 Brian Godman1,2,3,4*
Brian Godman1,2,3,4* Debashis Basu5Yogan Pillay6
Debashis Basu5Yogan Pillay6 Julius C. Mwita7Godfrey Mutashambara Rwegerera7,8Bene D. Anand Paramadhas9Celda Tiroyakgosi10
Julius C. Mwita7Godfrey Mutashambara Rwegerera7,8Bene D. Anand Paramadhas9Celda Tiroyakgosi10 Patrick Mbah Okwen11,12Loveline Lum Niba11,13Justice Nonvignon14Israel Sefah15
Patrick Mbah Okwen11,12Loveline Lum Niba11,13Justice Nonvignon14Israel Sefah15 Margaret Oluka16Anastasia N. Guantai17
Margaret Oluka16Anastasia N. Guantai17 Dan Kibuule17
Dan Kibuule17 Francis Kalemeera17Mwangana Mubita17Joseph Fadare18,19
Francis Kalemeera17Mwangana Mubita17Joseph Fadare18,19 Olayinka O. Ogunleye20,21Larry A. Distiller22Enos M. Rampamba2,23Jeffrey Wing24Debjani Mueller5,25
Olayinka O. Ogunleye20,21Larry A. Distiller22Enos M. Rampamba2,23Jeffrey Wing24Debjani Mueller5,25 Abubakr Alfadl26,27Adefolarin A. Amu28
Abubakr Alfadl26,27Adefolarin A. Amu28 Zinhle Matsebula29Aubrey Kalungia30Trust Zaranyika31Nyasha Masuka32Janney Wale33Ruaraidh Hill34
Zinhle Matsebula29Aubrey Kalungia30Trust Zaranyika31Nyasha Masuka32Janney Wale33Ruaraidh Hill34 Amanj Kurdi1,35
Amanj Kurdi1,35 Angela Timoney1,36Stephen Campbell37,38
Angela Timoney1,36Stephen Campbell37,38 Johanna C. Meyer2
Johanna C. Meyer2- 1Strathclyde Institute of Pharmacy and Biomedical Sciences, University of Strathclyde, Glasgow, United Kingdom
- 2Division of Public Health Pharmacy and Management, School of Pharmacy, Sefako Makgatho Health Sciences University, Pretoria, South Africa
- 3Division of Clinical Pharmacology, Karolinska Institute, Karolinska University Hospital Huddinge, Stockholm, Sweden
- 4Health Economics Centre, University of Liverpool Management School, Liverpool, United Kingdom
- 5Department of Public Health Medicine, Steve Biko Academic Hospital, University of Pretoria, Pretoria, South Africa
- 6HIV & AIDS, TB and Maternal, Child and Women’s Health, National Department of Health, Pretoria, South Africa
- 7Department of Internal Medicine, Faculty of Medicine, University of Botswana, Gaborone, Botswana
- 8Department of Medicine, Princess Marina Hospital, Gaborone, Botswana
- 9Department of Pharmacy, Nyangabgwe Hospital, Francistown, Botswana
- 10Botswana Essential Drugs Action Program, Ministry of Health and Wellness, Gaborone, Botswana
- 11Effective Basic Services (eBASE) Africa, Bamenda, Cameroon
- 12Faculty of Health and Medical Sciences, University of Adelaide, Adelaide, SA, Australia
- 13Department of Public Health, University of Bamenda, Bambili, Cameroon
- 14School of Public Health, University of Ghana, Legon, Ghana
- 15Department of Pharmacy, Keta Municipal Hospital, Ghana Health Service, Keta, Ghana
- 16Department of Pharmacology and Pharmacognosy, School of Pharmacy, University of Nairobi, Nairobi, Kenya
- 17Department of Pharmacy Practice and Policy, Faculty of Health Sciences, University of Namibia, Windhoek, Namibia
- 18Department of Pharmacology and Therapeutics, Ekiti State University, Ado-Ekiti, Nigeria
- 19Department of Medicine, Ekiti State University Teaching Hospital, Ado-Ekiti, Nigeria
- 20Department of Pharmacology, Therapeutics and Toxicology, Lagos State University College of Medicine, Lagos, Nigeria
- 21Department of Medicine, Lagos State University Teaching Hospital, Lagos, Nigeria
- 22Centre for Diabetes & Endocrinology (Pty) Ltd, Johannesburg, South Africa
- 23Department of Pharmacy, Tshilidzini Regional Hospital, Limpopo Department Of Health, Shayandima, South Africa
- 24School of Clinical Medicine, University of the Witwatersrand, Johannesburg, South Africa
- 25Charlotte Maxeke Medical Research Cluster, Johannesburg, South Africa
- 26National Medicines Board, Federal Ministry of Health, Khartoum, Sudan
- 27Unaizah College of Pharmacy, Qassim University, Unaizah, Saudi Arabia
- 28Eswatini Medical Christian University, Mbabane, Swaziland
- 29Raleigh Fitkin Memorial Hospital, Manzini, Swaziland
- 30Department of Pharmacy, School of Health Sciences, University of Zambia, Lusaka, Zambia
- 31Department of Medicine, University of Zimbabwe College of Health Sciences, Harare, Zimbabwe
- 32Independent Health Systems Consultant, Harare, Zimbabwe
- 33Independent Consumer Advocate, Brunswick, VIC, Australia
- 34Liverpool Reviews and Implementation Group, Liverpool University, Liverpool, United Kingdom
- 35Department of Pharmacology, College of Pharmacy, Hawler Medical University, Erbil, Iraq
- 36NHS Lothian Director of Pharmacy, NHS Lothian, Edinburgh, United Kingdom
- 37Centre for Primary Care, Division of Population Health, Health Services Research and Primary Care, University of Manchester, Manchester, United Kingdom
- 38NIHR Greater Manchester Patient Safety Translational Research Centre, School of Health Sciences, University of Manchester, Manchester, United Kingdom
Background: There has been an appreciable increase in the number of people in Africa with metabolic syndrome and Type 2 diabetes (T2DM) in recent years as a result of a number of factors. Factors include lifestyle changes, urbanisation, and the growing consumption of processed foods coupled with increasing levels of obesity. Currently there are 19 million adults in Africa with diabetes, mainly T2DM (95%), estimated to grow to 47 million people by 2045 unless controlled. This has a considerable impact on morbidity, mortality and costs in the region. There are a number of issues to address to reduce the impact of T2DM including improving detection rates and current access to services alongside addressing issues of adherence to prescribed medicines. There are also high rates of co-morbidities with infectious diseases such as HIV and tuberculosis in patients in Africa with T2DM that require attention.
Objective: Document ongoing activities across Africa to improve the care of patients with T2DM especially around issues of identification, access, and adherence to changing lifestyles and prescribed medicines. In addition, discussing potential ways forward to improve the care of patients with T2DM based on ongoing activities and experiences including addressing key issues associated with co-morbidities with infectious diseases.
Our Approach: Contextualise the findings from a wide range of publications including internet based publications of national approaches coupled with input from senior level government, academic and other professionals from across Africa to provide future guidance.
Ongoing Activities: A number of African countries are actively instigating programmes to improve the care of patients with T2DM starting with improved diagnosis. This recognises the growing burden of non-communicable diseases across Africa, which has been neglected in the past. Planned activities include programmes to improve detection rates and address key issues with diet and lifestyle changes, alongside improving monitoring of care and activities to enhance adherence to prescribed medicines. In addition, addressing potential complexities involving diabetes patients with infectious disease co-morbidities. It is too early to fully assess the impact of such activities,
Conclusion: There are a number of ongoing activities across Africa to improve the management of patients with diabetes including co-morbidities. However, more needs to be done considering the high and growing burden of T2DM in Africa. Ongoing research will help further benefit resource allocation and subsequent care.
Introduction
The number of overweight and obese people is rising across Africa as a result of changes in lifestyles and reduced physical activity, more sedentary lifestyles, changing dietary habits and easy access to inexpensive processed foods, cultural habits, and increasing urbanization (Owiredu et al., 2008; Mbanya et al., 2014; Cois and Day, 2015; Ofori-Asenso et al., 2016; Werfalli et al., 2016; Buse et al., 2017; Kingdom of Eswatini - Ministry of Health, 2017; Ministry of Health and Social Services Namibia, 2017; SEMDSA, 2017; Werfalli et al., 2016; Zekewos et al., 2018; Osei-Yeboah et al., 2019). Such changes are leading to an increase in the number of patients with metabolic syndrome and type 2 diabetes (T2DM) across the continent (Mbanya et al., 2014; Kharroubi and Darwish, 2015; Agyemang et al., 2016; Todowede and Sartorius, 2017). Studies in South Africa suggest over 50% of the adult population (18 years and above) are overweight or obese and rising (Cois and Day, 2015), and in Nigeria 62% and 49% respectively of adults are overweight or obese (Commodore-Mensah et al., 2014). Kenyan women were also reported to be significantly more likely to have abdominal obesity compared to men (50.2% vs. 12.1%) (Mohamed et al., 2018). However, diabetes in sub-Saharan Africa is also present in patients with low to normal body mass indices (BMIs), which may reflect genetic diversities compared with populations in other continents (Kibirige et al., 2019). Overall, diabetes mellitus is a growing problem across Africa with an estimated 19 million adults affected including 14.2 million in sub-Saharan Africa (SSA) (International Diabetes Federation, 2019). Numbers are likely to grow to 41.6 million across Africa by 2045, principally T2DM (International Diabetes Federation, 2019).
As mentioned, rapid urbanization in Africa is one of the principal risk factors for increasing rates of T2DM across the continent. SSA is often regarded as the world's fastest urbanizing region, with the global share of African urban residents projected to grow from 11.3% in 2010 to 20% in 2050 (Saghir and Santoro, 2018). The city of Johannesburg in South Africa has been a part of a world-wide initiative called “Cities Changing Diabetes,” the purpose of which is to improve the management of patients with diabetes in urban areas using the principles of halves, i.e., approximately 50% of people with diabetes are diagnosed, of whom 50% receive care, of whom 50% achieve treatment target (recommended glucose levels), of whom approximately 50% would subsequently lead a life free from diabetes related complications equating to 6% of those with diabetes (Napier et al., 2017).
Activities are just starting across Africa to improve the care of patients with T2DM (Table 1). Typically though, the awareness of diabetes among patients remains a major challenge in SSA with only a minority of patients currently aware of their diabetic status and being actively treated, with only a small percentage being diagnosed pre-diabetes (Zekewos et al., 2018; Manne-Goehler et al., 2019). This needs to be urgently addressed given the morbidity, mortality, and costs associated with diabetes (Glover et al., 2012; Glezeva et al., 2015; Low Wang et al., 2016; Atun et al., 2017; Adibe et al., 2018; Lewis et al., 2018; Pheiffer et al., 2018; Rwegerera et al., 2018; Mapa-Tassou et al., 2019). Eighty percent of early deaths due to non-communicable diseases (NCDs) including diabetes and cardiovascular diseases (CVD) currently occur in lower and middle income countries (LMICs), with the morbidity and mortality of diabetes and other NCDs such as CVD likely to be greater than communicable disease by 2025 (Peer et al., 2014; Renzaho, 2015; Issaka et al., 2018). Overall, SSA currently has the highest rate of morbidity and mortality associated with diabetes world-wide (Pastakia et al., 2017). In South Africa for instance as a result of changes in peoples' diet and lifestyle, diabetes has moved from being the fifth leading underlying cause of death in 2013 to now the second most common cause, representing 5.5% of all recorded deaths (Statistics South Africa, 2016; Moosa et al., 2019). T2DM also results in a lower health status and quality of life (Fasanmade and Dagogo-Jack, 2015; da Mata et al., 2016; Adibe et al., 2018; Rwegerera et al., 2018), with high rates of sight threatening retinopathy among diabetic patients in Africa (Glover et al., 2012; Jingi et al., 2015; Cairncross et al., 2017; Pastakia et al., 2017; Lewis et al., 2018) as well as nephropathy (Thomas et al., 2016; Wagnew et al., 2018) and neuropathy (Awadalla et al., 2017; Sun et al., 2020). Overall, populations of African origin appear to have the highest prevalence of microvascular complications of diabetes exacerbated by frequent high blood pressure and inappropriate diabetes control among the diabetes population along with challenges of access to appropriate care (Mbanya and Sobngwi, 2003; Mbanya et al., 2010).

Table 1 Synopsis of ongoing national and local activities to improve the management of patients with T2DM in sub-Saharan Africa.
Prevalence rates of T2DM vary considerably among individual African countries exacerbated by high rates of undiagnosed cases of diabetes (Atun et al., 2017; Stokes et al., 2017; Pheiffer et al., 2018; Asmelash and Asmelash, 2019; Manne-Goehler et al., 2019;) (Appendix 1). Overall, it is estimated that up to 70% or more of cases of diabetes are currently undiagnosed in SSA (Mbanya et al., 2010; Fasanmade and Dagogo-Jack, 2015; Pastakia et al., 2017). This is a concern as diabetes and its associated comorbidities increase cardiovascular diseases (CVD), which are responsible for approximately 70% of diabetes-related deaths (Glezeva et al., 2015; Low Wang et al., 2016; Mwita et al., 2017; Sarfo et al., 2018). It is hoped that ongoing activities across Africa (Table 1) will start to address this especially with mortality rates enhanced by uncontrolled hypertension as well as lack of control of HbA1c and lipid levels, especially low density lipoproteins (LDL-C), coupled with inactivity (U.K. Prospective Diabetes Study Group, 1995; UK Prospective Diabetes Study Group, 1998; MRC/BHF Heart Protection, 2002; Wan et al., 2017). Currently, only a minority of patients with diabetes in Africa achieve optimal therapeutic targets (Sobngwi et al., 2012; Pinchevsky et al., 2015; Manne-Goehler et al., 2019), which is a real concern.
The economic impact of diabetes in Africa is also increasing with growing prevalence rates with US$9.5billion currently spent on diabetes in Africa (International Diabetes Federation, 2019). Atun et al. recently estimated that in 2015, the overall cost of diabetes in SSA was 1.2% of the gross domestic product (GDP), with approximately US$10·81 billion spent on direct medical costs with out-of-pocket expenditure likely to exceed 50% of overall health expenditure in many of the countries (Atun et al., 2017). In Nigeria, estimates suggest the annual direct costs of diabetes are up to US$1.639 billion per year in view of its population size and current prevalence rates, with the estimated monthly direct medical costs for patients with T2DM in Cameroon at US$148 per patient and in Nigeria varying between $262.22 to $400.52 per patient (Mapa-Tassou et al., 2019). Median monthly healthcare expenditure in Kenya in households with diabetes was US$100.00 of which US$7.00 was on medicines (Wirtz et al., 2018). The effect of NCDs in the work place is also of growing concern across countries including Kenya and South Africa (Rasmussen et al., 2016).
Diagnosis rates need to be improved to achieve the World Health Organization's (WHO) 25×25 Global Action Plan (2013) as well as Sustainable Development Goal (SDG) 3 to reduce premature deaths due to NCDs by a third by 2030 (Joseph et al., 2017; Roth et al., 2017). Concerns with rising rates of T2DM and its impact will persist unless addressed. This includes access to diagnostic and monitoring equipment and essential medicines in the first place (Mbanya et al., 2010; Piloya-Were et al., 2016; Kibirige et al., 2017) along with adequate diagnostic facilities (Manne-Goehler et al., 2019) given current concerns with diagnosis rates. The WHO in 2015 found that in Africa only 51% of the countries had metformin routinely available and only 40% insulin, well below the 80% target (Atun et al., 2017). This is a major concern especially with only metformin along with gliclazide and glibenclamide included in the WHO essential medicines list (EML) (World Health Organization, 2019). There have been concerns though with hypoglycemia with sulfonyl ureas (SUs) (Naidoo et al., 2014). However, this applies more to glibenclamide than other SUs including glipizide, glimepiride, and gliclazide as well as gliclazide modified release (MR) (Abrahamson, 2015; Colagiuri et al., 2018; Kalra et al., 2018). This is reflected in the current South African guidelines recommending that glibenclamide should no longer be prescribed, with for instance gliclazide MR replacing the more general term SUs (Naidoo et al., 2014). Having said this in Nigeria, glibenclamide is still on the national EML; however, chlorpropamide is still being prescribed by some practitioners (Erah and Eroje, 2013; Federal Ministry of Health, Nigeria, 2016). There have also been concerns recently with limited availability of insulin analogues when needed especially with the increasing availability of lower costs biosimilars. However in the first instance, soluble insulin injections as well as intermediate acting insulins need to be made routinely available to T2DM patients within public healthcare systems across Africa in accordance with the 2019 WHO EML before potentially funding any analogue (World Health Organization, 2019).
The availability of medicines to treat patients with T2DM should improve with ongoing programs across Africa, including South Africa, to improve access to medicines in patients with chronic diseases (Meyer et al., 2017) as well as ongoing programs to reduce the costs of medicines as a barrier to their use (Sandoz - A Novartis Division, 2015). However, more remains to be done with continual concerns regarding the availability of metformin and insulins across Africa. Efficient procurement of medicines is critical to ensure that patients with diabetes within public healthcare systems are able to obtain an uninterrupted supply of their medicines (Wirtz et al., 2016).
Newer oral medicines for patients with T2DM such as the DPP4 (dipeptidyl peptidase-4) and SGLT2 (sodium/glucose cotransporter 2) inhibitors have also been proposed (Naidoo et al., 2014; Imprialos et al., 2017; Bailey and Day, 2019; Li et al., 2019). However, there are major issues with affordability within public healthcare systems struggling to routinely make available metformin and basic insulins. In addition, a number of patients with T2DM across Africa are ketosis prone and this is difficult to manage if their renal function is not routinely monitored in primary healthcare centers (PHCs). Moreover, it is difficult to estimate the true prevalence of patients who are ketosis prone across Africa. Ketosis-prone diabetes is an “atypical” form of diabetes particularly prevalent in diabetic patients in SSA with characteristics of both type 1 and type 2 diabetes (Ahrén et al., 1988; Mbanya et al., 2010; Sjöholm, 2019), principally though ketosis-prone T2DM (Sjöholm, 2019). Published figures suggest a prevalence up to 15% of the diabetes population in Africa have ketosis-prone diabetes (Sobngwi et al., 2002; Mbanya et al., 2010; Sjöholm, 2019); however, this could be an under estimate. In addition, there are also concerns with available resources and co-payments within public healthcare systems in Africa leading to continued endorsement and listing of appropriate SUs and metformin rather than funding newer oral medicines such as the DPP4 and SGLT2 inhibitors, as well as concerns with inertia with physicians prescribing insulins rather than again funding newer more expensive oral anti-diabetic medicines (Davies et al., 2018; Mwita et al., 2019).
Alongside this, many African countries currently have inadequate facilities to manage both the microvascular and macrovascular complications of T2DM (Atun et al., 2017). This includes addressing sub-optimal management of patients with T2DM with currently only a minority of patients in SSA achieving glycemic control (Mwita et al., 2012; Sobngwi et al., 2012; Kibirige et al., 2014; Pinchevsky et al., 2015; Kibirige et al., 2017; Manne-Goehler et al., 2019). Glycemic control is improved though in specialist centers in SSA (Sobngwi et al., 2012; Mwita et al., 2019; Rwegerera et al., 2019). This reflects the fact that NCDs such as diabetes have been relatively neglected over the last decade across Africa in favor of infectious diseases including human immunodeficiency viruses (HIV), tuberculosis (TB), and malaria due to their burden (Atun et al., 2017; Pastakia et al., 2017; South African Lancet National Commission, 2019). However, this is beginning to change (Table 1). Diabetic populations of African origin appear to have the highest prevalence of microvascular complications exacerbated by frequent hypertension and inappropriate diabetes control along with challenges with access to appropriate care (Mbanya and Sobngwi, 2003; Mbanya et al., 2010). Treatment of hypertension is a particular concern among the Black African population. Thiazide diuretics and calcium channels blockers rather than angiotensin-converting-enzyme inhibitors (ACE inhibitors) are now considered as the most effective antihypertensives in the Black African population (Choukem et al., 2007; James et al., 2014; SEMDSA Type 2 Diabetes Guidelines Expert Committee, 2017). Consequently, while ACE inhibitors are indicated for patients with diabetes and proteinuria, they have a lesser effect in reducing blood pressure in the Black African population and their prescribing needs to be carefully managed (Mbui et al., 2017; Mwita et al., 2019). There is also typically low use of statins among diabetic patients in Africa, which again needs to be urgently addressed to reduce future CV complications (Sobngwi et al., 2012; Uloko et al., 2012; Mwita et al., 2019).
Overall, a number of key issues have been identified surrounding the management of patients with T2DM in Africa that need to be addressed alongside issues of diagnosis and medicine availability. These include access to care in the first place, which is typically among public sector PHC facilities across most of SSA (Atun et al., 2017). Access to physicians and medicines continues to be a challenge especially if this involves high patient co-payments and/or there are long distances and queues to see a healthcare professional, both of which have economic and emotional consequences for patients (Mendenhall and Norris, 2015; Dube et al., 2017; Nashilongo et al., 2017). The prohibitive costs of medicines in some LMICs, which can account for up to 60% or more of total healthcare costs, does affect continued medicine use including adherence for long terms conditions such as T2DM if much of this is out-of-pocket (Cameron et al., 2009; Mhlanga and Suleman, 2014; Ofori-Asenso and Agyeman, 2016; Ong et al., 2018). For instance in Nigeria, typically household savings and family support are needed to fund treatments for patients with T2DM, with a mean monthly expenditure of US$356 per patient (Okoronkwo et al., 2016) similar to other studies (Mapa-Tassou et al., 2019). In addition, for patients with diabetes in Nigeria, the costs of medicines can account for over 70% of total direct medical costs (Fadare et al., 2015). Greater use of generic medicines could help reduce these costs (Akunne et al., 2016); however, there are issues with the quality of generics in Nigeria which needs to be addressed (Fadare et al., 2016).
Patient knowledge regarding diabetes and its management, including self-management, can also be poor among patients with T2DM in Africa (Mogre et al., 2017; Bonger et al., 2018; Stephani et al., 2018; Moosa et al., 2019). This is exacerbated by low levels of education among patients attending PHC facilities in SSA with CVD including T2DM and hypertension; however, this is not universal (Moosa et al., 2015; Kassahun et al., 2016; Nashilongo et al., 2017; Rampamba et al., 2017; Mufunda et al., 2018; Chang et al., 2019; Moosa et al., 2019; Niguse et al., 2019). In addition, there are concerns that being overweight and obese is still seen as a sign of affluence in a number of African communities, although changing, and appreciable weight loss still has the stigma of HIV and acquired immune deficiency syndrome (AIDS) associated with it. This is important especially in countries where there are high prevalence rates of HIV as well as high rates of patients with both HIV and T2DM as seen for instance in Botswana compared with high income countries (Hatsu et al., 2009; Rankgoane-Pono et al., 2018). Treatment, including adherence to agreed guidelines for patients with T2DM, and subsequent patient adherence to prescribed medicines, are also generally sub-optimal in LMICs including Africa (Igbojiaku et al., 2013; Awodele and Osuolale, 2015; Fadare et al., 2015; Moosa et al., 2015; Sapkota et al., 2015; Elsous et al., 2017; Abate, 2019; Moosa et al., 2019). A number of factors appear responsible for poor control of T2DM including the age of patients, their lack of perception of the consequences of diabetes, forgetfulness regarding taking medication, adverse effects of the prescribed medicines, living in rural areas, affordability, and issues of motivation including family support (Adegbola et al., 2016; Waari et al., 2018; Abate, 2019; Dedefo et al., 2019; Mwita et al., 2019; Rwegerera et al., 2019). There are also concerns with the concomitant management of hypertension and hypercholesterolemia along with controlling HbA1c in patients with T2DM in Africa (Gudina et al., 2011; Sobngwi et al., 2012; Mwita et al., 2019). Other potential factors impacting on key issues such as adherence include concomitant co-morbidities such as infectious diseases appreciably increasing the pill burden and regimen complexity (Libby et al., 2013). Treatments for HIV can themselves also lead to weight gain and obesity further complicating the management of T2DM patients with HIV (Bailey et al., 2016; Pastakia et al., 2017; Kumar and Samaras, 2018; Coetzee et al., 2019; Venter et al., 2019). A study undertaken in an HIV clinic in South Africa found the metabolic syndrome was seen in 20% of cases within 1 year after initiation of anti-retroviral treatment (ART) despite the young age of patients, presumably as a consequence of ART exposure (Julius et al., 2011). Similarly, diabetes increases the chances of patients getting TB nearly threefold (Pastakia et al., 2017). Consequently, T2DM patients with infectious disease co-morbidities must be carefully managed.
There have been a number of initiatives across Africa to improve identification, prevention, and management of T2DM to reduce subsequent morbidity, mortality, and costs. These include national strategies (Ministry of Public Health and Sanitation Kenya, 2010; Ministry of Health Ghana, 2012; National Department of Health, 2016a; National Department of Health, 2016b; Federal Ministry of Health, SIDCAIN, World Diabetes Foundation, 2017; Kingdom of Eswatini - Ministry of Health, 2017; Ministry of Health and Social Services Namibia, 2017; Mukanu et al., 2017) as well as the development of contextualized guidelines combined with research to demonstrate the need for strategies to improve guideline adherence and to assess their impact in practice (Igbojiaku et al., 2013; Mukanu et al., 2017; Pastakia et al., 2017; SEMDSA, 2017). There have also been strategies to improve access and availability of medicines (Sandoz - A Novartis Division, 2015; Meyer et al., 2017; Nuche-Berenguer and Kupfer, 2018; Shannon et al., 2019; Rockers et al., 2019), as well as strategies to improve the monitoring and follow-up of patients including advice on the doses of medicines prescribed (Pastakia et al., 2015; Morris-Paxton et al., 2018; Chang et al., 2019). However, such activities are not universal across Africa. Alongside this, there have been initiatives among African countries surrounding patient education and empowerment, along with support mechanisms such as the CCMDD initiative in South Africa, to improve access to treatment as well as adherence to suggested lifestyle changes and prescribed medicines (Ovbiagele, 2015; Kassahun et al., 2016; Jaam et al., 2017; Meyer et al., 2017; Amadi et al., 2018; Gathu et al., 2018; Mufunda et al., 2018; Stephani et al., 2018; Manne-Goehler et al., 2019; Rampamba et al., 2019). However, only a limited number of papers have been published assessing the impact of different initiatives in these patients (Sapkota et al., 2015; Gathu et al., 2018; Rampamba et al., 2019). We are also seeing the rise in mobile technologies to improve care including adherence to medicines (Farmer et al., 2019; Opoku et al., 2019), which will be one of the subjects for future research projects across Africa. Typically, multiple interventions are required to improve the care of patients with T2DM (Sapkota et al., 2015; Rockers et al., 2019). However, resources to expand such interventions to derive maximum benefits have to be balanced against ongoing needs in other high priority health conditions (Renzaho, 2015).
Consequently, the principal objective of this paper is to document and debate ongoing challenges and activities to improve the care of patients with T2DM in Africa especially around issues of adherence to changing lifestyles and prescribed medicines. This includes appraising key issues associated with co-morbidities with infectious diseases such as HIV and the resultant implications. There have been a number of systematic reviews looking at key issues surrounding the management of patients with diabetes in Africa including initiatives to strengthen healthcare systems (Brouwer et al., 2015; Atun et al., 2017; Hill et al., 2017; Issaka et al., 2018; Jaam et al., 2017; Nuche-Berenguer and Kupfer, 2018; Ong et al., 2018; Owolabi et al., 2018; Stephani et al., 2018; Wagnew et al., 2018; Asmelash and Asmelash, 2019; Manne-Goehler et al., 2019). We are also aware of the recent NCD research conference for Africa to share evidence and identifying research priorities (Juma et al., 2019). However to date, there have only been a limited number of publications that have comprehensively focused on all aspects of care covering diagnosis, prevention, education, and treatment including access to appropriate medicines for patients with T2DM and subsequent adherence rates. There have also been only a limited number of publications assessing the influence and impact of different interventions to improve the care of patients with T2DM across Africa. In view of this, we sought to document ongoing activities across Africa to improve the care of patients with T2DM as well as contextualize any findings from a wide range of co-authors from across Africa and wider to provide future guidance. This does not included issues of counterfeit medicines as this is outside the scope of this paper (Kawamura, 2011; Alghannam et al., 2014).
We have specifically chosen T2DM as this accounts for up to 95% of patients with diabetes in SSA (Fasanmade and Dagogo-Jack, 2015). In view of this, we believe our findings and subsequent implications should be of interest to key stakeholders across Africa and wider to help further improve the care of patients with T2DM building on current efforts. We will be monitoring these developments in the future.
Our Approach
We did not perform a systematic review since there have been an appreciable number of recent publications, including systematic reviews, discussing ongoing research in this area and its implications including current prevalence rates, health system concerns, as well as possible policies and ways to improve future care (Brouwer et al., 2015; Agyemang et al., 2016; Hill et al., 2017; Jaam et al., 2017; Pastakia et al., 2017; Issaka et al., 2018; Nuche-Berenguer and Kupfer, 2018; Owolabi et al., 2018; Stephani et al., 2018; Wagnew et al., 2018; Asmelash and Asmelash, 2019; Farmer et al., 2019; Manne-Goehler et al., 2019; Mapa-Tassou et al., 2019). In addition, a number of the references, especially regarding ongoing national activities, are typically only available on the Internet as some of these have only just been launched. It is too early to assess the influence and impact of such national activities on key patient parameters as well as suggested activities to address key elements in the care provided. As mentioned, there have only been a limited number of publications to date in this area and only a limited number of studies including Sapkota et al. from LMICs (Sapkota et al., 2015; Gathu et al., 2018; Rampamba et al., 2019).
To address this knowledge and policy gap, we used senior level personnel from governments and their advisers, clinicians, academia, rational medicine use advisers, health technology assessment (HTA) personnel, as well as patient organization personnel, to suggest future activities for all key stakeholder groups across Africa to improve the future care of patients with T2DM. This included both short- and long-term initiatives, with the advice given based on relevant publications known to the co-authors coupled with their considerable knowledge of ongoing activities in their own countries. This builds on policy gaps and other recent papers to help improve the care of patients with T2DM across Africa (Atun et al., 2017; Pastakia et al., 2017 Owolabi et al., 2018; Manne-Goehler et al., 2019). The co-authors came from a wide range of backgrounds and countries in terms of their geography, population size, GDP per capita, as well as progress toward universal healthcare. We have successfully used this approach before to stimulate debate in other priority healthcare areas and situations to provide future guidance (Godman et al., 2010; Godman et al., 2014a; Godman et al., 2014b; Campbell et al., 2015; Godman et al., 2015; Ermisch et al., 2016; Bochenek et al., 2017; Moorkens et al., 2017; Godman et al., 2018; Vella Bonanno et al., 2019; Godman et al., 2020).
We did not split the African countries into low- or middle-income countries as the burden of T2DM and its implications is growing across all of Africa. Consequently, countries can learn from each other. We also did not systematically review each paper for its quality using well-known scales such as the Newcastle-Ottawa scale or the Cochrane risk of bias tool as our emphasis was on contextualizing the findings rather than performing a systematic review for the reasons given (Marra et al., 2016; Ong et al., 2018; Almeida et al., 2018; da Silva et al., 2018; Saleem et al., 2019). In addition, we did not review each paper to assess whether the presence of diabetes, especially T2DM, had been defined according to WHO and other internationally recognized diagnostic criteria in view of the objectives of this paper (World Health Organisation, 2006; Manne-Goehler et al., 2019).
Ongoing Activities and the Implications
Ongoing initiatives and activities among a range of African countries to improve the identification and management of patients with T2DM will be described first before debating potential approaches among all key stakeholder groups to improve future identification and management of patients with T2DM across Africa. This includes the cascade of treating patients with T2DM starting with glucose testing, diagnosis, lifestyle advice, as well as the prescribing of medicines and counseling for adherence to prescribed medicines (Manne-Goehler et al., 2019). We are aware for instance that most guidelines on the management of patients with T2DM in LMICs including African countries are inadequate in terms of their applicability, clarity, and active plans for dissemination (Owolabi et al., 2018). We are also aware that national guidelines when produced are not always readily available in primary and community healthcare centers or routinely consulted (Mashalla et al., 2016; Matsitse et al., 2017).
As mentioned, there will be a particular focus on strategies to improve access to medicines and subsequent adherence rates to prescribed medicines based on the combined experiences of the co-authors and the published literature.
Ongoing Initiatives and Activities Among African Countries
Table 1 contains details of a range of activities being undertaken among SSA countries to improve the management of patients with T2DM.
Suggested Activities Among All Key Stakeholder Groups to Improve Future Management of Patients With T2DM
We have based suggested activities and initiatives that still need to be undertaken among key stakeholder groups across Africa to improve the cascade of patient management (Manne-Goehler et al., 2019), and subsequently reduce future morbidity, mortality, and costs due to T2DM and its complications, principally on the experiences of the co-authors in the absence of published data. These are contained in Boxes 1–5 and build on Table 1.
Box 1. Suggested activities among national governments and authorities.
A) Short term
● Prioritize the screening for diabetes at all health care facilities in the country including those with diabetes alongside infectious diseases such as TB (Segafredo et al., 2019). This includes providing the basic tools and technologies to identify at risk patients and to monitor their progress—including providing BP monitors in all clinics alongside glucose monitoring systems, with the provision of self-monitoring systems important for patients on insulin.
● Improve the routine availability of medicines in the public sector to treat patients with T2DM including addressing concerns with the current lack of metformin, SUs, or insulins when this occurs. This includes ensuring the availability and use of low cost quality medicines (generics) to reduce patient co-payments where applicable. Initiatives could include improved supply chain management incorporating better stock control and forecasting abilities—building on initiatives in South Africa such as the Central Chronic Medication Dispensing and Distribution (CCMDD) initiative (Meyer et al., 2017)—as well as improved regulatory controls limiting the availability of poor quality generics where this is a concern.
● Introduce or enhance the implementation of programs including educational programs among T2DM patients to improve their lifestyles in association with other groups such as patient associations and other relevant NGOs.
● Review and improve where pertinent the training of healthcare professionals in the management of patients with T2DM in both undergraduate and postgraduate programs to enhance the future quality of care. This can include instigating CPD activities, and builds on ongoing programs in Ghana, South Africa, and wider.
● Instigate/refine training programs at both undergraduate and postgraduate levels to improve the care of patients with T2DM. This can include developing and implementing CPD programs building on initiatives in Ghana to upskill their knowledge—including understanding of the different oral medicines to treat T2DM and insulin preparations as well as their role and place especially in patients with various co-morbidities.
● Instigate policies to enhance adherence to prescribed medicines and dietary modifications building on ongoing initiatives across SSA including Kenya and South Africa as well as learnings from other NCDs. This involves improved understanding of key factors influencing adherence including the level of education, family and support systems, and funding issues, which is critical to enhance the future care of T2DM patients. It is likely mobile technologies will play an increasing role.
● Instigate training and other measures to improve the detection and treatment of T2DM-related causes of blindness such as diabetic retinopathy as well as causes of renal complications including preventative measures along with general measures to improve BP control (Chawla et al., 2010; Cappuccio and Miller, 2016).
B) Longer term
● Leadership and governance
● Greater prioritization of NCDs especially T2DM with its implications for morbidity, mortality, and costs. As part of this, instigate activities to develop or refine national strategies to improve the care of patients with T2DM, building on current activities among SSA countries (Table 1). This can include implementing national NCD strategies with their emphasis on identification, healthy lifestyle changes (physical activity, healthy eating, limiting processed foods, and weight management—including addressing concerns with any stigma/negative perceptions associated with weight loss) along with adequate treatment of patients with T2DM based on agreed national guidelines (cognizant of local co-morbidities including infectious diseases among the different African countries).
● Conduct screening for NCDs including T2DM among at risk individuals including those with a family history of diabetes, overweight or obesity at schools, workplaces, churches, and shopping centers as well as in PHC facilities.
● Health workforce
● Strengthen health care systems including ambulatory care systems as well as policies and initiatives to better identify and manage patients with T2DM. This can include making better use of healthcare professionals and community health workers in primary/community health clinics as well as community pharmacists to help with education and medication adherence (Boxes 3 and 4).
● Seek to address shortages of physicians where applicable including training and utilizing of other healthcare professionals such as clinical associates (or clinical officers), nurses, and community pharmacists to help manage patients with T2DM. This can also include instigating home visits by healthcare professionals such as dieticians, diabetic nurse educators, and podiatrists, to improve the care of patients; however, instilling that complex cases must be rapidly referred to specialists.
● Task-shifting through utilization of mid-level workers (such as pharmacists, physiotherapists and podiatrists) to support the clinical management of NCDs. As a result, enhance the multidisciplinary approach to the management of patients with T2DM throughout the healthcare system.
● Undertake multidisciplinary research at local, regional, and national settings to improve the future care of patents with T2DM including adherence to medicines, and seek to instigate any findings.
● Financing
● Accelerate the introduction of universal healthcare in the public sector where patient co-payments are currently an issue to improve the care of patients with T2DM.
● Improved efficiency
● Strengthen HTA capabilities especially when Ministries of Health are confronted with a number of potential initiatives coupled with limited resources, building on ongoing initiatives across sub-Saharan Africa including Ghana, Kenya, and South Africa (Hernandez-Villafuerte et al., 2016; Mueller et al., 2017; Hollingworth et al., 2018; Southern African Health Technology Assessment Society (SAHTAS), 2019).
● Address the social and cultural determinants of health in patients with T2DM through leadership at a national level if not already underway—building on initiatives in Botswana, Ghana, Kenya, the Kingdom of Eswatini, Namibia, and South Africa to prevent or manage the risk factors associated with T2DM through greater stakeholder collaboration (MoH. Republic of Kenya Ministry of Health; National Department of Health South Africa, 2013; Ministry of Health and Social Services Namibia, 2017; Kingdom of Eswatini - Ministry of Health, 2017; Botswana National Multisectoral Strategy for the Prevention and Control of Non-Communicable Diseases, 2017; South African Lancet National Commission, 2019).
● Disseminate NCD information including T2DM regularly in national political forums, e.g., public speeches and in parliamentary debates.
● Strengthen the monitoring and evaluation of the management and treatment of T2DM to ensure that efforts are in line with the burden of NCDs. This includes regular auditing of the management of patients with T2DM against agreed national guidelines and seek to introduce quality indicators where concerns. Quality indicators can include HbA1c, BP, and lipid level goals developed with the help of all key stakeholders using robust methodologies (Campbell et al., 2011; Campbell et al., 2015).
● Research
● Continue to research methods to improve medication and dietary adherence including counseling, addressing concerns with processed foods and addressing patients' fears and beliefs including weight loss. In addition, researching potentially patient diaries and mobile messaging services as well as measures to enhance patient satisfaction with healthcare services (Habte et al., 2017; Waari et al., 2018; Moosa et al., 2019; Farmer et al., 2019; Rampamba et al., 2019). Subsequently, seek to instigate such findings.
● Fund ongoing research around diabetic phenotypes among the African population compared with other continents and its impact on key issues such as insulin resistance to improve future care (Pastakia et al., 2017; Kibirige et al., 2019).
NB: BP, Blood Pressure; CPD, Continual Professional Development; HTA, Health Technology Assessment; NCD, Non-communicable disease; NGOs, Non-governmental organizations; PHCs, Primary Healthcare Centres; SSA, sub-Saharan Africa; SUs, Sulphonylureas; TB, Tuberculosis; T2DM, Type 2 Diabetes.
Box 2. Suggested activities among physicians (hospital and ambulatory care).
A) Short term
● Instigate/refine training programs at both undergraduate and postgraduate levels to improve the care of patients with T2DM.
● This can include developing and implementing CPD programs building on initiatives in Ghana as well as programs to enhance timely diagnosis, management and follow-up of patients with T2DM including the management of patients with T2DM with HIV and TB.
● Instigate in-service training where pertinent including any updated guidelines for new medicines.
● Take part in Pharmaceutical (Drug) and Therapeutic Committees and other fora to ensure possible treatment decisions are in line with national guidelines and essential medicine lists, and evidence–based especially where co-morbidities.
● Ensure prompt referral of patients (ambulatory/primary care) to specialized centers where these exist and where necessary—including complex patients with multiple co-morbidities.
● Formulate care plans for patients and monitor prescribing (audit) against agreed guidance, especially those with co-morbidities including infectious diseases with rapid referral to specialist centers for more complex patients including those with multiple co-morbidities.
● Communicate with patients the importance of adherence to medicines, and seek to monitor this. This can be through diaries and other mechanisms including the use of mobile technologies.
B) Longer term
● Actively become involved in future research to improve the management of patients with T2DM across Africa given the high rate of co-morbidities especially infectious diseases in SSA compared with other continents as well as positive views toward overweight and obesity among populations especially in SSA.
NB: CPD, continuous professional development; HIV, human immunodeficiency virus; SSA, sub-Saharan Africa; TB, tuberculosis; T2DM,Type 2 Diabetes.
Box 3. Suggested activities among pharmacists (hospital and ambulatory care)
A) Short term
● Extend the role of pharmacists in hospitals and in the community to help improve the care of patients with T2DM. This can include counseling on issues of medication adherence, potential side-effects of medicines, and dispelling myths especially with community pharmacists often the first point of contact for patients with ailments in Africa.
● Encourage pharmacists to join national diabetes groups (such as ZEDMA in Zimbabwe) to help debate key issues regarding the use of medicines to treat patients with T2DM.
● Pharmacists as a vital part of the medicine supply chain need to instigate measures to reduce out-of-stock situations for essential medicines to treat patients with T2DM in public health facilities. The objective being to reduce reliance on private pharmacies especially where co-payments are an issue.
● Pharmacists should also monitor medicine availability in hospitals as part of DTC activities to help reduce out-of-stock situations, and work with physicians and others to instigate alternative medicines should the need arise.
● Pharmacists should also seek to encourage the use of generic medicines where possible to reduce patient co-payments where pertinent as well as healthcare costs.
B) Longer term
● Pharmacists need to become actively involved with auditing medicine use and providing support and other services to improve medication adherence. These can include mobile alerts, diaries, storyboards, and general information to enhance adherence, and can be part of DTC activities in hospitals as well as part of PHC activities in ambulatory care.
● Take part in research regarding factors impacting on medication adherence and possible ways to address this within their own health service, and seek to actively address and implement key findings.
NB: DTC, Drug and Therapeutic Committee; PHC, Primary Healthcare Centre; SSA, sub-Saharan Africa; T2DM, Type 2 diabetes.
Box 4. Suggested activities among other healthcare professionals in ambulatory and hospital care including nurse practitioners
A) Short term
● Use nurse practitioners and others to help screen for T2DM in the community especially at risk groups (Box 1)
● Work with other key stakeholders to provide accurate information to patients on the management of their condition including self-care to help prevent complications from occurring
B) Longer term
● Become involved with developing minimal standards of care for patients with T2DM in primary/community healthcare centers and subsequently monitoring the management of patients against agreed standards. This can include lifestyle changes and adherence to medicines as well as identifying acute and chronic complications for rapid referral
● Actively seek ways to provide support to patients and their caregivers to take control of their own health and to enhance adherence to lifestyle advice and any medicines prescribed
● Actively seek to improve the knowledge of medicines and self-management practices among fellow nurses and other community health workers regarding the care of patients with T2DM to enhance task shifting efforts at the primary/community level—ultimately helping to reduce time spent on long queues and the implications on key issues such as adherence. Concurrently with this, rapidly refer more complex patients to specialists given ongoing concerns
● Provide evidence–based care especially regarding complications of diabetes such as ulcers
● Take part in research initiatives to improve the future care of patients with T2DM, and seek to instigate the outcome of any research activities.
NB: T2DM, Type 2 diabetes.
Box 5. Suggested activities among patients/support services.
A) Short term
● Help communicate the importance of detection and management of T2DM including lifestyle changes and adherence to medicines to help reduce the morbidity and mortality of T2DM. This builds on progressive activities of a number of diabetes patient groups in SSA (Table 1) and is especially important where there are limited facilities to manage the complications of diabetes including renal complications, retinopathy and diabetic ulceration.
● Help to instigate communication and other programs to encourage patients to join national Diabetic Associations as well as generally encouraging patients and their carers to take part in peer education and support groups.
● Help provide easy to understand guidance to patients to help with their understanding of their condition as well as improve the management of their condition including lifestyle and medication advice. Such guidance should also help to dispel cultural and social stigmas associated with T2DM including those surrounding weight loss.
● Instigate activities encouraging recreational activities as well encouraging patients to ask questions when they are still unsure of their condition/instructions given and to seek prompt medical help when they experience changes in their condition.
● Seek generally to strengthen family support structures through education and socio-economic empowerment.
● Work with all key stakeholders to enhance their understanding of any concerns that patients and their support network may have regarding the management of T2DM and potential complications to better target educational and other activities.
B) Longer term
● Formulate and empower support groups among patients with T2DM such as adherence clubs to enhance the transfer of knowledge and self-management aspects among patients.
● Help longer term to develop innovative interventions tailored to the culture of patients in given African countries to enhance adherence to medication and lifestyle changes, such as storytelling, which have shown to be successful in other NCDs (Houston et al., 2011). This can increasingly be via mobile technologies and other support systems (Bonoto et al., 2017; Lewis et al., 2018; Farmer et al., 2019; Owolabi and Goon, 2019).
● Encourage greater involvement in the prevention of diabetes complications by self-monitoring of foot health and active participation in screening for eye, feet, and renal complications.
● Encourage key stakeholders to include patient support groups in future research activities and with the communication of their findings to improve future care.
NB: T2DM, Type 2 diabetes.
Suggested activities include increasing recognition of the burden of T2DM across Africa to raise its priority status. As a result, seek to appreciably reduce the number of patients across Africa currently not being diagnosed with T2DM including those with pre-diabetes. Concerns with the availability and use of medicines, especially those contained in the WHO EML, needs to be addressed including metformin. There are also concerns with poor adherence rates to prescribed medicines and prescribing guidelines, the routine availability of prescribed medicines, and the development of insulin resistance among diabetic patients. All these concerns need to be addressed to reduce future morbidity and mortality. The complexity of the management of patients with T2DM is enhanced if they have infectious diseases such as HIV and TB, which is appreciably more likely in SSA than high income countries where most guidelines emanate from. As a result, guidelines need be country and region specific taking into account genetic and other factors including patients with diabetes across Africa having low to normal BMIs, those with ketosis-prone T2DM, as well as appropriate management of those with co-morbidities including hypertension and infectious diseases. This is unlike the situation in many other continents.
Suggested activities will include those at governmental and national levels as well as among the different healthcare professional groups and patients to improve the future care of patients with T2DM. Potential initiatives to improve adherence rates to prescribed medicines will also be discussed given current concerns.
In addition, there is an ongoing need to improve HTA capabilities across Africa to help fully assess the effectiveness and cost-effectiveness of different approaches, including different treatment approaches, especially given limited available resources and potentially multiple possible initiatives. This can build on existing research across countries (Kriza et al., 2014; Hernandez-Villafuerte et al., 2016; Doherty et al., 2017; Mueller et al., 2017; Hollingworth et al., 2018; Juma et al., 2019) for evidence–based decision making.
Discussion and Conclusion
We believe this is the first comprehensive review to collate ongoing and planned activities across Africa to improve the management of patients with T2DM as well as suggest potential future strategies especially around medicine management. As a result, enable African countries to compare and contrast ongoing activities as well as debate potential future activities while the evidence base grows regarding their potential influence on reducing future morbidity, mortality, and costs due to T2DM.
It is encouraging to see that an appreciable number of African countries are actively instigating programs to improve the care of patients with T2DM starting with improving diagnosis (Table 1), with countries such as Cameroon looking to instigate pilot activities starting in key regions. This is important with T2DM a growing problem across Africa with an estimated 19 million adults in Africa currently with diabetes and increasing (International Diabetes Federation, 2019), and recognizes the growing burden of NCDs across Africa, and we will be reporting on some of the findings in the future.
Key national activities in Africa (Box 1) include health system strengthening as well as improving the subsequent management of patients with T2DM including those with co-morbidities. This starts with the development or refinement of national action plans to enhance the care of patients with NCDs including those with T2DM. Initial activities include improved screening and diagnosis of high risk patients at a number of venues including schools, workplaces, churches, and shopping centers as well as in PHC facilities. This includes patients with pre-diabetes especially those with other cardiovascular diseases (Kharroubi and Darwish, 2015; Mbugua et al., 2017; Todowede and Sartorius, 2017) to reduce future morbidity, mortality, and costs. Treatment approaches comprise both pharmacological treatments to prevent cardiovascular complications as well as lifestyle changes including diet changes.
Access to medicines is especially important across Africa with for instance up to 75% of patients having difficulties with obtaining insulin (Manne-Goehler et al., 2019). The very least is the routine availability of metformin, appropriate SUs, and soluble and intermediate insulins as well as the routine availability of monitoring equipment for T2DM patients on insulin. The development of universal health care as well as the assistance of donors and commercial organizations can be beneficial here (Sandoz - A Novartis Division, 2015; Meyer et al., 2017; Shannon et al., 2019). Initiatives to encourage the use of generics where possible, obtain low prices for quality medicines as well as instigate effective distribution systems can also enhance access to effective medicines in both public and community health centers (Cameron et al., 2012; Kaplan et al., 2012; Meyer et al., 2017; Pastakia et al., 2017). The development and instigation of evidence–based guidelines taking account of local co-morbidities including HIV and TB as well as genetics will also be a key step towards improving the management of patients with T2DM across Africa, enhanced by the auditing of current prescribing patterns (Pastakia et al., 2017; Owolabi et al., 2018). Furthermore, key stakeholder involvement in the production of country guidelines is seen as important to enhance their utilization building on the experiences in other countries (Gustafsson et al., 2011; Bjorkhem-Bergman et al., 2013; Eriksen et al., 2017).
A key concern across Africa is the multi-morbidity among patients with T2DM including co-morbidity with HIV and TB. This adds to the burden of the disease, exacerbated by these infectious conditions. Consequently, country specific guidelines need to be cognizant of this with rapid referral systems in place for more complex cases given the improved management of patients in tertiary centers. Prescribers need to be cognizant of the potential for HIV treatments to exacerbate diabetes and also for diabetes to exacerbate TB. This needs to be emphasized during physician and healthcare professional training, followed up by continuous professional development and other activities.
Concerns with the pharmacological management of patients with T2DM include adherence to medicines, which is typically sub-standard, as well as insulin resistance. A number of studies have shown the importance of healthcare professionals such as pharmacists, nurse practitioners, and community health workers, improving subsequent adherence and outcomes (Dube et al., 2017; Ong et al., 2018), with more studies planned given current concerns. We envisage that innovative approaches such as the increasing use of mobile technologies will be adopted to enhance adherence to lifestyle changes and medicines, and we will be monitoring this development in the future (Opoku et al., 2019; Owolabi and Goon, 2019). Countries can also continue to learn from each other to improve future care.
Whatever new initiatives or treatment approaches are chosen, it is likely that countries will need to expand on their HTA capabilities to assist with rational choices given continuing pressure on resources. This is already happening in countries such as Ghana and South Africa, and will expand further. Potential choices for governments consist of enhancing the infrastructure including public/community healthcare centers with multiple personnel incorporating physicians, medical officers, pharmacists, nurses, and others, to aid identification and reduce the development of complications in patients with T2DM and associated hospitalization. In addition, seek ways to address key issues regarding the availability of medicines for the management of diabetes and its complications including reducing co-payments where these exist. Multiple approaches also appear needed to address poor adherence rates to prescribed medicines where these occur, which will be the subject of future research projects.
In conclusion, we believe our findings and subsequent implications, including suggested activities (Boxes 1 to 5) for all key stakeholder groups, should be of interest to key groups across Africa and wider to improve the future care of patients with T2DM, building on current efforts (Table 1). This is essential given rising rates of obesity in Africa with their subsequent impact on morbidity, mortality, and costs. We will be monitoring these developments in the future especially as more studies become available evaluating ongoing initiatives among the different African countries and the implications.
Author Contributions
BG, JF, OO and JoM devised the concept of the paper. All authors subsequently contributed to its content and approved the final version.
Conflict of Interest
LD is employed by the Centre for Diabetes & Endocrinology (Pty) Ltd.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. However, a number of them are employed by national or regional governments in Ministries of Health or are advisers to them. In addition, advisers to the World Health Organisation.
References
Abate, T. W. (2019). Medication non-adherence and associated factors among diabetes patients in Felege Hiwot Referral Hospital, Bahir Dar city administration, Northwest Ethiopia. BMC Res. Notes 12 (1), 175.
Abrahamson, M. J. (2015). Should sulfonylureas remain an acceptable first-line add-on to metformin therapy in patients with type 2 diabetes? yes, they continue to serve us well! Diabetes Care 38 (1), 166–169.
Adegbola, S. A., Marincowitz, G. J., Govender, I., Ogunbanjo, G. A. (2016). Assessment of self-reported adherence among patients with type 2 diabetes in Matlala District Hospital, Limpopo Province. Afr. J. Prim. Health Care Fam. Med. 8 (1), e1–e5.
Adekanmbi, V. T., Uthman, O. A., Erqou, S., Echouffo-Tcheugui, J. B., Harhay, M. N., Harhay, M. O. (2019). Epidemiology of prediabetes and diabetes in Namibia, Africa: A multilevel analysis. J. Diabetes 11 (2), 161–172.
Adeloye, D., Ige, J. O., Aderemi, A. V., Adeleye, N., Amoo, E. O., Auta, A., et al. (2017). Estimating the prevalence, hospitalisation and mortality from type 2 diabetes mellitus in Nigeria: a systematic review and meta-analysis. BMJ Open 7 (5), e015424.
Adibe, M. O., Anosike, C., Nduka, S. O., Isah, A. (2018). Evaluation of health status of type 2 diabetes outpatients receiving care in a tertiary hospital in Nigeria. Pharm. Econ. - Open 2 (3), 337–345. doi: 10.1007/s41669-017-0056-x
Agyemang, C., Meeks, K., Beune, E., Owusu-Dabo, E., Mockenhaupt, F. P., Addo, J., et al. (2016). Obesity and type 2 diabetes in sub-Saharan Africans - Is the burden in today's Africa similar to African migrants in Europe? The RODAM study. BMC Med. 14 (1), 166.
Ahrén, B., Corrigan, C. B., Alberti, K. G. (1988). Plasma insulin and C-peptide responses to oral glucose in newly diagnosed diabetics in north-western Tanzania. East Afr. Med. J. 65, 847–851.
Akunne, O. O., Godman, B., Adedapo, A. D., Truter, I., Fadare, J. (2016). Statin prescribing among hypertensive patients in southwest Nigeria: findings and implications for the future. J. Comp. Effect. Res. 5 (3), 281–288.
Alghannam, A., Aslanpour, Z., Evans, S., Schifano, F. (2014). A systematic review of counterfeit and substandard medicines in field quality surveys. Integrated Pharm. Res. Pract. 3, 71–88.
Ali, Y. A., Almobarak, A. O., Awadalla, H., Elmadhoun, W. M., Ahmed, M. H. (2017). Obesity among Sudanese adults with diabetes: a population-based survey. Ann. Trans. Med. 5 (12), 252.
Almeida, P., Silva, T. B. C., de Assis Acurcio, F., Guerra Junior, A. A., Araujo, V. E., Diniz, L. M., et al. (2018). Quality of life of patients with type 1 diabetes mellitus using insulin analog glargine compared with NPH insulin: a systematic review and policy implications. Patient 11 (4), 377–389.
Amadi, C. E., Lawal, F. O., Mbakwem, A. C., Ajuluchukwu, J. N., Oke, D. A. (2018). Knowledge of cardiovascular disease risk factors and practice of primary prevention of cardiovascular disease by community pharmacists in Nigeria: a cross-sectional study. Int. J. Clin. Pharm. 40 (6), 1587–1595.
Aptantech (2019). Sanofi Kenya launches its first digital diabetes patient support program in Nairobi. Available at URL: https://aptantech.com/2019/05/sanofi-kenya-launches-its-first-digital-diabetes-patient-support-program-in-nairobi/.
Arthur, R. (2018). South Africa introduces sugar tax. Available at URL: https://www.beveragedaily.com/Article/2018/04/03/South-Africa-introduces-sugar-tax.
Asamoah-Boaheng, M., Sarfo-Kantanka, O., Tuffour, A. B., Eghan, B., Mbanya, J. C. (2019). Prevalence and risk factors for diabetes mellitus among adults in Ghana: a systematic review and meta-analysis. Int. Health 11 (2), 83–92.
Asmelash, D., Asmelash, Y. (2019). The burden of undiagnosed diabetes mellitus in adult African population: a systematic review and meta-analysis. J. Diabetes Res. 2019, 4134937.
Atun, R., Davies, J. I., Gale, E. A. M., Barnighausen, T., Beran, D., Kengne, A. P., et al. (2017). Diabetes in sub-Saharan Africa: from clinical care to health policy. Lancet Diabetes Endocrinol. 5 (8), 622–667.
Awadalla, H., Noor, S. K., Elmadhoun, W. M., Almobarak, A. O., Elmak, N. E., Abdelaziz, S. I., et al. (2017). Diabetes complications in Sudanese individuals with type 2 diabetes: Overlooked problems in sub-Saharan Africa? Diabetes Metab. Syndr. 11 (Suppl 2), S1047–S1s51.
Awodele, O., Osuolale, J. A. (2015). Medication adherence in type 2 diabetes patients: study of patients in Alimosho General Hospital, Igando, Lagos, Nigeria. Afr. Health Sci. 15 (2), 513–522.
Bailey, C. J., Day, C. (2019). The future of new drugs for diabetes management. Diabetes Res. Clin. Pract. 155, 107785.
Bailey, S. L., Ayles, H., Beyers, N., Godfrey-Faussett, P., Muyoyeta, M., du Toit, E., et al. (2016). Diabetes mellitus in Zambia and the Western Cape province of South Africa: prevalence, risk factors, diagnosis and management. Diabetes Res. Clin. Pract. 118, 1–11.
Bastawrous, A., Mathenge, W., Wing, K., Bastawrous, M., Rono, H., Weiss, H. A., et al. (2017). The incidence of diabetes mellitus and diabetic retinopathy in a population-based cohort study of people age 50 years and over in Nakuru, Kenya. BMC Endocr. Disord. 17 (1), 19.
Basu, S., Wagner, R. G., Sewpaul, R., Reddy, P., Davies, J. (2019). Implications of scaling up cardiovascular disease treatment in South Africa: a microsimulation and cost-effectiveness analysis. Lancet Global Health 7 (2), e270–ee80.
Bigna, J. J., Nansseu, J. R., Katte, J. C., Noubiap, J. J. (2018). Prevalence of prediabetes and diabetes mellitus among adults residing in Cameroon: a systematic review and meta-analysis. Diabetes Res. Clin. Pract. 137, 109–118.
Bjorkhem-Bergman, L., Andersen-Karlsson, E., Laing, R., Diogene, E., Melien, O., Jirlow, M., et al. (2013). Interface management of pharmacotherapy. Joint hospital and primary care drug recommendations. Eur. J. Clin. Pharmacol. 69 (Suppl 1), 73–78. doi: 10.1007/s00228-013-1497-5
Bochenek, T., Abilova, V., Alkan, A., Asanin, B., de Miguel Beriain, I., Besovic, Z., et al. (2017). Systemic measures and legislative and organizational frameworks aimed at preventing or mitigating drug shortages in 28 European and Western Asian countries. Front. Pharmacol. 8, 942.
Boehringer Ingelheim (2019). Breaking access and awareness barriers in hypertension and diabetes care through mobile technology. Available at URL: https://www.mea.boehringer-ingelheim.com/press-release/breaking-access-and-awareness-barriers-hypertension-and-diabetes-care-through-mobile.
Bonger, Z., Shiferaw, S., Tariku, E. Z. (2018). Adherence to diabetic self-care practices and its associated factors among patients with type 2 diabetes in Addis Ababa, Ethiopia. Patient Preference Adherence 12, 963–970.
Bonoto, B. C., de Araujo, V. E., Godoi, I. P., de Lemos, L. L., Godman, B., Bennie, M., et al. (2017). Efficacy of mobile apps to support the care of patients with diabetes mellitus: a systematic review and meta-analysis of randomized controlled trials. JMIR mHealth uHealth 5 (3), e4.
Bosu, W. K. (2012). A comprehensive review of the policy and programmatic response to chronic non-communicable disease in Ghana. Ghana Med. J. 46 (2 Suppl), 69–78.
Botswana National Multisectoral Strategy for the Prevention and Control of Non-Communicable Diseases (2017). Available at URL: https://www.iccp-portal.org/system/files/plans/20171129%20Botswana%20multisec%20NCDs%20strategy%20-%20final.pdf.
Brouwer, E. D., Watkins, D., Olson, Z., Goett, J., Nugent, R., Levin, C. (2015). Provider costs for prevention and treatment of cardiovascular and related conditions in low- and middle-income countries: a systematic review. BMC Public Health 15, 1183.
Burn, H., Pons, J. (2015). Diabetic retinopathy in Swaziland. Community Eye Health 28 (92), s18–s21.
Buse, K., Tanaka, S., Hawkes, S. (2017). Healthy people and healthy profits? Elaborating a conceptual framework for governing the commercial determinants of non-communicable diseases and identifying options for reducing risk exposure. Global Health 13 (1), 34.
Cairncross, J. P., Steinberg, W. J., Labuschagne, M. J. (2017). Prevalence of eye pathology in a group of diabetic patients at National District Hospital Outpatient Department in Bloemfontein, South Africa. Afr. J. Prim. Health Care Fam. Med. 9 (1), e1–e7. doi: 10.4102/phcfm.v9i1.1440
Cameron, A., Ewen, M., Ross-Degnan, D., Ball, D., Laing, R. (2009). Medicine prices, availability, and affordability in 36 developing and middle-income countries: a secondary analysis. Lancet 373 (9659), 240–249. doi: 10.1016/S0140-6736(08)61762-6
Cameron, A., Mantel-Teeuwisse, A. K., Leufkens, H. G., Laing, R. O. (2012). Switching from originator brand medicines to generic equivalents in selected developing countries: how much could be saved? Value In Health: J. Int. Soc. Pharmacoecon. Out. Res. 15 (5), 664–673.
Campbell, S. M., Kontopantelis, E., Hannon, K., Burke, M., Barber, A., Lester, H. E. (2011). Framework and indicator testing protocol for developing and piloting quality indicators for the UK quality and outcomes framework. BMC Fam. Pract. 12, 85.
Campbell, S. M., Godman, B., Diogene, E., Furst, J., Gustafsson, L. L., MacBride-Stewart, S., et al. (2015). Quality indicators as a tool in improving the introduction of new medicines. Basic Clin. Pharmacol. Toxicol. 116 (2), 146–157.
Cappuccio, F. P., Miller, M. A. (2016). Cardiovascular disease and hypertension in sub-Saharan Africa: burden, risk and interventions. Internal Emergency Med. 11 (3), 299–305.
Chang, H., Hawley, N. L., Kalyesubula, R., Siddharthan, T., Checkley, W., Knauf, F., et al. (2019). Challenges to hypertension and diabetes management in rural Uganda: a qualitative study with patients, village health team members, and health care professionals. Int. J. Equity Health 18 (1), 38.
Chawla, T., Sharma, D., Singh, A. (2010). Role of the renin angiotensin system in diabetic nephropathy. World J. Diabetes 1 (5), 141–145.
Choukem, S. P., Kengne, A. P., Dehayem, Y. M., Simo, N. L., Mbanya, J. C. (2007). Hypertension in people with diabetes in sub-Saharan Africa: revealing the hidden face of the iceberg. Diabetes Res. Clin. Pract. 77 (2), 293–299.
Coetzee, L., Bogler, L., De Neve, J. W., Barnighausen, T., Geldsetzer, P., Vollmer, S. H. I. V. (2019). Antiretroviral therapy and non-communicable diseases in sub-Saharan Africa: empirical evidence from 44 countries over the period 2000 to 2016. J. Int. AIDS Soc. 22 (7), e25364.
Cois, A., Day, C. (2015). Obesity trends and risk factors in the South African adult population. BMC Obes. 2, 42.
Colagiuri, S., Matthews, D., Leiter, L. A., Chan, S. P., Sesti, G., Marre, M. (2018). The place of gliclazide MR in the evolving type 2 diabetes landscape: a comparison with other sulfonylureas and newer oral antihyperglycemic agents. Diabetes Res. Clin. Pract. 143, 1–14.
Commodore-Mensah, Y., Samuel, L. J., Dennison-Himmelfarb, C. R., Agyemang, C. (2014). Hypertension and overweight/obesity in Ghanaians and Nigerians living in West Africa and industrialized countries: a systematic review. J. Hypertens. 32 (3), 464–472.
da Mata, A. R., Alvares, J., Diniz, L. M., da Silva, M. R., Alvernaz dos Santos, B. R., Guerra Junior, A. A., et al. (2016). Quality of life of patients with diabetes mellitus types 1 and 2 from a referal health centre in Minas Gerais, Brazil. Expert Rev. Clin. Pharmacol. 9 (5), 739–746.
da Silva, W. C., de Araujo, V. E., Lima, E., Dos Santos, J. B. R., Silva, M., Almeida, P., et al. (2018). Comparative effectiveness and safety of monoclonal antibodies (Bevacizumab, Cetuximab, and Panitumumab) in combination with chemotherapy for metastatic colorectal cancer: a systematic review and meta-analysis. BioDrugs: Clin. Immunother. Biopharm. Gene Ther. 32 (6), 585–606.
Davies, M. J., D'Alessio, D. A., Fradkin, J., Kernan, W. N., Mathieu, C., Mingrone, G., et al. (2018). Management of hyperglycemia in type 2 diabetes, 2018. a consensus report by the American diabetes association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 41 (12), 2669–2701. doi: 10.2337/dci18-0033
Dedefo, M. G., Ejeta, B. M., Wakjira, G. B., Mekonen, G. F., Labata, B. G. (2019). Self-care practices regarding diabetes among diabetic patients in West Ethiopia. BMC Res. Notes 12 (1), 212.
Diabetes Association of Botswana (2019). Available at URL: https://www.idf.org/our-network/regions-members/africa/members/1-botswana.html?layout=details&mid=20.
Diabetes Association of Namibia (2019). Available at URL: http://www.diabetes.iway.na/.
Diabetes Association of Nigeria (2019). Available at URL: https://www.idf.org/our-network/regions-members/africa/members/20-nigeria.html?layout=details&mid=143.
Diabetes Kenya. Available at URL: https://www.idf.org/our-network/regions-members/africa/members/13-kenya.html?layout=details&mid=122.
Djrolo, F., Adoukonou, T., Houehanou, C., Houinato, J. D., Houinato, D. (2015). Diabetes in Borgou department in Benin: prevalence and associated factors. J. Diabetes Mellitus 5, 90–96.
Doherty, J. E., Wilkinson, T., Edoka, I., Hofman, K. (2017). Strengthening expertise for health technology assessment and priority-setting in Africa. Glob. Health Action 10 (1), 1370194.
Dube, L., Rendall-Mkosi, K., Van den Broucke, S., Bergh, A.-M., Mafutha, N. G. (2017). Self-management support needs of patients with chronic diseases in a South African township: a qualitative study. J. Community Health Nurs. 34 (1), 21–31.
Elmadhoun, W. M., Noor, S. K., Ibrahim, A. A., Bushara, S. O., Ahmed, M. H. (2016). Prevalence of diabetes mellitus and its risk factors in urban communities of north Sudan: Population-based study. J. Diabetes 8 (6), 839–846.
El-Sayed, E. F., Awadalla, H., Noor, S. K., Elmadhoun, W. M., Sulaiman, A. A., Almobarak, A. O., et al. (2018). Sugar intake in Sudanese individuals was associated with some features of the metabolic syndrome: population based study. Diabetes Metab. Syndr. 12 (3), 245–250.
Elsous, A., Radwan, M., Al-Sharif, H., Abu Mustafa, A. (2017). Medications adherence and associated factors among patients with type 2 diabetes mellitus in the Gaza strip, Palestine. Front. Endocrinol. 8 (100), 1–9.
Eltom, M. A., Babiker Mohamed, A. H., Elrayah-Eliadarous, H., Yassin, K., Noor, S. K., Elmadhoun, W. M., et al. (2018). Increasing prevalence of type 2 diabetes mellitus and impact of ethnicity in north Sudan. Diabetes Res. Clin. Pract. 136, 93–99.
Erah, P. O., Eroje, H. I. (2013). Prescribing of antidiabetic medicines to older diabetes type 2 patients in Lagos, Nigeria. Niger. Q. J. Hosp. Med. 23 (1), 12–16.
Eriksen, J., Gustafsson, L. L., Ateva, K., Bastholm-Rahmner, P., Ovesjo, M. L., Jirlow, M., et al. (2017). High adherence to the ‘Wise List' treatment recommendations in Stockholm: a 15-year retrospective review of a multifaceted approach promoting rational use of medicines. BMJ Open 7 (4), e014345.
Ermisch, M., Bucsics, A., Vella Bonanno, P., Arickx, F., Bybau, A., Bochenek, T., et al. (2016). Payers' views of the changes arising through the possible adoption of adaptive pathways. Front. Pharmacol. 7, 305.
Fadare, J., Olamoyegun, M., Gbadegesin, B. A. (2015). Medication adherence and direct treatment cost among diabetes patients attending a tertiary healthcare facility in Ogbomosho, Nigeria. Malawi Med. J. 27 (2), 65–70.
Fadare, J. O., Adeoti, A. O., Desalu, O. O., Enwere, O. O., Makusidi, A. M., Ogunleye, O., et al. (2016). The prescribing of generic medicines in Nigeria: knowledge, perceptions and attitudes of physicians. Expert Rev. Pharmacoecon. Out. Res. 16 (5), 639–650.
Farmer, A., Bobrow, K., Leon, N., Williams, N., Phiri, E., Namadingo, H., et al. (2019). Mobile messaging support versus usual care for people with type 2 diabetes on glycemic control: protocol for a multicenter randomized controlled trial. JMIR Res. Protoc. 8 (6), e12377.
Fasanmade, O. A., Dagogo-Jack, S. (2015). Diabetes Care in Nigeria. Ann. Glob, Health 81 (6), 821–829. doi: 10.1016/j.aogh.2015.12.012
Federal Ministry of Health, Nigeria (2016). Essential Medicines list, sixth revision. Available from URL: https://apps.who.int/medicinedocs/documents/s23528en/s23528en.pdf.
Federal Ministry of Health, SIDCAIN, World Diabetes Foundation (2017). Diabetes and NCDs in Nigeria - perspectives, challenges & the way forward, Available at URL: http://sidcain.org/download/ABUJA%20Proceedings%20Reviewed%20Nov%202017.pdf.
Fox, M. P., Pascoe, S. J., Huber, A. N., Murphy, J., Phokojoe, M., Gorgens, M., et al. (2018). Assessing the impact of the national department of health's national adherence guidelines for chronic diseases in South Africa using routinely collected data: a cluster-randomised evaluation. BMJ Open 8 (1), e019680.
Gathu, C. W., Shabani, J., Kunyiha, N., Ratansi, R. (2018). Effect of diabetes self-management education on glycaemic control among type 2 diabetic patients at a family medicine clinic in Kenya: a randomised controlled trial. Afr. J. Prim. Health Care Fam. Med. 10 (1), e1–e9. doi: 10.4102/phcfm.v10i1.1762
Glezeva, N., Gallagher, J., Ledwidge, M., O'Donoghue, J., McDonald, K., Chipolombwe, J., et al. (2015). Heart failure in sub-Saharan Africa: review of the aetiology of heart failure and the role of point-of-care biomarker diagnostics. Trop. Med. Int. Health 20 (5), 581–588.
Glover, S. J., Burgess, P. I., Cohen, D. B., Harding, S. P., Hofland, H. W., Zijlstra, E. E., et al. (2012). Prevalence of diabetic retinopathy, cataract and visual impairment in patients with diabetes in sub-Saharan Africa. Br. J. Ophthalmol. 96 (2), 156–161.
Godman, B., Shrank, W., Andersen, M., Berg, C., Bishop, I., Burkhardt, T., et al. (2010). Policies to enhance prescribing efficiency in europe: findings and future implications. Front. In Pharmacol. 1, 141. doi: 10.3389/fphar.2010.00141
Godman, B., Wettermark, B., van Woerkom, M., Fraeyman, J., Alvarez-Madrazo, S., Berg, C., et al. (2014a). Multiple policies to enhance prescribing efficiency for established medicines in Europe with a particular focus on demand-side measures: findings and future implications. Front. In Pharmacol. 5, 106.
Godman, B., Malmstrom, R. E., Diogene, E., Jayathissa, S., McTaggart, S., Cars, T., et al. (2014b). Dabigatran - a continuing exemplar case history demonstrating the need for comprehensive models to optimize the utilization of new drugs. Front. Pharmacol. 5, 109.
Godman, B., Malmstrom, R. E., Diogene, E., Gray, A., Jayathissa, S., Timoney, A., et al. (2015). Are new models needed to optimize the utilization of new medicines to sustain healthcare systems? Expert Rev. Clin. Pharmacol. 8 (1), 77–94. doi: 10.1586/17512433.2015.990380
Godman, B., Bucsics, A., Vella Bonanno, P., Oortwijn, W., Rothe, C. C., Ferrario, A., et al. (2018). Barriers for Access to New Medicines: Searching for the Balance Between Rising Costs and Limited Budgets. Front. Public Health 6, 328.
Godman, B., Haque, M., McKimm, J., Abu Bakar, M., Sneddon, J., Wale, J., et al. (2020). Ongoing strategies to improve the management of upper respiratory tract infections and reduce inappropriate antibiotic use particularly among lower and middle-income countries: findings and implications for the future. Curr. Med. Res. Opin. 36 (2), 328–327.
Gudina, E. K., Amade, S. T., Tesfamichael, F. A., Ram, R. (2011). Assessment of quality of care given to diabetic patients at Jimma University Specialized Hospital diabetes follow-up clinic, Jimma, Ethiopia. BMC Endocr. Disord. 11, 19.
Gustafsson, L. L., Wettermark, B., Godman, B., Andersen-Karlsson, E., Bergman, U., Hasselstrom, J., et al. (2011). The ‘wise list'- a comprehensive concept to select, communicate and achieve adherence to recommendations of essential drugs in ambulatory care in Stockholm. Basic Clin. Pharmacol. Toxicol. 108 (4), 224–233.
Habte, B. M., Kebede, T., Fenta, T. G., Boon, H. (2017). Barriers and facilitators to adherence to anti-diabetic medications: Ethiopian patients' perspectives. Afr. J. Prim. Health Care Fam. Med. 9 (1), e1–e9. doi: 10.4102/phcfm.v9i1.1411
Hatsu, I., Baum, M. K., Huffman, F., Bussmann, H., Dusara, P., Makhema, J., et al. (2009). Diabetes in HIV Positive Adults in Botswana: Nutritional and Demographic Characteristics. FASEB J. 23 (Supplement 1), 547.15–547.15. Available at URL: https://www.fasebj.org/doi/abs/10.1096/fasebj.23.1_supplement.547.15.
Hernandez-Villafuerte, K., Li, R., Hofman, K. J. (2016). Bibliometric trends of health economic evaluation in Sub-Saharan Africa. Global Health 12 (1), 50.
Hill, J., Peer, N., Oldenburg, B., Kengne, A. P. (2017). Roles, responsibilities and characteristics of lay community health workers involved in diabetes prevention programmes: a systematic review. PloS One 12 (12), e0189069.
Hollingworth, S., Odame, E., Winch, A. (2018). Understanding data needs for HTA in Sub-Saharan Africa – a framework and Ghana case study. Available at URL: http://www.idsihealth.org/wp-content/uploads/2018/10/Data-Sources-.pdf
Houston, T. K., Allison, J. J., Sussman, M., Horn, W., Holt, C. L., Trobaugh, J., et al. (2011). Culturally appropriate storytelling to improve blood pressure: a randomized trial. Ann. Internal Med. 154 (2), 77–84.
Igbojiaku, O. J., Harbor, O. C., Ross, A. (2013). Compliance with diabetes guidelines at a regional hospital in KwaZulu-Natal, South Africa. Afr. J. Prim. Health Care Family Med. 5 (1), 447. doi: 10.4102/phcfm.v5i1.447
Imprialos, K., Faselis, C., Boutari, C., Stavropoulos, K., Athyros, V., Karagiannis, A., et al. (2017). SGLT-2 Inhibitors and cardiovascular risk in diabetes mellitus: a comprehensive and critical review of the literature. Curr. Pharm. Des. 23 (10), 1510–1521.
International Diabetes Feceration (2019). IDF Africa members. Available at URL: https://idf.org/our-network/regions-members/africa/members/25-south-africa.html.
Issaka, A., Paradies, Y., Stevenson, C. (2018). Modifiable and emerging risk factors for type 2 diabetes in Africa: a systematic review and meta-analysis protocol. Syst. Rev. 7 (1), 139.
Jaam, M., Ibrahim, M. I. M., Kheir, N., Awaisu, A. (2017). Factors associated with medication adherence among patients with diabetes in the Middle East and North Africa region: a systematic mixed studies review. Diabetes Res. Clin. Pract. 129, 1–15.
James, P. A., Oparil, S., Carter, B. L., Cushman, W. C., Dennison-Himmelfarb, C., Handler, J., et al. (2014). evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the eighth joint national committee (JNC 8). JAMA 311 (5), 507–520.
Jingi, A. M., Nansseu, J. R., Noubiap, J. J., Bilong, Y., Ellong, A., Mvogo, C. E. (2015). Diabetes and visual impairment in sub-Saharan Africa: evidence from Cameroon. J. Diabetes Metab. Disord. 14, 21.
Joseph, P., Leong, D., McKee, M., Anand, S. S., Schwalm, J. D., Teo, K., et al. (2017). Reducing the global burden of cardiovascular disease, part 1: the epidemiology and risk factors. Circ. Res. 121 (6), 677–694.
Julius, H., Basu, D., Ricci, E., Wing, J., Basu, J. K., Pocaterra, D., et al. (2011). The burden of metabolic diseases amongst HIV positive patients on HAART attending The Johannesburg Hospital. Curr. HIV Res. 9 (4), 247–252.
Juma, K., Juma, P. A., Mohamed, S. F., Owuor, J., Wanyoike, A., Mulabi, D., et al. (2019). First Africa non-communicable disease research conference 2017: sharing evidence and identifying research priorities. J. Glob. Health 8 (2), 020301.
Kalra, S., Bahendeka, S., Sahay, R., Ghosh, S., Md, F., Orabi, A., et al. (2018). Consensus recommendations on sulfonylurea and sulfonylurea combinations in the management of type 2 diabetes mellitus - international task force. Indian J. Endocrinol. Metab. 22 (1), 132–157.
Kaplan, W. A., Ritz, L. S., Vitello, M., Wirtz, V. J. (2012). Policies to promote use of generic medicines in low and middle income countries: a review of published literature, 2000-2010. Health Policy (Amsterdam Netherlands) 106 (3), 211–224.
Karinja, M., Pillai, G., Schlienger, R., Tanner, M., Ogutu, B. (2019). Care-seeking dynamics among patients with diabetes mellitus and hypertension in selected rural settings in Kenya. Int. J. Environ. Res. Public Health 16 (11), 1–15.
Kass, F. M. (2019). Sanofi partners with diabetes Kenya, Kenya diabetes study group and the international diabetes federation. Available at URL: https://www.kassfm.co.ke/home/2019/06/27/sanofi-partners-with-diabetes-kenya-kenya-diabetes-study-group-and-the-international-diabetes-federation-to-launch-a-nationwide-diabetes-management-training-for-2000-doctors-general-practitioners/.
Kassahun, T., Gesesew, H., Mwanri, L., Eshetie, T. (2016). Diabetes related knowledge, self-care behaviours and adherence to medications among diabetic patients in Southwest Ethiopia: a cross-sectional survey. BMC Endocr. Disord. 16 (1), 28.
Kawamura, N. (2011). Counterfeit diabetes medications. Diab. Health. Available at URL: https://www.diabeteshealth.com/counterfeit-diabetes-medications/.
Khalil, S., Almobarak, A. O., Awadalla, H., Elmadhoun, W. M., Noor, S. K., Sulaiman, A. A., et al. (2017). Low levels of physical activity in Sudanese individuals with some features of metabolic syndrome: population based study. Diabetes Metab. Syndr. 11 (Suppl 2), S551–S5s4.
Kharroubi, A. T., Darwish, H. M. (2015). Diabetes mellitus: the epidemic of the century. World J. Diabetes 6 (6), 850–867.
Khogali, S. S., Ali, W. A., Mohamed, S. Y., Abdelrahim, H. E., Mirghani, A. A., Ali, R. H., et al. (2018). Knowledge, attitude and practice of Sudanese individuals with type 2 diabetes about medication used in treatment of diabetes, hypertension and dyslipidaemia: a matter of debate or matter of concern? J. Public Health Emerg, 2, 23.
Khuzwayo, L. S., Moshabela, M. (2017). The perceived role of ward-based primary healthcare outreach teams in rural KwaZulu-Natal, South Africa. Afr. J. Prim. Health Care Fam. Med. 9 (1), e1–e5. doi: 10.4102/phcfm.v9i1.1388
Kibirige, D., Atuhe, D., Sebunya, R., Mwebaze, R. (2014). Suboptimal glycaemic and blood pressure control and screening for diabetic complications in adult ambulatory diabetic patients in Uganda: a retrospective study from a developing country. J. Diabetes Metab. Disord. 13 (1), 40.
Kibirige, D., Atuhe, D., Kampiire, L., Kiggundu, D. S., Donggo, P., Nabbaale, J., et al. (2017). Access to medicines and diagnostic tests integral in the management of diabetes mellitus and cardiovascular diseases in Uganda: insights from the ACCODAD study. Int. J. Equity Health 16 (1), 154.
Kibirige, D., Lumu, W., Jones, A. G., Smeeth, L., Hattersley, A. T., Nyirenda, M. J. (2019). Understanding the manifestation of diabetes in sub Saharan Africa to inform therapeutic approaches and preventive strategies: a narrative review. Clin. Diabetes Endocrinol. 5 (1), 2.
Kingdom of Eswatini - Ministry of Health (2017). 2017 National prevention and control of non communicable diseases (NCDs), Annual Program Report.
Kriza, C., Hanass-Hancock, J., Odame, E. A., Deghaye, N., Aman, R., Wahlster, P., et al. (2014). A systematic review of health technology assessment tools in sub-Saharan Africa: methodological issues and implications. Health Res. Policy Syst. 12, 66.
Kumar, S., Samaras, K. (2018). The impact of weight gain during HIV treatment on risk of pre-diabetes, diabetes mellitus, cardiovascular disease, and mortality. Front. Endocrinol. 9 (705), 1–4.
Lewis, A. D., Hogg, R. E., Chandran, M., Musonda, L., North, L., Chakravarthy, U., et al. (2018). Prevalence of diabetic retinopathy and visual impairment in patients with diabetes mellitus in Zambia through the implementation of a mobile diabetic retinopathy screening project in the Copperbelt province: a cross-sectional study. Eye 32 (7), 1201–1208.
Li, Z., Zhao, L., Yu, L., Yang, J. (2019). Head-to-head comparison of the hypoglycemic efficacy and safety between dipeptidyl peptidase-4 inhibitors and alpha-glucosidase inhibitors in patients with type 2 diabetes mellitus: a meta-analysis of randomized controlled trials. Front. Pharmacol. 10, 777.
Libby, A. M., Fish, D. N., Hosokawa, P. W., Linnebur, S. A., Metz, K. R., Nair, K. V., et al. (2013). Patient-level medication regimen complexity across populations with chronic disease. Clin. Ther. 35 (4), 385–98.e1.
Low Wang, C. C., Hess, C. N., Hiatt, W. R., Goldfine, A. B. (2016). Clinical update: cardiovascular disease in diabetes mellitus: atherosclerotic cardiovascular disease and heart failure in type 2 diabetes mellitus - mechanisms, management, and clinical considerations. Circulation 133 (24), 2459–2502.
Mabuza, D. (2018). in: Deputy President South Africa. Presidential Health Summit, Ekurhuleni, Johannesburg, 20 October. Available from URL: https://www.gov.za/speeches/address-deputy-president-david-mabuza-19-oct-2018-0000.
Magagula, S. V. (2017). A case study of the Essential Health Care Package in Swaziland. Regional Network for Equity in Health in east and southern Africa. Discussion paper 112 MoH Swaziland, IHI and TARSC and EQUINET. Available at URL: https://www.equinetafrica.org/sites/default/files/uploads/documents/Swaziland%20EHB%20case%20study%20rep%20final2017pv.pdf.
Manne-Goehler, J., Geldsetzer, P., Agoudavi, K., Andall-Brereton, G., Aryal, K. K., Bicaba, B. W., et al. (2019). Health system performance for people with diabetes in 28 low- and middle-income countries: a cross-sectional study of nationally representative surveys. PloS Med. 16 (3), e1002751.
Manyema, M., Veerman, J. L., Chola, L., Tugendhaft, A., Labadarios, D., Hofman, K. (2015). Decreasing the burden of type 2 diabetes in South Africa: the impact of taxing sugar-sweetened beverages. PloS One 10 (11), e0143050.
Mapa-Tassou, C., Katte, J. C., Mba Maadjhou, C., Mbanya, J. C. (2019). Economic impact of diabetes in Africa. Curr. Diabetes Rep. 19 (2), 5.
Marra, L. P., Araujo, V. E., Silva, T. B., Diniz, L. M., Guerra Junior, A. A., Acurcio, F. A., et al. (2016). Clinical effectiveness and safety of analog glargine in type 1 diabetes: a systematic review and meta-analysis. Diabetes Ther.: Res. Treat Educ. Diabetes Relat. Disord. 7 (2), 241–258.
Mashalla, Y. J., Sepako, E., Setlhare, V., Chuma, M., Bulang, M., Massele, A. Y. (2016). Availability of guidelines and policy documents for enhancing performance of practitioners at the Primary Health Care (PHC) facilities in Gaborone, Tlokweng and Mogoditshane, Republic of Botswana. J. Public Health Epidemiol. 8 (8), 127–135. doi: 10.5897/JPHE2016.0812
Matsitse, T. B., Helberg, E., Meyer, J. C., Godman, B., Massele, A., Schellack, N. (2017). Compliance with the primary health care treatment guidelines and the essential medicines list in the management of sexually transmitted infections in correctional centres in South Africa: findings and implications. Expert Rev. Anti-Infect. Ther. 15 (10), 963–972.
Mbanya, J. C., Sobngwi, E. (2003). Diabetes microvascular and macrovascular disease in Africa. J. Cardiovasc. Risk 10, 97–102.
Mbanya, J. C., Motala, A. A., Sobngwi, E., Assah, F. K., Enoru, S. T. (2010). Diabetes in sub-Saharan Africa. Lancet 375, 2254–2266.
Mbanya, J. C., Assah, F. K., Saji, J., Atanga, E. N. (2014). Obesity and type 2 diabetes in Sub-Sahara Africa. Curr. Diabetes Rep. 14 (7), 501.
Mbugua, S. M., Kimani, S. T., Munyoki, G. (2017). Metabolic syndrome and its components among university students in Kenya. BMC Public Health 17 (1), 909.
Mbui, J. M., Oluka, M. N., Guantai, E. M., Sinei, K. A., Achieng, L., Baker, A., et al. (2017). Prescription patterns and adequacy of blood pressure control among adult hypertensive patients in Kenya; findings and implications. Expert Rev. Clin. Pharmacol. 10 (11), 1263–1271.
Mendenhall, E., Norris, S. A. (2015). Diabetes care among urban women in Soweto, South Africa: a qualitative study. BMC Public Health 15, 1300.
Meyer, J. C., Schellack, N., Stokes, J., Lancaster, R., Zeeman, H., Defty, D., et al. (2017). Ongoing initiatives to improve the quality and efficiency of medicine use within the public healthcare system in South Africa; a preliminary study. Front. In Pharmacol. 8, 751.
Mhlanga, B. S., Suleman, F. (2014). Price, availability and affordability of medicines. Afr. J. Prim. Health Care Fam. Med. 6 (1), E1–E6. doi: 10.4102/phcfm.v6i1.604
Ministry of Health and Social Services - Primary Health Care Directorate, Family Health Division (2017). Non-communicable diseases (NCDs) programme. Available at URL: https://www.iccp-portal.org/system/files/plans/NAMIBIA%20NATIONAL%20MULTISECTORAL%20STRATEGIC%20PLAN%20FOR%20PREVENTION%20AND%20CONTROL%20OF%20NCDs.pdf.
Ministry of Health and Social Services Namibia (2013). Nutrition Guidelines for Prevention and Non-Communicable Diet Related Diseases [Internet] (Namibia: Windhoek). Available from URL: http://www.mhss.gov.na/documents/119527/364677/Nutrition+Guidelines+for+NCDRD-namibia.pdf/13ad87b2-61da-4c2a-9883-f050e02e5bc3.
Ministry of Health and Social Services Namibia (2017). Primary health care directorate, namibia. national multisectoral strategic plan for prevention and control of non-communicable diseases (NCDs) in Namibia 2017/18 – 2021/22. Available at URL: https://www.iccp-portal.org/system/files/plans/NAMIBIA%20NATIONAL%20MULTISECTORAL%20STRATEGIC%20PLAN%20FOR%20PREVENTION%20AND%20CONTROL%20OF%20NCDs.pdf.
Ministry of Health Ghana (2012). National policy for the prevention and control of chronic non-communicable diseases in Ghana. Available at URL: https://www.iccp-portal.org/sites/default/files/plans/national_policy_for_the_prevention_and_control_of_chronic_non-communicable_diseases_in_ghana(1).pdf.
Ministry of Public Health and Sanitation Kenya (2010). Kenya national diabetes strategy 2010-2015. Available at URL: https://www.worlddiabetesfoundation.org/sites/default/files/WDF09-436%20Kenya%20National%20Diabetes%20Strategy%202010-2015%20%20-%20Complete.pdf.
Mogre, V., Abanga, Z. O., Tzelepis, F., Johnson, N. A., Paul, C. (2017). Adherence to and factors associated with self-care behaviours in type 2 diabetes patients in Ghana. BMC Endocr. Disord. 17 (1), 20.
MoH. Republic of Kenya Ministry of Health. Kenya national strategy for the prevention and control of non-communicable diseases 2015 to 2020. Available at URL: http://www.who.int/nmh/ncd-task-force/kenya-strategy-ncds-2015-2020.pdf.
Mohamed, S. F., Mwangi, M., Mutua, M. K., Kibachio, J., Hussein, A., Ndegwa, Z., et al. (2018). Prevalence and factors associated with pre-diabetes and diabetes mellitus in Kenya: results from a national survey. BMC Public Health 18 (3), 1215.
Moorkens, E., Vulto, A. G., Huys, I., Dylst, P., Godman, B., Keuerleber, S., et al. (2017). Policies for biosimilar uptake in Europe: An overview. PloS One 12 (12), e0190147.
Moosa, A., Bezuidenhout, S., Meyer, J. C., Godman, B. (2019). Knowledge regarding medicines management of type-2 diabetes among patients attending a Community Health Centre in South Africa. J. Pharm. Health Serv. Res. 10, 13–21.
Moosa, A., Bezuidenhout, S., Meyer, J. C. (2015). Knowledge of type-2 diabetes among patients attending a community health centre in Pretoria, South Africa: patient centered treatment and care. Afr. J. Phys. Health Educ. Recr. Dance 21 (Suppl 2), 241–251. Available at URL: https://journals.co.za/content/ajpherd/21/sup-2?page=3.
Morris-Paxton, A. A., Rheeder, P., Ewing, R. G., Woods, D. (2018). Detection, referral and control of diabetes and hypertension in the rural Eastern Cape Province of South Africa by community health outreach workers in the rural primary healthcare project: Health in Every Hut. Afr. J. Prim. Health Care Fam. Med. 10 (1), e1–e8. doi: 10.4102/phcfm.v10i1.1610
MRC/BHF Heart Protection (2002). Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet 360 (9326), 7–22.
Mueller, D., Tivey, D., Croce, D. (2017). Health-technology assessment: Its role in strengthening health systems in developing countries. South. Afr. J. Public Health 2 (1), 6–11.
Mufunda, E., Ernersson, A., Hjelm, K. (2018). Limited knowledge of diabetes in patients attending an outpatient diabetes clinic at a referral hospital in Zimbabwe: a cross-sectional study. Pan Afr. Med. J. 29, 144.
Mukanu, M. M., Zulu, J. M., Mweemba, C., Mutale, W. (2017). Responding to non-communicable diseases in Zambia: a policy analysis. Health Res. Policy Syst. 15 (1), 34.
Murray, C. J., Lopez, A. D. (2013). Measuring the global burden of disease. N. Engl. J. Med. 369 (5), 448–457.
Mutowo, M., Gowda, U., Mangwiro, J. C., Lorgelly, P., Owen, A., Renzaho, A. (2015). Prevalence of diabetes in Zimbabwe: a systematic review with meta-analysis. Int. J. Public Health. 60 (1), 1–11.
Mwita, J. C., Mugusi, F., Lwakatare, J., Chiwanga, F. (2012). Hypertension control and other cardiovascular risk factors among diabetic patients at Muhimbili National Hospital, Tanzania. East Afr. J. Public Health 9 (2), 70–73.
Mwita, J. C., Magafu, M., Omech, B., Tsima, B., Dewhurst, M. J., Goepamang, M., et al. (2017). Undiagnosed and diagnosed diabetes mellitus among hospitalised acute heart failure patients in Botswana. SAGE Open Med. 5, 2050312117731473.
Mwita, J. C., Francis, J. M., Omech, B., Botsile, E., Oyewo, A., Mokgwathi, M., et al. (2019). Glycaemic, blood pressure and low-density lipoprotein-cholesterol control among patients with diabetes mellitus in a specialised clinic in Botswana: a cross-sectional study. BMJ Open 9 (7), e026807.
Naidoo, P., Rambiritch, V., Butkow, N., Saman, S. (2014). Optimal utilisation of sulphonylureas in resource-constrained settings. Cardiovasc. J. Afr. 25 (2), 83–85.
Namibia Diabetes lifestyle Foundation (2019). Available at URL: https://allevents.in/org/namibia-diabetes-lifestyle-foundation/7206342#.
Napier, A. D., Nolan, J. J., Bagger, M., Hesseldal, L., Volkmann, A. M. (2017). Study protocol for the cities changing diabetes programme: a global mixed-methods approach. BMJ Open 7 (11), e015240.
Nashilongo, M. M., Singu, B., Kalemeera, F., Mubita, M., Naikaku, E., Baker, A., et al. (2017). Assessing adherence to antihypertensive therapy in primary health care in Namibia: findings and implications. Cardiovasc. Drugs Ther. 31 (5-6), 565–578.
National Department of Health South Africa (2013). Strategic plan for the prevention and control of non-communicable diseases 2013-17. Available at URL: file:///C:/Users/mail/Desktop/My%20documents/Ongoing%20papers/South%20Afica%20Moosa/ZAF_B3_NCDs_STRAT_PLAN_1_29_1_3[2].pdf.
National Department of Health South Africa (2016a). Adherence guidelines for HIV, TB and NCDs. policy and service delivery guidelines to care, adherence to treatment and retention in care. Available at URL: https://www.nacosa.org.za/wp-content/uploads/2016/11/Integrated-Adherence-Guidelines-NDOH.pdf.
National Department of Health South Africa (2016b). Standard operating procedures for minimum package of interventions to suport linkage to care, adherence and retention in care, adherence guidelines for HIV, TB and NCDs. Pretoria, South Africa. Available from: http://www.differentiatedcare.org/Portals/0/adam/Content/_YiT3_-qmECUkmkpQvZAIA/File/SOP%20A5%20booklet%2020-05-2016.pdf.
NCD Risk Factor Collaboration (NCD-RisC) – Africa Working Group (2017). Trends in obesity and diabetes across Africa from 1980 to 2014: an analysis of pooled population-based studies. Int. J. Epidemiol.
Niguse, H., Belay, G., Fisseha, G., Desale, T., Gebremedhn, G. (2019). Self-care related knowledge, attitude, practice and associated factors among patients with diabetes in Ayder Comprehensive Specialized Hospital, North Ethiopia. BMC Res. Notes 12 (1), 34.
Noor, S. K., Bushara, S. O., Sulaiman, A. A., Elmadhoun, W. M., Ahmed, M. H. (2015). Undiagnosed diabetes mellitus in rural communities in Sudan: prevalence and risk factors. East Mediterr. Health J. 21 (3), 164–170.
Nuche-Berenguer, B., Kupfer, L. E. (2018). Readiness of sub-Saharan Africa healthcare systems for the new pandemic, diabetes: a systematic review. J. Diabetes Res. 2018, 9262395. doi: 10.1155/2018/9262395
Nzwili, F. (2018). Health policy watch - Kenya to launch universal health coverage pilot of free healthcare. Available at URL: https://www.healthpolicy-watch.org/kenya-to-launch-universal-health-coverage-pilot-of-free-healthcare/.
Ofori-Asenso, R., Agyeman, A. A. (2016). Irrational use of medicines—a summary of key concepts. Pharmacy 4, 35.
Ofori-Asenso, R., Agyeman, A. A., Laar, A., Boateng, D. (2016). Overweight and obesity epidemic in Ghana-a systematic review and meta-analysis. BMC Public Health 16 (1), 1239.
Ogbera, A. O., Ekpebegh, C. (2014). Diabetes mellitus in Nigeria: the past, present and future. World J. Diabetes 5 (6), 905–911.
Okoronkwo, I. L., Ekpemiro, J. N., Onwujekwe, O. E., Nwaneri, A. C., Iheanacho, P. N. (2016). Socioeconomic inequities and payment coping mechanisms used in the treatment of type 2 diabetes mellitus in Nigeria. Niger. J. Clin. Pract. 19 (1), 104–109.
Ong, S. E., Koh, J. J. K., Toh, S. E. S., Chia, K. S., Balabanova, D., McKee, M., et al. (2018). Assessing the influence of health systems on Type 2 Diabetes Mellitus awareness, treatment, adherence, and control: a systematic review. PloS One 13 (3), e0195086.
Onyango, E. M., Onyango, B. M. (2018). The rise of noncommunicable diseases in Kenya: an examination of the time trends and contribution of the changes in diet and physical inactivity. J. Epidemiol. Global Health 8 (1-2), 1–7.
Opoku, D., Busse, R., Quentin, W. (2019). Achieving sustainability and scale-up of mobile health noncommunicable disease interventions in sub-Saharan Africa: views of policy makers in Ghana. JMIR Mhealth Uhealth 7 (5), e11497.
Osei-Yeboah, J., Owiredu, W., Norgbe, G., Obirikorang, C., Lokpo, S., Ashigbi, E., et al. (2019). Physical activity pattern and its association with glycaemic and blood pressure control among people living with diabetes (PLWD) in the Ho municipality, Ghana. Ethiop. J. Health Sci. 29 (1), 819–830. doi: 10.4314/ejhs.v29i1.3
Ovbiagele, B. (2015). Tackling the growing diabetes burden in Sub-Saharan Africa: a framework for enhancing outcomes in stroke patients. J. Neurol. Sci. 348 (1-2), 136–141.
Owiredu, W. K. B. A., Adamu, M. S., Amidu, N., Woode, E., Bam, V., Plange-Rhule, J., et al. (2008). Obesity and cardiovascular risk factors in a pentecostal population in Kumasi-Ghana. J. Med. Sci. 8, 682–690.
Owolabi, E. O., Goon, D. T. (2019). The use of text messaging for improving adherence to anti-diabetic regimen and glycaemic control in low-resource settings of South Africa: a study protocol for a randomised controlled trial. Contemp. Clin. Trials Commun. 15, 100418.
Owolabi, M. O., Yaria, J. O., Daivadanam, M., Makanjuola, A. I., Parker, G., Oldenburg, B., et al. (2018). Gaps in guidelines for the management of diabetes in low- and middle-income versus high-income countries-a systematic review. Diabetes Care 41 (5), 1097–1105.
Pastakia, S. D., Ali, S. M., Kamano, J. H., Akwanalo, C. O., Ndege, S. K., Buckwalter, V. L., et al. (2013). Screening for diabetes and hypertension in a rural low income setting in western Kenya utilizing home-based and community-based strategies. Global Health 9, 21.
Pastakia, S. D., Cheng, S. Y., Kirui, N. K., Kamano, J. H. (2015). Dynamics, Impact, and Feasibility of self-monitoring of blood glucose in the rural, resource-constrained setting of western kenya. Clin. Diabetes: A Publ. Am. Diabetes Assoc. 33 (3), 136–143.
Pastakia, S. D., Pekny, C. R., Manyara, S. M., Fischer, L. (2017). Diabetes in sub-Saharan Africa - from policy to practice to progress: targeting the existing gaps for future care for diabetes. Diabetes Metab. Syndr. Obes. 10, 247–263.
Peer, N., Kengne, A. P., Motala, A. A., Mbanya, J. C. (2014). Diabetes in the Africa region: an update. Diabetes Res. Clin. Pract. 103 (2), 197–205.
Pheiffer, C., Pillay-van Wyk, V., Joubert, J. D., Levitt, N., Nglazi, M. D., Bradshaw, D. (2018). The prevalence of type 2 diabetes in South Africa: a systematic review protocol. BMJ Open 8 (7), e021029–e.
Piloya-Ware, T., Sunni, M., Ogie, G. D., Moran, A. (2016). Childhood diabetes in Africa. Curr. Opin. Endocrin. Diab. Obes. 23 (4), 306–311.
Pinchevsky, Y., Butkow, N., Chirwa, T., Raal, F. J. (2015). Glycaemic, blood pressure and cholesterol control in 25 629 diabetics. Cardiovasc. J. Afr. 26 (4), 188–192.
Rampamba, E. M., Meyer, J. C., Helberg, E., Godman, B. (2017). Knowledge of hypertension and its management among hypertensive patients on chronic medicines at primary health care public sector facilities in South Africa; findings and implications. Expert Rev. Cardiovasc. Ther. 15 (8), 639–647.
Rampamba, E., Meyer, J. C., Helberg, E. A., Godman, B. (2019). Empowering hypertensive patients on chronic medicines at primary health care facilities in South Africa with knowledge to improve disease management. J. Res. In Pharm. Pract. 8 (4), 208–213.
Rankgoane-Pono, G., Tshikuka, J. G., Magafu, M. G. M. D., Masupe, T., Molefi, M., Hamda, S. G., et al. (2018). Incidence of diabetes mellitus-related comorbidities among patients attending two major HIV clinics in Botswana: a 12-year retrospective cohort study. BMC Res. Notes 11 (1), 90.
Rasmussen, B., Sweeny, K., Sheehan, P. (2016). HEALTH AND THE ECONOMY - The Impact of Wellness on Workforce Productivity in Global Markets. A Report to the U.S. Chamber of Commerce’s Global Initiative on Health and Economy. Available at URL: https://www.uschamber.com/sites/default/files/documents/files/global_initiative_on_health_and_the_economy_-_report.pdf.
Renzaho, A. M. N. (2015). The post-2015 development agenda for diabetes in sub-Saharan Africa: challenges and future directions. Global Health Action 8, 27600.
Republic of Kenya ministry of health and sanitation (2010). Kenya National Diabetes Educators Manual. Available at URL: https://www.worlddiabetesfoundation.org/sites/default/files/Kenya%20National%20Diabetes%20Educators%20Manual.pdf.
Republic of South Africa (2019). National health insurance bill. B11-2019. Available from URL: https://www.gov.za/documents/national-health-insurance-bill-b-11-2019-6-aug-2019-0000.
Rockers, P. C., Laing, R. O., Ashigbie, P. G., Onyango, M. A., Mukiira, C. K., Wirtz, V. J. (2019). Effect of novartis access on availability and price of non-communicable disease medicines in Kenya: a cluster-randomised controlled trial. Lancet Global Health 7 (4), e492–e502.
Roth, G. A., Johnson, C., Abajobir, A., Abd-Allah, F., Abera, S. F., Abyu, G., et al. (2017). Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J. Am. Coll. Cardiol. 70 (1), 1–25.
Rwegerera, G. M., Moshomo, T., Gaenamong, M., Oyewo, T. A., Gollakota, S., Rivera, Y. P., et al. (2018). Health-related quality of life and associated factors among patients with diabetes mellitus in Botswana. Alex. J. Med. 54 (2), 111–118.
Rwegerera, G. M., Masaka, A., Pina-Rivera, Y., Moshomo, T., Gaenamong, M., Godman, B., et al. (2019). Determinants of glycemic control among diabetes mellitus patients in a tertiary clinic in Gaborone, Botswana: findings and implications. Hosp. Pract. (1995) 47 (1), 34–41.
Sackey, S. O. (1993). Draft programme document: non-communicable diseases control programme (Accra: MOH Ghana;).
Saghir, J., Santoro, J. (2018). Urbanization in sub-Saharan Africa - meeting challenges by bridging stakeholders. Available at URL: https://csis-prod.s3.amazonaws.com/s3fs-public/publication/180411_Saghir_UrbanizationAfrica_Web.pdf.
Saleem, Z., Godman, B., Hassali, M. A., Hashmi, F. K., Azhar, F., Rehman, I. U. (2019). Point prevalence surveys of health-care-associated infections: a systematic review. Pathog. Global Health, 1–15.
Sandoz - A Novartis Division (2015). Kenya is first country to launch “Novartis Access”, expanding affordable treatment options against chronic diseases. Available at URL: https://www.sandoz.com/news/media-releases/kenya-first-country-launch-novartis-access-expanding-affordable-treatment.
Sapkota, S., Brien, J.-A. E., Greenfield, J. R., Aslani, P. (2015). A systematic review of interventions addressing adherence to anti-diabetic medications in patients with type 2 diabetes–components of interventions. PloS One 10 (6), e0128581–e.
Sarfo, F. S., Mobula, L. M., Plange-Rhule, J., Ansong, D., Ofori-Adjei, D. (2018). Incident stroke among Ghanaians with hypertension and diabetes: a multicenter, prospective cohort study. J. Neurol. Sci. 395, 17–24.
Segafredo, G., Kapur, A., Robbiati, C., Joseph, N., de Sousa, J. R., Putoto, G., et al. (2019). Integrating TB and non-communicable diseases services: Pilot experience of screening for diabetes and hypertension in patients with Tuberculosis in Luanda, Angola. PloS One 14 (7), e0218052.
SEMDSA Type 2 Diabetes Guidelines Expert Committee (2017). SEMDSA 2017 guidelines for the management of type 2 diabetes mellitus. J. Endocr. Metab. Diabetes S. Afr. 22 (1 Suppl 1), S1–S196.
Shannon, G. D., Haghparast-Bidgoli, H., Chelagat, W., Kibachio, J., Skordis-Worrall, J. (2019). Innovating to increase access to diabetes care in Kenya: an evaluation of Novo Nordisk's base of the pyramid project. Glob. Health Action 12 (1), 1605704.
Shen, J., Kondal, D., Rubinstein, A., Irazola, V., Gutierrez, L., Miranda, J. J., et al. (2016). A multiethnic study of pre-diabetes and diabetes in LMIC. Global Heart 11 (1), 61–70.
Sobngwi, E., Mauvais-Jarvis, F., Vexiau, P., Mbanya, J. C., Gautier, J. F. (2002). Diabetes in Africans, part 2: ketosis prone atypical diabetes mellitus. Diabetes Metab. 28, 5–12.
Sobngwi, E., Ndour-Mbaye, M., Boateng, K. A., Ramaiya, K. L., Njenga, E. W., Diop, S. N., et al. (2012). Type 2 diabetes control and complications in specialised diabetes care centres of six sub-Saharan African countries: the Diabcare Africa study. Diabetes Res. Clin. Pract. 95 (1), 30–36.
South African Lancet National Commission (2019). Confronting the right to ethical and accountable quality health care in South Africa: A consensus report (Pretoria: National Department of Health). Available at URL: http://rhap.org.za/wp-content/uploads/2019/01/SA-Lancet-Report-Synopsis-South-Africa_Confronting-the-Right-to-Ethical-Accountable-Healthcare.pdf.
Southern African Health Technology Assessment Society (SAHTAS) (2019). Available at URL: http://www.htasa.org.za/.
Statistics South Africa (2016). Mortality and causes of death in South Africa, 2016: Findings from death notification. Available at URL: http://www.statssa.gov.za/publications/P03093/P030932016.pdf.
Stephani, V., Opoku, D., Beran, D. (2018). Self-management of diabetes in Sub-Saharan Africa: a systematic review. BMC Public Health 18 (1), 1148.
Stokes, A., Berry, K. M., McHiza, Z., Parker, W. A., Labadarios, D., Chola, L., et al. (2017). Prevalence and unmet need for diabetes care across the care continuum in a national sample of South African adults: evidence from the SANHANES-1, 2011-2012. PloS One 12 (10), e0184264.
Sun, J., Wang, Y., Zhang, X., Zhu, S., He, H. (2020). Prevalence of peripheral neuropathy in patients with diabetes: a systematic review and meta-analysis. Prim. Care Diabetes.
Thomas, M. C., Cooper, M. E., Zimmet, P. (2016). Changing epidemiology of type 2 diabetes mellitus and associated chronic kidney disease. Nat. Rev. Nephrol. 12 (2), 73–81.
Todowede, O. O., Sartorius, B. (2017). Prevalence of metabolic syndrome, discrete or comorbid diabetes and hypertension in sub-Saharan Africa among people living with HIV versus HIV-negative populations: a systematic review and meta-analysis protocol. BMJ Open 7 (7), e016602.
Tsima, B. M., Setlhare, V., Nkomazana, O. (2016). Developing the Botswana primary care guideline: an integrated, symptom-based primary care guideline for the adult patient in a resource-limited setting. J. Multidiscip. Healthc. 9, 347–354.
U.K. Prospective Diabetes Study Group (1995). U.K. prospective diabetes study 16. overview of 6 years' therapy of type II diabetes: a progressive disease. Diabetes 44 (11), 1249–1258.
UK Prospective Diabetes Study Group (1998). Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. BMJ (Clin. Res. Ed.) 317 (7160), 703–713.
Uloko, A. E., Ofoegbu, E. N., Chinenye, S., Fasanmade, O. A., Fasanmade, A. A., Ogbera, A. O., et al. (2012). Profile of Nigerians with diabetes mellitus - Diabcare Nigeria study group (2008): results of a multicenter study. Indian J. Endocrinol. Metab. 16 (4), 558–564.
Uloko, A. E., Musa, B. M., Ramalan, M. A., Gezawa, I. D., Puepet, F. H., Uloko, A. T., et al. (2018). Prevalence and risk factors for diabetes mellitus in Nigeria: a systematic review and meta-analysis. Diabetes Ther.: Res. Treat Educ. Diabetes Relat. Disord. 9 (3), 1307–1316.
Vella Bonanno, P., Bucsics, A., Simoens, S., Martin, A. P., Oortwijn, W., Gulbinovic, J., et al. (2019). Proposal for a regulation on health technology assessment in Europe - opinions of policy makers, payers and academics from the field of HTA. Expert Rev. Pharmacoecon. Out. Res. 19 (3), 251–261.
Venter, W. D. F., Moorhouse, M., Sokhela, S., Fairlie, L., Mashabane, N., Masenya, M., et al. (2019). Dolutegravir plus two different prodrugs of tenofovir to treat HIV. New Engl. J. Med.
Waari, G., Mutai, J., Gikunju, J. (2018). Medication adherence and factors associated with poor adherence among type 2 diabetes mellitus patients on follow-up at Kenyatta National Hospital, Kenya. Pan. Afr. Med. J. 29, 82.
Waari, G., Mutai, J., Gikunju, J. (2018). Medication adherence and factors associated with poor adherence among type 2 diabetes mellitus patients on follow-up at Kenyatta National Hospital, Kenya. Pan. Afr. Med. J. 29, 82.
Wagnew, F., Eshetie, S., Kibret, G. D., Zegeye, A., Dessie, G., Mulugeta, H., et al. (2018). Diabetic nephropathy and hypertension in diabetes patients of sub-Saharan countries: a systematic review and meta-analysis. BMC Res. Notes 11 (1), 565.
Wan, E. Y. F., Fung, C. S. C., Yu, E. Y. T., Chin, W. Y., Fong, D. Y. T., Chan, A. K. C., et al. (2017). Effect of multifactorial treatment targets and relative importance of hemoglobin a1c, blood pressure, and low-density lipoprotein-cholesterol on cardiovascular diseases in chinese primary care patients with type 2 diabetes mellitus: a population-based retrospective cohort study. J. Am. Heart Assoc. 6 (8), 1–13.
Werfalli, M., Engel, M. E., Musekiwa, A., Kengne, A. P., Levitt, N. S. (2016). The prevalence of type 2 diabetes among older people in Africa: a systematic review. Lancet Diabetes Endocrinol. 4 (1), 72–84.
WHO (2016). World Health Organisation, Diabetes Fact sheet July 2016. Available at URL: http://www.who.int/mediacentre/factsheets/fs312/en/.
WHO Africa (2018). Building health: Kenya"s move to universal health coverage. Available at URL: https://www.afro.who.int/news/building-health-kenyas-move-universal-health-coverage.
WHO Swaziland (2017). The Kingdom of Swaziland dedicates November to diabetes. Available at URL: https://afro.who.int/news/kingdom-swaziland-dedicates-november-diabetes.
Wirtz, V. J., Kaplan, W. A., Kwan, G. F., Laing, R. O. (2016). Access to medications for cardiovascular diseases in low- and middle-income countries. Circulation 133 (21), 2076–2085.
Wirtz, V. J., Turpin, K., Laing, R. O., Mukiira, C. K., Rockers, P. C. (2018). Access to medicines for asthma, diabetes and hypertension in eight counties of Kenya. Trop. Med. Int. Health 23 (8), 879–885.
World Diabetes Foundation (2018). WDF16-1429 - The project seeks to improve the integrated national health care infrastructure for the prevention, diagnosis and management of diabetes and its complications in the Central and Northwest Regions of Cameroon. Available at URL: https://www.worlddiabetesfoundation.org/projects/cameroon-wdf16-1429.
World Diabetes Foundation (2018). WDF16-1433. Strengthening diabetes care in Lagos state through 35 diabetes clinics, Nigeria. Available at URL: https://www.worlddiabetesfoundation.org/projects/nigeria-wdf16-1433.
World Health Organisation (2006). Definition and diagnosis of diabetes mellitus and intermediate hyperglycemia: report of a WHO/IDF consultation. Available at URL: https://apps.who.int/iris/bitstream/handle/10665/43588/9241594934_eng.pdf;jsessionid=75A0C3B74F6572D012AB00D9F8A23D4E?sequence=1.
World Health Organisation (2016). Diabetes - Lesotho. Available at URL: https://www.who.int/diabetes/country-profiles/lso_en.pdf?ua=1.
World Health Organization (2018). Noncommunicable diseases (NCD) country profiles Botswana. Available at URL: https://www.who.int/nmh/countries/bwa_en.pdf?ua=1.
World Health Organization (2019). Model list of essential medicines, 21st list. Available at URL: https://apps.who.int/iris/bitstream/handle/10665/325771/WHO-MVP-EMP-IAU-2019.06-eng.pdf?ua=1.
Zekewos, A., Loha, E., Egeno, T., Wubshet, K., Merga, Z. (2018). Prevalence of diabetes mellitus and associated factors in southern ethiopia: a community based study. Ethiop. J. Health Sci. 28 (4), 451–460. doi: 10.4314/ejhs.v28i4.11
Zimbabwe Diabetic Association (2019). Available at URL: https://www.idf.org/our-network/regions-members/africa/members/31-zimbabwe.html?layout=details&mid=142.
Appendix 1. Prevalence rates of pre-diabetes and diabetes among a range of African countries
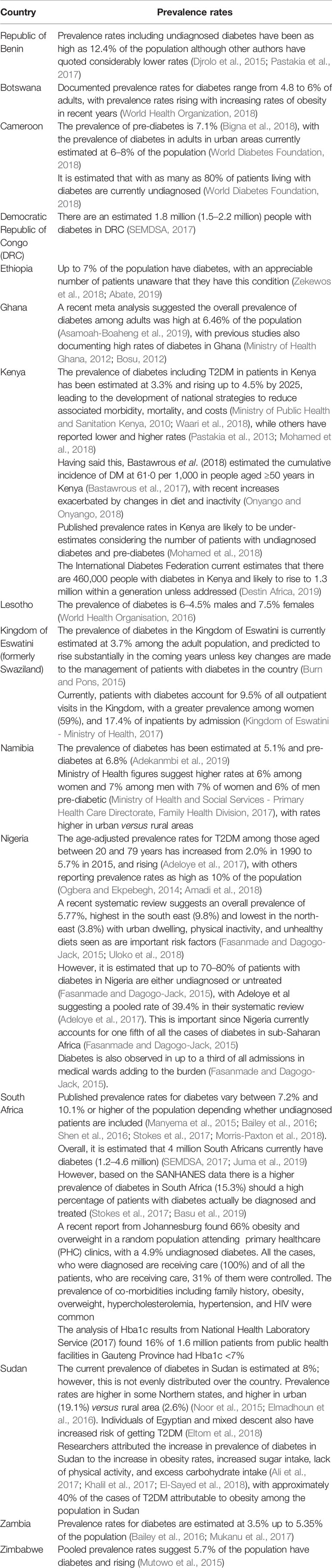
Keywords: Type 2 diabetes, Africa, national initiatives, diagnosis, medicines, adherence, patient groups
Citation: Godman B, Basu D, Pillay Y, Mwita JC, Rwegerera GM, Anand Paramadhas BD, Tiroyakgosi C, Okwen PM, Niba LL, Nonvignon J, Sefah I, Oluka M, Guantai AN, Kibuule D, Kalemeera F, Mubita M, Fadare J, Ogunleye OO, Distiller LA, Rampamba EM, Wing J, Mueller D, Alfadl A, Amu AA, Matsebula Z, Kalungia A, Zaranyika T, Masuka N, Wale J, Hill R, Kurdi A, Timoney A, Campbell S and Meyer JC (2020) Review of Ongoing Activities and Challenges to Improve the Care of Patients With Type 2 Diabetes Across Africa and the Implications for the Future. Front. Pharmacol. 11:108. doi: 10.3389/fphar.2020.00108
Received: 04 September 2019; Accepted: 28 January 2020;
Published: 20 March 2020.
Edited by:
Anne E. Sumner, National Institutes of Health (NIH), United StatesReviewed by:
Mansour Adam Mahmoud, Taibah University, Saudi ArabiaRanganath Muniyappa, National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), United States
Copyright © 2020 Godman, Basu, Pillay, Mwita, Rwegerera, Anand Paramadhas, Tiroyakgosi, Okwen, Niba, Nonvignon, Sefah, Oluka, Guantai, Kibuule, Kalemeera, Mubita, Fadare, Ogunleye, Distiller, Rampamba, Wing, Mueller, Alfadl, Amu, Matsebula, Kalungia, Zaranyika, Masuka, Wale, Hill, Kurdi, Timoney, Campbell and Meyer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Brian Godman, YnJpYW4uZ29kbWFuQHN0cmF0aC5hYy51aw==; QnJpYW4uR29kbWFuQGtpLnNl