 Bing Li
Bing Li Li Liang
Li Liang Jinmin Guo
Jinmin Guo
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pharmacol. , 03 April 2020
Sec. Drugs Outcomes Research and Policies
Volume 11 - 2020 | https://doi.org/10.3389/fphar.2020.00332
Background: Irritable bowel syndrome is a functional gastrointestinal disease. Evidence has suggested that probiotics may benefit IBS symptoms. However, clinical trials remain conflicting.
Aims: To implement a systematic review and meta-analysis of clinical trials regarding the efficacy and safety of probiotics for IBS patients.
Methods: We searched for relevant trials in Medline(1966 to Jan 2019), Embase(1974 to Jan 2019), the Cochrane Central Register of Controlled Trials(up to Jan 2019), the ClinicalTrials.gov trials register(up to Jan 2019), and Chinese Biomedical Literature Database(1978 to Jan 2019). Risk ratio (RR) and a 95% confidence interval (CI) were calculated for dichotomous outcomes. Standardized mean difference (SMD) and 95% CI were calculated for continuous outcomes.
Results: A total of 59 studies, including 6,761 patients, were obtained. The RR of the improvement or response with probiotics versus placebo was 1.52 (95% CI 1.32–1.76), with significant heterogeneity (I2 = 71%, P < 0.001). The SMD of Probiotics in improving global IBS symptoms vs. Placebo was -1.8(95% CI -0.30 to -0.06), with significant heterogeneity (I2 = 65%, P < 0.001). It was impossible to draw a determinate conclusion. However, there were differences in subgroup analyses of probiotics type, dose, treatment duration, and geographic position. Probiotics seem to be safe by the analysis of adverse events(RR = 1.07; 95% CI 0.92–1.24; I2 = 0, P = 0.83).
Conclusion: Probiotics are effective and safe for IBS patients. Single probiotics with a higher dose (daily dose of probiotics ≥1010) and shorter duration (< 8 weeks) seem to be a better choice, but it still needs more trials to prove it.
Irritable bowel syndrome (IBS) is a common functional gastrointestinal disorder associated with abdominal pain, bloating and altered bowel habits (Drossman et al., 2002). It affects 11% of the world-wide population (Lovell and Ford, 2012). IBS reduces health-related quality of life (HRQOL) (Gralnek et al., 2000; Wang et al., 2012) and leads to a significant economic healthcare burden. Although the exact etiology and pathogenesis underlying IBS are still incompletely understood, studies show that IBS was associated with the gastrointestinal (GI) microbiota, chronic low-grade mucosal inflammation, altered regulation of the gut-brain axis, immune function, visceral hypersensitivity, and psychosocial factors(Parkes et al., 2008; Dupont, 2014; Hayes et al., 2014). Since there is no effective cure for IBS, the treatment focuses on alleviating the particular symptoms. New therapeutic options for IBS include tricyclic antidepressants (Rahimi et al., 2009), spasmolytics (Tack et al., 2016), selective serotonin reuptake inhibitors (Bundeff and Woodis, 2014), lubiprostone (Chang et al., 2016) and linaclotide (Chey et al., 2011), and 5-hydroxytryptamine type-3 antagonists such as ramosetron and alosetron (Andresen et al., 2008). However, current treatments are not very useful or may cause adverse reactions (Trinkley and Nahata, 2014).
Evidence (Durban et al., 2013; Jalanka-Tuovinen et al., 2014) has suggested that intestinal microorganisms play an important role in IBS, as numerous studies have indicated that an irregular composition or metabolic activity of intestinal flora in patients with IBS (Simrén et al., 2013; Spiller et al., 2016; Thijssen et al., 2016; Hod et al., 2017; Shin et al., 2018). Therefore, the regulation of the gut microbiota by probiotics is a promising treatment for IBS (Hyland et al., 2014). Probiotics can improve intestinal flora and limit colonization of pathogenic bacteria (Guarner et al., 2012). Investigators have performed numerous clinical trials to assess the efficacy of probiotics for IBS. However, the conclusions have been controversial. Some trials have suggested that probiotics can improve global IBS symptoms (Lyra et al., 2016). Others have demonstrated no effect (Charbonneau et al., 2013). Several articles have not found an apparent effect of probiotics on global IBS symptoms, but have found improvement of individual IBS symptoms (Sisson et al., 2014). Therefore, we conducted this meta-analysis to examine the efficacy of global IBS symptoms improvement, global symptoms scores, and individual symptom scores, such as abdominal pain and bloating. Additionally, this study evaluated the safety of probiotics.
We included all eligible randomized placebo-controlled, trials (RCTs) of probiotics treatment in adult IBS. We searched Medline(1966 to Jan 2019), Embase(1974 to Jan 2019), the Cochrane Central Register of Controlled Trials(up to Jan 2019), the ClinicalTrials.gov trials register(up to Jan 2019), and Chinese Biomedical Literature Database(CBM) (1978 to Jan 2019) for relevant trials. We used the terms “probiotics” and “irritable bowel syndrome” both as medical subject heading (Mesh) and free text terms. The exact search strategy in Medline was (“probiotics”[MeSH Terms] OR “probiotics”[Title/Abstract]) AND (“irritable bowel syndrome”[MeSH Terms] OR “irritable bowel syndrome”[Title/Abstract]) AND (“randomized controlled trial” [pt] OR “randomized controlled trial” [tiab]).
We used the following eligibility criteria: (1) the studies were randomized controlled trials (RCTs) comparing probiotics with placebo; (2) diagnostic criteria included but were not limited to the Manning criteria, and Rome I, Rome II, or Rome III criteria. We did not exclude trials in which patients were stated to be diagnosed with IBS but no diagnostic criteria were described; (3) the age of participants were ≥ 18 years; (4) minimum treatment duration was 7 days. Studies were excluded if they met: (1) studies with inadequate information; (2) probiotics along with other drugs; (3) control group was not placebo; (4) data were not available after contacting the authors. There were no language limitation. Articles in foreign language were translated as needed.
The primary outcomes were the efficacy of probiotics on global IBS symptoms improvement or response to therapy. Secondary outcomes involved the effect on global symptoms scores and individual symptom scores, such as abdominal pain and bloating. The safety of probiotics was also evaluated.
Two reviewers extracted data from included trials independently. All data was inspected by a third reviewer. Any divergence was solved by consensus. Following data were extracted:author publication year, country, type of IBS(%), diagnostic criteria for IBS, recruitment, sample size, number of male/female, age, probiotic, dosage, duration of therapy, criteria to define symptom improvement or response, and outcomes.
Two reviewers performed the assessment of study quality independently. Disagreements were solved by discussion. The risk of bias were evaluated according to the Cochrane handbook (Higgins and Green, 2011). Random sequence generation and allocation concealment(selection bias), blinding of participants and personnel(performance bias), blinding of outcome assessment(detection bias), incomplete outcome data(attrition bias), selective reporting(reporting bias), and other biases were assessed.
Random effects model was used (Dersimonian and Laird, 1986) to get a conservative estimation for the effect. As dichotomous outcomes, the efficacy on global IBS symptoms improvement or overall symptom response and the safety of probiotics were evaluated by RR(risk ratio) and 95% CIs(confidence intervals). As continuous outcomes, global symptoms scores, and individual symptoms scores were assessed using standardised mean difference (SMD) and corresponding 95% CIs. A negative SMD was defined to indicate beneficial effects of probiotics compared with placebo for outcomes. Subgroup analyses based on probiotic type, dosage, and treatment duration were conducted.
Heterogeneity was tested by I2 statistic and the Cochran Q-test. I2 ≥ 50 and P < 0.10 were considered as a significant heterogeneity (Higgins et al., 2003). When there was significant heterogeneity, sensitivity analyses were conducted to give possible explanation. Review Manager version 5.3.5 (the Nordic Cochrane Center, Copenhagen, Denmark) was used to obtain forest plots of RRs and SMDs Egger test (Egger et al., 1997) (P < 0.10 defined existence of possible publication bias) and funnel plots was calculated by Stata Statistical Software: Release 13 (StataCorp LP; College Station, TX).
Based on network searching, a total of 4,830 citations were retrieved. By removing duplicates and screening titles and abstracts, 220 studies remained to be relevant (Figure 1). Excluding 161 studies for diverse reasons, 59 studies (Gade and Thorn, 1989; Nobaek et al., 2000; Niedzielin et al., 2001; Kim et al., 2003; Kajander et al., 2005; Kim et al., 2005; Niv et al., 2005; O'Mahony et al., 2005; Kim et al., 2006; Simren and Lindh, 2006; Whorwell et al., 2006; Guyonnet et al., 2007; Drouault-Holowacz et al., 2008; Enck et al., 2008; Kajander et al., 2008; Sinn et al., 2008; Zeng et al., 2008; Agrawal et al., 2009; Enck et al., 2009; Hong et al., 2009; Williams et al., 2009; Simrén et al., 2010; Choi et al., 2011; Guglielmetti et al., 2011; Michail and Kenche, 2011; Sondergaard et al., 2011; Cha et al., 2012; Cui and Hu, 2012; Dapoigny et al., 2012; Ducrotte et al., 2012; Farup et al., 2012; Kruis et al., 2012; Amirimani et al., 2013; Begtrup et al., 2013; Charbonneau et al., 2013; Roberts et al., 2013; Abbas et al., 2014; Jafari et al., 2014; Lorenzo-Zuniga et al., 2014; Ludidi et al., 2014; Pedersen et al., 2014; Shavakhi et al., 2014; Sisson et al., 2014; Stevenson et al., 2014; Yoon et al., 2014; Faghihi et al., 2015; Pineton de Chambrun et al., 2015; Yoon et al., 2015; Lyra et al., 2016; Majeed et al., 2016; Mezzasalma et al., 2016; Spiller et al., 2016; Thijssen et al., 2016; Hod et al., 2017; Ishaque et al., 2018; Khodadoostan et al., 2018; Kim et al., 2018; Preston et al., 2018; Sun et al., 2018), which contained 6,721 participants, were eligible evaluating. The agreement between the two researchers was well established (kappa value = 0.91). The characteristics of the included RCTs are presented in Table 1. The risk of bias was shown in Figure 2 and Figure 3. Twenty-three studies did not describe the details of the sequence generation process (Nobaek et al., 2000; Niedzielin et al., 2001; Niv et al., 2005; Simren and Lindh, 2006; Whorwell et al., 2006; Guyonnet et al., 2007; Enck et al., 2008; Zeng et al., 2008; Agrawal et al., 2009; Enck et al., 2009; Williams et al., 2009; Cui and Hu, 2012; Dapoigny et al., 2012; Charbonneau et al., 2013; Jafari et al., 2014; Ludidi et al., 2014; Pedersen et al., 2014; Sisson et al., 2014; Faghihi et al., 2015; Thijssen et al., 2016; Kim et al., 2018; Preston et al., 2018; Sun et al., 2018), and 35 studies did not describe the method of allocation concealment (Gade and Thorn, 1989; Nobaek et al., 2000; Niedzielin et al., 2001; Kajander et al., 2005; Niv et al., 2005; O'Mahony et al., 2005; Kim et al., 2006; Simren and Lindh, 2006; Whorwell et al., 2006; Guyonnet et al., 2007; Enck et al., 2008; Zeng et al., 2008; Agrawal et al., 2009; Enck et al., 2009; Williams et al., 2009; Choi et al., 2011; Cha et al., 2012; Cui and Hu, 2012; Dapoigny et al., 2012; Amirimani et al., 2013; Charbonneau et al., 2013; Jafari et al., 2014; Ludidi et al., 2014; Pedersen et al., 2014; Shavakhi et al., 2014; Stevenson et al., 2014; Yoon et al., 2014; Yoon et al., 2015; Majeed et al., 2016; Thijssen et al., 2016; Hod et al., 2017; Ishaque et al., 2018; Khodadoostan et al., 2018; Preston et al., 2018; Sun et al., 2018), which lead to an unclear risk of selection bias. The risk of blinding the participants and personnel was low, except two studies (Zeng et al., 2008; Pedersen et al., 2014) were at high risk and one (Cui and Hu, 2012) was unclear. The risk of outcome assessment was mostly unclear. However, one study (Pedersen et al., 2014) was an unblinded controlled trial, leading to a high risk of performance and detection bias. Attrition bias, reporting bias, and other biases were low.
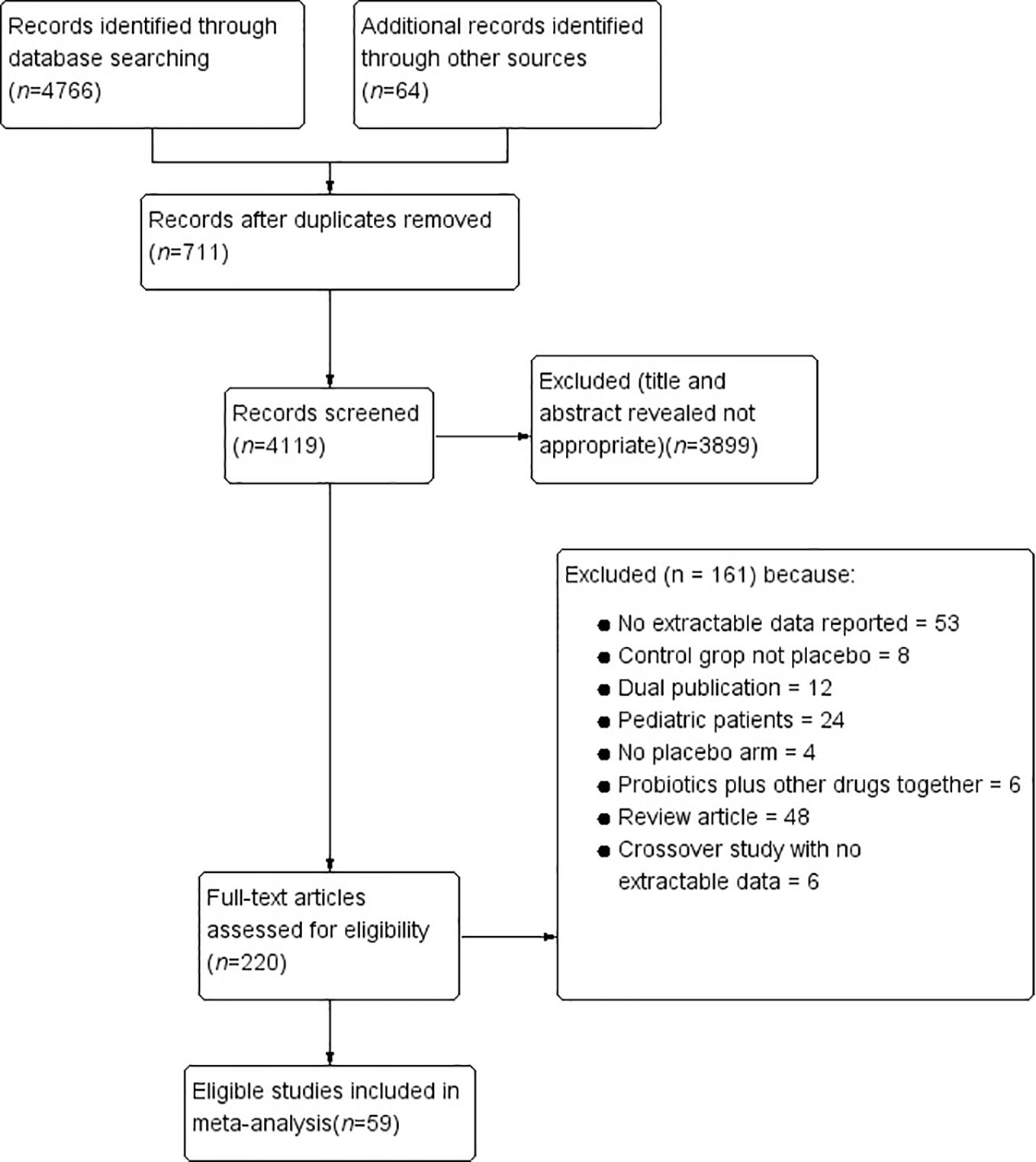
Figure 1 Flow diagram of the study selection process.
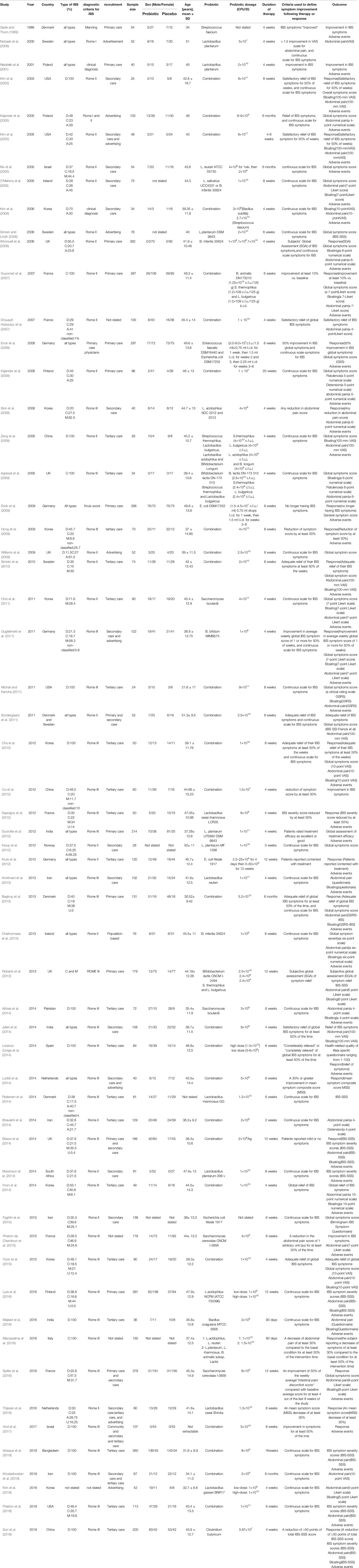
Table 1 Characteristics of randomized controlled trials of probiotics versus placebo in irritable bowel syndrome.

Figure 2 Risk of bias.
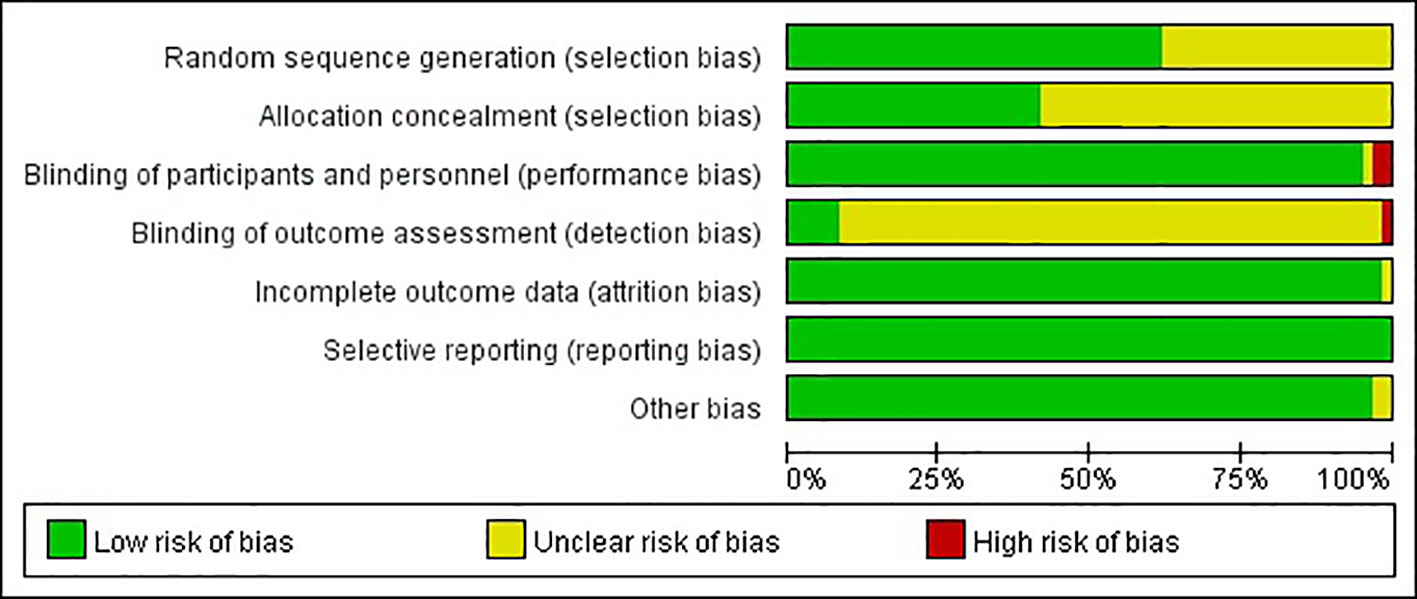
Figure 3 Risk of bias summary.
Thirty-five RCTs (Gade and Thorn, 1989; Nobaek et al., 2000; Niedzielin et al., 2001; Kim et al., 2003; Kajander et al., 2005; Kim et al., 2005; Whorwell et al., 2006; Guyonnet et al., 2007; Drouault-Holowacz et al., 2008; Enck et al., 2008; Sinn et al., 2008; Enck et al., 2009; Hong et al., 2009; Simrén et al., 2010; Guglielmetti et al., 2011; Sondergaard et al., 2011; Cha et al., 2012; Cui and Hu, 2012; Dapoigny et al., 2012; Ducrotte et al., 2012; Kruis et al., 2012; Begtrup et al., 2013; Roberts et al., 2013; Jafari et al., 2014; Lorenzo-Zuniga et al., 2014; Ludidi et al., 2014; Sisson et al., 2014; Yoon et al., 2014; Pineton de Chambrun et al., 2015; Yoon et al., 2015; Spiller et al., 2016; Mezzasalma et al., 2016; Thijssen et al., 2016; Hod et al., 2017; Sun et al., 2018) with 4,392 patients reported overall IBS symptoms improvement or response as a dichotomous outcome. There were two (Lorenzo-Zuniga et al., 2014; Mezzasalma et al., 2016) of these RCTs examining two different dose groups and one (Whorwell et al., 2006) examining three different dose groups. One (Gade and Thorn, 1989) RCT did not mention the dose of probiotics, so it was not included in the subgroup analysis of probiotics dose. Overall, 1,171(49.5%) of 2,367 patients in the group of probiotics declared symptoms improvement or response after therapy, compared with 644 (31.8%) of 2,025 in the placebo group. The RR of IBS symptoms improvement or response was 1.52(95% CI 1.32–1.76), with high heterogeneity (I2 = 71%, P < 0.001; Figure 4). The funnel plot suggested the existence of asymmetry (Egger test, P = 0.094; Figure S1), indicating possible publication bias. While 19 RCTs (Kim et al., 2003; Kajander et al., 2005; Kim et al., 2005; Drouault-Holowacz et al., 2008; Sinn et al., 2008; Hong et al., 2009; Simrén et al., 2010; Guglielmetti et al., 2011; Sondergaard et al., 2011; Ducrotte et al., 2012; Kruis et al., 2012; Begtrup et al., 2013; Roberts et al., 2013; Sisson et al., 2014; Lorenzo-Zuniga et al., 2014; Pineton de Chambrun et al., 2015; Mezzasalma et al., 2016; Spiller et al., 2016; Hod et al., 2017) with low bias risk were assessed, the effect was still significant (RR = 1.59; 95% CI 1.25–2.04).
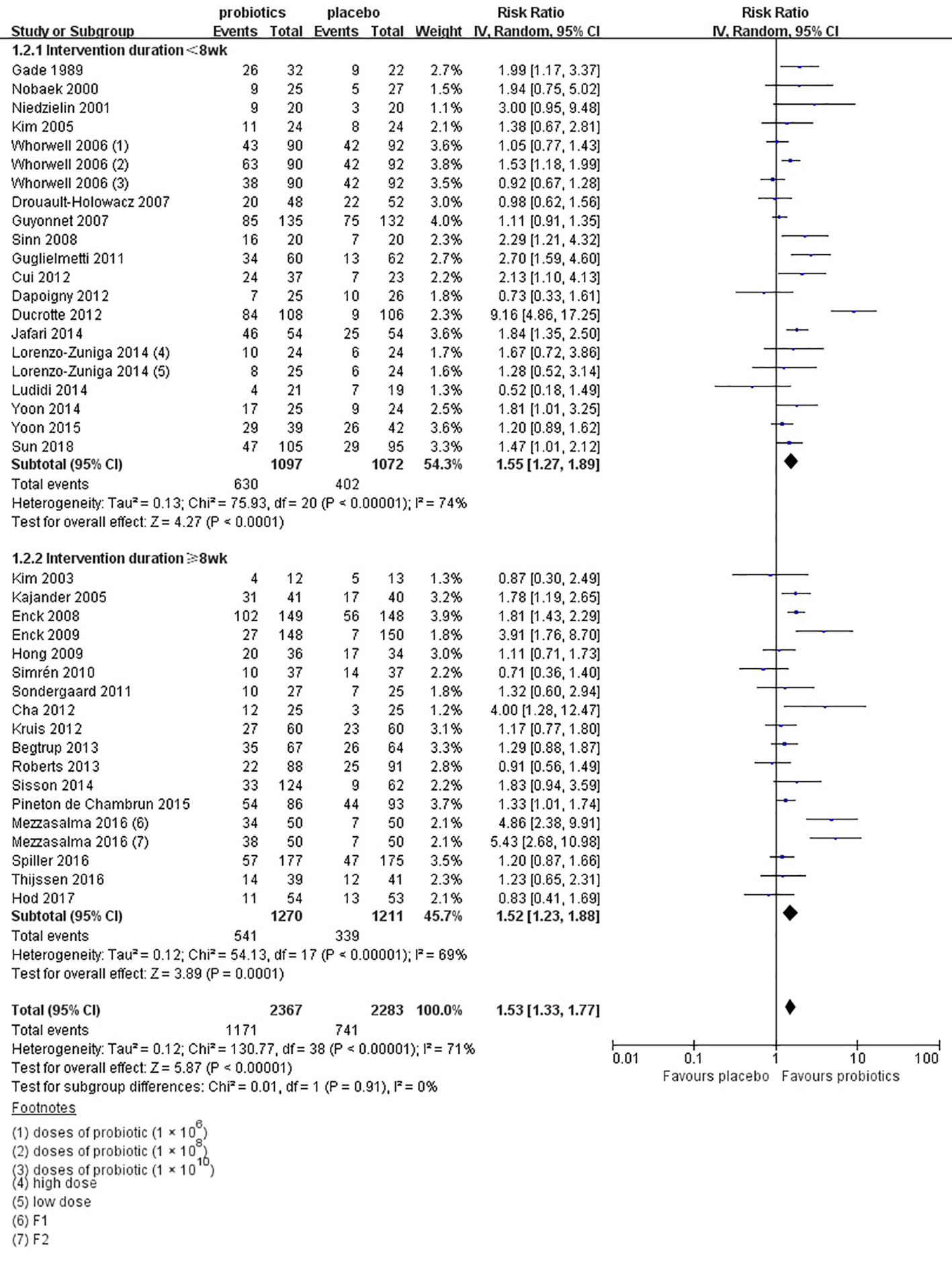
Figure 4 Forest plot of efficacy on IBS symptoms improvement or respond: subgroup of probiotics duration.
In the subgroup of duration, 18 studies (Gade and Thorn, 1989; Nobaek et al., 2000; Niedzielin et al., 2001; Kim et al., 2005; Whorwell et al., 2006; Guyonnet et al., 2007; Drouault-Holowacz et al., 2008; Sinn et al., 2008; Guglielmetti et al., 2011; Cui and Hu, 2012; Dapoigny et al., 2012; Ducrotte et al., 2012; Jafari et al., 2014; Lorenzo-Zuniga et al., 2014; Ludidi et al., 2014; Yoon et al., 2014; Yoon et al., 2015; Sun et al., 2018) evaluated a shorter duration (< 8 weeks) and 17 studies (Kim et al., 2003; Kajander et al., 2005; Enck et al., 2008; Enck et al., 2009; Hong et al., 2009; Simrén et al., 2010; Sondergaard et al., 2011; Cha et al., 2012; Kruis et al., 2012; Begtrup et al., 2013; Roberts et al., 2013; Sisson et al., 2014; Pineton de Chambrun et al., 2015; Mezzasalma et al., 2016; Spiller et al., 2016; Thijssen et al., 2016; Hod et al., 2017) used a longer duration (≥ 8 weeks). The RR of group with less than 8 weeks was 1.55 (95% CI 1.27–1.89; Figure 4), and the RR of group with more than 8 weeks was 1.52 (95% CI 1.23–1.88), with significant heterogeneity (I2 = 74%, P < 0.01; I2 = 69%, P < 0.01, respectively). In the subgroup of probiotics dose, high doses (daily dose of probiotics ≥ 1010) were assessed in 21 trials (Niedzielin et al., 2001; Kim et al., 2003; Kim et al., 2005; Whorwell et al., 2006; Guyonnet et al., 2007; Drouault-Holowacz et al., 2008; Hong et al., 2009; Simrén et al., 2010; Sondergaard et al., 2011; Cha et al., 2012; Ducrotte et al., 2012; Kruis et al., 2012; Begtrup et al., 2013; Roberts et al., 2013; Sisson et al., 2014; Lorenzo-Zuniga et al., 2014; Yoon et al., 2014; Yoon et al., 2015; Mezzasalma et al., 2016; Thijssen et al., 2016; Hod et al., 2017). A significant effect on symptoms (RR = 1.51; 95% CI 1.20–1.91; Figure S2) and statistically significant heterogeneity (I2 = 77%, P < 0.01) were suggested. Low doses (daily dose of probiotics < 1010) were evaluated in 15 trials (Nobaek et al., 2000; Kajander et al., 2005; Whorwell et al., 2006; Enck et al., 2008; Sinn et al., 2008; Enck et al., 2009; Guglielmetti et al., 2011; Cui and Hu, 2012; Dapoigny et al., 2012; Jafari et al., 2014; Lorenzo-Zuniga et al., 2014; Ludidi et al., 2014; Pineton de Chambrun et al., 2015; Spiller et al., 2016; Sun et al., 2018). A significant effect on symptoms (RR = 1.56; 95% CI 1.33–1.83) and significant heterogeneity were also detected (I2 = 54%, P < 0.01). In the subgroup of probiotics type, there were 15 studies using single probiotics (Gade and Thorn, 1989; Nobaek et al., 2000; Niedzielin et al., 2001; Whorwell et al., 2006; Sinn et al., 2008; Enck et al., 2009; Guglielmetti et al., 2011; Dapoigny et al., 2012; Ducrotte et al., 2012; Kruis et al., 2012; Pineton de Chambrun et al., 2015; Mezzasalma et al., 2016; Spiller et al., 2016; Thijssen et al., 2016; Sun et al., 2018) and 21 studies using combination probiotics (Kim et al., 2003; Kajander et al., 2005; Kim et al., 2005; Guyonnet et al., 2007; Drouault-Holowacz et al., 2008; Enck et al., 2008; Hong et al., 2009; Simrén et al., 2010; Sondergaard et al., 2011; Cha et al., 2012; Cui and Hu, 2012; Begtrup et al., 2013; Roberts et al., 2013; Jafari et al., 2014; Lorenzo-Zuniga et al., 2014; Ludidi et al., 2014; Sisson et al., 2014; Yoon et al., 2014; Yoon et al., 2015; Mezzasalma et al., 2016; Hod et al., 2017). The RR of single and combination group was 1.76 (95% CI 1.37–2.25; Figure S3) and 1.39 (95% CI 1.18–1.65), respectively. The I2 of the single probiotics subgroup was 69% (P < 0.01), and combination probiotics subgroup was 60% (P < 0.01), suggesting statistically significant heterogeneity. In the subgroup of geographic position, we assigned 2 trials (Kim et al., 2003; Kim et al., 2005) in USA to the North America group; five comparisons of three separate papers (Whorwell et al., 2006; Roberts et al., 2013; Sisson et al., 2014) in UK, five trials (Guyonnet et al., 2007; Drouault-Holowacz et al., 2008; Dapoigny et al., 2012; Pineton de Chambrun et al., 2015; Spiller et al., 2016) in France, and two trials (Ludidi et al., 2014; Thijssen et al., 2016) in Netherlands to the Western Europe group; two comparisons of one papers (Lorenzo-Zuniga et al., 2014) in Spain and two comparisons of one papers (Mezzasalma et al., 2016) in Italy to the South Europe group; two trials (Gade and Thorn, 1989; Begtrup et al., 2013) in Denmark, two trials (Nobaek et al., 2000; Simrén et al., 2010) in Sweden, one trials (Sondergaard et al., 2011) in Denmark and Sweden, and one trials (Kajander et al., 2005) in Finland to the Northern Europe group; one trials (Niedzielin et al., 2001) in Poland and four trials (Enck et al., 2008; Enck et al., 2009; Guglielmetti et al., 2011; Kruis et al., 2012) in Germany to the Central Europe group; five trials (Sinn et al., 2008; Hong et al., 2009; Cha et al., 2012; Yoon et al., 2014; Yoon et al., 2015) in Korea and two trials (Cui and Hu, 2012; Sun et al., 2018) in China to the East Asian group; one trials (Hod et al., 2017) in Israel to the West Asian group; and two trials (Ducrotte et al., 2012; Jafari et al., 2014) in India to the South Asian group. There was a statistically significant benefit in favor of probiotics in North America group (RR = 1.19; 95% CI 0.66–2.15; Figure 5), with no significant heterogeneity noted between the studies(I2 = 0%, P = 0.48), West Europe group(RR = 1.15; 95% CI 1.01–1.30; I2 = 25%, P = 0.20), Northern Europe group(RR = 1.45; 95% CI 1.10–1.91; I2 = 33%, P = 0.19) and East Asian group(RR = 1.55; 95% CI 1.21–1.98; I2 = 39%, P = 0.13).
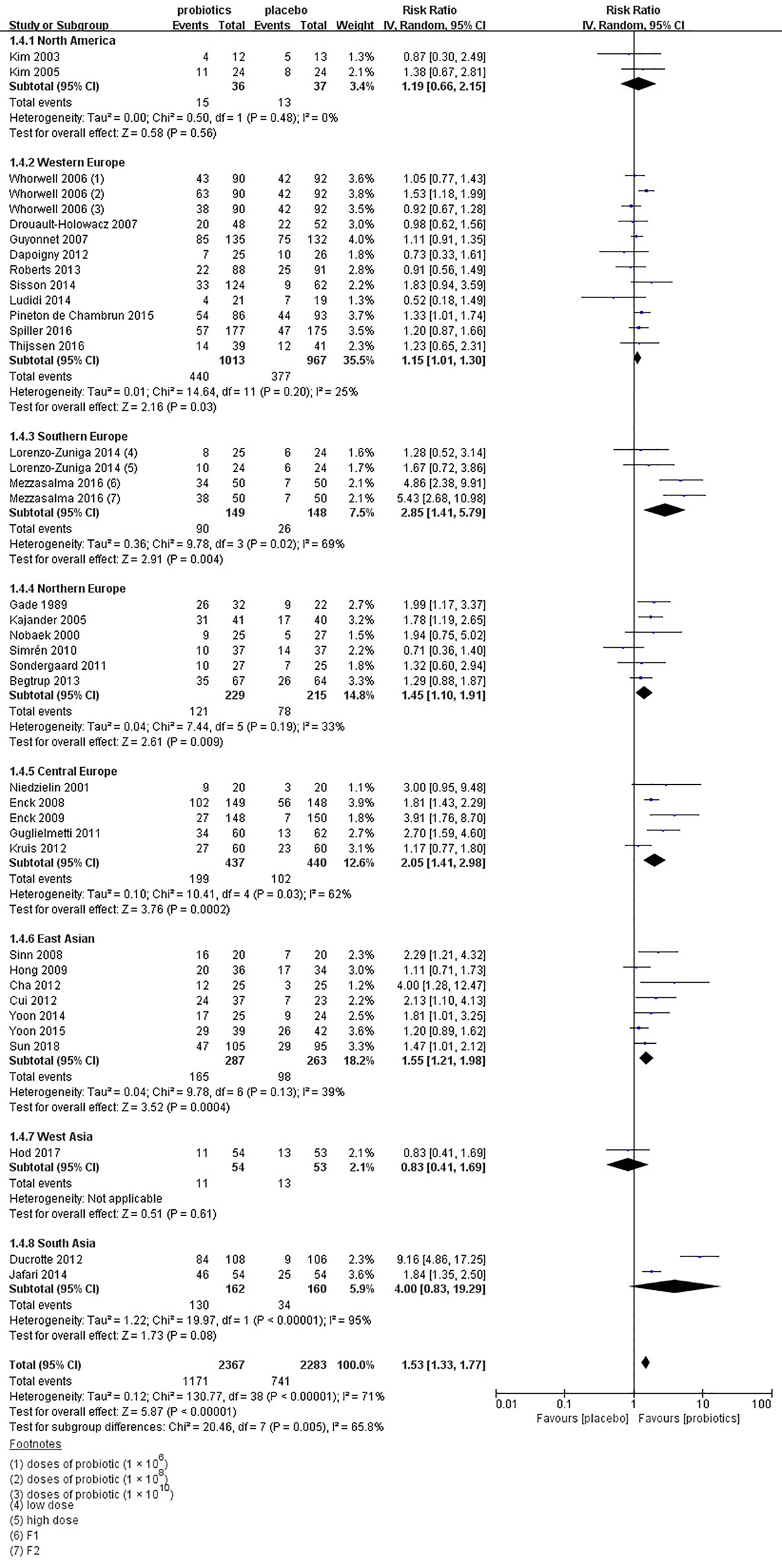
Figure 5 Forest plot of efficacy of probiotics on IBS symptoms improvement or respond: subgroup of geographic position.
There were 29 separate trials (Kim et al., 2003; Kajander et al., 2005; Niv et al., 2005; O'Mahony et al., 2005; Simren and Lindh, 2006; Whorwell et al., 2006; Kajander et al., 2008; Zeng et al., 2008; Agrawal et al., 2009; Williams et al., 2009; Simrén et al., 2010; Choi et al., 2011; Guglielmetti et al., 2011; Michail and Kenche, 2011; Sondergaard et al., 2011; Cha et al., 2012; Farup et al., 2012; Charbonneau et al., 2013; Begtrup et al., 2013; Roberts et al., 2013; Sisson et al., 2014; Pedersen et al., 2014; Stevenson et al., 2014; Faghihi et al., 2015; Yoon et al., 2015; Lyra et al., 2016; Spiller et al., 2016; Ishaque et al., 2018; Sun et al., 2018) including 35 comparisons with 3,726 patients reporting the efficacy of probiotics on global IBS symptoms scores. One (Spiller et al., 2016) of these RCTs examining two different dose groups and one (Whorwell et al., 2006) examining three different dose groups. There was a trial (Faghihi et al., 2015) did not mention the dose of probiotics, so it was not included in the subgroup analysis of probiotics dose. Two types of probiotics were used in one trial (O'Mahony et al., 2005), and three subtypes of IBS, including IBS with diarrhea (IBS-D), IBS with constipation (IBS-C), and IBS with mixed patterns of constipation and diarrhea (IBS-M), were detected separately in one RCT (Spiller et al., 2016). Probiotics had a statistically significant effect on improving the global IBS symptoms vs. placebo (SMD = -1.8; 95% CI -0.30 to -0.06; Figure 6). Heterogeneity was significant (I2 = 65%, P < 0.001). There was no significant asymmetry in funnel plot (Egger test, P = 0.689; Figure S4), indicating no proof of publication bias.
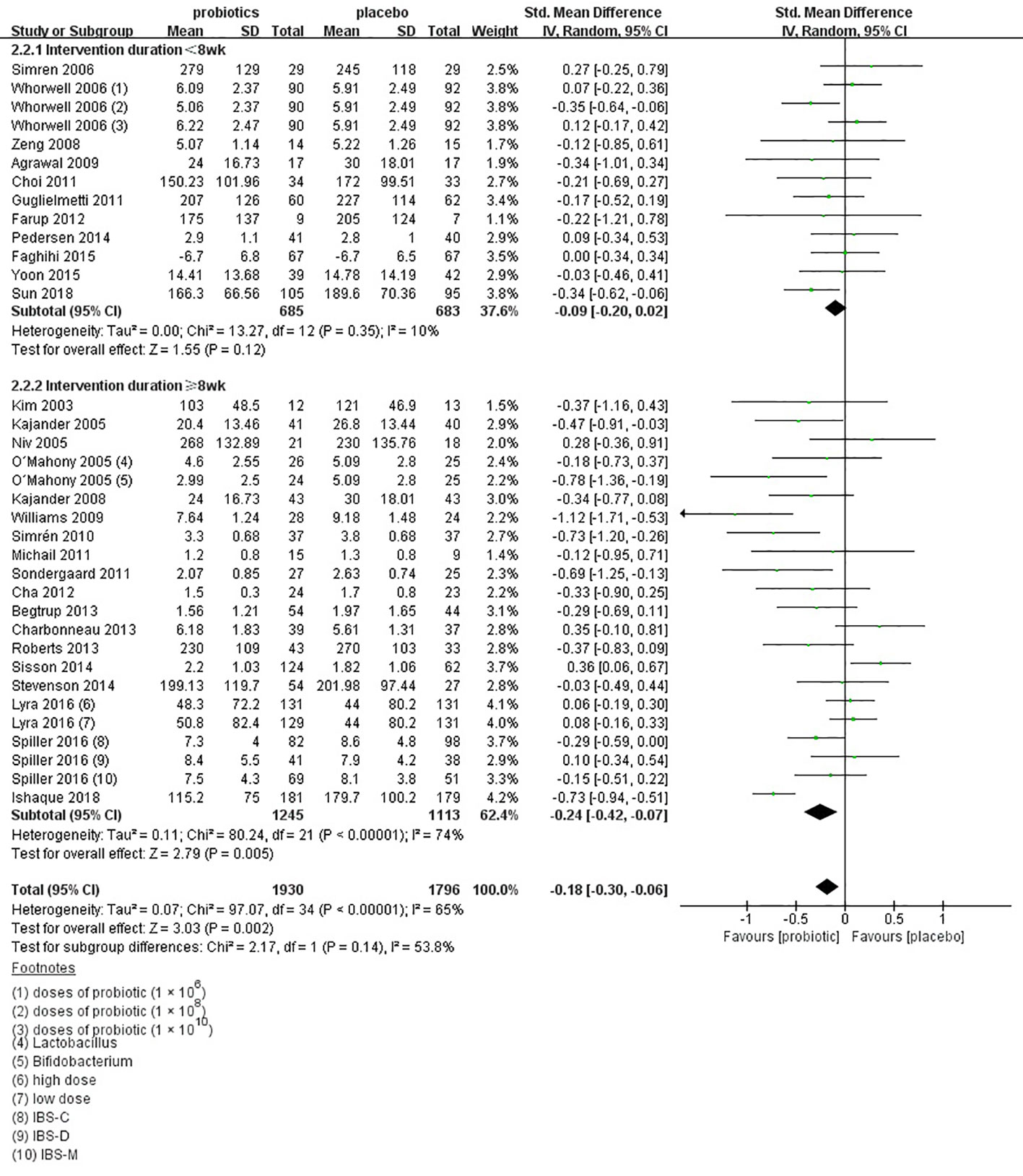
Figure 6 Forest plot of efficacy on global IBS symptoms scores: subgroup of probiotics duration.
In the subgroup of duration, 11 comparisons (Simren and Lindh, 2006; Whorwell et al., 2006; Zeng et al., 2008; Agrawal et al., 2009; Choi et al., 2011; Guglielmetti et al., 2011; Farup et al., 2012; Pedersen et al., 2014; Faghihi et al., 2015; Yoon et al., 2015; Sun et al., 2018) evaluated a shorter treatment duration (< 8 weeks). There was a beneficial effect on global IBS symptoms scores with probiotics (SMD -0.09; 95% CI -0.20 to 0.02) and low heterogeneity was found (I2 = 10%, P = 0.12). In the subgroup of probiotics dose, no significant differences were found, as shown in Figure S5. In the subgroup of probiotics type, 14 comparisons (Niv et al., 2005; O'Mahony et al., 2005; Simren and Lindh, 2006; Whorwell et al., 2006; Choi et al., 2011; Guglielmetti et al., 2011; Farup et al., 2012; Charbonneau et al., 2013; Pedersen et al., 2014; Stevenson et al., 2014; Faghihi et al., 2015; Lyra et al., 2016; Spiller et al., 2016; Sun et al., 2018) using single probiotics were found a beneficial efficacy on global IBS symptoms scores (SMD -0.06; 95% CI -0.16 to 0.14; Figure 7), with low heterogeneity (I2 = 33%, P = 0.12). In the subgroup of geographic position, we assigned 2 trials (Kim et al., 2003; Michail and Kenche, 2011) in USA to the North America group; seven comparisons of five separate papers (Whorwell et al., 2006; Agrawal et al., 2009; Williams et al., 2009; Roberts et al., 2013; Sisson et al., 2014) in UK, three comparisons of 1 papers (Spiller et al., 2016) in France, and three comparisons of two separate papers (O'Mahony et al., 2005; Charbonneau et al., 2013) in Ireland to the Western Europe group; two trials (Begtrup et al., 2013; Pedersen et al., 2014) in Denmark, two trials (Simren and Lindh, 2006; Simrén et al., 2010) in Sweden, one trials (Sondergaard et al., 2011) in Denmark and Sweden, four comparisons of three papers (Kajander et al., 2005; Kajander et al., 2008; Lyra et al., 2016) in Finland, and one trials (Farup et al., 2012) in Norway to the Northern Europe group; one trials (Guglielmetti et al., 2011) in Germany to the Central Europe group; three trials (Choi et al., 2011; Cha et al., 2012; Yoon et al., 2015) in Korea and two trials (Zeng et al., 2008; Sun et al., 2018) in China to the East Asian group; one trials (Niv et al., 2005) in Israel and one trials (Faghihi et al., 2015) in Iran to the West Asian group; and one trials (Ishaque et al., 2018) in Bangladesh to the South Asian group; and one trials (Stevenson et al., 2014) in South Africa to the South Africa group. There was a statistically significant benefit in favor of probiotics in North America group (SMD -0.25; 95% CI -0.82 to 0.32; Figure 8), with no significant heterogeneity noted between the studies (I2 = 0%, P = 0.68), East Asian group (SMD -0.24; 95% CI -0.43 to -0.05; I2 = 0%, P = 0.81), and South Asian group (SMD 0.06; 95% CI -0.24 to 0.36; I2 = 0%, P = 0.45).
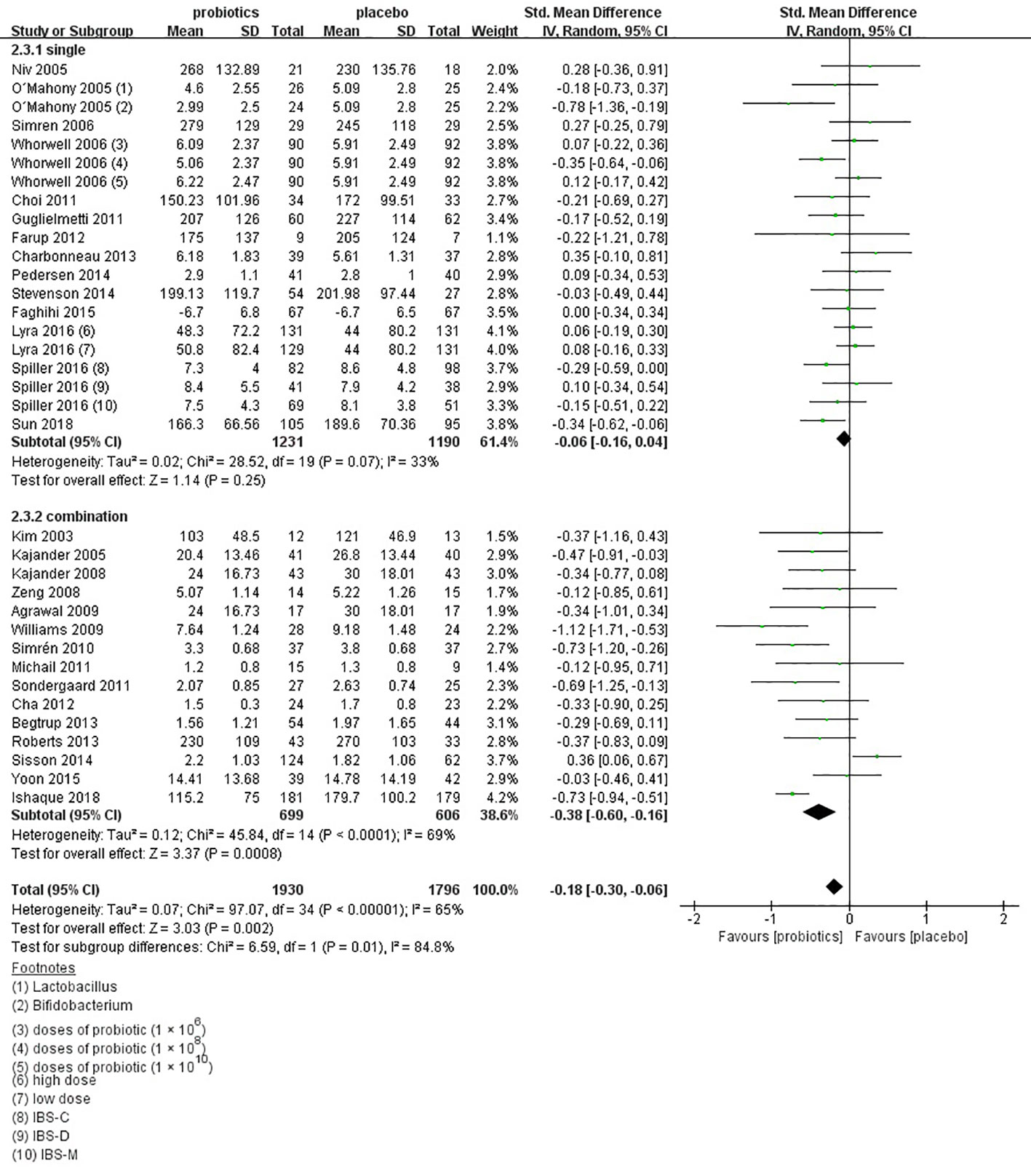
Figure 7 Forest plot of efficacy on global IBS symptoms scores: subgroup of probiotics type.
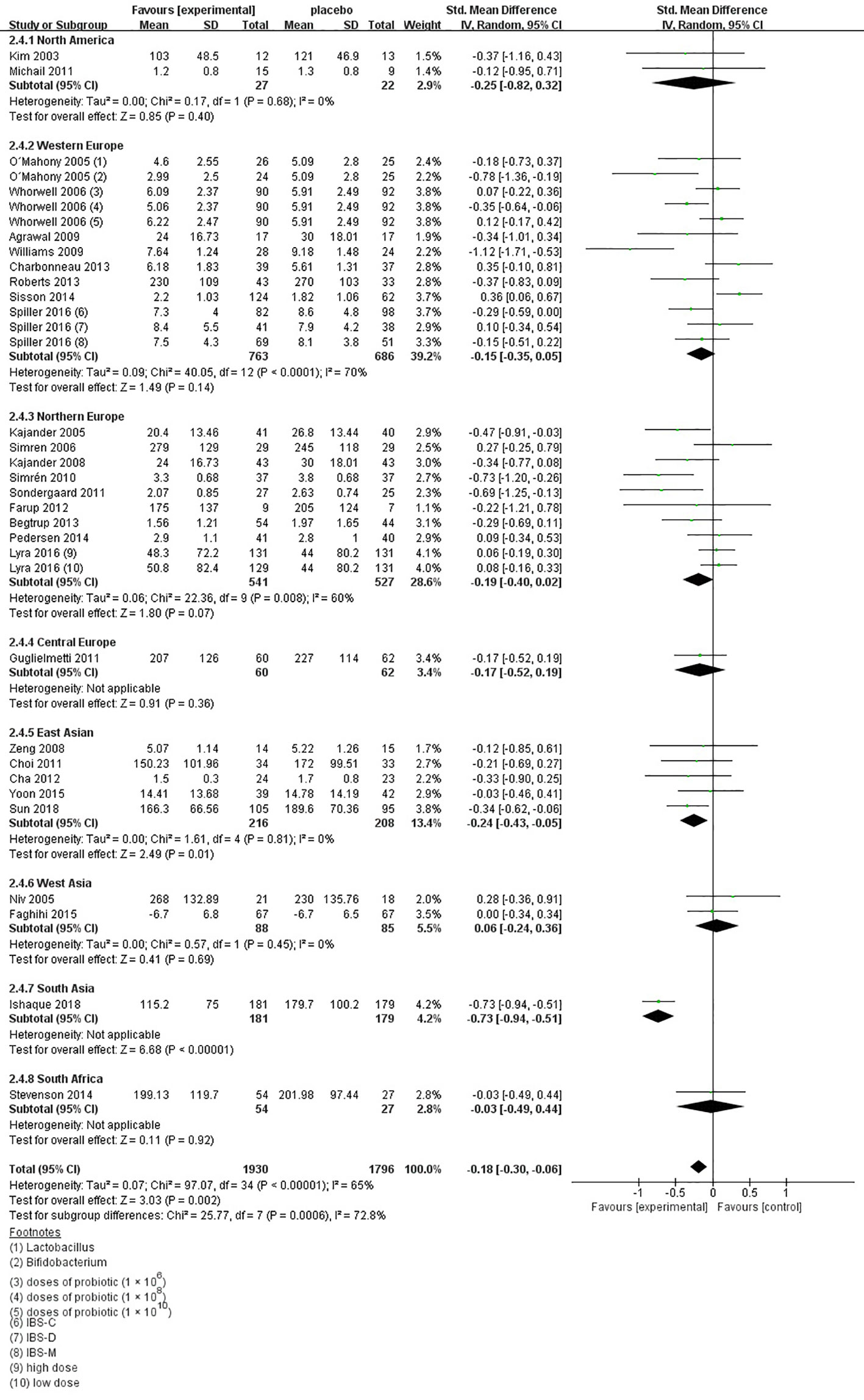
Figure 8 Forest plot of efficacy of probiotics on global IBS symptoms scores: subgroup of geographic position.
There were 38 trials (Nobaek et al., 2000; Kim et al., 2003; Kajander et al., 2005; Kim et al., 2005; O'Mahony et al., 2005; Kim et al., 2006; Whorwell et al., 2006; Guyonnet et al., 2007; Drouault-Holowacz et al., 2008; Kajander et al., 2008; Sinn et al., 2008; Zeng et al., 2008; Agrawal et al., 2009; Williams et al., 2009; Simrén et al., 2010; Choi et al., 2011; Guglielmetti et al., 2011; Michail and Kenche, 2011; Sondergaard et al., 2011; Cha et al., 2012; Amirimani et al., 2013; Begtrup et al., 2013; Charbonneau et al., 2013; Roberts et al., 2013; Abbas et al., 2014; Jafari et al., 2014; Shavakhi et al., 2014; Sisson et al., 2014; Yoon et al., 2014; Pineton de Chambrun et al., 2015; Yoon et al., 2015; Spiller et al., 2016; Lyra et al., 2016; Majeed et al., 2016; Ishaque et al., 2018; Khodadoostan et al., 2018; Kim et al., 2018; Sun et al., 2018) including 44 comparisons with 4,579 patients reporting efficacy of probiotics on abdominal pain. Probiotics had effect on improving abdominal pain (SMD -0.22; 95% CI -0.33 to -0.11; Figure S6), but significant heterogeneity existed (I2 = 70%, P < 0.001). However, in subgroup analysis of probiotics dose, 24 comparisons (Kim et al., 2003; Kim et al., 2005; O'Mahony et al., 2005; Kim et al., 2006; Whorwell et al., 2006; Guyonnet et al., 2007; Drouault-Holowacz et al., 2008; Zeng et al., 2008; Agrawal et al., 2009; Williams et al., 2009; Simrén et al., 2010; Choi et al., 2011; Michail and Kenche, 2011; Sondergaard et al., 2011; Cha et al., 2012; Amirimani et al., 2013; Begtrup et al., 2013; Roberts et al., 2013; Sisson et al., 2014; Yoon et al., 2014; Yoon et al., 2015; Lyra et al., 2016; Kim et al., 2018) using high dose were found a significant benefit over placebo (SMD = -0.14; 95% CI -0.26 to -0.01; Figure S7), with low heterogeneity (I2 = 39%, P = 0.03). There was no significant asymmetry in funnel plot (Egger test, P = 0.235; Figure S8), indicating no proof of publication bias.
Twenty-nine trials (Nobaek et al., 2000; Kim et al., 2003; Kim et al., 2005; O'Mahony et al., 2005; Kim et al., 2006; Whorwell et al., 2006; Guyonnet et al., 2007; Zeng et al., 2008; Agrawal et al., 2009; Williams et al., 2009; Simrén et al., 2010; Choi et al., 2011; Guglielmetti et al., 2011; Michail and Kenche, 2011; Cha et al., 2012; Amirimani et al., 2013; Begtrup et al., 2013; Charbonneau et al., 2013; Roberts et al., 2013; Sisson et al., 2014; Abbas et al., 2014; Jafari et al., 2014; Yoon et al., 2014; Yoon et al., 2015; Majeed et al., 2016; Lyra et al., 2016; Spiller et al., 2016; Kim et al., 2018; Sun et al., 2018) reported continuous data for the effect of probiotics on bloating scores in 3,496 patients. Probiotics had effect on improving bloating (SMD -0.13; 95% CI -0.24 to -0.03; Figure S9) and heterogeneity was found (I2 = 54%, P < 0.01). In the subgroup of probiotics duration, 19 comparisons (Nobaek et al., 2000; Kim et al., 2006; Whorwell et al., 2006; Guyonnet et al., 2007; Zeng et al., 2008; Agrawal et al., 2009; Choi et al., 2011; Guglielmetti et al., 2011; Amirimani et al., 2013; Abbas et al., 2014; Jafari et al., 2014; Yoon et al., 2014; Yoon et al., 2015; Kim et al., 2018; Sun et al., 2018) using a short treatment duration (<8 weeks) were found a significant benefit over placebo (SMD -0.13; 95% CI -0.27 to -0.01). Low heterogeneity was detected (I2 = 47%, P = 0.01).There was a beneficial effect on bloating in 22 comparisons (Kim et al., 2003; Kim et al., 2005; O'Mahony et al., 2005; Kim et al., 2006; Whorwell et al., 2006; Guyonnet et al., 2007; Zeng et al., 2008; Agrawal et al., 2009; Williams et al., 2009; Simrén et al., 2010; Choi et al., 2011; Michail and Kenche, 2011; Cha et al., 2012; Amirimani et al., 2013; Begtrup et al., 2013; Roberts et al., 2013; Sisson et al., 2014; Yoon et al., 2014; Yoon et al., 2015; Lyra et al., 2016; Kim et al., 2018) using high dose (SMD -0.07; 95% CI -0.20 to -0.06; Figure S10).Low heterogeneity among trials was discovered (I2 = 38%, P = 0.04).The funnel plot suggested the existence of asymmetry (Egger test, P = 0.095; Figure S11), indicating possible publication bias.
Forty studies (Gade and Thorn, 1989; Niedzielin et al., 2001; Kim et al., 2003; Kajander et al., 2005; Kim et al., 2005; Niv et al., 2005; O'Mahony et al., 2005; Kim et al., 2006; Whorwell et al., 2006; Guyonnet et al., 2007; Enck et al., 2008; Kajander et al., 2008; Sinn et al., 2008; Zeng et al., 2008; Enck et al., 2009; Hong et al., 2009; Simrén et al., 2010; Choi et al., 2011; Guglielmetti et al., 2011; Michail and Kenche, 2011; Cha et al., 2012; Dapoigny et al., 2012; Ducrotte et al., 2012; Kruis et al., 2012; Amirimani et al., 2013; Begtrup et al., 2013; Charbonneau et al., 2013; Abbas et al., 2014; Lorenzo-Zuniga et al., 2014; Sisson et al., 2014; Stevenson et al., 2014; Yoon et al., 2014; Pineton de Chambrun et al., 2015; Lyra et al., 2016; Majeed et al., 2016; Spiller et al., 2016; Hod et al., 2017; Ishaque et al., 2018; Preston et al., 2018; Sun et al., 2018) provided safety-related data, which was assessed by adverse events. Fourteen trials (Gade and Thorn, 1989; Niedzielin et al., 2001; Kim et al., 2003; Kajander et al., 2005; Kim et al., 2005; Kim et al., 2006; Sinn et al., 2008; Simrén et al., 2010; Michail and Kenche, 2011; Dapoigny et al., 2012; Lorenzo-Zuniga et al., 2014; Yoon et al., 2015; Hod et al., 2017; Ishaque et al., 2018) reported that there were no adverse events. Four trials (O'Mahony et al., 2005; Whorwell et al., 2006; Majeed et al., 2016; Spiller et al., 2016) reported adverse events of both arms. Difference was detected between probiotics and placebo (RR = 1.07; 95% CI 0.92–1.24; Figure 9), with low heterogeneity (I2 = 0, P = 0.83). The funnel plot suggested no evidence of asymmetry (Egger test, P = 0.808; Figure S12). Probiotics seem to be safer than placebo in IBS patients.
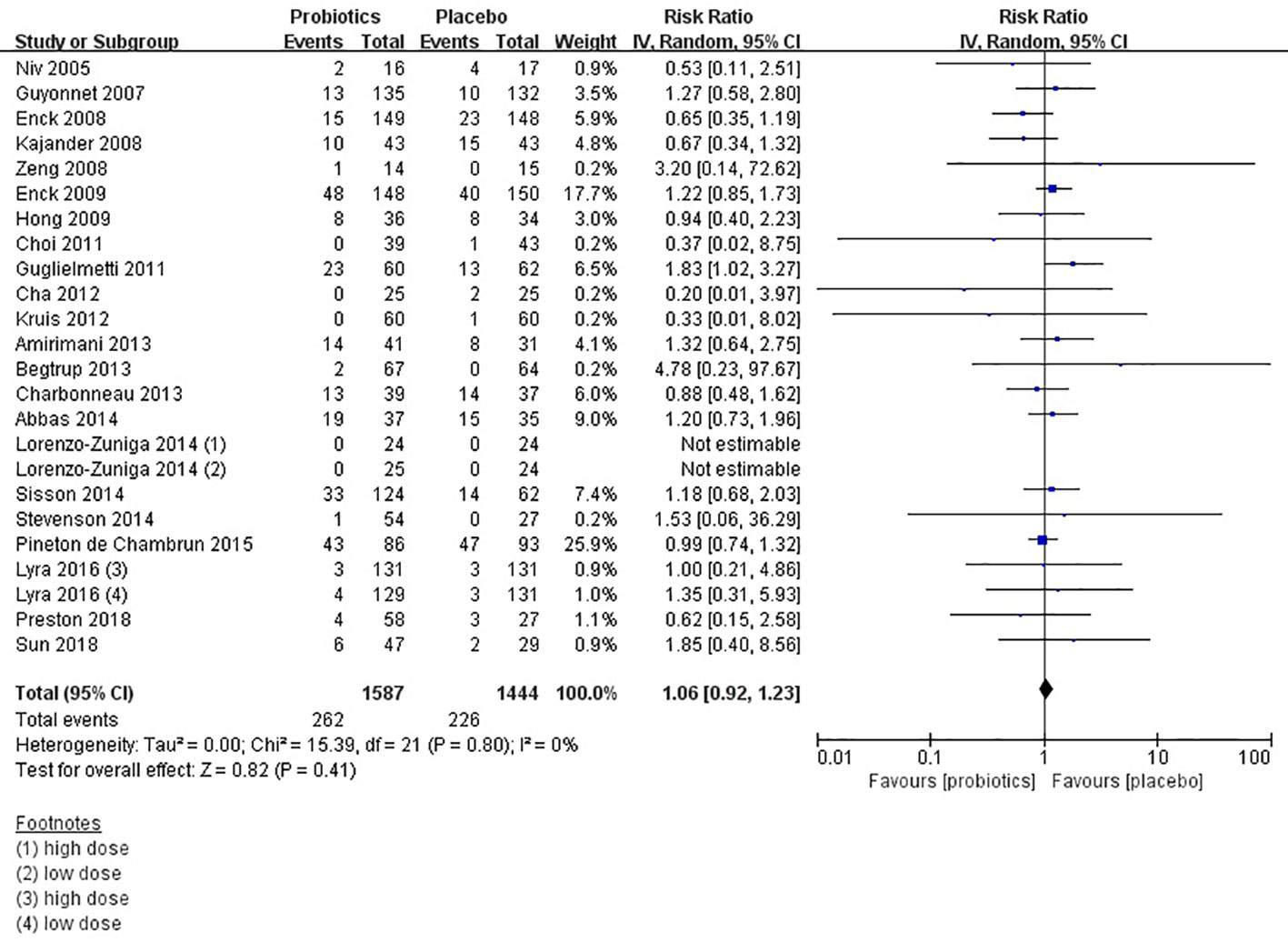
Figure 9 Forest plot of safety of probiotics in IBS.
Alterations of the intestinal microbiome could be relevant to IBS. Symptoms in IBS often developed after an infection, which was known as post-infectious IBS (Marshall et al., 2006; Marshall et al., 2007). Gut bacterial overgrowth may cause symptoms of IBS indistinguishable (Lin, 2004). Studies suggest that compared with the healthy group the colonic microbiome changes in IBS (Durban et al., 2013; Jalanka-Tuovinen et al., 2014). Despite there were many drugs and treatments for IBS, probiotics have shown beneficial (Simrén et al., 2013; Mozaffari et al., 2014). Probiotics may regulate immunity in IBS to protect the intestine (Major and Spiller, 2014). Probiotics also modify the gut microbiota, which improves some IBS symptoms, such as flatulence, bloating, and altered bowel habits (Jeffery et al., 2012; Tap et al., 2017).
Many pieces of evidence have suggested that probiotics may benefit IBS symptoms (Shavakhi et al., 2014; Stevenson et al., 2014; Yoon et al., 2014). However, the results of clinical trials have been conflicting. Our meta-analysis has indicated that probiotics may be beneficial and safe to improve symptoms of IBS compared with placebo. However, it was difficult to draw a precise conclusion as a result of the existence of significant heterogeneity and possible publication bias. We found that a shorter treatment duration (< 8 weeks) could reduce global IBS symptoms scores and bloating scores (Whorwell et al., 2006; Guyonnet et al., 2007; Drouault-Holowacz et al., 2008). As a chronic and recurrent disease (Sun et al., 2018), the improvement of IBS symptoms seems to be detected after a long time by taking probiotics continuously. However, according to current research shorter treatment duration seemed to be more beneficial. But due to many dropouts in the longer duration group, there may have an impact on research results, manifesting as greater improvement in the shorter duration group (Roberts et al., 2013). Although the use of single probiotics tended to have a beneficial effect on improving the bloating scores (Majeed et al., 2016; Spiller et al., 2016; Kim et al., 2018; Sun et al., 2018), it was unknown which strain or species was more beneficial than others. Using a high dose of probiotics may reduce abdominal pain scores and bloating scores (Yoon et al., 2014; Yoon et al., 2015; Kim et al., 2018). However, Lyra et al. tested two different doses (1010 CFU/D, and 109 CFU/D) of Lactobacillus acidophilus NCFM and reported that none of the outcomes showed a dose-response effect (Lyra et al., 2016). Small differences of dosage may contribute to no effect of dose. Probiotics could benefit overall IBS symptoms improvement in North America, West Europe, Northern Europe, and East Asian.We also found that probiotics could reduce global IBS symptoms scores in North America, East Asian, and South Asian. More pieces of evidence are needed. Probiotics seemed safe for patients with irritable bowel syndrome (O'Mahony et al., 2005; Whorwell et al., 2006; Majeed et al., 2016; Spiller et al., 2016), but more long-term trials are required to prove it.
Our meta-analysis is the first to assemble the efficacy and safety of probiotics for IBS patients with all diagnostic criteria by subgroup analyses of probiotic type, dose, treatment duration, and geographic position. We conducted this meta-analysis and systematic review using a rigorous and reproducible methodology. Two reviewers assessed eligibility and extracted data independently. The random-effects model was used to minimize the possibility of overestimating treatment results. We also tried to contact researchers of possibly eligible trials to get data. These comprehensive approaches included more than 3,300 IBS patients receiving probiotics treatment. Finally, subgroup analyses of probiotics type, dose, treatment duration, and geographic position were performed to evaluate the efficacy of treatment.
Our study has certain limitations. Bias risk of many studies was unknown, and the analysis shows considerable evidence of heterogeneity between trials. However, considering only studies with low bias risk, the positive effects remained. The number of studies on subgroup analyses of probiotics type, doses, and treatment duration was limited. It was not enough to detect significant differences in the efficacy of probiotics. In some studies, significant placebo effects have been found which can affect the results.
In summary, this meta-analysis has demonstrated moderate evidence for the use and safety of probiotics in IBS. A shorter treatment duration (< 8 weeks) and a single probiotic may be more beneficial. Probiotics seem to be safe for patients with irritable bowel syndrome. There is still a need for more clinical trials. Finally, probiotics may be a beneficial therapy for IBS patients.
All datasets generated for this study are included in the article/Supplementary Material.
LZ and BL conceived and designed this study. BL and LL searched and selected studies. HD and JG extracted essential information. BL and HS assessed the risk of bias. BL and HD performed statistical analyses. BL and HS interpreted the pooled results. BL, LL, and LZ drafted the manuscript. All authors approved the final manuscript.
This research was supported by the Youth Foundation of 960th Hospital of the PLA with a unique identifier of 2017QN03.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to express our appreciation to all authors listed in these all primary studies which were included in the current systematic review and meta-analysis.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2020.00332/full#supplementary-material
Abbas, Z., Yakoob, J., Jafri, W., Ahmad, Z., ND Islam, M. (2014). Cytokine and clinical response to Saccharomyces boulardii therapy in diarrhea-dominant irritable bowel syndrome: a randomized trial. Eur. J. Gastroenterol. Hepatol. 26, 630–639. doi: 10.1097/MEG.0000000000000094
Agrawal, A., Houghton, L. A., Morris, J., Reilly, B., Guyonnet, D., Goupil, F. N., et al. (2009). Clinical trial: the effects of a fermented milk product containing Bifidobacterium lactis DN-173 010 on abdominal distension and gastrointestinal transit in irritable bowel syndrome with constipation. Aliment. Pharmacol. Ther. 29, 104–114. doi: 10.1111/j.1365-2036.2008.03853.x
Amirimani, B., Nikfam, S., Albaji, M., Vahedi, S., Vahedi, H. (2013). Probiotic vs. Placebo in Irritable Bowel Syndrome: A Randomized Controlled Trial. Middle East J. Dig. Dis. 5, 98–102.
Andresen, V., Montori, V. M., Keller, J., West, C. P., Layer, P., Camilleri, M. (2008). Effects of 5-Hydroxytryptamine (Serotonin) Type 3 Antagonists on Symptom Relief and Constipation in Nonconstipated Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin. Gastroenterol. Hepatol. 6, 545–555. doi: 10.1016/j.cgh.2007.12.015
Begtrup, L. M., de Muckadell, O. B., Kjeldsen, J., Christensen, R. D., Jarbol, D. E. (2013). Long-term treatment with probiotics in primary care patients with irritable bowel syndrome-a randomised, double-blind, placebo controlled trial. Scand. J. Gastroenterol. 48, 1127–1135. doi: 10.3109/00365521.2013.825314
Bundeff, A. W., Woodis, C. B. (2014). Selective serotonin reuptake inhibitors for the treatment of irritable bowel syndrome. Ann. Pharmacother. 48, 777–784. doi: 10.1177/1060028014528151
Cha, B. K., Jung, S. M., Choi, C. H., Song, In-do., Lee, H. W., Kim, H. J., et al. (2012). The effect of a multispecies probiotic mixture on the symptoms and fecal microbiota in diarrhea-dominant irritable bowel syndrome: a randomized, double-blind, placebo-controlled trial. J. Clin. Gastroenterol. 46, 220–227. doi: 10.1097/MCG.0b013e31823712b1
Chang, L., Chey, W. D., Drossman, D., Losch-Beridon, T., Wang, M., Lichtlen, P., et al. (2016). Effects of baseline abdominal pain and bloating on response to lubiprostone in patients with irritable bowel syndrome with constipation. Aliment. Pharmacol. Ther. 44, 1114–1122. doi: 10.1111/apt.13807
Charbonneau, D., Gibb, R. D., Quigley, E. M. M. (2013). Fecal excretion of Bifidobacterium infantis 35624 and changes in fecal microbiota after eight weeks of oral supplementation with encapsulated probiotic. Gut. Microbes 4, 201–211. doi: 10.4161/gmic.24196
Chey, W. D., Lembo, A., Macdougall, J. E., Lavins, B. J., Schneier, H., Johnston, J. M. (2011). Efficacy and Safety of Once-Daily Linaclotide Administered Orally for 26 Weeks in Patients With IBS-C: Results From a Randomized, Double-Blind, Placebo-Controlled Phase 3 Trial. Gastroenterology 140, S–135. doi: 10.1016/S0016-5085(11)60550-7
Choi, C. H., Jo, S. Y., Park, H. J., Chang, S. K., Myung, S. J. (2011). A randomized, double-blind, placebo-controlled multicenter trial of saccharomyces boulardii in irritable bowel syndrome: effect on quality of life. J. Clin. Gastroenterol. 45, 679–683. doi: 10.1097/mcg.0b013e318204593e
Cui, S., Hu, Y., Lunaud, B., Cardot, J. M., A. (2012). Multistrain probiotic preparation significantly reduces symptoms of irritable bowel syndrome in a double-blind placebo-controlled study. Int. J. Clin. Exp. Med. 5, 238–244. doi: 10.1155/2012/952452
Dapoigny, M., Piche, T., Ducrotte, P., Lunaud, B., Cardot, J. M., Bern, A. (2012). Efficacy and safety profile of LCR35 complete freeze-dried culture in irritable bowel syndrome: a randomized, double-blind study. World J. Gastroenterol. 18, 2067–2075. doi: 10.3748/wjg.v18.i17.2067
Dersimonian, R., Laird, N. (1986). Meta-analysis in clinical trials. Control Clin. Trials 7, 177–178. doi: 10.1016/0197-2456(86)90046-2
Drossman, D. A., Camilleri, M., Mayer, E. A., Whitehead, W.E. (2002). AGA technical review on irritable bowel syndrome. Gastroenterology 123, 2108–2131. doi: 10.1053/gast.2002.37095
Drouault-Holowacz, S., Bieuvelet, S., Burckel, A., Cazaubiel, M., Dray, X., Marteau, P. (2008). A double blind randomized controlled trial of a probiotic combination in 100 patients with irritable bowel syndrome. Gastroen. Clin. Biol. 32, 147–152. doi: 10.1016/j.gcb.2007.06.001
Ducrotte, P., Sawant, P., Jayanthi, V. (2012). Clinical trial: Lactobacillus plantarum 299v (DSM 9843) improves symptoms of irritable bowel syndrome. World J. Gastroenterol. 18, 4012–4018. doi: 10.3748/wjg.v18.i30.4012
Dupont, H. L. (2014). Review article: evidence for the role of gut microbiota in irritable bowel syndrome and its potential influence on therapeutic targets. Aliment. Pharmacol. Ther. 39, 1033–1042. doi: 10.1111/apt.12728
Durban, A., Abellan, J. J., Jimenez-Hernandez, N., Artacho, A., Garrigues, V., Ortiz, V., et al. (2013). Instability of the faecal microbiota in diarrhoea-predominant irritable bowel syndrome. FEMS Microbiol. Ecol. 86, 581–589. doi: 10.1111/1574-6941.12184
Egger, M., Davey, S. G., Schneider, M., Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test. BMJ 315, 629–634. doi: 10.1136/bmj.315.7109.629
Enck, P., Zimmermann, K., Menke, G., Muller-lissner, S., Martens, U., Klosterhalfen, S. (2008). A mixture of Escherichia coli (DSM 17252) and Enterococcus faecalis (DSM 16440) for treatment of the irritable bowel syndrome - a randomized controlled trial with primary care physicians. Neurogastroenterol. Motil. 20, 1103–1109. doi: 10.1111/j.1365-2982.2008.01156.x
Enck, P., Zimmermann, K., Menke, G., Klosterhalfen, S. (2009). Randomized controlled treatment trial of irritable bowel syndrome with a probiotic E.-coli preparation (DSM17252) compared to placebo. Z Gastroenterol. 47, 209–214. doi: 10.1055/s-2008-1027702
Faghihi, A. H., Agah, S., Masoudi, M., Ghafoori, S. M., Eshraghi, A. (2015). Efficacy of Probiotic Escherichia coli Nissle 1917 in Patients with Irritable Bowel Syndrome: a Double Blind Placebo-controlled Randomized Trial. Acta Med. Indones 47, 201–208.
Farup, P. G., Jacobsen, M., Ligaarden, S. C., Rudi, K. (2012). Probiotics, symptoms, and gut microbiota: what are the relations? A randomized controlled trial in subjects with irritable bowel syndrome. Gastroenterol. Res. Pract. 2012, 214102. doi: 10.1155/2012/214102
Gade, J., Thorn, P. (1989). Paraghurt for patients with irritable bowel syndrome. A controlled clinical investigation from general practice. Scand. J. Prim Health Care 7, 23–26. doi: 10.3109/02813438909103666
Gralnek, I. M., Hays, R. D., Kilbourne, A., Naliboff, B., Mayer, E. A. (2000). The impact of irritable bowel syndrome on health-related quality of life. Gastroenterology 119, 654–660. doi: 10.1053/gast.2000.16484
Guarner, F., Khan, A. G., Garich, J., Eliakim, R., Gangl, A., Thompson, A., et al (2012). World Gastroenterology Organisation Global Guidelines[J]. J Clin Gastroenterol. 46 (6), 468–481. doi: 10.1097/MCG.0b013e3182549092
Guglielmetti, S., Mora, D., Gschwender, M., Popp, K. (2011). Randomised clinical trial: Bifidobacterium bifidum MIMBb75 significantly alleviates irritable bowel syndrome and improves quality of life–a double-blind, placebo-controlled study. Aliment. Pharmacol. Ther. 33, 1123–1132. doi: 10.1111/j.1365-2036.2011.04633.x
Guyonnet, D., Chassany, O., Ducrotte, P., Picard, C., Mouret, M., Mercier, C. -H., et al. (2007). Effect of a fermented milk containing Bifidobacterium animalis DN-173 010 on the health-related quality of life and symptoms in irritable bowel syndrome in adults in primary care: a multicentre, randomized, double-blind, controlled trial. Aliment. Pharmacol. Ther. 26, 475–486. doi: 10.1111/j.1365-2036.2007.03362.x
Hayes, P. A., Fraher, M. H., Quigley, E. M. (2014). Irritable bowel syndrome: the role of food in pathogenesis and management. Gastroenterol. Hepatol. 10, 164–174. doi: 10.1111/j.1751-2980.2009.00392.x
Higgins, J. P. T., Green, S. (2011). Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0 [updated March 2011]. in The Cochrane Collaboration. Available online at: http://handbook.cochrane.org.
Higgins, J. P. T., Thompson, S. G., Deeks, J. J., Altman, D. G. (2003). Measuring inconsistency in meta-analyses. BMJ 327, 557–560. doi: 10.1136/bmj.327.7414.557
Hod, K., Sperber, A. D., Ron, Y., Boaz, M., Dickman, R., Berliner, S., et al. (2017). A double-blind, placebo-controlled study to assess the effect of a probiotic mixture on symptoms and inflammatory markers in women with diarrhea-predominant IBS. Neurogastroenterol. Motil. 29, e13037. doi: 10.1111/nmo.13037
Hong, K. S., Kang, H. W., Im, J. P., Ji, G. E., Kim, S. G., Jung, H. C., et al. (2009). Effect of probiotics on symptoms in korean adults with irritable bowel syndrome. Gut. Liver 3, 101–107. doi: 10.5009/gnl.2009.3.2.101
Hyland, N. P., Quigley, E. M., Brint, E. (2014). Microbiota-host interactions in irritable bowel syndrome: epithelial barrier, immune regulation and brain-gut interactions. World J. Gastroenterol. 20, 8859–8866. doi: 10.3748/wjg.v20.i27.8859
Ishaque, S. M., Khosruzzaman, S. M., Ahmed, D. S., Sah, M. P. (2018). A randomized placebo-controlled clinical trial of a multi-strain probiotic formulation (Bio-Kult®) in the management of diarrhea-predominant irritable bowel syndrome. BMC Gastroenterol. 18, 71. doi: 10.1186/s12876-018-0788-9
Jafari, E., Vahedi, H., Merat, S., Riahi, A. (2014). Therapeutic effects, tolerability and safety of a multi-strain probiotic in Iranian adults with irritable bowel syndrome and bloating. Arch. Iran Med. 17, 466–470. doi: 0141707/AIM.003
Jalanka-Tuovinen, J., Salojarvi, J., Salonen, A., Immonen, O., Garsed, A., Kelly, F. M., et al. (2014). Faecal microbiota composition and host-microbe cross-talk following gastroenteritis and in postinfectious irritable bowel syndrome. Gut 63, 1737–1745. doi: 10.1136/gutjnl-2013-305994
Jeffery, I. B., O'Toole, P. W., Ohman, L., Claesson, M. J., Deane, J., Quigley, EMM, et al. (2012). An irritable bowel syndrome subtype defined by species-specific alterations in faecal microbiota. Gut 61, 997–1006. doi: 10.1136/gutjnl-2011-301501
Kajander, K., Hatakka, K., Poussa, T., Färkkilä, M. A. (2005). A probiotic mixture alleviates symptoms in irritable bowel syndrome patients: a controlled 6-month intervention. Aliment. Pharmacol. Ther. 22, 387–394. doi: 10.1111/j.1365-2036.2005.02579.x
Kajander, K., Myllyluoma, E., Rajilic-Stojanovic, M., Kyrönpalo, S., Rasmussen, M., Järvenpää, S., et al. (2008). Clinical trial: multispecies probiotic supplementation alleviates the symptoms of irritable bowel syndrome and stabilizes intestinal microbiota. Aliment. Pharmacol. Ther. 27, 48–57. doi: 10.1111/j.1365-2036.2007.03542.x
Khodadoostan, M., Shavakhi, A., Sherafat, Z., Shavakhi, A. (2018). Effect of Probiotic Administration Immediately and 1 Month after Colonoscopy in Diarrhea-predominant Irritable Bowel Syndrome Patients. Adv. BioMed. Res. 7, 94. doi: 10.4103/abr.abr_216_17
Kim, H. J., Camilleri, M., McKinzie, S., Lempke, M. B., Burton, D. D., Thomforde, G. M., et al. (2003). A randomized controlled trial of a probiotic, VSL#3, on gut transit and symptoms in diarrhoea-predominant irritable bowel syndrome. Aliment. Pharmacol. Ther. 17, 895–904. doi: 10.1046/j.1365-2036.2003.01543.x
Kim, H. J., Vazquez Roque, M. I., Camilleri, M., Stephens, D., Burton, D. D., Baxter, K., et al. (2005). A randomized controlled trial of a probiotic combination VSL# 3 and placebo in irritable bowel syndrome with bloating. Neurogastroenterol. Motil. 17, 687–696. doi: 10.1111/j.1365-2982.2005.00695.x
Kim, Y. G., Moon, J. T., Lee, K. M., Chon, N. R., Park, H. (2006). The effects of probiotics on symptoms of irritable bowel syndrome. Korean J. Gastroenterol. 47, 413–419. doi: 10.4166/kjg.2009.54.6.413
Kim, J. Y., Park, Y. J., Lee, H. J., Park, M. Y., Kwon, O. (2018). Effect of Lactobacillus gasseri BNR17 on irritable bowel syndrome: a randomized, double-blind, placebo-controlled, dose-finding trial. Food Sci. Biotechnol. 27, 853–857. doi: 10.1007/s10068-017-0296-7
Kruis, W., Chrubasik, S., Boehm, S., Stange, C., Schulze, J. (2012). A double-blind placebo-controlled trial to study therapeutic effects of probiotic Escherichia coli Nissle 1917 in subgroups of patients with irritable bowel syndrome. Int. J. Colorectal Dis. 27, 467–474. doi: 10.1007/s00384-011-1363-9
Lin, H. C. (2004). Small intestinal bacterial overgrowth: a framework for understanding irritable bowel syndrome. JAMA 292, 852–858. doi: 10.1001/jama.292.7.852
Lorenzo-Zuniga, V., Llop, E., Suarez, C., Alvarez, B., Abreu, L., Espadaler, J., et al. (2014). I.31, a new combination of probiotics, improves irritable bowel syndrome-related quality of life. World J. Gastroenterol. 20, 8709–8716. doi: 10.3748/wjg.v20.i26.8709
Lovell, R. M., Ford, A. C. (2012). Global Prevalence of and Risk Factors for Irritable Bowel Syndrome: A Meta-analysis. Clin. Gastroenterol. Hepatol. 10, 712–721.e4. doi: 10.1016/j.cgh.2012.02.029
Ludidi, S., Jonkers, D. M., Koning, C. J., Kruimel, J. W., Mulder, L., Vaart, I. B., et al. (2014). Randomized clinical trial on the effect of a multispecies probiotic on visceroperception in hypersensitive IBS patients. Neurogastroenterol. Motil. 26, 705–714. doi: 10.1111/nmo.12320
Lyra, A., Hillilä, M., Huttunen, T., Männikkö, S., Taalikka, M., Tennilä, J., et al. (2016). Irritable bowel syndrome symptom severity improves equally with probiotic and placebo. World J. Gastroenterol. 22, 10631–10642. doi: 10.3748/wjg.v22.i48.10631
Majeed, M., Nagabhushanam, K., Natarajan, S., Arumugam, S., Ali, F., Pande, F., et al. (2016). Bacillus coagulans MTCC 5856 supplementation in the management of diarrhea predominant Irritable Bowel Syndrome: a double blind randomized placebo controlled pilot clinical study. Nutr. J. 15, 21. doi: 10.1186/s12937-016-0140-6
Major, G., Spiller, R. (2014). Irritable bowel syndrome, inflammatory bowel disease and the microbiome. Curr. Opin. Endocrinol. Diabetes Obes. 21, 15–21. doi: 10.1097/MED.0000000000000032
Marshall, J. K., Thabane, M., Garg, A. X., Clark, W.F., Salvadori, M., Collins, S. M. (2006). Incidence and epidemiology of irritable bowel syndrome after a large waterborne outbreak of bacterial dysentery. Gastroenterology 131, 445–450. doi: 10.1016/S0399-8320(07)89359-6
Marshall, J. K., Thabane, M., Borgaonkar, M. R., James, C. (2007). Postinfectious Irritable Bowel Syndrome After a Food-Borne Outbreak of Acute Gastroenteritis Attributed to a Viral Pathogen. Clin. Gastroenterol. Hepatol. 5, 457–460. doi: 10.1016/j.cgh.2006.11.025
Mezzasalma, V., Manfrini, E., Ferri, E., Sandionigi, A., Ferla, B. L., Schiano, I., et al. (2016). A Randomized, Double-Blind, Placebo-Controlled Trial: The Efficacy of Multispecies Probiotic Supplementation in Alleviating Symptoms of Irritable Bowel Syndrome Associated with Constipation. BioMed. Res. Int. 2016, 1–10. doi: 10.1155/2016/4740907
Michail, S., Kenche, H. (2011). Gut Microbiota is Not Modified by Randomized, Double-Blind, Placebo-Controlled Trial of VSL#3 in Diarrhea-Predominant Irritable Bowel Syndrome. Probiotics Antimicrob. 3, 1–7. doi: 10.1007/s12602-010-9059-y
Mozaffari, S., Nikfar, S., Abdollahi, M. (2014). The safety of novel drugs used to treat irritable bowel syndrome. Expert Opin. Drug Saf. 13, 625–638. doi: 10.1517/14740338.2014.902932
Niedzielin, K., Kordecki, H., Birkenfeld, B. (2001). A controlled, double-blind, randomized study on the efficacy of Lactobacillus plantarum 299V in patients with irritable bowel syndrome. Eur. J. Gastroenterol. Hepatol. 13, 1143–1147. doi: 10.1097/00042737-200110000-00004
Niv, E., Naftali, T., Hallak, R., Vaisman, N. (2005). The efficacy of Lactobacillus reuteri ATCC 55730 in the treatment of patients with irritable bowel syndrome-a double blind, placebo-controlled, randomized study. Clin. Nutr. 24, 925–931. doi: 10.1016/j.clnu.2005.06.001
Nobaek, S., Johansson, M. L., Molin, G., Ahrné, S., Jeppsson, B. (2000). Alteration of intestinal microflora is associated with reduction in abdominal bloating and pain in patients with irritable bowel syndrome. Am. J. Gastroenterol. 95, 1231–1238. doi: 10.1016/S0002-9270(00)00807-8
O'Mahony, L., McCarthy, J., Kelly, P., Hurley, G., Luo, F., Chen, K., et al. (2005). Lactobacillus and bifidobacterium in irritable bowel syndrome: symptom responses and relationship to cytokine profiles. Gastroenterology 128, 541–551. doi: 10.1053/j.gastro.2004.11.050
Parkes, G. C., Brostoff, J., Whelan, K., Sanderson, J. D. (2008). Gastrointestinal Microbiota in Irritable Bowel Syndrome: Their Role in Its Pathogenesis and Treatment. Am. J. Gastroenterol. 103, 1557–1567. doi: 10.1111/j.1572-0241.2008.01869.x
Pedersen, N., Andersen, N. N., Végh, Z., Jensen, L., Ankersen, D. V., Felding, M., et al. (2014). Ehealth: low FODMAP diet vs Lactobacillus rhamnosus GG in irritable bowel syndrome. World J. Gastroenterol. 20, 16215–16226. doi: 10.3748/wjg.v20.i43.16215
Pineton de Chambrun, G., Neut, C., Chau, A., Cazaubiel, M., Pelerin, F., Justen, P., et al. (2015). A randomized clinical trial of Saccharomyces cerevisiae versus placebo in the irritable bowel syndrome. Dig. Liver Dis. 47, 119–124. doi: 10.1016/j.dld.2014.11.007
Preston, K., Krumian, R., Hattner, J., de Montigny, D., Stewart, M., Gaddam, S. (2018). Lactobacillus acidophilus CL1285, Lactobacillus casei LBC80R and Lactobacillus rhamnosus CLR2 improve quality-of-life and IBS symptoms: a double-blind, randomised, placebo-controlled study. Benef. Microbes 9, 697–706. doi: 10.3920/BM2017.0105
Rahimi, R., Nikfar, S., Rezaie, A., Abdollahi, M. (2009). Efficacy of tricyclic antidepressants in irritable bowel syndrome: a meta-analysis. World J. Gastroenterol. 15, 1548–1553. doi: 10.3748/wjg.15.1548
Roberts, L. M., McCahon, D., Holder, R., Wilson, S., Hobbs, F. D. (2013). A randomised controlled trial of a probiotic ‘functional food' in the management of irritable bowel syndrome. BMC Gastroenterol. 13, 45. doi: 10.1186/1471-230X-13-45
Shavakhi, A., Minakari, M., Farzamnia, S., Peykar, M. S., Taghipour, G., Tayebi, A., et al. (2014). The effects of multi-strain probiotic compound on symptoms and quality-of-life in patients with irritable bowel syndrome: a randomized placebo-controlled trial. Adv. BioMed. Res. 3, 140. doi: 10.4103/2277-9175.135157
Shin, S. P., Choi, Y. M., Kim, W. H., Hong, S. P., Park, J. M., Kim, J., et al. (2018). A double blind, placebo-controlled, randomized clinical trial that breast milk derived-Lactobacillus gasseri BNR17 mitigated diarrhea-dominant irritable bowel syndrome. J. Clin. Biochem. Nutr. 62, 179–186. doi: 10.3164/jcbn.17-73
Simrén, M., Ohman, L., Olsson, J., Svensson, U., Ohlson, K., Posserud, I., et al. (2010). Clinical trial: the effects of a fermented milk containing three probiotic bacteria in patients with irritable bowel syndrome - a randomized, double-blind, controlled study. Aliment. Pharmacol. Ther. 31, 218–227. doi: 10.1111/j.1365-2036.2009.04183.x
Simrén, M., Barbara, G., Flint, H. J., Spiegel, B. M., Spiller, R. C., Vanner, S. (2013). Intestinal microbiota in functional bowel disorders: a Rome foundation report. Gut 62, 159–176. doi: 10.1136/gutjnl-2012-302167
Simren, M. S. A., Lindh, A. (2006). Effects of Lactobacillus plantarum 299V on symptoms and rectal sensitivity in patients with irritable bowel syndrome (IBS) - a randomized double blind controlled trial. Gastroenterology 130, A600. doi: 10.1016/S0016-5085(06)60008-5
Sinn, D. H., Song, J. H., Kim, H. J., Lee, J. H., Son, H. J., Chang, D. K., et al. (2008). Therapeutic effect of Lactobacillus acidophilus-SDC 2012, 2013 in patients with irritable bowel syndrome. Digest. Dis. Sci. 53, 2714–2718. doi: 10.1007/s10620-007-0196-4
Sisson, G., Ayis, S., Sherwood, R. A., Bjarnason, I. (2014). Randomised clinical trial: a liquid multi-strain probiotic vs. placebo in the irritable bowel syndrome-a 12 week double-blind study. Aliment. Pharmacol. Ther. 40, 51–62. doi: 10.1111/apt.12787
Sondergaard, B., Olsson, J., Ohlson, K., Svensson, U., Bytzer, P., Ekesbo, R. (2011). Effects of probiotic fermented milk on symptoms and intestinal flora in patients with irritable bowel syndrome: a randomized, placebo-controlled trial. Scand. J. Gastroenterol. 46, 663–672. doi: 10.3109/00365521.2011.565066
Spiller, R., Pelerin, F., Cayzeele Decherf, A., Maudet, C., Housez, B., Cazaubiel, M., et al. (2016). Randomized double blind placebo-controlled trial of Saccharomyces cerevisiae CNCM I-3856 in irritable bowel syndrome: improvement in abdominal pain and bloating in those with predominant constipation. United Eur. Gastroenterol. J. 4, 353–362. doi: 10.1177/2050640615602571
Stevenson, C., Blaauw, R., Fredericks, E., Visser, J., Roux, S. (2014). Randomized clinical trial: Effect of lactobacillus plantarum 299 v on symptoms of irritable bowel syndrome. Nutrition 30, 1151–1157. doi: 10.1016/j.nut.2014.02.010
Sun, Y. Y., Li, M., Li, Y. Y., Li, L. X., Zhai, W. Z., Wang, P., et al. (2018). The effect of Clostridium butyricum on symptoms and fecal microbiota in diarrhea-dominant irritable bowel syndrome: a randomized, double-blind, placebo-controlled trial. Sci. Rep. 8, 2964. doi: 10.1038/s41598-018-21241-z
Tack, J., Vanuytsel, T., Corsetti, M. (2016). Modern Management of Irritable Bowel Syndrome: More Than Motility. Dig. Dis. 34, 566–573. doi: 10.1159/000445265
Tap, J., Derrien, M., Tornblom, H., Brazeilles, R., Cools-Portier, S, Dore, J., et al. (2017). Identification of an intestinal microbiota signature associated with severity of irritable bowel syndrome. Gastroenterology 152, 111–123. doi: 10.1053/j.gastro.2016.09.049.90. e8.
Thijssen, A. Y., Clemens, C. H., Vankerckhoven, V., Goossens, H., Jonkers, D. M., Masclee, A. A. (2016). Efficacy of Lactobacillus casei Shirota for patients with irritable bowel syndrome. Eur. J. Gastroenterol. Hepatol. 28, 8–14. doi: 10.1097/MEG.0000000000000484
Trinkley, K. E., Nahata, M. C. (2014). Medication management of irritable bowel syndrome. Digestion 89, 253–267. doi: 10.1159/000362405
Wang, Y., Hwee, L., Tai, D., Krishnamoorthy, T. L., Tan, T., Barbier, S., et al. (2012). The impact of Irritable Bowel Syndrome on health-related quality of life: a Singapore perspective. BMC Gastroenterol. 12, 104. doi: 10.1186/1471-230x-12-104
Whorwell, P. J., Altringer, L., Morel, J., Bond, Y., Charbonneau, D., O'Mahony, L., et al. (2006). Efficacy of an encapsulated probiotic Bifidobacterium infantis 35624 in women with irritable bowel syndrome. Am. J. Gastroenterol. 101, 1581–1590. doi: 10.1111/j.1572-0241.2006.00734.x
Williams, E. A., Stimpson, J., Wang, D., Plummer, S., Garaiova, I., Barker, M. E., et al. (2009). Clinical trial: A multistrain probiotic preparation significantly reduces symptoms of irritable bowel syndrome in a double-blind placebo-controlled study. Aliment. Pharmacol. Ther. 29, 97–103. doi: 10.1111/j.1365-2036.2008.03848.x
Yoon, J. S., Sohn, W., Lee, O. Y., Lee, S. P., Lee, K. N., Jun, D. W. (2014). Effect of multispecies probiotics on irritable bowel syndrome: a randomized, double-blind, placebo-controlled trial. J. Gastroenterol. Hepatol. 29, 52–59. doi: 10.1111/jgh.12322
Yoon, H., Park, Y. S., Lee, D. H., Seo, J. G., Shin, C. M., Kim, N. (2015). Effect of administering a multi-species probitic mixture on the changes in fecal microbiota and symptoms of irritable bowel syndrome: a randomized, double-blind, placebo-controlled trial. J. Clin. Biochem. Nutr. 57, 129–134. doi: 10.3164/jcbn.15-14
Keywords: efficacy, safety, irratable bowel syndrome, probiotics, meta-analysis
Citation: Li B, Liang L, Deng H, Guo J, Shu H and Zhang L (2020) Efficacy and Safety of Probiotics in Irritable Bowel Syndrome: A Systematic Review and Meta-Analysis. Front. Pharmacol. 11:332. doi: 10.3389/fphar.2020.00332
Received: 06 November 2019; Accepted: 06 March 2020;
Published: 03 April 2020.
Edited by:
Tahir Mehmood Khan, University of Veterinary and Animal Sciences, PakistanReviewed by:
Inayat Rehman, Monash University Malaysia, MalaysiaCopyright © 2020 Li, Liang, Deng, Guo, Shu and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Li Zhang, amp6eXl6bDEyMTBAMTYzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.