 Giulia Gantner
Giulia Gantner Deborah Spiess
Deborah Spiess Eliane Randecker
Eliane Randecker Katharina C. Quack Lötscher
Katharina C. Quack Lötscher Ana Paula Simões-Wüst
Ana Paula Simões-Wüst- Department of Obstetrics, University Hospital Zurich, University of Zurich, Zurich, Switzerland
Little is known about the treatment of mild mental disorders and/or symptoms (MDS) during pregnancy. Our main purpose was to compare the use of herbal medicines during pregnancy in women with and without MDS. A questionnaire consisting of 21 multiple-choice questions was distributed in the participating obstetrics clinics or birth centers in the Canton of Zurich, in Switzerland, from August 2018 to March 2019; 398 questionnaires were considered in the analysis. The use of any type of herbal medicines–including pharmaceutical herbal products as well as teas–during pregnancy was reported by 358 women (out of 398, 89.9%). Of these, 272 participants used pharmaceutical herbal products, whereby ginger (49.2%), raspberry leaf (42.7%), bryophyllum (37.8%), chamomile (27.2%), lavender (22%) and iron-rich herbs (12.3%) were the ones most commonly mentioned. More than half (207/398, 52.0%) of all participants reported suffering from MDS during pregnancy; only a few took (synthetic) psychoactive medications (5/398, 1.3%). The percentage of use of pharmaceutical herbal medicines was higher among women reporting MDS than among the remaining women (90.0 vs 75.9%; p < 0.001). At the same time, the prevalence of MDS was higher among users of pharmaceutical herbal products than among non-users (59.6 vs 34.0%; p = 0.001). Specific questions on candidate herbal medicines for the treatment of mild MDS revealed that bryophyllum (mentioned by 107 women), lavender (56 women) and valerian (20 women) were used to reduce stress, restlessness, sleep disorders and others, in part with perceived good to very good effectiveness and tolerability. The large majority of the pregnant women participating in the survey make use of herbal medicines. The particularly high prevalence of MDS among herbal medicine-users and the very rare use of synthetic psychoactive medications suggest that pregnant women rely on herbal medicines for treatment of mild MDS. The reported good effectiveness and tolerability of a few candidate herbal medicines deserve particular attention.
Introduction
Little is known about the treatment of mild mental disorders and/or symptoms (MDS) during pregnancy. Most medications for MDS may not only cause side-effects in the mother, but also easily cross the placental barrier and reach the foetus. Concerns on tolerability, teratogenicity and impact on neonatal outcomes exist (Sivojelezova et al., 2005; Rahimi et al., 2006; Grigoriadis et al., 2014; Yonkers et al., 2017; Gao et al., 2018). Pregnant women in need of such medications therefore face a dilemma between using and refraining from synthetic medications.
It is therefore understandable that a considerable proportion of women suffering from mild MDS opt for treatment with herbal medicines, which tend to be perceived as safe (Kalder et al., 2011; Pallivalappila et al., 2013). For instance in Germany, approximately one-fifth of the pregnant women who take herbal medications do it for psychological problems (Munstedt et al., 2013). Even though the toxicity of herbal medications taken during pregnancy has not in most cases been thoroughly investigated, a considerable proportion of health care professionals who deal with pregnant women–midwives, obstetricians, anaesthetists, and especially those with their own experiences–recommend herbal medicine (Stewart et al., 2014). In Switzerland, 40.6% of pregnant women reported using herbal medicine during pregnancy, which was higher than the average proportion detected in a multinational study [average 28.0% (Kennedy et al., 2013)].
Our main purpose was to compare the use of herbal medicines in women with and without MDS. Further goals were to characterise the use, perceived effectiveness and tolerability of a few candidate herbal medicines for mild MDS treatment.
Methods
Study Design
The present analysis is based on self-reported data from obstetric patients participating in a cross-sectional survey undertaken between August 2018 and March 2019.
Ethics Statement
The study was conducted in accordance with the Helsinki Declaration and with Swiss laws and regulations. In compliance with Swiss Federal Law on data protection (Human Research Act, Article 2), since the data were anonymously collected, no special authorisation was needed. This was confirmed by jurisdictional declaration of the ethics committee of Zurich (Enquire BASEC-Nr. Req-2017-00966; letter from December 14, 2017).
Selection and Description of Participants
The survey took place in the Canton of Zurich–often considered to be representative of the Swiss population as a whole–whose inhabitants correspond to one-sixth of the entire Swiss population. Eight obstetric clinics and birth centres agreed to participate. In these institutions, pregnant women (at or after 28 weeks of pregnancy) or women in the puerperium were invited to participate in the survey if they had not previously completed the questionnaire, could read German, English, French or Italian, and were not emergency patients.
The aim of our survey was to compare the use of herbal medicines during pregnancy in women with and without MDS. Assuming that twice as many pregnant women take herbal medicines for symptoms related to physical conditions than for symptoms related to mental diseases [40 and 20%, respectively, compare with Munstedt et al. (2013)], a sample size of 106 in each group would allow the detection of a difference between the percentage of women taking herbal medicines in the groups with and without MDS. The survey was pursued until 106 women taking (pharmaceutical) herbal medicines in each of the groups with and without MDS had participated.
Questionnaire
The questionnaire consisted of 21 multiple-choice questions and was available in German, English, French and Italian. Piloting of the questionnaire–distributed to 14 women, at least three per language–was conducted to ensure readability and clarity of the questions.
Four of the 21 (complex) questions were related to the intake of herbal medicines during pregnancy and were inspired by a previous survey (Zuzak et al., 2009). The questionnaire distinguished between herbal infusions/teas and pharmaceutical herbal medicines, but did not specify the type of preparation. For a selection of six herbs, detailed information on perceived effectiveness and tolerability was collected. In the questionnaire, the common names of the herbs were used, with a few exceptions (see Table 1, also for the correspondence between the used names and full taxonomic names).
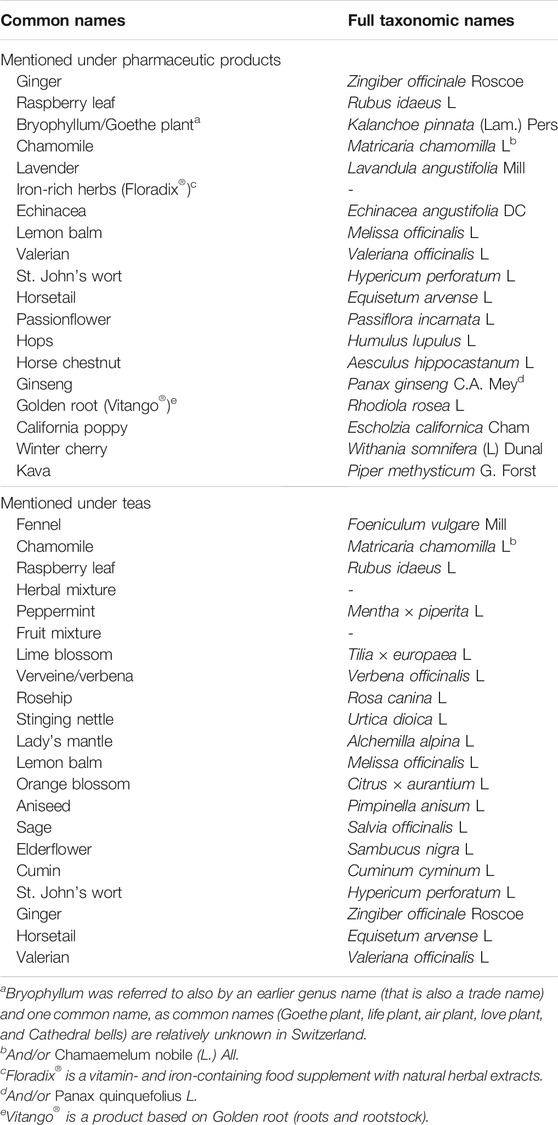
TABLE 1. Herbs mentioned in the questionnaire by common names and corresponding full taxonomical names.
To contextualise our results, data on sociodemographic characteristics, acute/chronic disorders and symptoms and synthetic/conventional medications were collected [in part published elsewhere (Randecker et al., 2020)]. To avoid counting missing answers as “non-use” answers, the questions on medicinal herbal medicines included the option “never used”; in these cases, the number of total answers differs from question to question.
We defined an existing MDS on the basis of specific questions. If the women reported suffering from acute or chronic mental disorder, or related symptoms, or reported taking psychotropic drugs, they were considered to have MDS. No MDS severity assessment was performed; psychotic diseases were not addressed in the questionnaire.
Data Collection
A total of 1,653 envelopes–each one containing an information sheet, the questionnaire and a post-paid envelope addressed to the Department of Obstetrics, University Hospital Zurich–were handed out to potential participants in obstetric clinics and birth centres in the Canton of Zurich. Professionals were instructed by the study team to distribute the envelopes to patients during prenatal check-ups or during hospitalisation in the early puerperium. Sealing of the envelopes after insertion of the completed questionnaires was emphasised to the patients to ensure anonymity. Data were entered manually into a Microsoft Excel file.
Statistical Data Analysis
Descriptive statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS), Version 25.0. for Windows (IBM® SPSS® Statistics). Pearson’s chi-square test was used to compare use of herbal medicines between participants with and without MDS, and MDS prevalence between herbal medicines users and non-users. A two-sided p-value smaller than 0.05 was considered statistically significant; no correction for multiple testing was applied. The number of missing answers is depicted either in the tables or corresponding legends.
Results
Number and Sociodemographic and Health-Related Characteristics of Participants
From a total of 1,653 questionnaires distributed, 398 were completed at or after 28 week’s gestation or shortly after birth and returned either by post or through collection boxes placed in the various institutions (overall response rate: 398/1,653, 24.1%). The 398 participants were treated at the following institutions: University Hospital Zurich (n = 164), City Hospital Triemli (n = 61), Hospital Zollikerberg (n = 50), Hospital Bülach (n = 40), Paracelsus-Hospital Richterswil (n = 31), Hospital Limmattal (n = 21) and Delphys Birthing Center (n = 8); in some cases, other institutions (n = 10), more than one institution (n = 10) or none were named (n = 3).
Most women completed the questionnaires in German (362/398, 91.0%), followed by English (28/398, 7.0%), Italian (5/398, 1.3%) and French (3/398, 0.8%). The survey population was comprised mainly of women between 18 and 43 years, with a medium to high level of education (high school to university). The majority of women were from Switzerland (202/398, 50.8%), followed by Germany (64/398, 16.1%) and other European countries (86/398, 21.6%), America (19/398, 4.8%), Asia (16/398, 4.0%), Africa (2/398, 0.5%) and Australia (1/398, 0.3%), others (6/398, 1.5%). The majority of participants had delivered in the days before receiving the questionnaire (221/371, 59.6%); the remaining women were either in pregnancy weeks 28–37 (79/371, 21.3%) or 38-42 (71/371, 19.1%). Women were slightly more often primiparous (193/372, 51.9%) than multiparous. For detailed data, see Supplementary Table S1.
About a quarter of women reported chronic disorders (101/373, 27.1%), of which allergies (29/373, 7.8%), thyroid disorders (24/373, 6.4%), and headaches/migraines (20/373, 5.4%) were the most common (Supplementary Table S2). The following pregnancy-related acute disorders were the most common: 18.6% of women (69/371) reported suffering from gastroesophageal reflux, 17.0% (63/371) from iron deficiency/anemia, and 14.3% (53/371) from morning sickness. The most commonly reported symptoms during pregnancy were fatigue (294/370, 79.5%), nausea (248/365, 67.9%), heartburn (211/359, 58.8%) and shortness of breath (191/359, 53.2%). For additional information on disorders and symptoms during pregnancy, see Supplementary Tables S2, S3, respectively.
MDS During Pregnancy
Four percent of the women (15/372) reported one of the following chronic mental disorders: minor depression (n = 5); mood disorder (n = 5); anxiety disorder (n = 3); major depression (n = 1) and sleeping disorder (n = 1). Moreover, a prevalence of acute mental disorders during pregnancy of 13.2% (48/371) was observed, which included sleeping disorder (n = 27); mood disorder (n = 13); minor depression (n = 5) and anxiety disorder (n = 3) (Supplementary Table S2). More than half (51.3%) of the participants reported having suffered from a mental symptom during pregnancy (204/398), namely: insomnia (145/338, 42.9%), anxiety (57/320, 17.8%), and depressive mood (33/335, 9.9%). Compared with the pre-pregnancy period, the prevalence of anxiety and insomnia was higher, whereas the prevalence of depressive mood was slightly lower during pregnancy (Supplementary Table S3). Figure 1A provides an overview of the prevalence of mental symptoms during and before pregnancy.
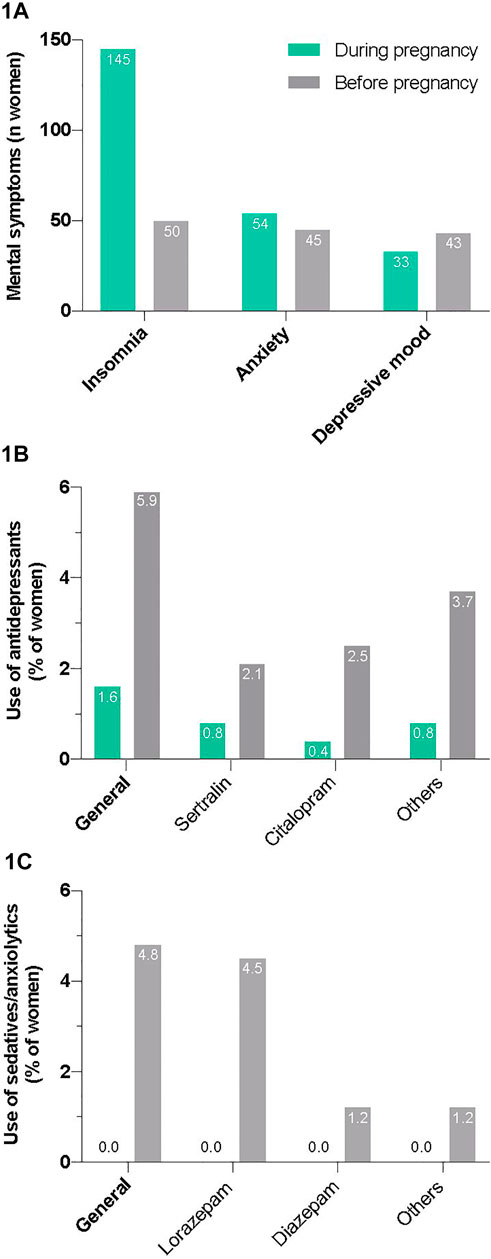
FIGURE 1. Perceived mental symptoms (A) and reported use of antidepressants (B) and sedatives/anxiolytics (C) during pregnancy and in the time before.
Only a few participants used antidepressants (5/315, 1.6%) and none used sedatives/anxiolytics during pregnancy (Figures 1B,C; Supplementary Table S4). The number of participants taking antidepressants and sedatives/anxiolytics before becoming pregnant was markedly higher (19/321 or 5.9%; and 15/315 or 4.8%, respectively). Two women (2/240; 0.8%) answered that they were taking an antidepressant not mentioned in the questionnaire during pregnancy, namely escitalopram (n = 1) and paroxetine (n = 1), both selective serotonin reuptake inhibitors (SSRIs); additional other sedatives/anxiolytics were not mentioned.
Use of Herbal Medicines in General and Versus MDS
The vast majority of women reported using some type of herbal medications, either as teas or as pharmaceutic/clinical medicines, during pregnancy (358/398, 89.9%). Of these, 272 participants (272/325, 83.7%) used pharmaceutical herbal products, most frequently ginger (49.2%), raspberry leaf (42.7%), bryophyllum (37.8%), chamomile (27.2%), lavender (22.0%) and iron-rich herbs (12.3%); see Table 2. The majority of participants (263/358, 86.5%) who reported using herbal medicines during pregnancy, also used herbal medicines before the current pregnancy. The consumption of teas was very widespread in our study population (Table 3).
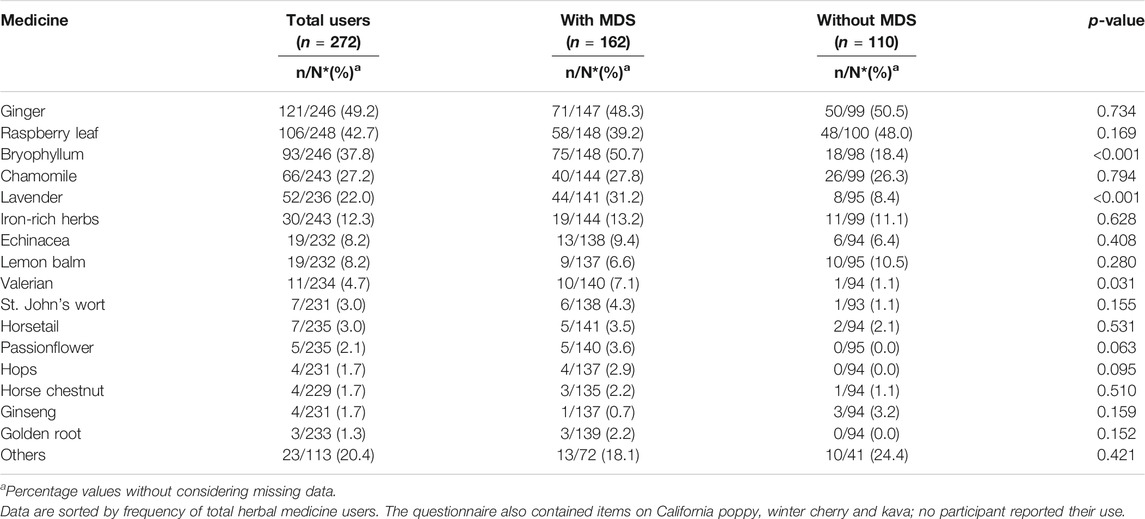
TABLE 2. Use of pharmaceutical herbal medicines during pregnancy by participants with and without mental disorders and/or symptoms (MDS).
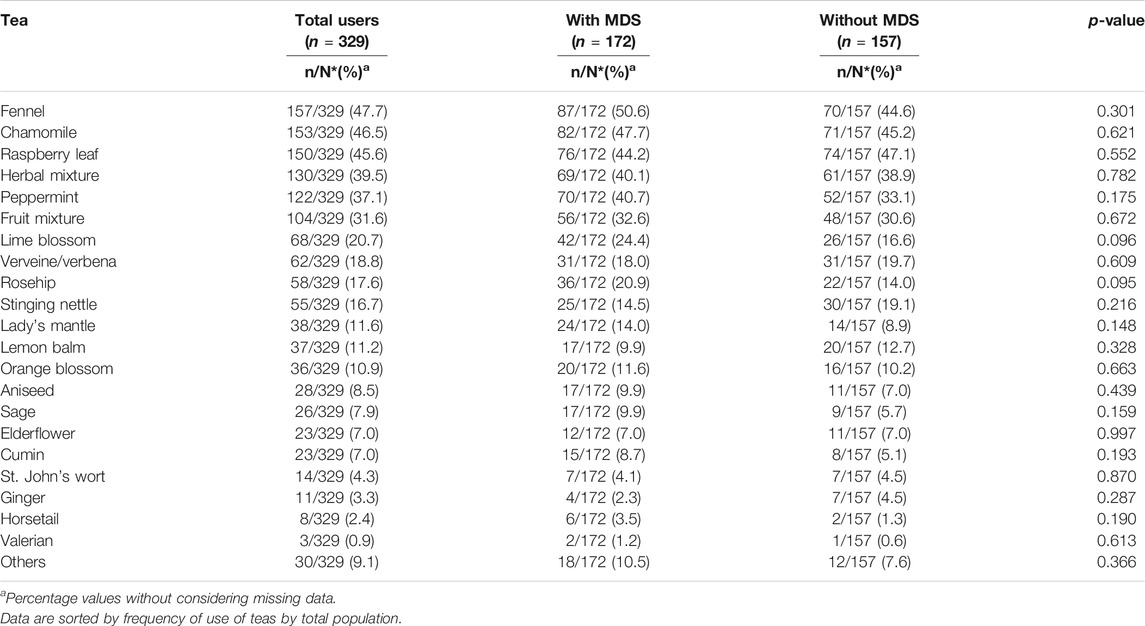
TABLE 3. The most commonly used teas during pregnancy considering mental disorders and/or symptoms (MDS).
The percentage of use of pharmaceutical herbal medicines was higher among women reporting MDS than among the remaining women (teas not considered; 162/180, 90.0% vs 110/145, 75.9%; p < 0.001). Almost 60% of the women who used pharmaceutical herbal medicines suffered from MDS (162/272, 59.6%), which is significantly higher than the corresponding value for non-users (18/53, 34.0%; p = 0.001). More than half of the women who used any type of herbal preparation, teas and pharmaceutical herbal medicines, reported MDS (192/358, 53.6%). Figure 2 shows the most frequently used herbal medicines, pharmaceutical herbal medicines and teas counted together. Several differences between the groups with and without MDS are apparent. Pregnant women with MDS also more often reported using medicines from integrative and complementary medicine than women without (Table 4).
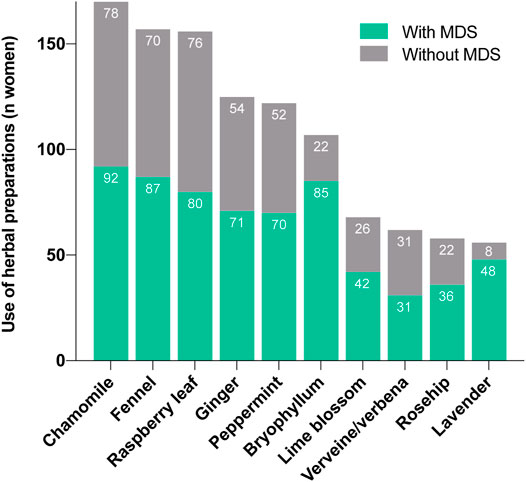
FIGURE 2. Comparison of the most frequently used herbal medicines (pharmaceutical products and teas) in women with and without mental disorders and/or symptoms (MDS).
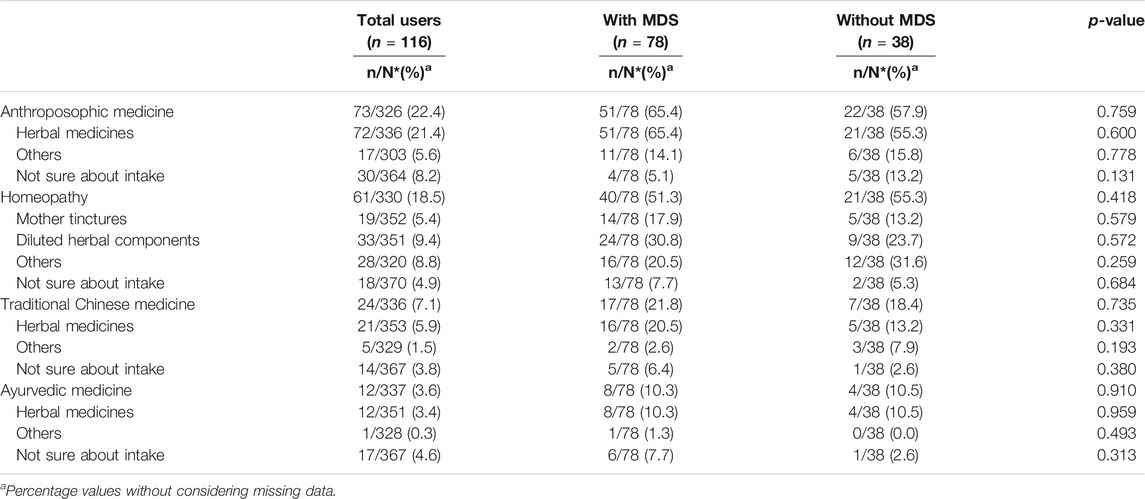
TABLE 4. Use of medicines from integrative and complementary medicine during pregnancy.
Effectiveness and Tolerability of Candidate Herbal Medicines for MDS Treatment
Some questions on the questionnaire specifically targeted the use of well-known plants for the treatment of mild MDS, namely St. John’s wort, hops, valerian, lavender, and bryophyllum.
St. John’s wort was taken by 3.5% of women who answered the corresponding questions (12/341), in half of the cases during pregnancy weeks 28–42. Three women reported good to very good tolerability (Figure 3) and moderate to good effectiveness. St. John’s wort was mostly taken for the treatment of mood disorders (4/12, 33.3%).
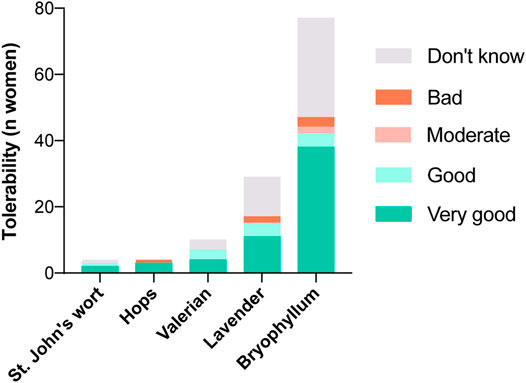
FIGURE 3. Experiences with candidate herbal medicines for the treatment of mental disorders and/or symptoms (MDS) during pregnancy regarding their tolerability.
Hops was used by 2.3% of women (8/343), in all phases of pregnancy. Hops was tolerated well: three of eight women reported very good tolerability and one of eight reported poor tolerability. Seven of eight women evaluated its effectiveness as very good. The two most frequently reported indications were stress and restlessness (both 3/8, 37.5%), followed by sleep disorders (2/8, 25.0%).
Valerian was used most frequently in the last trimester (7/20, 35.0%). Overall, 20 women reported using valerian (20/344, 5.8%), none of the participants reported poor tolerability and the majority tolerated the herb well (“very good” 4/20, 20.0%; “good” 3/20, 15.0%). As shown in Figure 4, half of the participants rated its effectiveness as very good (10/20, 50.0%). Valerian was used most commonly to overcome sleep disorders (9/20, 45.0%), and restlessness (8/20, 40.0%).
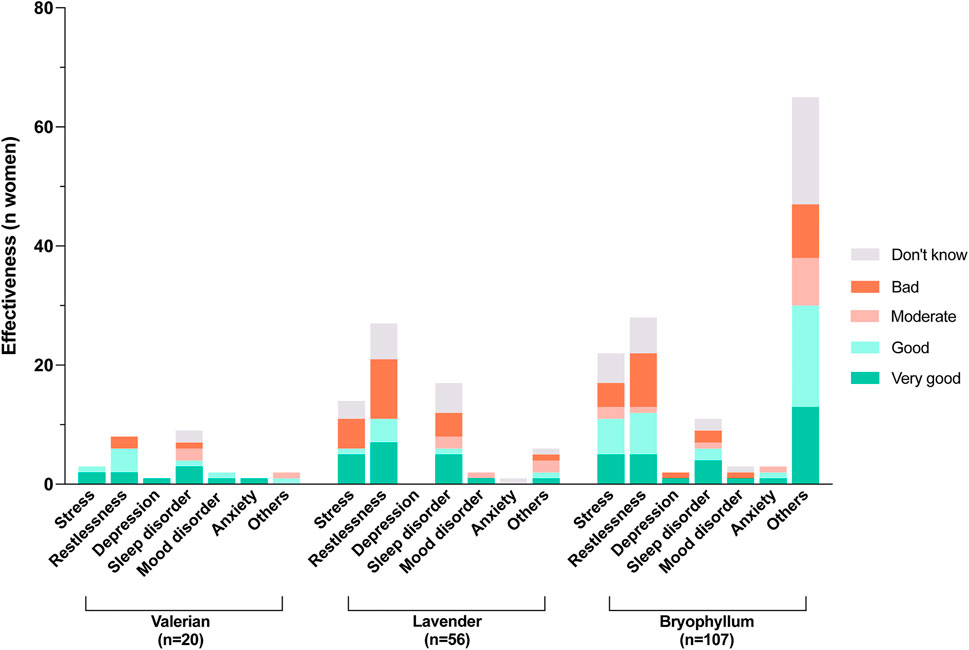
FIGURE 4. Experiences with candidate herbal medicines for the treatment of mental disorders and/or symptoms (MDS) during pregnancy regarding their effectiveness.
The use of lavender was also increased toward the end of pregnancy. Lavender was used by 16.2% of women (56/345) and 11 of 56 women rated its tolerability as very good. Its effectiveness was described as good to very good by almost half of the women who used it (26/56, 46.4%), but bad by 35.7% of women (20/56). Lavender was used mostly to combat restlessness (28/56, 50.0%), sleep disorders (19/56, 33.9%) and stress (15/56, 26.8%).
Bryophyllum was used during pregnancy by almost one-third of the participants (107/360, 29.7%). Of these, more than three-quarters used it during pregnancy weeks 28–42 (84/107, 78.5%). Only a few women (3/107) reported poor tolerability. Regarding the effectiveness of bryophyllum, 58.8% of women rated it good to very good (63/107, all indications together; comparable percentages in the main single indications; see Figure 4). Restlessness was mentioned as a main indication by 27.1% of women (29/107) and 22.4% (24/107) used bryophyllum for stress relief. Another 10.3% (11/107) reported using bryophyllum for sleep disorders. Sixty-six percent of the women who had used bryophyllum (71/107, 66.4%) reported taking the herbal medicine for other reasons than those listed, and the majority wrote that the indications were any type of contractions (44/107, 41.1%). In addition, some women reported using bryophyllum for uterus soothing (n = 3), against abdominal cramps/pain (n = 3), against general pain (n = 1) and against cervix shortening (n = 1).
Discussion
Main Findings
In our study population, the majority of women made use of herbal medicines, including pharmaceutical herbal products and teas. A wide variety of herbal products were mentioned by the survey participants, but ginger, raspberry leaf, bryophyllum, chamomile, lavender and iron-rich herbs were most commonly used. Our data further show that more than half (52.0%) of all participants had MDS during pregnancy, although few made use of (synthetic) psychoactive medications. The prevalence of MDS was higher among users of pharmaceutical herbal medicines than among non-users. Focusing on the most commonly used herbal medicines, users of bryophyllum and lavender reported suffering from MDS particularly often. Specific questions about candidate herbal medicines for the treatment of MDS revealed that bryophyllum (mentioned by 107 women), lavender (56 women) and valerian (20 women) were used to reduce stress, restlessness, sleep disorders and others, frequently with perceived good to very good effectiveness and tolerability.
Strengths and Limitations
All data were self-reported. While the number of pregnant participants (n = 398) can be considered a strength of the present survey, the moderate response rate of 24.1% is a limitation of the study. To avoid selections biases, following measures were taken: 1) all hospitals from the Canton of Zurich with an obstetrics ward were invited to participate; 2) the institutions that agreed to participate were regularly reminded of the survey; 3) the questionnaires were available in four languages (the three main country languages and English); 4) mental conditions were not mentioned in the title or cover letter of the questionnaire; 5) it was clearly stated that the survey was fully anonymous. Nevertheless, some selection bias due to interest in herbal medicines (mentioned in the title and cover letter) or the limited number of available questionnaire languages cannot be excluded. In the case of patients from the University Hospital Zurich (41.2% of survey participants), an internal analysis of the main patient demographic data revealed comparable characteristics to those of the survey participants (own unpublished observations). Finally, most questionnaires were handed over to women after delivery. While this can be considered a strength–as postpartum women are able to describe their use of herbal medicines throughout the whole pregnancy–it is conceivable that some participants may not have remembered the medicines taken at the beginning of pregnancy.
Use of Pharmaceutic Herbal Medicines During Pregnancy
The high use of herbal medicines observed in the present survey is consistent with findings of a previous pilot survey conducted in a comparable population in the late 1990s (Gut et al., 2004). Studies from other countries reported lower use, and a multinational study of the use of herbal medications in pregnancy in 23 countries, and involving 9,459 women, revealed a markedly lower rate [28.9% of the women (Kennedy et al., 2013)]. This could be related to different perceptions of “herbal medicines” among participants in the different studies. In general, women in our study seemed to be more likely to use herbal medicines if they were primiparous and had used herbal medicines in the past/before pregnancy (data not shown). This could also be seen in an Australian study (Low Dog, 2009), where the most commonly used herbals were ginger, cranberry, valerian, raspberry, chamomile and peppermint (Kennedy et al., 2013), which is similar to our results.
In the following, we will focus on the herbal medicines used by at least 20% of the participants, first with respect to frequency of use during pregnancy and effectiveness, then summarising what is known on their safety. Our finding that ginger was the most commonly used herbal medicine confirms the results of previous surveys, and corresponds well with the high prevalence of nausea during pregnancy found in our survey (67.9%). Ginger can be considered a possibly effective treatment for nausea and vomiting during pregnancy (Viljoen et al., 2014). Raspberry leaf was the second most commonly used herbal medicine among pregnant women in our study, in accordance with studies showing that it is often recommended by midwives (Allaire et al., 2000; Holst et al., 2009). It is used to strengthen or prepare the uterus, to soften the cervix, and to induce and shorten labor (Briggs et al., 2022). In a placebo-controlled randomized trial, raspberry leaf tablets did not shorten the first stage of labor, but resulted in a small shortening of the second stage and less forceps deliveries (Simpson et al., 2001). Bryophyllum was the third most commonly used herbal medicine. Because this plant is recommended in several perinatal centres in Switzerland for the treatment of anxiety states, restlessness, and sleep disturbances (Schenkel et al., 2018), the questionnaire contained additional questions about its use (see below). Nevertheless, most women used bryophyllum for the treatment of other disorders, often related to the attenuation of uterine contractions. In anthroposophic medicine, bryophyllum was introduced in the 1970s as a well-tolerated agent for the treatment of preterm labor (Fürer et al., 2016; Hamburger et al., 2017); in Switzerland it is recommended for this indication (Schenkel et al., 2018) and commonly used in the main perinatal institutions (Fürer et al., 2015). Chamomile, the fourth most commonly used medicine has been also widely used and is known as a treatment for nausea and vomiting during pregnancy (Sanaati et al., 2016). Finally, lavender was frequently used (see below for information on its anxiolytic effects).
The Committee on Herbal Medicinal Products (CHMP) of the European Medicine Agency (EMA) does not recommend the use of ginger (European Medicines Agency, 2012b), raspberry leaf (European Medicines Agency, 2014), chamomile (European Medicines Agency, 2015) and lavender (European Medicines Agency, 2012a) during pregnancy because of insufficient safety data; so far, no community herbal monograph was published on bryophyllum. According to a reference work on drugs in pregnancy (Briggs et al., 2022), ginger and raspberry leaf are classified as compatible with pregnancy, whereas about chamomile it is considered that human data are limited and no relevant human data are available. According to a systematic review and meta-analysis from 2014, ginger can be considered a harmless treatment for nausea and vomiting during pregnancy: here no significant differences were found between the ginger and placebo treated groups for all reported adverse effects in various studies (Viljoen et al., 2014). A systematic review come to comparable conclusions (Stanisiere et al., 2018). With respect to raspberry leaf use, an unclear association with caesarean sections (Nordeng et al., 2011) and an interaction with a conventional medicine (hypoglycaemia when used with insulin) have been reported (Cheang et al., 2016). A randomized trial, however, revealed no adverse effects for mother or child (Simpson et al., 2001). Several retrospective and prospective studies on the use of bryophyllum during pregnancy are indicative of a good safety profile (Lambrigger-Steiner et al., 2014; Fürer et al., 2015; Fürer et al., 2016; Hamburger et al., 2017; Simões-Wüst et al., 2018). A qualitative study pointed towards an association between regular use of chamomile during pregnancy and a higher incidence of threatening miscarriages and preterm labor [without correction for possible confounders; Cuzzolin et al. (2010)].
Herbal Medicines and MDS Treatment
Of the herbal medicines specifically addressed in the present questionnaire, there were several that–irrespective of pregnancy–are used in the treatment of mild MDS. Evidence for their use during pregnancy is still scarce, therefore the existing studies are briefly discussed below (on the herbal medicines used by at least 20 participants).
Valerian was mostly used to treat restlessness and sleep disorders. As a sleep-aid, its benefits and side effect profile have been shown in several studies (Dorn, 2000; Andreatini et al., 2002; Hattesohl et al., 2008). In a small survey conducted in southern Italy, no influence of valerian use on pregnancy and neonatal outcomes was found (n = 9) (Low Dog, 2009). Data from the Swedish Birth Register from 1995 to 2004 also suggest good safety, as no abnormalities were found in the infants of mothers who had taken phytotherapeutics–often valerian–during pregnancy (n = 787, 0.9% of all mothers in the register).
In our study, women reported using lavender more often during the last trimester of pregnancy, mainly against restlessness, sleep disorders and stress. Several clinical trials revealed good efficacy and tolerability of a medicine prepared from lavender flowers in the treatment of anxiety (Kasper et al., 2010; Woelk and Schlafke, 2010; Kasper et al., 2014). Furthermore, lavender tea has been shown to enhance the effects of the antidepressant citalopram (Nikfarjam et al., 2013). We are aware of only one previous study during pregnancy: in a randomised placebo-controlled trial, lavender cream was shown to reduce anxiety, stress and depression (Effati-Daryani et al., 2015).
Although most participants used bryophyllum to treat indications other than MDS, this plant was also used to treat restlessness, stress, sleep disorders, mood disorders, anxiety, and depression. In anthroposophic medicine, the use of bryophyllum medicines for mental disorders is well documented (Simões-Wüst et al., 2012). Prospective observational studies revealed improvements in sleep quality after treatment with bryophyllum in pregnant women (Lambrigger-Steiner et al., 2014) [and in cancer patients (Simões-Wüst et al., 2015)].
The particularly high prevalence of MDS among herbal medicine-users and the rare use of synthetic psychoactive medications suggest that pregnant women avoid them and prefer recurring to herbal medicines for mild MDS treatment. The reported positive experiences with some candidate herbal medicines for mild MDS treatment and their well-perceived tolerability deserve particular attention.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
GG and APS-W designed the study. GG developed the questionnaire, contacted the obstetric clinics and birth centres in the Canton of Zurich, performed the analyses of data on herbal medicines and wrote the first version of the manuscript. ER analysed the data on conventional medications and contributed to survey realization. DS and APS-W verified the analyses. All authors were involved in the interpretation of data, provided critical revision of the manuscript, then read and approved the submitted version. GG contribution constitutes her MD thesis, ER contribution constituted her Master’s thesis in pharmacy; APS-W supervised both theses.
Funding
DS contributed to this project while being financially supported by the Swiss National Science Foundation (SNF; Sinergia) grant CRSII5_177260. No additional funding sources.
Conflict of Interest
APS-W received research funding from Weleda AG, a company that produces Bryophyllum pinnatum-based medicines during the last 5 years.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We are indebted to all women who made the effort to fill in the questionnaire, therefore making this survey possible. We thank all professionals at the participating obstetrics clinics and birth centers who authorized and/or facilitated the distribution of the questionnaires. Alexandra Dolder is gratefully acknowledged for her support, Kristian Klaic for internal analyses. We thank all other scientists involved in the SNF project CRSII5_177260, the steering committee of the Swiss Academy for Perinatal Pharmacology and Thomas Dillner (Psychiatrist, Richterswil) for interesting discussions. Heather Murray is thanked for language corrections.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2021.729724/full#supplementary-material
References
Allaire, A. D., Moos, M. K., and Wells, S. R. (2000). Complementary and Alternative Medicine in Pregnancy: a Survey of North Carolina Certified Nurse-Midwives. Obstet. Gynecol. 95 (1), 19–23. doi:10.1016/s0029-7844(99)00481-0
Andreatini, R., Sartori, V. A., Seabra, M. L., and Leite, J. R. (2002). Effect of Valepotriates (Valerian Extract) in Generalized Anxiety Disorder: a Randomized Placebo-Controlled Pilot Study. Phytother Res. 16 (7), 650–654. doi:10.1002/ptr.1027
Briggs, G. G., Towers, C. V., and Forinash, A. B. (2022). Drugs in Pregnancy and Lactation. Philadelphia: Wolters Kluwer.
Cheang, K. I., Nguyen, T. T., Karjane, N. W., and Salley, K. E. (2016). Raspberry Leaf and Hypoglycemia in Gestational Diabetes Mellitus. Obstet. Gynecol. 128 (6), 1421–1424. doi:10.1097/AOG.0000000000001757
Cuzzolin, L., Francini-Pesenti, F., Verlato, G., Joppi, M., Baldelli, P., and Benoni, G. (2010). Use of Herbal Products Among 392 Italian Pregnant Women: Focus on Pregnancy Outcome. Pharmacoepidemiol. Drug Saf. 19 (11), 1151–1158. doi:10.1002/pds.2040
Dorn, M. (2000). Efficacy and Tolerability of Baldrian versus Oxazepam in Non-organic and Non-psychiatric Insomniacs: a Randomised, Double-Blind, Clinical, Comparative Study. Forsch Komplementarmed Klass Naturheilkd 7 (2), 79–84. doi:10.1159/000021314
Effati-Daryani, F., Mohammad-Alizadeh-Charandabi, S., Mirghafourvand, M., Taghizadeh, M., and Mohammadi, A. (2015). Effect of Lavender Cream with or without Foot-bath on Anxiety, Stress and Depression in Pregnancy: a Randomized Placebo-Controlled Trial. J. Caring Sci. 4 (1), 63–73. doi:10.5681/jcs.2015.007
European Medicines Agency (2012a). EMA/HMPC/143181/2010 Community Herbal Monograph on Lavandula Angustifolia Miller, Aetheroleum. [Online]. Available at: https://www.ema.europa.eu/en/documents/herbal-monograph/final-community-herbal-monograph-lavandula-angustifolia-miller-aetheroleum_en.pdf (Accessed 09 10, 2021).
European Medicines Agency (2014). EMA/HMPC/44211/2012 Community Herbal Monograph on Rubus Idaeus L., Folium. [Online]. Available at: https://www.ema.europa.eu/en/documents/herbal-monograph/final-community-herbal-monograph-rubus-idaeus-l-folium_en.pdf (Accessed 09 10, 2021).
European Medicines Agency (2015). EMA/HMPC/55843/2011 Community Herbal Monograph on Rubus Idaeus L., Folium. [Online]. Available at: https://www.ema.europa.eu/en/documents/herbal-monograph/final-community-herbal-monograph-rubus-idaeus-l-folium_en.pdf (Accessed 09 10, 2021).
European Medicines Agency (2012b). EMA/HMPC/749154/2010 Community Herbal Monograph on Zingiber Officinale Roscoe, Rhizoma, [Online]. Available at: https://www.ema.europa.eu/en/documents/herbal-monograph/final-community-herbal-monograph-zingiber-officinale-roscoe-rhizoma_en.pdf (Accessed 10 09, 2021).
Fürer, K., Simões-Wüst, A. P., von Mandach, U., Hamburger, M., and Potterat, O. (2016). Bryophyllum Pinnatum and Related Species Used in Anthroposophic Medicine: Constituents, Pharmacological Activities, and Clinical Efficacy. Planta Med. 82 (11-12), 930–941. doi:10.1055/s-0042-106727
Fürer, K., Simões-Wüst, A. P., Winkler, A., Amsler, N., Schnelle, M., and von Mandach, U. (2015). The Application of Bryophyllum Pinnatum Preparations in Obstetrics and Gynaecology – a Multicenter, Prospective Observational Study. Forsch Komplementmed 22 (4), 231–236. doi:10.1159/000437154
Gao, S. Y., Wu, Q. J., Sun, C., Zhang, T. N., Shen, Z. Q., Liu, C. X., et al. (2018). Selective Serotonin Reuptake Inhibitor Use during Early Pregnancy and Congenital Malformations: a Systematic Review and Meta-Analysis of Cohort Studies of More Than 9 Million Births. BMC Med. 16 (1), 205. doi:10.1186/s12916-018-1193-5
Grigoriadis, S., Vonderporten, E. H., Mamisashvili, L., Tomlinson, G., Dennis, C. L., Koren, G., et al. (2014). Prenatal Exposure to Antidepressants and Persistent Pulmonary Hypertension of the Newborn: Systematic Review and Meta-Analysis. BMJ 348, f6932. doi:10.1136/bmj.f6932
Gut, E., Melzer, J., von Mandach, U., and Saller, R. (2004). Natural Remedies during Pregnancy and Lactation. Gynakol Geburtshilfliche Rundsch 44 (4), 233–237. doi:10.1159/000079714
Hamburger, H., Potterat, O., Fürer, K., Simões-Wüst, A. P., and von Mandach, U. (2017). Bryophyllum Pinnatum – Reverse Engineering of an Anthroposophic Herbal Medicine. Nat. Product. Commun. 12, 1359–1364. doi:10.1177/1934578x1701200847
Hattesohl, M., Feistel, B., Sievers, H., Lehnfeld, R., Hegger, M., and Winterhoff, H. (2008). Extracts of Valeriana Officinalis L. s.L. Show Anxiolytic and Antidepressant Effects but Neither Sedative Nor Myorelaxant Properties. Phytomedicine 15 (1-2), 2–15. doi:10.1016/j.phymed.2007.11.027
Holst, L., Haavik, S., and Nordeng, H. (2009). Raspberry Leaf-Sshould it Be Recommended to Pregnant Women. Complement. Ther. Clin. Pract. 15 (4), 204–208. doi:10.1016/j.ctcp.2009.05.003
Kalder, M., Knoblauch, K., Hrgovic, I., and Münstedt, K. (2011). Use of Complementary and Alternative Medicine during Pregnancy and Delivery. Arch. Gynecol. Obstet. 283 (3), 475–482. doi:10.1007/s00404-010-1388-2
Kasper, S., Gastpar, M., Müller, W. E., Volz, H. P., Möller, H. J., Dienel, A., et al. (2010). Silexan, an Orally Administered Lavandula Oil Preparation, Is Effective in the Treatment of 'subsyndromal' Anxiety Disorder: a Randomized, Double-Blind, Placebo Controlled Trial. Int. Clin. Psychopharmacol. 25 (5), 277–287. doi:10.1097/YIC.0b013e32833b3242
Kasper, S., Gastpar, M., Müller, W. E., Volz, H. P., Möller, H. J., Schläfke, S., et al. (2014). Lavender Oil Preparation Silexan Is Effective in Generalized Anxiety Disorder-Aa Randomized, Double-Blind Comparison to Placebo and Paroxetine. Int. J. Neuropsychopharmacol. 17 (6), 859–869. doi:10.1017/S1461145714000017
Kennedy, D. A., Lupattelli, A., Koren, G., and Nordeng, H. (2013). Herbal Medicine Use in Pregnancy: Results of a Multinational Study. BMC Complement. Altern. Med. 13, 355. doi:10.1186/1472-6882-13-355
Lambrigger-Steiner, C., Simões-Wüst, A. P., Kuck, A., Fürer, K., Hamburger, M., and von Mandach, U. (2014). Sleep Quality in Pregnancy during Treatment with Bryophyllum Pinnatum: an Observational Study. Phytomedicine 21 (5), 753–757. doi:10.1016/j.phymed.2013.11.003
Low Dog, T. (2009). The Use of Botanicals during Pregnancy and Lactation. Altern. Ther. Health Med. 15 (1), 54–58. doi:10.1089/act.2009.15209
Münstedt, K., Dütemeyer, V., and Hübner, J. (2013). Patient's Considerations behind the Use of Methods from Complementary and Alternative Medicine in the Field of Obstetrics in Germany. Arch. Gynecol. Obstet. 288 (3), 527–530. doi:10.1007/s00404-013-2814-z
Nikfarjam, M., Parvin, N., Assarzadegan, N., and Asghari, S. (2013). The Effects of Lavandula Angustifolia Mill Infusion on Depression in Patients Using Citalopram: A Comparison Study. Iran Red Crescent Med. J. 15 (8), 734–739. doi:10.5812/ircmj.4173
Nordeng, H., Bayne, K., Havnen, G. C., and Paulsen, B. S. (2011). Use of Herbal Drugs during Pregnancy Among 600 Norwegian Women in Relation to Concurrent Use of Conventional Drugs and Pregnancy Outcome. Complement. Ther. Clin. Pract. 17 (3), 147–151. doi:10.1016/j.ctcp.2010.09.002
Pallivalappila, A. R., Stewart, D., Shetty, A., Pande, B., and McLay, J. S. (2013). Complementary and Alternative Medicines Use during Pregnancy: A Systematic Review of Pregnant Women and Healthcare Professional Views and Experiences. Evid. Based Complement. Alternat Med. 2013, 205639. doi:10.1155/2013/205639
Rahimi, R., Nikfar, S., and Abdollahi, M. (2006). Pregnancy Outcomes Following Exposure to Serotonin Reuptake Inhibitors: a Meta-Analysis of Clinical Trials. Reprod. Toxicol. 22 (4), 571–575. doi:10.1016/j.reprotox.2006.03.019
Randecker, E., Gantner, G., Spiess, D., Quack Lötscher, K., and Simões-Wüst, A. P. (2020). What Pregnant Women Are Taking: Learning from a Survey in the Canton of Zurich. [Online]. Available at: https://smw.ch/op-eds/post/what-pregnant-women-are-taking-learning-from-a-survey-in-the-canton-of-zurich (Accessed 04 15, 2021).
Sanaati, F., Najafi, S., Kashaninia, Z., and Sadeghi, M. (2016). Effect of Ginger and Chamomile on Nausea and Vomiting Caused by Chemotherapy in Iranian Women with Breast Cancer. Asian Pac. J. Cancer Prev. 17 (8), 4125–4129.
Schenkel, L., Simões-Wüst, A., Hösli, I., and von Mandach, U. (2018). Drugs in Pregnancy and Lactation - Medications Used in Swiss Obstetrics. Z. Geburtshilfe Neonatol 222, 152–165. doi:10.1055/s-0043-124975
Simões-Wüst, A. P., Hassani, T. A., Müller-Hübenthal, B., Pittl, S., Kuck, A., Meden, H., et al. (2015). Sleep Quality Improves during Treatment with Bryophyllum Pinnatum: An Observational Study on Cancer Patients. Integr. Cancer Ther. 14 (5), 452–459. doi:10.1177/1534735415580680
Simões-Wüst, A. P., Jeschke, E., Mennet, M., Schnelle, M., Matthes, H., and von Mandach, U. (2012). Prescribing Pattern of Bryophyllum Preparations Among a Network of Anthroposophic Physicians. Forsch Komplementmed 19 (6), 293–301. doi:10.1159/000345841
Simões-Wüst, A. P., Lapaire, O., Hösli, I., Wächter, R., Fürer, K., Schnelle, M., et al. (2018). Two Randomised Clinical Trials on the Use of Bryophyllum Pinnatum in Preterm Labour: Results after Early Discontinuation. Complement. Med. Res. 25 (4), 269–273. doi:10.1159/000487431
Simpson, M., Parsons, M., Greenwood, J., and Wade, K. (2001). Raspberry Leaf in Pregnancy: its Safety and Efficacy in Labor. J. Midwifery Womens Health 46 (2), 51–59. doi:10.1016/s1526-9523(01)00095-2
Sivojelezova, A., Shuhaiber, S., Sarkissian, L., Einarson, A., and Koren, G. (2005). Citalopram Use in Pregnancy: Prospective Comparative Evaluation of Pregnancy and Fetal Outcome. Am. J. Obstet. Gynecol. 193 (6), 2004–2009. doi:10.1016/j.ajog.2005.05.012
Stanisiere, J., Mousset, P. Y., and Lafay, S. (2018). How Safe Is Ginger Rhizome for Decreasing Nausea and Vomiting in Women during Early Pregnancy. Foods 7 (4), 50. doi:10.3390/foods7040050
Stewart, D., Pallivalappila, A. R., Shetty, A., Pande, B., and McLay, J. S. (2014). Healthcare Professional Views and Experiences of Complementary and Alternative Therapies in Obstetric Practice in North East Scotland: a Prospective Questionnaire Survey. BJOG 121 (8), 1015–1019. doi:10.1111/1471-0528.12618
Viljoen, E., Visser, J., Koen, N., and Musekiwa, A. (2014). A Systematic Review and Meta-Analysis of the Effect and Safety of Ginger in the Treatment of Pregnancy-Associated Nausea and Vomiting. Nutr. J. 13, 20. doi:10.1186/1475-2891-13-20
Woelk, H., and Schläfke, S. (2010). A multi-center, Double-Blind, Randomised Study of the Lavender Oil Preparation Silexan in Comparison to Lorazepam for Generalized Anxiety Disorder. Phytomedicine 17 (2), 94–99. doi:10.1016/j.phymed.2009.10.006
Yonkers, K. A., Gilstad-Hayden, K., Forray, A., and Lipkind, H. S. (2017). Association of Panic Disorder, Generalized Anxiety Disorder, and Benzodiazepine Treatment during Pregnancy with Risk of Adverse Birth Outcomes. JAMA Psychiatry 74 (11), 1145–1152. doi:10.1001/jamapsychiatry.2017.2733
Keywords: pregnancy, herbal medicines, phytopharmacy, mental health disorders, survey, bryophyllum, lavender, valerian
Citation: Gantner G, Spiess D, Randecker E, Quack Lötscher KC and Simões-Wüst AP (2021) Use of Herbal Medicines for the Treatment of Mild Mental Disorders and/or Symptoms During Pregnancy: A Cross-Sectional Survey. Front. Pharmacol. 12:729724. doi: 10.3389/fphar.2021.729724
Received: 23 June 2021; Accepted: 17 September 2021;
Published: 08 October 2021.
Edited by:
Shan-Yu Su, China Medical University, TaiwanReviewed by:
Kerry Hughes, Ethnopharm LLC, Granite Bay, CA, United StatesMagalie El Hajj, University of Bergen, Norway
Ahmed Mohamed Ahmed Abdelmawla, Assiut University, Egypt
Copyright © 2021 Gantner, Spiess, Randecker, Quack Lötscher and Simões-Wüst. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Paula Simões-Wüst, YW5hcGF1bGEuc2ltb2VzLXd1ZXN0QHVzei5jaA==