
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol. , 18 October 2021
Sec. Drugs Outcomes Research and Policies
Volume 12 - 2021 | https://doi.org/10.3389/fphar.2021.743259
This article is part of the Research Topic Evidence for Assessing Drug Safety and Drug Use in Older People View all 24 articles
 Xiangkai Zhao1,2,3,4,5†
Xiangkai Zhao1,2,3,4,5† Jian Zhang1,2,3,4,5†
Jian Zhang1,2,3,4,5† Jialin Guo1,2,3,4,5Jinxin Wang1,2,3,4,5Yuhui Pan1,2,3,4,5Xue Zhao1,2,3,4,5
Jialin Guo1,2,3,4,5Jinxin Wang1,2,3,4,5Yuhui Pan1,2,3,4,5Xue Zhao1,2,3,4,5 Wentao Sang1,2,3,4,5Kehui Yang1,2,3,4,5Fengyang Xu1,2,3,4,5
Wentao Sang1,2,3,4,5Kehui Yang1,2,3,4,5Fengyang Xu1,2,3,4,5 Feng Xu1,2,3,4,5*
Feng Xu1,2,3,4,5* Yuguo Chen1,2,3,4,5*
Yuguo Chen1,2,3,4,5*Background: Dual antiplatelet therapy combining aspirin with a P2Y12 adenosine diphosphate receptor inhibitor is a therapeutic mainstay for acute coronary syndrome (ACS). However, the optimal choice of P2Y12 adenosine diphosphate receptor inhibitor in elderly (aged ≥65 years) patients remains controversial. We conducted a meta-analysis to compare the efficacy and safety of ticagrelor and clopidogrel in elderly patients with ACS. Methods: We comprehensively searched in Web of Science, EMBASE, PubMed, and Cochrane databases through 29th March, 2021 for eligible randomized controlled trials (RCTs) comparing the efficacy and safety of ticagrelor or clopidogrel plus aspirin in elderly patients with ACS. Four studies were included in the final analysis. A fixed effects model or random effects model was applied to analyze risk ratios (RRs) and hazard ratios (HRs) across studies, and I2 to assess heterogeneity.
Results: A total number of 4429 elderly patients with ACS were included in this analysis, of whom 2170 (49.0%) patients received aspirin plus ticagrelor and 2259 (51.0%) received aspirin plus clopidogrel. The ticagrelor group showed a significant advantage over the clopidogrel group concerning all-cause mortality (HR 0.78, 95% CI 0.63–0.96, I2 = 0%; RR 0.79, 95% CI 0.66–0.95, I2 = 0%) and cardiovascular death (HR 0.71, 95% CI 0.56–0.91, I2 = 0%; RR 0.76, 95% CI 0.62–0.94, I2 = 5%) but owned a higher risk of PLATO major or minor bleeding (HR 1.46, 95% CI 1.13–1.89, I2 = 0%; RR 1.40, 95% CI 1.11–1.76, I2 = 0%). Both the groups showed no significant difference regarding major adverse cardiovascular events (MACEs) (HR 1.06, 95% CI 0.68–1.65, I2 = 77%; RR 1.04, 95% CI 0.69–1.58, I2 = 77%).
Conclusion: For elderly ACS patients, aspirin plus ticagrelor reduces cardiovascular death and all-cause mortality but increases the risk of bleeding. Herein, aspirin plus ticagrelor may extend lifetime for elderly ACS patients compared with aspirin plus clopidogrel. The optimal DAPT for elderly ACS patients may be a valuable direction for future research studies.
Dual antiplatelet therapy (DAPT) combining aspirin with a P2Y12 inhibitor is recommended in patients with ACS (Roffi et al., 2016; Ibanez et al., 2018; Collet et al., 2021). The common P2Y12 inhibitors contain ticagrelor, clopidogrel, prasugrel, and cangrelor (Valgimigli et al., 2018). Elderly ACS patients are commonly accompanied with a higher risk of recurrent ischemic events as well as bleeding complications, raising a critical challenge of selecting the optimal antiplatelet medicine (Capodanno and Angiolillo, 2010). The current guidelines did not give a clear answer to this question (Valgimigli et al., 2018). The problem of antiplatelet strategies in elderly ACS patients had received more clinical attention in recent years, and high-quality clinical studies have been published successively.
Contemporary data from observational studies and randomized controlled trials (RCTs) showed conflicting reports regarding the preference of ticagrelor or clopidogrel in elderly ACS patients. The results of the POPular AGE trial revealed that among elderly patients with non-ST elevation acute coronary syndrome (NSTE-ACS), clopidogrel reduced bleeding events without increasing the combined endpoints of all-cause mortality, myocardial infarction, stroke, and bleeding (Gimbel et al., 2020). However, the summary from a study about the efficacy and safety outcomes of ticagrelor compared with clopidogrel in elderly Chinese ACS patients showed that ticagrelor reduced the risk of MACEs without increasing the risk of bleeding (Wang and Wang, 2016). Besides, several subgroup data of RCTs drew debatable conclusions, and the analysis from the SWEDEHEART registry showed that aspirin plus ticagrelor was associated with a higher mortality, provoking some uncertainties on its use among the elderly (Wallentin et al., 2009; Husted et al., 2012; Capranzano and Angiolillo, 2020; Szummer et al., 2020). Current research studies could not give a perfect answer to this problem. Herein, we planned to conduct a meta-analysis to compare the efficacy and safety of ticagrelor and clopidogrel in elderly patients with ACS.
We comprehensively searched in Web of Science, EMBASE, PubMed, and Cochrane databases through 29th March, 2021 for eligible randomized controlled trials (RCTs) using the following keywords: “acute coronary syndrome,” “unstable angina,” “acute myocardial infarction,” “STEMI,” “NSTEMI,” “dual therapy,” “clopidogrel,” and “ticagrelor.”
Publications were included if they met the following conditions: 1) the design was a randomized clinical trial, 2) studies contained patients with acute coronary syndrome who were aged ≥65 years, 3) studies compared ticagrelor with clopidogrel, and 4) studies reported all-cause mortality, cardiovascular death, myocardial infarction, stroke, or any bleeding events.
We excluded studies that 1) did not report subgroup results about patients aged ≥65 years and 2) were not designed for humans.
Two reviewers (Xiangkai Zhao and Jian Zhang) independently extracted data based on the clinical characteristics of the patients, antiplatelet drugs, inclusion criteria, exclusion criteria, and outcomes after a 1-year follow-up.
The primary endpoints were defined as critical death events (all-cause mortality and cardiovascular death). The secondary endpoints were MACEs (a composite of cardiovascular death, myocardial infarction, or stroke) and bleeding events (PLATO major bleeding, PLATO minor bleeding, fatal bleeding, and PLATO major bleeding or PLATO minor bleeding).
The study selection, data collection, analysis, and reporting of the results were performed on the basis of the Cochrane Handbook for Systematic Reviews of Interventions published by the Cochrane Collaboration. We conducted statistical analysis using the RevMan 5 [Review Manager (RevMan) computer program, version 5.4.1, the Cochrane Collaboration, 2020]. Heterogeneity was assessed by the Q-statistic (p ≤ 0.05 was considered statistically significant) and I2 statistical test. Publication bias was visually estimated by using funnel plots. The fixed effects model (I2 ≤ 50%) or random effects model (I2 > 50%) was used to analyze risk ratios (RRs) or hazard ratios (HRs) across studies. Sensitivity analysis was carried out by using the method of checking the influence of an individual trial on the pooled endpoints by excluding each trial solely. Any discrepancies between the reviewers were solved by discussion. Risk of bias composites randomization generation, allocation concealment, blinding assessment, completeness of follow-up, absence of selective reporting, and other potential biases. The risk of bias of each study was assessed by the Cochrane Collaboration tool. The Grading of Recommendation, Assessment, Development, and Evaluation (GRADE) tool was used for the assessment of the reliability of each outcome. The certainty of the evidence was appraised as high, moderate, low, or very low.
We conducted this study based on previously published studies, and no patients or public were involved in this study.
In total, 13,062 articles were identified through the Web of Science, EMBASE, PubMed, and Cochrane databases (Supplementary Table S1). 13,026 articles were excluded by screening the title and abstract. At last, a total of 36 articles in full text were read, and only four clinical trials (Wallentin et al., 2009; Wang and Wang, 2016; Park et al., 2019; Gimbel et al., 2020) fulfilled the eligibility criteria. The literature search and screening processes are presented in Figure 1.
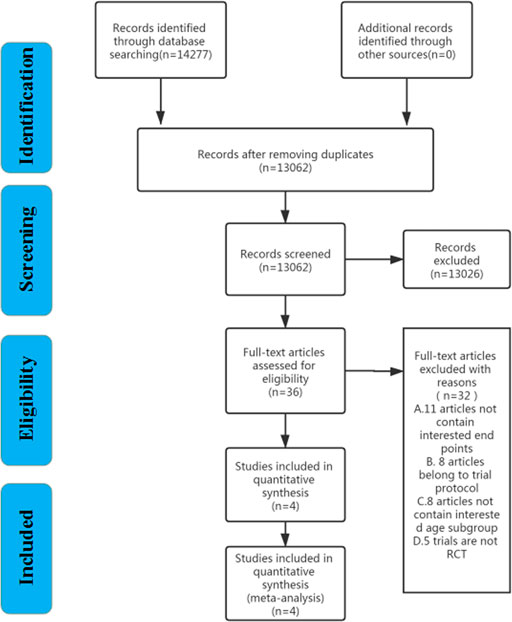
FIGURE 1. Flow diagram of the literature search and study.
The characteristics of the included studies are shown in Table 1. Four studies were included in the final analysis, and all four were prospective randomized controlled trials and reported their results for the 1-year follow-up period. A total number of 4,429 elderly patients with ACS were included in this analysis, 2,170 (49.0%) patients received aspirin plus ticagrelor, and 2,259 (51.0%) received aspirin plus clopidogrel. All participants were 65 years or older. ACS patients were treated with ticagrelor or clopidogrel on the basis of aspirin.
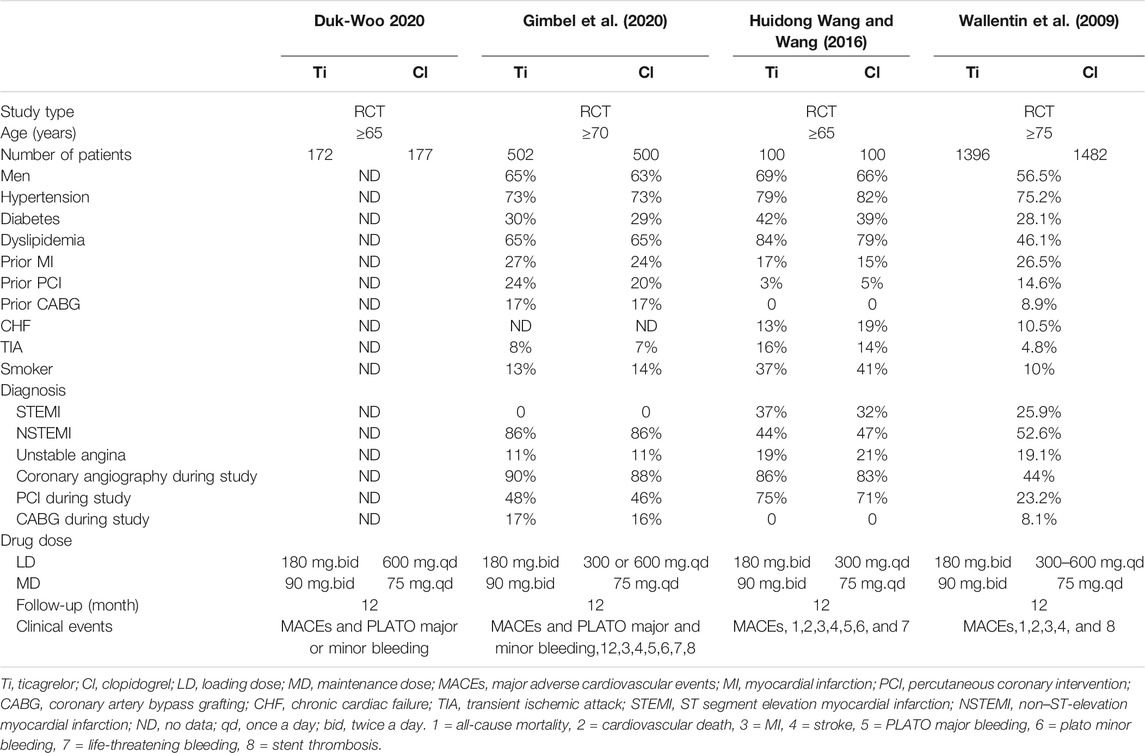
TABLE 1. Characteristics of the included trials.
The assessment of the risk of bias of each study is shown in Supplementary Figure S1, and all four trials had shown a low risk of bias. GRADE assessment shows that the outcomes of MACEs, all-cause mortality, cardiovascular death, MI, and stroke are of high quality, and PLATO major bleeding, PLATO minor bleeding, fatal bleeding, PLATO major or minor bleeding, and stent thrombosis are of low quality (Supplementary Table S2). We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist to improve the reporting quality of our study (Supplementary Table S3).
After a 1-year follow-up, elderly ACS patients who received ticagrelor performed a lower event rate in all-cause mortality (HR 0.78, 95% CI 0.63–0.96, I2 = 0%; RR 0.79, 95% CI 0.66–0.95, I2 = 0%) (Figure 2) and cardiovascular death (HR 0.71, 95% CI 0.56–0.91, I2 = 0%; RR 0.76, 95% CI 0.62–0.94, I2 = 5%) (Figure 3).
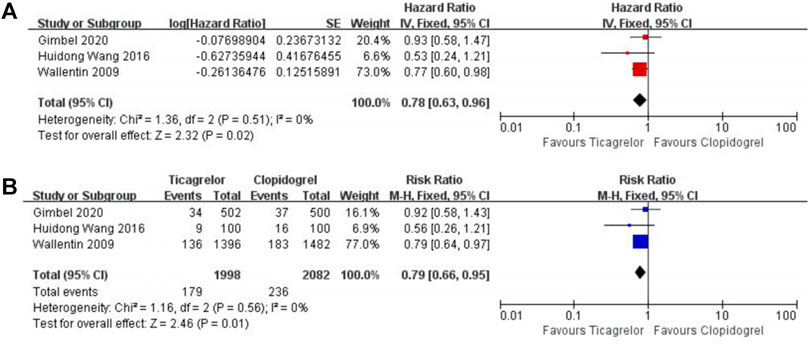
FIGURE 2. Meta-analysis with HR (A), RR (B), and 95% CI for all-cause mortality. Boxes are the relative risk estimates from each study; the horizontal bars are 95% CI. The size of the box is proportional to the weight of the study in the meta-analysis. HR, hazard ratio; RR, risk ratio; CI, confidence interval.
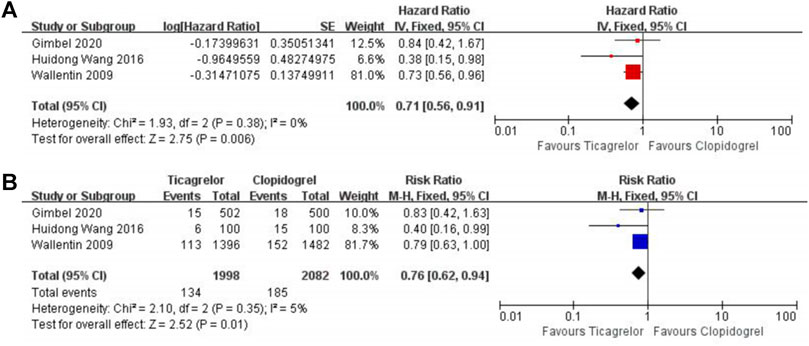
FIGURE 3. Meta-analysis with HR (A), RR (B), and 95% CI for cardiovascular death. Boxes are the relative risk estimates from each study; the horizontal bars are 95% CI. The size of the box is proportional to the weight of the study in the meta-analysis. HR, hazard ratio; RR, risk ratio; CI, confidence interval.
After 1 year of receiving DAPT therapy, ticagrelor showed clinical equipoise in terms of MACEs (HR 1.06, 95% CI 0.68–1.65, I2 = 77%; RR 1.04, 95% CI 0.69–1.58, I2 = 77%) (Figure 4), MI (HR 0.92, 95% CI 0.74–1.15, I2 = 44%; RR 0.94, 95% CI 0.77–1.14, I2 = 45%) (Supplementary Figure S2), stroke (HR 1.55,95% CI 0.98–2.46, I2 = 0%; RR 2.05, 95% CI 1.31–3.22, I2 = 0%) (Supplementary Figure S3), and stent thrombosis (RR 0.44, 95% CI 0.06–3.42, I2 = 57%) (Supplementary Figure S4). As for bleeding risk, the patients who received ticagrelor showed a higher risk of PLATO major or minor bleeding (HR 1.46, 95% CI 1.13–1.89, I2 = 0%; RR 1.40, 95% CI 1.11–1.76, I2 = 0%) (Figure 5). When focused on lethal bleeding (RR 2.71, 95% CI 0.8–9.13, I2 = 44%) (Figure 6), both PLATO major bleeding (HR 1.39, 95% CI 0.94–2.04, I2 = 0%; RR 1.38, 95% CI 0.95–2.00, I2 = 0%) (Supplementary Figure S5) and PLATO minor bleeding (HR 1.37, 95% CI 1.00–1.90, I2 = 0%; RR 1.33, 95% CI 0.99–1.80, I2 = 0%) (Supplementary Figure S6) groups showed a similar risk.
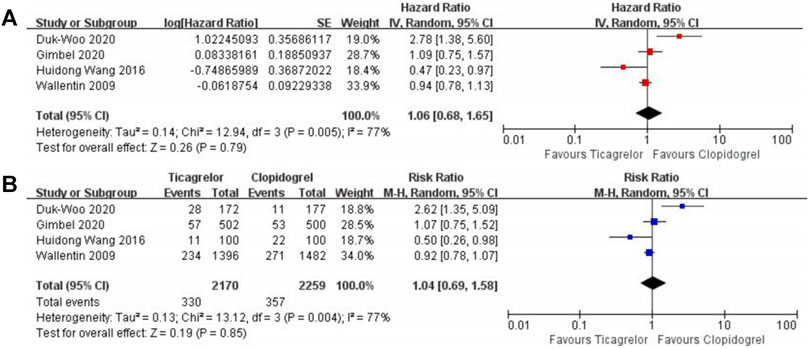
FIGURE 4. Meta-analysis with HR (A), RR (B), and 95% CI for the composite of cardiovascular death, myocardial infarction, and stroke. The boxes are the relative risk estimates from each study; the horizontal bars are 95% CI. The size of the box is proportional to the weight of the study in the meta-analysis. HR, hazard ratio; RR, risk ratio; CI, confidence interval.
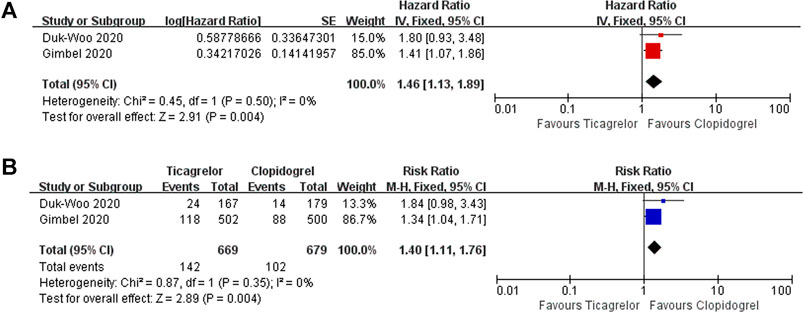
FIGURE 5. Meta-analysis with HR (A), RR (B), and 95% CI for the PLATO major bleeding or minor bleeding. Boxes are the relative risk estimates from each study; the horizontal bars are 95% CI. The size of the box is proportional to the weight of the study in the meta-analysis. HR, hazard ratio; RR, risk ratio; CI, confidence interval.

FIGURE 6. Meta-analysis with RR and 95% CI for fatal bleeding. Boxes are the relative risk estimates from each study; the horizontal bars are 95% CI. The size of the box is proportional to the weight of the study in the meta-analysis. HR, hazard ratio; RR, risk ratio; CI, confidence interval.
The primary finding of our study is that after a 1-year follow-up, aspirin plus ticagrelor reduced all-cause mortality and cardiovascular death but owned a higher risk of PLATO major or minor bleeding than aspirin plus clopidogrel. Our findings provided a new clinical thought for a better choice of P2Y12 adenosine diphosphate receptor inhibitor for elderly ACS patients.
Dual antiplatelet therapy combining aspirin with a P2Y12 adenosine diphosphate receptor inhibitor is a standard regimen for ACS. For the included RCTs, all studies were conducted on the basis of aspirin, so the end events were used for comparing the safety and efficacy between clopidogrel and ticagrelor.
The current guidelines recommended aspirin plus ticagrelor in patients with acute coronary syndrome (Valgimigli et al., 2018), but there was no explicit suggestion for elderly ACS patients. According to the report of the Philippine Heart Association ACS registry, the incidence of ACS was higher in the elderly (Reano et al., 2020). At the same time, older age groups were often excluded from clinical studies. Thus, the optimal choice of P2Y12 adenosine diphosphate receptor inhibitor for elderly patients was necessary to be confirmed as soon as possible. Data from different studies did not reach a consensus for this academic problem. In the famed PLATO study, the ticagrelor group showed significant advantages in reducing the risk of cardiovascular death (HR 0.73, CI 0.56–0.96, p = 0.47) and all-cause mortality (HR 0.77, CI 0.60–0.98, p = 0.76) versus clopidogrel in the subgroup which contained patients aged ≥75 years old, without increasing the overall bleeding risk (HR 1.02, CI 0.82–1.27, p = 0.89) (Wallentin et al., 2009). However, an RCT aiming to explore efficacy and safety outcomes of ticagrelor compared with clopidogrel in elderly Chinese ACS patients drew a different conclusion. Ticagrelor owned an extra advantage in reducing the risk of a composite of cardiovascular death, MI, and stroke (HR 0.473, CI 0.230–0.976, p = 0.043) (Wang and Wang, 2016). Surprisingly, the results of the POPular AGE trial revealed that ticagrelor increased the risk of bleeding with no superior co-primary net clinical benefit outcome (Gimbel et al., 2020), which posed a challenge to the traditional opinion about the ticagrelor advantage theory and stimulated our interests in exploring this issue. Our research studies supported the ticagrelor advantage theory that ticagrelor could reduce the risk of all-cause mortality and cardiovascular death. In other words, ticagrelor may extend survival time for elderly ACS patients compared with clopidogrel.
For the outcomes of MACEs, ticagrelor and clopidogrel showed comparable clinical benefits. The probable sources of heterogeneity for the outcomes of MACEs may come from different age cutoffs (Wallentin et al., 2009). The study by Wallentin et al. (2009) had cutoffs of 65 years (HR) and 75 years (RR), and the remaining study data had cutoffs of 65 (Wang and Wang, 2016), 70 (Gimbel et al., 2020), and 75 (Park et al., 2019) years. According to our results, when focusing on all-cause mortality and cardiovascular death solely, ticagrelor showed a significant advantage compared to clopidogrel in elderly ACS patients. Our results suggested that ticagrelor may have a higher application value in the advanced age-group.
Shreds of evidence suggested that ticagrelor had a higher risk of bleeding (Gimbel et al., 2020; Johnston et al., 2020; Silvain et al., 2020). Our research studies further confirmed this issue. Ages of the patients and drug properties were crucial reasons for higher bleeding risk. Age was a validated predictor of adverse prognosis, and the risk of bleeding increased with age (Eagle et al., 2004). Elderly patients with ACS often have multiple comorbidities, as well as a gradual decline in organismal function with advancing age. Age-related changes in thrombotic status, decreased vascular repair capacity, and clinical factors may lead to a greater difference in the safety of antiplatelet agents in the elderly than in young patients (Lopes and Alexander, 2009). As for the medication itself, ticagrelor works faster and more effectively. Ticagrelor has a binding site different from adenosine diphosphate, making its inhibition reversible. Besides, it can activate CYP2C19 without the liver, so ticagrelor has a stronger antiplatelet effect than clopidogrel (Birkeland et al., 2010; Guan et al., 2018). Stronger antiplatelet effect is commonly associated with a higher risk of bleeding, so an appropriate antiplatelet strategy is important for ACS patients, especially for elderly patients.
A higher risk of bleeding is not an absolute contraindication to the application of ticagrelor. According to our results, ticagrelor is a preferable choice compared with clopidogrel in reducing the occurrence of death in most elderly ACS patients. The occurrence of fatal or irreversible bleeding events is one of the main factors affecting the long-term survival of patients. Our results revealed that ticagrelor or clopidogrel shared a similar risk of fatal bleeding. Additional management measures were necessary for patients with ACS who were under a higher bleeding risk. For this issue, a recent clinical investigation indicated that ticagrelor monotherapy might be a suitable alternative option (Mehran et al., 2019). In addition, shortening DAPT duration (Palmerini et al., 2017) and enhancing the education of high-risk patients and their families are valuable in preventing bleeding events. Fatal or irreversible ischemia was also a clinically significant event for elderly ACS patients, the ATLAS ACS 2-TIMI 51 revealed an interesting phenomenon, and rivaroxaban therapy at an oral dose of 2.5 mg twice daily in patients treated with aspirin and clopidogrel was associated with a net reduction in fatal or irreversible events (Gibson et al., 2018). Therefore, with reasonable precautions, the risk of bleeding with ticagrelor could be minimized as much as possible.
Our meta-analysis has several advantages over previous research studies. First, we were the first to systematically conduct a meta-analysis of clopidogrel versus ticagrelor in elderly patients with ACS. Second, we used both RR and HR to comprehensively demonstrate the findings. Third, for high bleeding risk, we conducted a systematic analysis and gave reasonable monitoring and preventive suggestions. Finally, this meta-analysis gave a new direction for the prospective studies.
There are several limitations to our meta-analysis. First, our meta-analysis only contains four RCTs which may not reflect the real world, and two datasets of the included articles come from the subgroup analysis. We could not get individual patient data, so a detailed age-stratified analysis or the analysis of other bleeding definitions could not be performed. Second, in the study of the POPular AGE trial, 5% of patients in the ticagrelor group received prasugrel, which may result in the final results being subjected to some errors. Third, two studies are open-labeled randomized trials, introducing the potential for latent performance bias. In addition, we found the heterogeneity of Duk-Woo 2020 was significant when the heterogeneity tests were performed by sequential deletion. The probable reason might be that most patients received percutaneous coronary intervention in Duk-Woo 2020.
Our results reveal that aspirin plus ticagrelor reduces cardiovascular death and all-cause mortality but increases the risk of PLATO major bleeding or PLATO minor bleeding when compared with aspirin plus clopidogrel in elderly ACS patients. Herein, aspirin plus ticagrelor may extend lifetime for elderly ACS patients compared with aspirin plus clopidogrel. The low sample size of current studies cannot support a definite conclusion for this vital issue. Further studies focusing on DAPT of elderly ACS patients with larger population are still needed.
The original contributions presented in the study are included in the article/Supplementary Material; further inquiries can be directed to the corresponding authors.
XZ and JZ: writing—original draft. JG: methodology, software, and visualization. JW, YP, XZ, WS, KY, and FYX: data curation. FX and YC: writing—reviewing and editing.
This study was supported by the National Natural Science Foundation of China (81873950, 82072144, 81772036, 81671952, 81873953, and 82002017), the National Key R&D Program of China (2020YFC1512700, 2020YFC1512705, 2020YFC1512703, and 2020YFC0846600), the National S&T Fundamental Resources Investigation Project (2018FY100600 and 2018FY100602), Taishan Pandeng Scholar Program of Shandong Province (tspd20181220), Taishan Young Scholar Program of Shandong Province (tsqn20161065 and tsqn201812129), Key R&D Program of Shandong Province (2019GSF108075 and 2018GSF118003), the Interdisciplinary Young Researcher Groups Program of Shandong University (2020QNQT004), and the Fundamental Research Funds of Shandong University (2018JC011).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2021.743259/full#supplementary-material
Birkeland, K., Parra, D., and Rosenstein, R. (2010). Antiplatelet Therapy in Acute Coronary Syndromes: Focus on Ticagrelor. J. Blood Med. 1, 197–219. doi:10.2147/JBM.S9650
Capodanno, D., and Angiolillo, D. J. (2010). Antithrombotic Therapy in the Elderly. J. Am. Coll. Cardiol. 56 (21), 1683–1692. doi:10.1016/j.jacc.2010.04.063
Capranzano, P., and Angiolillo, D. J. (2020). Ticagrelor or Clopidogrel in Elderly Patients with Myocardial Infarction: When the Choice Makes the Difference. Circulation 142 (18), 1709–1712. doi:10.1161/CIRCULATIONAHA.120.050845
Collet, J. P., Thiele, H., Barbato, E., Barthélémy, O., Bauersachs, J., Bhatt, D. L., et al. (2021). 2020 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation. Eur. Heart J. 42 (14), 1289–1367. doi:10.1093/eurheartj/ehaa575
Eagle, K. A., Lim, M. J., Dabbous, O. H., Pieper, K. S., Goldberg, R. J., Van de Werf, F., et al. (2004). A Validated Prediction Model for All Forms of Acute Coronary Syndrome: Estimating the Risk of 6-month Postdischarge Death in an International Registry. JAMA 291 (22), 2727–2733. doi:10.1001/jama.291.22.2727
Gibson, C. M., Levitan, B., Gibson, W. J., Yee, M. K., Murphy, S. A., Yuan, Z., et al. (2018). Fatal or Irreversible Bleeding and Ischemic Events with Rivaroxaban in Acute Coronary Syndrome. J. Am. Coll. Cardiol. 72 (2), 129–136. doi:10.1016/j.jacc.2018.04.055
Gimbel, M., Qaderdan, K., Willemsen, L., Hermanides, R., Bergmeijer, T., de Vrey, E., et al. (2020). Clopidogrel versus Ticagrelor or Prasugrel in Patients Aged 70 Years or Older with Non-ST-elevation Acute Coronary Syndrome (POPular AGE): the Randomised, Open-Label, Non-inferiority Trial. Lancet 395 (10233), 1374–1381. doi:10.1016/s0140-6736(20)30325-1
Guan, W., Lu, H., and Yang, K. (2018). Choosing between Ticagrelor and Clopidogrel Following Percutaneous Coronary Intervention: A Systematic Review and Meta-Analysis (2007-2017). Medicine (Baltimore) 97 (43), e12978. doi:10.1097/MD.0000000000012978
Husted, S., James, S., Becker, R. C., Horrow, J., Katus, H., Storey, R. F., et al. (2012). Ticagrelor versus Clopidogrel in Elderly Patients with Acute Coronary Syndromes: a Substudy from the Prospective Randomized PLATelet Inhibition and Patient Outcomes (PLATO) Trial. Circ. Cardiovasc. Qual. Outcomes 5 (5), 680–688. doi:10.1161/CIRCOUTCOMES.111.964395
Ibanez, B., James, S., Agewall, S., Antunes, M. J., Bucciarelli-Ducci, C., Bueno, H., et al. (2018). 2017 ESC Guidelines for the Management of Acute Myocardial Infarction in Patients Presenting with ST-Segment Elevation: The Task Force for the Management of Acute Myocardial Infarction in Patients Presenting with ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 39 (2), 119–177. doi:10.1093/eurheartj/ehx393
Johnston, S. C., Amarenco, P., Denison, H., Evans, S. R., Himmelmann, A., James, S., et al. (2020). Ticagrelor and Aspirin or Aspirin Alone in Acute Ischemic Stroke or TIA. N. Engl. J. Med. 383 (3), 207–217. doi:10.1056/NEJMoa1916870
Lopes, R. D., and Alexander, K. P. (2009). Antiplatelet Therapy in Older Adults with Non-ST-segment Elevation Acute Coronary Syndrome: Considering Risks and Benefits. Am. J. Cardiol. 104 (5 Suppl. l), 16C–21C. doi:10.1016/j.amjcard.2009.06.021
Mehran, R., Baber, U., Sharma, S. K., Cohen, D. J., Angiolillo, D. J., Briguori, C., et al. (2019). Ticagrelor with or without Aspirin in High-Risk Patients after PCI. N. Engl. J. Med. 381 (21), 2032–2042. doi:10.1056/NEJMoa1908419
Palmerini, T., Della Riva, D., Benedetto, U., Bacchi Reggiani, L., Feres, F., Abizaid, A., et al. (2017). Three, Six, or Twelve Months of Dual Antiplatelet Therapy after DES Implantation in Patients with or without Acute Coronary Syndromes: an Individual Patient Data Pairwise and Network Meta-Analysis of Six Randomized Trials and 11 473 Patients. Eur. Heart J. 38 (14), 1034–1043. doi:10.1093/eurheartj/ehw627
Park, D. W., Kwon, O., Jang, J. S., Yun, S. C., Park, H., Kang, D. Y., et al. (2019). Clinically Significant Bleeding with Ticagrelor versus Clopidogrel in Korean Patients with Acute Coronary Syndromes Intended for Invasive Management: A Randomized Clinical Trial. Circulation 140 (23), 1865–1877. doi:10.1161/CIRCULATIONAHA.119.041766
Reaño, J. D. P., Shiu, L. A. B., Miralles, K. V., Dimalala, M. G. C., Pestaño, N. S., Punzalan, F. E. R., et al. (2020). A Systematic Review and Meta-Analysis on the Effectiveness of an Invasive Strategy Compared to a Conservative Approach in Patients > 65 Years Old with Non-ST Elevation Acute Coronary Syndrome. PLoS One 15 (2), e0229491. doi:10.1371/journal.pone.0229491
Roffi, M., Patrono, C., Collet, J. P., Mueller, C., Valgimigli, M., Andreotti, F., et al. (2016). 2015 ESC Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur. Heart J. 37 (3), 267–315. doi:10.1093/eurheartj/ehv320
Silvain, J., Lattuca, B., Beygui, F., Rangé, G., Motovska, Z., Dillinger, J. G., et al. (2020). Ticagrelor versus Clopidogrel in Elective Percutaneous Coronary Intervention (ALPHEUS): a Randomised, Open-Label, Phase 3b Trial. Lancet 396 (10264), 1737–1744. doi:10.1016/S0140-6736(20)32236-4
Szummer, K., Montez-Rath, M. E., Alfredsson, J., Erlinge, D., Lindahl, B., Hofmann, R., et al. (2020). Comparison between Ticagrelor and Clopidogrel in Elderly Patients with an Acute Coronary Syndrome: Insights from the SWEDEHEART Registry. Circulation 142 (18), 1700–1708. doi:10.1161/CIRCULATIONAHA.120.050645
Valgimigli, M., Bueno, H., Byrne, R. A., Collet, J. P., Costa, F., Jeppsson, A., et al. (2018). 2017 ESC Focused Update on Dual Antiplatelet Therapy in Coronary Artery Disease Developed in Collaboration with EACTS: The Task Force for Dual Antiplatelet Therapy in Coronary Artery Disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 39 (3), 213–260. doi:10.1093/eurheartj/ehx419
Wallentin, L., Becker, R. C., Budaj, A., Cannon, C. P., Emanuelsson, H., Held, C., et al. (2009). Ticagrelor versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 361 (11), 1045–1057. doi:10.1056/NEJMoa0904327
Keywords: elderly patients, ticagrelor, clopidogrel, acute coronary syndrome, meta-analysis
Citation: Zhao X, Zhang J, Guo J, Wang J, Pan Y, Zhao X, Sang W, Yang K, Xu F, Xu F and Chen Y (2021) Comparison of Safety and Efficacy Between Clopidogrel and Ticagrelor in Elderly Patients With Acute Coronary Syndrome: A Systematic Review and Meta-Analysis. Front. Pharmacol. 12:743259. doi: 10.3389/fphar.2021.743259
Received: 18 July 2021; Accepted: 14 September 2021;
Published: 18 October 2021.
Edited by:
Luciane Cruz Lopes, University of Sorocaba, BrazilReviewed by:
Fathi M. Sherif, University of Tripoli, LibyaCopyright © 2021 Zhao, Zhang, Guo, Wang, Pan, Zhao, Sang, Yang, Xu, Xu and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Feng Xu, eHVmZW5nc2R1QDEyNi5jb20=; Yuguo Chen, Y2hlbjkxOTA4NUBzZHUuZWR1LmNu
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.