 Simona Granata
Simona Granata Pierluigi Carratù
Pierluigi Carratù Giovanni Stallone
Giovanni Stallone Gianluigi Zaza
Gianluigi Zaza
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Pharmacol. , 23 August 2021
Sec. Renal Pharmacology
Volume 12 - 2021 | https://doi.org/10.3389/fphar.2021.710543
Kidney transplant recipients are at high risk of developing severe COVID-19 due to the coexistence of several transplant-related comorbidities (e.g., cardiovascular disease, diabetes) and chronic immunosuppression. As a consequence, a large part of SARS-CoV-2 infected patients have been managed with a reduction of immunosuppression. The mTOR-I, together with antimetabolites, have been often discontinued in order to minimize the risk of pulmonary toxicity and to antagonize pharmacological interaction with antiviral/anti-inflammatory drugs. However, at our opinion, this therapeutic strategy, although justified in kidney transplant recipients with severe COVID-19, should be carefully evaluated in asymptomatic/paucisymptomatic patients in order to avoid the onset of acute allograft rejections, to potentially exploit the mTOR-I antiviral properties, to reduce proliferation of conventional T lymphocytes (which could mitigate the cytokine storm) and to preserve Treg growth/activity which could reduce the risk of progression to severe disease. In this review, we discuss the current literature regarding the therapeutic potential of mTOR-Is in kidney transplant recipients with COVID-19 with a focus on pulmonary fibrosis.
Over the last few months, a large number of kidney transplant recipients worldwide have been diagnosed with COVID-19 (Elias et al., 2020; Kataria et al., 2020), and most of them have required intensive care unit (ICU) admission. The reported mortality rate for this patients’ population ranged between 20 and 30% (Akalin et al., 2020; Alberici et al., 2020; Banerjee et al., 2020; Cravedi et al., 2020; Elias et al., 2020; Fernández-Ruiz et al., 2020; Pereira et al., 2020
Main reasons for the dramatic negative clinical impact of COVID-19 pandemic on this fragile cohort of patients is the coexistence of suppression of the immune system by anti-rejection drugs (Banerjee et al., 2020; Cravedi et al., 2020; Pereira et al., 2020) and the occurrence of several comorbidities (Cravedi et al., 2020). Although cardiovascular diseases and diabetes (Li et al., 2020; Muniyappa and Gubbi, 2020) have been identified as major risk factors for worse outcomes from COVID-19 in kidney transplant patients (similar to non-transplant patients), also pulmonary disorders (e.g., chronic obstructive pulmonary disease, interstitial pulmonary fibrosis and chronic sequels of pulmonary bacterial and/or viral infections) have been associated with a significant increased risk of severe disease and death (Drake et al., 2020; Esposito et al., 2020; Higham et al., 2020).
Recent reports have suggested that pulmonary fibrosis associated with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection may be triggered by both viral- and immune-mediated mechanisms (Liu et al., 2020a) and exacerbated by the acute respiratory distress syndrome (ARDS), occurring in approximately 40% of patients with COVID-19 (Wu et al., 2020). ARDS is characterized by a diffuse alveolar damage with an acute inflammatory exudative process and the release of huge amounts of inflammatory cytokines (Huang et al., 2020) followed by oxidative stress (Chernyak et al., 2020), an organizing phase and an excessive deposition of collagen and extracellular matrix components (Vasarmidi et al., 2020). Additionally, in this condition, SARS-CoV-2 infection in alveolar epithelial cells may provoke an infiltration of immune cells into the lung and an innate immunity activation (Alon et al., 2021).
Adaptive immunity is also activated in COVID-19 patients mainly by antigen presenting dendritic cells, which produce large amounts of cytokines, including interleukin (IL)-6, IL-1β and tumor necrosis factor-alpha (TNF-α) and migrate to the regional lymph nodes to present viral antigen to naïve T cells, pushing their differentiation and migration into affected tissue (Gubernatorova et al., 2020). Among these, cytokines such as transforming growth factor-beta1 (TGF-β1) (Fernandez and Eickelberg, 2012), vascular endothelial growth factor (VEGF) (Barratt et al., 2018), IL-6 (Buonaguro et al., 2020), and TNF-α (Vasarmidi et al., 2020) play a vital role in pulmonary fibrosis.
More than 40% of recovered COVID-19 patients developed pulmonary fibrosis (Li et al., 2021; Zou et al., 2021) and pulmonary impairment also persists after recovery (Mo et al., 2020; Ahmad Alhiyari et al., 2021). The disease duration may impact this condition (approximately 61% of patients with a disease duration greater than 3 weeks developed an important lung fibrosis after ARDS) (Thille et al., 2013; George et al., 2020). This complication occurred more frequently in older, co-morbid patients (mainly with systemic hypertension, diabetes, cardiovascular disease, obesity) who recovered after ICU stay and receiving mechanical ventilation. Additionally, smoking, chronic alcoholism (Ojo et al., 2020) and laboratory findings (lymphopenia, leukocytosis, and elevated lactate dehydrogenase) could predispose individuals to severe lung injury leading to an increased risk of mortality or pulmonary fibrosis in survivors (Liu et al., 2020b).
In kidney transplant recipients, then, immunosuppressive agents may have an impact in pulmonary fibrosis (Gross et al., 1997). In particular, kidney transplant recipients treated with mammalian target of rapamycin inhibitors (mTOR-Is), particularly at high dosages, may develop pulmonary fibrosis (Pham et al., 2004; Weiner et al., 2007; Errasti et al., 2010; Xu et al., 2015; Tomei et al., 2016; Granata et al., 2018).
Numerous clinical data have reported an incidence of pulmonary complications in mTOR-I-treated kidney transplant recipients of 2–11%, with the onset of symptoms until 5 years after the initiation of sirolimus or everolimus therapy (Pham et al., 2004; Champion et al., 2006; Weiner et al., 2007; Alexandru et al., 2008; Rodríguez-Moreno et al., 2009; Errasti et al., 2010; Bertolini et al., 2011). There are several lung manifestations including lymphocytic interstitial pneumonitis, lymphocytic alveolitis, bronchiolitis obliterans with organizing pneumonia, focal pulmonary fibrosis, diffuse alveolar hemorrhage or a combination thereof (Morelon et al., 2001; Vlahakis et al., 2004; Vandewiele et al., 2010). This clinical variability and the absence of specific signs and symptoms do not facilitate diagnosis (Molas-Ferrer et al., 2013). Radiographic tests, computed tomography (CT) and bronchoalveolar lavage (BAL), even if often unspecific, are useful diagnostic tools. In some cases, it is also required a lung biopsy that may reveal different histological patterns including the intra-alveolar non-necrotizing epithelioid granuloma, lymphocytic interstitial inflammation and a focal pattern of organizing pneumonia (Kirby et al., 2012).
This pulmonary toxicity seems to be dose-dependent since clinical and radiologic improvement has been observed in a large number of kidney transplant recipients after mTOR-Is dose reduction (Pham et al., 2004; Errasti et al., 2010).
The pathogenic mechanism of mTOR-Is induced pulmonary toxicity is unknown but epithelial to mesenchymal transition (EMT) may have an important role (Zhang et al., 2016). During EMT, epithelial cells lose apical-basal polarity and cell-cell junctions and gain some mesenchymal traits of migration, invasion, and ability to produce extracellular matrix (ECM) (Kalluri and Weinberg, 2009). High dosages of mTOR-I may activate this complex biological process. A massive mTORC1 inhibition, may lead to a down-regulation of S6K and a subsequent hyper-activation of mTORC2 that, sustaining the phosphorylation of AKT at S473, could induce a feedback loop that stimulates PI3K-AKT signaling activating the cellular/molecular machinery leading to fibrosis (Wan et al., 2007; Breuleux et al., 2009; Masola et al., 2013).
Additionally, being EMT regulated by several signaling factors such as TGF-β, epidermal growth factor (EGF), fibroblast growth factor (FGF), IL-1, connective tissue growth factor (CTGF), insulin-like growth factor-2 (IGF-2), nuclear factor-kB (NF-kB) and Wnt (Nieto et al., 2016), pro-fibrotic mTOR-I-associated effects may be enhanced by concomitant pathological conditions including viral and bacterial infections.
Contrarily, other studies have reported that mTOR-I, whether administrated at low dosage, may exert anti-fibrotic effects (Huber et al., 2011; Kurdián et al., 2012; Zaza et al., 2014). Pontrelli et al., have described that rapamycin, reducing plasminogen activator inhibitor (PAI)-1 expression, was able to decrease extracellular matrix deposition in all renal compartments of patients with chronic allograft nephropathy (Pontrelli et al., 2008).
Therefore, based on these results, we encourage transplant clinicians, whenever possible, to prescribe low dose of everolimus/sirolimus in kidney transplant recipients in order to maximize therapeutic efficacy (also anti-fibrotic) and minimize the risk of developing this complication.
The PI3K/AKT/mTOR pathway has been shown to be targeted by various viruses, including influenza virus, herpesvirus, hepatitis C virus and adenovirus (Moody et al., 2005; Sodhi et al., 2006; Bose et al., 2012; Le Sage et al., 2016), and recent studies have clearly reported its activation also during SARS-CoV-2 infection (Appelberg et al., 2020; Lokhande and Devarajan, 2021). The viruses subvert the mTOR pathway to sustain protein synthesis, cell survival and promote virus replication (Moody et al., 2005). mTOR is an evolutionarily conserved serine/threonine kinase, component of two multi-subunit complexes, mTORC1 and mTORC2. Activated mTORC1 induces metabolic effects such as mRNA translation, ribosome biogenesis, protein synthesis, mitochondrial metabolism, and adipogenesis. mTORC2 promotes cell survival, regulates the actin cytoskeleton, ion transport, and cell growth (Dowling et al., 2010). Thus, targeting this pathway might reduce SARS-CoV-2 pathogenicity.
This effect has been also observed in rapamycin-treated cells infected with MERS-CoV and 1918 influenza A virus (Kindrachuk et al., 2015; Ranadheera et al., 2018). Likewise in patients with severe H1N1 pneumonia, early adjuvant treatment with rapamycin and corticosteroids was associated with a rapid virus clearance and a significant clinical improvement (Wang et al., 2014).
In addition, as reported by Garcia et al., nanomolar concentrations of berzosertib, AZD2014 and Torin-2 may exert important anti-SARS-CoV-2 effects by targeting PI3K/AKT/mTOR pathway (Garcia et al., 2021).
Contrarily, an in vitro study performed in a human hepato cellular carcinoma cell line demonstrated that rapamycin and Torin-1 failed to block viral infection (Appelberg et al., 2020). However, Akt inhibitor MK-2206, probably by stabilization of mTORC1, showed significant inhibition of viral replication.
Furthermore, the therapeutic potential of mTOR-Is in SARS-CoV-2 infection could also be linked to their immunomodulatory properties.
mTOR pathway, in fact, has a central role in B and T cells development/proliferation. In B cells, mTOR inhibition, through the down-regulation of the transcription factor BCL6, may inhibit germinal center formation (Raybuck et al., 2018) and the proliferation of germinal center B cells thereby hindering development of memory B cells and long-lived plasma cells (Ye et al., 2017). In contrast rapamycin seems to have a minimal effect during the differentiation of germinal center B cells into long-lived plasma cells as well as on the maintenance of already-differentiated long-lived plasma cells (Ye et al., 2017). This effect could influence the response to vaccination in mTOR-I treated kidney transplant recipients.
Moreover, rapamycin, downregulating the expression of activation-induced cytidine deaminase (AID), could also decrease antibody class-switch recombination altering the pattern of immunoglobulin (Ig) G and IgM specificities (Zhang et al., 2013). It has been speculated that this effect may lead to a reduction of the early-stage antibodies crossreactivity against SARS-CoV-2 and to a decrease of the antibody dependant enhancement (LDE). Both these conditions may antagonize the onset and development of severe symptoms (Zheng et al., 2020).
Specific deletion of mTOR in T cells, then, might impair their differentiation in Th1, Th2 or Th17 effector cells (by a direct down-regulation of STAT and other lineage specific transcription factors (Delgoffe et al., 2009)) and induce a significant enhancement of regulatory T cells (Treg) (Battaglia et al., 2005).
At the same time, these agents may have immunostimulatory effects on memory CD8+ (Araki et al., 2009) and CD4+ T cells (Ye et al., 2017) by promoting the enhancement of memory precursor effector cells that could differentiate into long-lived memory cells (Araki et al., 2009; Ye et al., 2017).
Additionally, mTOR-I when given at the early onset of the cytokine storm phase can hinder the IL-6 pathway and NLRP3 inflammasome-dependent release of IL-1β, thus preventing the progression to severe forms of COVID-19 (Omarjee et al., 2020).
mTOR activation can also increase the activity of anti-inflammatory cytokine IL-10 and inhibit the proinflammatory cytokine TNF-α (Weichhart et al., 2015). Therefore, it is unquestionable that mTOR-Is could act as a double edge sword in patients with COVID-19 (Ghasemnejad-Berenji, 2021) and a correct use of this medication may have a “yin or yang” clinical effects. The ongoing trials (NCT04341675, NCT04461340, NCT04948203) that evaluates the effects of sirolimus treatment in hospitalized COVID-19 patients will provide more information in the next future.
NCT04341675 compares sirolimus (6 mg on day 1 followed by 2 mg daily for the next 13 days or until hospital discharge, whatever happens sooner) versus placebo in hospitalized patients with severe COVID-19. The primary outcome is death or progression to respiratory failure requiring advanced respiratory at day 28.
NCT04461340 asseses the efficacy and safety of sirolimus as an adjuvant agent to the standard treatment protocol against COVID-19. It is a single-blinded randomized study in which participants are randomly assigned to sirolimus (oral dose of 6 mg on day 1 followed by 2 mg daily for 9 days) plus national standard of care therapy against COVID-19 or only national standard of care therapy against COVID-19.
Interestingly, the trial NCT04948203 evaluates the efficacy of sirolimus in preventing post-COVID-19 pulmonary fibrosis. The hospitalized patients with <10% pulmonary fibrosis, evaluated by CT at admission, are divided in three groups according to different dose regimens of sirolimus (0.5, 1 or 2 mg orally daily) for 14 days. Pulmonary fibrosis is, then, evaluated by CT scan after 12 weeks.
In COVID-19 kidney transplant recipients, at the moment, we do not have enough evidence to support the hypothesis that mTOR-I may antagonize recovery or promote pulmonary complications and contrasting results have been obtained in observational studies (Cravedi et al., 2020; Alberici et al., 2020; Fernández-Ruiz et al., 2020; Caillard et al., 2020; Coll et al., 2021; Favà et al., 2020; Hilbrands et al., 2020; Pérez-Sáez et al., 2020; Salto-Alejandre et al., 2021; Søfteland et al., 2021; Bossini et al., 2020; Crespo et al., 2020; Rodriguez-Cubillo et al., 2020; Meziyerh et al., 2020; Guillen et al., 2020; Zhang et al., 2020; Lauterio et al., 2020; Tanaka et al., 2020; Heron et al., 2021; Nair et al., 2020; Devresse et al., 2020; Maritati et al., 2020; Trujillo et al., 2020; Lubetzky et al., 2020) (Table 1). In studies with large cohort of kidney transplant recipients approximately 10–15% of them were treated with mTOR-Is and more than 50% of these patients stopped this treatment after hospital admission. However, this did not impact the clinical outcomes. Expert opinions suggested to discontinue this drug category in patients tested positive for COVID-19 with or without clinical or radiological evidence of lung disease (Vistoli et al., 2020). This choice could be due to the pulmonary toxicity associated with mTOR-Is (Meziyerh et al., 2020) or to a possible interaction between mTOR-Is and antiviral drugs commonly used in COVID-19 patients (Maggiore et al., 2020). The co-administration of hydroxychloroquine and chloroquine with mTOR-I (all CYP3A4 inhibitors) may theoretically increase their blood concentrations with the development of potential adverse effects/toxicities (including QT-prolongation) (Mirjalili et al., 2020). This condition has been also described in patients treated with Lopinavir/Ritonavir, protease inhibitor largely used in the treatment of human immunodeficiency virus (HIV) and 50–90% reduction in dose of sirolimus and discontinuation of everolimus hase been proposed (Barau et al., 2009; Meziyerh et al., 2020).
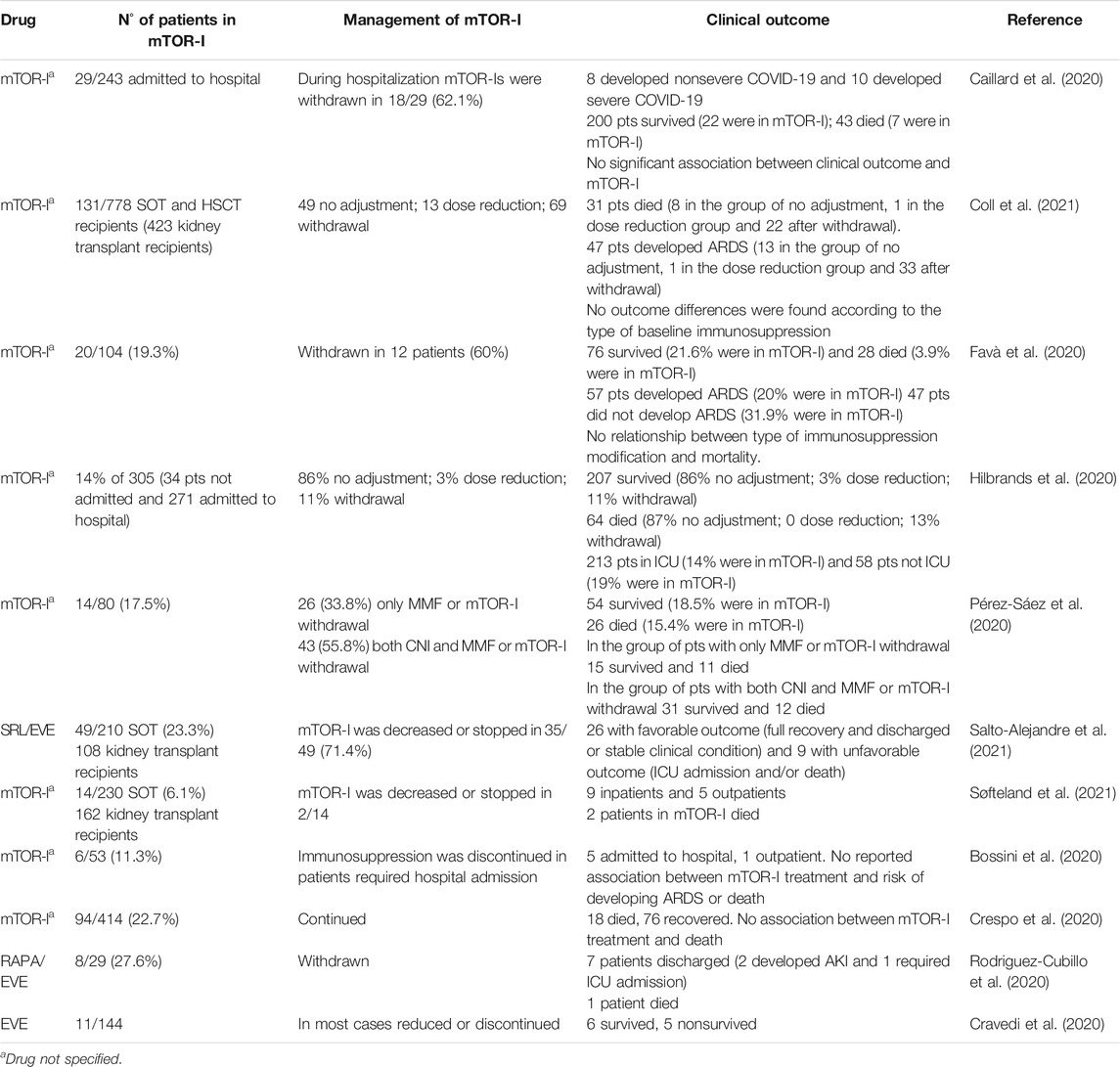
TABLE 1. Management of mTOR-I therapy and outcomes in kidney transplant recipients with COVID-19
However, although a withdrawal of immunosuppression may have positive effects by restoring the host immunity, it could expose patients to a high risk of acute rejection with negative clinical and psychological impact.
Therefore, mTOR-Is discontinuation should be reserved to kidney transplant recipients with severe COVID-19, while it should be, if possible, avoid in asymptomatic/paucisymptomatic patients in order to do not increase their risk to develop an immune-mediated graft impairment and to take advantage of some potential antiviral proprieties of these agents.
Several clinical trials have reported a reduced rate of Cytomegalovirus and BKV infections in kidney transplant recipients treated with mTOR-Is alone or associated to low dosages of calcineurin inhibitors (CNI) compared to those in standard dose CNI regimen (Tedesco Silva et al., 2010; Brennan et al., 2011; Mallat et al., 2017; Tedesco-Silva et al., 2019; Hauser et al., 2021). The exact mechanism behind this protection is not clear. Compelling data suggest an antivirial role of mTOR-I by blocking cellular proliferation and impairing pathways critical for infection, signaling, and replication (Liacini et al., 2010; Clippinger et al., 2011). In addition, mTOR-I may have a direct anti-viral activity by increasing the percentage of multifunctional virus-specific CD4 T cells (Hauser et al., 2021).
Furthermore, at the moment, the impact of the co-treatment of mTOR-I with other drugs frequently employed in the treatment of COVID-19 kidney transplant recipients (including corticosteroids, anti-inflammatory agents, monoclonal antibodies) has been only partially elucidated. We can only suppose that, being mTOR a central kinase of the cellular metabolism, its inhibition may have consequence on the pharmacological effects of these agents. As reported by Weichhart et al., corticosteroids, inducing the expression of REDD1, may potentiate the pharmacological inhibition of the mTOR pathway. This is in line with previous data obtained in patients affected by H1N1 influenza virus (Weichhart et al., 2011). Additionally, the inhibition of mTOR, preventing the immune hyperactivation of the signal via the STAT3 pathway may reduce the expression of receptors for IL-6 and IL-6 production (Terrazzano et al., 2020), that may influence the pharmacological effects of Tocilizumab.
All the above mentioned effects need to be analyzed in specific research project involving organ transplant recipients.
Solid organ transplant candidates and recipients are identified as a priority population for COVID-19 vaccines, given the higher risks associated with immunosuppressed status. Currently, vaccines employable for transplant recipients are BNT162b2 (Pfizer-BioNTech) and mRNA-1273 (Moderna).
However, data regarding safety, immunogenicity, and efficacy in these patients are scarce. Some evidence indicates that solid organ transplant recipients who receive mRNA-based vaccines have low immunization rates (Benotmane et al., 2021; Boyarsky et al., 2021; Danthu et al., 2021; Grupper et al., 2021; Husain et al., 2021; Korth et al., 2021; Sattler et al., 2021) and also in patients with full dose vaccination has reported the development of COVID-19 (Caillard et al., 2021; Tsapepas et al., 2021). When quantitative titers were available, they were frequently below the median titer in immunocompetent patients. Moreover, Rincon-Arevalo et al., have recently described markedly diminished generation of antigen-specific B cells, especially, plasmablasts and memory B cells in kidney transplant recipients (Rincon-Arevalo et al., 2021).
Factors associated with negative humoral response to vaccine were older age, high-dose corticosteroids treatments, maintenance with triple immunosuppressive medications and a regimen that includes anti-metabolite (Boyarsky et al., 2021; Grupper et al., 2021; Husain et al., 2021). The effect of mTOR-I on COVID-19 vaccine is controversial, with some studies reporting a more favorable humoral response (Benotmane et al., 2021; Cucchiari et al., 2021) and other that obtained opposing results (Rozen-Zvi et al., 2021) or no differences in immunosuppressive drugs between kidney transplant recipients tested positive and negative for SARS-CoV-2 IgG (Korth et al., 2021).
Previous studies evaluating the response to vaccination in kidney transplant recipients reported that everolimus or sirolimus are associated with a significant rise in the antigen-specific IgG antibody level after pneumococcal, tetanus and influenza vaccines (Willcocks et al., 2007; Struijk et al., 2010). This could be due to the increment of CD8+ effector memory T cells obtained by mTOR-I (Araki et al., 2009; Turner et al., 2011).
However, being these studies not COVID-19 specific and contrasting, we cannot draw definite conclusion on the effects of these drugs on COVID-19 vaccine response. The result of ongoing studies on this topic will help in future to better define this relationship.
The rapid spread of COVID-19 has pushed physicians to make clinical decisions by the principle of maximizing benefits for the largest number of patients. However, the optimal medical management of kidney transplant recipients with SARS-CoV-2 infection has not yet been established.
The most common approach is the withdrawal of immunosuppressive drugs (including mTOR-ihibitors) in these patients to potentiate their immunocompetence and minimize the risk of clinical complications of severe COVID-19.
However, at our opinion, in kidney transplant recipients in mTOR-Is-based immunosuppressive therapy, this “discontinuation strategy” should be reserved for patients with severe COVID-19. Instead, in asymptomatic patients or those with mild COVID-19 symptoms, a “wait and see approach” or a reduction of the dosage of these agents may be useful to minimize the risk of acute allograft rejection development and to exploit their potential anti-viral and anti-fibrotic effects. The reduction of the dosage may partially restore the host immunity facilitating the disease recovery, antagonize/mitigate the onset of cytokine storm, and preserve Treg growth and activity, which could reduce the progression to severe COVID-19.
Moreover, additional clinical studies aimed to evaluate the impact of mTOR-I on the vaccines and to assess the efficacy and safety of the use of mTOR-I alone or in combination with other new anti-fibrotic agents in kidney transplant recipients with COVID-19 are necessary to allow a more efficient treatment of the acute clinical phase and facilitate the recovery from post-acute COVID-19. Indeed, while most people with COVID-19 recover completely within a few weeks, some patients experience lasting symptoms (fatigue, shortness of breath, cough, joint pain, depression, muscle pain, headache, intermittent fever) that can continue for weeks or even months after initial recovery.
Finally, we believe that molecular biology (particularly omics techniques) may represent powerful methods that could help kidney transplant clinicians to discover new therapeutic strategies for SARS-CoV-2 infection, to select new biomolecular targets and to personalize its treatments (Zaza et al., 2015).
SG and GZ searched the literature and wrote the manuscript. PC and GS contributed to the literature analysis and revised the manuscript. All authors read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ARDS, acute respiratory distress syndrome; EVE, everolimus; ICU, intensive care unit; RAPA, rapamycin; SRL, sirolimus; SOT, solid organ transplantation; HSCT, hematopoietic stem cell transplantation; MMF, mycophenolate mofetil.
Ahmad Alhiyari, M., Ata, F., Islam Alghizzawi, M., Bint I Bilal, A., Salih Abdulhadi, A., and Yousaf, Z. (2021). Post COVID-19 Fibrosis, an Emerging Complicationof SARS-CoV-2 Infection. IDCases 23, e01041. doi:10.1016/j.idcr.2020.e01041
Akalin, E., Azzi, Y., Bartash, R., Seethamraju, H., Parides, M., Hemmige, V., et al. (2020). Covid-19 and Kidney Transplantation. N. Engl. J. Med. 382 (25), 2475–2477. doi:10.1056/NEJMc2011117
Alberici, F., Delbarba, E., Manenti, C., Econimo, L., Valerio, F., Pola, A., et al. (2020). A Single center Observational Study of the Clinical Characteristics and Short-Term Outcome of 20 Kidney Transplant Patients Admitted for SARS-CoV2 Pneumonia. Kidney Int. 97 (6), 1083–1088. doi:10.1016/j.kint.2020.04.002
Alexandru, S., Ortiz, A., Baldovi, S., Milicua, J. M., Ruíz-Escribano, E., Egido, J., et al. (2008). Severe Everolimus-Associated Pneumonitis in a Renal Transplant Recipient. Nephrol. Dial. Transpl. 23 (10), 3353–3355. doi:10.1093/ndt/gfn401
Alon, R., Sportiello, M., Kozlovski, S., Kumar, A., Reilly, E. C., Zarbock, A., et al. (2021). Leukocyte Trafficking to the Lungs and beyond: Lessons from Influenza for COVID-19. Nat. Rev. Immunol. 21 (1), 49–64. doi:10.1038/s41577-020-00470-2
Appelberg, S., Gupta, S., Svensson Akusjärvi, S., Ambikan, A. T., Mikaeloff, F., Saccon, E., et al. (2020). Dysregulation in Akt/mTOR/HIF-1 Signaling Identified by Proteo-Transcriptomics of SARS-CoV-2 Infected Cells. Emerg. Microbes Infect. 9 (1), 1748–1760. doi:10.1080/22221751.2020.1799723
Araki, K., Turner, A. P., Shaffer, V. O., Gangappa, S., Keller, S. A., Bachmann, M. F., et al. (2009). mTOR Regulates Memory CD8 T-Cell Differentiation. Nature 460 (7251), 108–112. doi:10.1038/nature08155
Banerjee, D., Popoola, J., Shah, S., Ster, I. C., Quan, V., and Phanish, M. (2020). COVID-19 Infection in Kidney Transplant Recipients. Kidney Int. 97 (6), 1076–1082. doi:10.1016/j.kint.2020.03.018
Barau, C., Blouin, P., Creput, C., Taburet, A. M., Durrbach, A., and Furlan, V. (2009). Effect of Coadministered HIV-Protease Inhibitors on Tacrolimus and Sirolimus Blood Concentrations in a Kidney Transplant Recipient. Fundam. Clin. Pharmacol. 23 (4), 423–425. doi:10.1111/j.1472-8206.2009.00706.x
Barratt, S. L., Flower, V. A., Pauling, J. D., and Millar, A. B. (2018). VEGF (Vascular Endothelial Growth Factor) and Fibrotic Lung Disease. Int. J. Mol. Sci. 19 (5), 1269. doi:10.3390/ijms19051269
Battaglia, M., Stabilini, A., and Roncarolo, M. G. (2005). Rapamycin Selectively Expands CD4+CD25+FoxP3+ Regulatory T Cells. Blood 105 (12), 4743–4748. doi:10.1182/blood-2004-10-3932
Benotmane, I., Gautier-Vargas, G., Cognard, N., Olagne, J., Heibel, F., Braun-Parvez, L., et al. (2021). Low Immunization Rates Among Kidney Transplant Recipients Who Received 2 Doses of the mRNA-1273 SARS-CoV-2 Vaccine. Kidney Int. 99 (6), 1498–1500. doi:10.1016/j.kint.2021.04.005
Bertolini, L., Vaglio, A., Bignardi, L., Buzio, C., De Filippo, M., Palmisano, A., et al. (2011). Subclinical Interstitial Lung Abnormalities in Stable Renal Allograft Recipients in the Era of Modern Immunosuppression. Transpl. Proc 43 (7), 2617–2623. doi:10.1016/j.transproceed.2011.06.033
Bose, S. K., Shrivastava, S., Meyer, K., Ray, R. B., and Ray, R. (2012). Hepatitis C Virus Activates the mTOR/S6K1 Signaling Pathway in Inhibiting IRS-1 Function for Insulin Resistance. J. Virol. 86 (11), 6315–6322. doi:10.1128/JVI.00050-12
Bossini, N., Alberici, F., Delbarba, E., Valerio, F., Manenti, C., Possenti, S., et al. (2020). Kidney Transplant Patients with SARS-CoV-2 Infection: The Brescia Renal COVID Task Force Experience. Am. J. Transpl. 20 (11), 3019–3029. doi:10.1111/ajt.16176
Boyarsky, B. J., Werbel, W. A., Avery, R. K., Tobian, A. A. R., Massie, A. B., Segev, D. L., et al. (2021). Antibody Response to 2-Dose SARS-CoV-2 mRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 325 (21), 2204–2206. doi:10.1001/jama.2021.7489
Brennan, D. C., Legendre, C., Patel, D., Mange, K., Wiland, A., McCague, K., et al. (2011). Cytomegalovirus Incidence between Everolimus versus Mycophenolate in De Novo Renal Transplants: Pooled Analysis of Three Clinical Trials. Am. J. Transpl. 11 (11), 2453–2462. doi:10.1111/j.1600-6143.2011.03674.x
Breuleux, M., Klopfenstein, M., Stephan, C., Doughty, C. A., Barys, L., Maira, S. M., et al. (2009). Increased AKT S473 Phosphorylation after mTORC1 Inhibition Is Rictor Dependent and Does Not Predict Tumor Cell Response to PI3K/mTOR Inhibition. Mol. Cancer Ther. 8 (4), 742–753. doi:10.1158/1535-7163.MCT-08-0668
Buonaguro, F. M., Puzanov, I., and Ascierto, P. A. (2020). Anti-IL6R Role in Treatment of COVID-19-Related ARDS. J. Transl Med. 18 (1), 165. doi:10.1186/s12967-020-02333-9
Caillard, S., Anglicheau, D., Matignon, M., Durrbach, A., Greze, C., Frimat, L., et al. (2020). An Initial Report from the French SOT COVID Registry Suggests High Mortality Due to COVID-19 in Recipients of Kidney Transplants. Kidney Int. 98 (6), 1549–1558. doi:10.1016/j.kint.2020.08.005
Caillard, S., Chavarot, N., Bertrand, D., Kamar, N., Thaunat, O., Moal, V., et al. (2021). Occurrence of Severe COVID-19 in Vaccinated Transplant Patients. Kidney Int. -2538 (21), 0085005099–S8500513. doi:10.1016/j.kint.2021.05.011
Champion, L., Stern, M., Israël-Biet, D., Mamzer-Bruneel, M. F., Peraldi, M. N., Kreis, H., et al. (2006). Brief Communication: Sirolimus-Associated Pneumonitis: 24 Cases in Renal Transplant Recipients. Ann. Intern. Med. 144 (7), 505–509. doi:10.7326/0003-4819-144-7-200604040-00009
Chernyak, B. V., Popova, E. N., Prikhodko, A. S., Grebenchikov, O. A., Zinovkina, L. A., and Zinovkin, R. A. (2020). COVID-19 and Oxidative Stress. Biochemistry (Mosc) 85 (12), 1543–1553. doi:10.1134/S0006297920120068
Clippinger, A. J., Maguire, T. G., and Alwine, J. C. (2011). The Changing Role of mTOR Kinase in the Maintenance of Protein Synthesis during Human Cytomegalovirus Infection. J. Virol. 85 (8), 3930–3939. doi:10.1128/JVI.01913-10
Coll, E., Fernández-Ruiz, M., Sánchez-Álvarez, J. E., Martínez-Fernández, J. R., Crespo, M., Gayoso, J., et al. (2021). COVID-19 in Transplant Recipients: The Spanish Experience. Am. J. Transpl. 21 (5), 1825–1837. doi:10.1111/ajt.16369
Cravedi, P., Mothi, S. S., Azzi, Y., Haverly, M., Farouk, S. S., Pérez-Sáez, M. J., et al. (2020). COVID-19 and Kidney Transplantation: Results from the TANGO International Transplant Consortium. Am. J. Transpl. 20 (11), 3140–3148. doi:10.1111/ajt.16185
Crespo, M., Mazuecos, A., Rodrigo, E., Gavela, E., Villanego, F., Sánchez-Alvarez, E., et al. (2020). Respiratory and Gastrointestinal COVID-19 Phenotypes in Kidney Transplant Recipients. Transplantation 104 (11), 2225–2233. doi:10.1097/TP.0000000000003413
Cucchiari, D., Egri, N., Bodro, M., Herrera, S., Del Risco‐Zevallos, J., Casals‐Urquiza, J., et al. (2021). Cellular and Humoral Response after MRNA‐1273 SARS‐CoV‐2 Vaccine in Kidney Transplant Recipients. Am. J. Transpl. 21, 2727–2739. doi:10.1111/ajt.16701
Danthu, C., Hantz, S., Dahlem, A., Duval, M., Ba, B., Guibbert, M., et al. (2021). Humoral Response after SARS-Cov-2 mRNA Vaccine in a Cohort of Hemodialysis Patients and Kidney Transplant Recipients. J. Am. Soc. Nephrol. ASN.2021040490.
Delgoffe, G. M., Kole, T. P., Zheng, Y., Zarek, P. E., Matthews, K. L., Xiao, B., et al. (2009). The mTOR Kinase Differentially Regulates Effector and Regulatory T Cell Lineage Commitment. Immunity 30 (6), 832–844. doi:10.1016/j.immuni.2009.04.014
Devresse, A., Belkhir, L., Vo, B., Ghaye, B., Scohy, A., Kabamba, B., et al. (2020). COVID-19 Infection in Kidney Transplant Recipients: A Single-Center Case Series of 22 Cases from Belgium. Kidney Med. 2 (4), 459–466. doi:10.1016/j.xkme.2020.06.001
Dowling, R. J., Topisirovic, I., Fonseca, B. D., and Sonenberg, N. (2010). Dissecting the Role of mTOR: Lessons from mTOR Inhibitors. Biochim. Biophys. Acta 1804 (3), 433–439. doi:10.1016/j.bbapap.2009.12.001
Drake, T. M., Docherty, A. B., Harrison, E. M., Quint, J. K., Adamali, H., Agnew, S., et al. (2020). Outcome of Hospitalization for COVID-19 in Patients with Interstitial Lung Disease: An International Multicenter Study. Am. J. Respir. Crit. Care Med. 202 (12), 1656–1665. doi:10.1164/rccm.202007-2794OC
Elias, M., Pievani, D., Randoux, C., Louis, K., Denis, B., Delion, A., et al. (2020). COVID-19 Infection in Kidney Transplant Recipients: Disease Incidence and Clinical Outcomes. J. Am. Soc. Nephrol. 31 (10), 2413–2423. doi:10.1681/ASN.2020050639
Errasti, P., Izquierdo, D., Martín, P., Errasti, M., Slon, F., Romero, A., et al. (2010). Pneumonitis Associated with Mammalian Target of Rapamycin Inhibitors in Renal Transplant Recipients: a Single-center Experience. Transpl. Proc 42 (8), 3053–3054. doi:10.1016/j.transproceed.2010.07.066
Esposito, A. J., Menon, A. A., Ghosh, A. J., Putman, R. K., Fredenburgh, L. E., El-Chemaly, S. Y., et al. (2020). Increased Odds of Death for Patients with Interstitial Lung Disease and COVID-19: A Case-Control Study. Am. J. Respir. Crit. Care Med. 202 (12), 1710–1713. doi:10.1164/rccm.202006-2441LE
Favà, A., Cucchiari, D., Montero, N., Toapanta, N., Centellas, F. J., Vila-Santandreu, A., et al. (2020). Clinical Characteristics and Risk Factors for Severe COVID-19 in Hospitalized Kidney Transplant Recipients: A Multicentric Cohort Study. Am. J. Transpl. 20 (11), 3030–3041. doi:10.1111/ajt.16246
Fernandez, I. E., and Eickelberg, O. (2012). The Impact of TGF-β on Lung Fibrosis: from Targeting to Biomarkers. Proc. Am. Thorac. Soc. 9 (3), 111–116. doi:10.1513/pats.201203-023AW
Fernández-Ruiz, M., Andrés, A., Loinaz, C., Delgado, J. F., López-Medrano, F., San Juan, R., et al. (2020). COVID-19 in Solid Organ Transplant Recipients: A Single-center Case Series from Spain. Am. J. Transpl. 20 (7), 1849–1858. doi:10.1111/ajt.15929
Garcia, G., Sharma, A., Ramaiah, A., Sen, C., Purkayastha, A., Kohn, D. B., et al. (2021). Antiviral Drug Screen Identifies DNA-Damage Response Inhibitor as Potent Blocker of SARS-CoV-2 Replication. Cell Rep 35 (1), 108940. doi:10.1016/j.celrep.2021.108940
George, P. M., Wells, A. U., and Jenkins, R. G. (2020). Pulmonary Fibrosis and COVID-19: the Potential Role for Antifibrotic Therapy. Lancet Respir. Med. 8 (8), 807–815. doi:10.1016/S2213-2600(20)30225-3
Ghasemnejad-Berenji, M. (2021). mTOR Inhibition: a Double-Edged Sword in Patients with COVID-19?. Hum. Cel 34 (2), 698–699. doi:10.1007/s13577-021-00495-2
Granata, S., Santoro, G., Masola, V., Tomei, P., Sallustio, F., Pontrelli, P., et al. (2018). In Vitro Identification of New Transcriptomic and miRNomic Profiles Associated with Pulmonary Fibrosis Induced by High Doses Everolimus: Looking for New Pathogenetic Markers and Therapeutic Targets. Int. J. Mol. Sci. 19 (4), 1250. doi:10.3390/ijms19041250
Gross, D. C., Sasaki, T. M., Buick, M. K., and Light, J. A. (1997). Acute Respiratory Failure and Pulmonary Fibrosis Secondary to Administration of Mycophenolate Mofetil. Transplantation 64 (11), 1607–1609. doi:10.1097/00007890-199712150-00020
Grupper, A., Rabinowich, L., Schwartz, D., Schwartz, I. F., Ben‐Yehoyada, M., Shashar, M., et al. (2021). Reduced Humoral Response to mRNA SARS‐CoV‐2 BNT162b2 Vaccine in Kidney Transplant Recipients without Prior Exposure to the Virus. Am. J. Transpl. 21, 2719–2726. doi:10.1111/ajt.16615
Gubernatorova, E. O., Gorshkova, E. A., Polinova, A. I., and Drutskaya, M. S. (2020). IL-6: Relevance for Immunopathology of SARS-CoV-2. Cytokine Growth Factor. Rev. 53, 13–24. doi:10.1016/j.cytogfr.2020.05.009
Guillen, E., Pineiro, G. J., Revuelta, I., Rodriguez, D., Bodro, M., Moreno, A., et al. (2020). Case Report of COVID-19 in a Kidney Transplant Recipient: Does Immunosuppression Alter the Clinical Presentation?. Am. J. Transpl. 20 (7), 1875–1878. doi:10.1111/ajt.15874
Hauser, I. A., Marx, S., Sommerer, C., Suwelack, B., Dragun, D., Witzke, O., et al. (2021). Effect of Everolimus-Based Drug Regimens on CMV-specific T-Cell Functionality after Renal Transplantation: 12-month ATHENA Subcohort-Study Results. Eur. J. Immunol. 51 (4), 943–955. doi:10.1002/eji.202048855
Heron, V. C., Bach, C. T., Holmes, N. E., and Whitlam, J. B. (2021). Complete Recovery from COVID-19 of a Kidney-Pancreas Transplant Recipient: Potential Benefit from Everolimus?. BMJ Case Rep. 14 (1), e238413. doi:10.1136/bcr-2020-238413
Higham, A., Mathioudakis, A., Vestbo, J., and Singh, D. (2020). COVID-19 and COPD: a Narrative Review of the Basic Science and Clinical Outcomes. Eur. Respir. Rev. 29 (158), 200199. doi:10.1183/16000617.0199-2020
Hilbrands, L. B., Duivenvoorden, R., Vart, P., Franssen, C. F. M., Hemmelder, M. H., Jager, K. J., et al. (2020). COVID-19-related Mortality in Kidney Transplant and Dialysis Patients: Results of the ERACODA Collaboration. Nephrol. Dial. Transpl. 35 (11), 1973–1983. doi:10.1093/ndt/gfaa261
Huang, C., Wang, Y., Li, X., Ren, L., Zhao, J., Hu, Y., et al. (2020). Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 395 (10223), 497–506. doi:10.1016/S0140-6736(20)30183-5
Huber, T. B., Walz, G., and Kuehn, E. W. (2011). mTOR and Rapamycin in the Kidney: Signaling and Therapeutic Implications beyond Immunosuppression. Kidney Int. 79 (5), 502–511. doi:10.1038/ki.2010.457
Husain, S. A., Tsapepas, D., Paget, K. F., Chang, J. H., Crew, R. J., Dube, G. K., et al. (2021). Postvaccine Anti-SARS-CoV-2 Spike Protein Antibody Development in Kidney Transplant Recipients. Kidney Int. Rep. 6 (6), 1699–1700. doi:10.1016/j.ekir.2021.04.017
Kalluri, R., and Weinberg, R. A. (2009). The Basics of Epithelial-Mesenchymal Transition. J. Clin. Invest. 119 (6), 1420–1428. doi:10.1172/JCI39104
Kataria, A., Yakubu, I., Winstead, R., Gowda, M., and Gupta, G. (2020). COVID-19 in Kidney Transplantation: Epidemiology, Management Considerations, and the Impact on Kidney Transplant Practice. Transpl. Direct 6 (8), e582. doi:10.1097/TXD.0000000000001031
Kindrachuk, J., Ork, B., Hart, B. J., Mazur, S., Holbrook, M. R., Frieman, M. B., et al. (2015). Antiviral Potential of ERK/MAPK and PI3K/AKT/mTOR Signaling Modulation for Middle East Respiratory Syndrome Coronavirus Infection as Identified by Temporal Kinome Analysis. Antimicrob. Agents Chemother. 59 (2), 1088–1099. doi:10.1128/AAC.03659-14
Kirby, S., Satoskar, A., Brodsky, S., Pope-Harman, A., Nunley, D., Hitchcock, C., et al. (2012). Histological Spectrum of Pulmonary Manifestations in Kidney Transplant Recipients on Sirolimus Inclusive Immunosuppressive Regimens. Diagn. Pathol. 7, 25. doi:10.1186/1746-1596-7-25
Korth, J., Jahn, M., Dorsch, O., Anastasiou, O. E., Sorge-Hädicke, B., Eisenberger, U., et al. (2021). Impaired Humoral Response in Renal Transplant Recipients to SARS-CoV-2 Vaccination with BNT162b2 (Pfizer-BioNTech). Viruses 13 (5), 756. doi:10.3390/v13050756
Kurdián, M., Herrero-Fresneda, I., Lloberas, N., Gimenez-Bonafe, P., Coria, V., Grande, M. T., et al. (2012). Delayed mTOR Inhibition with Low Dose of Everolimus Reduces TGFβ Expression, Attenuates Proteinuria and Renal Damage in the Renal Mass Reduction Model. PLoS One 7 (3), e32516. doi:10.1371/journal.pone.0032516
Lauterio, A., Valsecchi, M., Santambrogio, S., De Carlis, R., Merli, M., Calini, A., et al. (2020). Successful Recovery from Severe COVID-19 Pneumonia after Kidney Transplantation: The Interplay between Immunosuppression and Novel Therapy Including Tocilizumab. Transpl. Infect. Dis. 22 (5), e13334. doi:10.1111/tid.13334
Le Sage, V., Cinti, A., Amorim, R., and Mouland, A. J. (2016). Adapting the Stress Response: Viral Subversion of the mTOR Signaling Pathway. Viruses 8 (6), 152. doi:10.3390/v8060152
Li, M., Dong, Y., Wang, H., Guo, W., Zhou, H., Zhang, Z., et al. (2020). Cardiovascular Disease Potentially Contributes to the Progression and Poor Prognosis of COVID-19. Nutr. Metab. Cardiovasc. Dis. 30 (7), 1061–1067. doi:10.1016/j.numecd.2020.04.013
Li, X., Shen, C., Wang, L., Majumder, S., Zhang, D., Deen, M. J., et al. (2021). Pulmonary Fibrosis and its Related Factors in Discharged Patients with New corona Virus Pneumonia: a Cohort Study. Respir. Res. 22 (1), 203. doi:10.1186/s12931-021-01798-6
Liacini, A., Seamone, M. E., Muruve, D. A., and Tibbles, L. A. (2010). Anti-BK Virus Mechanisms of Sirolimus and Leflunomide Alone and in Combination: toward a New Therapy for BK Virus Infection. Transplantation 90 (12), 1450–1457. doi:10.1097/TP.0b013e3182007be2
Liu, J., Zheng, X., Tong, Q., Li, W., Wang, B., Sutter, K., et al. (2020). Overlapping and Discrete Aspects of the Pathology and Pathogenesis of the Emerging Human Pathogenic Coronaviruses SARS-CoV, MERS-CoV, and 2019-nCoV. J. Med. Virol. 92 (5), 491–494. doi:10.1002/jmv.25709
Liu, X., Zhou, H., Zhou, Y., Wu, X., Zhao, Y., Lu, Y., et al. (2020). Risk Factors Associated with Disease Severity and Length of Hospital Stay in COVID-19 Patients. J. Infect. 81 (1), e95–e97. doi:10.1016/j.jinf.2020.04.008
Lokhande, A. S., and Devarajan, P. V. (2021). A Review on Possible Mechanistic Insights of Nitazoxanide for Repurposing in COVID-19. Eur. J. Pharmacol. 891, 173748. doi:10.1016/j.ejphar.2020.173748
Lubetzky, M., Aull, M. J., Craig-Schapiro, R., Lee, J. R., Marku-Podvorica, J., Salinas, T., et al. (2020). Kidney Allograft Recipients, Immunosuppression, and Coronavirus Disease-2019: a Report of Consecutive Cases from a New York City Transplant center. Nephrol. Dial. Transpl. 35 (7), 1250–1261. doi:10.1093/ndt/gfaa154
Maggiore, U., Abramowicz, D., Crespo, M., Mariat, C., Mjoen, G., Peruzzi, L., et al. (2020). How Should I Manage Immunosuppression in a Kidney Transplant Patient with COVID-19? an ERA-EDTA DESCARTES Expert Opinion. Nephrol. Dial. Transpl. 35 (6), 899–904. doi:10.1093/ndt/gfaa130
Mallat, S. G., Tanios, B. Y., Itani, H. S., Lotfi, T., McMullan, C., Gabardi, S., et al. (2017). CMV and BKPyV Infections in Renal Transplant Recipients Receiving an mTOR Inhibitor-Based Regimen versus a CNI-Based Regimen: A Systematic Review and Meta-Analysis of Randomized, Controlled Trials. Clin. J. Am. Soc. Nephrol. 12 (8), 1321–1336. doi:10.2215/CJN.13221216
Maritati, F., Cerutti, E., Zuccatosta, L., Fiorentini, A., Finale, C., Ficosecco, M., et al. (2020). SARS-CoV-2 Infection in Kidney Transplant Recipients: Experience of the Italian Marche Region. Transpl. Infect. Dis. 22 (5), e13377. doi:10.1111/tid.13377
Masola, V., Zaza, G., Granata, S., Gambaro, G., Onisto, M., and Lupo, A. (2013). Everolimus-induced Epithelial to Mesenchymal Transition in Immortalized Human Renal Proximal Tubular Epithelial Cells: Key Role of Heparanase. J. Transl Med. 11, 292. doi:10.1186/1479-5876-11-292
Meziyerh, S., Zwart, T. C., van Etten, R. W., Janson, J. A., van Gelder, T., Alwayn, I. P. J., et al. (2020). Severe COVID-19 in a Renal Transplant Recipient: A Focus on Pharmacokinetics. Am. J. Transpl. 20 (7), 1896–1901. doi:10.1111/ajt.15943
Mirjalili, M., Shafiekhani, M., and Vazin, A. (2020). Coronavirus Disease 2019 (COVID-19) and Transplantation: Pharmacotherapeutic Management of Immunosuppression Regimen. Ther. Clin. Risk Manag. 16, 617–629. doi:10.2147/TCRM.S256246
Mo, X., Jian, W., Su, Z., Chen, M., Peng, H., Peng, P., et al. (2020). Abnormal Pulmonary Function in COVID-19 Patients at Time of Hospital Discharge. Eur. Respir. J. 55 (6), 2001217. doi:10.1183/13993003.01217-2020
Molas-Ferrer, G., Soy-Muner, D., Anglada-Martínez, H., Riu-Viladoms, G., Estefanell-Tejero, A., and Ribas-Sala, J. (2013). Interstitial Pneumonitis as an Adverse Reaction to mTOR Inhibitors. Nefrologia 33 (3), 297–300. doi:10.3265/Nefrologia.pre2013.Jan.11439
Moody, C. A., Scott, R. S., Amirghahari, N., Nathan, C. O., Young, L. S., Dawson, C. W., et al. (2005). Modulation of the Cell Growth Regulator mTOR by Epstein-Barr Virus-Encoded LMP2A. J. Virol. 79 (9), 5499–5506. doi:10.1128/JVI.79.9.5499-5506.2005
Morelon, E., Stern, M., Israël-Biet, D., Correas, J. M., Danel, C., Mamzer-Bruneel, M. F., et al. (2001). Characteristics of Sirolimus-Associated Interstitial Pneumonitis in Renal Transplant Patients. Transplantation 72 (5), 787–790. doi:10.1097/00007890-200109150-00008
Muniyappa, R., and Gubbi, S. (2020). COVID-19 Pandemic, Coronaviruses, and Diabetes Mellitus. Am. J. Physiol. Endocrinol. Metab. 318 (5), E736–E741. doi:10.1152/ajpendo.00124.2020
Nair, V., Jandovitz, N., Hirsch, J. S., Nair, G., Abate, M., Bhaskaran, M., et al. (2020). COVID-19 in Kidney Transplant Recipients. Am. J. Transpl. 20 (7), 1819–1825. doi:10.1111/ajt.15967
Nieto, M. A., Huang, R. Y., Jackson, R. A., and Thiery, J. P. (2016). EMT: 2016. Cell 166 (1), 21–45. doi:10.1016/j.cell.2016.06.028
Ojo, A. S., Balogun, S. A., Williams, O. T., and Ojo, O. S. (2020). Pulmonary Fibrosis in COVID-19 Survivors: Predictive Factors and Risk Reduction Strategies. Pulm. Med. 2020, 6175964. doi:10.1155/2020/6175964
Omarjee, L., Janin, A., Perrot, F., Laviolle, B., Meilhac, O., and Mahe, G. (2020). Targeting T-Cell Senescence and Cytokine Storm with Rapamycin to Prevent Severe Progression in COVID-19. Clin. Immunol. 216, 108464. doi:10.1016/j.clim.2020.108464
Pereira, M. R., Mohan, S., Cohen, D. J., Husain, S. A., Dube, G. K., Ratner, L. E., et al. (2020). COVID-19 in Solid Organ Transplant Recipients: Initial Report from the US Epicenter. Am. J. Transpl. 20 (7), 1800–1808. doi:10.1111/ajt.15941
Pérez-Sáez, M. J., Blasco, M., Redondo-Pachón, D., Ventura-Aguiar, P., Bada-Bosch, T., Pérez-Flores, I., et al. (2020). Use of Tocilizumab in Kidney Transplant Recipients with COVID-19. Am. J. Transpl. 20 (11), 3182–3190. doi:10.1111/ajt.16192
Pham, P. T., Pham, P. C., Danovitch, G. M., Ross, D. J., Gritsch, H. A., Kendrick, E. A., et al. (2004). Sirolimus-associated Pulmonary Toxicity. Transplantation 77 (8), 1215–1220. doi:10.1097/01.tp.0000118413.92211.b6
Pontrelli, P., Rossini, M., Infante, B., Stallone, G., Schena, A., Loverre, A., et al. (2008). Rapamycin Inhibits PAI-1 Expression and Reduces Interstitial Fibrosis and Glomerulosclerosis in Chronic Allograft Nephropathy. Transplantation 85 (1), 125–134. doi:10.1097/01.tp.0000296831.91303.9a
Ranadheera, C., Coombs, K. M., and Kobasa, D. (2018). Comprehending a Killer: The Akt/mTOR Signaling Pathways Are Temporally High-Jacked by the Highly Pathogenic 1918 Influenza Virus. EBioMedicine 32, 142–163. doi:10.1016/j.ebiom.2018.05.027
Raybuck, A. L., Cho, S. H., Li, J., Rogers, M. C., Lee, K., Williams, C. L., et al. (2018). B Cell-Intrinsic mTORC1 Promotes Germinal Center-Defining Transcription Factor Gene Expression, Somatic Hypermutation, and Memory B Cell Generation in Humoral Immunity. J. Immunol. 200 (8), 2627–2639. doi:10.4049/jimmunol.1701321
Rincon-Arevalo, H., Choi, M., Stefanski, A. L., Halleck, F., Weber, U., Szelinski, F., et al. (2021). Impaired Humoral Immunity to SARS-CoV-2 BNT162b2 Vaccine in Kidney Transplant Recipients and Dialysis Patients. Sci. Immunol. 6 (60), eabj1031. doi:10.1126/sciimmunol.abj1031
Rodriguez-Cubillo, B., de la Higuera, M. A. M., Lucena, R., Franci, E. V., Hurtado, M., Romero, N. C., et al. (2020). Should Cyclosporine Be Useful in Renal Transplant Recipients Affected by SARS-CoV-2?. Am. J. Transpl. 20 (11), 3173–3181. doi:10.1111/ajt.16141
Rodríguez-Moreno, A., Ridao, N., García-Ledesma, P., Calvo, N., Pérez-Flores, I., Marques, M., et al. (2009). Sirolimus and Everolimus Induced Pneumonitis in Adult Renal Allograft Recipients: Experience in a center. Transpl. Proc 41 (6), 2163–2165. doi:10.1016/j.transproceed.2009.06.003
Rozen-Zvi, B., Yahav, D., Agur, T., Zingerman, B., Ben-Zvi, H., Atamna, A., et al. (2021). Antibody Response to SARS-CoV-2 mRNA Vaccine Among Kidney Transplant Recipients: a Prospective Cohort Study. Clin. Microbiol. Infect. 27, 1173–e4. doi:10.1016/j.cmi.2021.04.028
Salto-Alejandre, S., Jiménez-Jorge, S., Sabé, N., Ramos-Martínez, A., Linares, L., Valerio, M., et al. (2021). Risk Factors for Unfavorable Outcome and Impact of Early post-transplant Infection in Solid Organ Recipients with COVID-19: A Prospective Multicenter Cohort Study. PLoS One 16 (4), e0250796. doi:10.1371/journal.pone.0250796
Sattler, A., Schrezenmeier, E., Weber, U. A., Potekhin, A., Bachmann, F., Straub-Hohenbleicher, H., et al. (2021). Impaired Humoral and Cellular Immunity after SARS-CoV-2 BNT162b2 (Tozinameran) Prime-Boost Vaccination in Kidney Transplant Recipients. J. Clin. Invest. 131, 150175. doi:10.1172/JCI150175
Sodhi, A., Chaisuparat, R., Hu, J., Ramsdell, A. K., Manning, B. D., Sausville, E. A., et al. (2006). The TSC2/mTOR Pathway Drives Endothelial Cell Transformation Induced by the Kaposi's Sarcoma-Associated Herpesvirus G Protein-Coupled Receptor. Cancer Cell 10 (2), 133–143. doi:10.1016/j.ccr.2006.05.026
Søfteland, J. M., Friman, G., Zur‐Mühlen, B., Ericzon, B. G., Wallquist, C., Karason, K., et al. (2021). COVID‐19 in Solid Organ Transplant Recipients: A National Cohort Study from Sweden. Am. J. Transpl. 21, 2762–2773. doi:10.1111/ajt.16596
Struijk, G. H., Minnee, R. C., Koch, S. D., Zwinderman, A. H., van Donselaar-van der Pant, K. A., Idu, M. M., et al. (2010). Maintenance Immunosuppressive Therapy with Everolimus Preserves Humoral Immune Responses. Kidney Int. 78 (9), 934–940. doi:10.1038/ki.2010.269
Tanaka, R., Kakuta, Y., Tsutahara, K., Nakagawa, M., Ichimaru, N., Sakaguchi, K., et al. (2020). Successful Recovery from Coronavirus Disease 2019 in a Living Kidney Transplant Recipient Using Low-Dose Methylprednisolone. IJU Case Rep. 4 (1), 22–24. doi:10.1002/iju5.12226
Tedesco Silva, H., Cibrik, D., Johnston, T., Lackova, E., Mange, K., Panis, C., et al. (2010). Everolimus Plus Reduced-Exposure CsA versus Mycophenolic Acid Plus Standard-Exposure CsA in Renal-Transplant Recipients. Am. J. Transpl. 10 (6), 1401–1413. doi:10.1111/j.1600-6143.2010.03129.x
Tedesco-Silva, H., Pascual, J., Viklicky, O., Basic-Jukic, N., Cassuto, E., Kim, D. Y., et al. (2019). Safety of Everolimus with Reduced Calcineurin Inhibitor Exposure in De Novo Kidney Transplants: An Analysis from the Randomized TRANSFORM Study. Transplantation 103 (9), 1953–1963. doi:10.1097/TP.0000000000002626
Terrazzano, G., Rubino, V., Palatucci, A. T., Giovazzino, A., Carriero, F., and Ruggiero, G. (2020). An Open Question: Is it Rational to Inhibit the mTor-dependent Pathway as COVID-19 Therapy?. Front. Pharmacol. 11, 856. doi:10.3389/fphar.2020.00856
Thille, A. W., Esteban, A., Fernández-Segoviano, P., Rodriguez, J. M., Aramburu, J. A., Vargas-Errázuriz, P., et al. (2013). Chronology of Histological Lesions in Acute Respiratory Distress Syndrome with Diffuse Alveolar Damage: a Prospective Cohort Study of Clinical Autopsies. Lancet Respir. Med. 1 (5), 395–401. doi:10.1016/S2213-2600(13)70053-5
Tomei, P., Masola, V., Granata, S., Bellin, G., Carratù, P., Ficial, M., et al. (2016). Everolimus-induced Epithelial to Mesenchymal Transition (EMT) in Bronchial/pulmonary Cells: when the Dosage Does Matter in Transplantation. J. Nephrol. 29 (6), 881–891. doi:10.1007/s40620-016-0295-4
Trujillo, H., Caravaca-Fontán, F., Sevillano, Á., Gutiérrez, E., Caro, J., Gutiérrez, E., et al. (2020). SARS-CoV-2 Infection in Hospitalized Patients with Kidney Disease. Kidney Int. Rep. 5 (6), 905–909. doi:10.1016/j.ekir.2020.04.024
Tsapepas, D., Husain, S. A., King, K. L., Burgos, Y., Cohen, D. J., and Mohan, S. (2021). Perspectives on COVID-19 Vaccination Among Kidney and Pancreas Transplant Recipients Living in New York City. Am. J. Health Syst. Pharm., zxab272. doi:10.1093/ajhp/zxab272
Turner, A. P., Shaffer, V. O., Araki, K., Martens, C., Turner, P. L., Gangappa, S., et al. (2011). Sirolimus Enhances the Magnitude and Quality of Viral-specific CD8+ T-Cell Responses to Vaccinia Virus Vaccination in Rhesus Macaques. Am. J. Transpl. 11 (3), 613–618. doi:10.1111/j.1600-6143.2010.03407.x
Vandewiele, B., Vandecasteele, S. J., Vanwalleghem, L., and De Vriese, A. S. (2010). Diffuse Alveolar Hemorrhage Induced by Everolimus. Chest 137 (2), 456–459. doi:10.1378/chest.09-0780
Vasarmidi, E., Tsitoura, E., Spandidos, D. A., Tzanakis, N., and Antoniou, K. M. (2020). Pulmonary Fibrosis in the Aftermath of the COVID-19 Era (Review). Exp. Ther. Med. 20 (3), 2557–2560. doi:10.3892/etm.2020.8980
Vistoli, F., Furian, L., Maggiore, U., Caldara, R., Cantaluppi, V., Ferraresso, M., et al. (2020). COVID-19 and Kidney Transplantation: an Italian Survey and Consensus. J. Nephrol. 33 (4), 667–680. doi:10.1007/s40620-020-00755-8
Vlahakis, N. E., Rickman, O. B., and Morgenthaler, T. (2004). Sirolimus-associated Diffuse Alveolar Hemorrhage. Mayo Clin. Proc. 79 (4), 541–545. doi:10.4065/79.4.541
Wan, X., Harkavy, B., Shen, N., Grohar, P., and Helman, L. J. (2007). Rapamycin Induces Feedback Activation of Akt Signaling through an IGF-1r-dependent Mechanism. Oncogene 26 (13), 1932–1940. doi:10.1038/sj.onc.1209990
Wang, C. H., Chung, F. T., Lin, S. M., Huang, S. Y., Chou, C. L., Lee, K. Y., et al. (2014). Adjuvant Treatment with a Mammalian Target of Rapamycin Inhibitor, Sirolimus, and Steroids Improves Outcomes in Patients with Severe H1N1 Pneumonia and Acute Respiratory Failure. Crit. Care Med. 42 (2), 313–321. doi:10.1097/CCM.0b013e3182a2727d
Weichhart, T., Haidinger, M., Katholnig, K., Kopecky, C., Poglitsch, M., Lassnig, C., et al. (2011). Inhibition of mTOR Blocks the Anti-inflammatory Effects of Glucocorticoids in Myeloid Immune Cells. Blood 117 (16), 4273–4283. doi:10.1182/blood-2010-09-310888
Weichhart, T., Hengstschläger, M., and Linke, M. (2015). Regulation of Innate Immune Cell Function by mTOR. Nat. Rev. Immunol. 15 (10), 599–614. doi:10.1038/nri3901
Weiner, S. M., Sellin, L., Vonend, O., Schenker, P., Buchner, N. J., Flecken, M., et al. (2007). Pneumonitis Associated with Sirolimus: Clinical Characteristics, Risk Factors and Outcome-Aa Single-centre Experience and Review of the Literature. Nephrol. Dial. Transpl. 22 (12), 3631–3637. doi:10.1093/ndt/gfm420
Willcocks, L. C., Chaudhry, A. N., Smith, J. C., Ojha, S., Doffinger, R., Watson, C. J., et al. (2007). The Effect of Sirolimus Therapy on Vaccine Responses in Transplant Recipients. Am. J. Transpl. 7 (8), 2006–2011. doi:10.1111/j.1600-6143.2007.01869.x
Wu, C., Chen, X., Cai, Y., Xia, J., Zhou, X., Xu, S., et al. (2020). Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 180 (7), 934–943. doi:10.1001/jamainternmed.2020.0994
Xu, X., Dai, H., Geng, J., Wan, X., Huang, X., Li, F., et al. (2015). Rapamycin Increases CCN2 Expression of Lung Fibroblasts via Phosphoinositide 3-kinase. Lab. Invest. 95 (8), 846–859. doi:10.1038/labinvest.2015.68
Ye, L., Lee, J., Xu, L., Mohammed, A. U., Li, W., Hale, J. S., et al. (2017). mTOR Promotes Antiviral Humoral Immunity by Differentially Regulating CD4 Helper T Cell and B Cell Responses. J. Virol. 91 (4), e01653–16. doi:10.1128/JVI.01653-16
Zaza, G., Granata, S., Tomei, P., Dalla Gassa, A., and Lupo, A. (2015). Personalization of the Immunosuppressive Treatment in Renal Transplant Recipients: the Great challenge in "omics" Medicine. Int. J. Mol. Sci. 16 (2), 4281–4305. doi:10.3390/ijms16024281
Zaza, G., Granata, S., Tomei, P., Masola, V., Gambaro, G., and Lupo, A. (2014). mTOR Inhibitors and Renal Allograft: Yin and Yang. J. Nephrol. 27 (5), 495–506. doi:10.1007/s40620-014-0103-y
Zhang, H., Chen, Y., Yuan, Q., Xia, Q. X., Zeng, X. P., Peng, J. T., et al. (2020). Identification of Kidney Transplant Recipients with Coronavirus Disease 2019. Eur. Urol. 77 (6), 742–747. doi:10.1016/j.eururo.2020.03.030
Zhang, S., Pruitt, M., Tran, D., Du Bois, W., Zhang, K., Patel, R., et al. (2013). B Cell-specific Deficiencies in mTOR Limit Humoral Immune Responses. J. Immunol. 191 (4), 1692–1703. doi:10.4049/jimmunol.1201767
Zhang, X. L., Xing, R. G., Chen, L., Liu, C. R., and Miao, Z. G. (2016). PI3K/Akt Signaling Is Involved in the Pathogenesis of Bleomycin-induced P-ulmonary F-ibrosis via R-egulation of E-pithelial-mesenchymal T-ransition. Mol. Med. Rep. 14 (6), 5699–5706. doi:10.3892/mmr.2016.5960
Zheng, Y., Li, R., and Liu, S. (2020). Immunoregulation with mTOR Inhibitors to Prevent COVID-19 Severity: A Novel Intervention Strategy beyond Vaccines and Specific Antiviral Medicines. J. Med. Virol. 92 (9), 1495–1500. doi:10.1002/jmv.26009
Keywords: mTOR-inhibitors, COVID-19, pulmonary fibrosis, kidney transplantation, SARS-CoV-2, everolimus, sirolimus
Citation: Granata S, Carratù P, Stallone G and Zaza G (2021) mTOR-Inhibition and COVID-19 in Kidney Transplant Recipients: Focus on Pulmonary Fibrosis. Front. Pharmacol. 12:710543. doi: 10.3389/fphar.2021.710543
Received: 16 May 2021; Accepted: 11 August 2021;
Published: 23 August 2021.
Edited by:
Harry Van Goor, University Medical Center Groningen, NetherlandsReviewed by:
Naoka Murakami, Brigham and Women’s Hospital and Harvard Medical School, United StatesCopyright © 2021 Granata, Carratù, Stallone and Zaza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gianluigi Zaza, Z2lhbmx1aWdpLnphemFAdW5pdnIuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.