
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol. , 05 August 2021
Sec. Drugs Outcomes Research and Policies
Volume 12 - 2021 | https://doi.org/10.3389/fphar.2021.691606
 Zhe Chen1,2,3,4†
Zhe Chen1,2,3,4† Siyu Li1,2,3,5†
Siyu Li1,2,3,5† Linan Zeng1,2,3Yan Liu1,2,3,4Miao Zhang1,2,3Imti Choonara6Lingli Zhang1,2,3*
Linan Zeng1,2,3Yan Liu1,2,3,4Miao Zhang1,2,3Imti Choonara6Lingli Zhang1,2,3*Background: Accessibility of medicines for children is a matter of global concern. Medicines prescribed for children are often off-label. To formulate appropriate policies and undertake necessary interventions to improve access to medicines for children, it is necessary to evaluate the accessibility of medicines for children. However, there is no systematic review of the medicine accessibility for children.
Methods: Relevant studies were identified through searching Pubmed, Embase, CNKI, Wanfang, VIP, World Health Organization website, and Health Action International website. Besides, the references of included studies as a supplementary search were read. We extracted the basic information of articles (the first author, published year, the name of journal, research institution, etc.), the basic study characteristics (survey area, survey time, survey method, survey medicine lists, the number of medicine outlets surveyed, etc.), and the study results (the current situation of the accessibility of medicines for children, including the availability, price, and affordability of medicines for children, etc.). Two reviewers independently selected studies and extracted the data. Descriptive analysis methods to analyze the current situation of the accessibility of children’s medicines were used.
Results: A total of 18 multicenter cross-sectional studies were included in this systematic review, which were from low-income and middle-income countries. Seventeen studies (17/18, 94.4%) used the WHO/Health Action International (HAI) medicine price methodology to investigate the accessibility of medicines for children. Fifteen studies (15/18, 83.3%) were selected to investigate medicines based on the WHO Model List of Essential Medicines for Children (WHO EMLc). In the public sectors, the availability of originator brands (OBs) ranged from 0 to 52.0%, with a median of 24.2%, and the availability of lowest-priced generics (LPGs) ranged from 17.0 to 72.6%, with a median of 38.1%. In the private sectors, the availability of OBs ranged from 8.9 to 80%, with a median of 21.2%. The availability of LPGs ranged from 20.6 to 72.2%, with a median of 35.9%. In most regions, the availability of OBs in the private sectors was higher than in the public sectors. Collectively, in the price of medicines for children, the median price ratio (MPR) of the OBs in the public sectors and private sectors were much higher than that of the LPGs. And the affordability of the LPGs in the public sectors and private sectors was higher than that of originator brands (OBs).
Conclusion: The availability of medicines for children is low in both the public sectors and private sectors in low-income and middle-income countries. The MPR of originator brands (OBs) is higher than that of lowest-priced generics (LPGs), and the most lowest-priced generics (LPGs) have better affordability.
In 2019, an estimated 5.2 million children under 5 years old died mostly from preventable and treatable causes. The leading causes of death in children under 5 years of age are preterm birth complications, birth asphyxia/trauma, pneumonia, congenital anomalies, diarrhea, and malaria. However, more than half of deaths associated with the potential complications can be prevented or treated with access to medicine treatment (World Health Organization, 2020). Unfortunately, the availability of medicines for children is low.
Nonavailability of child-size medicines encourages the use of adult dosage forms, splitting them into parts before giving them to a child. This practice is not scientific and is far from rational since children are not just miniature adults. Their anatomical and physiological characteristics are very different from those of adults. To extremely avoiding the risks of medicines use in children, medicines used by children should suit a children’s size, age, physiologic condition, and treatment requirements (Zhang et al., 2013; Ivanovska et al., 2014; Batchelor and Marriott, 2015; Zhang et al., 2017). To satisfy children’s basic medicine needs, WHO has published seven editions of the WHO Model List of Essential Medicines for Children (EMLc) (World Health Organization, 2019a) from October 2007 to July 2019. Besides, in 2009, the WHO launched the “Better Medicines for Children” initiative and “Make Medicines Child Size” campaign to enhance the accessibility of safe, effective, and quality medicines for children by promoting awareness and action through research, regulatory measures, and policy changes (Finney, 2019).
So far, a large number of researchers around the world have conducted a series of studies to evaluate the accessibility of medicines, and most of the studies have adapted the WHO/HAI standardized methodology. According to the data recorded by the WHO website, as of 2019, 76 studies from 55 countries world-wide have been conveyed by using the WHO/HAI standardized methodology (World Health Organization, 2019b). Among them, seven studies have evaluated the accessibility of medicines on essential medicines for children, and the results demonstrated that the overall availability of medicines for children was low (World Health Organization, 2019a).
To improve access to medicines for children, it is necessary to evaluate the accessibility of medicines for children. However, there is no systematic review of the medicine accessibility for children. Therefore, this review aims to systematically evaluate the current situation of children’s medicines accessibility globally and provide evidence for relevant organizations to formulate appropriate policies and undertake necessary interventions to improve medicine accessibility for children.
Data sourced from Pubmed, Embase, CNKI, Wanfang, VIP, World Health Organization website, and Health Action International website were collected. References of the included studies were also searched for a supplementary study. The search strategy was adjusted specifically for each database and included a combination of medical subject headings and free text terms for (“child*” or “pediatri*”) and (“medicine*” or “drug*” or “medication*”) and (“access*” or “availab*” or “afford*” or “price*”). The deadline for all retrieval was January 2021.
The following studies were included: 1) Participants: children (0–18 years), which were classified according to the International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use Criteria (ICH, 2000). 2) Intervention: medicines for children. 3) Outcomes: the current situation of children’s medicines accessibility, including availability, price, or affordability. 4) Type of study: no limit.
The following studies were excluded: 1) non-Chinese and non-English literature, 2) editorials, reviews, conference abstracts, and any unobtainable full-texts, 3) only investigated the availability of a single medicine or medicine dosage form.
Combie scale (CROMBIE I, 1996) to evaluate the risk of bias in included studies were used from the following seven aspects: 1) the design was scientific; 2) the data collection strategy was reasonable; 3) the sample response rate was reported; 4) the sample was representative of the population; 5) the study purpose and method were reasonable; 6) the test power was reported; 7) the statistical method was reasonable. Combie scale categorized each item with “yes,” “no” and “unclear,” and gave them “1,” “0” and “0.5” points. If an item was not suitable for a study, it would be expressed as “-” and one point was recorded. The total score of this scale was 7.0 points, 6.0–7.0 was A-level (the quality of a study is high), 4.0–5.5 was B-level (the quality of a study is medium), and less than 4.0 was C-level (the quality of a study is low). Two researchers assessed the risk of bias independently, and their disputes reached an agreement by discussing, or deciding by another researcher.
Two independent reviewers screened all the titles and abstracts to determine potential eligible studies. They independently applied the eligibility criteria to perform the final selection. When discrepancies occurred between both reviewers, they would discuss and identify the reasons to either include or exclude the studies and then make the final decision. If they could not reach an agreement, the final decision would be based on a third reviewer. Two reviewers independently extracted data from included studies and cross-checked them. The extracted data included: 1) the basic information of articles (the first author, published year, the name of the published journal, research institution, etc.); 2) the basic study characteristics (survey area, survey time, research method, survey medicine lists, the number of medicine outlets surveyed, etc.); 3) the study results (the current situation of the accessibility of medicines for children, including the availability, price, and affordability of medicines for children, etc.).
We used descriptive analysis methods to analyze the current situation of accessibility of children’s medicines. For studies that directly reported the availability, price, and affordability of children’s medicines in general, we extracted relevant data. For other studies that only reported the original data of a single medicine, we made corresponding calculations based on the original data provided. Since the percentage of the medicine availability and the price of medicines do not follow a normal distribution, we used the median and quartile range to represent them.
For initial screening, 4,732 records were identified. After removing duplicates and irrelevant records by screening for titles and abstracts, 79 studies were assessed for eligibility at full-text screening. Eventually, a total of 18 studies were enrolled in this systematic review (Figure 1).
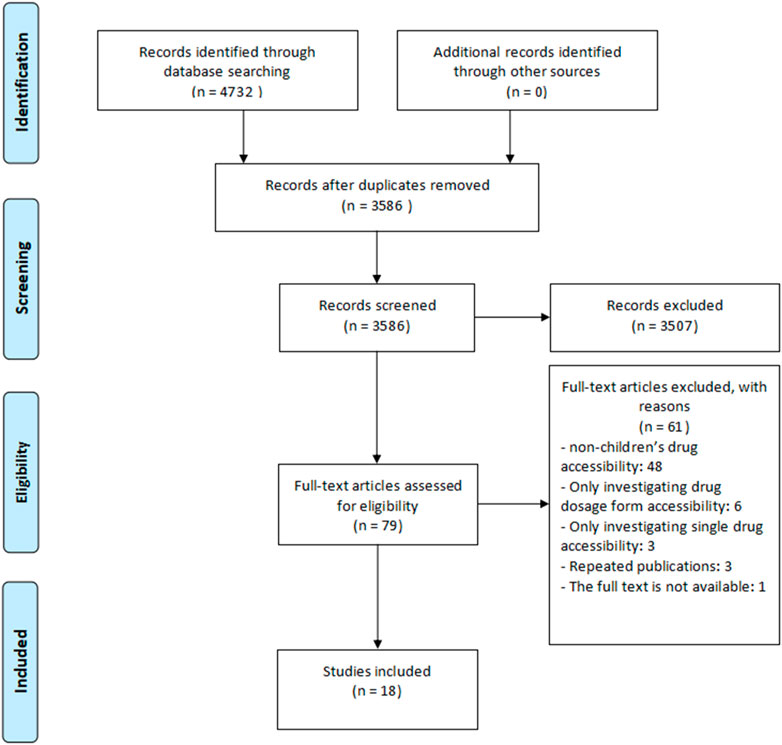
FIGURE 1. Flow diagram of the study selection process.
The 18 included studies were all multicenter cross-sectional surveys and were conducted from 2009 to 2019 (Balasubramaniam et al., 2011; Anson et al., 2012; Ravindran et al., 2012; Balasubramaniam et al., 2014; Nsabagasani et al., 2015; Swain et al., 2015; Sado and Sufa, 2016; Xiao et al., 2017; Abrha et al., 2018; Gereltuya et al., 2018; Saisai et al., 2018; Sun et al., 2018; Guoxu et al., 2019; Neha et al., 2019; Orubu et al., 2019; Demerew and Ahmed, 2020; Xiao et al., 2020; Yi et al., 2020). All studies were conducted in low-income and middle-income countries, including China (6/18), India (3/18), Ethiopia (3/18), Sri Lanka (2/18), Uganda (1/18), Nigeria (1/18), Mongolia (1/18), Guatemala (1/18). Among them, 17 studies (17/18, 94.4%) used the WHO/Health Action International (HAI) medicine price methodology to investigate the accessibility of medicines for children. The WHO/HAI standardized methodology (World Health Organization and Health Action International, 2008) was a research method jointly developed by WHO and HAI in 2000 to standardize studies on the accessibility of medicines. The WHO/HAI standardized methodology was often used for evaluating the accessibility of medicines including medicine availability, price, and affordability. Only one study conducted a cross-sectional survey using a self-formulating questionnaire and its methods to the selecting investigated areas and medicine outlets were not following WHO/HAI standardized methodology. In addition, 15 studies (15/18, 83.3%) selected medicines based on the WHO Model List of Essential Medicines for Children (WHO EMLc). The remaining three studies focused on the WHO recommended priority life-saving medicines for children under five (Nsabagasani et al., 2015; Abrha et al., 2018; Demerew and Ahmed, 2020) (Table 1).
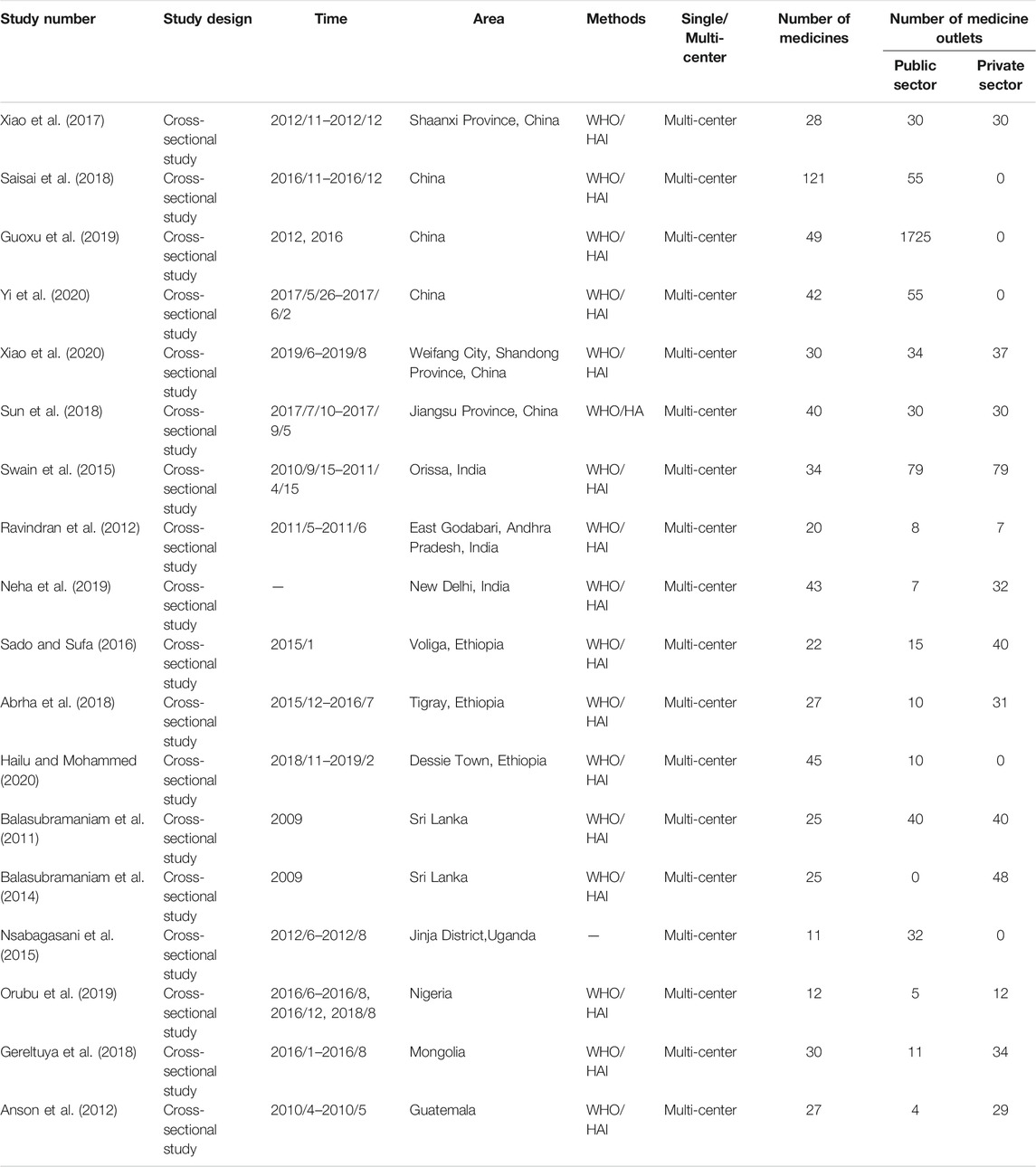
TABLE 1. Basic characteristics of included studies.
The score range of included studies was 5.5–7. Among 18 studies, 17 studies (94.4%, 17/18) were evaluated as high quality, and one study (5.6%, 1/18) was evaluated as medium quality. Four studies (22.2%, 4/18) were considered as unwell-represented samples. The sixth item (Reported the power of test) of the Crombie Scale was not suitable for these included studies, because all these studies were only descriptive statistics (Table 2).

TABLE 2. The quality of included studies.
Fourteen studies reported the availability of medicines for children. The availability of medicines was calculated as the percentage (%) of the surveyed outlets where the medicines were found on the day of data collection. In general, as the percentage was less than 30%, it means the availability of medicines was very low; 30–49%, low availability; 50–80%, high availability; >80%, very high availability.
In the public sectors, the availability of OBs ranged from 0 to 52.0% with a median of 24.2%, and the availability of LPGs ranged from 17.0 to 72.6% with a median of 38.1%. In the private sectors, the availability of OBs ranged from 8.9 to 80.0% with a median of 21.2%. The availability of LPGs ranged from 20.6 to 72.2% with a median of 35.9%. In most regions, the availability of OBs in the private sectors was higher than in the public sectors (Table 3).
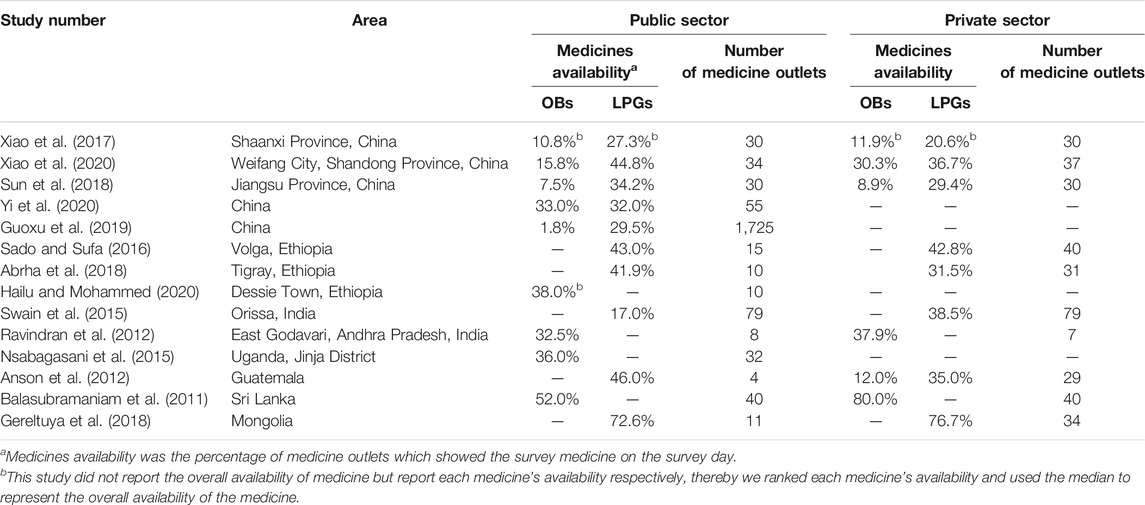
TABLE 3. Availability of medicines for children.
Twelve studies reported the price of medicines for children, which were evaluated by the MPR. The MPR was the ratio of the median unit (each tablet, capsule, milliliter, press, etc.) price of a medicine to the International Reference Price (IRP) (Management Sciences for Health, 2015). If MPR <1, it means that the price of the medicine in the survey area was lower than the IRP; if MPR >1, it means that the price of the medicine was higher than the IRP. The IRP of medicines comes from the Guidelines for International Medicine Price Indicator Guide issued by the Management Sciences for Health (MSH) and is updated regularly. If the retail price of medicines in the public sectors does not exceed 1.5 times the IRP, MPR <1.5, or the retail price of medicines in the private sectors does not exceed 2 times IRP, MPR <2, the prices are considered reasonable (Abrha et al., 2018; Sun et al., 2018; Demerew and Ahmed, 2020; Xiao et al., 2020; Yi et al., 2020).
The results showed that the MPR of the OBs in the public sectors and the private sectors was much higher than that of the LPGs. The MPR of the OBs in the public sectors was 5.43 (1.80–25.92) (median (25th percentile of MPR, 75th percentile of MPR)), and in the private sectors was 3.80 (1.00–8.22). The MPR of the LPGs in the public sectors was 1.77 (0.56–7.00), and in the private sectors was 1.54 (0.71–13.10). Meanwhile, the percentages of the OBs and the LPGs in the public sectors with MPR>1.5 were 91.2%, 41.5%, and the percentages of the OBs and the LPGs in the private sectors with MPR>2.0 were 86.5%, 50.3% (Table 4).
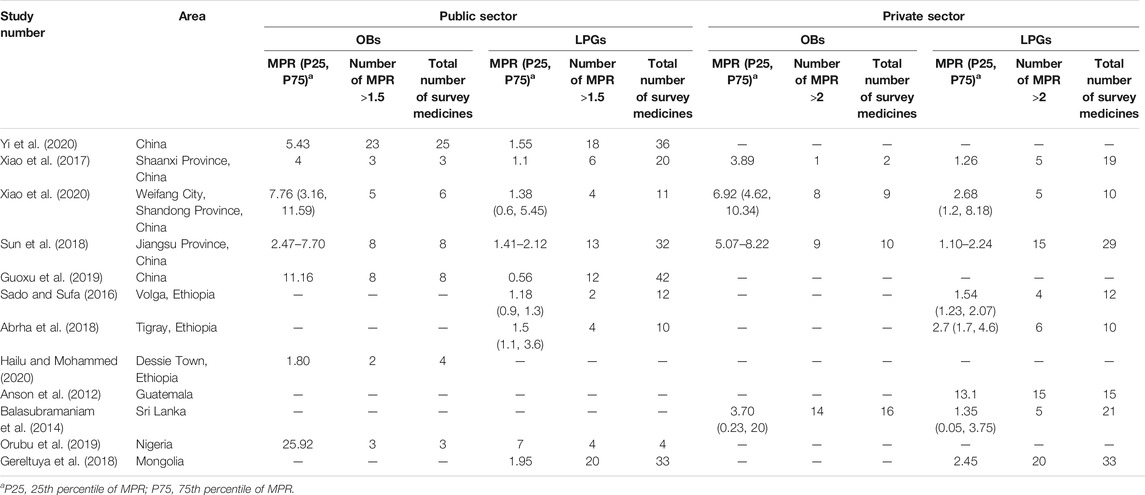
TABLE 4. Prices of medicines for children.
Eleven studies reported the affordability of medicines for children. The affordability was estimated by using median local prices and the average salary of the lowest-paid unskilled government employee. It was defined as “number of days” wages of a lowest-paid unskilled government worker cost on standard medicine therapy. Following the international standard treatment guidelines, the cost of standard doses medicines to treat a certain disease (a chronic disease in 1 month) was calculated (World Health Organization, 2010). The ratio less than one represented the cost of the medicine less than the minimum wage for 1 day, thus, the medicine was considered affordable. For each medicine, data were collected for both OB. OB was defined as the product that is first authorized worldwide for marketing, and the LPG equivalent was found at each medicine outlet (Cameron et al., 2009).
The results showed that in the public sectors, the percentages of affordable medicines for the OBs and the LPGs were 48.5% (16/33) and 83.6% (97/116), and in the private sectors were 68.8% (11/16) and 72.2% (52/72). The affordability of LPGs in the public sectors and the private sectors was higher than that of OBs. It is notably indicating that the affordability of LPGs was better in most regions, while the costs of OBs were higher, which cost a day wage or more than a day wage (Table 5).
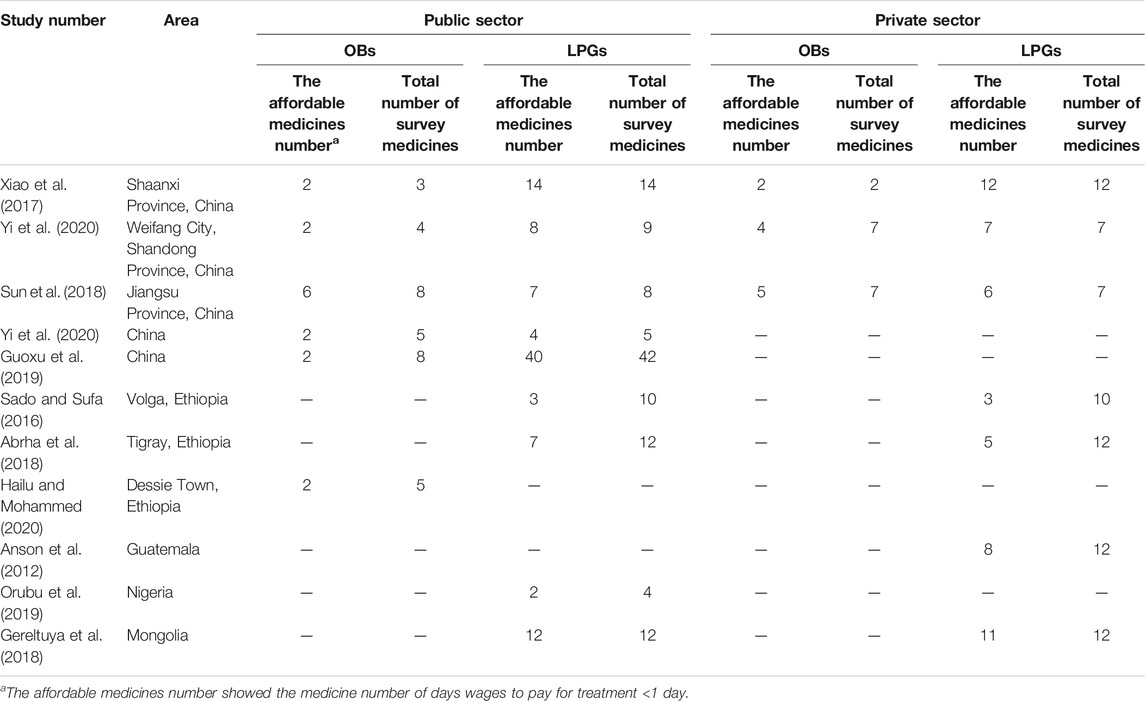
TABLE 5. Affordability of medicines for children.
There were 18 studies included in this systematic review. Fifteen studies (15/18, 83.3%) selected medicines based on a core medicines list from the WHO EMLc and a supplementary medicines list from the National Essential Medicines List (NEML). These medicines were selected to represent a series of treatments for commonly acute and chronic conditions that cause substantial morbidity and mortality. In global, regional, and national treatment guidelines, the selected medicines were recommended as first-line options of treatment available for standard formulations and widely used in many countries or regions (The lists of medicines in each survey for children were presented in Supplementary Appendix I).
Seventeen studies (17/18, 94.4%) used the WHO/Health Action International (HAI) medicine price methodology. Before the WHO/HAI standardized methodology was developed, only a few small studies have been investigated in low-income and middle-income countries to assess medicine prices and generate international comparisons. The lack of consistent or reproducible methodologies limits the comparability of these studies’ results and contributes to the vulnerability in criticism (Andersson, 1993). Therefore, a resolution endorsed by the Member States of the WHO developed a standardized method for measuring medicine prices promoting the launch of the WHO/Health Action International (HAI) Project on Medicine Prices and Availability. The WHO/HAI standardized methodology has allowed for the survey of medicine prices and availability in a standardized way, with multiple steps to ensure data quality (such as clearly stipulating how to identify survey areas and survey medicine outlets, select survey medicines, collect and analyze data, etc.). The common list of 30 core medicines with specified dosage forms and strengths allows for more reliable international comparisons and supplementary medicines ensures local relevance at the country level (Cameron et al., 2009). Since the development of WHO/HAI standardized methodology, WHO has worked on a more alternative and sophisticated way for longitudinal data collection with respect to the price and availability of medicines. In 2016, WHO developed an innovative multi-language tool to rapidly collect and analyze data on the price and availability of medicines in health facilities and procurement center–WHO Essential Medicines and Health Products Price and Availability Monitoring Mobile Application (WHO EMP MedMon) This novel tool has improved considering the elements of the WHO/HAI methodology for “Measuring medicine prices, availability, affordability and price components” (WHO, 2018). Moreover, the WHO EMP MedMon App allows users to routinely monitor medicines’ prices and availability in a sustainable, cost-effective, and timely manner. This tool can avoid duplication of efforts and potential manual entry errors by providing photo and barcode capture to identify data when data is collected on paper and then transferred to an electronic format. Furthermore, the tool is customized for any country’s need to collect routine medicines’ data in a fraction of the time and can connect to WHO Medmon’s Power BI platform for interactive analytics and reporting. WHO has tested the application in several pilots, collecting several types of price and availability data, and these results indicate the good feasibility and real-time of this tool (WHO, 2018).
Despite its many strengths, the WHO/HAI methodology also has several limitations. Firstly, differences in quality across products and differences in patent status between countries are not accounted for Ridley (2005). Such as, in India, there are a large number of generic manufacturers and the pricing regulations in force do not recognize medicine patents. Secondly, the reliability of the median price ratio (MPR) as a metric for comparison depends on each medicine’s median international reference price (IRP) which is susceptible to the number of supplier prices. When few supplier prices are available or when the buyer price is used as a substitute, MPR results can be skewed by a particularly high or low IRP. Concurrently, the survey method is more complicated and requires much manpower, material, and time. In addition, most of the medicine availability data obtained are the availability of medicines in the sectors on the survey day, and it cannot reflect each of these sectors’ monthly or annual average supply of medicines. The results in our review indicated that the availability of most medicines for children was low in the public sectors and private sectors, and the prices of medicines exceeded IRP. The public sector’s availability of medicines for children was consistently low, which could be due to high demand but insufficient supply, as general public sectors’ medicines are available for free or at low cost. This could be due to a combination of factors further, such as inadequate funding, lack of incentives for maintaining stocks, inability to forecast accurately, inefficient distribution systems, or leakage of medicines for private resale (Cameron et al., 2009). The availability in the private sector was slightly higher, but in many countries, it was still low, and the higher private sector prices could hinder access to medicines in children. Although the policy on the accessibility of medicines for children has improved in recent years, there may be a lack of compulsory regulations on medicine procurement and pricing. The consistency, system, and accuracy of the policy need to be improved.
Firstly, this review only included Chinese and English articles, which could have a language bias. Also, some of the studies included in this review were conducted 5 years ago. Many countries have taken measures on improving the accessibility of medicines for children (such as the medical insurance catalogue and the national essential medicine catalogue will be revised regularly). Therefore, the previous survey results could not be fully consistent with the current accessibility of medicines in these regions. Importantly, the medicine availability data is the availability of medicines in surveyed sectors on the survey day, which could not truly reflect the monthly or annual average medicine supply of these sectors. It also needs to considered that most of the included studies adapted the WHO/HAI standardized methodology to investigate and evaluate the medicine price and affordability, in which only a small number of medicines could obtain the data of price and affordability, so these data may not accurately reflect the real situation of local children’s medicine prices and affordability. Lastly, all of the included studies investigated the accessibility of medicines for children in low-income and middle-income countries, and these survey results could not apply to high-income countries.
Based on the results of this review, the data confirmed that substantial opportunities exist to increase availability, lower prices, and improve the affordability of children’s medicines in all regions and countries. Countries should establish a regular investigation and report system for the accessibility of children’s medicines to regularly investigate the availability, prices, and affordability of medicines. Routinely monitored and timely report the investigation and evaluation results to relevant departments is crucial. Medicine prices, availability, and affordability should be surveyed and reported at least every 2 years by using the WHO/HAI methodology (Cameron et al., 2009). These data provided for countries can develop, implement, assess, and adjust national policies and medicine prices to improve the availability and affordability of children’s medicines. The WHO MEDMON tool may be an appropriate tool to help any country to create its own routine data collection systems for real-time monitoring, and to assist the government to assess policy interventions’ effect. In the third WHO Fair Pricing Forum on reaching fairer prices of medicines and health tools ended on 22 April 2021, WHO announced that later this year, they would launch its updated MEDMON to monitor availability and prices of health products in several countries. Simultaneously, WHO would continue to support these countries with the development of national or regional price monitoring systems and hosting further webinar and training to strengthen policy-makers’ capacity (WHO, 2021). Further, encouraging the use of those low-cost generic medicines with the dominant efficacy may be able to significantly reduce medical expenditures and increase medicine affordability.
The availability of medicines for children in both public sectors and private sectors in low-income and middle-income countries is low. The MPR of OBs is higher than that of LPGs, and the LPGs is implicated with the better affordability.
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
LLZ and IC contributed to the conception and design of the study. ZC, SL, MZ, and YL conducted the systematic review including screening of abstracts and full text and extracting the data. ZC, SL, and LNZ performed the analyses and wrote the manuscript. All authors revised it critically for important intellectual content and gave their approval of the final version.
Sichuan Province Science and Technology Plan Project (No. 2020YFS0035). Subproject of Science and Technology Plan Project of Sichuan Province (20ZDYF3101).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2021.691606/full#supplementary-material
Abrha, S., Tadesse, E., Atey, T. M., Molla, F., Melkam, W., Masresha, B., et al. (2018). Availability and Affordability of Priority Life-Saving Medicines for Under-Five Children in Health Facilities of Tigray Region, Northern Ethiopia. BMC Pregnancy Childbirth 18 (1), 464. doi:10.1186/s12884-018-2109-2
Andersson, F. (1993). Methodological Aspects of International Drug price Comparisons. Pharmacoeconomics 4 (4), 247–256. doi:10.2165/00019053-199304040-00003
Anson, A., Ramay, B., de Esparza, A., and Bero, L. (2012). Availability, Prices and Affordability of the World Health Organization’s Essential Medicines for Children in Guatemala. Globalization Health 8 (1), 22. doi:10.1186/1744-8603-8-22
Balasubramaniam, R., Benaragama, B. V. S. H., and Ranganathan, S. S. (2011). A National Survey of Availability of Key Essential Medicines for Children in Sri Lanka. Ceylon Med. J. 56 (3), 101–107. doi:10.4038/cmj.v56i3.3597
Balasubramaniam, R., Benaragama, B. V. S. H., and Ranganathan, S. S. (2014). A National Survey of Price and Affordability of Key Essential Medicines for Children in Sri Lanka. Indian J. Pediatr. 81 (4), 362–367. doi:10.1007/s12098-013-1024-9
Batchelor, H. K., and Marriott, J. F. (2015). Paediatric Pharmacokinetics: Key Considerations. Br. J. Clin. Pharmacol. 79 (3), 395–404. doi:10.1111/bcp.12267
Cameron, A., Ewen, M., Ross-Degnan, D., Ball, D., and Laing, R. (2009). Medicine Prices, Availability, and Affordability in 36 Developing and Middle-Income Countries: A Secondary Analysis. Lancet 373 (9659), 240–249. doi:10.1016/S0140-6736(08)61762-6
CROMBIE I (1996). Pocket Guide to Critical Appraisal[M]. London, United Kingdom: John Wiley & Sons, 113.
Demerew, H. A., and Ahmed, M. S. (2020). Availability, Price, and Affordability of WHO Priority Maternal and Child Health Medicine in Public Health Facilities of Dessie, North-East Ethiopia. BMC Med. Inform. Decis. Mak. 20, 221. doi:10.1186/s12911-020-01247-2
Finney, E. (2019). Children’s Medicines: A Situational Analysis. Available at: http://www.who.int/childmedicines/progress/CM_analysis.pdf (Accessed December 28, 2020).
Gereltuya, D., Bruce, S., Tsetsegmaa, S., Gantuya, D., and Byambatsogt, G. (2018). Availability, Affordability and Costs of Pediatric Medicines in Mongolia. BMC Pediatr. 18 (1), 149. doi:10.1186/s12887-018-1123-x
Guoxu, W., XiaoLing, W., Xin, L. I., LiYing, L. I., Jing, C., and Lu-Wen, S. H. I. (2019). A Surveyon the Availabilityprice and Affordability of Essential Medicine for Children in Eastern China. China Health Pol. Res. 12 (10), 72–78. doi:10.3969/j.issn.1674-2982.2019.10.011
Hailu, A. D., and Mohammed, S. A. (2020). Availability, Price, and Affordability of WHO Priority Maternal and Child Health Medicine in Public Health Facilities of Dessie, North East Ethiopia. BMC Med. Inform. Decis. Mak. 20 (1), 221.
Ivanovska, V., Rademaker, C. M. A., van Dijk, L., and Mantel-Teeuwisse, A. K. (2014). Pediatric Drug Formulations: a Review of Challenges and Progress. Pediatrics 134 (2), 361–372. doi:10.1542/peds.2013-3225
Management Sciences for Health(2015). The International Medical Products Price Guide. Available at: https://mshpriceguide.org/en/ (Accessed February 1, 2021).
Neha, F., Alexandra, M., Abhishek, S., Chanchal, S., Bhumika, R., Singh, A. R., et al. (2019). Evaluating Access to Essential Medicines for Treating Childhood Cancers: A Medicines Availability, Price and Affordability Study in New Delhi, India. BMJ Glob. Health. 4 (2), e001379. doi:10.1136/bmjgh-2018-001379
Nsabagasani, X., Ogwal-Okeng, J., Mbonye, A., Ssengooba, F., Muhumuza, S., and Hansen, E. H. (2015). Availability and Utilization of the WHO Recommended Priority Lifesaving Medicines for Under Five-Year Old Children in Public Health Facilities in Uganda: A Cross-Sectional Survey. J. Pharm. Pol. Pract. 8 (1), 1–7. doi:10.1186/s40545-015-0038-2
Orubu, E. S. F., Robert, F. O., Samuel, M., and Megbule, D. (2019). Access to Essential Cardiovascular Medicines for Children: a Pilot Study of Availability, price and Affordability in Nigeria, Health Pol. Plann. 34 (Suppl. 3), iii20–iii26. doi:10.1093/heapol/czz057
Ravindran, L., Bandyopadhyay, M., Bagchi, C., and Tripathi, S. K. (2012). A Preliminary Assessment of Availability and Pricing of Children’s Medicines in Government Hospitals and Private Retail Pharmacies in a District of Andhra Pradesh. Indian J. Pharmacol. 44 (4), 536–537. doi:10.4103/0253-7613.99347
Ridley, D. B. (2005). Price Differentiation and Transparency in the Global Pharmaceutical Marketplace. Pharmacoeconomics 23 (7), 651–658. doi:10.2165/00019053-200523070-00002
Sado, E., and Sufa, A. (2016). Availability and Affordability of Essential Medicines for Children in the Western Part of Ethiopia: Implication for Access. BMC Pediatr. 16, 40. doi:10.1186/s12887-016-0572-3
Saisai, L., Wei, X. U., WenWen, D. U., and YangBing, F. U. (2018). Study on the Availability of Pediatric Essential Medicines in China: Based on the Surveys in 19 Provinces. China Health Pol. Res. 11 (12), 12–18. doi:10.3969/j.issn.1674-2982.2018.12.003
Sun, X., Wei, J., Yao, Y., Chen, Q., You, D., Xu, X., et al. (2018). Availability, Prices and Affordability of Essential Medicines for Children: A Cross-Sectional Survey in Jiangsu Province, China. BMJ Open 8(10), e023646, doi:10.1136/bmjopen-2018-023646
Swain, T., Rath, B., Dehury, S., Tarai, A., Das, P., Samal, R., et al. (2015). Pricing and Availability of Some Essential Child Specific Medicines in Odisha. Indian J. Pharmacol. 47 (5), 496. doi:10.4103/0253-7613.165197
The International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH) (2000). Guidance for Industry E11 Clinical Investigation of Medicinal Products in the Pediatric Population. Available at: http://www.fda.gov/cder/guidance/index.htm.
Wang, X., Fang, Y., Yang, S., Jiang, M., Yan, K., Wu, L., et al. (2017). Access to Paediatric Essential Medicines: A Survey of Prices, Availability, Affordability and Price Components in Shaanxi Province, China. PLoS One 9 (3), e90365. doi:10.1371/journal.pone.0090365
WHO (2018). MedMon - WHO Essential Medicines and Health Products Price and Availability Monitoring Mobile Application. Available at: https://www.who.int/news/item/18-02-2018-medmon-mobile-application (Accessed July 17, 2021).
WHO (2021). Fair Pricing Forum Ends With Good Intentions and New Undertakings From WHO. Available at: https://www.who.int/news/item/23-04-2021-fair-pricing-forum-ends-with-good-intentions-and-new-undertakings-from-who (Accessed July 17, 2021).
World Health Organization (2010). Model Formulary for Children. Available at: https://apps.who.int/iris/bitstream/handle/10665/44309/9789241599320_eng.pdf;jsessionid=442F096E06B02875FF204841FA2A804D?sequence=1 (Accessed January 10, 2021).
World Health Organization (2019a). 7th WHO Model List of Essential Medicines for Children. Available at: https://www.who.int/medicines/publications/essentialmedicines/en/ (Accessed December 25, 2020).
World Health Organization (2019b). Better Medicines for Children:Country Implementation. Available at: http://www.who.int/childmedicines/countries/en/ (Accessed December 10, 2020).
World Health Organization (2020). Children: Reducing Mortality. Available at: https://www.who.int/en/news-room/fact-sheets/detail/children-reducing-mortality (Accessed February 3, 2021).
World Health Organization, Health Action International (2008). Measuring Medicine Prices, Availability, Affordability and price Components. 2nd Edn. Switzerland: World Health Organization and Health Action International.
Xiao, W., Anchao, Z., He, W., and Li, M. (2020). Evaluation Study on the Availability and Prices of Paediatric Essential Drugs in Weifang. China Pharm. Aff. 34 (9), 1085–1092. doi:10.16153/j.1002-7777.2020.09.013
Yi, D., Zhiping, L., Hong, X., and Zhu, L. (2020). A Multicenter Survey of the Accessibility of Essential Medicines for Children in China. Chin. J. Pediatr. 58 (4), 301–307. doi:10.3760/cma.j.cn112140-20190820-00527
Zhang, L., Li, B., Liu, Z., Li, M., Zheng, H., and Sun, Y. (2017). Promoting Innovation and Access to Quality, Safe, Efficacious, and Affordable Medicines for Children: A China Approach on the 69th World Health Assembly. J. Evid. Based Med. 10 (2), 70–75. doi:10.1111/jebm.12250
Keywords: children, medicine, accessibility, systematic review, availability, price, affordability
Citation: Chen Z, Li S, Zeng L, Liu Y, Zhang M, Choonara I and Zhang L (2021) Accessibility of Medicines for Children: A Systematic Review. Front. Pharmacol. 12:691606. doi: 10.3389/fphar.2021.691606
Received: 07 April 2021; Accepted: 29 July 2021;
Published: 05 August 2021.
Edited by:
Irene Lenoir-Wijnkoop, Utrecht University, NetherlandsReviewed by:
Aukje K. Mantel-Teeuwisse, Utrecht University, NetherlandsCopyright © 2021 Chen, Li, Zeng, Liu, Zhang, Choonara and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lingli Zhang, emhhbmdsaW5nbGlAc2N1LmVkdS5jbg==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.