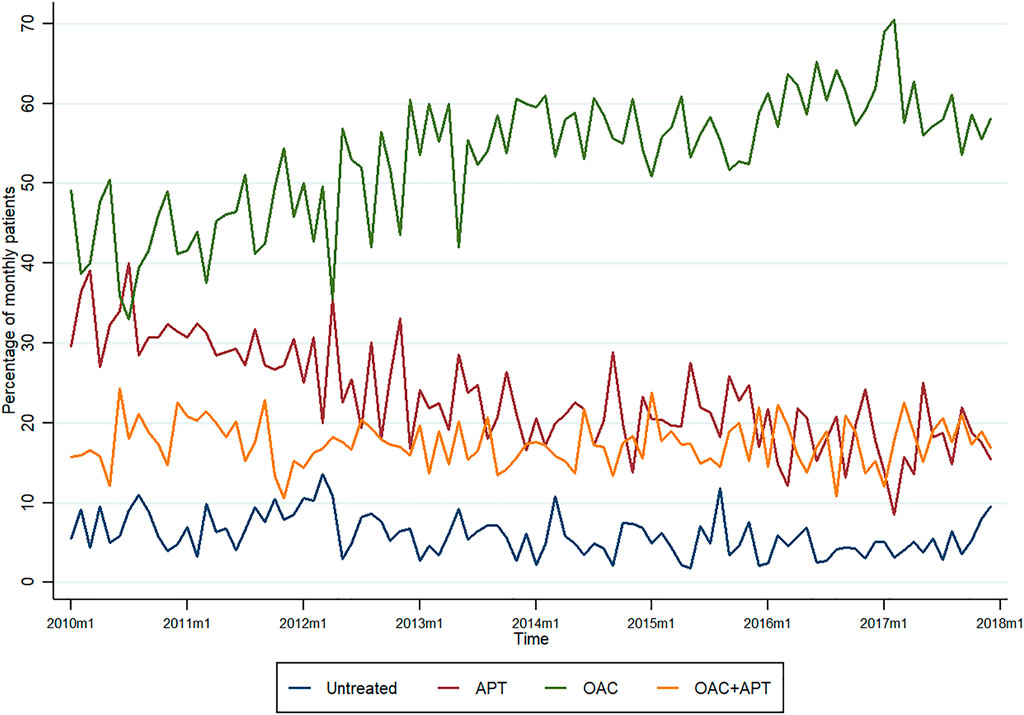
FIGURE 2. Temporal trends of treatment strategies in stroke survivors with atrial fibrillation.
At the beginning of the study period, the proportion of use did not differ much between OAC and APT (ranging from 30 to 40% for APT and from 40 to 50% for OAC), with the percentages of patients with no treatment and those treated with OAC + APT, being considerably lower.
The trend for untreated patients was relatively stable (5–10%) along the study period (although fluctuations are observed). A similar pattern was observed for OAC + APT, ranging from 15 to 20% most of the period.
Overall, there was an increase in the percentage of patients prescribed oral anticoagulants (from nearly 50% at the beginning to just under 60% at the end of the study period), reaching the lowest proportion in mid-2012 (35%) and a peak in 2017 (around 70%), whereas an important decrease in the prescription of antiplatelets is observed (from around 30–15%). The “breaking point” being 2012, when a steep rise is observed for OAC and an important reduction (halving the proportion of prescriptions) is observed for APT over time (Figure 2).
Table 2 shows mean time (in days) to treatment initiation from index date, by treatment strategy. Patients treated with APT had the shortest time to start of treatment (8.02; CI: 7.59–8.45), followed by OAC patients (9.86; CI: 9.52–10.19). Patients managed with OAC + APT had the longest time to treatment (16.47; 15.86–17.09), doubling that of APT patients.
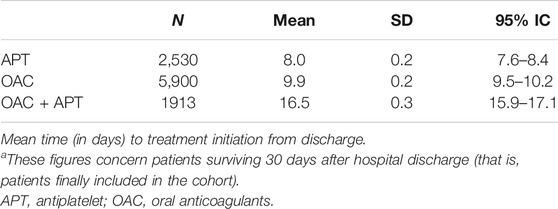
TABLE 2. Time to treatment initiation from dischargea in a cohort of patients with atrial fibrillation who survived a stroke, by treatment strategy (secondary prevention).
In the adjusted analysis, compared to OAC treatment, no treatment antiplatelet treatment post-stroke were positively associated with female sex and certain comorbidities such as congestive heart failure, liver or renal disease, dementia, cancer and VTE, and previous bleeding (IC hemorrhage and GI bleeding). However, the strongest predictors were previous treatment being the same as the current treatment strategy. See Figure 3 and Supplementary Table S2.
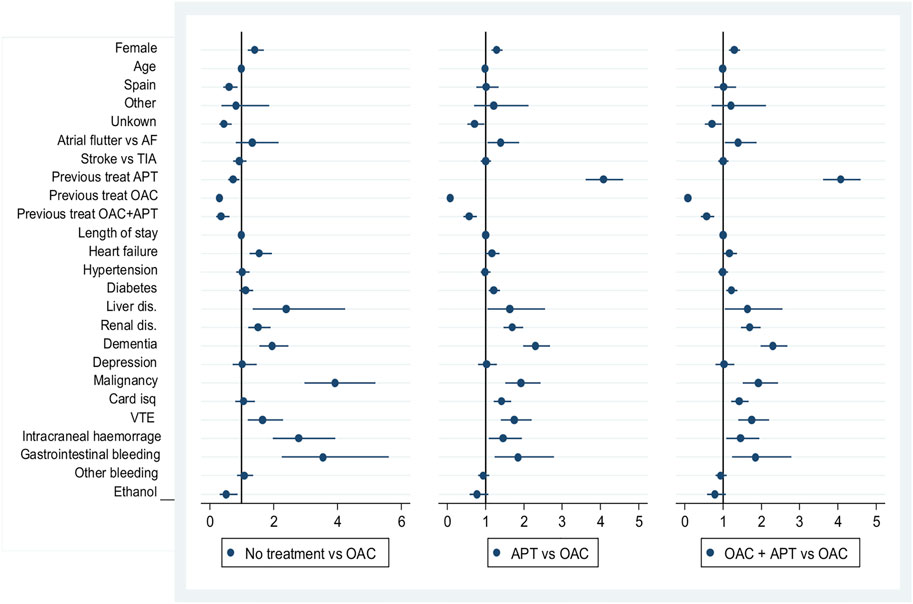
FIGURE 3. Predictors of treatment strategies in stroke survivors with atrial fibrillation.
Predictors of the combined OAC + APT prescription were previous use of the same treatment strategy (OR 7.56, 95% CI: 6.11–9.35) or previous antiplatelet use (OR 5.3, 95% CI: 4.54–6.19) and to a lesser extent diabetes, liver disease, coronary heart disease, and VTE.
Incident rates of the clinical outcomes assessed are shown in Table 3.
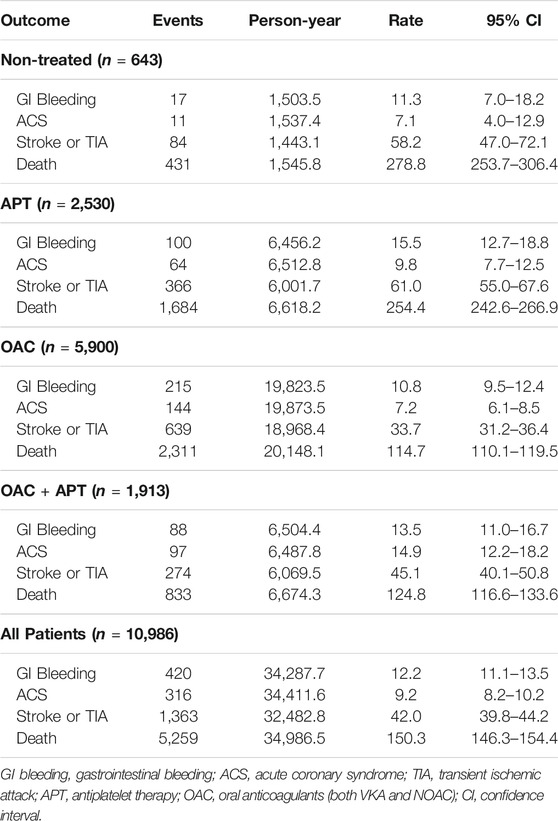
TABLE 3. Incidence rates of clinical outcomes in patients with atrial fibrillation who survived a stroke, by treatment strategy.
Incident rates of GI bleeding for the whole population were 12.25 per 1,000 person-years (95% CI: 11.13–13.48), with the highest rates seen for those treated with APT (15.49, 95% CI: 12.73–18.84) and the lowest rates seen for OAC-treated patients (10.48, 95% CI: 9.49–12.39).
Regarding ACS, incident rates for the whole population were 9.18 per 1,000 person-years (95% CI: 8.22–10.22). Patients treated with OAC + APT showed the highest rates of ACS (14.95, 95% CI: 12.25–18.24), whereas those untreated showed the lowest rates (7.15, 95% CI: 3.96–12.92).
Incident rates for recurrent stroke were 41.96 per 1,000 person-years (95% CI: 39.79–44.25) overall, with the highest rates seen for those treated with APT (60.98, 95% CI: 55.04–67.56) and the lowest rates seen for patients treated with OAC (33.69, 95% CI: 31.17–36.40).
Regarding mortality, incident rates were 150.31 per 1,000 person-years (95% CI: 146.3–154.4) overall. Patients not receiving treatment showed the highest rates of mortality (278.82, 95% CI: 253.7–306.4) whereas those treated with OAC showed the lowest rates (114.7, 95% CI: 110.1–119.5).
Despite the existence of clinical guidelines and given the complexity of decision-making physicians face with these patients, the real-life management of people with AF who have survived a stroke and the extent to which recommendations are met are largely unknown to date. We identified a large population-based cohort of patients with AF, discharged alive after a stroke, and found four treatment strategies adopted by their physicians: no treatment (6%), antiplatelet treatment (23%), OAC treatment (54%), and OAC + antiplatelets (17%), meaning that–at least-about one-third of the patients with AF did not receive the recommended therapy after suffering a stroke. Regarding temporal trends in the treatment strategies, overall, an increase in the case of OAC and reduction in the case of APT is observed, especially from 2012 onwards. Prescription trends in these two treatments behave like a “mirror” with increases in use of one of them corresponding with decreases in use of the other, suggesting that a high proportion of those patients treated with antiplatelets at the beginning of the study period are being treated with OAC at the end. No treatment and OAC + APT treatment remained relatively stable along the study period, although slight fluctuations were observed. Time to treatment initiation ranged between 8 days for APT patients and 16 days for OAC + APT patients.
The most important predictors of no treatment or antiplatelet treatment (vs. OAC) were having previously the same treatment strategy, previous bleeding, female sex, and certain comorbidities. Regarding OAC + APT treatment, the strongest predictors were the previous use of the same treatment strategy or antiplatelets and to a lesser extent diabetes, liver disease, ischemic heart disease, and VTE.
Regarding clinical outcomes, we found that patients treated with OAC (the recommended therapy, overall) had the lowest rates of GI bleeding, recurrent stroke/TIA, and mortality, whereas those treated with APT had the highest rates of GI bleeding and recurrent stroke/TIA. Those treated with OAC + APT showed the highest rates of ACS, and untreated patients showed the highest rates of mortality (followed by those treated with APT).
Guidelines recommend long-term OAC treatment for the secondary prevention of stroke in patients with AF (Kernan et al., 2014; Klijn et al., 2019) and OAC in combination with antiplatelet treatment—mainly P2Y12 inhibitors—in the case of acute coronary syndrome co-existence (Klijn et al., 2019; Hindricks et al., 2021). Therefore, the finding of 6% of patients receiving no treatment at all and 23% receiving only antiplatelets after suffering a stroke shows a huge room for improvement in the management of these patients. It is true that when analyzing the time trends of routine care, we observed a decrease in the prescription of antiplatelet treatment, but still around 15% of patients were treated with these drugs at the end of the study period (2018). The great increase in the use of OAC and corresponding decrease in that of APT from 2012 onwards, might be a consequence of diverse factors: 1) the introduction into the market of NOAC drugs, which happened at the end of 2011 in Spain and grew rapidly as a safe-and in many cases was seen as a more convenient-alternative to VKA, increasing the initial OAC prescription in patients with AF both in Spain (Rodríguez-Bernal et al., 2017) and overseas (Desai et al., 2014). 2) The change in recommendations for management of these patients, with USA guidelines explicitly stating in 2014 that antiplatelet therapy cannot be recommended for stroke prevention in AF patients (Kernan et al., 2014), a recommendation adopted later on by European guidelines, with OAC therapy recommended over no treatment or antiplatelet treatment for secondary stroke prevention (Klijn et al., 2019).
In regards to time to treatment initiation (not taking into account the therapeutic strategy used), it was within the recommended days 3–14, except for OAC + APT, which was started later. These figures concern patients surviving 30 days after hospital discharge (that is, patients finally included in the cohort). It has been shown that patients treated with OAC after 14 days, have a higher risk of an ischemic event or bleeding (Paciaroni et al., 2015). It could be assumed that it applies also for combined therapy.
Regarding predictors of treatment strategy in the real world, we found that the most important predictors of no treatment or antiplatelet treatment (vs. OAC) were having previously the same treatment strategy, previous bleeding, female sex, and certain comorbidities. Keeping AF patients untreated or treated with APT even after suffering a stroke, suggests a strong therapeutic inertia (Khunti and Davies, 2017) for the management of stroke survivors with AF. The fact that previous bleeding was also a strong determinant shows the reluctance of physicians to prescribe OAC to patients with a high or moderate bleeding risk. However, it has been shown that APT has a similar (or even higher in the elderly) bleeding risk than OAC, but an inferior profile in avoiding stroke events (Mant et al., 2007; Lip, 2011). Regarding female sex as a determinant for no treatment or APT treatment, this team of researchers finds no reasonable explanation for this association.
Stroke occurrence and age are the most important risk factors for recurrence of stroke (Hindricks et al., 2021); therefore, it is likely that an important percentage of these patients suffer a preventable undesired event as a consequence of the undertreatment. In fact, when assessing the association of each management strategy with clinical outcomes, we found that patients treated with APT had the highest rates of GI bleeding and recurrent stroke/TIA, whereas untreated patients showed the highest rates of mortality. On the other hand, patients treated with OAC had the lowest rates of GI bleeding, recurrent stroke/TIA, and mortality. These results are in line with recommendations on OAC treatment as the first line therapy in prevention of stroke recurrence.
Our study has reliable data on clinical characteristics including diagnoses and procedures, health service utilization, and prescription and dispensing, and individual-level data on sociodemographics, retrieved through the linkage of several electronic databases including EMR, which is an advantage over studies that base their data on administrative claims. Besides, our cohort is population-based. It uses data of the population covered by the public health system, which virtually covers the totality of the inhabitants of the region. The most important limitation of our study is that information biases due to absent registration, or differing data recording practices in the EMR might exist, although this is an inherent problem of any study using data from routine clinical practice. Moreover, misclassification (on exposure and covariates) is expected to be non-differential across groups of study subjects. Additionally, when constructing the CHADS risk score, INR was not included, given the unavailability of data for INR values. However, it is unlikely that scores have been affected to the extent of misclassifying patients along the score ranges. Finally, we present clinical outcome incidence in a descriptive manner, so no associations or causal relationships can be inferred.
In this large population-based cohort using real-world data, nearly 30% of AF patients who suffered a stroke received no treatment or were treated with APT, which overall is not recommended. Treatment was started within 2 weeks as recommended, except for OAC + APT, which was started later. The strong association of APT treatment or no treatment with the same management before stroke occurrence suggests a strong therapeutic inertia and opposes recommendations. These two management strategies were associated with the highest rates of most adverse outcomes assessed. An inadequate prescription poses a great risk on patients with AF and stroke; thus, monitoring their management is necessary and should be setting-specific.
The datasets presented in this article are not readily available because we have no permission to make generated datasets available. We have been granted access to data by the Valencia Health Department, so we could make the analysis for this study but are not allowed to share it. Requests to access the datasets should be directed to Unit of Analysis of Health Information Systems (Servicio de Análisis De Sistemas de Información Sanitaria). Valencia Health Department (www.san.gva.es).
The studies involving human participants were reviewed and approved by the Institutional Review Board of the Public Health General Directorate of the Valencia Health Authority and the Center for Public Health Research (September 29, 2017) and by the Ethics Committee for Drug Research of the “Hospital Clínico-Universitario de Valencia” (September 5, 2018). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements. All patient data were transferred to the research team anonymized and de-identified prior to analysis. The Regulatory Commission of Access to Ambulatory Care Information of the Valencia Health Authority approved the cession of this anonymized data.
GS-G conceived the study. IH carried out the main statistical analyses. CR-B drafted the manuscript with relevant input from GS-G. FS-S and DB-Q prepared the database and assisted with statistical analysis. CR-B, FS-S, DB-Q, JR-A, IH, and GS-G participated in the study design and interpretation of data and contributed to the critical revision of the manuscript for important intellectual content. All authors agree to be accountable for all aspects of the work and have read and approved the final manuscript.
CR-B was funded at the start of this work by the Instituto de Salud Carlos III, Spanish Ministry of Health, co-financed by the European Regional Development Fund (grant number RD16/0001/0011) and currently through a competitive grant (Sara Borrell CD19/00137). FS-S was funded by the Instituto de Salud Carlos III, Spanish Ministry of Health through the REDISSEC network (grant number RD16/0001/0011). The views presented here are those of the authors and not necessarily those of the FISABIO Foundation, the Valencia Ministry of Health or the study sponsors. The funding sources have no access to study data, did not participate in any way in the design or conduct of the study, data analysis, or decisions regarding the dissemination of findings, the development of the manuscript, or its publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2021.789783/full#supplementary-material
Carnero Montoro, L., Roldán Rabadán, I., Marín Ortuño, F., Bertomeu Martínez, V., Muñiz García, J., and Anguita Sánchez, M. (2017). Differences in the Characteristics and Management of Patients with Atrial Fibrillation Followed-Up by Cardiologists and Other Specialists. Rev. Esp Cardiol. (Engl Ed. 70 (10), 883–886. English, Spanish. doi:10.1016/j.rec.2016.11.038
Desai, N. R., Krumme, A. A., Schneeweiss, S., Shrank, W. H., Brill, G., Pezalla, E. J., et al. (2014). Patterns of Initiation of Oral Anticoagulants in Patients with Atrial Fibrillation- Quality and Cost Implications. Am. J. Med. 127 (11), 1075–1082.e1. doi:10.1016/j.amjmed.2014.05.013
Flach, C., Muruet, W., Wolfe, C. D. A., Bhalla, A., and Douiri, A. (2020). Risk and Secondary Prevention of Stroke Recurrence: A Population-Base Cohort Study. Stroke 51 (8), 2435–2444. doi:10.1161/STROKEAHA.120.028992
García-Sempere, A., Orrico-Sánchez, A., Muñoz-Quiles, C., Hurtado, I., Peiró, S., Sanfélix-Gimeno, G., et al. (2020). Data Resource Profile: The Valencia Health System Integrated Database (VID). Int. J. Epidemiol. 49 (3), 740–741e. doi:10.1093/ije/dyz266
Hata, J., Tanizaki, Y., Kiyohara, Y., Kato, I., Kubo, M., Tanaka, K., et al. (2005). Ten Year Recurrence after First Ever Stroke in a Japanese Community: The Hisayama Study. J. Neurol. Neurosurg. Psychiatry 76 (3), 368–372. doi:10.1136/jnnp.2004.038166
Hindricks, G., Potpara, T., Dagres, N., Arbelo, E., Bax, J. J., Blomström-Lundqvist, C., et al. ESC Scientific Document Group (2021). 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 42 (5), 546–547. Erratum in: Eur Heart J. 2021 Feb 1;42(5):507. Erratum in: Eur Heart J. 2021 Feb 1;42(5):373-498. PMID: 32860505. doi:10.1093/eurheartj/ehaa612
Jørgensen, H. S., Nakayama, H., Reith, J., Raaschou, H. O., and Olsen, T. S. (1996). Acute Stroke with Atrial Fibrillation. The Copenhagen Stroke Study. Stroke 27 (10), 1765–1769. doi:10.1161/01.str.27.10.1765
Kakkar, A. K., Mueller, I., Bassand, J. P., Fitzmaurice, D. A., Goldhaber, S. Z., Goto, S., et al. GARFIELD Registry Investigators (2013). Risk Profiles and Antithrombotic Treatment of Patients Newly Diagnosed with Atrial Fibrillation at Risk of Stroke: Perspectives from the International, Observational, Prospective GARFIELD Registry. PLoS One 8 (5), e63479. doi:10.1371/journal.pone.0063479
Kernan, W. N., Ovbiagele, B., Black, H. R., Bravata, D. M., Chimowitz, M. I., Ezekowitz, M. D., et al. (2014). Guidelines for the Prevention of Stroke in Patients with Stroke and Transient Ischemic Attack: a Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 45 (7), 2160–2236. Epub 2014 May 1. Erratum in: Stroke. 2015 Feb;46(2):e54. PMID: 24788967. doi:10.1161/STR.0000000000000024
Khunti, K., and Davies, M. J. (2017). Clinical Inertia-Time to Reappraise the Terminology? Prim. Care Diabetes 11 (2), 105–106. doi:10.1016/j.pcd.2017.01.007
Klijn, C. J., Paciaroni, M., Berge, E., Korompoki, E., Kõrv, J., Lal, A., et al. (2019). Antithrombotic Treatment for Secondary Prevention of Stroke and Other Thromboembolic Events in Patients with Stroke or Transient Ischemic Attack and Non-valvular Atrial Fibrillation: A European Stroke Organisation Guideline. Eur. Stroke J. 4 (3), 198–223. doi:10.1177/2396987319841187
Lane, D. A., and Lip, G. Y. (2012). Use of the CHA(2)DS(2)-VASc and HAS-BLED Scores to Aid Decision Making for Thromboprophylaxis in Nonvalvular Atrial Fibrillation. Circulation 126 (7), 860–865. doi:10.1161/CIRCULATIONAHA.111.060061
Lin, H. J., Wolf, P. A., Kelly-Hayes, M., Beiser, A. S., Kase, C. S., Benjamin, E. J., et al. (1996). Stroke Severity in Atrial Fibrillation. The Framingham Study. Stroke 27 (10), 1760–1764. doi:10.1161/01.str.27.10.1760
Lip, G. Y. (2011). The Role of Aspirin for Stroke Prevention in Atrial Fibrillation. Nat. Rev. Cardiol. 8 (10), 602–606. doi:10.1038/nrcardio.2011.112
Lozano, R., Naghavi, M., Foreman, K., Lim, S., Shibuya, K., Aboyans, V., et al. (2012). Global and Regional Mortality from 235 Causes of Death for 20 Age Groups in 1990 and 2010: a Systematic Analysis for the Global Burden of Disease Study 2010. Lancet 380, 2095–2128. doi:10.1016/S0140-6736(12)61728-0
Mant, J., Hobbs, F. D., Fletcher, K., Roalfe, A., Fitzmaurice, D., Lip, G. Y., et al. (2007). Warfarin versus Aspirin for Stroke Prevention in an Elderly Community Population with Atrial Fibrillation (The Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): a Randomised Controlled Trial. Lancet 370 (9586), 493–503. doi:10.1016/S0140-6736(07)61233-1
Mohan, K. M., Crichton, S. L., Grieve, A. P., Rudd, A. G., Wolfe, C. D., and Heuschmann, P. U. (2009). Frequency and Predictors for the Risk of Stroke Recurrence up to 10 Years after Stroke: The South London Stroke Register. J. Neurol. Neurosurg. Psychiatry 80 (9), 1012–1018. doi:10.1136/jnnp.2008.170456
Murray, C. J., Vos, T., Lozano, R., Naghavi, M., Flaxman, A. D., Michaud, C., et al. (2012). Disability-adjusted Life Years (DALYs) for 291 Diseases and Injuries in 21 Regions, 1990-2010: a Systematic Analysis for the Global Burden of Disease Study 2010. Lancet 380, 2197–2223. doi:10.1016/S0140-6736(12)61689-4
Paciaroni, M., Agnelli, G., Falocci, N., Caso, V., Becattini, C., Marcheselli, S., et al. (2015). Early Recurrence and Cerebral Bleeding in Patients with Acute Ischemic Stroke and Atrial Fibrillation: Effect of Anticoagulation and its Timing: The RAF Study. Stroke 46 (8), 2175–2182. doi:10.1161/STROKEAHA.115.008891
Rodríguez-Bernal, C. L., Hurtado, I., García-Sempere, A., Peiró, S., and Sanfélix-Gimeno, G. (2017). Oral Anticoagulants Initiation in Patients with Atrial Fibrillation: Real-World Data from a Population-Based Cohort. Front. Pharmacol. 8, 63. doi:10.3389/fphar.2017.00063
Rothwell, P. M., Coull, A. J., Giles, M. F., Howard, S. C., Silver, L. E., Bull, L. M., et al. (2004). Change in Stroke Incidence, Mortality, Case-Fatality, Severity, and Risk Factors in Oxfordshire, UK from 1981 to 2004 (Oxford Vascular Study). Lancet 363, 1925–1933. doi:10.1016/S0140-6736(04)16405-2
Sabouret, P., Bricard, M., Hermann, M. A., Cotté, F. E., Deret-Bixio, L., and Rushton-Smith, S. (2015). Discrepancy between Guidelines for Stroke Prevention in Atrial Fibrillation and Practice Patterns in Primary Care. The Nationwide French AFIGP Survey. Arch. Cardiovasc. Dis. 108 (11), 544–553. doi:10.1016/j.acvd.2015.05.005
Seiffge, D. J., Werring, D. J., Paciaroni, M., Dawson, J., Warach, S., Milling, T. J., et al. (2019). Timing of Anticoagulation after Recent Ischaemic Stroke in Patients with Atrial Fibrillation. Lancet Neurol. 18 (1), 117–126. doi:10.1016/S1474-4422(18)30356-9
Steinberg, B. A., and Piccini, J. P. (2014). Anticoagulation in Atrial Fibrillation. BMJ 348, g2116. doi:10.1136/bmj.g2116
Keywords: secondary prevention, stroke, atrial fibrillation, real-world data, treatment strategies, oral anticoagulants, antiplatelets
Citation: Rodríguez-Bernal CL, Sanchez-Saez F, Bejarano-Quisoboni D, Riera-Arnau J, Sanfélix-Gimeno G and Hurtado I (2021) Real-World Management and Clinical Outcomes of Stroke Survivors With Atrial Fibrillation: A Population-Based Cohort in Spain. Front. Pharmacol. 12:789783. doi: 10.3389/fphar.2021.789783
Received: 05 October 2021; Accepted: 26 November 2021;
Published: 13 December 2021.
Edited by:
Elisabetta Poluzzi, University of Bologna, ItalyReviewed by:
Julia Perrier, INSERM U1219 Bordeaux Population Health Centre Recherche (BPH), FranceCopyright © 2021 Rodríguez-Bernal, Sanchez-Saez, Bejarano-Quisoboni, Riera-Arnau, Sanfélix-Gimeno and Hurtado. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Clara L. Rodríguez-Bernal, cm9kcmlndWV6X2NsYWJlckBndmEuZXM=
†These authors share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.