
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pharmacol. , 27 March 2019
Sec. Pharmacogenetics and Pharmacogenomics
Volume 10 - 2019 | https://doi.org/10.3389/fphar.2019.00236
This article is part of the Research Topic Establishing Genetic Pleiotropy to Identify Common Pharmacological Agents for Common Diseases View all 5 articles
 Jiecan Zhou1,2,3,4
Jiecan Zhou1,2,3,4 Fazhong He1,2,3
Fazhong He1,2,3 Bao Sun1,2,3Rong Liu1,2,3Yongchao Gao1,2,3Huan Ren1,2,3Yan Shu5
Bao Sun1,2,3Rong Liu1,2,3Yongchao Gao1,2,3Huan Ren1,2,3Yan Shu5 Xiaoping Chen1,2,3
Xiaoping Chen1,2,3 Zhaoqian Liu1,2,3
Zhaoqian Liu1,2,3 Honghao Zhou1,2,3Sheng Deng6
Honghao Zhou1,2,3Sheng Deng6 Heng Xu7Jianmin Li8*Linyong Xu9*
Heng Xu7Jianmin Li8*Linyong Xu9* Wei Zhang1,2,3*
Wei Zhang1,2,3*Tribbles homolog 3 (TRIB3) mediating signaling pathways are closely related to blood pressure regulation. Our previous findings suggested a greater benefit on vascular outcomes in patients carrying TRIB3 (251, A > G, rs2295490) G allele with good glucose and blood pressure control. And TRIB3 (rs2295490) AG/GG genotypes were found to reduce primary vascular events in type 2 diabetic patients who received intensive glucose treatment as compared to those receiving standard glucose treatment. However, the effect of TRIB3 genetic variation on antihypertensives was not clear in essential hypertension patients. A total of 368 patients treated with conventional dosage of antihypertensives (6 groups, grouped by atenolol/bisoprolol, celiprolol, doxazosin, azelnidipine/nitrendipine, imidapril, and candesartan/irbesartan) were enrolled in our study. Genetic variations were successfully identified by sanger sequencing. A linear mixed model analysis was performed to evaluate blood pressures among TRIB3 (251, A > G) genotypes and adjusted for baseline age, gender, body mass index, systolic blood pressure (SBP), diastolic blood pressure (DBP), total cholesterol and other biochemical factors appropriately. Our data suggested that TRIB3 (251, A > G) AA genotype carriers showed better antihypertensive effect than the AG/GG genotype carriers [P = 0.014 for DBP and P = 0.042 for mean arterial pressure (MAP)], with a maximal reduction of DBP by 4.2 mmHg and MAP by 3.56 mmHg after azelnidipine or nitrendipine treatment at the 4th week. Similar tendency of DBP-change and MAP-change was found for imidapril (ACEI) treatment, in which marginally significances were achieved (P = 0.073 and 0.075, respectively). Against that, we found that TRIB3 (251, A > G) AG/GG genotype carriers benefited from antihypertensive therapy of ARBs with a larger DBP-change during the period of observation (P = 0.036). Additionally, stratified analysis revealed an obvious difference of the maximal blood pressure change (13 mmHg for the MAP between male and female patients with AA genotype who took ARBs). Although no significant difference in antihypertensive effect between TRIB3 (251, A > G) genotypes in patients treated with α, β-ADRs was observed, we found significant difference in age-, sex-dependent manner related to α, β-ADRs. In conclusion, our data supported that TRIB3 (251, A > G) genetic polymorphism may serve as a useful biomarker in the treatment of hypertension.
Essential hypertension (EH) can be defined as a rise in blood pressure for unknown cause. It can increase risks for cerebral, cardiac, and renal events. It usually clusters with other cardiovascular risk factors such as aging, being overweight, insulin resistance, diabetes, and hyperlipidaemia (Messerli et al., 2007; Sun et al., 2019). Human tribbles homolog 3 (TRIB3) is organized as four exons, encoding a 358-amino-acid protein. TRIB3 proteins disrupts insulin signaling by binding directly to Akt and blocking activation of the kinase, which contributes to insulin resistance and other physiological processes of vessel (Du et al., 2003; Prudente and Trischitta, 2015). AKT mediates the phosphatidylinositol 3′-kinase-protein kinase B-endothelial nitric oxide (NO) synthase (PI3K-AKT-eNOS)-dependent pathway in the cardiovascular protective effect of insulin, which is crucial for NO synthase activation, eventually leading to increased NO production, vasodilation and blood flow (Yu et al., 2011). Other signaling molecules such as bone morphogenetic proteins type II receptor (BMRPII) and bone morphogenetic proteins (BMP) also interact with TRIB3 and modulate the vascular effect (Kiss-Toth et al., 2004; West et al., 2004; Chan et al., 2007). Accumulating evidences supported that some drugs or active materials affect vascular functions by regulating TRIB3. For example, the amiloride derivative phenamil promotes contractile phenotype of vascular smooth muscle cells (vSMCs) by activating TRIB3 gene transcription (Chan et al., 2011; Kim et al., 2014). Homocysteine, which is significantly associated with hypertension could up-regulate the expression of TRIB3, thus leading to the endothelial dysfunction (Chan et al., 2011; Zou et al., 2011).
A single nucleotide polymorphism (SNP) variant in human TRIB3 exon 2, which results in a glutamine (Q) to arginine (R) missense mutation in a conserved motif at position 84, confers stronger Akt binding, resulting in reduced Akt phosphorylation (Fischer et al., 2017). Since Prudente S first reported the relationship between TRIB3 missense Q84R (rs2295490) polymorphism and insulin resistance or its related cardiovascular events (Prudente et al., 2005), numerous clinical studies have confirmed the risk of genetic variant associated with vascular events, especially the deleterious role of TRIB3 R84 (Gong et al., 2009; Formoso et al., 2011; Prudente et al., 2015; Zhang et al., 2015). Among patients with metabolic syndrome and the control group, patients with TRIB3 RR84 genotype had significantly higher level of serum semaphorin 3E than those with QQ84 or QR84 genotypes (Qin et al., 2017), individuals with RR84 genotype also showed further decreased serum obestatin. Increased serum semaphorin 3E or decreased serum obestatin might in part exacerbate insulin resistance and carotid atherosclerosis (Cui et al., 2012). In human endothelial cells, data demonstrate that the TRIB3 R84 variant impairs insulin signaling and NO production (Andreozzi et al., 2008). These vascular disease-related studies suggested a possible link between TRIB3 and EH.
Studies showed that imidapril mediated various actions, such as vasodilation, anticoagulation, hypotension, atherosclerosis and other cardiovascular protection via bradykinin-eNOS-NO pathway (Kobayashi et al., 2000; Chen et al., 2003). Celiprolol triggered PI3K-Akt and increased eNOS expression (Kobayashi et al., 2003), and doxazosin also increased the expression of eNOS accompanying with NO production via cAMP/cGMP/adrenalin signaling pathway (Stojkov et al., 2013, 2014). Azelnidipine significantly increased eNOS expression levels in the brain as well as in the heart and aorta (Kimura et al., 2007). Zhang, et al. demonstrated that valsartan significantly down-regulated the expression of TRIB3 mRNA level and improved the cardiac function in rats with diabetic cardiomyopathy (Zhang et al., 2006).
These data indicate that TRIB3 has an integral role in regulating the blood pressure, and its genetic variation (251, A > G) may cause a variability of antihypertensive drug therapy. Our previous findings have suggested a greater benefit on vascular outcomes in patients carrying TRIB3 (rs2295490) G allele with good glucose and blood pressure control (He et al., 2016). TRIB3 (rs2295490) AG/GG genotypes were found to reduce primary vascular events in patients who received intensive glucose treatment as compared to those receiving standard glucose treatment in type 2 diabetic patients (He et al., 2018). However, to our knowledge, there is no study to evaluate the association between TRIB3 Q84R polymorphism and the effect of antihypertensive drugs in patients with EH.
The study protocol was approved by the Ethical Committee of the Institute of Clinical Pharmacology, Central South University (Hunan, China). Clinical study was registered at the Chinese Clinical Trial Register with the registration number ChiCTR-RO-120026121. All the patients participating in the study were given written informed consent. The clinical data and DNA samples were graciously provided by Shanghai Institute of Hypertension, Ruijin Hospital affiliated with Shanghai Jiao Tong University. According to study design, all the patients fulfilled the following inclusion and exclusion criteria: male or female patients, heart rates within 55∼90 beats/min, systolic blood pressure (SBP) ≥ 140 mmHg and/or diastolic blood pressure (DBP) ≥ 90 mmHg were included. Patients with secondary hypertension, coronary heart disease, diabetes, obesity (BMI.30 kg/m2), stroke, renal or liver dysfunction, malignant tumor or pregnancy and those whose blood pressure measurements above 180/110 mmHg or remaining lower than 140/90 mmHg during the wash-out period, were withdrawn from the study. In our study, a total of 368 unrelated subjects with primary mild to moderate EH, aged from 26 to 81 years were recruited for genetic screening. All the patients were enrolled after a run-in period of 2 weeks and assigned to receive the drugs for 4 weeks or more. The patients were followed up every 2 weeks at the weekend, and details of the protocol were shown in Table 1. According to the study protocol, 86 samples were excluded from 454 eligible patients due to the small sample size, not contactable and fail to meet inclusion criteria. At last, a total of 368 patients were included in our study. The medications include β-adrenoceptor antagonists (β-ADRs, atenolol, bisoprolol and celiprolol), α-adrenoceptor antagonist (α-ADR, doxazosin), calcium channel blockers (CCBs, azelnidipine and compound nitrendipine), ACE-inhibitor (ACEI, imidapril) and angiotensin receptor blocker (ARB, candesartan and irbesartan). All patients received monotherapy. Details are shown in Figure 1.
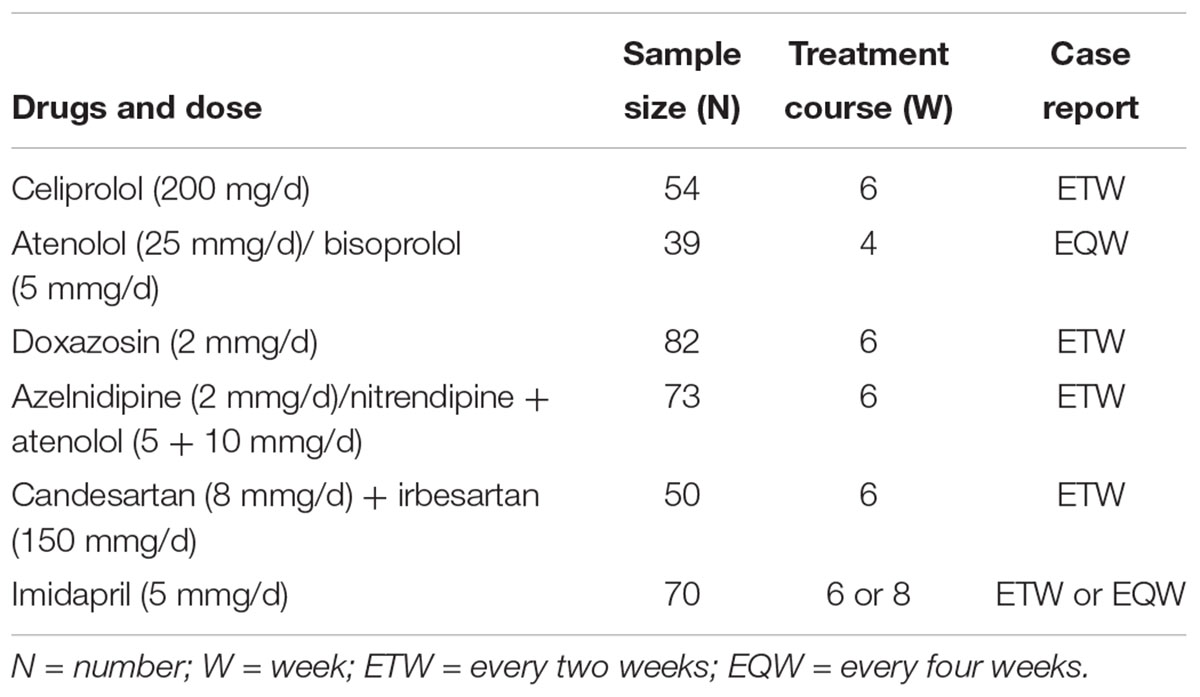
Table 1. The protocols of the related drugs to a total of 368 eligible patients in the study.
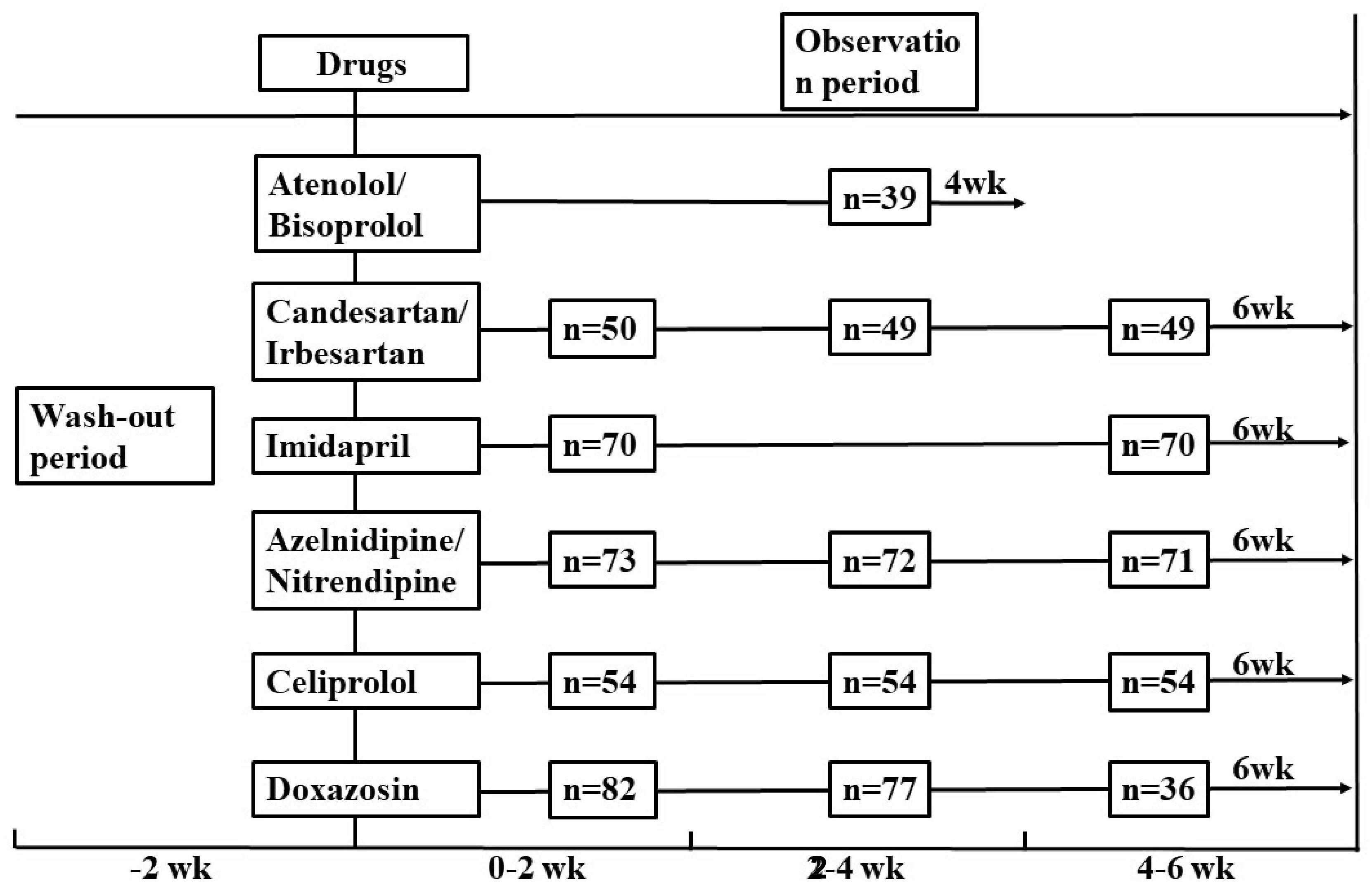
Figure 1. Study protocol and visit time to 368 patients with related drugs in the study. wk, week.
Blood pressure determinations were performed on the morning after a light breakfast with subjects in the seated position and following a 30 min quiet resting period. Blood pressure and heart rate were measured by trained nurses, with an automatic blood pressure monitor with intellisense, which allows the detection of alteration of the heart rate by greater than or equal to beat/min and the blood pressure by greater than or equal to 1 mmHg. Detected results were then validated by supervisors with the mercury sphygmomanometer. The blood pressure values were determined by the average of three measurements taken every 10 min. Values of SBP and DBP were defined by Korotkoff phase I and V, respectively. Pulse pressure was calculated as PP = (SBP- DBP); mean arterial pressure (MAP) was calculated as MBP = DBP + (PP/3) (Wain et al., 2011).
Tribbles homolog 3 (251, A > G) genotypes were determined by sanger sequencing. The PCR primers for TRIB3 (251, A > G) were shown as follows: the sense primer, 5′GTTGCCCCTGAGCCCACCTACT3′; and the antisense primer, 5′TCCCTGGATGCTTCCCCACTAA3′. The product length was 286 bp. The reaction mixture (25 μl) contained: 10 × PCR buffer (2.5 μl), 10 × dNTP (2.5 μl), 10 μM for each of the sense and antisense primers (0.5 μl), H2O (16.8 μl), gDNA (2 μl), Taq polymerase (0.2 μl). Temperature cycling was proceeded as follows: initial denaturation for 5 min at 94°C, followed by 36 cycles of denaturation 30 s at 94°C, annealing at 57°C for 30 s, and elongation at 72°C for 30 s, and a terminal extension for 5 min. Genotypes were determined without knowledge of the status of patients, Ten percent blinded, random DNA samples from the patients were genotyped twice, with 100% concordance. And sequencing was assisted by Shanghai Majorbio Bio-pharm Technology Company.
All the analyses were performed with SPSS (version 19.0 for windows; Chicago, IL, United States). Allele frequencies were determined by the genotypes of all the participants. Continuous data were presented as mean values ± standard error (SE), and categorical variable was shown as frequencies and percentages. The Hardy–Weinberg equilibrium analysis was carried out for the genotypes of participants using the χ2-test. Difference in baseline characteristics among the phenotypes were assessed by independent-samples T-test.
The linear mixed model was used to examine the efficacy of TRIB3 (251, A > G). This allowed the use of time-dependent and time-independent covariates within the model to be analyzed. Furthermore, this model has been found to work well for small sample sizes with missing data (Patel et al., 2007; Chen et al., 2015). The outcome measures included ΔSBP, ΔDBP and ΔMAP. These measures were analyzed individually, with the main effects of genotype, follow-up time and their interaction, as well as subjects’ intercept serving as random effects. The best fit model was decided after checking the smallest Akaike Information Criterion (AIC), and the Schwarz Bayesian Criterion (BIC) values. The covariance structure adopted for the final model was the Unstructured (UN) which means each variance and each covariance is estimated uniquely from the data. Models were additionally adjusted for the fixed effects of baseline age, sex, body mass index (BMI), SBP, DBP, total cholesterol, heart rate, triglyceride, high-density lipoprotein (HDL), low-density lipoprotein (LDL), fasting blood-glucose (FBG) and other biochemical factors appropriately. The linear mixed model analysis was done by using the PASW 19.0 for Windows (SPSS Inc., Chicago, IL, United States). Functions in nlme package of R statistical computing environment (R Foundation —for Statistical Computing, Vienna, Austria) were used to confirm the analysis. Stratified Analysis was used to address whether significant interaction was present between age-genotype and sex-genotype. A two-tailed P-value < 0.05 was considered significant.
In this study, 368 patients were genotyped unambiguously for TRIB3 (251, A > G) genetic variation. Our data showed that the frequency of TRIB3 (251, A > G) G allele was 18.5% in Chinese population. Genotype frequencies of TRIB3 (251, A > G) AA, AG and GG were 66.0, 31.0 and 3.0%, respectively. All the allele frequencies were in Hardy-Weinberg equilibrium (P > 0.05). Owing to the low frequency of the GG genotype, we combined the AG and GG genotypes as one group for the following analysis. Baseline characteristics of the patients stratified by TRIB3 genotypes are shown in Table 2. No significant differences between AA and AG+GG genotype groups in age, BMI, HR, BP or other clinical characteristics, such as FBG, triglyceride, cholesterol, HDL and LDL, etc. were observed.
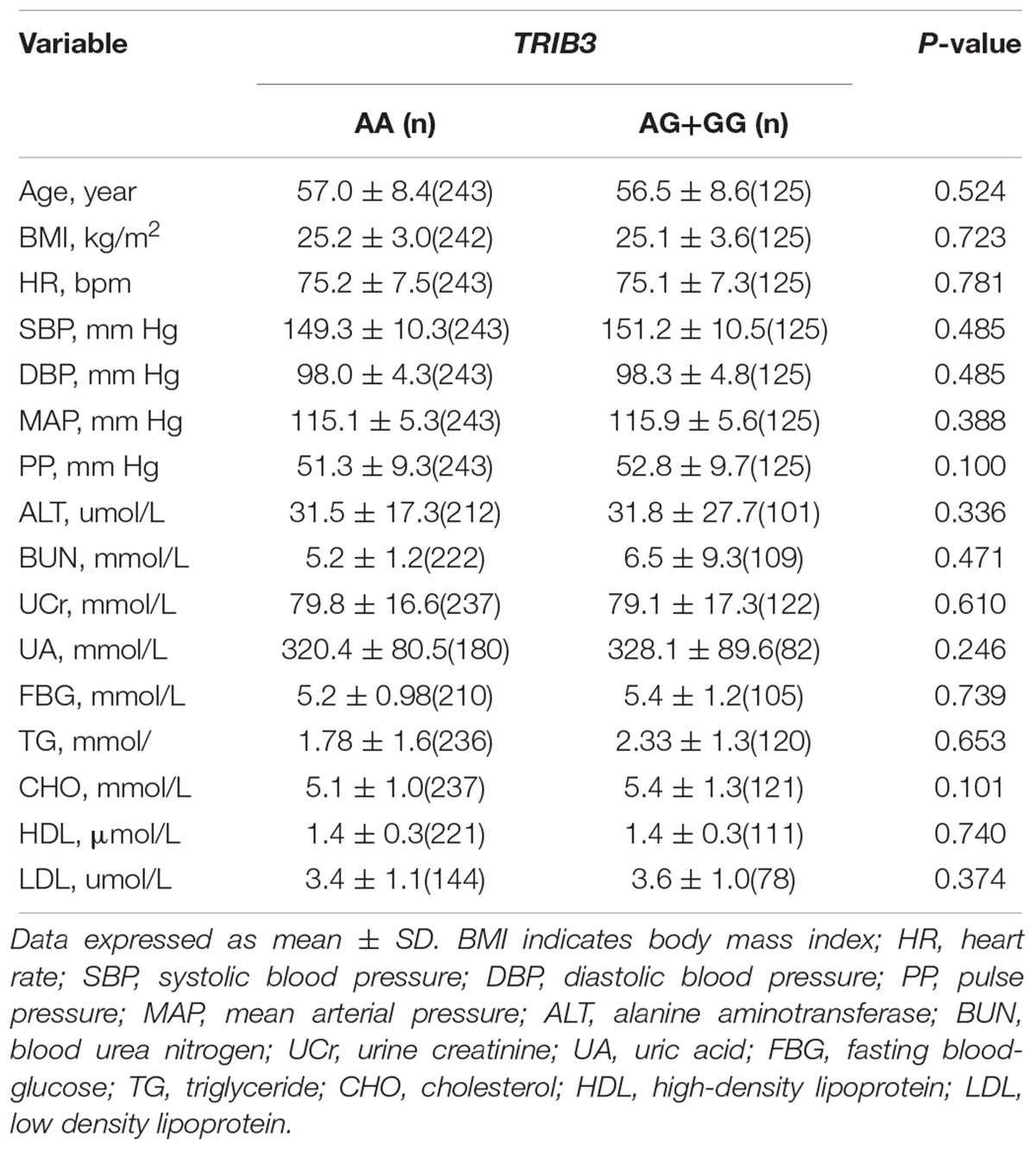
Table 2. Baseline characteristics of patients with essential hypertension stratified by TRIB3 genotype.
As shown in Figure 2A, the DBP-change and MAP-change from baseline response to TRIB3 (251, A > G) variant was significantly reduced (AA genotype compared to AG/GG genotype carriers) after CCBs administration. A similar tendency of DBP-change and MAP-change was found for imidapril (ACEI) treatment (Figure 2C), in which a marginally significant difference was achieved (P = 0.073 and 0.075, respectively). Inversely, DBP change from baseline after ARBs prescription was significantly increased for the AA genotype carriers compared to AG/GG genotype (Figure 2B). In the stratified analysis, there were significant differences in BP-change (blood pressure, include SBP or DBP or MAP) of AG/GG carriers between older and younger age or male and female (Supplementary Figures S1, S2). Nevertheless, no association between TRIB3 (251, A > G) genetic polymorphism and α-ADR or β-ADR drug response was observed in our study cohort (Figures 3A,B).
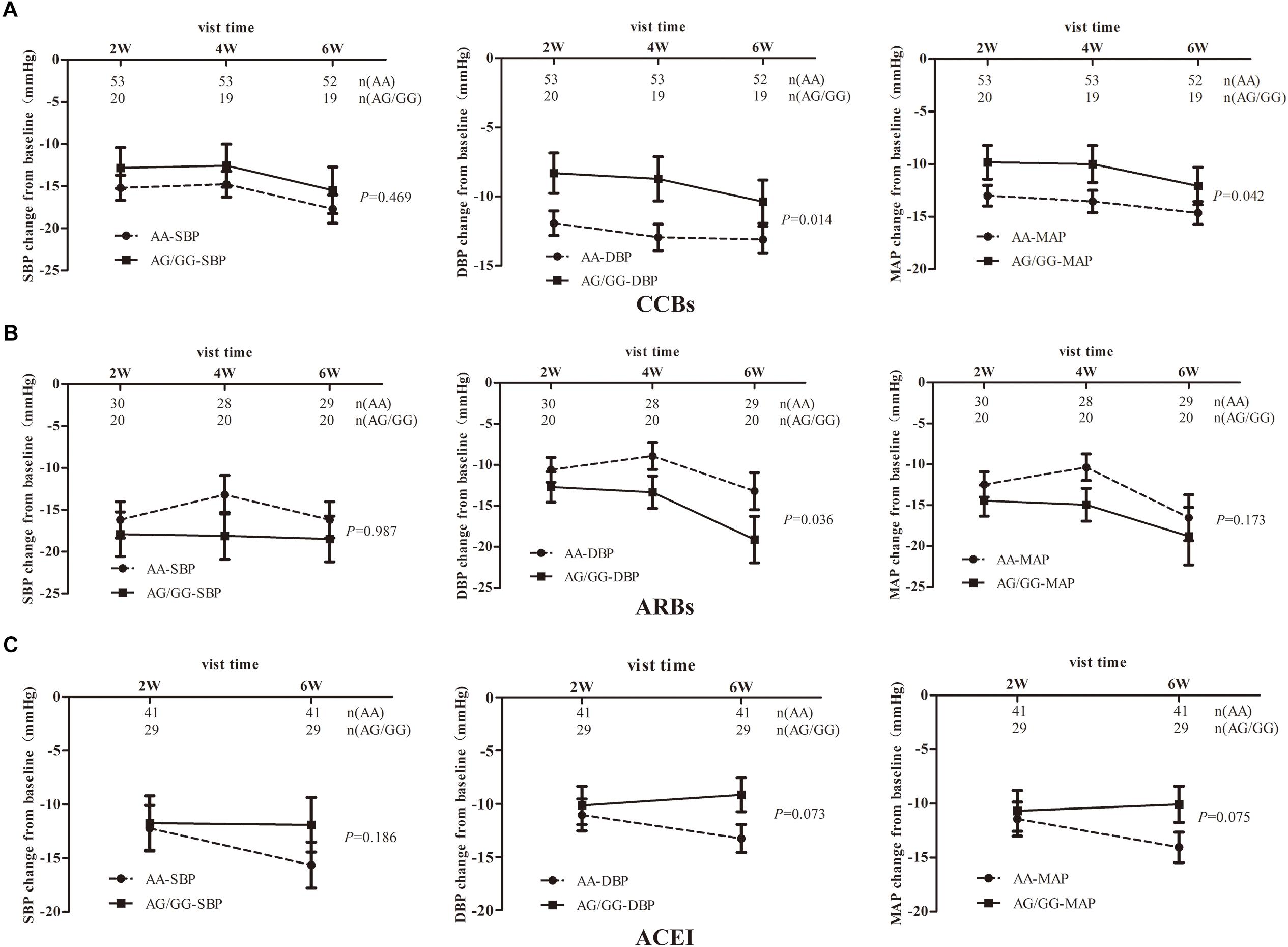
Figure 2. The relationship between TRIB3 (251, A > G) genetic polymorphism and the hypotensive effects of the antihypertensives monotherapy in EH patients. Panels (A–C) respectively depicts that BP-changes from baseline in EH patients carrying the TRIB3 (251, A > G) AA and AG/GG genotypes after treatment with the drugs of CCBs, ARBs and ACEIs for 6 weeks. P-value were calculated by the linear mixed model and adjusted for baseline age, BMI, gender, SBP, DBP, total cholesterol, heart rate, triglyceride, HDL, LDL, FBG and other biochemical factors appropriately. Error bar indicated 95% confidence interval.
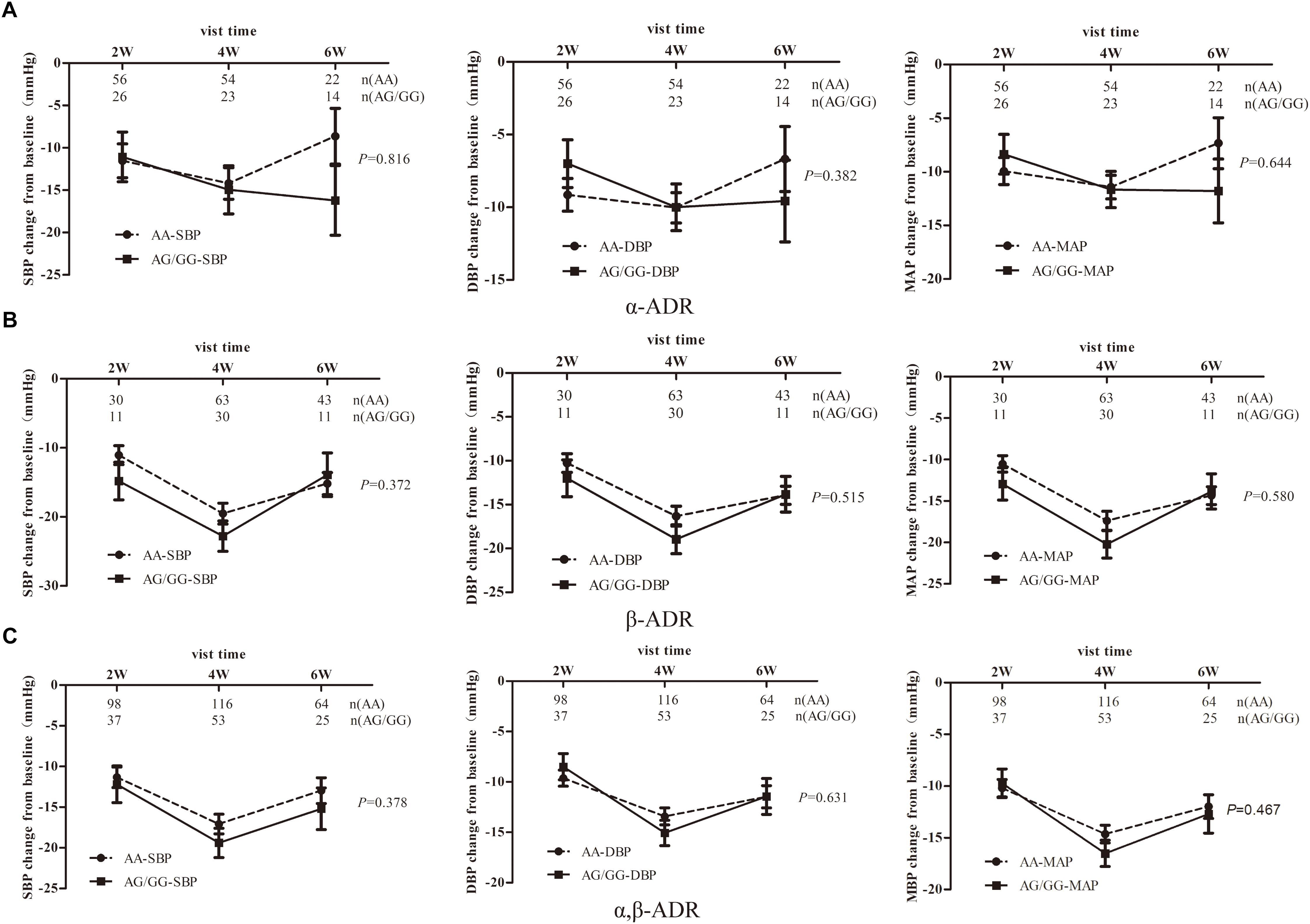
Figure 3. The relationship between TRIB3 (251, A > G) genetic polymorphism and the hypotensive effects of α,β-ADRs monotherapy in EH patients. Panels (A–C) respectively depicts that BP- changes from baseline in EH patients carrying the TRIB3 (251, A > G) AA and AG/GG genotypes after treatment with α-ADR, β-ADR and α, β-ADRs for 6 weeks. P-value were adjusted for baseline age, BMI, gender, SBP, DBP, total cholesterol, heart rate, triglyceride, HDL, LDL, FBG and other biochemical factors appropriately. Error bar indicated 95% confidence interval.
As studies showed that α, β-ADRs were all playing a role in the cAMP/cGMP/adrenalin signaling pathways to induce the transcription of eNOS in a time-dependent manner[18], we combined α, β-ADRs treatment groups in the analysis model. However, there was no significant change between AG/GG and AA genotype in the linear mixed model (Figure 3C). Stratified analysis was then used to explore the difference in SBP-, DBP-, MAP-change from baseline after α, β-ADRs therapy. In the sex stratification analysis, BP-change from baseline was significantly reduced for male compared to female in AG/GG genotype (Figure 4). And in the analysis of age stratification, we took 50,55,60 as the boundaries for analysis respectively, and found that 55 was the most appropriate cut-off value. The results showed that people with age younger than 55 years old had more significant antihypertensive effects in AG/GG genotype carriers (Figure 5).
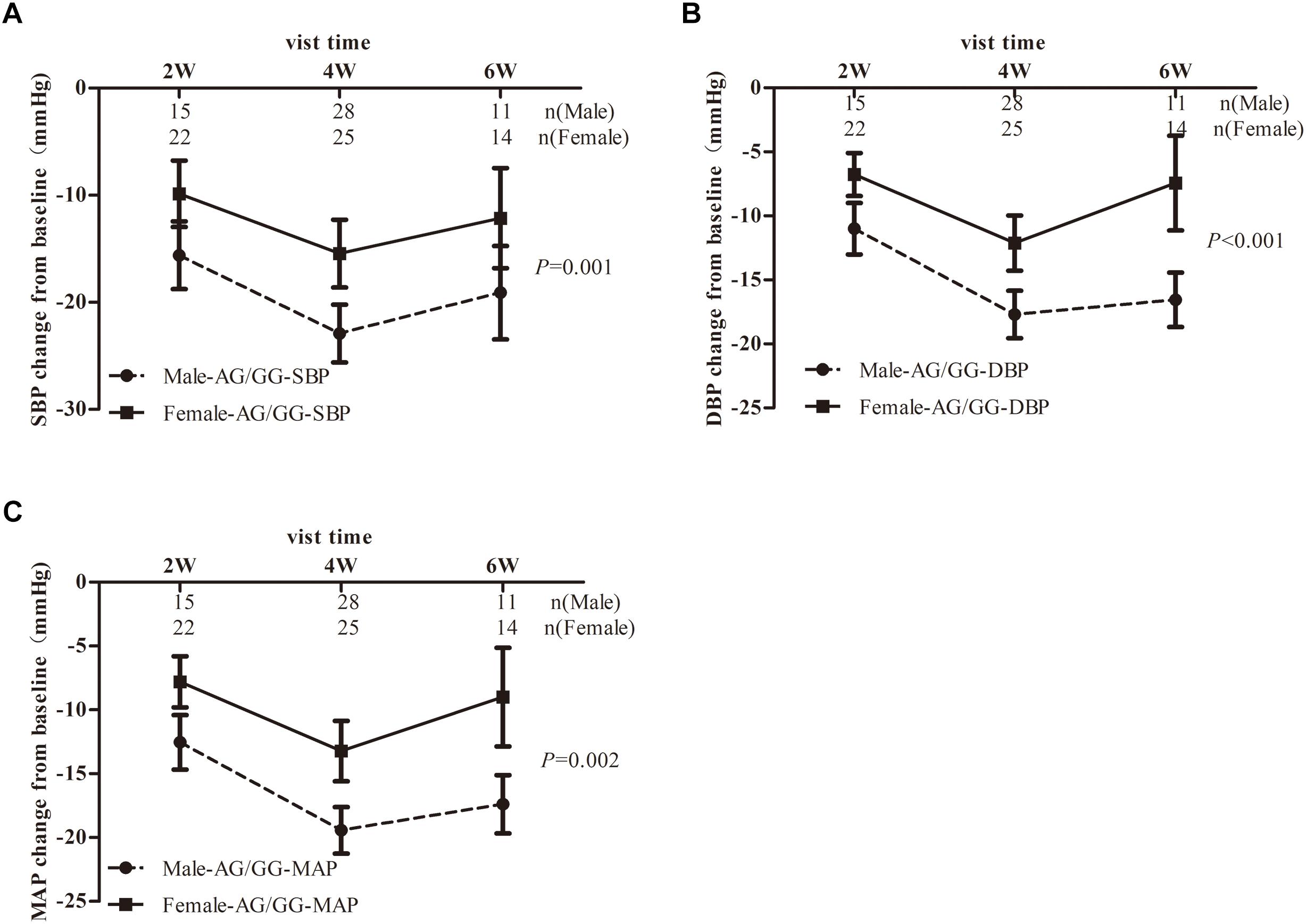
Figure 4. Blood pressure response to α,β-ADR blocker therapy in EH patients stratified by sex dependent of TRIB3 genotype. Panels (A–C) respectively depicts that SBP-, DBP-, MAP- changes from baseline in EH patients carrying the TRIB3 (251, A > G) AA and AG/GG genotypes after treatment with α, β-ADRs for 6 weeks. P-value were adjusted for baseline age, BMI, SBP, DBP, total cholesterol, heart rate, triglyceride, HDL, LDL, FBG and other biochemical factors appropriately. Error bar indicated 95% confidence interval.
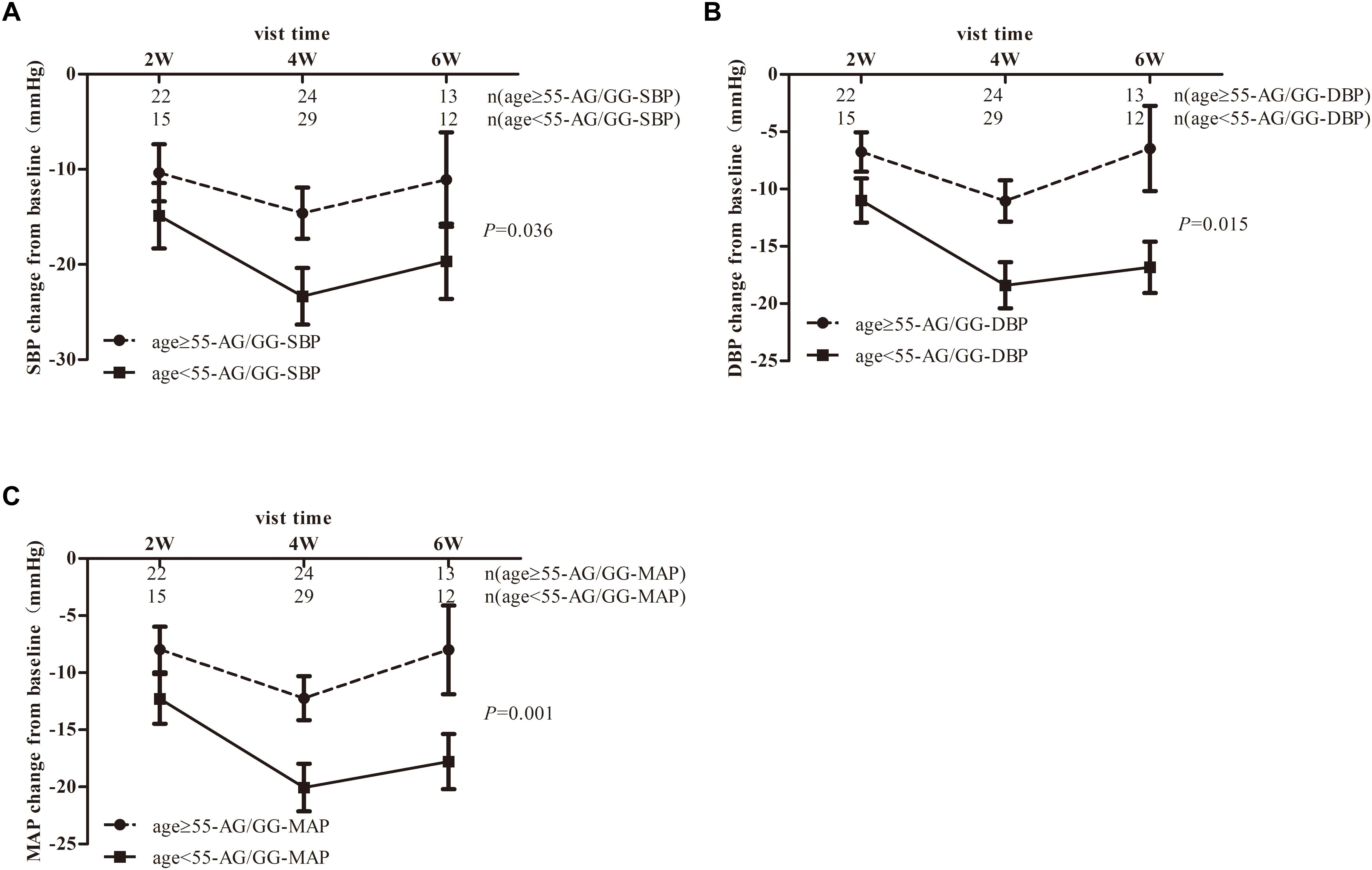
Figure 5. Blood pressure response to α,β-ADR blocker therapy in EH patients stratified by age-specific to TRIB3 genotype. Panels (A–C) respectively depicts that SBP-, DBP-, MAP- changes from baseline in EH patients carrying the TRIB3 (251, A > G) AA and AG/GG genotypes after treatment with α, β-ADRs for 6 weeks. P-value were adjusted for baseline BMI, gender, SBP, DBP, total cholesterol, heart rate, triglyceride, HDL, LDL, FBG and other biochemical factors appropriately. Error bar indicated 95% confidence interval. The stratification based on a boundary of age-55 showed the largest difference in blood pressure decrease after analysis of age-50, 55, 60.
In this study we showed that TRIB3 (251, A > G) genetic variation had a significant clinical relevance to the efficacy of certain class of antihypertensive drugs in individuals with EH treatment. It has been demonstrated that a better effect on BP response was observed in TRIB3 Q84R (rs2295490, 251 A > G) AA genotype carriers than AG/GG carriers after taking a routine dosage of ACEI and CCBs antihypertensives. After stratification analysis for age and sex, we found a more significant difference between these two genotype carriers. Studies have shown that CCBs and ACEI have an excellent antioxidant stress effect via increasing eNOS expression and NO synthesis (Kanno et al., 2001; Koyama et al., 2007). TRIB3, has been identified affecting insulin action by binding to and inhibiting Akt phosphorylation, which also regulated eNOS and NO. In human and mice, insulin can relax bladder via activating PI3K-AKT-eNOS pathway and lead to a three folds increase in NO synthesis than baseline in AA-but not in TRIB3 AG/GG genotype carriers (Leiria et al., 2013). Meanwhile, insulin had almost no effect on NO synthesis for AG/GG genotype carriers in human umbilical vein endothelial cells (Andreozzi et al., 2008). Taken together, our results are consistent with the deleterious role of TRIB3 G allele on NO production, which may lead to a weaker response to ACEI and CCBs antihypertensives.
On the contrary, a better response to ARBs was found on AG/GG genotype carriers than AA genotype carriers. This phenomenon may be interpreted as the different mechanisms of Angiotensin. The published literature has reported that Ang-(1-7) can elevate blood pressure by promoting pro-inflammatory and pro-thrombotic effects. Moreover, Ang IV can activate AT4R, and may contribute to cardiac damage (Ruiz-Ortega et al., 2007; Velkoska et al., 2011). Likewise, Yang et al. (2010) has demonstrated that Ang IV increased blood pressure and reduced renal blood flow through counteracting the presence of AT2 receptors in mice. Other studies revealed that Ang IV can ameliorate AngII-induced cardiac injury via AT4R and protect against acute cerebral ischemia via Ang IV-AT4R, NO-dependent mechanisms (Faure et al., 2006; Yang et al., 2011). As mentioned above, an Ang-(1-7) triggered mechanism involving AT1R-, AT4R-, mass receptors and cGMP-PKG-NO pathway may cause the different antihypertensive effect of ACEI and ARB among individuals induced by TRIB3 (251, A > G) genetic polymorphism. In addition, ARB could down-regulate TRIB3 mRNA level and a dual function of ARB on eNOS expression may also lead to the opposite relationship between TRIB3 G allele and antihypertensive effects of ACEI and ARBs (Zhang et al., 2006; Myojo et al., 2014).
In the ARB and ACEI treatment groups, we noticed that the difference in antihypertensive efficacy between different carriers of TRIB3 genotypes became more significant as time went on, which may be due to an increase in local eNOS mRNA expression and a decrease in angiotensin II in the LV, leading to the amelioration of myocardial remodeling in hypertensive condition (Kobayashi et al., 2000). Reversed results of ARBs were also shown in the sex stratification. In this drug treatment group, female of AA genotype but not those with G allele have stronger antihypertensive efficacy compared to male. In the treatment of ACEIs, older (age ≥ 55) patients with AA genotype have stronger antihypertensive efficacy compared to younger patients (age < 55). The specific mechanism needs more in-depth discussion and exploration.
In EH patients treated with α, β-ADRs, we did not observe significant difference of antihypertensive effect on response to TRIB3 genotypes. However, it is interesting to note that TRIB3 (251, A > G) variance was associated with α, β-ADRs monotherapy in Chinese population with EH in an age-dependent and sex-specific manner. And between the age groups and the sex groups, there is a significant difference in BP-change from baseline only limited to patients with TRIB3 (251, A > G) AG/GG genotype, while the mechanism is unclear. In addition, our study has shown that among G allele carriers, males or youngers are more likely to have a better antihypertensive effect (Figures 4, 5). This may be attributed to the inconsistent distribution of adrenoceptor in a sex-dependent manner. The regulation of estrogen may also result in greater adrenoceptor blocker reactivity in males than in females (Luksha et al., 2005; Al-Gburi et al., 2017). Researches showed that aging decreases cardiac beta-adrenergic responsiveness in model systems and in humans in vivo with multiple mechanisms including downregulation and decreased agonist binding of beta 1-receptors, uncoupling of beta 2-receptors, and abnormal G protein-mediated signal transduction (White et al., 1994).
Reduction in BP by 1–4 mm was also a question be worthy to think about, in the research of Lewington et al. (2002) a 2 mm Hg lower usual SBP was associated with approximately 10% lower stroke mortality and about 7% lower mortality from ischaemic heart disease or other vascular causes in middle age. In general, a 20 mm Hg difference in usual SBP is approximately equivalent in its hazards to a 10 mm Hg difference in usual DBP (Lewington et al., 2002). Therefore, we make hypothesis that for every 1 mm Hg reduction in diastolic blood pressure in the general normotensive population, the mortality rate of vascular-related events can be reduced by 7–10%. For patients with high blood pressure, a decrease of several mmHg of BP may not bring such a big benefit, but we can still assume the benefit exists.
In recent years it became evident that the vast majority of genetic variants in genes of importance for drug treatment are rare, with minor allele frequencies <1%. Also, recent approximations based on analyses of population-scale sequencing projects estimate that such rare variants account for 30–40% of the interindividual variability in drug response (Lauschke and Ingelman-Sundberg, 2018). Some low-frequency genetic variants detected by re-sequencing of TRIB3 can partially account for cardiovascular clinical outcomes in diabetes. But the association was especially strong among individuals who also carried the common R84 variant (Prudente et al., 2015). Other studies reported that the variation at 5′-untranslated region of the gene may have a strong impact on translational efficiency and serve an important function on gene expression regulating (Hughes, 2006). Several additional infrequent nonsynonymous single-nucleotide polymorphisms have been identified in the genomic region encompassing the human TRIB3 gene (dbSNP2) whose function and potential biological relevance have never, so far, been addressed. These may lead us to speculate that rare and common variants in TRIB3 may act together to alter drug efficacy.
Our study was a well-controlled drug clinical trial in which patients received monotherapy. Nevertheless, some limitations should be considered in the interpretation of our findings. On the one hand, diet habits, lifestyle factors may affect the antihypertensive effect of drugs. Such as a daily mean of 30 min of vigorous exercise, a DASH style diet, modest alcohol intake up to 10 g/day, non-narcotic analgesic use less than once per week, and intake of 400 μg/day or more of supplemental folic acid may lead to lower risk of hypertension (Forman et al., 2009). These factors also have the potential to make patients have a distinguishing antihypertensive effect. However, our results do not exclude the influence of these factors because of the lack of these information. On the other hand, polymorphisms of other genes may also be involved in the interaction between heredity and drug efficacy or affect vascular function (He et al., 2015; Shen et al., 2019).
In conclusion, the results of the present study suggest that the TRIB3 (251, A > G) polymorphism was associated with the response of antihypertensive drugs therapy in Chinese EH patients,. Although this data may prove TRIB3 (251, A > G) genetic variation is useful in clinical therapy, combining other genetic markers to identify individuals at high risk of cardiovascular abnormalities may bring a better clinical outcome. Further pharmacogenomics studies on TRIB3 merit attention.
JZ, FH, JL, LX, and WZ were responsible for the study design. JZ, FH, and BS were responsible for the experiments. JZ and FH did the data processing and statistical analysis. JZ, FH, and BS wrote and interpreted the manuscript. FH and BS were responsible for data management and contributed reagents and materials. RL, YG, HR, YS, XC, ZL, HZ, SD, and HX calibrated and discussed the manuscripts.
The work was supported by National Scientific Foundation of China (Nos. 81573511, 81874329, 81522048, and 81273595), the National Key R&D Plan (No. 2016YFC0905000), the ‘863’ Project (No. 2012AA02A518).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We are grateful to the Shanghai Institute of Hypertension in Ruijin Hospital for supporting our clinical trials. We also thank Dr. Tang jie for her advice on revision of language.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2019.00236/full#supplementary-material
FIGURE S1 | Blood pressure response to CCBs, ARBs, and ACEI therapy in EH patients stratified by age-specific to TRIB3 genotype. A–C respectively depicts that BP changes from baseline in EH patients carrying the TRIB3 (251, A>G) AA and AG/GG genotypes after treatment with CCBs, ARBs, and ACEI for 6 weeks respectively. P-value were adjusted for baseline BMI, sex, SBP, DBP, total cholesterol, heart rate, triglyceride, HDL, LDL, FBG, and other biochemical factors appropriately. Error bar indicated 95% confidence interval. The stratification based on a boundary of age-55 showed the largest difference in blood pressure decrease after analysis of age-50, 55, 60.
FIGURE S2 | Blood pressure response to CCBs, ARBs, and ACEI therapy in EH patients stratified by sex dependent of TRIB3 genotype. A–C respectively depicts that BP changes from baseline in EH patients carrying the TRIB3 (251, A>G) AA and AG/GG genotypes after treatment with CCBs, ARBs, and ACEI for 6 weeks respectively. P-value were adjusted for baseline age, BMI, SBP, DBP, total cholesterol, heart rate, triglyceride, HDL, LDL, FBG, and other biochemical factors appropriately. Error bar indicated 95% confidence interval.
Al-Gburi, S., Deussen, A., Zatschler, B., Weber, S., Künzel, S., El-Armouche, A., et al. (2017). Sex-difference in expression and function of beta-adrenoceptors in macrovessels: role of the endothelium. Basic Res. Cardiol. 112:29. doi: 10.1007/s00395-017-0617-2
Andreozzi, F., Formoso, G., Prudente, S., Hribal, M. L., Pandolfi, A., Bellacchio, E., et al. (2008). TRIB3 R84 variant is associated with impaired insulin-mediated nitric oxide production in human endothelial cells. Arterioscler. Thromb. Vasc. Biol. 28, 1355–1360. doi: 10.1161/atvbaha.108.162883
Chan, M. C., Nguyen, P. H., Davis, B. N., Ohoka, N., Hayashi, H., Du, K., et al. (2007). A novel regulatory mechanism of the bone morphogenetic protein (BMP) signaling pathway involving the carboxyl-terminal tail domain of BMP type II receptor. Mol. Cell Biol. 27, 5776–5789. doi: 10.1128/mcb.00218-07
Chan, M. C., Weisman, A. S., Kang, H., Nguyen, P. H., Hickman, T., Mecker, S. V., et al. (2011). The amiloride derivative phenamil attenuates pulmonary vascular remodeling by activating NFAT and the bone morphogenetic protein signaling pathway. Mol. Cell Biol. 31, 517–530. doi: 10.1128/mcb.00884-10
Chen, R., Iwai, M., Wu, L., Suzuki, J., Min, L. J., Shiuchi, T., et al. (2003). Important role of nitric oxide in the effect of angiotensin-converting enzyme inhibitor imidapril on vascular injury. Hypertension 42, 542–547. doi: 10.1161/01.hyp.0000092440.52239.39
Chen, Y. L., Pan, A. W., Hsiung, P. C., Chung, L., Lai, J. S., Shur-Fen, Gau S, et al. (2015). Life adaptation skills training (LAST) for persons with depression: a randomized controlled study. J. Affect. Disord. 185, 108–114. doi: 10.1016/j.jad.2015.06.022
Cui, A. D., Gai, N. N., Zhang, X. H., Jia, K. Z., Yang, Y. L., and Song, Z. J. (2012). Decreased serum obestatin consequent upon TRIB3 Q84R polymorphism exacerbates carotid atherosclerosis in subjects with metabolic syndrome. Diabetol. Metab. Syndr. 4:52. doi: 10.1186/1758-5996-4-52
Du, K., Herzig, S., Kulkarni, R. N., and Montminy, M. (2003). TRB3: a tribbles homolog that inhibits Akt/PKB activation by insulin in liver. Science 300, 1574–1577. doi: 10.1126/science.1079817
Faure, S., Chapot, R., Tallet, D., Javellaud, J., Achard, J. M., and Oudart, N. (2006). Cerebroprotective effect of angiotensin IV in experimental ischemic stroke in the rat mediated by AT(4) receptors. J. Physiol. Pharmacol. 57, 329–342.
Fischer, Z., Das, R., Shipman, A., Fan, J. Y., Pence, L., Bouyain, S., et al. (2017). A Drosophila model of insulin resistance associated with the human TRIB3 Q/R polymorphism. Dis. Model. Mech. 10, 1453–1464. doi: 10.1242/dmm.030619
Forman, J. P., Stampfer, M. J., and Curhan, G. C. (2009). Diet and lifestyle risk factors associated with incident hypertension in women. JAMA 302, 401–411. doi: 10.1001/jama.2009.1060
Formoso, G., Di, Tomo P, Andreozzi, F., Succurro, E., Di Silvestre, S., Prudente, S., et al. (2011). The TRIB3 R84 variant is associated with increased carotid intima-media thickness in vivo and with enhanced MAPK signalling in human endothelial cells. Cardiovasc. Res. 89, 184–192. doi: 10.1093/cvr/cvq255
Gong, H. P., Wang, Z. H., Jiang, H., Fang, N. N., Li, J. S., Shang, Y. Y., et al. (2009). TRIB3 functional Q84R polymorphism is a risk factor for metabolic syndrome and carotid atherosclerosis. Diabetes Care 32, 1311–1313. doi: 10.2337/dc09-0061
He, F., Liu, M., Chen, Z., Liu, G., Wang, Z., Liu, R., et al. (2016). Assessment of human tribbles homolog 3 genetic variation (rs2295490) effects on type 2 diabetes patients with glucose control and blood pressure lowering treatment. EBioMedicine 13, 181–189. doi: 10.1016/j.ebiom.2016.10.025
He, F., Luo, J., Zhang, Z., Luo, Z., Fan, L., He, Y., et al. (2015). The RGS2 (-391, C > G) genetic variation correlates to antihypertensive drug responses in Chinese patients with essential hypertension. PLoS One 10:e0121483. doi: 10.1371/journal.pone.0121483
He, F., Shu, Y., Wang, X., Liu, X., Liu, G., Chen, Z., et al. (2018). Intensive glucose control reduces the risk effect of TRIB3, SMARCD3, and ATF6 genetic variation on diabetic vascular complications. Front. Pharmacol. 9:1422. doi: 10.3389/fphar.2018.01422
Hughes, T. A. (2006). Regulation of gene expression by alternative untranslated regions. Trends Genet 22, 119–122. doi: 10.1016/j.tig.2006.01.001
Kanno, S., Wu, Y. J., Lee, P. C., Billiar, T. R., and Ho, C. (2001). Angiotensin-converting enzyme inhibitor preserves p21 and endothelial nitric oxide synthase expression in monocrotaline-induced pulmonary arterial hypertension in rats. Circulation 104, 945–950. doi: 10.1161/hc3401.093155
Kim, S., Hata, A., and Kang, H. (2014). Down-regulation of miR-96 by bone morphogenetic protein signaling is critical for vascular smooth muscle cell phenotype modulation. J. Cell Biochem. 115, 889–895. doi: 10.1002/jcb.24730
Kimura, Y., Hirooka, Y., Sagara, Y., and Sunagawa, K. (2007). Long-acting calcium channel blocker, azelnidipine, increases endothelial nitric oxide synthase in the brain and inhibits sympathetic nerve activity. Clin. Exp. Hypertens. 29, 13–21. doi: 10.1080/10641960601096745
Kiss-Toth, E., Bagstaff, S. M., Sung, H. Y., Jozsa, V., Dempsey, C., Caunt, J. C., et al. (2004). Human tribbles, a protein family controlling mitogen-activated protein kinase cascades. J. Biol. Chem. 279, 42703–42708. doi: 10.1074/jbc.M407732200
Kobayashi, N., Hara, K., Watanabe, S., Higashi, T., and Matsuoka, H. (2000). Effect of imidapril on myocardial remodeling in L-NAME–induced hypertensive rats is associated with gene expression of NOS and ACE mRNA. Am. J. Hypertens. 13, 199–207. doi: 10.1016/S0895-7061(99)00117-X
Kobayashi, N., Mita, S., Yoshida, K., Honda, T., Kobayashi, T., Hara, K., et al. (2003). Celiprolol activates eNOS through the PI3K-Akt pathway and inhibits VCAM-1 Via NF-κB induced by oxidative stress. Hypertension 42, 1004–1013. doi: 10.1161/01.hyp.0000097547.35570.70
Koyama, Y., Takeishi, Y., Takahashi, H., Shishido, T., Arimoto, T., Niizeki, T., et al. (2007). Azelnidipine inhibits H2O2-induced cell death in neonatal rat cardiomyocytes. Cardiovasc. Drugs Ther. 21, 69–72. doi: 10.1007/s10557-007-6008-4
Lauschke, V. M., and Ingelman-Sundberg, M. (2018). How to consider rare genetic variants in personalized drug therapy. Clin. Pharmacol. Ther. 103, 745–748. doi: 10.1002/cpt.976
Leiria, L. O., Sollon, C., Báu, F. R., Mónica, F. Z., D’Ancona, C. L., De Nucci, G., et al. (2013). Insulin relaxes bladder via PI3K/AKT/eNOS pathway activation in mucosa: unfolded protein response-dependent insulin resistance as a cause of obesity-associated overactive bladder. J. Physiol. 591, 2259–2273. doi: 10.1113/jphysiol.2013.251843
Lewington, S., Clarke, R., Qizilbash, N., Peto, R., and Collins, R. (2002). Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 360, 1903–1913. doi: 10.1016/S0140-6736(02)11911-8
Luksha, L., Poston, L., Gustafsson, J. A., Aghajanova, L., and Kublickiene, K. (2005). Gender-specific alteration of adrenergic responses in small femoral arteries from estrogen receptor-beta knockout mice. Hypertension 46, 1163–1168. doi: 10.1161/01.HYP.0000185648.48498.c1
Messerli, F. H., Williams, B., and Ritz, E. (2007). Essential hypertension. Lancet 370, 591–603. doi: 10.1016/s0140-6736(07)61299-9
Myojo, M., Nagata, D., Fujita, D., Kiyosue, A., Takahashi, M., Satonaka, H., et al. (2014). Telmisartan activates endothelial nitric oxide synthase via Ser1177 phosphorylation in vascular endothelial cells. PLoS One 9:e96948. doi: 10.1371/journal.pone.0096948
Patel, A., Advance Collaborative Group, MacMahon, S., Chalmers, J., Neal, B., Woodward, M., et al. (2007). Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): a randomised controlled trial. Lancet 370, 829–840. doi: 10.1016/s0140-6736(07)61303-8
Prudente, S., Bailetti, D., Mendonca, C., Mannino, G. C., Fontana, A., Andreozzi, F., et al. (2015). Infrequent TRIB3 coding variants and coronary artery disease in type 2 diabetes. Atherosclerosis 242, 334–339. doi: 10.1016/j.atherosclerosis.2015.07.030
Prudente, S., Hribal, M. L., Flex, E., Turchi, F., Morini, E., De Cosmo, S., et al. (2005). The functional Q84R polymorphism of mammalian Tribbles homolog TRB3 is associated with insulin resistance and related cardiovascular risk in Caucasians from Italy. Diabetes 54, 2807–2811. doi: 10.2337/diabetes.54.9.2807
Prudente, S., and Trischitta, V. (2015). The TRIB3 Q84R polymorphism, insulin resistance and related metabolic alterations. Biochem. Soc. Trans. 43, 1108–1111. doi: 10.1042/bst20150115
Qin, R. R., Song, M., Li, Y. H., Wang, F., Zhou, H. M., Liu, M. H., et al. (2017). Association of increased serum sema3E with TRIB3 Q84R polymorphism and carotid atherosclerosis in metabolic syndrome. Ann. Clin. Lab. Sci. 47, 47–51.
Ruiz-Ortega, M., Esteban, V., and Egido, J. (2007). The regulation of the inflammatory response through nuclear factor-kappab pathway by angiotensin IV extends the role of the renin angiotensin system in cardiovascular diseases. Trends Cardiovasc. Med. 17, 19–25. doi: 10.1016/j.tcm.2006.10.003
Shen, J., Liu, M., Xu, J., Sun, B., Xu, H., and Zhang, W. (2019). ARL15 overexpression attenuates high glucose-induced impairment of insulin signaling and oxidative stress in human umbilical vein endothelial cells. Life Sci. 220, 127–135. doi: 10.1016/j.lfs.2019.01.030
Stojkov, N. J., Baburski, A. Z., Bjelic, M. M., Sokanovic, S. J., Mihajlovic, A. I., Drljaca, D. M., et al. (2014). In vivo blockade of alpha1-adrenergic receptors mitigates stress-disturbed cAMP and cGMP signaling in Leydig cells. Mol. Hum. Reprod. 20, 77–88. doi: 10.1093/molehr/gat052
Stojkov, N. J., Janjic, M. M., Kostic, T. S., and Andric, S. A. (2013). Orally applied doxazosin disturbed testosterone homeostasis and changed the transcriptional profile of steroidogenic machinery, cAMP/cGMP signalling and adrenergic receptors in Leydig cells of adult rats. Andrology 1, 332–347. doi: 10.1111/j.2047-2927.2012.00035.x
Sun, B., He, F., Sun, L., Zhou, J., Shen, J., Xu, J., et al. (2019). Cause-specific risk of major adverse cardiovascular outcomes and hypoglycemic in patients with type 2 diabetes: a multicenter prospective cohort study. Endocrine 63, 44–51. doi: 10.1007/s12020-018-1715-0
Velkoska, E., Dean, R. G., Griggs, K., Burchill, L., and Burrell, L. M. (2011). Angiotensin-(1-7) infusion is associated with increased blood pressure and adverse cardiac remodelling in rats with subtotal nephrectomy. Clin. Sci. 120, 335–345. doi: 10.1042/cs20100280
Wain, L. V., Verwoert, G. C., O’Reilly, P. F., Shi, G., Johnson, T., Johnson, A. D., et al. (2011). Genome-wide association study identifies six new loci influencing pulse pressure and mean arterial pressure. Nat. Genet. 43, 1005–1011. doi: 10.1038/ng.922
West, J., Fagan, K., Steudel, W., Fouty, B., Lane, K., Harral, J., et al. (2004). Pulmonary hypertension in transgenic mice expressing a dominant-negative BMPRII gene in smooth muscle. Circ. Res. 94, 1109–1114. doi: 10.1161/01.res.0000126047.82846.20
White, M., Roden, R., Minobe, W., Khan, M. F., Larrabee, P., Wollmering, M., et al. (1994). Age-related changes in beta-adrenergic neuroeffector systems in the human heart. Circulation 90, 1225–1238. doi: 10.1161/01.CIR.90.3.1225
Yang, H., Zeng, X. J., Wang, H. X., Zhang, L. K., Dong, X. L., Guo, S., et al. (2011). Angiotensin IV protects against angiotensin II-induced cardiac injury via AT4 receptor. Peptides 32, 2108–2115. doi: 10.1016/j.peptides.2011.09.015
Yang, R., Walther, T., Gembardt, F., Smolders, I., Vanderheyden, P., Albiston, A. L., et al. (2010). Renal vasoconstrictor and pressor responses to angiotensin IV in mice are AT1a-receptor mediated. J. Hypertens. 28, 487–494. doi: 10.1097/HJH.0b013e3283343250
Yu, Q., Gao, F., and Ma, X. L. (2011). Insulin says NO to cardiovascular disease. Cardiovasc. Res. 89, 516–524. doi: 10.1093/cvr/cvq349
Zhang, W., Yang, Z., Li, X., Wen, J., Zhang, H., Wang, S., et al. (2015). The functional Q84R polymorphism of TRIB3 gene is associated with diabetic nephropathy in Chinese type 2 diabetic patients. Gene 555, 357–361. doi: 10.1016/j.gene.2014.11.031
Zhang, W., Zhong, M., Tang, M. X., Ma, X., Miao, Y., Sun, H., et al. (2006). Effect of valsartan on Tribble 3 gene expression in rats with experimental diabetic cardiomyopathy. Zhonghua Xin Xue Guan Bing Za Zhi 34, 212–216.
Keywords: TRIB3, rs2295490, polymorphism, antihypertensive agents, essential hypertension
Citation: Zhou J, He F, Sun B, Liu R, Gao Y, Ren H, Shu Y, Chen X, Liu Z, Zhou H, Deng S, Xu H, Li J, Xu L and Zhang W (2019) Polytropic Influence of TRIB3 rs2295490 Genetic Polymorphism on Response to Antihypertensive Agents in Patients With Essential Hypertension. Front. Pharmacol. 10:236. doi: 10.3389/fphar.2019.00236
Received: 03 December 2018; Accepted: 26 February 2019;
Published: 27 March 2019.
Edited by:
Tracy A. O’Mara, QIMR Berghofer Medical Research Institute, AustraliaReviewed by:
Volker Martin Lauschke, Karolinska Institutet (KI), SwedenCopyright © 2019 Zhou, He, Sun, Liu, Gao, Ren, Shu, Chen, Liu, Zhou, Deng, Xu, Li, Xu and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wei Zhang, eWpzZDIwMDNAMTYzLmNvbQ== Jianmin Li, TGVvNzgwMzA3QHNpbmEuY29t Linyong Xu, eHlibXNAMTYzLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.