
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Pharmacol. , 30 April 2021
Sec. Drugs Outcomes Research and Policies
Volume 12 - 2021 | https://doi.org/10.3389/fphar.2021.612941
This article is part of the Research Topic Outcomes of Cardiovascular Drug Use in the Older Population View all 13 articles
 Armando Silva Almodóvar1,2
Armando Silva Almodóvar1,2 Milap C. Nahata1,3*
Milap C. Nahata1,3*Heart failure (HF) is associated with significant morbidity, mortality, compromised quality of life and socioeconomic burden worldwide. This chronic condition is becoming an increasingly important concern given the increased prevalence of HF among aging populations. Significant contributors toward escalating health care costs are emergency room visits and hospitalizations associated with HF. An important strategy to improve health care outcomes and reduce unnecessary costs is to identify and reduce the prescribing of potentially harmful medications (PHMs) among adults with HF. Previous studies in patients with HF found roughly 10–50% of them were prescribed at least one PHM in ambulatory care and inpatient health care settings. This opinion highlights recent findings from studies assessing prevalence of PHMs, associations between PHM prescribing and characteristics, and what can be done to improve patient outcomes and reduce the use of PHMs and associated health care costs in adults with HF.
Heart failure (HF) is associated with compromised quality of life, and significant morbidity, mortality, and socioeconomic burden worldwide. It is estimated that up to 7% of the population in some industrialized countries is diagnosed with HF (Savarese and Lund, 2017). A systematic review reported annual per patient cost of care ranged from $868 to $25,532 depending on the country (Lesyuk et al., 2018). Inpatient treatment of heart failure is estimated to comprise 44–96% of the overall cost of treatment (Lesyuk et al., 2018). Two-thirds of patients with HF experienced a rehospitalization within the first year hospital discharge in the US (Curtis et al., 2008). Reducing avoidable exacerbations of HF and optimizing medication regimens are necessary to mitigate avoidable health care utilization.
It is estimated that patients with HF utilize 7 prescriptions daily in addition to over-the-counter medications and supplements (Masoudi et al., 2005). Furthermore, one in two patients following a HF-related hospitalization utilized more than 10 prescriptions chronically (Unlu et al., 2019). It is estimated that 82% of patients using more than 7 medications may experience a significant drug-drug interaction (Goldberg et al., 1996). Additionally, medication related treatment failure and new medical problems may cost the US approximately $528.4 billion annually (Watanabe et al., 2018). Medication related problems such as drug-drug interactions, drug-disease interactions, and suboptimal dosing of medications can occur in fragmented health care systems where patients utilize multiple health care providers. This is problematic among patients with HF in whom worsening disease control can quickly lead to avoidable emergency department (ED) visits and hospitalizations.
The American Heart Association (AHA) and the European Society of Cardiology (ESC) published statements detailing a list of potentially harmful medications (PHMs) known to exacerbate or cause HF and included a detailed description of their quality of evidence (Page et al., 2016; El Hadidi et al., 2020). Additionally, heart failure management guidelines published by the AHA in collaboration with the American College of Cardiology and the Heart Failure Society of America (Yancy et al., 2017), the ESC (Ponikowski et al., 2016), the National Heart Foundation of Australia and Cardiac Society of Australia and New Zealand (Atherton et al., 2018), and the Japanese Circulation Society in collaboration with the Japanese Heart Failure Society (Tsutsui et al., 2019) identified certain medications that should be avoided among patients with HF. Despite these publications, little has been done to reduce prescribing of these medications among patients with HF through a systematic approach. Recent research has demonstrated that dedicated clinical decision support systems (CDSS) can improve guideline directed prescribing for the treatment of HF in ambulatory care settings (McKie et al., 2020) and electronic engagement of patients can also positively improve prescribing (Allen et al., 2021). However, a review by Kao et al. (Kao et al., 2020) reported on the need for greater innovation within electronic health records (EHRs), such as triggered alerts within a CDSS to reduce prescribing of PHMs for optimal management of patients with HF. This opinion reviewed evidence describing the prevalence of PHM prescribing among patients with HF and has suggested strategies about how health care systems can reduce prescribing of PHMs through triggered alerts within a CDSS and pharmacovigilance programs to reduce medication burden, and potentially avoidable health care utilization.
Since the publication of the AHA scientific statement, several studies have examined the prescribing of PHM among adults. Presently, the analysis of PHM prescribing among patients with HF can be divided into three settings: hospitalizations (Caughey et al., 2019; Alvarez et al., 2020; Goyal et al., 2020) administrative claims, (Alvarez et al., 2019; Silva Almodóvar and Nahata, 2020) and within an outpatient clinic (Brinker et al., 2020). These studies in large part assessed PHMs among patients in the United States (US) (Alvarez et al., 2019; Alvarez et al., 2020; Brinker et al., 2020; Goyal et al., 2020; Silva Almodóvar and Nahata, 2020) while one study assessed PHM prescribing in Australia (Caughey et al., 2019). Complete information on the studies assessed in this opinion can be found in Table 1.
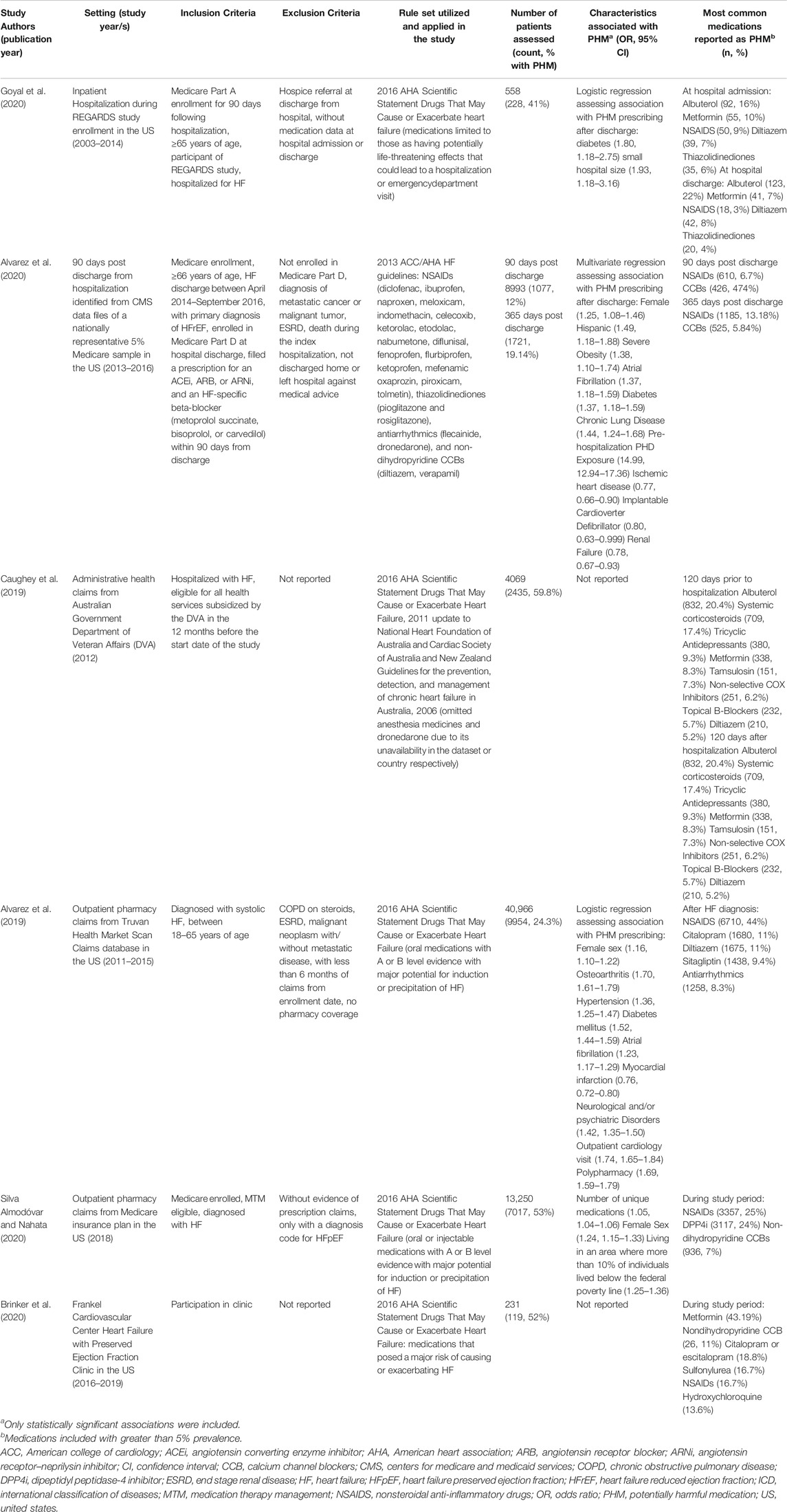
TABLE 1. Summary of studies reporting potentially harmful medication prescribing in patients with heart failure.
Goyal et al. (Goyal et al., 2020) assessed the prescribing of PHMs among older adults participating in a nationally representative cohort before and after a HF-related hospitalization. This study found 41% of individuals hospitalized for HF were using a PHM (Goyal et al., 2020). Upon discharge, 36% of patients still utilized a PHM. Alvarez et al. (Alvarez et al., 2020) conducted a similar analysis among Medicare patients with reduced ejection fraction HF (HFrEF) at 90 and 365 days after discharge from a HF-related hospitalization. This study found 12% of patients were with PHM at 90 days after a HF-related hospitalization and the prevalence increased to 19% at 1 year (Alvarez et al., 2020). It is important to note this study limited their identification of PHMs to medications mentioned in the 2013 ACC/AHA HF guideline potentially resulting in an underestimation of PHM prescribing (Alvarez et al., 2020).
Caughey et al. (Caughey et al., 2019) assessed PHM prescribing at 120 days before and after a HF-related hospitalization utilizing an Australian Department of Veteran Affairs claims database. Authors found almost 60% of their cohort were prescribed PHMs at 120 days prior to a HF-related hospitalization while 56% continued to be prescribed a PHM after 120 days (Caughey et al., 2019). The most common medications identified as PHMs in these studies included albuterol, metformin, non-dihydropyridine calcium channel blockers (CCBs), tricyclic antidepressants, systemic corticosteroids, and tamsulosin (Caughey et al., 2019; Alvarez et al., 2020; Goyal et al., 2020). These medications have been associated with an increased risk of hospitalization, increased (ED) visits, or exacerbation or precipitation of HF (Page et al., 2016).
Two studies assessed PHM prescribing by analyzing administrative claims data (Alvarez et al., 2019; Silva Almodóvar and Nahata, 2020). Alvarez et al. (Alvarez et al., 2019) found 24% of adults under 65 years of age with HFrEF were prescribed a PHM (Alvarez et al., 2019). A separate study using claims for one Medicare insurance plan assessed patients with HF who were enrolled in Medicare and eligible for Medication Therapy Management (MTM) services (Silva Almodóvar and Nahata, 2020). This study assessed medication prescribing in a Medicare cohort with significant comorbidity burden which was at greater risk for drug-drug and drug-disease interactions (Silva Almodóvar and Nahata, 2020). This study found 53% of patients were prescribed a PHM (Silva Almodóvar and Nahata, 2020). These studies may have underestimated the prevalence of PHM in their populations given they limited their PHMs to only medications with evidence derived from randomized clinical trials, meta-analyses, single randomized trials, or nonrandomized studies (Alvarez et al., 2019; Silva Almodóvar and Nahata, 2020). The most common PHMs prescribed in these studies were NSAIDs, nondihydropyridine CCBs, dipeptidyl peptidase-4 inhibitors (DPP4i), citalopram, specific antiarrhythmics, and thiazolidinediones (Alvarez et al., 2019; Silva Almodóvar and Nahata, 2020). In addition to the previously mentioned medications, use of NSAIDs, DPP4is, citalopram, antiarrhythmics, and thiazolidinediones among patients with HF may lead to a potentially avoidable hospitalization or ED visit (Page et al., 2016).
Finally, a study by Brinker et al. (Brinker et al., 2020) examined the prescribing of PHMs among a cohort with preserved ejection fraction HF (HFpEF) in one outpatient clinic. Approximately, 52% of patients were with a PHM. The most commonly prescribed PHMs in this study were metformin, non-dihydropyridine CCBs, and citalopram or escitalopram.
Examining patient characteristics associated with the prescribing of PHM may inform which patient populations would likely benefit most from targeted interventions. Goyal et al. (Goyal et al., 2020) reported patients with diabetes and those admitted to small hospitals with PHM prescribing had greater odds of having a PHM at discharge. Among Medicare patients that were hospitalized with HF, patients with PHM prescribing prior to the hospitalization, female sex, atrial fibrillation, severe obesity, diabetes, and chronic lung disease were with higher odds of PHM after a HF-related discharge; patients with ischemic heart disease, implantable cardioverter defibrillator, and renal failure were with significantly lower odds of PHM prescribing after a HF-related discharge (Alvarez et al., 2020).
In adults under 65 years of age, polypharmacy, use of loop diuretics, an outpatient cardiology visit, female sex, and diagnoses of osteoarthritis, hypertension, diabetes mellitus, atrial fibrillation, peripheral vascular disorder, neurological/psychiatric disorders, and chronic obstructive pulmonary disease were associated with prescribing of PHM; patients with history of a myocardial infarction were with lower odds of PHM prescribing (Alvarez et al., 2019). Among Medicare patients who were eligible for an MTM service, female sex, increasing number of prescriptions, residence in higher levels of poverty and greater number of prescribers and pharmacies were associated with PHM prescribing (Silva Almodóvar and Nahata, 2020). It is important to note the only characteristic of prescribers assessed was prescriber specialty. One study found that physician primary care providers prescribed the largest number of PHMs among MTM eligible patients with HF (Silva Almodóvar and Nahata, 2020).
Numerous studies have provided clear evidence for the prescribing of PHMs among patients with HF, which can lead to unnecessary health care utilization. Inpatient care represented 44–96% of the global cost of the management of HF; it is estimated to represent approximately 62–84% of the annual costs in the US. (Lesyuk et al., 2018) An obvious question is: what can be done to address this issue? One strategy would be to implement triggered alerts in an electronic health record’s CDSS using rule sets adapted from the AHA scientific statement, ESC’s position statement and heart failure prescribing guidelines to identify and prevent prescribing of PHMs in patients with HF. Smaller hospitals relative to larger hospitals may benefit more from this type of intervention given patients at these hospitals had greater odds of having a PHM (Goyal et al., 2020).
This type of triggered alert within a CDSS can draw the health care provider’s attention to the patient’s previously established diagnosis of HF, the offending drug’s potential for harm, and suggest a safer medication. This would allow the provider to make the most educated therapeutic decision at the point of prescribing. To the authors’ knowledge current electronic interventions are primarily focused on improving prescribing of medications meant to treat HF and research is needed to evaluate the use of these technologies to reduce rates of PHM prescribing. A previous systematic review found implementation of CDSS improved provider compliance with clinical practice related to the screening and treatment of cardiovascular related illnesses (Njie et al., 2015). McKie et al. (McKie et al., 2020) found CDSS significantly improved guideline recommended treatment of patients with HF in a primary care setting. However, another study in patients with HF in a hospital setting reported roughly 3.6 alerts per patient resulting in provider alert fatigue (Wadhwa et al., 2008). The risk for alert fatigue emphasizes the need to carefully design the triggered alerts with user feedback to ensure optimal uptake and efficacy.
In addition to the implementation of well-designed triggered alerts, dedicated pharmacovigilance programs need to be implemented to identify and resolve potential drug-drug interactions, drug-disease interactions, and adverse events. Targeted programs for PHMs among patients with heart failure can reduce prescribing of PHMs and thus reduce potentially avoidable health care utilization. As an example, the Centers for Medicare and Medicaid Services currently requires Medicare insurance plan providers to utilize MTM programs to optimize health outcomes and reduce the risk of medication related adverse events (Medication therapy management Centers for Medicare and Medicaid Services, 2020). MTM programs may incorporate automated algorithm driven electronic reviews and manual reviews of medication claims by health care providers to decrease and prevent prescribing of harmful medications.
It would be important for these programs to utilize health care providers with expertize in the comprehensive management of multiple concurrent medications as patients with heart failure and comorbidities such as diabetes, severe obesity, hypertension, atrial fibrillation, chronic lung disease, osteoarthritis, hypertension, peripheral vascular disorder, or neurological/psychiatric disorders had greater odds of using a PHM (Alvarez et al., 2019; Alvarez et al., 2020; Goyal et al., 2020). Presently, MTM services are largely provided by clinical pharmacists who evaluate medication regimens and communicate with patients and prescribers to improve medication use (Centers for Medicare and Medicaid Services, 2018). These programs can address medication use after prescribing, given they would have access to diagnostic and prescription claims data for patients that may have been siloed across different health care systems and pharmacies. These features are especially important as patients with multiple prescribers and with multiple pharmacies presented with greater odds of having a PHM (Silva Almodóvar and Nahata, 2020).
Wide adoption of these programs across health care systems and insurance plans can significantly improve their ability to reduce the prevalence of PHMs. Previous research found MTM programs to be especially helpful in improving medication adherence and prescribing of medications in patients with HF (Perloth et al., 2013). However, the effects of MTM programs on reducing contraindicated medications among patients with HF may depend on the type of insurance program (Buhl et al., 2017). Targeted reviews within these programs have been found effective in initiating a large number of medication changes to reduce adverse outcomes (Buhl et al., 2017; Ferries et al., 2019). Thus, implementation of targeted programs and adoption of MTM services among health care systems and payers such as insurance plans may reduce prevalence of PHMs, hospitalizations, and health care utilization among patients with HF.
The prevalence of HF is expected to increase by 46% by 2030 (Benjamin et al., 2017). Given 10–50% of patients with HF utilized at least one PHM, there is an urgent need to develop and implement efficient and effective tools and programs to optimize medication management of patients with HF (Alvarez et al., 2019; Caughey et al., 2019; Alvarez et al., 2020; Brinker et al., 2020; Goyal et al., 2020; Silva Almodóvar and Nahata, 2020). The implementation of triggered alerts targeting PHM medications among patients with HF within the CDSSs across all health care systems and pharmacovigilance programs including MTM among insurance plan providers are likely to reduce the prescribing of PHMs, and thus improve health outcomes and reduce unnecessary health care utilization among adults with HF.
MN conceived of the idea. ASA conducted the literature review. ASA took lead in the writing of the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that ASA’s position is funded by SinfoníaRx: a TRHC solution. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
The opinions expressed herein are solely those of the authors and do not reflect the opinions or views of TRHC, its companies, or its employees.
ASA is affiliated with SinfoníaRx.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Allen, L. A., Venechuk, G., McIlvennan, C. K., Page, R. L., Knoepke, C. E., Helmkamp, L. J., et al. (2021). An electronically delivered patient-activation tool for intensification of medications for chronic heart failure with reduced ejection fraction. Circulation 143 (5), 427–437. doi:10.1161/CIRCULATIONAHA.120.051863
Alvarez, P. A., Gao, Y., Girotra, S., Mentias, A., Briasoulis, A., and Vaughan Sarrazin, M. S. (2020). Potentially harmful drug prescription in elderly patients with heart failure with reduced ejection fraction. ESC Heart Fail. 7 (4), 1862–1871. doi:10.1002/ehf2.12752
Alvarez, P. A., Truong, C. N., Briasoulis, A., and Ganduglia-Cazaban, C. (2019). Prescription of potentially harmful drugs in young adults with heart failure and reduced ejection fraction. Am. J. Cardiol. 123 (9), 1458–1463. doi:10.1016/j.amjcard.2019.01.052
Atherton, J. J., Sindone, A., De Pasquale, C. G., Driscoll, A., MacDonald, P. S., Hopper, I., et al. (2018). National heart foundation of Australia and cardiac society of Australia and New Zealand: guidelines for the prevention, detection, and management of heart failure in Australia 2018. Heart Lung Circ. 27 (10), 1123–1208. doi:10.1016/j.hlc.2018.06.1042
Benjamin, E. J., Blaha, M. J., Chiuve, S. E., Cushman, M., Das, S. R., Deo, R., et al. (2017). Heart disease and stroke statistics-2017 update: a report from the American heart association, Circulation 135 (10):e146-e603. doi:10.1161/CIR.0000000000000485
Brinker, L. M., Konerman, M. C., Navid, P., Dorsch, M. P., McNamara, J., Willer, C. J., et al. (2020). Complex and potentially harmful medication patterns in heart failure with preserved ejection fraction. Am. J. Med. 134 (3):374–382. doi:10.1016/j.amjmed.2020.07.023
Buhl, A., Augustine, J., Taylor, A. M., Martin, R., and Warholak, T. L. (2017). Positive medication changes resulting from comprehensive and noncomprehensive medication reviews in a Medicare Part D population. Jmcp 23 (3), 388–394. doi:10.18553/jmcp.2017.23.3.388
Caughey, G. E., Shakib, S., Barratt, J. D., and Roughead, E. E. (2019). Use of medicines that may exacerbate heart failure in older adults: therapeutic complexity of multimorbidity. Drugs Aging 36 (5), 471–479. doi:10.1007/s40266-019-00645-0
Centers for Medicare and Medicaid Services (2018). Fact sheet summary of 2019 MTM programs. Available at: https://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovContra/Downloads/CY2019-MTM-Fact-Sheet.pdf (Accessed October 5, 2020).
Curtis, L. H., Whellan, D. J., Hammill, B. G., Hernandez, A. F., Anstrom, K. J., Shea, A. M., et al. (2008). Incidence and prevalence of heart failure in elderly persons, 1994-2003. Arch. Intern. Med. 168 (4), 418–424. doi:10.1001/archinternmed.2007.80
El Hadidi, S., Rosano, G., Tamargo, J., Agewall, S., Drexel, H., Kaski, JC., et al. (2020). Potentially inappropriate prescriptions in heart failure with reduced ejection fraction: ESC position statement on heart failure with reduced ejection fraction-specific inappropriate prescribing. Eur. Heart J. Cardiovasc. Pharmacother. pvaa 108 doi:10.1093/ehjcvp/pvaa108
Ferries, E., Dye, J. T., Hall, B., Ndehi, L., Schwab, P., and Vaccaro, J. (2019). Comparison of medication therapy management services and their effects on health care utilization and medication adherence. Jmcp 25 (6), 688–695. doi:10.18553/jmcp.2019.25.6.688
Goldberg, R. M., Mabee, J., Chan, L., and Wong, S. (1996). Drug-drug and drug-disease interactions in the ED: analysis of a high-risk population. Am. J. Emerg. Med. 14 (5), 447–450. doi:10.1016/S0735-6757(96)90147-3
Goyal, P., Kneifati-Hayek, J., Archambault, A., Mehta, K., Levitan, E. B., Chen, L., et al. (2020). Prescribing patterns of heart failure-exacerbating medications following a heart failure hospitalization. JACC: Heart Fail. 8 (1), 25–34. doi:10.1016/j.jchf.2019.08.007
Kao, D. P., Trinkley, K. E., and Lin, C.-T. (2020). Heart failure management innovation enabled by electronic health records. JACC: Heart Fail. 8 (3), 223–233. doi:10.1016/j.jchf.2019.09.008
Lesyuk, W., Kriza, C., and Kolominsky-Rabas, P. (2018). Cost-of-illness studies in heart failure: a systematic review 2004-2016. BMC Cardiovasc. Disord. 18 (1), 74. doi:10.1186/s12872-018-0815-3
Masoudi, F. A., Baillie, C. A., Wang, Y., Bradford, W. D., Steiner, J. F., Havranek, E. P., et al. (2005). The complexity and cost of drug regimens of older patients hospitalized with heart failure in the United States, 1998-2001. Arch. Intern. Med. 165 (18), 2069–2076. doi:10.1001/archinte.165.18.2069
McKie, P. M., Kor, D. J., Cook, D. A., Kessler, M. E., Carter, R. E., Wilson, P. M., et al. (2020). Computerized advisory decision support for cardiovascular diseases in primary care: a cluster randomized trial. Am. J. Med. 133 (6), 750–756. e2. doi:10.1016/j.amjmed.2019.10.039
Medication therapy management Centers for Medicare and Medicaid Services (2020). Available at: https://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovContra/MTM (Accessed September 30, 2020).
Njie, G. J., Proia, K. K., Thota, A. B., Finnie, R. K. C., Hopkins, D. P., Banks, S. M., et al. (2015). Clinical decision support systems and prevention. Am. J. Prev. Med. 49 (5), 784–795. doi:10.1016/j.amepre.2015.04.006
Page, R. L., O’Bryant, C. L., Cheng, D., Dow, T. J., Ky, B., Stein, C. M., et al. (2016). Drugs That May Cause or Exacerbate Heart Failure: a Scientific Statement From the American Heart Association [published correction appears in Circulation]. Circulation 134 (6), e32–e69. doi:10.1161/cir.0000000000000426
Perloth, D., Marrufo, G., Montesinos, A., Lewis, C., Dixit, A., Li, B., et al. (2013). Medication therapy management in chronically ill populations: final report. Burlingame, CA: Acumen LLC.
Ponikowski, P., Voors, A. A., Stefan, D. A., Bueno, H., Cleland, J. G. F., Coats, A. J. S., et al. (2016). ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 37 (Issue 27), 2129–2200. doi:10.1093/eurheartj/ehw128
Savarese, G., and Lund, L. H. (2017). Global public health burden of heart failure. Card. Fail. Rev. 03 (1), 7–11. doi:10.15420/cfr.2016:25:2
Silva Almodóvar, A., and Nahata, M. C. (2020). Potentially harmful medication use among Medicare patients with heart failure. Am J Cardiovasc Drugs. 20 (6). 603–610. doi:10.1007/s40256-020-00396-z
Tsutsui, H., Isobe, M., Ito, H., Ito, H., Okumura, K., Ono, M., et al. (2019). JCS 2017/JHFS 2017 guideline on diagnosis and treatment of acute and chronic heart failure ― digest version ―. Circ. J. 83 (10), 2084–2184. doi:10.1253/circj.CJ-19-0342
Unlu, O., Dharamdasani, T., Archambault, A., Diaz, I., Chen, L., Levitan, E., et al. (2019). Polypharmacy increases in prevalence and severity following a heart failure hospitalization. J. Am. Coll. Cardiol. 73 (9 Suppl. 1), 789. doi:10.1016/s0735-1097(19)31396-8http://www.onlinejacc.org/content/73/9_Supplement_1/789.abstract
Wadhwa, R., Fridsma, D. B., Saul, M. I., Penrod, L. E., Visweswaran, S., Cooper, G. F., et al. (2008). Analysis of a failed clinical decision support system for management of congestive heart failure. AMIA Annu. Symp. Proc. 2008, 773–777.
Watanabe, J. H., McInnis, T., and Hirsch, J. D. (2018). Cost of prescription drug-related morbidity and mortality. Ann. Pharmacother. 52 (9), 829–837. doi:10.1177/1060028018765159
Yancy, C. W., Jessup, M., Bozkurt, B., Butler, J., Casey, D. E., Colvin, M. M., et al. (2017). ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of cardiology/American heart association task force on clinical practice guidelines and the heart failure society of America. Circulation 136 (6), e137–e161. doi:10.1161/cir.0000000000000509
Keywords: heart failure, potentially harmful medication, health care utilization, clinical decision support systems, medication therapy management, pharmacovigilance
Citation: Silva Almodóvar A and Nahata MC (2021) Implementing Clinical Decision Support Tools and Pharmacovigilance to Reduce the Use of Potentially Harmful Medications and Health Care Costs in Adults With Heart Failure. Front. Pharmacol. 12:612941. doi: 10.3389/fphar.2021.612941
Received: 01 October 2020; Accepted: 03 March 2021;
Published: 30 April 2021.
Edited by:
Marleen Van Der Kaaij, Amstelland Hospital, NetherlandsReviewed by:
Natasa Duborija-Kovacevic, University of Montenegro, MontenegroCopyright © 2021 Silva Almodóvar and Nahata. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Milap C. Nahata, TmFoYXRhLjFAb3N1LmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.