 Cameron Mura
Cameron Mura Saskia Preissner
Saskia Preissner Robert Preissner
Robert Preissner Philip E. Bourne
Philip E. Bourne
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Pharmacol. , 11 August 2021
Sec. Drugs Outcomes Research and Policies
Volume 12 - 2021 | https://doi.org/10.3389/fphar.2021.700703
This Perspective examines a recent surge of information regarding the potential benefits of acid-suppression drugs in the context of COVID-19, with a particular eye on the great variability (and, thus, confusion) that has arisen across the reported findings, at least as regards the popular antacid famotidine. The degree of inconsistency and discordance reflects contradictory conclusions from independent, clinical-based studies that took roughly similar approaches, in terms of both experimental design (retrospective, observational, cohort-based, etc.) and statistical analysis workflows (propensity-score matching and stratification into sub-cohorts, etc.). The contradictions and potential confusion have ramifications for clinicians faced with choosing therapeutically optimal courses of intervention: e.g., do any potential benefits of famotidine suggest its use in a particular COVID-19 case? (If so, what administration route, dosage regimen, duration, etc. are likely optimal?) As succinctly put this March in Freedberg et al. (2021), “…several retrospective studies show relationships between famotidine and outcomes in COVID-19 and several do not.” Beyond the pressing issue of possible therapeutic indications, the conflicting data and conclusions related to famotidine must be resolved before its inclusion/integration in ontological and knowledge graph (KG)–based frameworks, which in turn are useful for drug discovery and repurposing. As a broader methodological issue, note that reconciling inconsistencies would bolster the validity of meta-analyses which draw upon the relevant data-sources. And, perhaps most broadly, developing a system for treating inconsistencies would stand to improve the qualities of both 1) real world evidence-based studies (retrospective), on the one hand, and 2) placebo-controlled, randomized multi-center clinical trials (prospective), on the other hand. In other words, a systematic approach to reconciling the two types of studies would inherently improve the quality and utility of each type of study individually.
To begin systematically structuring the rapidly accumulating information on COVID-19 (Triggle et al., 2021)—in the hopes of clarifying and reconciling the discrepancies, and eventually maturing the information into clinically-actionable knowledge and understanding—let us view this topic along three “axes” implied by our opening sentence: namely, we consider 1) a context-of-disease (COD) axis, 2) a degree-of-(therapeutic)-benefit (DOB) axis, and 3) a mechanism-of-action (MOA) axis. We now treat each of these in turn; note that these “axes” are of nominal type, in terms of classification levels and typologies (Stevens, 1946).
The MOA axis may be the most straightforward to conceptualize, as it simply describes the MOA of a putative drug—i.e., the mechanistic, molecular-level etiological basis (to the extent known), in whatever might be the most salient pharmacological pathways for that compound. As a concrete example, known gastroenterological acid-suppression agents may act either: 1) as proton-pump inhibitors (PPIs), sterically occluding proton efflux via the H+/K+-ATPase pumps that mediate the final step of acid release in the gastric mucosa, or 2) as histamine type-2 receptor antagonists (H2RAs), whereby specific binding to this subtype of G-protein coupled receptor blocks the downstream signaling and effector cascades that otherwise would have been triggered by the cognate ligand, i.e., histamine (Eldanasory et al., 2020; Ennis and Tiligada, 2021). An example of a widely used PPI is omeprazole (e.g., Prilosec®), and famotidine (e.g., Pepcid®) and ranitidine (e.g., Zantac®) are examples of popular over-the-counter H2RAs. In the context of our present example, the MOAs of these two particular classes of GI drugs are mutually exclusive—i.e., a drug 𝒟 acts by one pathway 𝒫1 (PPI-blocker) or another 𝒫2 (H2RA), but not both. Such basic, molecular-level selectivity is not always the case, and, indeed, the approach of polypharmacology (Xie et al., 2012) relaxes the rigidity of the “one gene, one disease, one drug” view by recognizing that, in vivo, a given drug compound likely has multiple targets in multiple physiological pathways; indeed, generally speaking the potential multiplicity of drug···target linkages can be leveraged to beneficial effect. Further consideration of “off-target” effects (beneficial or detrimental) is beyond the scope of our present treatment. Here, we only note that a recent study (Malone et al., 2021) offers a detailed and insightful analysis of possible on–/off–target properties of famotidine, particularly as regards 1) hypothesis testing of its MOA, and 2) discrepancies that can arise among different studies because of differences in dosage, single- and multi-agent treatment regimes, pharmacokinetic–related properties (e.g., ADME), and so on; notably, that work concluded that off-target (i.e., non-H2R) pathways likely do not play a major role in the case of famotidine as a potential COVID-19 therapeutic.
One can envision developing more quantitative descriptors of the entities that populate the MOA axis and their interrelationships (to move from our nominal scale towards something more like an ordinal scale) by employing approaches such as the Coronavirus Infectious Disease Ontology (Liu et al., 2021) to represent the targets of 𝒟 in the 𝒫1, 𝒫2, etc. pathways, the possible side-effects, and so on. [Note that CIDO is one of many biomedical ontologies gathered at BioPortal (Whetzel et al., 2011).] A potential source of confusion in the recent famotidine literature, taken in totality, is that recent meta-analyses (Sethia et al., 2020b; Kamal et al., 2021; Sun et al., 2021) of retrospective, observational, cohort-based studies have not always enforced a clean delineation between the two MOAs mentioned above (i.e., PPI, H2RA), at least when drawing their conclusions. As a case in point, some primary studies have found that famotidine is beneficial whereas PPIs offered “no protective effect” (Freedberg et al., 2020a); another study found no positive effect of famotidine and also no deleterious effect of PPIs (Elmunzer et al., 2020); another found no association between PPIs and a different H2RA (ranitidine), in terms of likelihoods of both COVID-19 infection and death (Fan et al., 2021); a pair of studies found no evidence for additional risks or benefits, for neither famotidine nor PPIs (Cheung et al., 2020; Shoaibi et al., 2021); and, finally, another recent study (Zhou et al., 2020) found greater risks of association with morbidity or severe illness for famotidine and PPIs (each one, individually). Such incongruities, viewed holistically across all of the studies, result in internal inconsistencies when meta-analyses then draw upon a set of such studies: there is no clear “combining” rule to harmonize otherwise inconsistent data sources and data values. Also, in some sense, comparing drugs with different MOAs, under the umbrella of a single, global analysis (be it a meta-analysis or a manual/human-expert analysis), is akin to comparing apples and oranges: they are of fundamentally different types, and attempts to compare them are ill-posed in the ontological sense of semantic networks, structured reasoning, KGs, and so forth [reviewed in Kanza and Frey (2019)]. From a pharmacogenomics and drug discovery perspective, a key goal would be the development of ontology-based knowledge representation graphs (or semantic models) of the cellular pathways wherein famotidine might intervene pharmacologically (Figure 1). Such an approach could enable systematic, automated discovery—via reasoning over the graph—of potential new targets, new drug leads, and prediction of new drug/target pairs (using existing software systems and toolkits); however, constructing such a framework would require resolution of inconsistencies among the primary data used to build the semantic network’s relationships (Figure 1A).
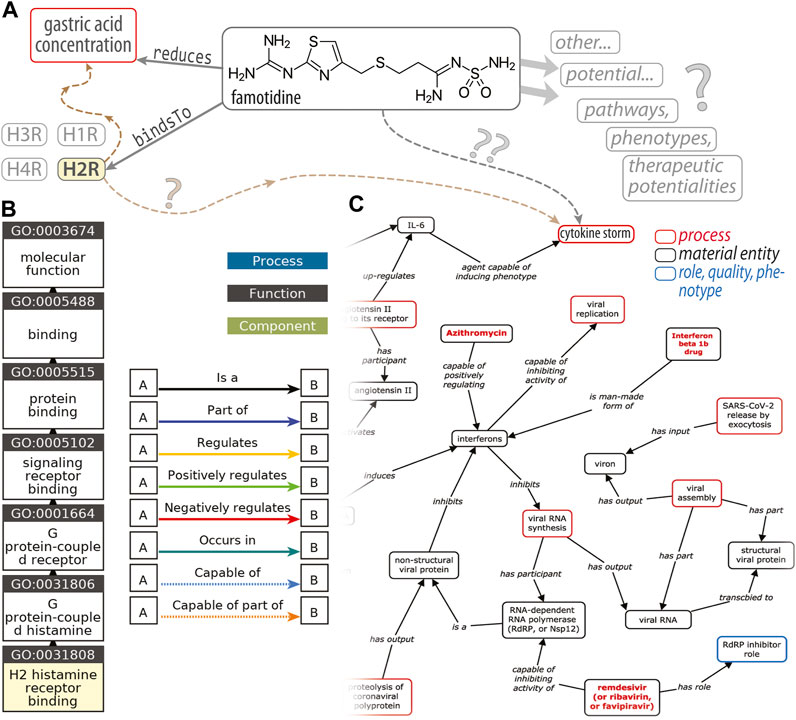
FIGURE 1. An ontological perspective on famotidine and COVID-19. This diagram (A) illustrates the types of RDF triple associations, consisting of a (subject, predicate, object) triplet, that express the relations between entities that underlie an ontology. In this simplified example, one such triple would be (famotidine, bindsTo, H2R) (histamine type-2 receptor) and another is (famotidine, reduces, gastric acid concentration); H1R, H3R and H4R denote other subtypes of histamine receptors. The brown dashed arrows (at left) are placeholders to signify the H2R‐triggered signaling cascades that ultimately modulate gastric acid levels. Question marks (“?”) decorate linkages where our knowledge is either quite tenuous or vague. The GO “ancestor chart”, in (B), illustrates a concept hierarchy for the term GO:0031808, corresponding to a particular molecular function named “H2 histamine receptor binding”; traversing this concept/class hierarchy, from the leaf (bottom) to the root (top; “molecular function”), corresponds to a traversal of successively broader categories of concepts/classes [e.g., the H2R is_a type of (i.e., a subset of) GPCRs]. Panel (C), adapted from Liu et al. (2021), is an excerpt of a KG of host–coronavirus drug/interactions, including at the upper-right a putative link between famotidine and the cytokine storm.
A few studies have begun considering the possible sources of discrepancies and heterogeneities, to which at least some of the inconsistencies in the famotidine/COVID-19 literature can be attributed. Some such sources relate to differences in study designs, or are otherwise methodological in nature—e.g., Freedberg et al.'s (2020b) description of potential biases from residual confounders in the baseline characteristics of case-matched cohorts. There also exists the possibility of spurious links (or, inversely, masked associations) because of underlying physiological factors, e.g., Sethia et al.'s (2020a) description of the impacts of 1) potentially great differences in disease severity on treatment outcomes (without adequately accounting for such in case-matching and stratification methods to obtain sub-cohorts), 2) heterogeneity in classification of the severity of illness, 3) whether these variations are factored into the case-matching and stratification stages, 4) variation in the regimen for famotidine treatment, including administration route (oral, intravenous), dosage levels, timings with respect to onset of disease symptoms and duration of treatment [see also Malone (2021)], and 5) confounding factors from co-medications or comorbidities among patients who do more/less well with famotidine. On a broad, population-wide scale, discrepancies also can stem from latent confounders related to different societal/health systems of countries, distributions of ethnicities, and so on. On a finer scale, some of the sources of differences will be at a more basic (molecular) level, and likely quite difficult to elucidate: for instance, 1) Singh et al. (2020) note that fine-grained details such as the levels of calcium in various famotidine formulations may be “mechanistically relevant to disease outcomes”; and 2) in general, pharmacogenomic factors (Roden et al., 2019) will govern the potential efficacy of famotidine as a therapeutic, and these will vary on an individual, case-by-case basis.
The degree-of-benefit (DOB) axis is relatively easy to conceptualize: For famotidine (or in general any putative drug, 𝒟), this categorical descriptor can be considered as being essentially tripartite: “neutral/no association”, “pro-famotidine”, “anti-famotidine.” The utility of the descriptor for a given drug compound will be specific to disease context—i.e., it would not hold universally across all diseases. A drug 𝒟 may be negatively indicated for a particular ailment or illness ℐ1 (e.g., AIDS) whereas the same drug would be indicated in another illness ℐ2 (e.g., COVID-19). That is to say, symbolically, that the DOB for a given drug in two different disease contexts may be dissimilar,
The context-of-disease (COD) axis accounts for the fact that, in addition to being subjective, the term “beneficial” is also vague: it can be gauged by various types of outcomes/criteria, even for a single disease or given set of indications. In the context of COVID-19 and other infectious diseases, a putative drug may be “beneficial” as regards its impact upon 1) transmissibility, e.g., Fan et al. (2021) considered if usage of the H2RA ranitidine modulates susceptibility to SARS-CoV-2 infection; 2) disease severity indicators, e.g., the likelihood of cases reaching the point of mechanical ventilation, the WHO Severity Index [Yeramaneni et al. (2021) used this ordinal scale in their COVID-19 study], or other measures; and 3) mortality rates, frequencies or related metrics. Unlike the MOA axis the entities along the COD axis can overlap, at least in our current example of COVID-19 and acid-suppressing drugs—for example, there is no a priori reason why a given drug cannot be beneficial in two senses, e.g., by diminishing transmissibility of SARS-CoV-2 and by reducing the severity of the disease trajectory once it has been contracted [note, though, that in general different cellular/molecular-scale pathways (MOAs) can underlie similar organismal-level outcomes].
We suspect that some incongruities in how these MOA, COD and DOB axes have been (implicitly) treated in the various, independent studies is what has led to the contradictory indications regarding famotidine and COVID-19 (anti-famotidine, neutral, pro-famotidine) in the published literature. Harmonizing the findings across the literature is an important goal from the perspectives of both bioinformatics and clinical standards-of-care/best practices for a given disease.
Finally, now to trace the evolution of what we know about the potential benefits (DOB) of H2RAs, PPIs, etc. (different MOAs) on the transmission, severity, and mortality (various CODs) of COVID-19, let us consider the many literature reports that have accumulated in the past year. By grouping these studies conceptually and thematically we can begin to identify the following three “Eras” in the progression of the literature (and our understanding) as regards famotidine and COVID-19:
• Era 1: Primary research studies by independent groups: These ≈10 analyses generally have been retrospective, observational (some cohort-based, some case-series) and single-site/center. Most of the studies attempted to statistically adjust for confounders (e.g., via propensity score matching), though with varying degrees of rigor and caution (see the study cited in Era 3, below). Despite many similarities in design, there have emerged two contradictory sets of studies: 1) several studies concluded in favor of using famotidine in COVID-19 i.e., Freedberg et al. (2020a), Janowitz et al. (2020), Mather et al. (2020) and Hogan et al. (2020), while 2) a roughly equal number did not, i.e., Cheung et al. (2020), Elmunzer et al. (2020), Zhou et al. (2020), Fan et al. (2021) and Yeramaneni et al. (2021). In the second category of reports which were less enthusiastic about famotidine, some did suggest against the usage of famotidine (Cheung et al., 2020; Yeramaneni et al., 2021; Zhou et al., 2020), while others found no association for famotidine or PPIs and COVID-19 therapeutic value (Elmunzer et al. (2020) and Fan et al. (2021)).
• Era 2: Meta-analyses of the primary literature reports: Three such analyses have appeared thus far, with again varying results: Sethia et al. (2020b) were cautiously pro-famotidine, while Sun et al. (2021) and Kamal et al. (2021) were more neutral/negative, determining for the most part that no association (positive or negative) was statistically justifiable. Why the inconsistency in whether or not famotidine is indicated for COVID-19, even at the level of a meta-analysis? One contributing factor could be that different database inclusion criteria were used in these different meta-analyses (cf. Methods sections in each of these three studies). For instance, Sun et al. (2021) drew upon several Chinese databases and did not sample the medRxiv or SSRN preprint collections, whereas Sethia et al. (2020b) included medRix and SSRN but not the several Chinese databases. This could be a source of discrepancy between the meta-analyses. Furthermore, it is perhaps unsurprising that the meta-analysis which did reach a more favorable conclusion as regards indicating famotidine (i.e., Sethia et al.) leaned most heavily on studies from the primary literature which were, themselves, most strongly in favor of famotidine on average (see those cited in Era 1, above); in contrast, the meta-analysis which found no/less-favorable association between famotidine and positive COVID outcomes (i.e., Sun et al.) included a subset of case/cohort-studies that generally reached less favorable conclusions [e.g., Cheung et al. (2020); Shoaibi et al. (2021); Yeramaneni et al. (2021)]. The third meta-analysis, of Kamal et al. (2021), does not serve as a “tie-breaker” here, as it finds a “lack of consistent association” between COVID-19 outcomes and the use of acid-suppression drugs (for both famotidine and PPIs). Finally, as can generally occur in bibliometric meta-analyses, a “positive-outcome” publication bias (Fanelli, 2012) may exist in the data sources, with negative findings never having made it to the primary, peer-reviewed literature.
• Era 3: Origins of the discrepancies? Without resorting to a meta-meta-analysis(!), Etminan et al. (2020) recently supplied a thorough and incisive critique of factors that may limit the consistency of the conclusions drawn thus far from the primarily retrospective, observational, single-site studies, such as those in Elmunzer et al. (2020), Freedberg et al. (2020a) and Mather et al. (2020). In particular, likely sources were identified for several types of biases, including residual confounding bias and sparse-data bias, immortal time bias (and somewhat related selection bias effects), and reverse causality bias [the latter can be understood via causal directed acyclic graph (cDAG) models, which can elucidate the structure of these epidemiological biases]. Here, we simple note that: 1) Some of these sources of bias are rather more difficult to control for, or statistically identify and account for, than others (because of causal relationships, limited data, etc.); 2) In principle, biases, in and of themselves, do not necessarily result in inconsistencies among a series of primary research studies. That is, bias and inconsistency are not equivalent phenomena: conceivably, each study within a series of studies could suffer from similar biases, and nevertheless still be self-consistent. Regardless, Etminan et al. highlight several improvements that can be made in future approaches to statistically elucidate famotidine ↔ COVID-19 relationships.
Perhaps some inconsistencies can be resolved by viewing famotidine and its potential roles in COVID-19 through a more mechanistic, molecular-level lens? Alongside the observational, patient-based studies, the potential MOA for a therapeutic role of famotidine has been explored in a few publications. In particular, a recent review by Ennis and Tiligada (2021) offers a cogent and authoritative treatment of the connection between histamine receptor antagonists (e.g., famotidine) and COVID-19, while histamine release theory was also the subject of accounts by Eldanasory et al. (2020) and Ghosh et al. (2020) regarding the role of this versatile signaling molecule in pro-inflammatory pathways—including the destructive “cytokine storm” that appears to underlie much of the pathophysiology of COVID-19, at least with respect to pulmonary consequences (fibrosis, etc.) and the resultant acute respiratory distress. More generally, famotidine and other GI-related drugs appear in a comprehensive review by Tarighi et al. (2021) of drug repurposing in the age of COVID, and a recent letter by Singh et al. (2020) considered the question of what (molecularly) underlies the efficacy of treatment of COVID with famotidine? These mechanistic, biomolecular directions offer hope, as it is often the case that multiple disparate (and seemingly contradictory) phenomena, or sets of observations, at a macroscopic/organismal level become reconciled when viewed at the molecular level—i.e., by appealing to the underlying cellular and physiological pathways. Indeed, we suspect that the reconciliation and harmonization of independent, contradictory findings, such as for famotidine and COVID-19, ultimately will lie along two paths: 1) molecular-level examination of whatever pathways are thought to be most salient for the macroscopic phenomena of interest (clinical-level observations), and 2) multi-scale, integrative modeling of the interaction and build-up of microscopic phenomena (e.g., drug-protein interactions) through many hierarchical levels (organellar ↣ subcellular ↣ cellular ↣ tissues ↣ ···) up through to the organismal level, and eventually even populations (therapeutic outcomes, like altering the course of an infection).
A key motivation for reconciling conflicts in the famotidine × COVID-19 literature, in terms of basic drug discovery/repurposing and modeling COVID-19-drug interactions, stems from the importance of data consistency and harmonization in creating ontology-based knowledge graphs of biomolecular systems. Figure 1 schematizes the types of Resource Description Framework (RDF) “triples” used to express the relationships between distinct entities in an ontology [Andronis et al. (2011), Blake (2013), and Hastings (2017) offer introductions/primers on ontologies]. The example in Figure 1 also denotes other histamine receptors (H1R, H3R, H4R) in order to emphasize that any given pairwise relationship does not exist in isolation: all simpler relationships are embedded within physiological contexts that typically involve many entities (with varying degrees of confidence in the linkages). While RDF triples capture relationships between entities, the other aspect of an ontology is a higher-level structuring or organization (typically hierarchical) for the collection of classes/concepts (of which a given entity is an instance) that span the ontology’s domain of knowledge. A gene ontology [GO; Ashburner et al. (2000)] “ancestor chart”, shown in Figure 1B, illustrates such a concept hierarchy for the term GO:0031808, corresponding to H2R-binding. The excerpt of a host···coronavirus drug/interactions map (Figure 1C) is a graph-based representation that reflects both aforementioned aspects of an ontology, namely 1) the structural interrelationships among concepts/entities (some broad, some specific, some subsets of others, etc.) as well as 2) the pairwise associations (RDF triples) from which such KGs are built. These “semantic network” approaches are compelling and powerful for many reasons [reviewed in Andronis et al. (2011) and Kanza and Frey (2019)], including that the KG can be used for drug discovery, pharmacogenomics modeling, and “big data” endeavors (data integration across scales); one manner in which this is achieved is by “reasoning” over the KG, beyond the initial confines (or domain) of the data sources. The success of all such efforts rests upon the data being systematized against a controlled vocabulary, syntactically well-formed, and so on. A key determinant of our ability to build such graphs is that there not be internal inconsistencies, such as “✓
Together with the findings from several sets of prospective clinical trials that have been underway—including NCT04504240, NCT04370262 and NCT04545008 in the United States, and other efforts internationally [e.g., Samimagham et al. (2020)]—we anticipate that detailed biomolecular studies can help clarify the contradictory relationships that have been reported thus far between famotidine and COVID-19. That, in turn, will enable the creation of more robust, efficacious and predictive ontological frameworks for drug discovery and pharmacological repurposing.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Conception and design: CM Acquisition, analysis and interpretation of data: CM, SP, RP, and PB Drafting of the manuscript: CM, SP, RP, and PB Supervision: RP and PB Critical revision of the manuscript: CM, SP, RP, and PB Final approval: all authors.
This work was supported by TRR295, KFO339, and DFG PR1562/1-1 (RP). Portions of this work were also supported by the University of Virginia School of Data Science and by NSF CAREER award MCB-1350957.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank RW Malone for bringing to our attention some studies from the literature, particularly as regards the potential mechanisms of action of famotidine.
COD, context of disease; COVID-19, coronavirus disease 2019; DOB, degree of benefit; GPCR, G-protein coupled receptor; KG, knowledge graph; MOA, mechanism/mode of action; RDF, resource description framework; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Aguila, E. J. T., and Cua, I. H. Y. (2020). Repurposed GI Drugs in the Treatment of COVID-19. Dig. Dis. Sci. 65, 2452–2453. doi:10.1007/s10620-020-06430-z
Andronis, C., Sharma, A., Virvilis, V., Deftereos, S., and Persidis, A. (2011). Literature mining, ontologies and information visualization for drug repurposing. Brief. Bioinform. 12, 357–368. doi:10.1093/bib/bbr005
Ashburner, M., Ball, C. A., Blake, J. A., Botstein, D., Butler, H., Cherry, J. M., et al. (2000). Gene Ontology: tool for the unification of biology. Nat. Genet. 25, 25–29. doi:10.1038/75556
Blake, J. A. (2013). Ten quick tips for using the gene ontology. PLoS Comput. Biol. 9, e1003343. doi:10.1371/journal.pcbi.1003343
Cheung, K. S., Hung, I. F., and Leung, W. K. (2020). Association between famotidine use and COVID-19 severity in Hong Kong: a territory-wide study. Gastroenterology 160 (5), 1898–1899. doi:10.12809/hkmj208507
Eldanasory, O. A., Eljaaly, K., Memish, Z. A., and Al-Tawfiq, J. A. (2020). Histamine release theory and roles of antihistamine in the treatment of cytokines storm of COVID-19. Trav. Med. Infect. Dis. 37, 101874. doi:10.1016/j.tmaid.2020.101874
Elmunzer, B. J., Wolf, B. J., Scheiman, J. M., Tierney, W. M., and Taylor, J. R. (2020). Association between Preadmission Acid Suppressive Medication Exposure and Severity of Illness in Patients Hospitalized with COVID-19. Gastroenterology 160 (4), 1417–1422.
Ennis, M., and Tiligada, K. (2021). Histamine receptors and COVID-19. Inflamm. Res. 70, 67–75. doi:10.1007/s00011-020-01422-1
Etminan, M., Nazemipour, M., Sodhi, M., and Mansournia, M. A. (2020). Potential Biases in Studies of Acid Suppressing Drugs and COVID-19 Infection. Gastroenterology 160 (5), 1443–1446.
Fan, X., Liu, Z., Miyata, T., Dasarathy, S., Rotroff, D. M., Wu, X., et al. (2021). Effect of Acid Suppressants on the Risk of COVID-19: A Propensity Score-Matched Study Using UK Biobank. Gastroenterology 160, 455–458. doi:10.1053/j.gastro.2020.09.028
Fanelli, D. (2012). Negative results are disappearing from most disciplines and countries. Scientometrics 90, 891–904. doi:10.1007/s11192-011-0494-7
Freedberg, D. E., Wang, T. C., and Abrams, J. A. (2020b). Famotidine and COVID-19. Gastroenterology 161 (1), 360–361.
Freedberg, D. E., Wang, T. C., and Abrams, J. A. (2021). Famotidine and COVID-19: Author Reply. Gastroenterology 160 (5), 1900–1901.
Freedberg, D. E., Conigliaro, J., Wang, T. C., Tracey, K. J., Callahan, M. V., Abrams, J. A., et al. (2020a). Famotidine Use Is Associated with Improved Clinical Outcomes in Hospitalized COVID-19 Patients: A Propensity Score Matched Retrospective Cohort Study. Gastroenterology 159, 1129–1131. e1123. doi:10.1053/j.gastro.2020.05.053
Gallo, K., Goede, A., Eckert, A., Moahamed, B., Preissner, R., and Gohlke, B.-O. (2021). PROMISCUOUS 2.0: a resource for drug-repositioning. Nucleic Acids Res. 49, D1373–D1380. doi:10.1093/nar/gkaa1061
Ghosh, R., Chatterjee, S., Dubey, S., and Lavie, C. J. (2020). Famotidine against SARS-CoV2: A Hope or Hype? Mayo Clinic Proc. 95, 1797–1799. doi:10.1016/j.mayocp.2020.05.027
Hastings, J. (2017). Primer on Ontologies. Methods Mol. Biol. 1446, 3–13. doi:10.1007/978-1-4939-3743-1_1
Hogan Ii, R. B., Hogan III, R. B., Cannon, T., Rappai, M., Studdard, J., Paul, D., et al. (2020). Dual-histamine receptor blockade with cetirizine - famotidine reduces pulmonary symptoms in COVID-19 patients. Pulm. Pharmacol. Ther. 63, 101942. doi:10.1016/j.pupt.2020.101942
Janowitz, T., Gablenz, E., Pattinson, D., Wang, T. C., Conigliaro, J., Tracey, K., et al. (2020). Famotidine use and quantitative symptom tracking for COVID-19 in non-hospitalised patients: a case series. Gut 69, 1592–1597. doi:10.1136/gutjnl-2020-321852
Kamal, F., Khan, M. A., Sharma, S., Imam, Z., and Howden, C. W. (2021). Lack of consistent associations between pharmacological gastric acid suppression and adverse outcomes in patients with COVID-19: meta-analysis of observational studies. Gastroenterology 160(7), 2588–2590.
Kanza, S., and Frey, J. G. (2019). A new wave of innovation in Semantic web tools for drug discovery. Expert Opin. Drug Discov. 14, 433–444. doi:10.1080/17460441.2019.1586880
Liu, Y., Hur, J., Chan, W. K. B., Wang, Z., Xie, J., Sun, D., et al. (2021). Ontological modeling and analysis of experimentally or clinically verified drugs against coronavirus infection. Scientific Data 8, 16. doi:10.1038/s41597-021-00799-w
Malone, R. W. (2021). More than Just Heartburn: Does Famotidine Effectively Treat Patients with COVID-19? Dig. Dis. Sci. doi:10.1007/s10620-021-06875-w
Malone, R. W., Tisdall, P., Fremont-Smith, P., Liu, Y., Huang, X. P., White, K. M., et al. (2021). COVID-19: Famotidine, Histamine, Mast Cells, and Mechanisms. Front. Pharmacol. 12, 633680. doi:10.3389/fphar.2021.633680
Mather, J. F., Seip, R. L., and Mckay, R. G. (2020). Impact of Famotidine Use on Clinical Outcomes of Hospitalized Patients with COVID-19. Am. J. Gastroenterol. 115, 1617–1623. doi:10.14309/ajg.0000000000000832
Roden, D. M., Mcleod, H. L., Relling, M. V., Williams, M. S., Mensah, G. A., Peterson, J. F., et al. (2019). Pharmacogenomics. The Lancet 394, 521–532. doi:10.1016/s0140-6736(19)31276-0
Samimagham, H. R., Hassani Azad, M., Haddad, M., Arabi, M., Hooshyar, D., and Kazemijahromi, M. (2020). The Efficacy of Famotidine in improvement of outcomes in Hospitalized COVID-19 Patients: A structured summary of a study protocol for a randomised controlled trial. Trials 21, 848. doi:10.1186/s13063-020-04773-6
Sasaki, T., Yamaya, M., Yasuda, H., Inoue, D., Yamada, M., Kubo, H., et al. (2005). The proton pump inhibitor lansoprazole inhibits rhinovirus infection in cultured human tracheal epithelial cells. Eur. J. Pharmacol. 509, 201–210. doi:10.1016/j.ejphar.2004.12.042
Sethia, R., Prasad, M., and Garg, P. K. (2020a). Letter to the editor: Famotidine and mortality in COVID-19. Gastroenterology.
Sethia, R., Prasad, M., Mahapatra, S. J., Nischal, N., Soneja, M., Garg, P., et al. (2020b). Efficacy of Famotidine for COVID-19: A Systematic Review and Meta-Analysis. medRxiv. doi:10.1101/2020.09.28.20203463
Shoaibi, A., Fortin, S. P., Weinstein, R., Berlin, J. A., and Ryan, P. (2021). Comparative Effectiveness of Famotidine in Hospitalized COVID-19 Patients. Am. J. Gastroenterol. 116 (4), 692–699.
Singh, V. P., El-Kurdi, B., and Rood, C. (2020). What underlies the benefit of famotidine formulations used during COVID-19? Gastroenterology.
Stevens, S. S. (1946). On the Theory of Scales of Measurement. Science 103, 677–680. doi:10.1126/science.103.2684.677
Sun, C., Chen, Y., Hu, L., Wu, Y., Liang, M., Ayaz Ahmed, M., et al. (2021). Does Famotidine Reduce the Risk of Progression to Severe Disease, Death, and Intubation for COVID-19 Patients? A Systemic Review and Meta-Analysis. Dig. Dis. Sci., 1–9. doi:10.1007/s10620-021-06872-z
Tarighi, P., Eftekhari, S., Chizari, M., Sabernavaei, M., Jafari, D., and Mirzabeigi, P. (2021). A review of potential suggested drugs for coronavirus disease (COVID-19) treatment. Eur. J. Pharmacol. 895, 173890. doi:10.1016/j.ejphar.2021.173890
Triggle, C. R., Bansal, D., Ding, H., Islam, M. M., Farag, E., Hadi, H. A., et al. (2021). A Comprehensive Review of Viral Characteristics, Transmission, Pathophysiology, Immune Response, and Management of SARS-CoV-2 and COVID-19 as a Basis for Controlling the Pandemic. Front. Immunol. 12, 631139. doi:10.3389/fimmu.2021.631139
Whetzel, P. L., Noy, N. F., Shah, N. H., Alexander, P. R., Nyulas, C., Tudorache, T., et al. (2011). BioPortal: enhanced functionality via new Web services from the National Center for Biomedical Ontology to access and use ontologies in software applications. Nucleic Acids Res. 39, W541–W545. doi:10.1093/nar/gkr469
Xie, L., Xie, L., Kinnings, S. L., and Bourne, P. E. (2012). Novel computational approaches to polypharmacology as a means to define responses to individual drugs. Annu. Rev. Pharmacol. Toxicol. 52, 361–379. doi:10.1146/annurev-pharmtox-010611-134630
Yeramaneni, S., Doshi, P., Sands, K., Cooper, M., Kurbegov, D., and Fromell, G. (2021). Famotidine Use Is Not Associated with 30-day Mortality: A Coarsened Exact Match Study in 7158 Hospitalized Patients with Coronavirus Disease 2019 from a Large Healthcare System. Gastroenterology 160, 919–921. doi:10.1053/j.gastro.2020.10.011
Keywords: COVID-19, histamine (H2) receptor, famotidine, knowledge graph, disease ontology, antagonist action
Citation: Mura C, Preissner S, Preissner R and Bourne PE (2021) A Birds-Eye (Re)View of Acid-Suppression Drugs, COVID-19, and the Highly Variable Literature. Front. Pharmacol. 12:700703. doi: 10.3389/fphar.2021.700703
Received: 26 April 2021; Accepted: 26 July 2021;
Published: 11 August 2021.
Edited by:
Michael Thiede, IUBH University of Applied Sciences, GermanyReviewed by:
Kurt Neumann, Independent researcher, Kerékteleki, HungaryCopyright © 2021 Mura, Preissner, Preissner and Bourne. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Robert Preissner, cm9iZXJ0LnByZWlzc25lckBjaGFyaXRlLmRl; Philip E. Bourne, cGViNmFAdmlyZ2luaWEuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.