 Ismaeel Yunusa
Ismaeel Yunusa Marie Line El Helou
Marie Line El Helou Saud Alsahali
Saud Alsahali- 1School of Pharmacy, Massachusetts College of Pharmacy and Health Sciences, Boston, MA, United States
- 2School of Pharmacy, Lebanese American University, Byblos, Lebanon
- 3Unaiz College of Pharmacy, Qassim University, Qassim, Saudi Arabia
Dementia affects more than 40 million people worldwide. When it is accompanied by psychosis, symptom management is especially challenging. Although no drug has been approved by the US Food and Drug Administration (FDA) for psychosis in patients with dementia, atypical antipsychotics are used off-label in severe cases in patients who do not respond to non-pharmacological interventions. However, antipsychotic use in elderly patients with dementia-related psychosis (DRP) is associated with adverse reactions including motor function disorders, cognitive impairment, cerebrovascular events, and increased risk of death. In 2017, the US FDA granted breakthrough therapy designation to the new antipsychotic pimavanserin for the treatment of DRP. Topline result of the pivotal phase III HARMONY (NCT03325556) trial suggests that pimavanserin reduces the relapse of psychosis by 2.8-folds compared to placebo. This favorable result may open path for the potential approval of pimavanserin in DRP. In this review, we discuss the pharmacological activity, clinical efficacy and safety of pimavanserin as a novel atypical antipsychotic with potentials to address the unmet needs of older adults with DRP.
Background
It is estimated that 44 million people worldwide are currently living with dementia and this number is expected to triple by 2050 (Alzheimers.net, 2013). In addition to cognitive impairment, dementia is often accompanied by behavioral and psychological symptoms. Indeed, up to 90% of people with dementia experience behavioral and psychotic symptoms of dementia (BPSD) throughout the course of the disease (Selbæk et al., 2013). These symptoms include depression, psychosis, aggression, and agitation and they can lead to complications that further reduce the patient’s quality of life. Different subtypes of dementia diseases including Alzheimer’s disease (AD), dementia with Lewy bodies, frontotemporal dementia, and vascular dementia exhibit dementia-related psychosis (DRP). These psychotic symptoms present as delusions, with a reported prevalence ranging between 30%–40% and hallucinations, with a prevalence of 5%–20% (Flint, 1991; Sultzer, 2004). According to Reeves and colleagues (2012), DRP is a “logical attempt to understand the environment” in the context of a degraded cognitive integrity. Psychosis aggravates the clinical course of dementia and creates profound stress on caregivers and family members, which may lead to placing patients in long-term care facilities earlier in the course of the illness (Koppel and Greenwald, 2014).
To date, no drug has received approval by the US Food and Drug Administration (FDA) for treating DRP. Given the severity and high prevalence of BPSD and the lack of FDA-approved pharmacological treatment, many classes of drugs (antipsychotics, antidepressants, and anticonvulsants) have been utilized off-label for the management of BPSD. The most widely used and most effective drugs for this purpose are the atypical antipsychotics, including aripiprazole, risperidone, olanzapine, and quetiapine (Alzheimer’s Association, 2013.). However, antipsychotic use in elderly patients with DRP is associated with adverse reactions that include motor function disorder, cognitive impairment, cerebrovascular events (stroke and transient ischemic attack), and increased risk of death (Schneider et al., 2006; Huybrechts et al., 2012; Zhai et al., 2016). In this review, we focus on pimavanserin, a novel antipsychotic that was granted the FDA’s breakthrough therapy designation for the treatment of DRP in 2017 (Tan, 2019). This designation indicates the FDA will fast-track its review and development.
Pharmacology of Pimavanserin
Pimavanserin is the active pharmaceutical ingredient of Nuplazid®, which was approved by the FDA in 2016 for the treatment of hallucinations and delusions associated with psychosis in patients suffering from Parkinson’s disease. Its exact mechanism of action is unclear. The drug exhibits a combination of inverse agonist and antagonist activity at the serotonin 2A receptors (5-HT2A) and, to a lesser extent, at the 5-HT2C receptors in the central nervous system, which is believed to contribute to its antipsychotic activity. Pimavanserin is absorbed in the gastrointestinal tract and is highly bound to plasma protein (approximately 95%). Following the administration of a single 34-mg dose of pimavanserin, the time to maximum plasma concentration is six hours, the half-life is approximately 57 h and the mean (standard deviation, SD) apparent volume of distribution is 2,173 (307) L. Pimavanserin is metabolized in the liver predominantly by cytochrome P450 (CYP3A4 and CYP3A5) and does not cause significant CYP3A4 inhibition or induction. It has a major active N-desmethylated metabolite AC-279, whose half-life is 200 h (Paspe Cruz, 2017).
Pimavanserin is the first atypical antipsychotic that does not induce clinically significant antagonism of adrenergic, dopaminergic, histaminergic, or muscarinic receptors (see Table 1 for comparison with other atypical antipsychotics) (Paspe Cruz, 2017). This may explain the absence of movement-related disorders seen with other antipsychotics. The most frequent adverse reactions are peripheral edema (7%), nausea (7%), and state of confusion (6%) (FDA, 2018).
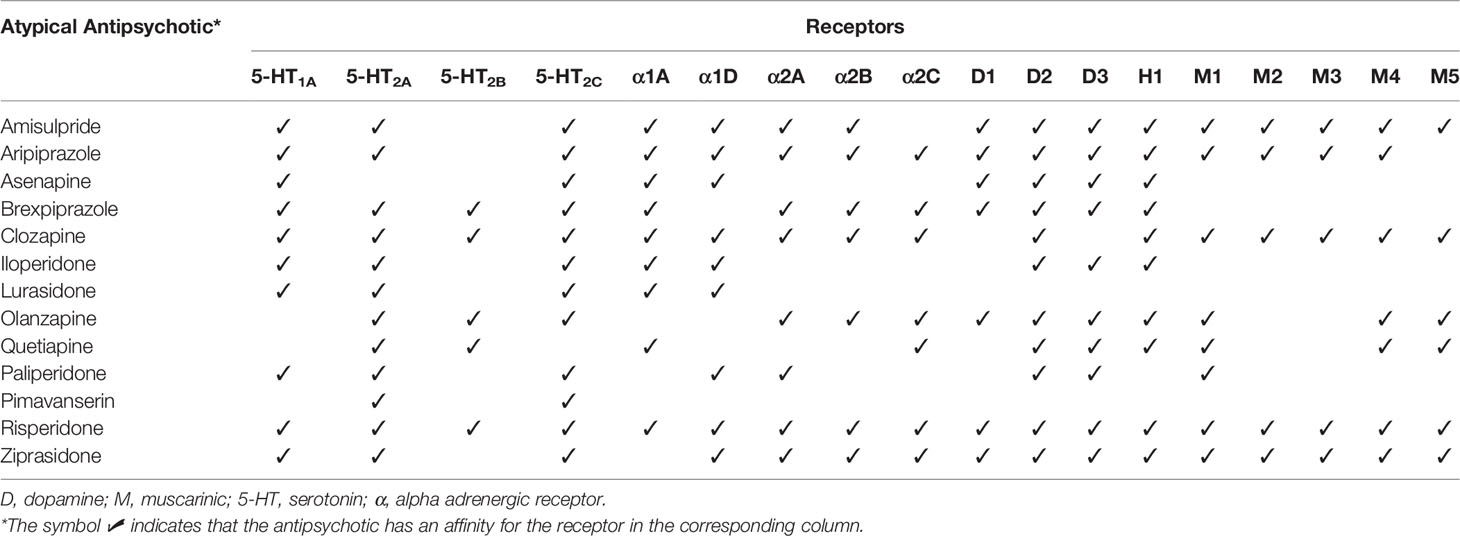
Table 1 Receptor selectivity of pimavanserin and other atypical antipsychotics (Nasrallah, 2008; Hacksell et al., 2014; Mauri et al., 2014; Kusumi et al., 2015; Siafis et al., 2018).
Approval for Treating Parkinson’s Disease-Related Psychosis
The efficacy of pimavanserin for treating hallucinations and delusions associated with Parkinson’s disease was demonstrated in a 6-week, randomized, placebo-controlled, parallel-group phase III study by Cummings et al. The study randomized 199 patients (mean age 72 years) with Parkinson’s disease psychosis (hallucinations and/or delusions) to receive either pimavanserin 34 mg daily or placebo. The outcome was assessed with the Parkinson’s disease-adapted scale for assessment of positive symptoms (SAPS-PD). The group receiving pimavanserin showed a significantly improved SAPS-PD score at week 6 compared to the group receiving placebo. Indeed, a 5.79 point improvement [least square (LS) mean change] in the SAPS-PD score was observed with pimavanserin compared to a 2.73-point improvement for placebo (treatment difference of 3.06 points; p = 0.001). Overall, pimavanserin was well tolerated with no significant safety concerns or worsening of motor function (Cummings et al., 2014).
A post-hoc subgroup analysis of the results revealed a significant improvement in the SAPS-PD score of PD patients with cognitive impairment (n = 50) treated with pimavanserin compared to those on placebo, with no adverse effect on cognition. Moreover, pimavanserin led to better improvement in the SAPS-PD score in the subgroup of patients with cognitive impairment (treatment difference of 5.71 points; p = 0.002) than in the overall PD population (treatment difference of 3.06 points; p = 0.001), suggesting a more robust effect in the former group than the latter (Cummings et al., 2018). Based on this finding, it was extrapolated that pimavanserin may also be a potential treatment for dementia with Lewy bodies, which is also characterized by movement disorders and is associated with psychotic symptoms in 75% of patients (Lyketsos et al., 2002). Despite data from this subgroup analysis suggesting a better safety profile, pimavanserin, like other antipsychotics, carries a black box warning stating that “elderly patients with DRP treated with antipsychotic drugs are at an increased risk of death” (FDA, 2018).
Clinical Evidence From Trials In Dementia-Related Psychosis
A phase II randomized, double-blind, placebo-controlled, single-center clinical trial assessed the safety and efficacy of pimavanserin 34 mg daily versus placebo for the treatment of AD psychosis. Completed in 2016, the study included 181 participants (mean age 86 years) from multiple affiliated nursing-home sites across the United Kingdom (UK). The primary endpoint was the mean change in the Neuropsychiatric Inventory-Nursing Home version (NPI-NH) psychosis score, from baseline to week 6. At week 6, patients in the pimavanserin group showed significant improvement in the NPI-NH psychosis score compared to patients in the placebo group. Mean change in the NPI-NH psychosis score from baseline at week 6 was −3.76 points [standard error (SE), 0.65] for pimavanserin and −1.93 points (SE, 0.63) for placebo [mean difference −1.84 (95% CI –3.64 to −0.04); p = 0.045] (Ballard et al., 2018). However, in this trial, a significant difference in efficacy between pimavanserin and placebo was not seen at 12 weeks of treatment (Table 2). Although agitation was higher in patients receiving pimavanserin (21%) than in those receiving placebo (14%), the overall adverse event profile was similar in the two groups. No detrimental effect was observed on cognition or motor function in either group (Ballard et al., 2018).
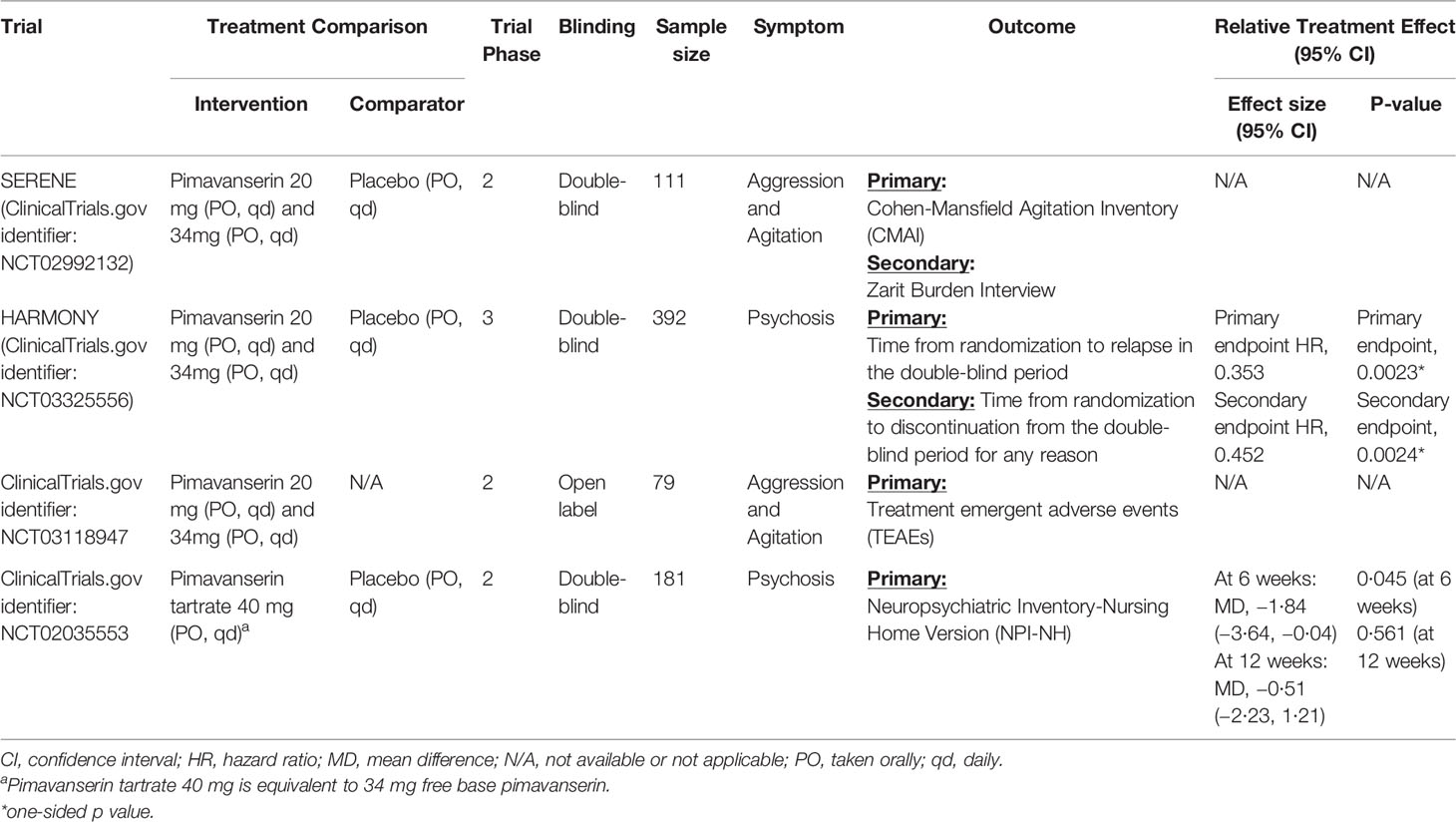
Table 2 Summary of completed and ongoing clinical trials for pimavanserin in dementia-related psychosis.
Two other trials are currently evaluating pimavanserin in patients with dementia: the SERENE trial (ClinicalTrials.gov number: NCT02992132) and the HARMONY trial (ClinicalTrials.gov number: NCT03325556). The SERENE trial is a double-blind, placebo-controlled phase II trial examining the safety and efficacy of pimavanserin to treat agitation and aggression in people with AD. Patients are given either 34 or 20 mg of daily pimavanserin, or a placebo for three months. Patients who successfully complete the SERENE trial are eligible to take part in an open-label extension study (ClinicalTrials.gov number: NCT03118947) that assesses the safety and tolerability of 34 or 20 mg of pimavanserin taken for a year. The SERENE trial was completed in February 2018, and its extension was completed in February 2019 (ClinicalTrials.gov, 2019a; ClinicalTrials.gov, 2019b; Tan, 2019). To our knowledge, no data from this phase II clinical trial and its extension have been published to date.
The HARMONY trial is a phase III, double-blind, placebo-controlled study evaluating the efficacy of pimavanserin versus placebo in preventing a relapse of psychotic symptoms in patients with DRP who are stabilized after 12 weeks of open label pimavanserin treatment. Unlike the phase II trials that were restricted to patients with AD, this phase III trial also includes patients with Lewy body dementia, Parkinson’s disease dementia, frontotemporal dementia, and vascular dementia. During an initial open-label, 3-month period, all patients receive 34 mg of pimavanserin daily. After this period, patients are randomized to continue receiving 34 mg of pimavanserin daily, to switch to 20 mg daily, or to be given a placebo. HARMONY started in September 2017, and recent topline results suggested that pimavanserin reduced the risk of relapse of psychosis by 2.8-fold compared to placebo in patients with DRP (see Table 2) (Acadia Pharmaceuticals, 2019; Tan, 2019).
Potential Off-Label Use
An International Delphi consensus panel of 11 experts in the management of BPSD chose risperidone as the recommended pharmacological option for this indication, and regarding future treatments, the greatest priority was placed on pimavanserin (Kales et al., 2019). Given its approval for Parkinson’s-related psychosis, its selection by the consensus panel for future treatments, and the promising published results from the phase II and III clinical trials indicating pimavanserin’s favorable efficacy/safety profile over placebo than the current pharmacological options, pimavanserin is likely to be used off-label for the treatment of DRP pending its potential approval. However, to our knowledge, there is no published data on the status of its likely off-label use in clinical practice.
Conclusion
Preliminary clinical evidence suggest that pimavanserin may have a positive benefit-risk profile for the short-term treatment of DRP, which contributed to it’s designation by the FDA as a breakthrough therapy for this indication. Results from the phase III HARMONY trial will open the path for the FDA’s priority review and a potential approval of pimavanserin for DRP.
Author Contributions
IY, ME, and SA determined the outline, reviewed the literature, wrote, verified, and approved the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Acadia Pharmaceuticals (2019). ACADIA pharmaceuticals presents positive top-line results from pivotal phase 3 harmony trial of pimavanserin in patients with dementia-related psychosis at 12th clinical trials on Alzheimer’s Disease (CTAD) Meeting. Accessed on 20 Dec 2019. https://ir.acadia-pharm.com/news-releases/news-release-details/acadia-pharmaceuticals-presents-positive-top-line-results?field_nir_news_date_value[min]=.
Alzheimer’s Association (2013). Challenging behaviors: common questions. accessed on 17 Aug 2019. https://www.alz.org/national/documents/statements_antipsychotics.pdf.
Alzheimers.net (2013). Alzheimer’s Will be a Global Epidemic by 2050. Accessed on 17 Aug 2019. https://www.alzheimers.net/2013-12-11/alzheimers-global-epidemic-by-2050.
Ballard, C., Banister, C., Khan, Z., Cummings, J., Demos, G., Coate, B., et al. (2018). Evaluation of the safety, tolerability, and efficacy of pimavanserin versus placebo in patients with Alzheimer’s disease psychosis: a phase 2, randomised, placebo-controlled, double-blind study. Lancet Neurol. 17, 213–222. doi: 10.1016/S1474-4422(18)30039-5
ClinicalTrials.gov (2019a). A 52-week open-label extension study of pimavanserin for the treatment of agitation and aggression in subjects with Alzheimer’s Disease. https://clinicaltrials.gov/ct2/show/NCT03118947?term=Pimavanserin&cond=Alzheimer+Disease&rank=2 Accessed on 18 Aug 2019.
ClinicalTrials.gov (2019b). Study to examine the safety and efficacy of pimavanserin for the treatment of agitation and aggression in alzheimer’s disease (SERENE). https://clinicaltrials.gov/ct2/show/NCT02992132?term=Pimavanserin&cond=Alzheimer+Disease&rank=3#studydescAccessed on 18 Aug 2019.
Cummings, J., Isaacson, S., Mills, R., Williams, H., Chi-Burris, K., Corbett, A., et al. (2014). Pimavanserin for patients with Parkinson’s disease psychosis: a randomised, placebo-controlled phase 3 trial. Lancet. 383 (9916), 533–540. doi: 10.1016/S0140-6736(13)62106-6
Cummings, J., Ballard, C., Tariot, P., Owen, R., Foff, E., Youakim, J., et al. (2018). Pimavanserin: potential treatment for dementia-related psychosis. J. Prev. Alzheimers Dis. 5 (4), 253–258. doi: 10.14283/jpad.2018.29
Flint, A. J. (1991). Delusions in dementia: a review. J. Neuropsychiatry Clin. Neurosci. 3 (2), 121–130. doi: 10.1176/jnp.3.2.121
Food and Drug Administration (FDA) (2018). nuplazid label. Accessed on August 20, 2019 https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/207318s002s004lbl.pdf.
Hacksell, U., Burstein, E. S., McFarland, K., Mills, R. G., Williams, H. (2014). On the discovery and development of pimavanserin: a novel drug candidate for Parkinson’s psychosis. Neurochem. Res. 39 (10), 2008–2017. doi: 10.1007/s11064-014-1293-3
Huybrechts, K. F., Gerhard, T., Crystal, S., Olfson, M., Avorn, J., Levin, R., et al. (2012). Differential risk of death in older residents in nursing homes prescribed specific antipsychotic drugs: population-based cohort study. BMJ. 344, e977. doi: 10.1136/bmj.e977
Kales, H., Lyketsos, C., Miller, E., Ballard, C. (2019). Management of behavioral and psychological symptoms in people with Alzheimer’s disease: An international Delphi consensus. Int. Psychogeriatric. 31 (1), 83–90. doi: 10.1017/S1041610218000534
Koppel, J., Greenwald, B. S. (2014). Optimal treatment of Alzheimer’s disease psychosis: challenges and solutions. Neuropsychiatr. Dis. Treat. 10, 2253–2262. doi: 10.2147/NDT.S60837
Kusumi, I., Boku, S., Takahashi, Y. (2015). Psychopharmacology of atypical antipsychotic drugs: from the receptor binding profile to neuroprotection and neurogenesis. Psychiatry Clin. Neurosci. 69 (5), 243–258. doi: 10.1111/pcn.12242
Lyketsos, C. G., Lopez, O., Jones, B., Fitzpatrick, A. L., Breitner, J., DeKosky, S. (2002). Prevalence of neuropsychiatric symptoms in dementia and mild cognitive impairment: results from the cardiovascular health study. JAMA. 288, 1475–1483. doi: 10.1001/jama.288.12.1475
Mauri, M. C., Paletta, S., Maffini, M., Colasanti, A., Dragogna, F., Di Pace, C., et al. (2014). Clinical pharmacology of atypical antipsychotics: an update. EXCLI J. 13, 1163–1191.
Nasrallah, H. A. (2008). Atypical antipsychotic-induced metabolic side effects: insights from receptor-binding profiles. Mol. Psychiatry 13 (1), 27–35. doi: 10.1038/sj.mp.4002066
Paspe Cruz, M. (2017). Pimavanserin (Nuplazid): a treatment for hallucinations and delusions associated with Parkinson’s Disease. P&T 42 (6), 368–371.
Reeves, S. J., Gould, R. L., Powell, J. F., Howard, R. J. (2012). Origins of delusions in Alzheimer’s disease. Neurosci. Biobehav. Rev. 36 (10), 2274–2287. doi: 10.1016/j.neubiorev.2012.08.001
Schneider, L. S., Tariot, P. N., Dagerman, K. S., Davis, S. M., Hsiao, J. K., Ismail, M. S., et al. (2006). Effectiveness of atypical antipsychotic drugs in patients with Alzheimer’s disease. N Engl. J. Med. 355, 1525–1538. doi: 10.1056/NEJMoa061240
Selbæk, G., Engedal, K., Bergh, S. (2013). The prevalence and course of neuropsychiatric symptoms in nursing home patients with dementia: a systematic review. J. Am. Med. Dir Assoc. 14 (3), 161–169. doi: 10.1016/j.jamda.2012.09.027
Siafis, S., Tzachanis, D., Samara, M., Papazisis, G. (2018). Antipsychotic drugs: from receptor-binding profiles to metabolic side effects. Curr. Neuropharmacol. 16 (8), 1210–1223. doi: 10.2174/1570159✓15666170630163616
Sultzer, D. L. (2004). Psychosis and antipsychotic medications in Alzheimer’s disease: clinical management and research perspectives. Dement. Geriatr. Cognit. Disord. 17 (1–2), 78–90. doi: 10.1159/000074279
Tan, V. (2019). Pimavanserin. https://alzheimersnewstoday.com/pimavanserin/ Accessed on 18 August 2019.
Keywords: pimavanserin, dementia, behavioral and psychological symptoms of dementia, dementia-related psychosis, neuropsychiatric symptoms of dementia, Alzheimer's disease, Antipsychotic, Atypical antipsychotic
Citation: Yunusa I, El Helou ML and Alsahali S (2020) Pimavanserin: A Novel Antipsychotic With Potentials to Address an Unmet Need of Older Adults With Dementia-Related Psychosis. Front. Pharmacol. 11:87. doi: 10.3389/fphar.2020.00087
Received: 28 August 2019; Accepted: 27 January 2020;
Published: 26 February 2020.
Edited by:
Lydia Gimenez-Llort, Autonomous University of Barcelona, SpainReviewed by:
Danilo De Gregorio, McGill University, CanadaYanbo Zhang, University of Saskatchewan, Canada
Copyright © 2020 Yunusa, El Helou and Alsahali. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ismaeel Yunusa, aXNtYWVlbHJ4QGdtYWlsLmNvbQ==