 Mihajlo Jakovljevic
Mihajlo Jakovljevic Thomas E. Getzen
Thomas E. Getzen- 1Faculty of Medical Sciences, University of Kragujevac, Kragujevac, Serbia
- 2Risk, Insurance, and Healthcare Management Department, Temple University, Philadelphia, PA, USA
Historical Patterns of Global Health Spending
Over the past century medical technology has provided bold gains extending human longevity for almost several decades in most welfare economies worldwide. These public health victories came at the cost of huge increase in health spending. The USA, the largest health care market where total health expenditure (THE) grew from 4% of GDP to 15%, may serve as an example of such changes. The secular trend consisting of rising wages and incomes constitutes major factor in the rising resources dedicated to the medical care. Business cycle booms and recessions affected health care spending slowly and with a significant lag. In this sense health expenditures should not be compared to short term, quarterly or yearly fluctuations in Gross Domestic Product (GDP) but correlates well to “smoothed” income over the previous 3–6 years (Getzen, 1990).
Growth of health expenditure is driven by several underlying issues: population birth rates, per-capita income, inflation and so called “excess growth” that is mostly explained by medical technology advances or increased patient demand for services. This “excess growth” is responsible for raising the share of health care in national GDP, and thus challenging fiscal sustainability. Evidence of excess growth is seen in health insurance premiums that persistently rise faster than tax revenues or wages. Isolated excess cost growth was the key underlying reason for the surmountable surge in health care costs visible in the United States since the late 1950s. Unlike the contemporary post WWII era, previous historical records testify of stable medical costs of about 4% of GDP from 1929 to the late 1950s. U.S. Census records of employment in clinical medicine and published consumer expenditure evidence from 1850–1950 show that these costs were mostly keeping pace with wages. If they were slightly exceeding wages it was only about 0.5% annually thus it took more than a century for them to double, much slower than the quadrupling from 1960 to 2000 (Getzen, 2000). Major causes of such a sudden rise in health expenditures were huge economic development, distinctively extended longevity, control of contagious diseases, rising availability of income used to fund research in medicine, effective financing instruments, and ultimately significant discoveries in medical technologies that supported public willingness for further investment into potential novel biological drugs, implants, robotic surgery, radiation therapy, organ transplants, and other wonder technologies (Getzen, 2014).
With several decades delay, due to dissemination of knowledge and improved societal welfare across the globe, similar developments began at the far smaller scale in a large number of low and middle income world economies. Among 160 such nations in the beginning of 1990s long term trends have revealed 16 countries which made greater investments in health care and its core outcomes than most comparable nations. These countries were described by Goldman-Sachs as the world's leading emerging markets. They are listed under the acronyms BRICS (Brazil, Russia, India, China, South Africa) and Next Eleven (N-11: Bangladesh, Egypt, Indonesia, Iran, South Korea, Mexico, Nigeria, Pakistan, the Philippines, Turkey, and Vietnam). This ongoing evolution will most likely shape the appearance of global demand and supply of medical services in XXI century and we believe that therefore it deserves closer examination.
Growth of Health Care Spending in Low and Middle Income Countries Since 1995
The last two decades have been particularly dynamic due to ending the Cold War and accelerated pace of globalization. Contemporary evolution was promising for most nations with average world THE rising from 5.7 to 6.8% GDP [a 19.3% gain or approximately 1% yearly increase over 19 years (Table 1)]. Since 1995 World Health Organization (WHO) has established and disseminated National Health Accounts (NHA) system worldwide. These efforts allowed reliable international comparison of financial flows among national health systems with diverse historical legacies. The World Bank (WB) introduced the measure of gross national income (GNI) classification of countries in 1987 with their Atlas method and GNI per capita indexed in US$ currency (World Bank Income Groups, 2015). Availability of national income per capita strongly influences health expenditure. The correlation is straightforward with a secular trend visible in long time horizons in most world regions. We applied historical lists of WB income classification to reveal patterns in global health spending. Participation of 160 low and middle income countries (as defined by WB in 1995) in global health spending (in million const. 2005 $US) was 10.7%. Nineteen years later the world was a much different place. Global welfare of nations recorded bold increases while 23 countries crossed the WB threshold for high income economies. The remaining 137 low and middle income countries (as defined by WB in 2013) were now spending 14.6% of global THE expressed in millions of constant 2005 $US. The landscape of national medical spending has evolved in favor of developing regions. The 160 countries classified as low and middle by WB in 1995 grew from 26.1% of global THE in 1995 to 39.7% in 2013. While high income economies still dominate the global landscape of medical spending, the growth of emerging economies has reduced their share of the total.
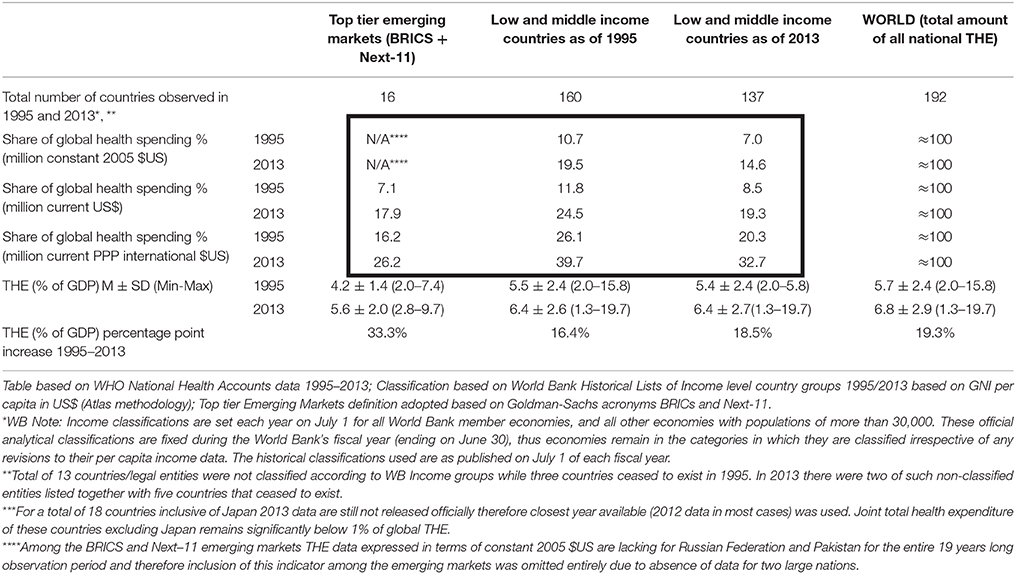
Table 1. Transformation of Global Total Health Expenditure (THE) 1995–2013.
Causes of Changes and Leadership of BRICs + Next-11 Emerging Nations
Jim O'Neil's grouping of BRICs was driven primarily designating those whose nominal and purchase power parity (PPP) adjusted GDP growth rates significantly outpaced those of most OECD nations before and during the worldwide economic recession. Similar ongoing development characterizes another group, identified by Goldman-Sachs' as the “Next Eleven.” Profound changes with deep and lasting impact to the global demand for and provision of healthcare services and associated expenditure have occurred. Rapid expansion of civil middle class in most of these societies has been a major underlying factor (Jakovljevic, 2015). Substantial gains in overall welfare are reflected in the expansion of health insurance coverage and diversity of medical services provided. Growth of purchasing power effectively improved affordability of advanced medical care that remains out-of-pocket expense. We witness continuing movement of global growth in health care markets from the established mature economies toward the emerging ones. Slower economic growth in most saturated high-income markets is a contributing factor. Consumer demand for medical services remains larger in traditional wealthy countries, but their share has been decreasing steadily for at least two decades.
Total amount of health care spending among BRICS and Next-11 nations became approximately six fold stronger since 1995. Share of Global Health Spending (million current US$) of these emerging nations grew almost two and a half times. This pace of development is far faster compared to that of vast majority of remaining low and middle income countries across the globe. If we observe per capita health spending it appears that general government expenditure on health and private expenditure is consistently stronger among BRICS compared to N-11. Such a historical trend was actually present prior to 1990s and spending differentials continued to exist as paths diverted even further in recent years. Out-of-pocket (OOP) expenditure on health is a significant outlier in this regard. Although both country group averages were similar at the start, N-11 OOP spending soon exceeded BRICs. These facts indicate better success rates among the BRICs in terms of reimbursement policies and insurance coverage over the past 20 years (Jakovljevic, 2014).
Prospects for the Future
Observation of health spending trends over 20 years is still insufficient to understand a “medical transformation” taking place in major national health systems worldwide. Limitations to our judgment might be imposed by reliability and comparability of large international datasets as well (Rayne, 2013). Nevertheless contemporary transformation of global health spending lays grounds for some forecasts on likely scenarios for the future. Low and middle income countries are likely to become more relevant contributor to the global health care market in the long run. Minor proportion of these countries will likely become high income economies over the next decade. Vast majority of them will continue to experience serious obstacles to the fiscal feasibility of their national health systems. Crucial challenges will remain population aging, prosperity disease and rapid urbanization leaving vulnerable rural areas. Universal health insurance coverage will still be a distant policy target for most of these governments with the notable exception of Russian Federation (Jakovljevic et al., in press). Large out of pocket expenses and informal payments will leave ordinary citizens, living close to the poverty line, vulnerable to the illness-induced catastrophic household expenditure (McIntyre et al., 2006). In some world regions with still young populations, communicable diseases control and satisfactory maternal and neonatal medical care provision shall still be a long way ahead (Barik and Thorat, 2015). Regardless of all the aforementioned weaknesses of developing world regions, it appears that most successful among these nations will become even more important players in global health arena. Heavily domination of People's Republic of China (He and Meng, 2016) followed by India in medical spending worldwide will exceed that of all other emerging markets combined. As we approach 2050 it is highly likely that financing of health care in top tier emerging nations will converge toward OECD average in terms of its effectiveness and affordability of medical care to the ordinary citizen (Jakovljevic, 2016). Major imperatives for national policy makers shall remain how to achieve universal health coverage, what services would be covered by basic insurance package and at what cost. Future research in the field should primarily be focused on key causes of out-of-pocket medical spending growth, deepening social gap among the rich and poor communities leading to health inequalities and effectiveness of contemporary policies in low and middle income countries.
Data Report Methodology
Public data sources used were WHO issued Global Health Expenditure Database relying on NHA records: http://apps.who.int/nha/database/Select/Indicators/en and World Bank (WB) Income Groups; Historical country classifications based on Atlas method: http://data.worldbank.org/about/country-and-lending-groups. Filters applied to these extensive data sources were indicators referring to the national level and Global Total Health Expenditure (THE) expressed in following units: million constant 2005 $US, million current US$, million current PPP international $US and THE percentage share of national Gross Domestic Product available (GDP). Data were acquired based on reported values to the WHO and WB by the national authorities as well as independent assessments and calculations provided by WHO and WB and officially released in respective years. Readers are free to access and reuse these publicly available data at the links provided above.
Author Contributions
MJ and TG have jointly developed the research questions, study design, did all the calculations and prepared manuscript for this Data report. Therefore, they share the first authorship in this paper.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The Ministry of Education Science and Technological Development of the Republic of Serbia has funded the underlying study behind reported results through Grant OI 175014. Publication of results was not contingent to Ministry's censorship or approval.
References
Barik, D., and Thorat, A. (2015). Issues of unequal access to public health in India. Front. Public Health 3:245. doi: 10.3389/fpubh.2015.00245
Getzen, T. (1990). “Macro forecasting of national health expenditures,” in Advances in Health Economics and Health Services Research, Vol. 11, eds L. Rossiter and R. Scheffler (New York, NY: Jai Press), 27–48.
Getzen, T. (2000). Forecasting health expenditures: short, medium and long (long) term. J. Health Care Finance 26, 56–72.
Getzen, T. (2014). “Getzen macroeconomic dynamics of health: lags and variability in mortality, employment and spending,” in Encyclopedia of Health Economics, Vol. 2, ed A. J. Culyer (San Diego, CA: Elsevier), 165–176.
He, J. A., and Meng, Q. (2016). Chinese National Health Care Reform: On the Mend? Available online at: http://repository.lib.ied.edu.hk/jspui/handle/2260.2/18545
Jakovljevic, M. (2014). The key role of leading emerging BRIC markets for the future of global health care. Ser. J. Exp. Clin. Res. 15, 139–143. doi: 10.2478/SJECR20140018
Jakovljevic, M. B. (2015). BRIC's growing share of global health spending and their diverging pathways. Front. Public Health 3:135. doi: 10.3389/fpubh.2015.00135
Jakovljevic, M. M. (2016). Comparison of historical medical spending patterns among the BRICS and G7. J. Med. Econ. 19, 70–77. doi: 10.3111/13696998.2015.1093493
Jakovljevic, M., Potapchikova, E., Popovich, L., Barik, D., McIntyre, D., and Getzen, T. (in press). Evolving health expenditure landscape of the BRICS nations. Health Econ.
McIntyre, D., Thiede, M., Dahlgren, G., and Whitehead, M. (2006). What are the economic consequences for households of illness and of paying for health care in low-and middle-income country contexts? Soc. Sci. Med. 62, 858–865. doi: 10.1016/j.socscimed.2005.07.001
Rayne, S. (2013). The Mess of International Health Care Cost Datasets. Available online at: http://www.americanthinker.com/articles/2013/11/the_mess_of_international_health_care_cost_datasets.html
World Bank Income Groups (2015). World Bank Income Groups. Available online at: http://data.worldbank.org/about/country-and-lending-groups
Keywords: low–middle income, developing world, third world, health expenditure, medical spending
Citation: Jakovljevic M and Getzen TE (2016) Growth of Global Health Spending Share in Low and Middle Income Countries. Front. Pharmacol. 7:21. doi: 10.3389/fphar.2016.00021
Received: 08 October 2015; Accepted: 25 January 2016;
Published: 12 February 2016.
Edited by:
Michael P. Jones, Macquarie University, AustraliaCopyright © 2016 Jakovljevic and Getzen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mihajlo Jakovljevic, c2lkYXJ0YWdvdGhhbWFAZ21haWwuY29t; amFrb3ZsamV2aWNtQG1lZGYua2cuYWMucnM=