 Winnie de Bruijn1
Winnie de Bruijn1 Cristina Ibáñez2
Cristina Ibáñez2 Pia Frisk3
Pia Frisk3 Hanne Bak Pedersen4
Hanne Bak Pedersen4 Ali Alkan5Patricia Vella Bonanno6Ljiljana S. Brkičić7
Ali Alkan5Patricia Vella Bonanno6Ljiljana S. Brkičić7 Anna Bucsics8Guillaume Dedet9Jaran Eriksen10Joseph O. Fadare11Jurij Fürst12Gisselle Gallego13,14Isabella P. Godói15,16Augusto A. Guerra Júnior15,16Hakkı Gürsöz5Saira Jan17,18Jan Jones19
Anna Bucsics8Guillaume Dedet9Jaran Eriksen10Joseph O. Fadare11Jurij Fürst12Gisselle Gallego13,14Isabella P. Godói15,16Augusto A. Guerra Júnior15,16Hakkı Gürsöz5Saira Jan17,18Jan Jones19 Roberta Joppi20Saim Kerman5Ott Laius21
Roberta Joppi20Saim Kerman5Ott Laius21 Newman Madzikwa22
Newman Madzikwa22 Einar Magnússon23Mojca Maticic24Vanda Markovic-Pekovic25,26
Einar Magnússon23Mojca Maticic24Vanda Markovic-Pekovic25,26 Amos Massele27Olayinka Ogunleye28,29
Amos Massele27Olayinka Ogunleye28,29 Aisling O'Leary30Jutta Piessnegger31
Aisling O'Leary30Jutta Piessnegger31 Catherine Sermet32
Catherine Sermet32 Steven Simoens33Celda Tiroyakgosi34Ilse Truter35Magnus Thyberg36Kristina Tomekova37Magdalena Wladysiuk38Sotiris Vandoros39
Steven Simoens33Celda Tiroyakgosi34Ilse Truter35Magnus Thyberg36Kristina Tomekova37Magdalena Wladysiuk38Sotiris Vandoros39 Elif H. Vural5
Elif H. Vural5 Corinne Zara2
Corinne Zara2 Brian Godman10,40*
Brian Godman10,40*
- 1Department of Pharmaceutical Sciences, Utrecht University, Utrecht, Netherlands
- 2Catalan Health Service - Servei Català de la Salut, Barcelona, Spain
- 3Public Health Services Committee, Stockholm County Council, Stockholm, Sweden
- 4Health Technologies and Pharmaceuticals, Division of Health Systems and Public Health, WHO Regional Office for Europe, Copenhagen, Denmark
- 5Turkish Medicines and Medical Devices Agency, Ministry of Health, Ankara, Turkey
- 6Independent Pharmaceutical Consultant, Mellieha, Malta
- 7Croatian Health Insurance Fund, Zagreb, Croatia
- 8Department of Finance, University of Vienna, Vienna, Austria
- 9Ministry of Health, Paris, France
- 10Division of Clinical Pharmacology, Department of Laboratory Medicine, Karolinska Institutet, Karolinska University Hospital Huddinge, Stockholm, Sweden
- 11Department of Pharmacology, Ekiti State University, Ado-Ekiti, Nigeria
- 12Health Insurance Institute, Ljubljana, Slovenia
- 13School of Medicine, The University of Notre Dame Australia, Darlinghurst, NSW, Australia
- 14Department of Pharmacology and Clinical Neuroscience, Umea University, Umea, Sweden
- 15School of Pharmacy, Graduate Program in Medicines and Pharmaceutical Assistance, Federal University of Minas Gerais, Belo Horizonte, Brazil
- 16Department of Social Pharmacy, SUS Collaborating Centre – Health Technology Assessment and Excellence in Health, College of Pharmacy, Federal University of Minas Gerais, Belo Horizonte, Brazil
- 17Clinical Pharmacy, Rutgers State University of New Jersey, Piscataway, NJ, USA
- 18Horizon Blue Cross Blue Shield of New Jersey, Newark, NJ, USA
- 19Scottish Medicines Consortium, Glasgow, UK
- 20Pharmaceutical Drug Department, Azienda Sanitaria Locale of Verona, Verona, Italy
- 21State Agency of Medicines, Tartu, Estonia
- 22Ministry of Health and Child Care, Harrare, Zimbabwe
- 23Department of Health Services, Ministry of Health, Reykjavík, Iceland
- 24Clinic for Infectious Diseases and Febrile Illnesses, University Medical Centre Ljubljana, Ljubljana, Slovenia
- 25Faculty of Medicine, University of Banja Luka, Banja Luka, Bosnia and Herzegovina
- 26Ministry of Health and Social Welfare, Banja Luka, Bosnia and Herzegovina
- 27Department of Clinical Pharmacology, School of Medicine, University of Botswana, Gaborone, Botswana
- 28Clinical Pharmacology Unit, Department of Medicine, Lagos State University Teaching Hospital, Lagos, Nigeria
- 29Department of Pharmacology and Therapeutics, Lagos State University College of Medicine, Lagos, Nigeria
- 30National Centre for Pharmacoeconomics, Dublin, Ireland
- 31Hauptverband der Österreichischen Sozialversicherungsträger, Wien, Austria
- 32IRDES, Paris, France
- 33Department of Pharmaceutical and Pharmacological Sciences, KU Leuven, Leuven, Belgium
- 34Ministry of Health, Nelson Mandela Drive, Gaborone, Botswana
- 35Drug Utilisation Research Unit, Faculty of Health Sciences, Nelson Mandela Metropolitan University, Port Elizabeth, South Africa
- 36Stockholms Läns Landsting, Hälso-och Sjukvårdsförvaltningen, Stockholm, Sweden
- 37Faculty of Management, Comenius University, Bratislava, Slovakia
- 38HTA Consulting, Cracow, Poland
- 39School of Management and Business, King's College London, London, UK
- 40Strathclyde Institute of Pharmacy and Biomedical Sciences, University of Strathclyde, Glasgow, UK
Background: Infection with the Hepatitis C Virus (HCV) is a widespread transmittable disease with a diagnosed prevalence of 2.0%. Fortunately, it is now curable in most patients. Sales of medicines to treat HCV infection grew 2.7% per year between 2004 and 2011, enhanced by the launch of the protease inhibitors (PIs) boceprevir (BCV) and telaprevir (TVR) in addition to ribavirin and pegylated interferon (pegIFN). Costs will continue to rise with new treatments including sofosbuvir, which now include interferon free regimens.
Objective: Assess the uptake of BCV and TVR across Europe from a health authority perspective to offer future guidance on dealing with new high cost medicines.
Methods: Cross-sectional descriptive study of medicines to treat HCV (pegIFN, ribavirin, BCV and TVR) among European countries from 2008 to 2013. Utilization measured in defined daily doses (DDDs)/1000 patients/quarter (DIQs) and expenditure in Euros/DDD. Health authority activities to influence treatments categorized using the 4E methodology (Education, Engineering, Economics and Enforcement).
Results: Similar uptake of BCV and TVR among European countries and regions, ranging from 0.5 DIQ in Denmark, Netherlands and Slovenia to 1.5 DIQ in Tayside and Catalonia in 2013. However, different utilization of the new PIs vs. ribavirin indicates differences in dual vs. triple therapy, which is down to factors including physician preference and genotypes. Reimbursed prices for BCV and TVR were comparable across countries.
Conclusion: There was reasonable consistency in the utilization of BCV and TVR among European countries in comparison with other high priced medicines. This may reflect the social demand to limit the transmission of HCV. However, the situation is changing with new curative medicines for HCV genotype 1 (GT1) with potentially an appreciable budget impact. These concerns have resulted in different prices across countries, with their impact on budgets and patient outcomes monitored in the future to provide additional guidance.
Introduction
The incidence and prevalence of patients with hepatitis C virus (HCV) infection is growing. However, the true worldwide incidence remains unknown due to heterogeneous registration and case definitions (European Centre for Desease Prevention Control, 2010). Overall, it is believed that the diagnosed global prevalence of HCV is approximately 2.0% (1.7–2.3%) for adults, which corresponds to approximately 104 (87–124) million persons world-wide (Table 1; McGowan et al., 2013; Mohd Hanafiah et al., 2013; European Association for the Study of the Liver, 2014; Hope et al., 2014; Wedemeyer et al., 2015). Others have suggested higher figures at 2.8% globally (Lemoine and Asia, 2014), leading to estimated prevalence rates of 150–184 million world-wide (Ramachandran et al., 2012; Mohd Hanafiah et al., 2013; Lemoine and Asia, 2014; Phelan and Cook, 2014; Barua et al., 2015; Cure et al., 2015; Norton, 2015; Fraser et al., 2016), with approximately 85% of patients living in low to middle income (LMIC) countries (Phelan and Cook, 2014). However, estimated figures for South Africa are lower at 0.1–1.7% (Fraser et al., 2016). In 2013, diagnosis rates vs. the estimated prevalence rates varied from 81% in Sweden and 43% in Belgium to just 16% in Turkey (Table 1; Dore et al., 2014; Wedemeyer et al., 2015).
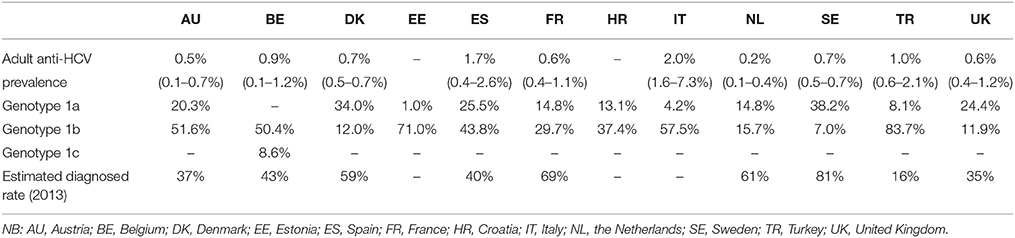
Table 1. Reported anti-HCV prevalence rates (adjusted for the adult population), genotype 1 (GT1) distribution and estimated diagnose and treatment rate (Dore et al., 2014; Gower et al., 2014; Hope et al., 2014; Wedemeyer et al., 2015).
Annually up to 0.5 million people die from the consequences of chronic hepatitis C infection, mainly in Africa, Asia and Eastern Europe (Lozano et al., 2012). Most people are unaware of their HCV infection due to the slow progress of the disease (Yehia et al., 2014), with sequelae of chronic hepatitis potentially appearing up to 20–30 years later. These include liver cirrhosis, which occurs in 10–20% of patients with hepatitis C, and develops into a 1–5% annual risk of hepatocellular carcinoma and 3–6% annual risk of hepatic decompensation (Thein et al., 2008; Westbrook and Dusheiko, 2014). In 2012, cirrhosis of the liver was the tenth leading cause of death in LMIC countries (globally the twelfth leading cause), with liver cancer the ninth leading cause of death in upper-middle-income countries (globally the sixteenth leading cause) (World Health Organisation, 2012; Lemoine and Asia, 2014).
Until 2011, treatment choices and their effectiveness were limited, especially for patients with genotype 1 (GT1). GT1 HCV-patients account for up to 60% of HCV infections worldwide, and predominate in Eastern, Northern and Southern Europe as well as North America and Japan (Schalm et al., 1997; McHutchison et al., 1998; Poynard et al., 1998; Cebolla and Björnberg, 2012; Messina et al., 2014). Cure rates, defined as sustained virological response (SVR), were typically only seen in 35–43% of patients with GT1 following dual therapy with ribavirin and pegylated interferons (pegIFNs) (Schalm et al., 1997; McHutchison et al., 1998; Poynard et al., 1998; Manns et al., 2013; Mathurin, 2013; Chou et al., 2014; Kohli et al., 2014). However, the serious side-effects associated with these treatments, coupled with complex regimens, resulted in problems with adherence. This led to less than 50% of patients typically completing their treatment course (McHutchison et al., 2002; Lo Re et al., 2011; Brennan and Shrank, 2014).
In 2011, the direct acting antivirals (DAAs) boceprevir (BCV), and telaprevir (TVR) became available (Chou et al., 2014)1,2. BCV and TVR are only licensed for GT1. Consequently physicians need to test for genotypes before starting treatment1, 2. BCV and TVR improved SVR (RR, 2.05; 95% CI 1.70–2.48) when combined with ribavirin and pegIFNs (triple therapy) (Chou et al., 2014; Kohli et al., 2014; Manzano-Robleda et al., 2015)3; however, there were more adverse events (RR, 1.05; 1–1.03; NNH 77.59) (Manzano-Robleda et al., 2015). In recent years, second generation DAAs have become available with encouraging cure rates up to 90–95% of patients, potentially providing shorter treatment courses and less side effects than previous treatment approaches (Kohli et al., 2014; Childs-Kean and Hand, 2015)3. These were sofosbuvir, simeprevir, daclatasvir and ledipasvir approved by the European Medicine Agency (EMA) in late 2013 and 20144,5,6,7. More recently, combinations of DAAs have also been approved by EMA providing further options for highly effective, safe and well tolerated treatment of HCV GT1 patients (Kohli et al., 2014)8.
These developments resulted in the anti HCV therapeutics market expanding at a compounded annual growth rate (CAGR) of 2.7% between 2004 and 20119,10, with growth rates appreciably higher after this10. This has resulted in worldwide sales of sofosbuvir already at US$12.4 billion in 2014 (Trooskin et al., 2015). In the US, treatments for hepatitis C became the fourth most expensive speciality medicine class in 2014 with sofosbuvir already capturing 37.5% of the HCV market11. These growth rates in expenditure are due not only to the price of these new treatments at over US$50,000/patient/course in some countries, but also the effectiveness and limited side-effects of the second generation DAAs (Mohd Hanafiah et al., 2013; Brennan and Shrank, 2014; Senior, 2014). In addition, these new treatments are being used in patients with advanced liver disease, such as those with decompensated cirrhosis awaiting transplantation, appreciably increasing the pool of eligible patients.
We are already seeing that some European health authorities are unable to fund new high priced medicines, exacerbated by their continual launch (Experts in Chronic Myeloid Leukemia, 2013; Kantarjian et al., 2013; Godman et al., 2015)12. This will impact on available funding for new treatments for HCV despite their undoubted effectiveness (Brennan and Shrank, 2014; Lemoine and Asia, 2014; Trooskin et al., 2015; Norton, 2015). The arrival of cost-effective second generation DAAs has fuelled the debate over pricing and reimbursement decisions across Europe given typically reimbursement for new expensive cancer treatments and those for orphan diseases despite often limited health gain, as well as whether there should be a greater focus on the budget impact of new medicines rather than just their cost-effectiveness (Kantarjian et al., 2013; Simoens et al., 2013; Cohen and Felix, 2014; Godman et al., 2015; Messori, 2015a)13.
Consequently, the aim of this initial study is to compare the uptake of BCV and TVR among European countries from a health authority perspective alongside implemented activities to influence their prescribing. We will subsequently build on the findings, including current activities among health authorities regarding second generation DAAs including price negotiations, to provide future direction and guidance to health authorities (Civaner, 2012; Lemoine and Asia, 2014)10. This will involve specific studies to ascertain utilization and expenditure of second generation DAAs alongside negotiated prices.
Methods
This was a retrospective cross sectional descriptive observational study involving twelve countries and regions from across Europe. Health authorities were contacted to provide aggregated data on the utilization and expenditure of BCV and TVR. This was purely voluntary as there was no funding for them and no funding to purchase utilization data from commercial sources. We have used this approach before when analysing the influence of different health authority measures to enhance the prescribing of generic atypical antipsychotics, proton-pump inhibitors, renin-angiotensin inhibitors, selective serotonin re-uptake inhibitors and statins across Europe (Godman et al., 2010a, 2014a; Vonèina et al., 2011; Moon et al., 2014).
The European countries and regions that provided utilization and expenditure data typically cover 100% of their population. However, there are differences in their geography, i.e., central, eastern, and western European countries, epidemiology, and financing of as well as available resources for healthcare (Table 2). This is important given the heterogeneity of European healthcare systems and suggested approaches when conducting cross national studies (Cacace et al., 2013). The only exception to health authority data is Turkey, where data from the Ministry of Health were sourced from Intercontinental Marketing Services (IMS).
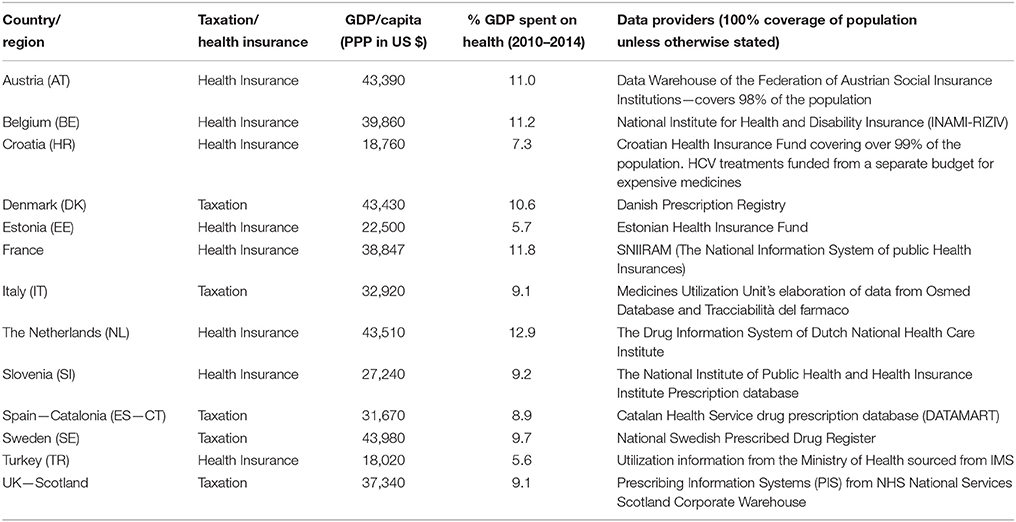
Table 2. Details of methods of financing healthcare, GDP spent on health and data providers (Godman et al., 2010a, 2013a; Atun et al., 2013; Hesse et al., 2013)14.
The region of Catalonia is included as it is difficult to obtain comprehensive drug utilization data from across Spain, and Catalonia is one of the principal autonomous communities in Spain, which has been active over a number of years with initiatives to improve the quality and efficiency of prescribing (Coma et al., 2009; Björkhem-Bergman et al., 2013). Tayside was also included, representing a region in Scotland, since at the time it was difficult to obtain drug utilization data from across Scotland.
Utilization Data
Utilization data were collected in Defined Daily Doses (DDD)16, with Table 3 providing details of the DDDs used.
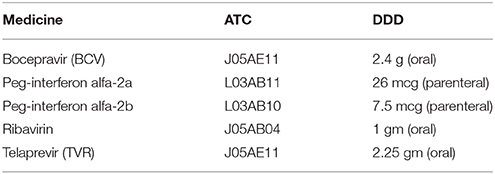
Table 3. DDDs for medicines to treat Hepatitis C15.
Population data from Eurostat were used to calculate DDDs per 1000 inhabitants per quarter (DIQs)17. Calculations were performed using the quarterly time period since the treatment period for HCV treatments is at least 12 weeks, and mostly 24 or 48 weeks, thereby providing a realistic denominator.
Results were calculated using two approaches. Firstly, the utilization of BCV and TVR was calculated separately to compare their uptake across countries. Due to the lack of patient specific data and different algorithms for BCV and TVR, their utilization was not combined. The second approach was an estimation of percentages of treated patients with triple therapy (ribavirin + pegIFN + TVR + BCV) vs. dual-therapy (ribavirin + pegIFN). This was again because we did not have access to individual patient data nor to prevalence rates. The percentage of treated patients was estimated through assessing the utilization of BCV and TVR in relation to ribavirin. Ribavirin is used as a proxy for dual-therapy because it is typically administered with pegIFNs, although we are aware that some patients with GT3 may be administered ribavirin without pegIFN. We acknowledge that there are differences in GT1 prevalence rates among European countries (Cornberg et al., 2011; Deuffic-Burban et al., 2012), that treatment algorithm data are not always available and there are different opinions and barriers to care (McGowan et al., 2013). Differences in GT1 prevalence rates and current treatment approaches are the most important uncertainties in this analysis. Consequently, we made a number of caveats to give a more realistic approach.
Estimates for GT1 is between 35 and 75% (Cornberg et al., 2011; Deuffic-Burban et al., 2012) of patients with chronic HCV (Table 1). In our approach, we used 45–65% to give a reasonable perspective. TVR treatment length varies between 12 of 48 weeks (25%) for patients with cirrhosis to 12 of 24 weeks (50%) for patients without cirrhosis and early SVR responses. For BCV, treatment length varies between 32 of 48 (67%) weeks for some treatment naïve patient without cirrhosis, mainly relapsers and partial responders, and 44 of 48 (92%) weeks for patients with cirrhosis (Christensen et al., 2012; Hofmann et al., 2012; Lagging et al., 2012; Leroy et al., 2012; Orlent et al., 2012; Ramachandran et al., 2012)1, 2. Sixty five and forty five percent GT1 prevalence rates were combined with percentages of treatment length, e.g., for TVR this was 25% use and 45% GT1 prevalence (25% of 45%) equating to 11.25%. Subsequently, the numbers used to estimate the potential for triple therapy are between 11.3 and 32.5% utilization for TVR and 30.2 and 59.7% utilization for BCV (Table 4). These findings define the second approach in an attempt to estimate the number of patients receiving triple therapy as a percentage of all HCV treated patients.
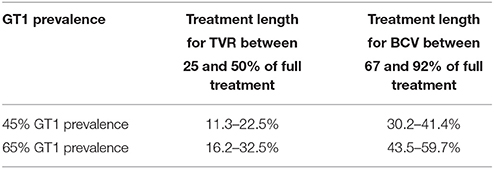
Table 4. Calculated percentages for triple therapy vs. all HCV treated patients.
Reimbursement Expenditure Data
Reimbursement expenditure was calculated in Euros per DDD (EUR/DDD). Exchange rates for Croatia, Denmark, Poland, Sweden and Switzerland where pertinent were calculated using the following conversion rates (conversion date 1-January 2008 as this was the start of the data collection period): 1 EUR = 7.6 HRK (Croatian Kuna), 7.46 DKK (Danish Krone), 9.44 SEK (Swedish krona), 1.65 CHF (Swiss franc), and 3.60 PLN (Polish zloty)18.
Descriptive Review of National and Regional Health Authority Demand-Side Activities Regarding HCV Drug Treatment for BCV and TVR
Measures undertaken by health authorities to potentially influence the subsequent utilization of BCV and TVR were collected and collated using the 4E—Education, Engineering, Economics, and Enforcement (Wettermark et al., 2009) methodology. This method was developed in order to make it easier to understand and compare the complexity and multiplicity of healthcare policies across countries and their potential impact and/or influence (Coma et al., 2009; Wettermark et al., 2009; Godman et al., 2010a,b; Godman et al., 2013b, 2014a; Garuoliene et al., 2011; Vonèina et al., 2011; Malmström et al., 2013). Table 5 shows definitions and gives some examples of the four dimensions.
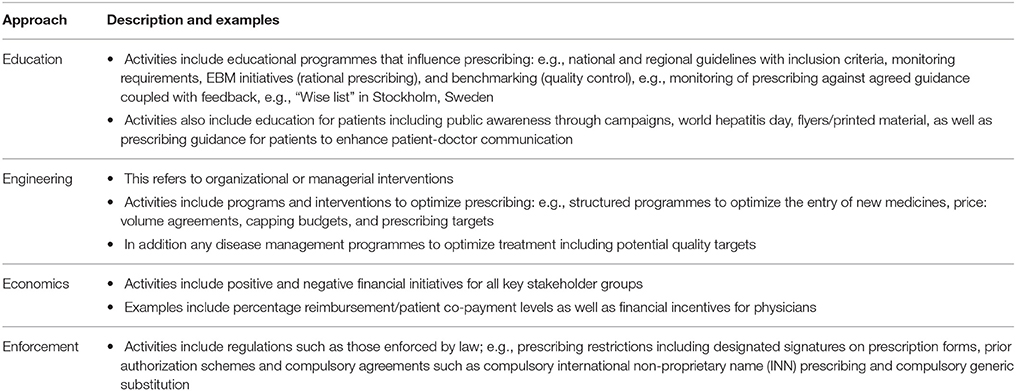
Table 5. Description 4E method—Education, Engineering, Economics, and Enforcement (Garuoliene et al., 2010; Godman et al., 2010a,b, 2014b, 2015; Maticic, 2014; Moon et al., 2014; Putrik et al., 2014; Campbell et al., 2015).
Country data were collected through an interactive and iterative process. Answers to the developed questionnaire were provided in written format by the co-authors, and subsequently checked for accuracy. Alternatively, country profiles were provided by one of the co-authors (Winnie De Bruijn) based on published sources as well as web-based articles. As a result, more European countries were included in the country profiles of ongoing activities regarding BCV and TVR than provided utilization data. Subsequent answers were re-checked and re-confirmed with the co-authors to enhance the robustness of the country profiles. This method has been used in previous publications involving health authority personnel (Garuoliene et al., 2010, 2011; Godman et al., 2010a,b, 2013b, 2014a,b; Vonèina et al., 2011; Malmström et al., 2013); consequently, applied in this research project.
All country profiles were supplemented with data from the WHO Hepatitis report19 and Euro Hepatitis Index 2012 report (Cebolla and Björnberg, 2012).
Patient consent as well as ethics approval was not required as aggregate utilization and expenditure data were obtained from anonymised health authority databases (Table 2). This is in line with previous publications involving anonymised aggregated health authority data Europe (Godman et al., 2010a, 2014a; Vonèina et al., 2011; Moon et al., 2014).
Results
General
In the majority of countries studied, both BCV and TVR were reimbursed. Exceptions included Bosnia and Herzegovina as well as Estonia (Table 6). Technically in Sweden only TVR is included in the national reimbursement scheme. However, in practice, both BCV and TVR are free for patients as both medicines are free for infectious diseases under the Infectious Disease Act.
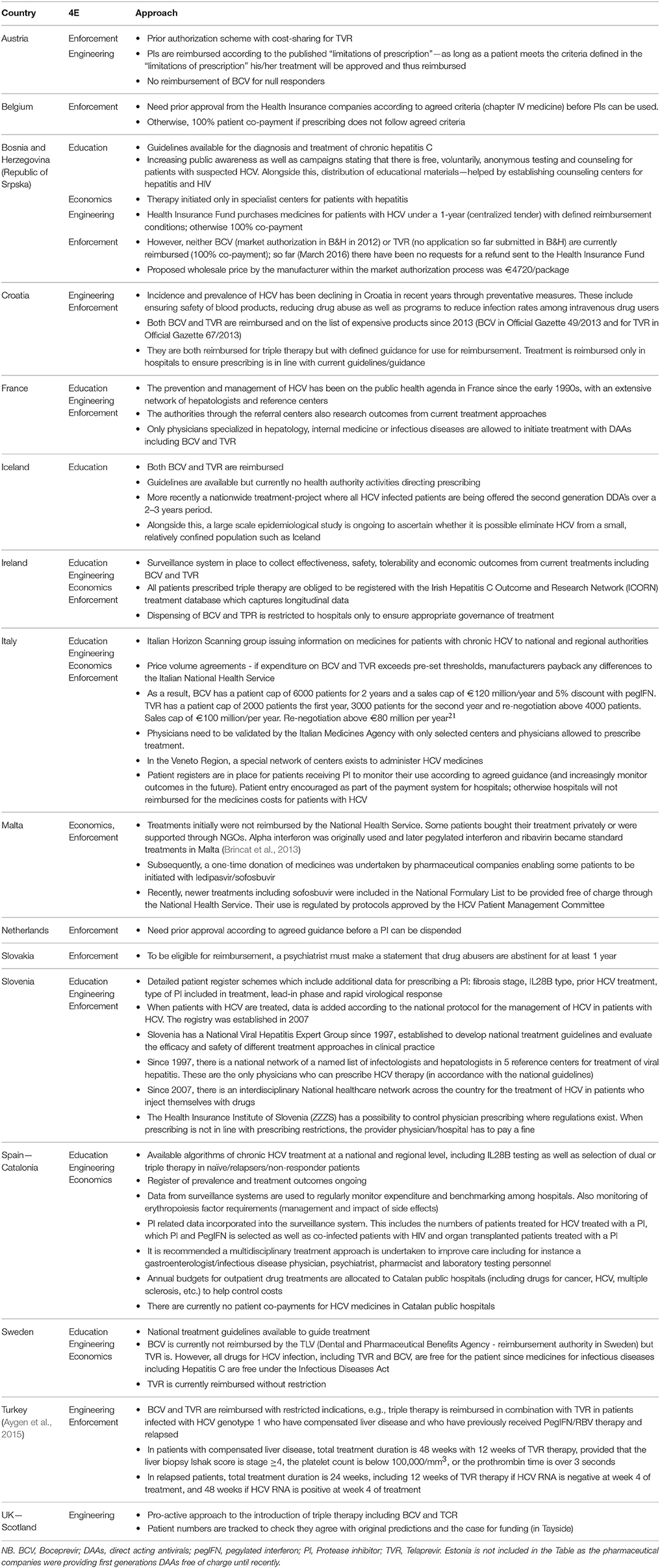
Table 6. Summary of most important demand side measures among European countries to influence the prescribing of BCV and TVR post-launch.
Activities among by Health Authorities to Influence the Prescribing of BCV and TVR
Table 6 summarizes the variety of measures broken down by the 4E method (Table 5) implemented by the various European countries to improve the management of patients with HCV. This includes any measures regarding subsequent utilization of BCV and TVR.
All European countries studied had a national strategy plan to manage patients with HCV, which typically included prevention and control programmes and/or guidelines19. All clinical guidelines available in English typically followed the strict EMA recommendations, e.g., besides SVR monitoring, there were also clear starting and stopping rules prior to initiating treatment and continuing treatment (European Association for the Study of the Liver, 2011; Hofmann et al., 2012; Lagging et al., 2012; Leroy et al., 2012; Orlent et al., 2012; Ramachandran et al., 2012)1, 2. Where countries mostly differed was their opinion regarding genotyping interleukin 28B (IL28B) polymorphism. Some countries and regions recommend routine testing, e.g., Catalonia, whilst others currently do not test.
All countries studied had a surveillance system for either acute and/or chronic HCV infections. Unfortunately current registries are heterogeneous and differ mostly in case definition (European Centre for Desease Prevention Control, 2010; Cornberg et al., 2011; Yehia et al., 2014)20. The EMA Committee for Medicinal Products for Human Use (CHMP) emphasized that the prescribing of BCV and TVR must be undertaken by professionals with knowledge and experience of HCV, including testing and treatment1, 2. Consequently, triple therapy must be prescribed by doctors who specialize in HCV management1, 2. This is typically the case for BCV and TVR, which are only licensed for GT1. This means physicians are obliged to test for genotypes before starting treatment.
All European countries that reimbursed triple therapy typically had no patient co-payment. We are aware that risk sharing agreements and discounts are used by health authorities to control budgets, enabling patients to have access to new high priced medicines (Adamski et al., 2010; Ferrario and Kanavos, 2013). However, data on the extent of any discounts are typically lacking as such arrangements are confidential. As a result, we were unable to document any cost/DDD data for BCV and TVR in Scotland (Tayside). Reimbursement for HIV co-infection and treatment before and after liver transplantation currently exists in a number of European countries including Austria, Ireland, Catalonia, Scotland, Slovakia, Slovenia and Sweden.
Utilization
The uptake of BCV and TVR varied between the countries and over time (Figures 1A,B). The highest uptake for TVR was in Tayside (Scotland) in the second quarter of 2012 at 2.4 DIQs. The highest uptake of BCV was in Belgium at 1.32 DIQs. Subsequently all countries showed a decrease of HCV medicines between approximately 6 months after triple therapy reimbursement, e.g., the Netherlands, Belgium, and Slovenia, and 12 months after triple therapy reimbursement, e.g., Austria, Denmark, Catalonia and Sweden. Utilization of BCV was highest in Belgium with 38% in third quarter after reimbursement (Q1 2013) and lowest in Italy and Estonia.
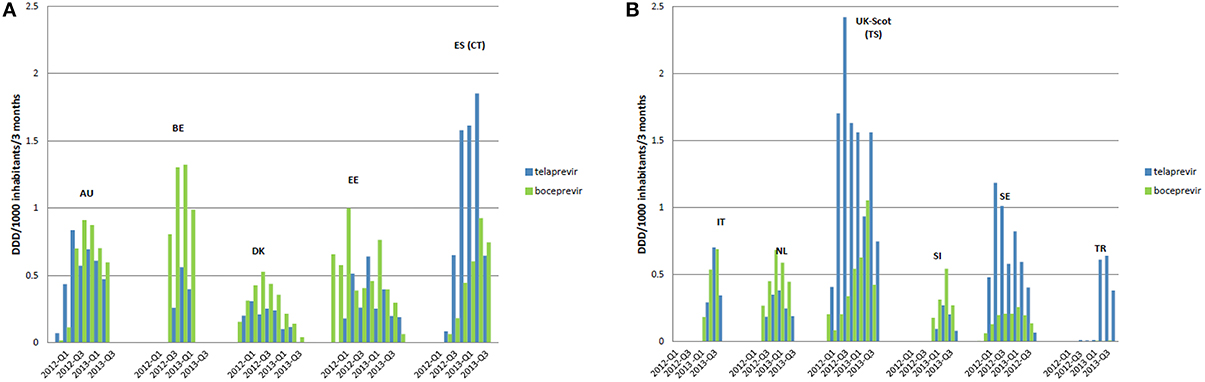
Figure 1. Uptake BCV and TVR across European countries from the month first reimbursed. Each Bar represents a 3 month period. Only the first quarter of 2012 and 2013 is displayed in the legend to include all countries. (A) Included countries are: AU, Austria; BE, Belgium; DK, Denmark; EE, Estonia; ES (CT), Catalonia (Spain). (B) Included countries are: IT, Italy; NL, the Netherlands; UK-Scot (TS), Tayside (Scotland); SI, Slovenia; SE, Sweden; TR, Turkey.
The upper and lower range (dotted lines in Figures 2, 3) illustrate the utilization of BCV and TVR if all potential patients with GT1 prevalence of 45–65% were treated (see comments in Table 4). For TVR, only Sweden meets the upper limit, which equates to the 65% GT1 prevalence and greatest percentage of therapy containing TVR. Only Austria, Estonia, Italy, and Catalonia do not meet the lower limit, indicating that even in a hypothetical situation with low GT1 prevalence and a short DAA treatment length, not all patients who should receive triple therapy actually receive it. For BCV, Belgium touches the lower limit with lowest GT1 prevalence and a lowest percentage of treatment containing BCV. Due to lack of patient specific data, prevalence data and different algorithms, the utilization of BCV and TVR are not consolidated. However, after adding BCV and TVR together, Belgium, Denmark, the Netherlands and Sweden appear to have the highest uptake of triple therapy vs. dual therapy.
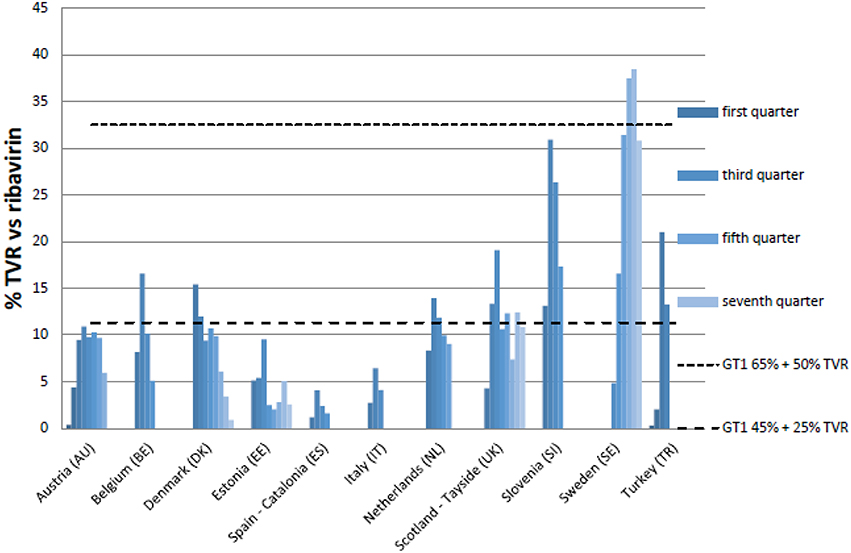
Figure 2. Percentage utilization of TVR vs. ribavirin in quarters following reimbursement. NB: Upper range genotype 1 prevalence (=GT1) is 65% and highest percentages (50%) triple therapy containing TVR (mostly non-cirrhotic patients). Lower range GT1 prevalence is only 45% and lowest percentages (25%) triple therapy containing TVR (mostly cirrhotic patients).
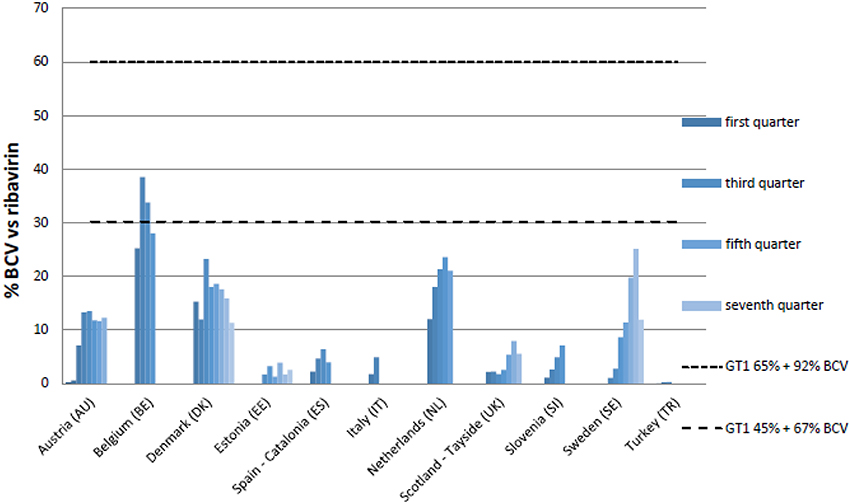
Figure 3. Percentage utilization of BCV vs. ribavirin in quarters following reimbursement. Upper range genotype 1 prevalence (=GT1) is 65% and highest percentages (92%) triple therapy containing BVC (mostly cirrhotic patients). Lower range GT1 prevalence is only 45% and lowest percentages (67%) triple therapy containing BVC (mostly naïve non-cirrhotic patients).
Expenditure Data
Table 7 contains reimbursed expenditure/DDD data for both BCV and TVR up to May 2013. Turkey was excluded as only IMS data were available. Estonia was excluded as these medicines have only recently been reimbursed, and Scotland (Tayside) was excluded as reimbursed data included confidential discounts; consequently unavailable for analysis. There were no differences in the documented prices between medicines dispensed in hospital pharmacies for out-patients or community pharmacies. However, this did not include any confidential discounts as part of risk sharing or other agreements (Adamski et al., 2010; Ferrario and Kanavos, 2013; Vogler et al., 2013).
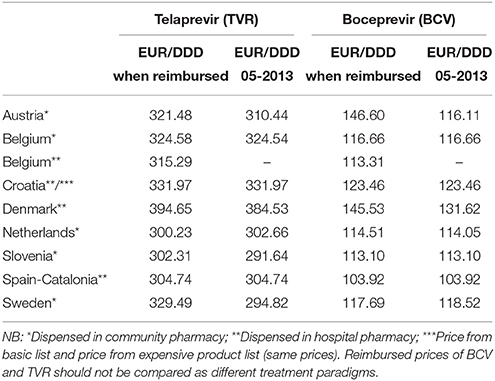
Table 7. Reimbursed Euro per DDD (EUR/DDD) from the time of reimbursement until the latest available data (May 2013) of TVR and BCV.
For both BCV and TVR, Denmark appeared to pay the highest reimbursed price at 131.52 and 384.53 EUR/DDD respectively. Catalonia (Spain) appeared to pay the lowest reimbursed price at 103.92 EUR/DDD for BCV and Slovenia the lowest reimbursed price for TVR at 291.64 EUR/DDD. Only Austria had a major price decrease from EUR 146.60 to EUR 116.1 per DDD during the course of the study following agreements.
Total expenditure for HCV treatments was decreasing in all countries before the reimbursement of BCV and TVR, especially in Catalonia and Austria (Figure 4), and again prior to the availability of the newer second generation DAAs, at the end of 2012 and beginning of 2013. Denmark and Slovenia had the lowest increase in EUR/1000 inhabitants/3 months after the reimbursement of BCV and TVR. This was 99 and 89% respectively between the lowest and highest EUR/1000 inhabitants/3 months from just before impending reimbursement of these two medicines to just after. This compares with a rise of 385% in Catalonia.
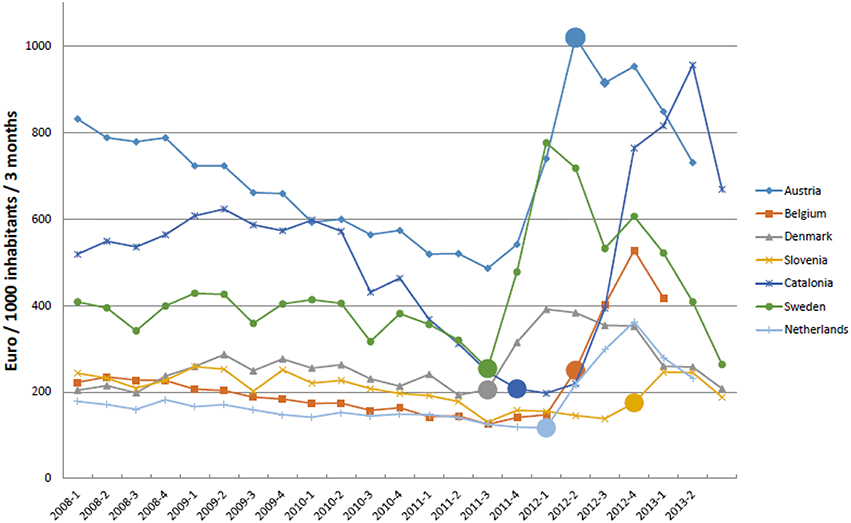
Figure 4. Expenditure on treatments for HCV (Euro/1000 inhabitants/quarter) from 2008 to 2013. NB: ⃝ = reimbursement agreed BVC. Sweden and Denmark first quarter after EMA approval are included.
Discussion
Our analysis showed reasonable consistency in the uptake of BCV and TVR among the European countries studied (Figure 1) compared with appreciable differences that have been seen in the utilization of new high priced medicines to treat patients with rheumatoid arthritis, type 2 diabetes and cancer across Europe (Hoebert et al., 2012; Jönsson et al., 2014; Putrik et al., 2014; Nolte and Corbett). This is despite appreciable differences among the participating countries in their level of spending on healthcare as well as the percentage of GDP they spend on health (Table 1). This might be explained firstly by the fact that all European countries followed EMA labeled indications with strict regulations for clear genotyping and SVR monitoring. Secondly, there were relatively few measures implemented among European health authorities to influence physician prescribing of either BCV or TVR apart from directing prescribing to specialists and specialist centers and entering patients into registries. Thirdly, both treatments were typically 100% reimbursed although there are exceptions (Table 6).
The rapid uptake of BCV and TVR across countries (Figure 1) may be explained by expectancy among professionals and patients regarding the increased efficacy of these first generation DAAs vs. previous regimens. This resulted in countries placing patients on waiting lists to receive triple therapy soon after BCV and TVR were reimbursed. Whilst we cannot say this with certainty, this is in line with decreasing costs of ribavirin and pegIFNs before reimbursement of the new PIs (Figure 4). Additionally, European guidelines advised postponing HCV treatment until the new DAAs including sofosbuvir became available in view of their greater efficacy and tolerability as well as reduced length of treatment (European Association for the Study of the Liver, 2011; Hatzakis et al., 2011).
The consistency in the utilization of BCV and TVR across Europe appears promising, especially considering a desire to reduce infection rates whilst attempting to keep the budgets for these medicines manageable. Any differences in utilization rates of BCV and TVR between countries (Figure 1) could potentially be explained by differences in HCV and GT1 prevalence variations as well as local physician preferences and knowledge rather than any specific health authority interventions (Table 6). However, we cannot comment further as we did not have access to patient level data. In addition, we did not explore key issues among specialist physicians involved in the management of patients with HCV.
Reimbursed prices for BCV and TVR (EUR/DDD) also appeared comparable among the European countries studied. This did not include risk-sharing agreements including rebates and discounts as information about these agreements is limited, with the exception of Italy. This is because such measures are typically confidential.
The upper and lower ranges identified in Figures 2, 3 suggest that the uptake of triple therapy appears reasonable in a number of the studied countries based on the assumptions of GT1 prevalence and treatment algorithms (Table 4); although, lower in some countries. However, there needs to be caution when interpreting these results as a number of assumptions were made (Table 4), and we are aware of the concerns with current estimated prevalence rates for HCV GT1 (Table 1). Utilization data can also be complicated by other factors, which include patients being selected for dual therapy if they have a low HCV RNA viral load after 4 weeks or ILB28B favorable CC polymorphism. Analysis of subsequently available patient level data in Stockholm, Sweden, showed that among patients initiated on treatment in 2012, total (TVR+BCV)/ribavirin was approximately 64% in 2012, which corresponds to Figures 2, 3 (Frisk, Personal Communication). However, in Catalonia, TVR+BCV/ribavirin was used in approximately 18.6% of patients, which is higher than in our study (Ibáñez, Personal Communication). In a recent report involving Italy, France, Germany, Spain and UK, most gastroenterologists stated that triple therapy would be prescribed more for non-responders in the first year of its availability. By 2014, 60% of treatment-naïve patients were expected to be treated with triple therapy22. This wide predicted variation in the prescribing of DAAs was not seen in practice (Figures 1A,B), with the utilization of BCV and TVR (Figures 1A,B) appearing more similar compared with the appreciable differences in the utilization of other high priced medicines, e.g., TNF alpha inhibitors and those to treat patients with cancer or Type 2 diabetes (Hoebert et al., 2012; Jönsson et al., 2014; Putrik et al., 2014; Nolte and Corbett).
One reason for the lower than expected surge in the use of triple therapy in Europe could be that efficacy and safety data from clinical trials are not always replicated in clinical practice and side effects can be more frequent and severe. This is especially the case in treatment-experienced HCV patients as observed in the French cohort reported by Hézode et al. (2013, 2014). The same phenomenon has been seen in Ireland where the effectiveness in patients entered into the registry (Table 6) was considerably lower than those seen from the clinical trials (O'Leary, Personal Communication). Published studies in the US have shown that the uptake of triple therapy was also relatively low, although TVR (INCIVEK®) reached 1 US$ billion within a short time and US$1.6 billion after the first year23. In a small study (487 GT1 patients), only 18.7% of patients received triple therapy in the first year after FDA approval (Chen et al., 2013). Reasons not to start triple therapy were principally contraindications (50%). Of all the patients who started triple therapy, 21% discontinued it. This was mostly because of side effects (Chen et al., 2013). Other studies have also concluded that side effects are the most frequent barrier for chronic HCV treatment (McGowan et al., 2013).
Consequently, side effects and complexity of drug treatment posology of PIs may explain the decrease in utilization and expenditure of BCV and TVR in recent years among European countries (Figures 1, 4) coupled with the anticipation of the new second generation DAAs, with less side effects, shorter treatment durations, the potential for interferon free regimens and the potential for cures (Brennan and Shrank, 2014; Kohli et al., 2014)3. We are aware for instance that in Catalonia, France and Sweden, a number of potentially eligible patients for BCV and TVR were put on waiting lists until the launch of the second generation DAAs, and probably in other countries as well.
This observation is strengthened by recent findings showing that sofosbuvir, after TVR, was the fastest growing prescribed medicine in the US with sales of US$2.27 billion in the first quarter of 201424 reaching, as mentioned, US$12.4 billion worldwide in 2014. This accounted for 37.5% of expenditure on HCV medicines among managed care organizations in 2014 (Trooskin et al., 2015)11. This expenditure is helped by the cost of a standard 12-week course of sofosbuvir and simeprevir being initially at US$84 000 and US$66,000 in the US respectively, with sofosbuvir initially priced at between Euro 50,000 and 60,000 per 12-week course among Eurozone countries, although U$54,000 (€44,000) in the UK and €41,000 in France (Brennan and Shrank, 2014; Lemoine and Asia, 2014; Phelan and Cook, 2014; van de Ven et al., 2014; Trooskin et al., 2015; Iyengar et al., 2016). These prices, coupled with the prevalence of HCV, have already resulted in activities among countries to control costs through price negotiations and other strategies. This is not surprising with potential sales of US$15 trillion if an estimated 180 million people worldwide with HCV were treated with sofosbuvir (Montazerhodjat et al., 2016). Table 8 summarizes some of the activities, exacerbated for instance by the authorities in France initially being charged sofosbuvir at 756 times the cost of its production in France (Phelan and Cook, 2014).
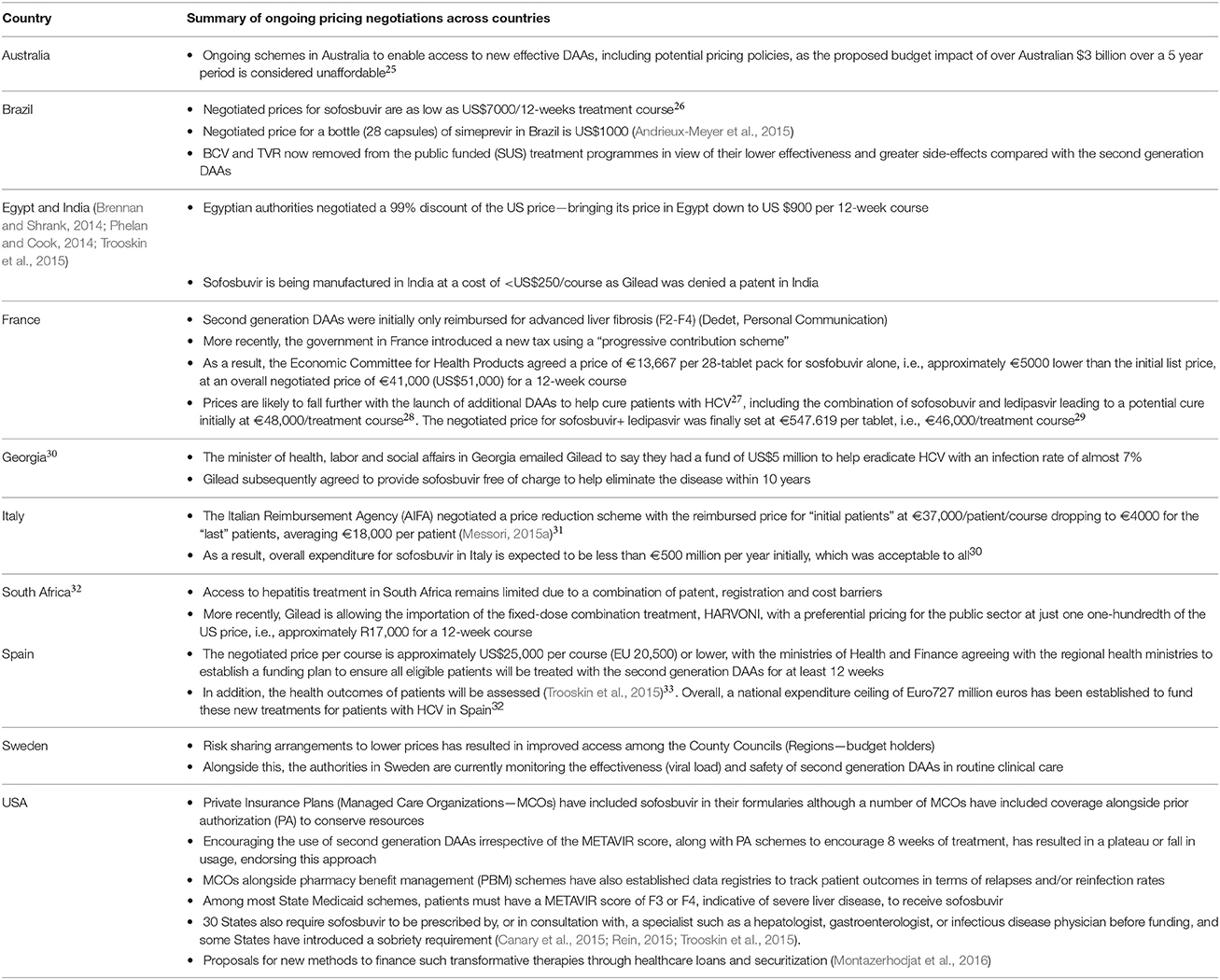
Table 8. Price negotiations and other strategies across countries to reduce the expenditure burden of second generation DAAs.
There are also ongoing activities among other African countries including Botswana and Zimbabwe given the higher prevalence of HCV in developing countries and the potential for generic agreements. These differences in policies for the second generation DAAs is already leading to considerable differences in their utilization rates in Europe34.
Recent analysis has shown there is still appreciable variation in the price of second generation DAAs across countries (Andrieux-Meyer et al., 2015). For instance, the price per bottle of sofosbuvir (28 tablets) ranges from $300 (India and Pakistan) and $402 (Nigeria—current market survey) to $20,590 in Switzerland, and for daclatasvir from $175 in Egypt and $252 in Nigeria (current market survey) to $14,899 in Germany (Andrieux-Meyer et al., 2015). Overall, prices are generally substantially lower in LMIC countries although there are outliers, with little correlation between prices and per capita income levels among higher income countries, e.g., the price for a bottle of simeprevir ranges from U$9166 in Spain to US$14,865 in Australia (Andrieux-Meyer et al., 2015).
It is likely that prices of second generation DAAs will continue falling across countries with estimates of manufacturing for 12-week courses at US$10-$30 for daclatasvir, US$68–$136 for sofosbuvir, US$100–$210 for faldaprevir and US$130–$270 for simeprevir (Hill et al., 2014) coupled with increased competition. This should also help the management of patients with genotypes 4, 5, and 6 that are mainly present in Africa, the Middle East and Asia, where resources are more limited (Papastergiou and Karatapanis, 2015). Their availability as oral therapies coupled with the potential of avoiding genotyping with its associated facilities and costs should further help with increased usage and price negotiations (Ford et al., 2014; Younossi et al., 2015).
Prices should also fall further following the inclusion of sofosbuvir, simeprevir dasabuvir and daclatasvir in the 19th edition of the WHO Model List of Essential Medicines along with comments to negotiate affordable prices35. This alongside the formation of consortia, which is already happening in the US with State Medicaid schemes, following the example of ARVs where prices reduced substantially following strong pressure from multiple stakeholders (Lemoine and Asia, 2014). In addition, the potential development of a Global Fund for treatments for patients with HCV or other mechanisms (Phelan and Cook, 2014).
The undoubted effectiveness of the second generation DAAs is making European and other health authorities re-think their approaches to valuing new high priced medicines. This includes new medicines for patients with cancer, as well as those for orphan diseases, which are being reimbursed at high prices despite often very limited health gain in view of patient pressure and other factors (Fojo and Grady, 2009; Hughes-Wilson et al., 2012; Experts in Chronic Myeloid Leukemia, 2013; Kantarjian et al., 2013; Simoens et al., 2013; Cohen and Felix, 2014; Ghinea et al.). This will continue and be the subject of future research projects among the co-authors. Future research will also include assessing the utilization and expenditure on second generation DAAs in clinical practice among European countries as they become standards of care (Childs-Kean and Hand, 2015), building on early analysis by the French authorities and others33.
Conclusion
There appears to be reasonable consistency in the uptake and utilization of BCV and TVR among the studied European countries in comparison with other new high priced medicines. This may reflect the high social impact of chronic HCV treatment, especially with few health authority measures implemented to influence physician prescribing. However, using ribavirin as a benchmark hints at differences in the utilization of BCV and TVR. This may indicate that the prescribing of dual vs. triple therapy differs across countries. This cannot be explained by looking at health authority activities for these two treatments and may just reflect physician preference. Consequently, more information including GT1 prevalence data and data on treatment algorithms (including treatment length and treatment period containing PI) is needed to explain this.
There are also ongoing activities with the second generation DAAs across countries to reduce their costs in view of their undoubted effectiveness and tolerability alongside their considerable budget impact. This will be the subject of future research to provide additional guidance to authorities in the face of continuing resource pressures.
Author Contributions
WdB, CI, PF, HBP, and BG contributed to the design of the paper and the methodology. They also produced the first and subsequent drafts. AA, PVB, AB, LB, GD, JE, JOF, JF, GG, IG, AG, HG, SJ, JJ, RJ, SK, OL, NM, EM, MM, VM-P, AM, OO, AO'L, JP, CS, SS, CT, IT, MT, KT, MW, SV, EV, and CZ provided data on the utilization of BCV and TVR and/or ongoing measures within their own countries to improve the prevention and/or management of HCV. They also critiqued successive drafts of the paper. All authors read and approved the final manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We acknowledge the help of Paolo Siviero, ex AIFA in Italy, for his help with providing data and information from Italy. We wish to thank Theresa Bucsics, Department of Gastroenterology and Hepatology, Medical University of Vienna, for her helpful comments. This work was in part supported by grants from the World Health Organization and the Karolinska Institutet, Sweden. The write-up was in part supported by a Newton Advanced Fellowship awarded to Professor Augusto Afonso Guerra Junior by the Academy of Medical Sciences, through the UK Government's Newton Fund programme. It was also in part supported by a VR-Link grant from Swedish Research Council (VR-Link 2013-6710) to AM. GG has been supported by the Swedish Research Council Carl Wilhelm Scheeles Guest Professorship.
Footnotes
1. ^European Medicine Agency. Incivo - telaprevir [Internet]. [cited 18 Nov 2015] Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/002313/human_med_001487.jsp&mid=WC0b01ac058001d124
2. ^European Medicine Agency. Victrelis - boceprevir [Internet]. [cited 18 Nov 2015] Available from: http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/002332/human_med_001464.jsp&mid=WC0b01ac058001d124
3. ^California Technology Assessment Forum. The Comparative Clinical Effectiveness and the Value of Simeprevir and Sofosbuvir in the Treatment of Chronic Hepatitis C Infection: Final Report. San Francisco: California Technology Assessment Forum; April 15, 2014. Available at URL: http://icer-review.org/wp-content/uploads/2016/02/CTAF_Hep_C_Apr14_final.pdf (Accessed 8 July 2017).
4. ^European Medicine Agency. EPAR Sovaldi sofosbuvir. [cited 2015 Nov] Available at URL: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Summary_for_the_public/human/002798/WC500160599.pdf
5. ^European Medicine Agency. EPAR Olysio simeprevir. [cited 2015 Nov] Available at URL: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Summary_for_the_public/human/002777/WC500167869.pdf
6. ^European Medicine Agency. EPAR daclatasvir. [Cited 2015 Nov]. 2014. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/003768/WC500172849.pdf
7. ^European Medicine Agency. EPAR Ledipasvir. Harvoni [Cited 2015 Nov]. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Summary_for_the_public/human/003850/WC500177997.pdf
8. ^European Medicine Agency. EPAR ombitasvir/paritaprevir/ritonavir. [cited 2015 Oct] Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Summary_for_the_public/human/003839/WC500184000.pdf
9. ^Médecins Sans Frontières. THE DIAGNOSIS AND TREATMENT OF HEPATITIS C?: A technical landscape. 2013. Available at URL: http://www.msfaccess.org/sites/default/files/MSF_assets/HepC/Docs/HepC_brief_TechnicalLandscape_ENG_2013.pdf (Accessed 15 Oct 2015).
10. ^Research and Markets. Hepatitis C Therapeutics Market to 2018 - Expected Launch of GS-7977 in 2015 will Pave the Way for an Oral Interferon-free Combination Therapy [Internet]. 2012. [cited 2015 Sept] Available from: http://www.researchandmarkets.com/research/ngbvll/hepatitis_c
11. ^Express Scripts. The 2014 Drug Trend Report. [cited 2015 Sept]. Available at URL: http://lab.express-scripts.com/~/media/PDFs/Drug%20Trend%20Report/ExpressScripts_DrugTrendReport.ashx (Last Accessed 8 July 2016).
12. ^EFPIA. HEALTH and GROWTH - Evidence Compendium. October 30th, 2013. Available from URL: http://www.efpia.eu/uploads/Modules/Documents/health-and-growth_evidence-compendium.pdf
13. ^WHO. Access to new medicines in Europe: technical review of policy initiatives and opportunities for collaboration and research. Available at URL: http://www.euro.who.int/en/health-topics/Health-systems/medicines/publications2/2015/access-to-new-medicines-in-europe-technical-review-of-policy-initiatives-and-opportunities-for-collaboration-and-research.
14. ^Health expenditure, total (% of GDP) - World Health Organization Global Health Expenditure database [Internet]. [cited 2015 Aug 17]. Available from: http://data.worldbank.org/indicator/SH.XPD.TOTL.ZS
15. ^ATC/DDD Index 2013 [cited 2015 Sept]. Available from: http://www.whocc.no/
16. ^World Health Organization (WHO). Introduction to Drug Utilization Research World Health Organization WHO International Working Group for Drug Statistics Methodology, Collaborating Centre for Drug Utilization Research and Clinic. 2003. [cited 2015 Oct]. Available at URL: http://www.who.int/medicines/areas/quality_safety/safety_efficacy/Drug%20utilization%20research.pdf
17. ^Eurostat. Population on 1 January. [cited 2015 Sept] Available from: http://epp.eurostat.ec.europa.eu/tgm/table.do?tab=table&language=en&pcode=tps00001&tableSelection=1&footnotes=yes&labeling=labels&plugin=1
18. ^Current and Historical Rate Tables. [cited 2015 Sept] Available from: http://www.xe.com/currencytables/?from=EUR&date=2008-01-01
19. ^World Health Organization (WHO). Global policy report on the prevention and control of viral hepatitis IN WHO MEMBER STATES. 2013. [cited 2015 Aug] Available at URL: http://apps.who.int/iris/bitstream/10665/85397/1/9789241564632_eng.pdf?ua=1
20. ^ECDC. Annual epidemiological report on communicable diseases in Europe 2009. [cited 2015 Sept] Available from: http://www.ecdc.europa.eu/en/publications/Publications/1011_SUR_Annual_Epidemiological_Report_on_Communicable_Diseases_in_Europe.pdf
21. ^Cicchetti A. La tensión regulación- innovación en las decisiones de precio y re-embolso de nuevos medicamentos en Italia. [cited 2015 Jan] Available from: http://www.fgcasal.org/fgcasal/database/documentos/PharmaMar-FGC_2012_AMERICO_CICCHETTI-2.pdf
22. ^HCV new drug research. Hepatitis C News; European Gastroenterologists Will Prescribe Telaprevir and Boceprevir to Nonresponder and Treatment-Naive Patients Following Launch [Internet]. 2011 Available from: http://hepatitiscnewdrugs.blogspot.dk/2011/04/hepatitis-c-news-european.html (Accessed 10 Oct 2015).
23. ^Incivek set to break record for fastest product launch [Internet]. EvaluatePharma. [cited 2015 Nov]. Available from: http://epvantage.com/Universal/View.aspx?type=Story&id=261529&isEPVantage=yes
24. ^Gilead Sciences Announces First Quarter 2014 Financial Results [Internet]. Gilead Sciences Inc. 2014. [cited 2015 Nov] Available from: http://www.gilead.com/news/press-releases/2014/4/gilead-sciences-announces-first-quarter-2014-financial-results [Internet] (Accessed 8 July 2016).
25. ^PBAC. Australian Government Department of Health. March 2015 PBAC MEETING – POSITIVE RECOMMENDATIONS. [Cited Sept 2015]. Available from: http://www.pbs.gov.au/info/industry/listing/elements/pbac-meetings/pbac-outcomes/2015-03.
26. ^Hepatitis C Society. Sofosbuvir Cost. Available from URL: http://esofosbuvir.com/sofosbuvir-drug/sofosbuvir-cost/ (Accessed 8 July 2016).
27. ^PMlive. France agrees lowest Sovaldi pricing in EU. Government brings cost of hepatitis C drug to €5,000 below list price. Available at URL: http://www.pmlive.com/pharma_news/france_agrees_lowest_sovaldi_pricing_in_eu_618661 (Accessed 8 July 2016).
28. ^Hepatitis News. French Strike Deal for Sofosbuvir. Available at URL: https://gareth-williams-gcuc.squarespace.com/hepatitis-articles/2015/10/26/french-strike-deal-for-sofosbuvir?rq=french-strike-deal-for-sofosbuvir (Accessed 8 July 2016).
29. ^Avis relatif aux prix de spécialités pharmaceutiques publiés en application de l'article L. 162-16-5 du code de la sécurité sociale. Available at URL: https://www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000030741836 (Accessed 8 July 2016).
30. ^Irish Times. How to sell a $1000 pill for $10 without losing money. Available at URL: http://www.irishtimes.com/business/health-pharma/how-to-sell-a-1-000-pill-for-10-without-losing-money-1.2554351 (Accessed Oct 2015).
31. ^Messori (2015b). Available from: http://www.bmj.com/content/351/bmj.h4988/rr (Accessed 8 July 2016).
32. ^Daily Maverick. Health-e: South Africa's “other” virus. http://www.dailymaverick.co.za/article/2015-11-30-health-e-south-africas-other-virus/#.V3q1oqSzHIU (Accessed Feb 2016).
33. ^Campillo-Artero, C. The merry-go-round of approval, pricing and reimbursement of new drugs (Part 2). Available at URL: http://www.hspm.org/countries/spain25062012/livinghit.aspx?Section=3.2%20Population%20coverage%20and%20basis%20for%20entitlement&Type=Section#6Themerry-go-roundofapproval,pricingandreimbursementofnewdrugs(Part2) (Accessed 8 July 2016).
34. ^CNAMTS. Ameliorér la qualité du système de sante et maîtriser les depenses. Propositions de l'Assuarance Maladie pour 2016. [Internet]. Available from: http://www.ameli.fr/rapport-charges-et-produits-2016/ (Accessed Feb 2016).
35. ^World Health Organization “19th WHO Model List of Essential Medicines (April 2015)”. Geneva. Available at URL: http://www.who.int/medicines/publications/essentialmedicines/EML2015_8-May-15.pdf (Accessed Oct 2015).
References
Adamski, J., Godman, B., Ofierska-Sujkowska, G., Osiñska, B., Herholz, H., Wendykowska, K., et al. (2010). Risk sharing arrangements for pharmaceuticals: potential considerations and recommendations for European payers. BMC Health Serv. Res. 10:153. doi: 10.1186/1472-6963-10-153
Andrieux-Meyer, I., Cohn, J., de Araújo, E. S. A., and Hamid, S. S. (2015). Disparity in market prices for hepatitis C virus direct-acting drugs. Lancet Glob. Heal. 3, e676–e677. doi: 10.1016/S2214-109X(15)00156-4
Atun, R., Aydın, S., Chakraborty, S., Sümer, S., Aran, M., Gürol, I., et al. (2013). Universal health coverage in Turkey: enhancement of equity. Lancet 382, 65–99. doi: 10.1016/S0140-6736(13)61051-X
Aygen, B., Yıldız, O., Akhan, S., Çelen, M. K., Ural, O., Koruk, S. T., et al. (2015). Retreatment of Chronic Hepatitis C Infection with Telaprevir: preliminary results in Turkey. Balkan. Med. J. 32, 266–272. doi: 10.5152/balkanmedj.2015.15366
Barua, S., Greenwald, R., Grebely, J., Dore, G. J., Swan, T., and Taylor, L. E. (2015). Restrictions for medicaid reimbursement of sofosbuvir for the treatment of hepatitis C virus infection in the United States. Ann. Int. Med. 163, 215–223. doi: 10.7326/M15-0406
Björkhem-Bergman, L., Andersén-Karlsson, E., Laing, R., Diogene, E., Melien, O., Jirlow, M., et al. (2013). Interface management of pharmacotherapy. Joint hospital and primary care drug recommendations. Eur. J. Clin. Pharmacol. 69(Suppl. 1), 73–78. doi: 10.1007/s00228-013-1497-5
Brennan, T., and Shrank, W. (2014). New expensive treatments for hepatitis C infection. JAMA 312, 593–594. doi: 10.1001/jama.2014.8897
Brincat, A. A., Deguara, M., Taliana, K., Rogers, M., and Pocock, J. (2013). The management of patients positive to hepatitis C virus antibody in Malta. Malta Med. J. 25, 72–77.
Cacace, M., Ettelt, S., Mays, N., and Nolte, E. (2013). Assessing quality in cross-country comparisons of health systems and policies: towards a set of generic quality criteria. Health Policy 112, 156–162. doi: 10.1016/j.healthpol.2013.03.020
Campbell, S. M., Godman, B., Diogene, E., Fürst, J., Gustafsson, L. L., MacBride-Stewart, S., et al. (2015). Quality indicators as a tool in improving the introduction of new medicines. Basic. Clin. Pharmacol. Toxicol. 116, 146–157. doi: 10.1111/bcpt.12295
Canary, L., Klevens, R., and Holmberg, S. (2015). Limited access to new hepatitis C virus treatment under state medicaid programs. Ann. Int. Med. 163, 226–228. doi: 10.7326/M15-0320
Cebolla, B., and Björnberg, A. (2012). Euro Hepatitis Index Report - Health Consumer Powerhouse. Available online at: http://www.healthpowerhouse.com/files/euro-hepatitis-index-2012/Report-Hepl-HCP-121104-2-w-Cover.pdf
Chen, E. Y., Sclair, S. N., Czul, F., Apica, B., Dubin, P., Martin, P., et al. (2013). A small percentage of patients with hepatitis C receive triple therapy with boceprevir or telaprevir. Clin. Gastroenterol. Hepatol. 11, 1014–1020.e1–e2. doi: 10.1016/j.cgh.2013.03.032
Childs-Kean, L. M., and Hand, E. O. (2015). Simeprevir and sofosbuvir for treatment of Chronic Hepatitis C Infection. Clin. Ther. 37, 243–267. doi: 10.1016/j.clinthera.2014.12.012
Chou, R., Hartung, D., Rahman, B., Wasson, N., and Cottrell, E. B. (2014). Comparative effectiveness of antiviral treatment for Hepatitis C Virus infection in adults: a systematic review. Ann. Int. Med. 158, 114–123. doi: 10.7326/0003-4819-158-2-201301150-00576
Christensen, P. B., Clausen, M. R., Krarup, H., Laursen, A. L., Schlichting, P., and Weis, N. (2012). Treatment for hepatitis B virus (HBV) and hepatitis C virus (HCV) infection - Danish national guidelines 2011. Dan. Med. J. 59, C4465.
Civaner, M. (2012). Sale strategies of pharmaceutical companies in a “pharmerging” country: the problems will not improve if the gaps remain. Health Policy 106, 225–232. doi: 10.1016/j.healthpol.2012.05.006
Cohen, J. P., and Felix, A. (2014). Are payers treating orphan drugs differently? J. Mark. Access Health Policy 2, 1–5. doi: 10.3402/jmahp.v2.23513
Coma, A., Zara, C., Godman, B., Agustí, A., Diogène, E., Wettermark, B., et al. (2009). Policies to enhance the efficiency of prescribing in the Spanish Catalan region: impact and future direction. Expert Rev. Pharmacoecon Outcomes Res. 9, 569–81. doi: 10.1586/erp.09.58
Cornberg, M., Razavi, H. A., Alberti, A., Bernasconi, E., Buti, M., Cooper, C., et al. (2011). A systematic review of hepatitis C virus epidemiology in Europe, Canada and Israel. Liver Int. 31(Suppl. 2), 30–60. doi: 10.1111/j.1478-3231.2011.02539.x
Cure, S., Guerra, I., Cammà, C., Craxì, A., and Carosi, G. (2015). Cost-effectiveness of sofosbuvir plus ribavirin with or without pegylated interferon for the treatment of chronic hepatitis C in Italy. J. Med. Econ. 18, 678–690. doi: 10.3111/13696998.2015.1040024
Deuffic-Burban, S., Deltenre, P., Buti, M., Stroffolini, T., Parkes, J., Mühlberger, N., et al. (2012). Predicted effects of treatment for HCV infection vary among European countries. Gastroenterology 143, 974–985.e14. doi: 10.1053/j.gastro.2012.05.054
Dore, G. J., Ward, J., and Thursz, M. (2014). Hepatitis C disease burden and strategies to manage the burden. J. Viral Hepat. 21(Suppl. 1), 1–4. doi: 10.1111/jvh.12253
European Association for the Study of the Liver (2011). EASL clinical practice guidelines: management of Hepatitis C virus infection. J. Hepatol. 55, 245–264. doi: 10.1016/j.jhep.2011.02.023
European Association for the Study of the Liver (2014). EASL clinical practice guidelines: management of Hepatitis C Virus infection. J. Hepatol. 60, 392–420. doi: 10.1016/j.jhep.2013.11.003
European Centre for Desease Prevention Control (2010). Hepatitis B and C in the EU Neighbourhood: Prevalence. Burden: Burden of Disease and Screening Policies.
Experts in Chronic Myeloid Leukemia (2013). The price of drugs for chronic myeloid leukemia (CML) is a re fl ection of the unsustainable prices of cancer drugs: from the perspective of a large group of CML experts. Blood 121, 4439–4442. doi: 10.1182/blood-2013-03-490003
Ferrario, A., and Kanavos, P. (2013). Managed Entry Agreements for Pharmaceuticals: The European Experience. LSE. Available onlinje at: http://eprints.lse.ac.uk/50513/1/__Libfile_repository_Content_Ferrario%2C%20A_Ferrario_Managed_%20entry_%20agreements_2013_Ferrario_Managed_%20entry_%20agreements_2013.pdf (Accessed on: 15 Oct 2015).
Fojo, T., and Grady, C. (2009). How much is life worth: cetuximab, non-small cell lung cancer, and the $440 billion question. J. Natl. Cancer Inst. 101, 1044–1048. doi: 10.1093/jnci/djp177
Ford, N., Swan, T., Beyer, P., Hirnschall, G., Easterbrook, P., and Wiktor, S. (2014). Simplification of antiviral hepatitis C virus therapy to support expanded access in resource-limited settings. J. Hepatol. 61(Suppl. 1). S132–S138. doi: 10.1016/j.jhep.2014.09.019
Fraser, I., Burger, J., Lubbe, M., Dranitsaris, G., Sonderup, M., and Stander, T. (2016). Cost-effectiveness modelling of sofosbuvir-containing regimens for Chronic Genotype 5 Hepatitis C Virus Infection in South Africa. Pharmacoeconomics 34, 403–417. doi: 10.1007/s40273-015-0356-x
Garuoliene, K., Alonderis, T., and Marcinkevic, M. (2010). Pharmaceutical policy and the effects of the economic crisis: Lithuania. Eurohealth 17, 1–4.
Garuoliene, K., Godman, B., Gulbinoviè, J., Wettermark, B., and Haycox, A. (2011). European countries with small populations can obtain low prices for drugs: Lithuania as a case history. Expert Rev Pharmacoecon Outcomes Res. 11, 343–349. doi: 10.1586/erp.11.24
Ghinea, N., Kerridge, I., and Lipworth, W. If we don't Talk About Value, Cancer Drugs Will Become Terminal for Health Systems [Internet]. Available online at: http://theconversation.com/if-we-dont-talk-about-value-cancer-drugs-will-become-terminal-for-health-systems-44072 (Accessed on Oct 2015).
Godman, B., Bishop, I., Finlayson, A. E., Campbell, S., Kwon, H.-Y., and Bennie, M. (2013b). Reforms and initiatives in Scotland in recent years to encourage the prescribing of generic drugs, their influence and implications for other countries. Expert Rev Pharmacoecon Outcomes Res. 13, 469–482. doi: 10.1586/14737167.2013.820956
Godman, B., De Bruyn, K., Miranda, J., Raschi, E., Bennie, M., and Barbui, C. (2013a). Generic atypical antipsychotic drugs in Belgium: their influence and implications. J. Comp. Eff. Res. 2, 551–561. doi: 10.2217/cer.13.75
Godman, B., Malmström, R. E., Diogene, E., Gray, A., Jayathissa, S., and Timoney, A. (2015). Are new models needed to optimise the utilisation of new medicines to sustain healthcare systems? Expert Rev. Clin. Pharmacol. 8, 77–94. doi: 10.1586/17512433.2015.990380
Godman, B., Malmström, R. E., Diogene, E., Jayathissa, S., McTaggart, S., Cars, T., et al. (2014b). Dabigatran - a continuing exemplar case history demonstrating the need for comprehensive models to optimize the utilization of new drugs. Front. Pharmacol. 5:109. doi: 10.3389/fphar.2014.00109
Godman, B., Petzold, M., Bennett, K., Bennie, M., Bucsics, A., Finlayson, A. E., et al. (2014a). Can authorities appreciably enhance the prescribing of oral generic risperidone to conserve resources? Findings from across Europe and their implications. BMC Med. 12:98. doi: 10.1186/1741-7015-12-98
Godman, B., Shrank, W., Andersen, M., Berg, C., Bishop, I., Burkhardt, T., et al. (2010a). Policies to enhance prescribing efficiency in europe: findings and future implications. Front. Pharmacol. 1:141. doi: 10.3389/fphar.2010.00141
Godman, B., Shrank, W., Andersen, M., Berg, C., Bishop, I., Burkhardt, T., et al. (2010b). Comparing policies to enhance prescribing efficiency in Europe through increasing generic utilization: changes seen and global implications. Expert Rev. Pharmacoecon. Outcomes Res. 10, 707–722. doi: 10.1586/erp.10.72
Gower, E., Estes, C. C., Hindman, S., Razavi-Shearer, K., and Razavi, H. (2014). Global epidemiology and genotype distribution of the hepatitis C virus. J. Hepatol. 61, S45–S57. doi: 10.1016/j.jhep.2014.07.027
Hatzakis, A., Wait, S., Bruix, J., Buti, M., Carballo, M., Cavaleri, M., et al. (2011). The state of hepatitis B and C in Europe: report from the hepatitis B and C summit conference. J. Viral Hepat. 18(Suppl. 1), 1–16. doi: 10.1111/j.1365-2893.2011.01499.x
Hesse, U., Godman, B., Petzold, M., Martin, A., and Malmström, R. (2013). Impact of delisting ARBs, apart from losartan, on ARB utilisation patterns in Denmark: implications for other countries. Appl. Heal Econ. Heal Policy 11, 677–685. doi: 10.1007/s40258-013-0059-4
Hézode, C., Fontaine, H., Dorival, C., Larrey, D., Zoulim, F., Canva, V., et al. (2013). Triple therapy in treatment-experienced patients with HCV-cirrhosis in a multicentre cohort of the French Early Access Programme (ANRS CO20-CUPIC) - NCT01514890. J. Hepatol. 59, 434–441. doi: 10.1016/j.jhep.2013.04.035
Hézode, C., Fontaine, H., Dorival, C., Zoulim, F., Larrey, D., Canva, V., et al. (2014). Effectiveness of telaprevir or boceprevir in treatment-experienced patients with HCV genotype 1 infection and cirrhosis. Gastroenterology 147, 132–142.e4. doi: 10.1053/j.gastro.2014.03.051
Hill, A., Khoo, S., Fortunak, J., Simmons, B., and Ford, N. (2014). Minimum costs for producing hepatitis C direct-acting antivirals for use in large-scale treatment access programs in developing countries. Clin. Infect. Dis. 58, 928–936. doi: 10.1093/cid/ciu012
Hoebert, J. M., Mantel-Teeuwisse, A. K., van Dijk, L., Bijlsma, J. W. J., and Leufkens, H. G. M. (2012). Do rheumatoid arthritis patients have equal access to treatment with new medicines? Tumour necrosis factor-alpha inhibitors use in four European countries. Health Policy 104, 76–83. doi: 10.1016/j.healthpol.2011.10.011
Hofmann, W. P., Sarrazin, C., and Zeuzem, S. (2012). Current standards in the treatment of chronic hepatitis C. Dtsch. Arztebl. Int. 109, 352–358. doi: 10.3238/arztebl.2012.0352
Hope, V. D., Eramova, I., Capurro, D., and Donoghoe, M. C. (2014). Prevalence and estimation of hepatitis B and C infections in the WHO European Region: a review of data focusing on the countries outside the European Union and the European Free Trade Association. Epidemiol. Infect. 142, 270–286. doi: 10.1017/S0950268813000940
Hughes-Wilson, W., Palma, A., Schuurman, A., and Simoens, S. (2012). Paying for the Orphan Drug System: break or bend? Is it time for a new evaluation system for payers in Europe to take account of new rare disease treatments? Orphanet. J. Rare Dis. 7:74. doi: 10.1186/1750-1172-7-74
Iyengar, S., Tay-Teo, K., Vogler, S., Beyer, P., Wiktor, S., de Joncheere, K., et al. (2016). Prices, costs, and affordability of new medicines for Hepatitis C in 30 countries: an economic analysis. PLoS med. 13:e1002032. doi: 10.1371/journal.pmed.1002032
Jönsson, B., Ramsey, S., and Wilking, N. (2014). Cost effectiveness in practice and its effect on clinical outcomes. J. Cancer Policy 2, 12–21. doi: 10.1016/j.jcpo.2014.02.001
Kantarjian, H. M., Fojo, T., Mathisen, M., and Zwelling, L. A. (2013). Cancer drugs in the United States: Justum Pretium–the just price. J. Clin. Oncol. 31, 3600–3604. doi: 10.1200/JCO.2013.49.1845
Kohli, A., Shaffer, A., Sherman, A., and Kottilil, S. (2014). Treatment of Hepatitis C. JAMA. 312, 631. doi: 10.1001/jama.2014.7085
Lagging, M., Duberg, A.-S., Wejstål, R., Weiland, O., Lindh, M., Aleman, S., et al. (2012). Treatment of hepatitis C virus infection in adults and children: updated Swedish consensus recommendations. Scand. J. Infect. Dis. 44, 502–521. doi: 10.3109/00365548.2012.669045
Lemoine, M., and Asia, E. (2014). Hepatitis C, A Global Issue: access to care and new therapeutic and preventive approaches in resource-constrained areas. Semin. Liver Dis. 34, 89–97 doi: 10.1055/s-0034-1371082
Leroy, V., Serfaty, L., Bourlière, M., Bronowicki, J.-P., Delasalle, P., Pariente, A., et al. (2012). Protease inhibitor-based triple therapy in chronic hepatitis C: guidelines by the French Association for the Study of the Liver. Liver Int. 32, 1477–14492. doi: 10.1111/j.1478-3231.2012.02856.x
Lo Re, V. III., Teal, V., Localio, A., Amorosa, V., Kaplan, D., and Gross, R. (2011). Relationship between adherence to hepatitis C virus therapy and virologic outcomes: a cohort study. Annals of internal medicine. Ann. Intern. Med. 155, 353–360. doi: 10.7326/0003-4819-155-6-201109200-00003
Lozano, R., Naghavi, M., Foreman, K., Lim, S., Shibuya, K., Aboyans, V., et al. (2012). Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380, 2095–2128. doi: 10.1016/S0140-6736(12)61728-0
Malmström, R. E., Godman, B. B., Diogene, E., Baumgärtel, C., Bennie, M., Bishop, I., et al. (2013). Dabigatran - a case history demonstrating the need for comprehensive approaches to optimize the use of new drugs. Front. Pharmacol. 4:39. doi: 10.3389/fphar.2013.00039
Manns, M. P., Pockros, P. J., Norkrans, G., Smith, C. I., Morgan, T. R., Häussinger, D., et al. (2013). Long-term clearance of hepatitis C virus following interferon α-2b or peginterferon α-2b, alone or in combination with ribavirin. J. Viral Hepat. 20, 524–529. doi: 10.1111/jvh.12074
Manzano-Robleda, M. C., Ornelas-arroyo, V., Barrientos-gutiérrez, T., Méndez-sánchez, N., Uribe, M., and Chávez-tapia, N. C. (2015). Boceprevir and telaprevir for chronic genotype 1 hepatitis C virus infection. A systematic review and meta-analysis. Ann. Hepatol. 14, 46–57.
Mathurin, P. (2013). HCV burden in Europe and the possible impact of current treatment. Dig. Liver Dis. 45, S314–S317. doi: 10.1016/j.dld.2013.07.009
Maticic, M. (2014). A national multidisciplinary healthcare network for treatment of hepatitis C in people who inject drugs in Slovenia. BMC Infect Dis. 14(Suppl 6):S6. doi: 10.1186/1471-2334-14-S6-S6
McGowan, C. E., Monis, A., Bacon, B. R., Mallolas, J., Goncales, F. L., Goulis, I., et al. (2013). A global view of hepatitis C: physician knowledge, opinions, and perceived barriers to care. Hepatology 57, 1325–1332. doi: 10.1002/hep.26246
McHutchison, J. G., Manns, M., Patel, K., Poynard, T., Lindsay, K. L., Trepo, C., et al. (2002). Adherence to combination therapy enhances sustained response in genotype-1–infected patients with chronic hepatitis C. Gastroenterology 123, 1061–1069. doi: 10.1053/gast.2002.35950
McHutchison, J., Stuart, C., Schiff, E., Shiffman, M., Lee, W., and Rustgi, V. (1998). Interferon alfa-2b alone or in combination with ribavirin as initial treatment for chronic hepatitis C. NEJM 339, 1485–1492. doi: 10.1056/NEJM199811193392101
Messina, J. P., Humphreys, I., Flaxman, A., Brown, A., Cooke, G. S., Pybus, O. G., et al. (2014). Global distribution and prevalence of hepatitis C virus genotypes. Hepatology 61, 77–87. doi: 10.1002/hep.27259
Messori, A. (2015a). Newest treatments for hepatitis C: how can we manage sustainability? Clin. Infect. Dis. 16, 1891–1892. doi: 10.1093/cid/civ667
Messori, A. (2015b). Value-based pricing is inadequate for both high budget-impact drugs and orphan drugs: exploring original methods to overcome this limitation by adjusting prices according to the number of potential patients. BMJ 351:h4988.
Mohd Hanafiah, K., Groeger, J., Flaxman, A. D., and Wiersma, S. T. (2013). Global epidemiology of hepatitis C virus infection: new estimates of age-specific antibody to HCV seroprevalence. Hepatology 57, 1333–1342. doi: 10.1002/hep.26141
Montazerhodjat, V., Weinstock, D. M., and Lo, A. W. (2016). Buying cures versus renting health: financing health care with consumer loans. Sci. Transl. Med. 8, 327ps6. doi: 10.1126/scitranslmed.aad6913
Moon, J. C., Godman, B., Petzold, M., Alvarez-Madrazo, S., Bennett, K., Bishop, I., et al. (2014). Different initiatives across Europe to enhance losartan utilization post generics: impact and implications. Front. Pharmacol. 5:219. doi: 10.3389/fphar.2014.00219
Nolte, E., and Corbett, J. International Variation in Drug Usage Variation: An Exploratory Analaysis of the “Causes” of Variation [Internet]. [cited 2015 Mar 8]. Available online at: http://www.rand.org/pubs/research_reports/RR899.html
Norton, A. (2015). Hepatitis C Drugs Will ‘Strain Budgets’ at Current Prices: Study - The New Therapies Have Remarkably High Cure Rates. Available online at: URL: http://consumer.healthday.com/infectious-disease-information-21/hepatitis-news-373/hepatitis-c-drugs-will-strain-budgets-at-current-prices-study-697479.html
Orlent, H., Deltenre, P., Francque, S., Laleman, W., Moreno, C., Bourgeois, S., et al. (2012). Update of the Belgian Association for the Study of the Liver guidelines for the treatment of chronic hepatitis C genotype 1 with protease inhibitors. Acta Gastroenterol. Belg. 75, 245–259.
Papastergiou, V., and Karatapanis, S. (2015). Current status and emerging challenges in the treatment of hepatitis C virus genotypes 4 to 6. World J. Clin. Cases. 3, 210–220. doi: 10.12998/wjcc.v3.i3.210
Phelan, M., and Cook, C. (2014). A treatment revolution for those who can afford it? Hepatitis C treatment: new medications, profits and patients. BMC Infect Dis. 14(Suppl 6):S5. doi: 10.1186/1471-2334-14-S6-S5
Poynard, T., Marcellin, P., Lee, S. S., Niederau, C., Minuk, G. S., Ideo, G., et al. (1998). Randomised trial of interferon alpha2b plus ribavirin for 48 weeks or for 24 weeks versus interferon alpha2b plus placebo for 48 weeks for treatment of chronic infection with hepatitis C virus. International Hepatitis Interventional Therapy Group (IHIT). Lancet 352, 1426–1432.
Putrik, P., Ramiro, S., Kvien, T. K., Sokka, T., Pavlova, M., Uhlig, T., et al. (2014). Inequities in access to biologic and synthetic DMARDs across 46 European countries. Ann. Rheum. Dis. 73, 198–206. doi: 10.1136/annrheumdis-2012-202603
Ramachandran, P., Fraser, A., Agarwal, K., Austin, A., Brown, A., Foster, G. R., et al. (2012). UK consensus guidelines for the use of the protease inhibitors boceprevir and telaprevir in genotype 1 chronic hepatitis C infected patients. Aliment. Pharmacol. Ther. 35, 647–662. doi: 10.1111/j.1365-2036.2012.04992.x
Schalm, S. W., Hansen, B. E., Chemello, L., Bellobuono, A., Brouwer, J. T., Weiland, O., et al. (1997). Meta-analysis of individual patient data from European centers. J. Hepatol. 26, 961–966. doi: 10.1016/S0168-8278(97)80103-1
Senior, M. (2014). Sovaldi makes blockbuster history, ignites drug pricing unrest. Nat. Biotechnol. 32, 501–502. doi: 10.1038/nbt0614-501
Simoens, S., Picavet, E., Dooms, M., Cassiman, D., and Morel, T. (2013). Cost-effectiveness assessment of orphan drugs: a scientific and political conundrum. Appl. Health Econ. Health Policy. 11, 1–3. doi: 10.1007/s40258-012-0004-y
Thein, H.-H., Yi, Q., Dore, G. J., and Krahn, M. D. (2008). Estimation of stage-specific fibrosis progression rates in chronic hepatitis C virus infection: a meta-analysis and meta-regression. Hepatology 48, 418–431. doi: 10.1002/hep.22375
Trooskin, S. B., Reynolds, H., and Kostman, J. R. (2015). Access to costly new hepatitis C drugs: medicine, money, and advocacy. Clin. Infect. Dis. 61, 1825–1830. doi: 10.1093/cid/civ677
van de Ven, N., Fortunak, J., Simmons, B., Ford, N., Cooke, G. S., Khoo, S., et al. (2014). Minimum target prices for production of direct-acting antivirals and associated diagnostics to combat Hepatitis C Virus. Hepatology 61, 1174–1182. doi: 10.1002/hep.27641
Vogler, S., Zimmermann, N., Habl, C., and Mazag, J. (2013). The role of discounts and loss leaders in medicine procurement in Austrian hospitals - a primary survey of official and actual medicine prices. Cost Effect. Resour. Alloc. 11:15. doi: 10.1186/1478-7547-11-15
Vonèina, L., Strizrep, T., Godman, B., Bennie, M., Bishop, I., Campbell, S., et al. (2011). Influence of demand-side measures to enhance renin-angiotensin prescribing efficiency in Europe: implications for the future. Expert Rev. Pharmacoecon. Outcomes Res. 11, 469–479. doi: 10.1586/erp.11.42
Wedemeyer, H., Dore, G. J., and Ward, J. W. (2015). Estimates on HCV disease burden worldwide - filling the gaps. J. Viral Hepat. 22(Suppl. 1), 1–5. doi: 10.1111/jvh.12371
Westbrook, R. H., and Dusheiko, G. (2014). Natural history of hepatitis C. J. Hepatol. 61(1 Suppl.), S58–S68. doi: 10.1016/j.jhep.2014.07.012
Wettermark, B., Godman, B., Jacobsson, B., and Haaijer-Ruskamp, F. M. (2009). Soft regulations in pharmaceutical policy making: an overview of current approaches and their consequences. Appl. Health Econ. Health Policy 7, 137–147. doi: 10.1007/BF03256147
World Health Organisation (2012). The 10 Leading Causes of Death by Country Income Group. Available onlie at: http://www.who.int/mediacentre/factsheets/fs310/en/index1.html.
Yehia, B. R., Schranz, A. J., Umscheid, C. A., and Lo Re, V. (2014). The treatment cascade for chronic hepatitis C virus infection in the United States: a systematic review and meta-analysis. PLoS ONE 9:e101554. doi: 10.1371/journal.pone.0101554
Keywords: boceprevir, cross national drug utilization study, demand-side measures, Hepatitis C, introduction new medicines, sofosbuvir, telaprevir
Citation: de Bruijn W, Ibáñez C, Frisk P, Bak Pedersen H, Alkan A, Vella Bonanno P, Brkičić LS, Bucsics A, Dedet G, Eriksen J, Fadare JO, Fürst J, Gallego G, Godói IP, Guerra Júnior AA, Gürsöz H, Jan S, Jones J, Joppi R, Kerman S, Laius O, Madzikwa N, Magnússon E, Maticic M, Markovic-Pekovic V, Massele A, Ogunleye O, O'Leary A, Piessnegger J, Sermet C, Simoens S, Tiroyakgosi C, Truter I, Thyberg M, Tomekova K, Wladysiuk M, Vandoros S, Vural EH, Zara C and Godman B (2016) Introduction and Utilization of High Priced HCV Medicines across Europe; Implications for the Future. Front. Pharmacol. 7:197. doi: 10.3389/fphar.2016.00197
Received: 29 April 2016; Accepted: 21 June 2016;
Published: 22 July 2016.
Edited by:
Dominique J. Dubois, Université Libre de Bruxelles, BelgiumReviewed by:
Domenico Criscuolo, Genovax, ItalyMichael Hans Thiede, Health Economics and Policy, Germany
Copyright © 2016 de Bruijn, Ibáñez, Frisk, Bak Pedersen, Alkan, Vella Bonanno, Brkičić, Bucsics, Dedet, Eriksen, Fadare, Fürst, Gallego, Godói, Guerra Júnior, Gürsöz, Jan, Jones, Joppi, Kerman, Laius, Madzikwa, Magnússon, Maticic, Markovic-Pekovic, Massele, Ogunleye, O'Leary, Piessnegger, Sermet, Simoens, Tiroyakgosi, Truter, Thyberg, Tomekova, Wladysiuk, Vandoros, Vural, Zara and Godman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Brian Godman, YnJpYW4uZ29kbWFuQGtpLnNl