 Ria Benko1*
Ria Benko1* Maria Matuz1Zoltan Juhasz2Julia Bognar3Reka Bordas1Gyongyver Soos1Edit Hajdu2Zoltan Peto4
Maria Matuz1Zoltan Juhasz2Julia Bognar3Reka Bordas1Gyongyver Soos1Edit Hajdu2Zoltan Peto4- 1Department of Clinical Pharmacy, University of Szeged, Szeged, Hungary
- 2First Department of Internal Medicine, Infectology Unit, University of Szeged, Szeged, Hungary
- 3Grove Lodge One, Norwich, United Kingdom
- 4Emergency Department, University of Szeged, Szeged, Hungary
Background: Lower urinary tract infections (LUTIs) are amongst the most common community acquired infections with frequent antibiotic prescribing.
Objectives: To assess empiric antibiotic choice in different types of lower urinary tract infections. We also aimed to identify determinants of fluoroquinolone prescribing, as well as to determine the rate of short antibiotic courses. The frequencies of executing laboratory tests and recommending analgesics/anti-inflammatory drugs were also assessed.
Methods: A prospective observational study was performed in 19 different Hungarian primary care practices. Participating general practitioners (GPs) filled out data sheets for each patient with a suspected urinary tract infection. Details of drug use were evaluated. Comparison of different LUTI groups were made by descriptive statistics and univariate analysis. Possible determinants of fluoroquinolone prescribing were assessed by logistic regression.
Results: Data sheets of 372 patients were analyzed. The majority of patients (68.82%) had acute uncomplicated cystitis. While antibiotics were prescribed for almost every patient (uncomplicated cases: 92.58%, complicated cases: 94.83%), analgesics/anti-inflammatory drugs were recommended at a rate of 7.81% in uncomplicated, and 13.79% in complicated cystitis cases. Ciprofloxacin was the most commonly prescribed antibacterial agent in both types of cystitis. Short-term antibiotic therapy was prescribed in one third of relevant cases. Logistic regression found a weak association between fluoroquinolone use and patient’s age and presence of complicating factors.
Conclusions: Many aspects of suboptimal cystitis management were identified (e.g. unnecessarily broad spectra agents, too long antibiotic courses). In this study, patient characteristics has weakly influenced fluoroquinolone prescribing. Based on these results there is considerable room for improvement in primary care antibiotic therapy of cystitis in Hungary.
Introduction
To combat antibiotic resistance by lowering selection pressure, rationalizing antibiotic use for the most frequent community infections should be the key target of any antibiotic stewardship programmes. Lower urinary tract infections (LUTIs) are among the most commonly encountered illnesses in the ambulatory care (e.g. almost half of all women will experience at least one episode of cystitis during their lifetime), with consequently high antibiotic prescribing (Bonkat et al., 2017; Tyrstrup et al., 2017; Dumpis et al., 2018).
The classification of urinary tract infections is based on the affected anatomical site, and can be further stratified into uncomplicated or complicated types based on the presence or absence of complicating factors (e.g. diabetes mellitus) (Bonkat et al., 2017; Reynard and Biers, 2019). Compared to uncomplicated LUTI, the pathogen spectrum of complicated LUTIs is much wider, and these bacteria are more likely to be resistant to antibiotics, thus their empirical treatment tends to utilize broad-spectrum antibiotics (Bonkat et al., 2017). Unfortunately, the widely used coding system of diseases (International Statistical Classification of Diseases and Related Health Problems (ICD) version 10) does not follow this classification, which limits the capabilities of database studies. Previous drug utilisation studies based on the national health care database of Hungary revealed suboptimal antibiotic use in various infections (Juhasz et al., 2013; Matuz et al., 2015). The aim of this study was to overcome the limitations of database studies by exploiting clinical data that enables correct diagnosing and further stratification of cases. Based on these exact patient-specific data we have assessed the empiric antibiotic choice in complicated and uncomplicated LUTIs. Determinants of fluoroquinolone prescribing, the use of analgesics/anti-inflammatory drugs and the frequency of laboratory urine analysis (microbiological and chemical) were also evaluated.
Methods
A prospective observational study was conducted. General practitioners (GPs) were invited and voluntarily participated, without any financial incentives. Twenty-five GPs accepted participation (response rate: 51%), and 19 GPs (i.e. 19 different primary care unit from various geographical location) contributed throughout the study. GPs were asked to fill in a data sheet for all consecutive patients who first presented with a suspected urinary tract infection. The following data were recorded: patient’s demography, drug allergy, presence of complicating factors, clinical signs, history of urinary tract infections in the previous year, performed lab tests and treatments. Doctors’ specialty and experience (number of practicing years) were derived from a public national database (National Health Registration and Training Centre).
All patients over 16 years of age were eligible for inclusion. Pregnant women, as well as cases with a suspected upper UTI (pyelonephritis), or genital or sexually transmitted infection (e.g. vaginal discharge) and cases where crucial data (e.g. prescribed/recommended therapy) were missing were excluded. Based on the recorded signs/complaints and comorbidities we classified each case as an uncomplicated or complicated lower urinary tract infection according to the guideline of the European Urological Association (Bonkat et al., 2017). The followings were considered as complicating factors: male gender, diabetes mellitus, presence of indwelling catheter/stent/tube, reconstruction of the urinary tract, recent instrumentational intervention within the urinary tract, functional/anatomical defects (e.g. obstruction, incontinence), renal failure, kidney transplant, and immunosuppression. In accordance with the widely accepted definition, we defined recurrent cystitis as a minimum of 2 infectious episodes within 6 months, or 3 infectious episodes within a year (Bonkat et al., 2017). Antibiotics were classified according to the WHO ATC (Anatomical-Therapeutic-Chemical) index (version 2019). Short-term antibiotic course was defined as prescribing a single dose of fosfomycin, a 3-day-course of fluoroquinolone, a 5-day-course of beta-lactam and 5–7 days of nitrofurantoin therapy for uncomplicated cystitis (Reynard and Biers, 2019).
Patient age, diagnostic measures and prescribed/recommended therapy was compared in complicated and uncomplicated cystitis by descriptive methods and univariate analysis (Fischer’s and Welch’s tests). Potential influencing factors of fluoroquinolone prescribing (patient-specific characteristics: age, gender, recurrent cystitis, presence of complicating factors; GP-specific factors: years of practicing, and specializations) were analyzed by logistic regression. Statistical analyses were performed with the R statistical software (version 3.5).
The study protocol was approved by the Regional Human Medical Biology Research Ethical Board of the University of Szeged, Hungary. The ethical approval did not allowed the identification and follow-up of patients, hence the therapeutic outcomes could not be evaluated.
Results
Overall, 510 data sheets were collected. A total of 138 patients were excluded (because of pregnancy, n = 11; genital/sexually transmitted infection, n = 11; suspected kidney infection, n = 74; missing data, n = 42), thus data sheets of 372 patients were analyzed. Most patients were female (n = 342, 91.94%), diagnosed with uncomplicated cystitis (n = 256, 68.82%). Recurrent cystitis was present in one fifth of patients (n = 71, 19.07%).
The average age of those diagnosed with complicated cystitis was significantly higher (64.44 ± 16.30 years vs. 48.12 ± 19.56), and recurrent cystitis was also slightly more frequent in this patient group. (Table 1).
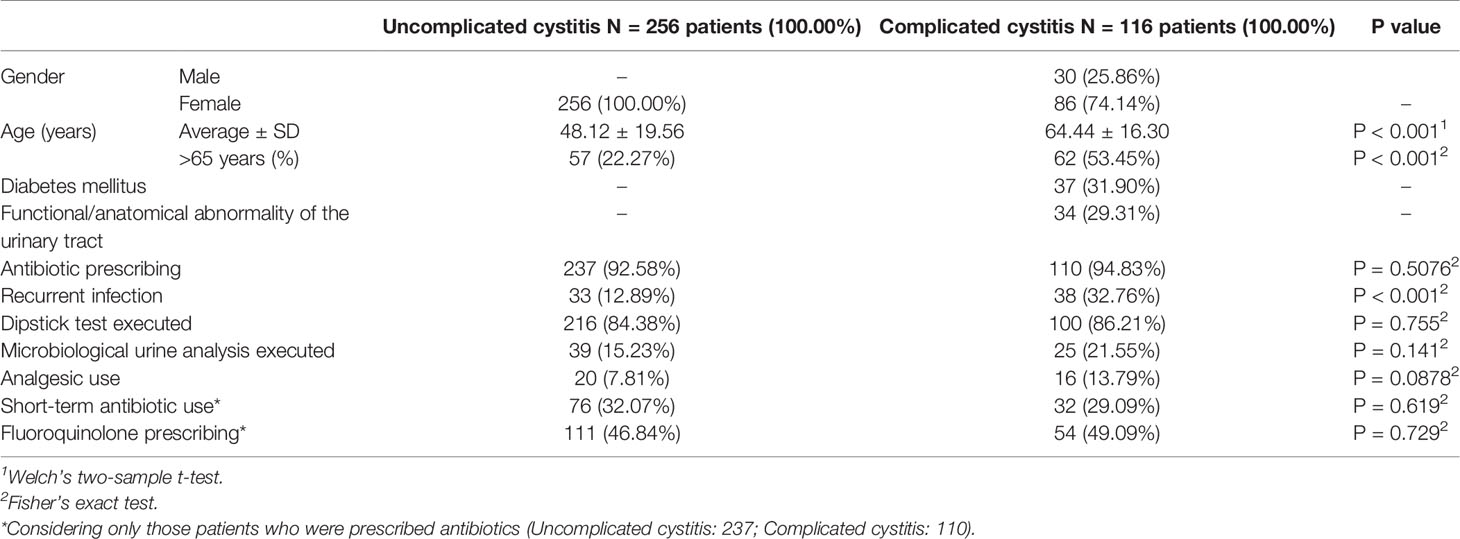
Table 1 General patient characteristics, diagnostics and therapeutics.
Diagnostic measures and details of prescribed/recommended therapies are summarized in Table 1 and Figure 1. Those with complicated cystitis had higher age and higher rate of recurrent infection (Table 1). With some exceptions, urine analysis was extensively performed (in over 85% of cases) in both cystitis types, while microbiological analysis of midstream urine was performed only in a minority of cases (15.23% in uncomplicated and 21.55% in complicated cystitis, see Table 1). Antibiotic was prescribed for 347 patients (93.28%), however, antibiotic prescription rate of individual GPs ranged between 50.00% and 100.00%. Analgesics/anti-inflammatory drugs was recommended in 1 per 10 cases, while individual GP’s recommendation rate ranged between 4.17% and 100.00%. Using non-antibiotic treatment only (analgesic/anti-inflammatory agent OR cranberry product OR herbal tea) was recommended in as few as 11 cases (2.96%).
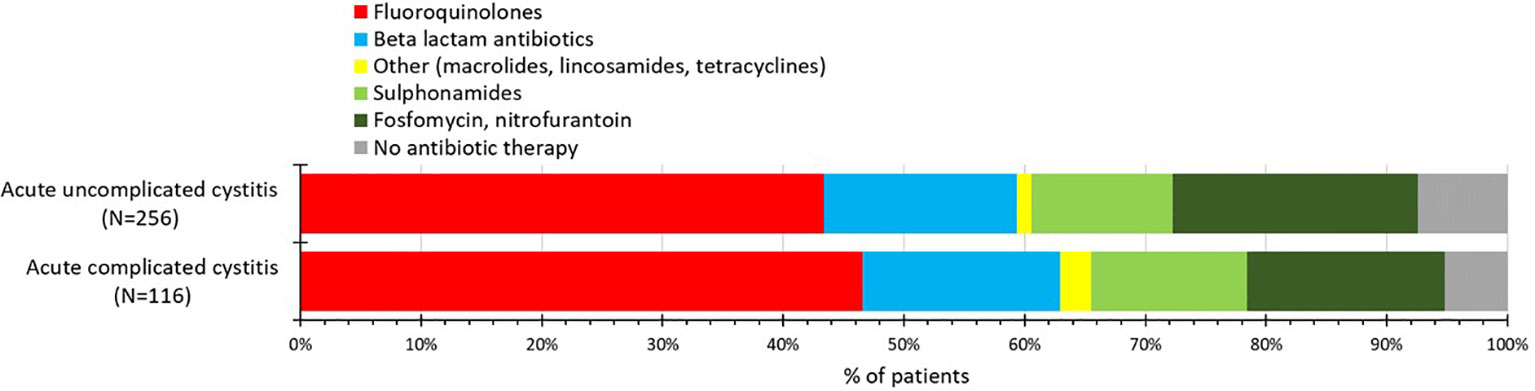
Figure 1 Antibiotic prescription at initial presentation.
The most frequently prescribed antibiotics are shown in Table 2. Although their rankings differed, the top five antibiotics were the same in both types of cystitis. Ciprofloxacin was the most widely used agent. Sulphamethoxazol-trimethoprim and fosfomycin were among the most frequently prescribed antibacterials. Nitrofurantoin was prescribed rarely (uncomplicated cystitis: 4 cases, complicated cystitis: 6 cases). Guideline-recommended short-term antibiotic course was initiated in ~30% of cases (Table 2).
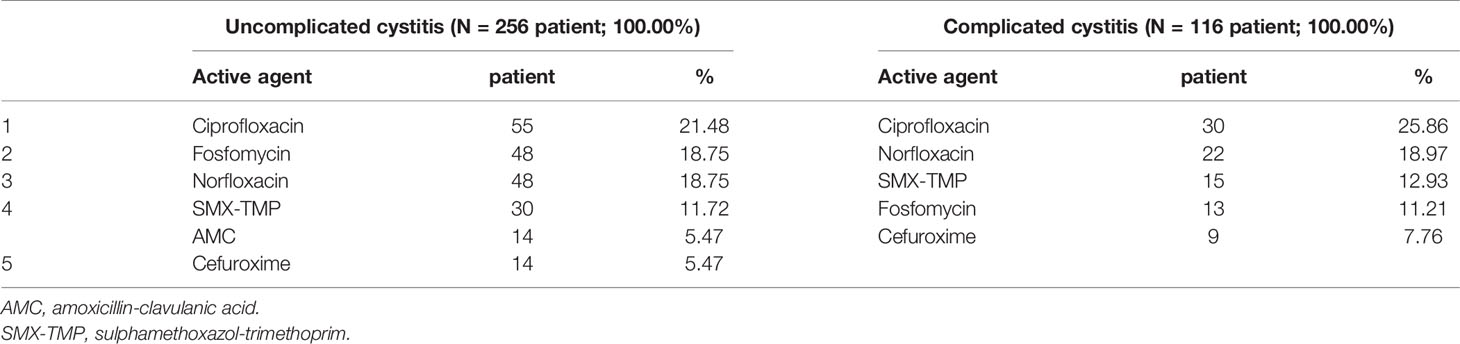
Table 2 Most frequently prescribed systemic antibiotics.
Only evidence of a weak association was found between patient characteristics and fluoroquinolone prescribing (Table 3): younger adults and those with complicating factors tended to be treated with fluoroquinolones (odds ratio age: 0.98 yearly; odds ratio complicating factors: 1.80). The frequency of fluoroquinolone prescribing varied substantially: some of the GPs did not prescribe these agents at all, while a single GP prescribed this antibiotic in 85.71% of cystitis cases diagnosed in her practice.
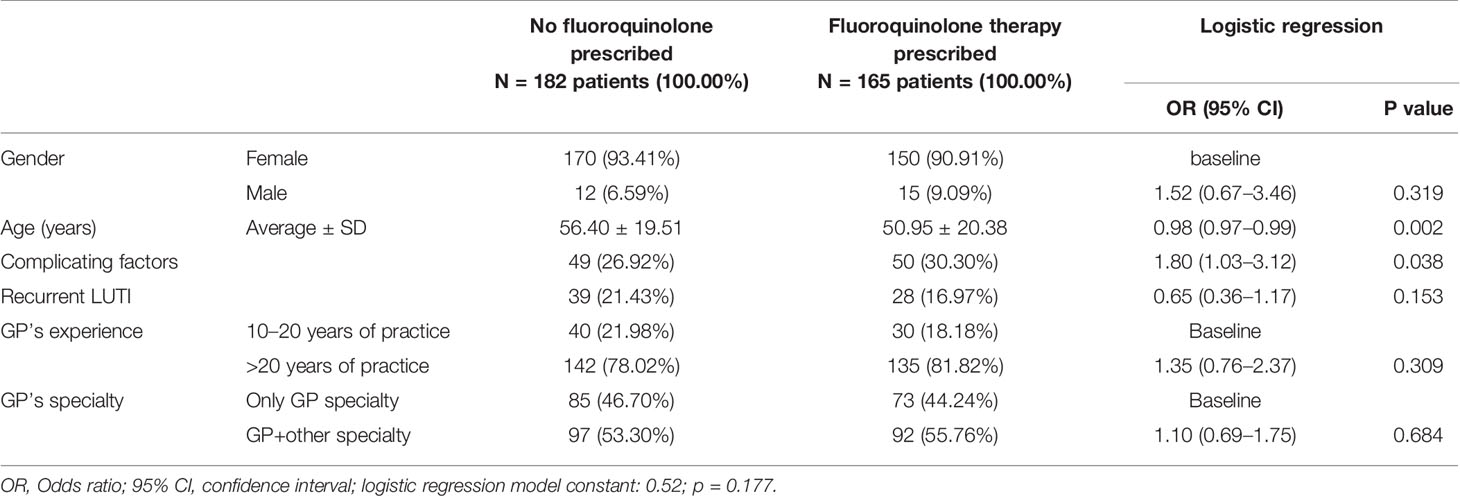
Table 3 Fluoroquinolone prescribing with regard to patient- and GP-specific factors.
Discussion
The burden of urinary tract infections is high worldwide (Foxman, 2014). However, field studies to provide more insight into the clinical practice of the outpatient management of UTIs in adults are scarce (Martinez et al., 2007; Llor et al., 2011; Denes et al., 2012; Butler et al., 2017; Dumpis et al., 2018). The main objective of our study was to fill in this gap by assessing empiric antibiotic choice in different lower urinary tract infections (i.e. complicated and uncomplicated cystitis). No significant difference has been observed in the antibiotic prescribing patterns for the two types of cystitis.
As antibiotics are unambiguously superior to placebo for urinary tract infections (Falagas et al., 2009), antibiotic use can be considered optimal in every LUTI case. The rate of antibiotic prescribing for LUTI in this study (over 90%) meets international quality indicators (Adriaenssens et al., 2011; Le Marechal et al., 2018) and correlates well with findings of antibiotic utilisation studies for other countries, except the Netherlands and Latvia where antibiotic prescription rate is reported to be less than 60% and around 70% in acute urinary tract infections in adults, respectively (Martinez et al., 2007; Llor et al., 2011; Butler et al., 2017). The lower prescription rate in these countries may be explained by the more frequent application of delayed or conditional antibiotic prescribing (Gagyor et al., 2012; Gagyor et al., 2015).
The use of analgesics/anti-inflammatory agents was found to be limited, which can be explained by the lack of such recommendations in national and international guidelines on urological infections (Ministry of Health, 2010; Bonkat et al., 2017). This is in contrast to the German guideline which only recommends symptomatic treatment in uncomplicated cystitis with mild to moderate symptoms (Kranz et al., 2017).
Short-course oral antibacterial treatment has been proven to be as effective as long courses of antibiotics in the ambulatory management of LUTIs (Dawson-Hahn et al., 2017). However, in our study only 1 in 3 patients with uncomplicated cystitis received a short-term antibiotic course, a finding similar to other studies (Llor et al., 2011; Denes et al., 2012; Hawker et al., 2014; Durkin et al., 2018; Phamnguyen et al., 2019). This may be explained by the fact that pharmacies can dispense only complete boxes of medicines instead of a certain number of tablets actually needed,
The GPs in this study performed urine analysis (i.e. a urine dipstick test) in the majority of cases in both types of cystitis. As dipstick analysis is considered to have little added value when typical urinary tract symptoms are present (Bonkat et al., 2017), unnecessary testing can be presumed in some cases. On the other hand, as dipstick analysis may also give information on the causative bacterial class (i.e nitrite test is positive if Enterobacteriaceae is present) its use can be justified.
Microbiological confirmation of UTI is recommended in all cases of complicated infections and recurrent urinary tract symptoms (Bonkat et al., 2017). Unfortunately, microbiological analysis was requested at a suboptimal rate (i.e only in 21.55% in complicated LUTI) which can be partly explained by logistic issues (lack of local laboratories and long distance between the GP’s practice and laboratories) that hamper timely identification of the pathogens (Hajdu et al., 2009). The Flexicult system (Bates et al., 2014; Hullegie et al., 2017), aimed for point-of-care diagnoses of UTI and susceptibility testing of urinary pathogens is not used in Hungary due to the lack of reimbursement (and also this is the case for other point-of-care tests utilized in other e.g. Scandinavian countries).
The pattern of antibiotic use was similar for both uncomplicated and complicated cystitis, and showed a high dominance of fluoroquinolones. The use of fluoroquinolones in UTI varies greatly in the literature, but none of the European countries (except for a non-recent publication from France)(Denes et al., 2012) reported such a high ratio of fluoroquinolone prescribing. In Norway, Denmark, Sweden and the Netherlands the use of fluoroquinolone agents were reported to be below 10%, thanks to strict and well-functioning antibiotic stewardships (Agdestein et al., 2011; Tyrstrup et al., 2017; Dumpis et al., 2018; Holm et al., 2019). In Latvia and Lithuania, fluoroquinolones are reported to be used in 23% and 25% of uncomplicated UTI cases, respectively (Dumpis et al., 2018). Similar rates for fluoroquinolone use in cystitis (22%) was reported for Belgium (Tyrstrup et al., 2017). In contrast, a relatively frequent fluoroquinolone use (30% of all cases) in uncomplicated UTI has been reported from the US recently, and this rate was even higher in the preceding years (Durkin et al., 2018; Cowart et al., 2019). The decreasing trend is explained by the publication of an FDA black box warning on fluoroquinolones in 2016 (Cowart et al., 2019). In Hungary no up-to-date guidelines are available for the antibiotic prescribing in UTIs, and the previous guidelines (that still pop-up as the first hit in a google search) recommended the use of fluoroquinolones in all types of UTIs (Nephrology, 2006; Ministry of Health, 2010). Thus, in fact, our findings are not surprising, but the high fluoroquinolone dominance is unwanted, especially if we consider the 2018 safety review-based restrictions (European Medicines Agency, 2019) of the European Commission on fluoroquinolone prescribing (valid since 11 March 2019 in all EU countries).
Only weak determinants of fluoroquinolone prescribing were identified: younger age and presence of complicating factors were found to influence the rate of fluoroquinolone therapy. As fluoroquinolones have a high potential to generate resistance (Schito et al., 2009), and the fluoroquinolone resistance of E.coli already exceeds 20% in urine samples in Hungary (Hungarian National Bacteriological Surveillance Management Team, National Centre for Epidemiology), the high use of fluoroquinolones demonstrated in our study is clearly worrisome. Qualitative studies are needed to better explore the high differences in fluoroquinolone prescribing rate of individual GPs.
Patients with uncomplicated cystitis were prescribed fosfomycin in 18.75% of all cases and nitrofurantoin in only 4 cases which is suboptimal according to international quality indicators (Adriaenssens et al., 2011). These data are also regarded as worrisome, as these two drugs have their renaissance in the treatment of uncomplicated LUTI due to their preserved effectiveness (Gardiner et al., 2019). On the other hand, these agents (i.e. fosfomycin and nitrofurantoin) should be avoided in complicated cystitis due to their lack of activity against the potential uropathogens in these cases (Bonkat et al., 2017). Nevertheless, fosfomycin was among the top five agents prescribed for complicated cystitis.
Regarding sulphamethoxazol-trimethoprim (SMX-TMP), its first line use should be limited to uncomplicated cases, and only when local resistance patterns permit this choice. In Hungary, the prevalence of E. coli strains resistant to sulphamethoxazol-trimethoprim is reported to be above 20% (Hungarian National Bacteriological Surveillance Management Team National Centre for Epidemiology), but considering that resistance surveillance systems may overestimate resistance patterns (Schmiemann et al., 2012), SMX-TMP use can be accepted as a rational choice in uncomplicated cystitis.
The strengths of our survey include the ability to exploit clinical data. Also, by applying common diagnostic and classification criteria, misclassification bias could be avoided, and the choice of antibiotic could be justified. A limitation of our study is the voluntary participation of GPs. As volunteering GPs may be more concerned about their rational antibiotic prescribing practices, the global prescribing patterns in Hungary might be more suboptimal than presented in this study.
Conclusions
Our study has found similar patterns of antibiotic use in both types of cystitis (with high fluoroquinolone dominance), and identified suboptimal antibiotic use from various aspects. Patient characteristics has weakly influenced fluoroquinolone prescribing More prudent use of antibiotics in lower urinary tract infections is urgently needed.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by the Regional Human Medical Biology Research Ethical Board of the University of Szeged. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
RBe, MM, ZJ, JB, EH, and ZP had the original idea for the manuscript. ZJ and EH organized data collection. RBo, MM, JB, GS, and ZP contributed to the analysis. RBo, MM, and JB drafted the manuscript, which was reviewed and approved by ZP, ZJ, GS, and EH.
Funding
The study was funded by the University of Szeged.
Conflict of Interest
Author JB is employed at Grove Lodge One, though she was not at the time the study was conducted.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We are grateful to all participating GPs. The authors thank Dora Bokor, PharmD, for proofreading the manuscript. Preliminary analysis of this work is present in a PhD thesis (Juhasz, 2017).
References
Adriaenssens, N., Coenen, S., Tonkin-Crine, S., Verheij, T. J. M., Little, P., Goossens, H. (2011). European surveillance of antimicrobial consumption (ESAC): disease-specific quality indicators for outpatient antibiotic prescribing. BMJ Qual. Saf. 20, 764–772. doi: 10.1136/bmjqs.2010.049049
Agdestein, B., Lindbæk, M., Gjelstad, S. (2011). [Do general practitioners follow the national guidelines for treating urinary tract infections with antibiotics]? Tidsskrift Den Norske Laegeforening: Tidsskrift Praktisk Med. 131, 1641–1644. doi: 10.4045/tidsskr.10.0396
Bates, J., Thomas-Jones, E., Pickles, T., Kirby, N., Gal, M., Bongard, E., et al. (2014). Point of care testing for urinary tract infection in primary care (POETIC): protocol for a randomised controlled trial of the clinical and cost effectiveness of FLEXICULT informed management of uncomplicated UTI in primary care. BMC Fam. Pract. 15, 187. doi: 10.1186/s12875-014-0187-4
Bonkat, G., Pickard, R., Bartoletti, R., Bruyère, F., Geerlings, S. E., Wagenlehner, F. (2017). EAU Guidelines on Urological Infections. European Association of Urology. Available at: https://uroweb.org/wp-content/uploads/19-Urological-infections_2017_web.pdf.
Butler, C. C., Francis, N., Thomas-Jones, E., Llor, C., Bongard, E., Moore, M., et al. (2017). Variations in presentation, management, and patient outcomes of urinary tract infection: a prospective four-country primary care observational cohort study. Br. J. Gen. Pract. 67, e830–e841. doi: 10.3399/bjgp17X693641
Cowart, K., Worley, M., Rouby, N. E., Sando, K. (2019). Evaluation of FDA boxed warning on prescribing patterns of fluoroquinolones for uncomplicated urinary tract infections. Ann. Pharmacother., 1060028019865224. doi: 10.1177/1060028019865224
Dawson-Hahn, E. E., Mickan, S., Onakpoya, I., Roberts, N., Kronman, M., Butler, C. C., et al. (2017). Short-course versus long-course oral antibiotic treatment for infections treated in outpatient settings: a review of systematic reviews. Fam. Pract. 34, 511–519. doi: 10.1093/fampra/cmx037
Denes, E., Prouzergue, J., Ducroix-Roubertou, S., Aupetit, C., Weinbreck, P. (2012). Antibiotic prescription by general practitioners for urinary tract infections in outpatients. Eur. J. Clin. Microbiol. Infect. Dis.: Off. Publ. Eur. Soc. Clin. Microbiol. 31, 3079–3083. doi: 10.1007/s10096-012-1668-9
Dumpis, U., Hahlin, A., Varvuolyte, S., Stenmark, S., Veide, S., Valinteliene, R., et al. (2018). Antibiotic prescription and clinical management of common infections among general practitioners in Latvia, Lithuania, and Sweden: a pilot survey with a simple protocol. Eur. J. Clin. Microbiol. Infect. Dis. 37, 355–361. doi: 10.1007/s10096-017-3141-2
Durkin, M. J., Keller, M., Butler, A. M., Kwon, J. H., Dubberke, E. R., Miller, A. C., et al. (2018). An assessment of inappropriate antibiotic use and guideline adherence for uncomplicated urinary tract infections. Open Forum Infect. Dis. 5, ofy198. doi: 10.1093/ofid/ofy198
European Medicines Agency. (2019). Disabling and potentially permanent side effects lead to suspension or restrictions of quinolone and fluoroquinolone antibiotics. EMA’s human medicines committee (CHMP) Available at: https://www.ema.europa.eu/en/medicines/human/referrals/quinolone-fluoroquinolone-containing-medicinal-products.
Falagas, M. E., Kotsantis, I. K., Vouloumanou, E. K., Rafailidis, P. I. (2009). Antibiotics versus placebo in the treatment of women with uncomplicated cystitis: a meta-analysis of randomized controlled trials. J. Infect. 58, 91–102. doi: 10.1016/j.jinf.2008.12.009
Foxman, B. (2014). Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect. Dis. Clinics North America 28, 1–13. doi: 10.1016/j.idc.2013.09.003
Gagyor, I., Hummers-Pradier, E., Kochen, M. M., Schmiemann, G., Wegscheider, K., Bleidorn, J. (2012). Immediate versus conditional treatment of uncomplicated urinary tract infection - a randomized-controlled comparative effectiveness study in general practices. BMC Infect. Dis. 12, 146. doi: 10.1186/1471-2334-12-146
Gagyor, I., Bleidorn, J., Kochen, M. M., Schmiemann, G., Wegscheider, K., Hummers-Pradier, E. (2015). Ibuprofen versus fosfomycin for uncomplicated urinary tract infection in women: randomised controlled trial. BMJ 351, h6544. doi: 10.1136/bmj.h6544
Gardiner, B. J., Stewardson, A. J., Abbott, I. J., Peleg, A. Y. (2019). Nitrofurantoin and fosfomycin for resistant urinary tract infections: old drugs for emerging problems. Aust. Prescr. 42, 14–19. doi: 10.18773/austprescr.2019.002
Hajdu, E., Benko, R., Matuz, M., Peto, Z., Hegedus, A., Soos, G., et al. (2009). [Microbiological service for intensive care units in Hungary]. Orv. Hetil. 150, 1037–1042. doi: 10.1556/OH.2009.28592
Hawker, J. I., Smith, S., Smith, G. E., Morbey, R., Johnson, A. P., Fleming, D. M., et al. (2014). Trends in antibiotic prescribing in primary care for clinical syndromes subject to national recommendations to reduce antibiotic resistance, UK 1995-2011: analysis of a large database of primary care consultations. J. Antimicrob. Chemother. 69, 3423–3430. doi: 10.1093/jac/dku291
Holm, A., Cordoba, G., Aabenhus, R. (2019). Prescription of antibiotics for urinary tract infection in general practice in Denmark. Scand. J. Prim. Health Care 37, 83–89. doi: 10.1080/02813432.2019.1569425
Hullegie, S., Wootton, M., Verheij, T. J. M., Thomas-Jones, E., Bates, J., Hood, K., et al. (2017). Clinicians’ interpretations of point of care urine culture versus laboratory culture results: analysis from the four-country POETIC trial of diagnosis of uncomplicated urinary tract infection in primary care. Fam. Pract. 34, 392–399. doi: 10.1093/fampra/cmx009
Hungarian National Bacteriological Surveillance Management Team National Centre for Epidemiology. (2016). National Bacteriological Surveillance annual report. Available at: www.oek.hu.
Juhasz, Z., Benko, R., Matuz, M., Viola, R., Soos, G., Hajdu, E. (2013). Treatment of acute cystitis in Hungary: comparison with national guidelines and with disease-specific quality indicators. Scand. J. Infect. Dis. 45, 612–615. doi: 10.3109/00365548.2013.777157
Juhasz, Z. (2017). Evaluation of the Hungarian ambulatory antibacterial use in urinary tract infections with different methods. Hungarian Doctoral Council. Available at: http://doktori.bibl.u-szeged.hu/3150/2/T%C3%A9zis_angol.pdf.
Kranz, J., Schmidt, S., Lebert, C., Schneidewind, L., Schmiemann, G., Wagenlehner, F. (2017). Uncomplicated bacterial communityacquired urinary tract infection in adults. Dtsch Arztebl Int. 114, 866–873. doi: 10.3238/arztebl.2017.0866
Le Marechal, M., Tebano, G., Monnier, A. A., Adriaenssens, N., Gyssens, I. C., Huttner, B., et al. (2018). Quality indicators assessing antibiotic use in the outpatient setting: a systematic review followed by an international multidisciplinary consensus procedure. J. Antimicrob. Chemother. 73, vi40–vi49. doi: 10.1093/jac/dky117
Llor, C., Rabanaque, G., Lopez, A., Cots, J. M. (2011). The adherence of GPs to guidelines for the diagnosis and treatment of lower urinary tract infections in women is poor. Family Pract. 28, 294–299. doi: 10.1093/fampra/cmq107
Martinez, M. A., Inglada, L., Ochoa, C., Villagrasa, J. R. (2007). Assessment of antibiotic prescription in acute urinary tract infections in adults. J. Infect. 54, 235–244. doi: 10.1016/j.jinf.2006.05.015
Matuz, M., Bognar, J., Hajdu, E., Doro, P., Bor, A., Viola, R., et al. (2015). Treatment of community-acquired pneumonia in adults: analysis of the national dispensing database. Basic Clin. Pharmacol. Toxicol. 117, 330–334. doi: 10.1111/bcpt.12426
Ministry of Health. (2010). Diagnoses and management of uncomplicated urinary tract infections, Ministry of Health. Available at: http://www.kozlonyok.hu/kozlonyok/Kozlonyok/6/PDF/2010/4.pdf.
Nephrology, H. P. C. of I. M. (2006). Evaluation and treatment of uncomplicated urinary tract infections. Hungarian Professional College of Internal Medicine and Nephrology.
Phamnguyen, T. J., Murphy, G., Hashem, F. (2019). Single centre observational study on antibiotic prescribing adherence to clinical practice guidelines for treatment of uncomplicated urinary tract infection. Infect. Dis. Health 24, 75–81. doi: 10.1016/j.idh.2018.10.005
Reynard J, B. F., Biers S, N. N. (2019). Oxford Handbook of Urology. 4th edition (Fourth: Oxford University Press).
Schito, G. C., Naber, K. G., Botto, H., Palou, J., Mazzei, T., Gualco, L., et al. (2009). The ARESC study: an international survey on the antimicrobial resistance of pathogens involved in uncomplicated urinary tract infections. Int. J. Antimicrob. Agents 34, 407–413. doi: 10.1016/j.ijantimicag.2009.04.012
Schmiemann, G., Gagyor, I., Hummers-Pradier, E., Bleidorn, J. (2012). Resistance profiles of urinary tract infections in general practice–an observational study. BMC Urol. 12, 33. doi: 10.1186/1471-2490-12-33
Tyrstrup, M., van der Velden, A., Engstrom, S., Goderis, G., Molstad, S., Verheij, T., et al. (2017). Antibiotic prescribing in relation to diagnoses and consultation rates in Belgium, the Netherlands and Sweden: use of European quality indicators. Scand. J. Prim. Health Care 35, 10–18. doi: 10.1080/02813432.2017.1288680
Keywords: lower urinary tract infection, management, antibiotic choice, fluoroquinolone use, symptomatic treatment, antibiotic stewardship
Citation: Benko R, Matuz M, Juhasz Z, Bognar J, Bordas R, Soos G, Hajdu E and Peto Z (2019) Treatment of Cystitis by Hungarian General Practitioners: A Prospective Observational Study. Front. Pharmacol. 10:1498. doi: 10.3389/fphar.2019.01498
Received: 30 August 2019; Accepted: 19 November 2019;
Published: 19 December 2019.
Edited by:
Luciane Cruz Lopes, Universidade de Sorocaba, BrazilReviewed by:
Tore Wentzel-Larsenm, Norwegian Centre for Violence and Traumatic Stress Studies, NorwayDaniela Oliveira De Melo, Federal University of São Paulo, Brazil
Copyright © 2019 Benko, Matuz, Juhasz, Bognar, Bordas, Soos, Hajdu and Peto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ria Benko cmlhLmJlbmtvQHBoYXJtLnUtc3plZ2VkLmh1YmVua29yaWFAZ21haWwuY29t