
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol., 18 February 2021
Sec. Neuropharmacology
Volume 12 - 2021 | https://doi.org/10.3389/fphar.2021.625610
This article is part of the Research TopicStimulant Use and Addictive DisorderView all 22 articles
 Arantza Sanvisens1Anna Hernández-Rubio1
Arantza Sanvisens1Anna Hernández-Rubio1 Paola Zuluaga1
Paola Zuluaga1 Daniel Fuster1
Daniel Fuster1 Esther Papaseit2Sara Galan1
Esther Papaseit2Sara Galan1 Magí Farré2
Magí Farré2 Robert Muga1*
Robert Muga1*Objective: Cocaine Use Disorder (CUD) has been associated with multiple complications and premature death. The purpose of the present study was to analyze the relationship between baseline medical comorbidity and long-term medical outcomes (i.e., hospitalization, death) in a cohort of patients primarily admitted for detoxification. In addition, we aimed to analyze cause-specific mortality.
Methods: longitudinal study in CUD patients admitted for detoxification between 2001 and 2018. Substance use characteristics, laboratory parameters and medical comorbidity by VACS Index were assessed at admission. Follow-up and health-related outcomes were ascertained through visits and e-health records. Kaplan-Meier and Cox regression models were used to analyze survival and predictors of hospitalization and death.
Results: 175 patients (77.7% men) were included. Age at admission was 35 years [IQR: 30–41 years], 59.4% of the patients being intranasal users, 33.5% injectors, and 7.1% smokers. Almost 23% of patients had concomitant alcohol use disorder, 39% were cannabis users and 9% opiate users. The median VACS Index score on admission was 10 points [IQR: 0–22]. After 12 years [IQR: 8.6–15 years] of follow-up there were 1,292 (80.7%) ED admissions and 308 (19.3%) hospitalizations. The incidence rate of ED admission and hospitalization was 18.6 × 100 p-y (95% CI: 15.8–21.8 × 100 p-y). Mortality rate was 1.4 × 100 p-y (95% CI: 0.9–2.0 × 100 p-y) and, baseline comorbidity predicted hospitalization and mortality: those with VACS Index >40 were 3.5 times (HR:3.52, 95% CI: 1.19–10.4) more likely to dye with respect to patients with VACS < 20.
Conclusion: addiction care warrants optimal stratification of medical comorbidity to improve health outcomes and survival of CUD patients seeking treatment of the disorder.
Cocaine is the second most widely used illegal drug in Western Europe after cannabis. According to the European Monitoring Center for Drugs and Drug Addiction (EMCDDA), about four million people aged 15–64 have used cocaine in the last year, and the number of users has increased in recent years (European Monitoring Center for Drugs and Drug Addiction (EMCDDA), 2019).
According to the EDADES population survey on alcohol and drugs, 2% of the general population aged 15–64 in Spain uses cocaine (Observatorio Español de las Drogas y las Adicciones, 2019). Moreover, 54% of people who have used cocaine in the last year have used it in the last month (Observatorio Español de las Drogas y las Adicciones, 2019). In Catalonia (Spain), 24% of people who seek treatment for substance use disorder (SUD) have a cocaine use disorder (CUD), and this percentage has increased in recent years (Subdirecció General de Drogodependències, 2018).
CUD has been associated with serious systemic complications, frequent use of healthcare resources (i.e., emergency department (ED) admissions, hospitalization), and premature death (Degenhardt et al., 2011; Butler et al., 2017). In fact, cocaine use can aggravate inflammatory diseases and alter immune functions that favor the progression of cardiovascular, respiratory, or infectious diseases (Taylor et al., 2016; Bachi et al., 2017). In addition, it has been communicated that cocaine intoxication can cause acute kidney injury, hepatotoxicity, and disseminated intravascular coagulation (Vitcheva, 2012; Filho et al., 2019). On the other hand, cocaine use has been associated with an increased risk of HIV infection and hepatitis C virus (HCV) infection even in the absence of injecting drug use (Macías et al., 2008; Deiss et al., 2012).
In addition, patients with CUD show a high prevalence of psychiatric comorbidities, such as mood disorders (12–62%), anxiety disorders (21–45%) and suicidal tendencies, among others (Vergara-Moragues et al., 2012; Warden et al., 2016). Cocaine use has also been associated with traffic accidents and violence (Giovanardi et al., 2005; Pavarin et al., 2011).
Polysubstance use is common among cocaine users, especially alcohol consumption, but the concurrent use of marijuana and opiates is also prevalent, and has been associated with poor health outcomes (Stinson et al., 2005; Timko et al., 2018). In the US, the second wave of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) estimated that 79% of people with CUD have a concomitant alcohol use disorder (AUD) (Stinson et al., 2005).
A recent systematic review and meta-analysis on healthcare utilization demonstrated that in SUD patients, hospitalization and ED admissions are 5 and 7 times more frequent, respectively, compared to the general population (Lewer et al., 2020). In addition, the death rate of patients with CUD ranges from 0.5 to 6.2 × 100 person-years (p-y) and is considered to be 4 to 8 times higher than the death rate of the general population (Arendt et al., 2011; Degenhardt et al., 2011).
Our hypothesis is that the chronicity of CUD is suggestive of the presence of multiple medical complications, which leads to the excessive use of healthcare resources (i.e., ED visits and hospitalization). We aimed to analyze the relationship between baseline medical comorbidity, use of health resources, and long-term health outcomes among those seeking treatment for CUD.
This was a longitudinal study of patients admitted to the addiction treatment unit of a tertiary hospital (Germans Trias i Pujol University Hospital) between January 2001 and May 2018. The unit admits patients diagnosed with SUD in an area in the north of Barcelona (Spain) with 400,000 inhabitants. There were 837 admissions for addiction treatment between January 2001 and May 2018, of which 195 (23.3%) were due to CUD in 175 patients. In those who were admitted more than once, only the first admission was analyzed.
The patients came from local primary care centers and from two municipal outpatient addiction clinics, one in Badalona (250,000 inhabitants) and the other in Santa Coloma de Gramenet (150,000 inhabitants), both located in the metropolitan area of Barcelona (Spain). The main admission criteria for CUD treatment were as follows: failure in outpatient treatment, concurrent dependency on other addictive drugs or alcohol, serious concurrent medical problems, severe impairment of psychosocial functioning, lack of family and social support, and use of crack or freebase cocaine or intravenous cocaine abuse, among others.
All patients received a diagnosis of CUD according to the Diagnostic and Statistical Manual of Mental Disorders, fourth Ed (DSM-IV) and fifth Ed (DSM-5). Due to the transition from DSM-IV to DSM-5, not all participants were evaluated under the same DSM.
On admission, data on the use of cocaine and other substances (i.e., alcohol, cannabis, opiates) were collected, including age of onset, route of administration, and duration. DSM criteria were used to diagnose AUD. Cannabis and opiates use was ascertained through urinalysis at admission. For the purposes of this study, patients were classified according to the route of cocaine administration as either intranasal or non-intranasal users (i.e., injectors, smokers).
In all patients, blood samples were drawn for biochemical and hematological parameters, and for serologic testing for human immunodeficiency virus (HIV) infection and hepatitis C virus (HCV) infection. Anthropometric data (i.e., height and weight) were obtained as well.
Medical comorbidity on admission was analyzed using the VACS Index (Veterans Aging Cohorts Study Index). VACS Index assigns a score based on age and on blood parameters, such as hemoglobin, platelets, aspartate and alanine aminotransferase levels, creatinine, HIV infection, CD4 lymphocytes, HIV RNA, and HCV infection. The VACS Index ranges from 0 to 164 points, with a higher score indicating greater comorbidity. The VACS Index has been associated with an increased risk of hospitalization and death in patients with and without HIV infection (Blackstock et al., 2013; Justice et al., 2013; Tate et al., 2013). In HIV-negative patients, HIV RNA is considered undetectable.
The patients were followed up until September 30, 2018 through in-person visits and review of the ED visits and hospitalization e-health records of the Catalan health department. The diagnoses made during the ED visits and hospitalization were coded according to the 10th revision of the International Classification of Diseases (ICD-10). The diagnostic coding was carried out by two members of the research team (AS and RM) independently; coding discrepancies were resolved by consensus.
Mortality was analyzed by cross-referencing the data with the National Death Index as of September 30, 2018. The causes of death were established by reviewing the medical history.
All patients gave written informed consent, and the study design was approved by the Ethics Committee of the Germans Trias i Pujol University Hospital (approval number PI-13-082). The methods were in compliance with the ethical standards for medical research and the principles of good clinical practice in accordance with the World Medical Association’s Declaration of Helsinki.
Descriptive statistics were expressed as median and interquartile range (IQR) for quantitative variables and as absolute frequencies and percentages for qualitative variables.
We used the chi-square test to detect significant differences in qualitative variables and t-Student test for differences in quantitative variables. The Kruskal-Wallis equality-of-populations rank test and Mann-Whitney U test were used to analyze differences in the distribution of episodes during follow-up.
Rates were calculated in p-y by dividing the number of observed events during the study period by the sum of all individual follow-up times. The survival estimates were analyzed using the Kaplan-Meier curves. Cox regression models were used to analyze the risk factors of first hospitalization after discharge and mortality. The sex, variables related to substance use, and the VACS Index score were included in the analysis. All covariates that were statistically significant in the univariate analysis were included in the multivariate analysis. Prior to implementing the statistical models, we checked the proportional hazard assumptions using tests and graphs based on the Schoenfeld residuals.
p-values <0.05 were considered statistically significant. Statistical analysis was performed using Stata software (version 11.1, College Station, Texas, United States).
The study included 175 patients (77.7% men) aged 35 years [IQR: 30–41 years]. The age of onset of cocaine use was 22 years [IQR: 18–26 years], with 59.4% of the patients being intranasal users, 33.5% injectors, and 7.1% smokers. Moreover, 22.9% of the patients had concomitant AUD. According to the screening for illegal drugs in urine samples, 39.4% were cannabis users and 9% opiate users. Overall, 58.1% of the patients used alcohol or other substances in addition to cocaine. The most common combinations of substances were cocaine and cannabis (27.5%), cocaine and alcohol (14.4%), and cocaine, alcohol, and cannabis (7.5%).
The laboratory test results for hemoglobin, total cholesterol, and gamma-glutamyl transferase were 14.2 g/dl [IQR: 12.9–15.3 g/dl], 170 mg/dl [IQR: 147–201 mg/dl], and 28 U/L [IQR: 17–62 U/L], respectively. Moreover, 24.7% of the patients were HIV-positive and 47.4% were anti-HCV positive.
The body mass index (BMI) was 19.5 kg/m2 [IQR: 16.4–23.0 kg/m2]. The median VACS Index score on admission was 10 points [IQR: 0–22; range 0–69]. Table 1 shows the sociodemographic characteristics, alcohol and substance use, and clinical and blood parameters.
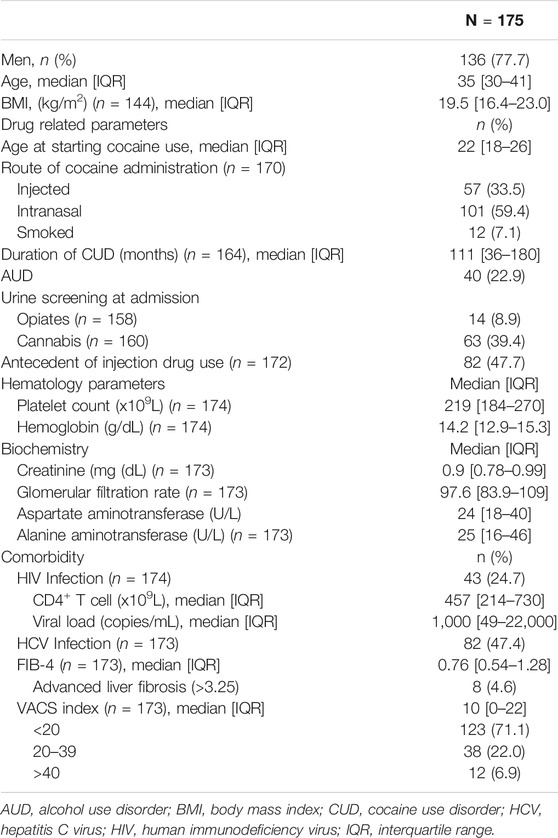
TABLE 1. Sociodemographic characteristics, alcohol and substance use, and clinical and blood parameters in 175 patients admitted for the treatment of CUD in metropolitan Barcelona, Spain.
Table 2 shows the socio-demographics, substance use characteristics, and clinical and blood parameters of CUD patients that were hospitalized during follow-up. Hospitalization was significantly more frequent in women (p = 0.049), in those with antecedent of injecting drug use (p = 0.028), and in HIV-positive and HCV-positive patients (p = 0.001 and p = 0.047, respectively).
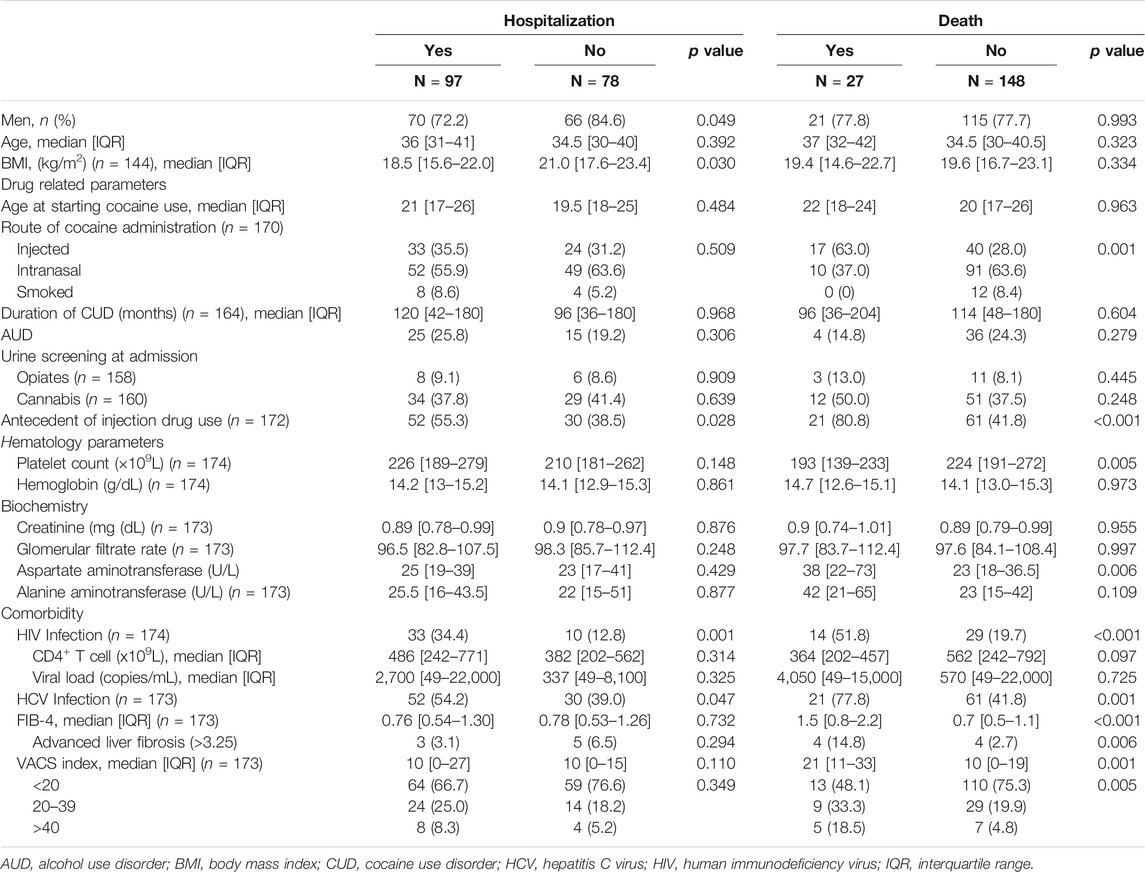
TABLE 2. Baseline characteristics of CUD patients according to hospitalization and death during follow-up.
The median follow-up time was 12.1 years [IQR: 8.6–15.1 years] with a total time of 1,973.2 p-y. At the end of the study, there were 1,292 (80.7%) ED admissions and 308 (19.3%) hospitalizations. The median number of ED admissions and hospitalizations per patient were 5 [IQR: 1–10] and 1 [IQR: 0–2], respectively. The vast majority (85.1%) of the patients presented at least one episode of ED admission or hospitalization. Statistically significant differences were observed in the distribution of episodes (either ED admission or hospitalization) according to gender and HIV status; specifically, women (z = −2.704, p = 0.007) and HIV-positive patients (z = −2.291, p = 0.022) had a greater number of episodes (Figure 1). The probability of having an ED admission or hospitalization was 50% after 2.5 years (95% CI: 1.9–3.7 years) (Figure 2A).
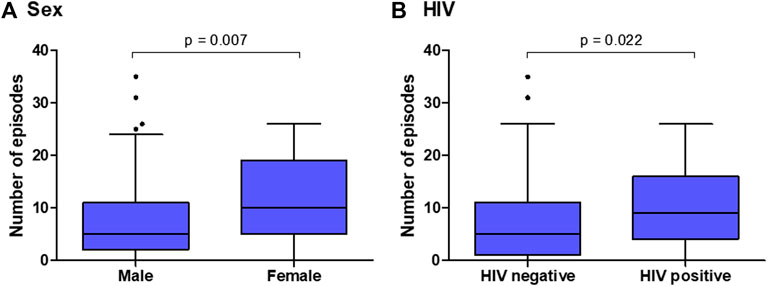
FIGURE 1. ED admissions or hospitalizations by (A) sex and (B) HIV infection status in a cohort of 175 patients admitted for treatment of CUD in metropolitan Barcelona, Spain.
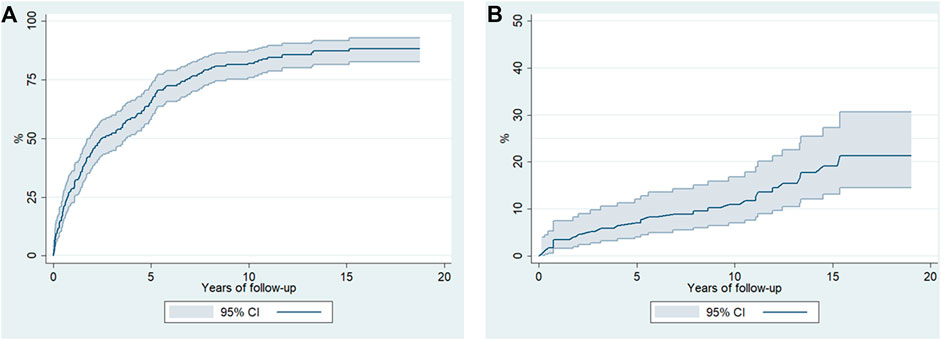
FIGURE 2. Kaplan-Meier estimates (95% confidence intervals) for (A) ED visits or hospitalization episodes of 175 CUD patients and for (B) survival after being admitted for detoxification in metropolitan Barcelona, Spain.
The incidence rate of ED admission or hospitalization was 18.6 × 100 p-y (95% CI: 15.8–21.8 × 100 p-y), which was significantly higher in women (rate ratio (RR): 1.8, 95% CI: 1.22–2.60, p = 0.002) and in patients with concomitant AUD (RR: 2.0, 95% CI: 1.3–2.9, p < 0.001). Figure 3A shows the incidence of episodes according to baseline medical comorbidity.
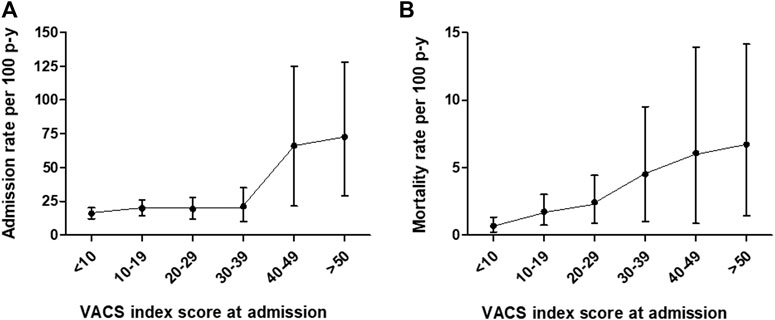
FIGURE 3. Comorbidity (VACS Index)-adjusted incidence rates (95% confidence intervals) of (A) ED admission or hospitalization episodes and (B) mortality in a cohort of 175 patients seeking treatment of CUD in metropolitan Barcelona, Spain.
In terms of ED admissions, 19% were related to trauma/injuries (i.e., fractures, contusions, wounds), 19% to non-specific/unclassified symptoms, 10% to substance use, and 8.5% to mental disorder.
Regarding hospitalization, almost 40% of the episodes were related to mental health, 11% to the liver/digestive system, and 10.4% to respiratory conditions (i.e., pneumonia). Figure 4 shows the distribution of ED admission and hospitalization episodes according to the main diagnosis.
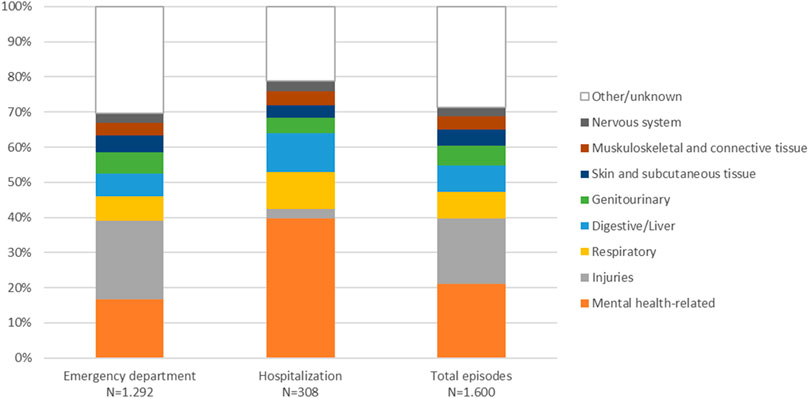
FIGURE 4. Distribution of 1,292 ED admissions and 308 hospitalizations according to ICD-10 diagnostic codes.
Table 3 shows the risk factors for hospitalization. Specifically, being women (hazard ratio (HR): 1.61, 95% CI: 1.02–2.58), presenting concomitant AUD (HR: 1.42, 95% CI: 1.18–1.71), and having VACS Index >40 (HR: 2.59, 95% CI: 1.13–5.94) were significantly associated with a higher probability of hospitalization.
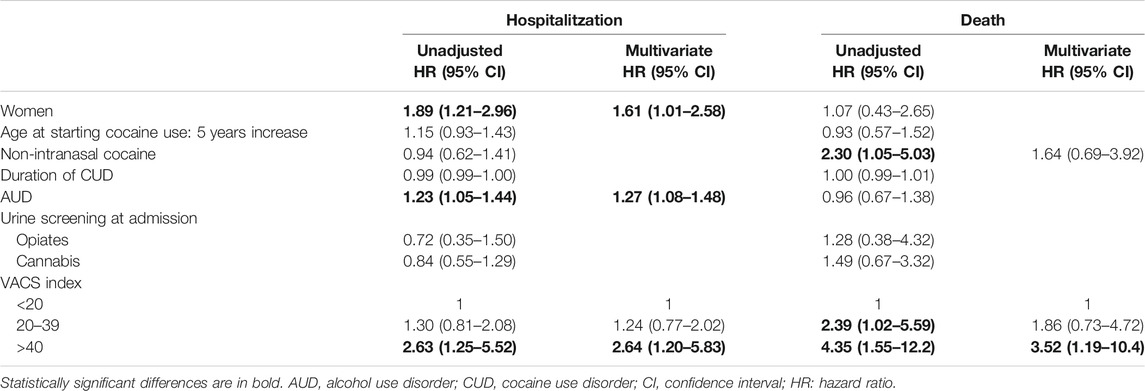
TABLE 3. Cox regression model for predictors of hospitalization and death in a cohort of 175 patients admitted for treatment of CUD in metropolitan Barcelona, Spain.
Of the patients included in the study, 15.4% (n = 27) died during the follow-up and the death rate was 1.4 × 100 p-y (95% CI: 0.9–2.0 × 100 p-y). Table 2 shows the differences between those who died and those who survived; all-cause mortality was significantly associated with current or past injecting drug use (p = 0.001 and p < 0.001, respectively), HIV infection (p < 0.001), HCV infection (p < 0.001), advanced liver fibrosis (p = 0.006) and higher scores in VACS Index (p = 0.005).
Figure 2B shows the estimate (Kaplan-Meier) of survival after admission for CUD treatment. The multivariate analysis showed that medical comorbidity was the only predictor of death; patients with VACS >40 showed 3.5 times greater probability of death (HR 3.52, 95% CI: 1.19–10.4) compared to patients with VACS Index <20 (Table 3). Figure 3B shows death rates according to VACS Index.
The cause of death was determined in 77.7% (21/27) of cases; the main causes were drug-related in 40% (n = 8; 5 overdoses, 3 unattended deaths in the context of current drug use), cancer in 19% (n = 4), infectious diseases in 9.5% (n = 2), cardiovascular diseases in 9.5% (n = 2), and liver cirrhosis in 9.5% (n = 2).
This longitudinal study in patients with CUD who were followed for 12 years confirms the prognostic value of a comorbidity index in predicting the risk of hospitalization and death in patients seeking treatment for the disorder. VACS is a multiorgan system injury index validated in 2013 for HIV-positive patients, although it has been described as a reliable index for HIV-negative patients as well and as a predictor of health outcomes such as hospitalization (Tate et al., 2013; Barakat et al., 2015; Hotton et al., 2017). To the best of our knowledge, this is the first time that VACS Index was analyzed in a cohort of HIV-positive and HIV-negative patients with CUD. Our results support the use of medical comorbidity rates in patients with SUD who start treatment, although more studies are required to confirm these findings.
In this study, VACS Index at baseline reflected moderate organ system damage, even though 47 and 25% of the patients had HCV and HIV infection, respectively. Despite moderate comorbidity, those with a VACS Index score over 40 were up to 2.6 times more likely to require hospitalization than those with a VACS score under 20. On the other hand, women with CUD and AUD were at a higher risk of hospitalization. Concomitant AUD is frequent in CUD and has been described as an indicator of poor health outcomes (Timko et al., 2018). Specifically, cocaethylene, the metabolite resulting from the concomitant use of alcohol and cocaine, has a known toxicity (Jones, 2019). This potent stimulant is more toxic than cocaine itself and has a longer half-life. On the other hand, the increased risk of hospitalization for women with CUD requires an accurate evaluation of the continuum of care and care coordination after discharge.
It was interesting to confirm that medical comorbidity was the only predictor of death in this cohort with a high prevalence of polysubstance use. Some studies on CUD indicate that the risk of death is higher in men, in those with a history of injected drugs, in those with an early onset of use, in those who drink alcohol, or in those with psychiatric comorbidity (Arendt et al., 2011; de la Fuente et al., 2014). However, there are hardly any studies on the medical comorbidity of CUD other than HIV infection and HCV infection. VACS Index analyzes kidney and liver function in addition to age, hemoglobin and HIV and HCV infections, thus reflecting the general health status. The recent 2019 version includes albumin, blood cell count, and BMI (Tate et al., 2019), which may improve the prognostic value of VACS.
It was interesting to note that BMI was below 19.5 kg/m2 in 50% of the patients in this study and below 16.4 kg/m2 in 25%, which indicates that being underweight might be associated with CUD or an underlying disease. A population study in adults aged 18–45 years demonstrated that the BMI of cocaine users is lower than that of non-users, although those BMI values were much higher than those observed in this study (Qureshi et al., 2014).
On the other hand, death rates in this hospital-based cohort were higher than that reported by another Spanish study of patients recruited in outpatient clinics (de la Fuente et al., 2014), although clearly lower than that reported by our group in past decades (Sanvisens et al., 2014).
ED admissions for accidents/injuries and non-specific symptoms were the most frequent during follow-up, suggesting that they could be related to continued substance use or complications derived from such use. The first systematic review and meta-analysis on healthcare utilization in patients with SUD was published in 2019 and shows that hospitalization and ED admissions are 5 and 7 times more frequent, respectively, in this group than in the general population (Lewer et al., 2020). In Spain, 38.4% of drug-related ED admissions can be attributed to cocaine (Miró et al., 2019). Furthermore, a study reveals that 18% of those admitted to an ED for cocaine use are readmitted in the following year (Miro et al., 2010).
Mental health-related complications, accidents/injuries, respiratory/lung related conditions, and digestive/liver diseases were other diagnoses frequently observed during follow-up. About 40% of the episodes were related to SUD either due to an associated mental illness or to trauma/accidents associated with substance use. These results are consistent with those presented in individuals who use illicit drugs (Aitken et al., 2013; Kendall et al., 2017). The pulmonary complications resulting from cocaine use could be due to several reasons, although the route of administration is relevant (Mégarbane and Chevillard, 2013); cocaine's respiratory toxicity can be immediate (i.e., acute lung injury or hypersensitivity reaction) or delayed (i.e., chronic obstructive pulmonary disease, cancer) (Mégarbane and Chevillard, 2013). A recent study shows that cocaine users are at increased risk for pulmonary hypertension (Alzghoul et al., 2020).
In terms of digestive/liver comorbidity, our findings are consistent with those observed in other studies (Pavarin et al., 2011). Liver decompensation was another frequent reason for clinical attention; however, a study in patients coinfected with HIV and HCV was unable to demonstrate an association between cocaine/crack use and evolution of liver fibrosis (Martel-Laferrière et al., 2017). Therefore, it is likely that alcohol abuse in the patients could explain those findings.
Cardiovascular complications in this long-term followed-up cohort were less frequent than expected, despite the extensive scientific literature on CUD and acute coronary syndrome (Lippi et al., 2010; Carrillo et al., 2011). However, the results are consistent with those reported in other cohorts with low frequency of coronary ischemic complications (Qureshi et al., 2014).
This study has several limitations that should be mentioned. First, socioeconomic and baseline psychiatric comorbidity data were not available, which could have facilitated the interpretation of some findings during follow-up. Second, temporary changes in cocaine use (i.e., remission or exacerbation of use) were not analyzed. In this sense, retention in care is critical for achieving remission of CUD. The high rate of ED admissions of the patients in this study and the diagnoses of episodes related to continued substance use suggest low treatment retention. Third, patients from this study were evaluated with different DSM versions; however, criteria for admission were similar throughout the study period and mainly related to the severity of CUD. Fourth, this study had a limited number of patients, which impairs the interpretation of some associations due to lack of statistical power (i.e., route of cocaine administration). In addition, this study was carried out in a single unit which limits the generalization of the findings.
In contrast, the strength of this study among patients seeking treatment for CUD highlights the challenges in measuring medical comorbidity with an index that has proven to be useful in the context of SUD. Most studies on cocaine-related morbidity are conducted in EDs with patients with acute intoxication (Arendt et al., 2011; Qureshi et al., 2014; Miró et al., 2019; Santurtún et al., 2020), which prevents an accurate clinical assessment of comorbidity. Finally, understanding the risk factors for mortality allows us to target preventive interventions to increase retention in care among those seeking treatment for the disorder.
The datasets generated for this study are available on request to the corresponding author.
The studies involving human participants were reviewed and approved by the Ethics Committee of the Germans Trias i Pujol University Hospital (approval number PI-13-082). The patients/participants provided their written informed consent to participate in this study.
AS and RM designed the study and wrote the first draft of the manuscript. AHR and SG reviewed e-health records and managed the databases. AS managed the literature searches and statistical analysis. RM, PZ and DF recruited the study population and took care of patients. AS and RM reviewed the literature and made contributions to the interpretation of data. AS, EP, MF, and RM contributed to the discussion section. All the authors revised and approved the final manuscript.
This work was funded by the Ministry of Science, Innovation and Universities, Carlos III Health Institute (ISCIII), Spain and European Fund for Regional Development (FEDER), (grant numbers RD16/0017/0003, PI17/00174, PI20/00883); the Ministry of Health, Social Services and Equality, National Plan on Drugs (PNSD), Spain (grant number 2018/020 and 2020/024); the Agency for Management of University and Research Grants, Government of Catalonia (grant number 2017SGR316). DF is attached to the Research Intensification Program of the Carlos III Health Institute (grant number INT19/00026). PZ is attached to the Joan Rodés Program of the Carlos III Health Institute (grant number JR20/00016).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Aitken, C., Kerr, T., Hickman, M., Stoové, M., Higgs, P., and Dietze, P. (2013). A cross-sectional study of emergency department visits by people who inject drugs. Emerg. Med. J. 30, 421–422. doi:10.1136/emermed-2012-201170
Alzghoul, B. N., Abualsuod, A., Alqam, B., Innabi, A., Palagiri, D. R., Gheith, Z., et al. (2020). Cocaine use and pulmonary hypertension. Am. J. Cardiol. 125, 282–288. doi:10.1016/j.amjcard.2019.10.008
Arendt, M., Munk-Jørgensen, P., Sher, L., and Jensen, S. O. (2011). Mortality among individuals with cannabis, cocaine, amphetamine, MDMA, and opioid use disorders: a nationwide follow-up study of Danish substance users in treatment. Drug Alcohol Depend. 114, 134–139. doi:10.1016/j.drugalcdep.2010.09.013
Bachi, K., Mani, V., Jeyachandran, D., Fayad, Z. A., Goldstein, R. Z., and Alia-Klein, N. (2017). Vascular disease in cocaine addiction. Atherosclerosis 262, 154–162. doi:10.1016/j.atherosclerosis.2017.03.019
Barakat, L. A., Juthani-Mehta, M., Allore, H., Trentalange, M., Tate, J., Rimland, D., et al. (2015). Comparing clinical outcomes in HIV-infected and uninfected older men hospitalized with community-acquired pneumonia. HIV Med. 16, 421–430. doi:10.1111/hiv.12244
Blackstock, O. J., Tate, J. P., Akgün, K. M., Crystal, S., Duggal, M., Edelman, E. J., et al. (2013). Sex disparities in overall burden of disease among hiv-infected individuals in the veterans affairs healthcare system. J. Gen. Intern. Med. 28 Suppl 2, S577. doi:10.1007/s11606-013-2346-z
Butler, A. J., Rehm, J., and Fischer, B. (2017). Health outcomes associated with crack-cocaine use: systematic review and meta-analyses. Drug Alcohol Depend. 180, 401–416. doi:10.1016/j.drugalcdep.2017.08.036
Carrillo, X., Curós, A., Muga, R., Serra, J., Sanvisens, A., and Bayes-Genis, A. (2011). Acute coronary syndrome and cocaine use: 8-year prevalence and inhospital outcomes. Eur. Heart J. 32, 1244–1250. doi:10.1016/j.ycar.2012.01.08210.1093/eurheartj/ehq504
de la Fuente, L., Molist, G., Espelt, A., Barrio, G., Guitart, A., Bravo, M. J., et al. (2014). Mortality risk factors and excess mortality in a cohort of cocaine users admitted to drug treatment in Spain. J. Subst. Abuse Treat. 46, 219–226. doi:10.1016/j.jsat.2013.07.001
Degenhardt, L., Singleton, J., Calabria, B., McLaren, J., Kerr, T., Mehta, S., et al. (2011). Mortality among cocaine users: a systematic review of cohort studies. Drug Alcohol Depend. 113, 88–95. doi:10.1016/j.drugalcdep.2010.07.026
Deiss, R. G., Lozada, R. M., Burgos, J. L., Strathdee, S. A., Gallardo, M., Cuevas, J., et al. (2012). HIV prevalence and sexual risk behaviour among non-injection drug users in Tijuana, Mexico. Global Publ. Health 7, 175–183. doi:10.1080/17441692.2010.549141
European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) (2019). European monitoring Centre for drugs and drug addiction (2019), European drug report 2019: trends and developments. Brussels, Belgium: Publications Office of the European Union.
Filho, J. C. C. L., Ogawa, M. Y., De Souza Andrade, T. H., De Andrade Cordeiro Gadelha, S., Fernandes, P. F. C. B. C., Queiroz, A. L., et al. (2019). Spectrum of acute kidney injury associated with cocaine use: report of three cases. BMC Nephrol. 20, 99. doi:10.1186/s12882-019-1279-0
Giovanardi, D., Castellana, C. N., Pisa, S., Poppi, B., Pinetti, D., Bertolini, A., et al. (2005). Prevalence of abuse of alcohol and other drugs among injured drivers presenting to the emergency department of the University Hospital of Modena, Italy. Drug Alcohol Depend. 80, 135–138. doi:10.1016/j.drugalcdep.2005.04.010
Hotton, A. L., Weber, K. M., Hershow, R. C., Anastos, K., Bacchetti, P., Golub, E. T., et al. (2017). Prevalence and predictors of hospitalizations among HIV-infected and at-risk HIV-uninfected women. J. Acquir. Immune Defic. Syndr. 75, e27–e35. doi:10.1097/QAI.0000000000001278
Jones, A. W. (2019). Forensic drug profile: cocaethylene. J. Anal. Toxicol. 43, 155–160. doi:10.1093/JAT/BKZ007
Justice, A. C., Modur, S. P., Tate, J. P., Althoff, K. N., Jacobson, L. P., Gebo, K. A., et al. (2013). Predictive accuracy of the veterans aging cohort study index for mortality with HIV infection: a north american cross cohort analysis. J. Acquir. Immune Defic. Syndr. 62, 149–163. doi:10.1097/QAI.0b013e31827df36c
Kendall, C. E., Boucher, L. M., Mark, A. E., Martin, A., Marshall, Z., Boyd, R., et al. (2017). Erratum to: a cohort study examining emergency department visits and hospital admissions among people who use drugs in Ottawa, Canada. Harm Reduct. J. 14, 42. doi:10.1186/s12954-017-0169-7
Lewer, D., Freer, J., King, E., Larney, S., Degenhardt, L., Tweed, E. J., et al. (2020). Frequency of health-care utilization by adults who use illicit drugs: a systematic review and meta-analysis. Addiction 115, 1011–1023. doi:10.1111/add.14892
Lippi, G., Plebani, M., and Cervellin, G. (2010). Cocaine in acute myocardial infarction. Adv. Clin. Chem. 51, 53–70. doi:10.1016/S0065-2423(10)51003-5
Macías, J., Palacios, R. B., Claro, E., Vargas, J., Vergara, S., Mira, J. A., et al. (2008). High prevalence of hepatitis C virus infection among noninjecting drug users: association with sharing the inhalation implements of crack. Liver Int. 28, 781–786. doi:10.1111/j.1478-3231.2008.01688.x
Martel-Laferrière, V., Nitulescu, R., Cox, J., Cooper, C., Tyndall, M., Rouleau, D., et al. (2017). Cocaine/crack use is not associated with fibrosis progression measured by AST-to-Platelet Ratio Index in HIV-HCV co-infected patients: a cohort study. BMC Infect. Dis. 17, 80. doi:10.1186/s12879-017-2196-0
Mégarbane, B., and Chevillard, L. (2013). The large spectrum of pulmonary complications following illicit drug use: features and mechanisms. Chem. Biol. Interact. 206, 444–451. doi:10.1016/j.cbi.2013.10.011
Miró, Ò., Dargan, P. I., Wood, D. M., Dines, A. M., Yates, C., Heyerdahl, F., et al. (2019). Epidemiology, clinical features and management of patients presenting to European emergency departments with acute cocaine toxicity: comparison between powder cocaine and crack cocaine cases. Clin. Toxicol. 57, 718–726. doi:10.1080/15563650.2018.1549735
Miro, O., Galicia, M., Sanchez, M., and Nogué, S. (2010). Factores que determinan la reconsulta a urgencias tras una atención urgente por consumo de cocaína. Emergencias 22, 408–414, http://emergencias.portalsemes.org/numeros-anteriores/volumen-22/numero-6/factores-que-determinan-la-reconsulta-a-urgencias-tras-una-atencion-urgente-por-consumo-de-cocaina/.
Observatorio Español de las Drogas y las Adicciones (2019). EDADES 2017—informe web actualizado marzo 2019 OEDA. Available at: moz-extension://a8bef36a-8935-4d90-87ae-d41d2b63b348/enhanced-reader.html?openApp&pdf=http%3A%2F%2Fwww.pnsd.mscbs.gob.es%2Fprofesionales%2FsistemasInformacion%2FsistemaInformacion%2Fpdf%2FEDADES_2017_Informe.pdf (Accessed March 30, 2020).
Pavarin, R., Lugoboni, F., Mathewson, S., Ferrari, A. M., Guizzardi, G., and Quaglio, G. (2011). Cocaine-related medical and trauma problems: a consecutive series of 743 patients from a multicentre study in Italy. Eur. J. Emerg. Med. 18, 208–214. doi:10.1097/MEJ.0b013e3283440f25
Qureshi, A., Chaudhry, S., and Suri, M. (2014). Cocaine use and the likelihood of cardiovascular and all-cause mortality: data from the third national health and nutrition examination survey mortality follow-up study. J. Vasc. Interv. Neurol. 7, 76–82. doi:10.1212/wnl.78.1_meetingabstracts.p07.031
Santurtún, A., García Blanco, A., Fdez-Arroyabe, P., Santurtún, M., and Zarrabeitia, M. T. (2020). Cocaine in hospital admissions for diseases of the circulatory system and as the underlying cause of death: analysis and discussion. Cardiovasc. Toxicol. 20, 20–27. doi:10.1007/s12012-019-09537-6 (Accessed October 15, 2020)
Sanvisens, A., Vallecillo, G., Bolao, F., Rivas, I., Fonseca, F., Fuster, D., et al. (2014). Temporal trends in the survival of drug and alcohol abusers according to the primary drug of admission to treatment in Spain. Drug Alcohol Depend. 136, 115–120. doi:10.1016/j.drugalcdep.2013.12.022
Stinson, F. S., Grant, B. F., Dawson, D. A., Ruan, W. J., Huang, B., and Saha, T. (2005). Comorbidity between DSM-IV alcohol and specific drug use disorders in the United States: results from the national epidemiologic survey on alcohol and related conditions. Drug Alcohol Depend. 80, 105–116. doi:10.1016/j.drugalcdep.2005.03.009
Subdirecció General de Drogodependències (2018). Sistema d’Informació sobre Drogodependències de Catalunya. Available at: http://drogues.gencat.cat/ca/professionals/epidemiologia/sid/ (Accessed October 15, 2020).
Tate, J. P., Justice, A. C., Hughes, M. D., Bonnet, F., Reiss, P., Mocroft, A., et al. (2013). An internationally generalizable risk index for mortality after one year of antiretroviral therapy. AIDS 27, 563–572. doi:10.1097/QAD.0b013e32835b8c7f
Tate, J. P., Sterne, J. A. C., and Justice, A. C. (2019). Albumin, white blood cell count, and body mass index improve discrimination of mortality in HIV-positive individuals. AIDS 33, 903–912. doi:10.1097/QAD.0000000000002140
Taylor, A. L., Denniston, M. M., Klevens, R. M., McKnight-Eily, L. R., and Jiles, R. B. (2016). Association of hepatitis C virus with alcohol use among U.S. Adults: nhanes 2003–2010. Am. J. Prev. Med. 51, 206–215. doi:10.1016/j.amepre.2016.02.033
Timko, C., Han, X., Woodhead, E., Shelley, A., and Cucciare, M. A. (2018). Polysubstance use by stimulant users: health outcomes over 3 years. J. Stud. Alcohol Drugs 79, 799–807. doi:10.15288/jsad.2018.79.799
Vergara-Moragues, E., González-Saiz, F., Lozano, O. M. O., Betanzos Espinosa, P., Fernández Calderón, F., Bilbao-Acebos, I., et al. (2012). Psychiatric comorbidity in cocaine users treated in therapeutic community: substance-induced versus independent disorders. Psychiatr. Res. 200, 734–741. doi:10.1016/j.psychres.2012.07.043
Vitcheva, V. (2012). Cocaine toxicity and hepatic oxidative stress. Curr. Med. Chem. 19, 5677–5682. doi:10.2174/092986712803988929
Warden, D., Sanchez, K., Greer, T., Carmody, T., Walker, R., dela Cruz, A., et al. (2016). Demographic and clinical characteristics of current comorbid psychiatric disorders in a randomized clinical trial for adults with stimulant use disorders. Psychiatr. Res. 246, 136–141. doi:10.1016/j.psychres.2016.09.007
Keywords: cocaine use disorder, VACS index, comorbidity, mortality, hospitalization
Citation: Sanvisens A, Hernández-Rubio A, Zuluaga P, Fuster D, Papaseit E, Galan S, Farré M and Muga R (2021) Long-Term Outcomes of Patients With Cocaine Use Disorder: A 18-years Addiction Cohort Study. Front. Pharmacol. 12:625610. doi: 10.3389/fphar.2021.625610
Received: 03 November 2020; Accepted: 14 January 2021;
Published: 18 February 2021.
Edited by:
Qi Wang, Southern Medical University, ChinaReviewed by:
Yadong Guo, Central South University, ChinaCopyright © 2021 Sanvisens, Hernández-Rubio, Zuluaga, Fuster, Papaseit, Galan, Farré and Muga. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Robert Muga, cm11Z2EuZ2VybWFuc3RyaWFzQGdlbmNhdC5jYXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.