
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Pediatr. , 03 March 2025
Sec. Pediatric Endocrinology
Volume 13 - 2025 | https://doi.org/10.3389/fped.2025.1499664
 Marion Garcia1,2Isabelle Oliver Petit3Camille Franchet4
Marion Garcia1,2Isabelle Oliver Petit3Camille Franchet4 Olivier Abbo5Audrey Cartault3
Olivier Abbo5Audrey Cartault3 Frédérique Savagner1,2,6*
Frédérique Savagner1,2,6*
Background: Cowden syndrome (CS) is a complex and rare hereditary disorder characterized by a high risk of developing both benign and malignant tumors. Germline variants in the PTEN gene lead to this autosomal dominant syndrome, which predisposes individuals to lesions of the skin and mucous membranes, as well as breast, thyroid, endometrial, and kidney cancers. Early identification of symptoms is essential for implementing effective therapeutic strategies, especially in managing thyroid cancer risk.
Case presentation: During a tonsillectomy in an 8-year-old boy, the surgeon incidentally noted a left lateralized thyroid swelling. The clinical picture of Cowden syndrome was further supported by the presence of macrocephaly and intellectual disability since birth along with rare and atypical thyroid disorder marked by a toxic adenoma. Genetic analysis of both the tissue and blood samples confirmed the diagnosis. The clinical manifestation of thyroid issues in a young child may indicate CS, a condition that is often poorly assessed by clinicians. Family history revealed that the boy's father and sister also carry the same heterozygous variant, presenting a spectrum of Cowden syndrome manifestations.
Conclusion: Molecular analysis of the PTEN gene should be considered in young patients with thyroid nodules or nodules associated with abnormal thyroid function test, even without clear evidence of Cowden syndrome, particularly if there is a family history of thyroid, breast, or hamartoma-related conditions.
Cowden syndrome (CS) is a rare genetic disease affecting 1/200,000 to 1/250,000 people worldwide transmitted through an autosomal dominant mode (1). This genodermatosis affecting both infants and adults is characterized by multiple hamartomas and a high-risk predisposition to cancer. It is associated to germline loss of function variants in the PTEN gene as a tumor suppressor regulating cell growth and division through the P13K/AKT/mTOR signaling pathway (2). The Cowden syndrome was first described in 1963 by Lloyd and Dennis in a 20-year-old patient named Rachel Cowden who was diagnosed with thyroid, breast and oral mucosa lesions (3, 4). In childhood, presentation includes macrocephaly for nearly 95% of cases, as a major criteria defined by the National Comprehensive Cancer Network (NCCN) (5–7). Other minor criteria such as intellectual disability, lipomas, thyroid goiter may point to this diagnosis when two of them were combined, especially for affected relatives without macrocephaly. Benign thyroid lesions are the most common minor criterion (75% of cases) while thyroid cancer affects approximatively 24% of all CS patients (8). In adults, thyroid lesions predominantly manifest in women at a younger age compared to sporadic nodules whereas no correlation with gender or puberty has been noted for children and adolescents (9, 10). Notably, children with CS exhibit significant thyroid involvement with up to 50% diagnosed with benign lesions at a mean age of 9 years and a incidence of 4%–12%, mainly of the follicular pattern (8). Thyroid hormone profiles are generally normal without anti-thyroid antibodies although hormonal dysfunction may arise if thyroid nodules are diagnosed late (10). To date, if goiter and some grave's diseases has been described in CS, only one case of non-autoimmune hyperthyroidism has been documented in the literature (12–14).
Due to the risk of thyroid cancer, thyroidectomy should be considered for PTEN-positive patients upon detection of thyroid nodules, despite no discernible difference in the natural history of thyroid cancer (1, 11). A benign thyroid disorder can progress to a malignant tumor in the presence of somatic cancer driver genes as TSHR for hyperfunctioning nodules, with the risk for cancer identified only through aggressive histological features (15–17). It is particularly true for adults whereas for children, thyroidectomy should be considered depending on the size of the nodule and the location of the mutation (18). Our case underscores the importance of early CS diagnosis that may initially manifest as a simple thyroid dysfunction in childhood but present a large thyroid nodule with a risk of cancer development pressing early thyroidectomy. Recent comprehensive guidelines advocate for surveillance starting at age 18 for thyroid cancer risk in pediatric patients with CS and susceptibility to thyroid disorders (11). However, additional research is needed to improve clinical outcomes for affected individuals and understand the global risk of carcinogenesis.
An 8-year-old boy, placed in foster care at birth, was referred to a surgeon due to severe sleep apnea syndrome persisting for 2 years. During the tonsil removal, a left-sided cervical swelling in the thyroid region was discovered, confirmed by ultrasound to be a isthmic 45 mm thyroid nodule EU-TIRADS 3 with a 2%–4% risk of malignancy (19). Despite the current recommendations (20), thyroid scintigraphy was not performed as first line ultrasound imaging identifying a large nodule was considered sufficient. Fine-needle aspiration cytology classified the nodule as benign follicular features [Bethesda class II (21),]. Definitive histology following thyroid surgery confirmed a large follicular adenoma (Figure 1A). Indeed, the thyroid gland contained a solitary tumor, well delimitated by a thin capsule, with no evidence of capsular or vascular invasion. The nodule was composed of normofollicular and macrofollicular areas. Cytologically, no nuclear features of papillary thyroid carcinoma appeared. Next Generation Sequencing was secondarily performed on the nodule and an alteration in PTEN gene appeared, corresponding to the patient's germline mutation [i.e., p.(Lys125Thr) with a variant allele frequency of 74.4%]. Moreover, no additional pathogenic variant neither in RAF and RAS nor in TSHR and GNAS1 genes was shown.
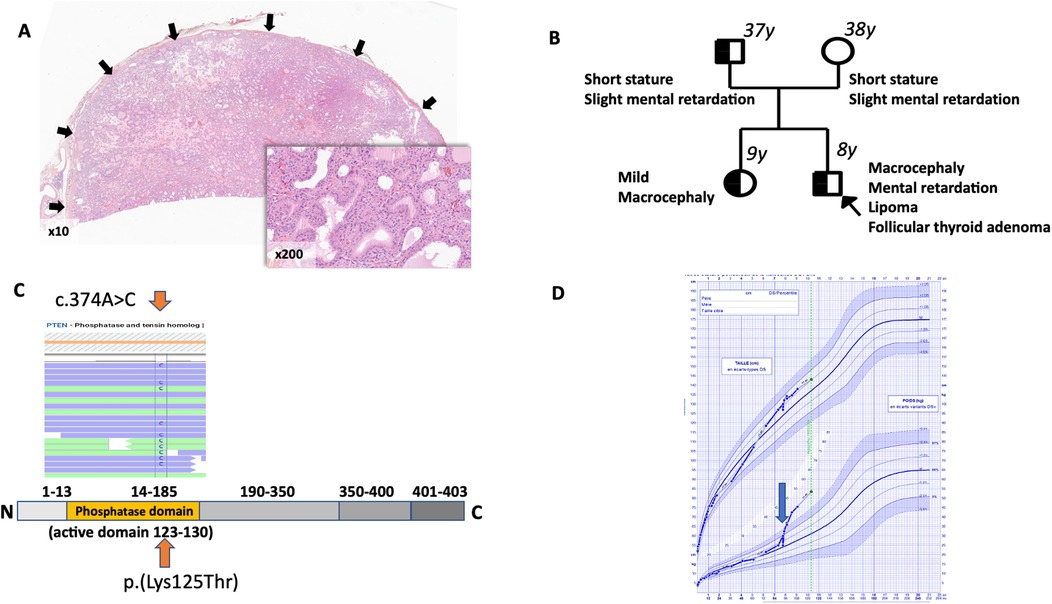
Figure 1. (A) histologic examination of thyroid tumor (magnification ×10): follicular adenoma is fully delimitated by a thin capsule (arrows) with neither capsular nor vascular invasion. Insert (magnification ×200): This nodule is being characterized by a normo- and macrofollicular growth pattern with no nuclear features of papillary thyroid carcinoma. (B) Localization of the PTEN variant. Germline heterozygous variant c.374A>C was detected (orange arrow) by Next Generation Sequencing (Illumina, custom thyroid cancer panel) in exon 5 of the PTEN gene (LRG_492, NM_177438.3); The sequencing depth was 874× and 786× respectively for blood (allele frequency 49.8%) and tissue (allele frequency 74.4%) samples (Integrative Genomic Viewer Software). No additional PTEN variants were identified at the somatic level. (C) Family pedigree. Individuals screened for PTEN germline variant are indicated by a black border with age at molecular diagnosis for each patient explored. Heterozygous positive variants are indicated by a black filling. Clinical phenotypes are associated to each patient. The proband is marked with an arrow. (D) Growth curve of the male child. At 8 years old growth increased (+4.7 SD in weight) was noted (blue arrow).
The foster family had not reported particular issues in childhood. However, two months prior to the tonsil surgery, clinical signs of hyperthyroidism caused by the hypersecreting nodule were retrospectively identified. These included heavy sweating, tremors and nervousness which were consistent with the hormonal assessment conducted after tonsil surgery: TSH of 0.01 IU/ml (reference range: 0.27–0.42 IU/ml), FT4 of 16.1 pg/ml (reference range: 9.3–17 pg/ml), FT3 of 6 pg/ml (reference range: 2–4.4) and negative TSHR and TPO antibodies. Calcitonin level was not measured. Pharmacological treatment with methimazole at 0.5 mg/kg per day for 6 months, achieved balanced euthyroidism within one month. Clinical investigations revealed primary nonprogressive macrocephaly (+2SD) associated with hydramnios at birth, mild axial hypotonia, strabismus, minimal cutaneous manifestations and slight intellectual disability consistent with NCCN criteria for CS diagnosis (5).
Due to foster care status for the proband and his sister, biological parents were subsequently evaluated. Both non-consanguineous parents exhibited mild intellectual disability and short stature. At the age of 36, the father has a head circumference of 60.1 cm (reference range: 52.5–58.5 cm) and presents with spondylolisthesis which could retrospectively be associated with PTEN-related vertebral hemangiomas (22). His sister displayed mild macrocephaly (+1SD) and tall stature and no neurodevelopmental delay. All patients have signed an informed consent. Genetic analysis via CGH-array was negative for both children. Next generation sequencing of a familial thyroid cancer gene panel (see Supplementary Table 1) revealed a heterozygous missense variant c.374A>C in exon 5 of the PTEN gene (NM_000314) resulting in the substitution of a basic lysine residue with an hydroxylic threonine residue p.(Lys125Thr) confirmed by sanger analysis (Figure 1B). This variant in the phosphatase tensin domain of the protein was referred as likely pathogenic (class 4) in LOVD and using missense predictive software (GeneBe, SIFT, Polyphen-2, Franklin, AlphaMissense, Revel and Clinpred) according to the American College of Medical Genetics classification. It was located in a hotspot region for mutations that abrogate PTEN's phosphatase activity and was not currently referenced in gnomAD exome or Clinvar databases (18). Molecular analysis confirmed the presence of this variant in his sister and father but not in his mother (Figure 1C). However, all relatives have had normal thyroid ultrasounds and TSH levels so far.
Given the size of the thyroid nodule and the presence of hyperthyroidism, a total thyroidectomy was performed 6 months after fine-needle aspiration cytology. Euthyroidism was achieved with a daily L-T4 dose of 112 µg. Hyperthyroidism was primarily caused by the delayed management of the thyroid mass. Due to euthyroidism following surgery and increased food requirements related to CS, a deviation in the growth curve was observed, with a +4.7 SD in weight (Figure 1D) associated to +1SD in height.
The incidental discovery of a benign thyroid lesion associated with hyperthyroidism in this 8-year-old boy has significantly impacted the medical care and surveillance of this index case within a Cowden syndrome family. Hyperthyroidism or toxic adenoma in CS have been described very rarely in the literature to date (14). Just as rarely, medullary thyroid cancer can coexist with hyperfunctioning goiter (23). However, in our case, macrocephaly did not warrant measuring calcitonin. In our case, normalization of thyroid hormone levels resulted in a significant shift in the growth curve in relation to metabolic syndrome and obesity observed for CS, despite insulin sensitivity (24). We postulate that hyperthyroidism may have mitigated the typical weight gain observed in CS patients during childhood (25). Euthyroidism obtained after thyroid surgery subsequently revealed an increase in adiposity, linked to PTEN-enhanced insulin signaling in the muscle and liver, as previously reported (24).
A total thyroidectomy has been recommended relative to the large thyroid nodule identified and the potential risk of thyroid cancer progression during adolescence (26). Recommendations for thyroid cancer surveillance vary among expert panels with a consensus on annual monitoring through neck palpation, thyroid ultrasound and serum TSH measurement starting at age 18 or 5–10 years before the age of the first known thyroid cancer case in the family (5, 11). However, ultrasound surveillance could be adapted based on initial results, especially to limit ultrasounds in children and adolescents (27). Children with PTEN-related syndromes are rarely at risk of developing hyperthyroidism except in case of concomitant Graves’ disease, as referred in the literature (13). Regular thyroid function monitoring is crucial for individuals with PTEN variants to rapidly manage any related issues. Recently, pathogenic variants in exon 5 of the PTEN gene have been associated with an increased cancer risk, prompting the consideration of starting surveillance from age 10 (28). Exon 5 encodes the core catalytic domain of the PTEN protein (active site between amino acid 123 and 130) and resulting mutations disrupt the pan-phosphatase (lipid and protein) activity that regulates the PI3K cascade (29, 30). Given the familial variant's location in exon 5, the boy's sister, who currently shown no nodules, undergoes annual follow-up.
Considering the prevalence of somatic PTEN variants in follicular adenomas and mostly benign thyroid lesions in CS, PTEN mutations may play a role in early neoplastic follicular cell growth that could explain the frequency of thyroid pathologies in CS (31, 32). Furthermore, the presence of follicular adenomas in children and young adults should raise suspicion of inherited conditions, primarily CS or DICER1 syndrome, necessitating family screening (33).
The risk for developing thyroid cancer as well as breast, kidney, endometrial and colorectal cancer is increased in both PTEN-positive adults and children, with the risk being higher in adults (26). The risk for developing other types of cancer remains comparable to that of the general population (34). The NCCN (v.2021) has established guidelines for surveillance once a PTEN gene mutation is identified, regardless of its location within the gene. This includes comprehensive clinical examination starting at age 18 or earlier if there is a cancer diagnosis in the family. Colonoscopy from age 35 and then every 5 years should be considered if symptomatic or if polyps are detected. Renal ultrasound from age 40, repeated every 1–2 years, can aid in early cancer detection. Dermatological, psychomotor and dental examinations may also be integrated into the surveillance protocol. Patient education on recognizing signs and symptoms of malignant tumor development is crucial due to the increased carcinogenic risk associated with the syndrome. Management strategies must be tailored accordingly, distinguishing this approach from that used for the general population.
In conclusion, the case of this 8-year-old boy illustrates an incidental finding of CS based on unusual hyperthyroidism and a challenging family history relative to foster cares. Multidisciplinary care and personalized medical attention are essential for managing the risk of malignant progression in this syndrome.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
The studies involving humans were approved by ALL patients have provided written informed consents, especially the legal guardians of both children, for genetic analysis and participation to this study and publication of this case report. The studies were conducted in accordance with the local legislation, the ethic commitee of the academic hospital of Toulouse and institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
MG: Writing – original draft. IO: Data curation, Investigation, Writing – review & editing. CF: Data curation, Formal Analysis, Methodology, Writing – review & editing. OA: Data curation, Investigation, Writing – review & editing. AC: Data curation, Investigation, Writing – review & editing. FS: Writing – review & editing, Writing – original draft.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We would like to thank Elisa Thoa and Mathieu Jimenez for their support for biological management.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2025.1499664/full#supplementary-material
1. Magaña M, Landeta-Sa AP, López-Flores Y. Cowden disease: a review. Am J Dermatopathol. (2022) 44:705. doi: 10.1097/DAD.0000000000002234
2. Saji M, Ringel MD. The PI3K-AKT-mTOR pathway in initiation and progression of thyroid tumors. Mol Cell Endocrinol. (2010) 321:20–8. doi: 10.1016/j.mce.2009.10.016
3. Szabo Yamashita T, Baky F, McKenzie TJ, Thompson GB, Farley D, Lyden ML, et al. Occurrence and natural history of thyroid cancer in patients with Cowden syndrome. Eur Thyroid J. (2020) 9:1–4. doi: 10.1159/000506422
4. Lloyd KM, Dennis M. Cowden’s disease. A possible new symptom complex with multiple system involvement. Ann Intern Med. (1963) 58:136–42. doi: 10.7326/0003-4819-58-1-136
5. Tischkowitz M, Colas C, Pouwels S, Hoogerbrugge N. Cancer surveillance guideline for individuals with PTEN hamartoma tumour syndrome. Eur J Hum Genet. (2020) 28:1387–93. doi: 10.1038/s41431-020-0651-7
6. Martín-Valbuena J, Gestoso-Uzal N, Justel-Rodríguez M, Isidoro-García M, Marcos-Vadillo E, Lorenzo-Hernández SM, et al. PTEN hamartoma tumor syndrome: clinical and genetic characterization in pediatric patients. Childs Nerv Syst. (2024) 40:1689–97. doi: 10.1007/s00381-024-06301-2
7. Macken WL, Tischkowitz M, Lachlan KL. PTEN hamartoma tumor syndrome in childhood: a review of the clinical literature. Am J Med Genet C Semin Med Genet. (2019) 181:591–610. doi: 10.1002/ajmg.c.31743
8. Hauser-Casamenti S, Hauser F, Lombardi T, Samson J. Syndrome de Cowden: présentation de 7 cas (2 ème partie). Med Buccale Chir Buccale. (2011) 17:147–65. doi: 10.1051/mbcb/2011108
9. Hoda SA. Diagnostic pathology and molecular genetics of the thyroid: a comprehensive guide for practicing thyroid pathology. Am J Clin Pathol. (2019) 152:115. doi: 10.1093/ajcp/aqz019
10. Tuli G, Munarin J, Mussa A, Carli D, Gastaldi R, Borgia P, et al. Thyroid nodular disease and PTEN mutation in a multicentre series of children with PTEN hamartoma tumor syndrome (PHTS). Endocrine. (2021) 74:632–7. doi: 10.1007/s12020-021-02805-y
11. Jonker LA, Lebbink CA, Jongmans MC, Nievelstein RA, Merks JH, Van Dijkum EN, et al. Recommendations on surveillance for differentiated thyroid carcinoma in children with PTEN hamartoma tumor syndrome. Eur Thyroid J. (2020) 9:234–42. doi: 10.1159/000508872
12. Patraquim C, Fernandes V, Martins S, Antunes A, Marques O, Carvalho JL, et al. A pediatric case of Cowden syndrome with Graves’ disease. Case Rep Pediatr. (2017) 2017:2750523. doi: 10.1155/2017/2750523
13. Manimaran S, Ramanathan R, Subramanian S. Pediatric challenges with Cowden syndrome and Graves’ disease: a case report. Cureus. (2024) 16:e58090. doi: 10.7759/cureus.58090
14. Starink TM, van der Veen JP, Arwert F, de Waal LP, de Lange GG, Gille JJ, et al. The Cowden syndrome: a clinical and genetic study in 21 patients. Clin Genet. (1986) 29:222–33. doi: 10.1111/j.1399-0004.1986.tb00816.x
15. Xu B, Ghossein R. Poorly differentiated thyroid carcinoma. Semin Diagn Pathol. (2020) 37:243–7. doi: 10.1053/j.semdp.2020.03.003
16. Macerola E, Poma AM, Vignali P, Basolo A, Ugolini C, Torregrossa L, et al. Molecular genetics of follicular-derived thyroid cancer. Cancers (Basel). (2021) 13:1139. doi: 10.3390/cancers13051139
17. Eszlinger M, Niedziela M, Typlt E, Jaeschke H, Huth S, Schaarschmidt J, et al. Somatic mutations in 33 benign and malignant hot thyroid nodules in children and adolescents. Mol Cell Endocrinol. (2014) 393:39–45. doi: 10.1016/j.mce.2014.05.023
18. Matreyek KA, Stephany JJ, Ahler E, Fowler DM. Integrating thousands of PTEN variant activity and abundance measurements reveals variant subgroups and new dominant negatives in cancers. Genome Med. (2021) 13:165. doi: 10.1186/s13073-021-00984-x
19. Russ G, Bonnema SJ, Erdogan MF, Durante C, Ngu R, Leenhardt L. European thyroid association guidelines for ultrasound malignancy risk stratification of thyroid nodules in adults: the EU-TIRADS. Eur Thyroid J. (2017) 6:225–37. doi: 10.1159/000478927
20. Durante C, Hegedüs L, Czarniecka A, Paschke R, Russ G, Schmitt F, et al. 2023 European thyroid association clinical practice guidelines for thyroid nodule management. Eur Thyroid J. (2023) 12:e230067. doi: 10.1530/ETJ-23-0067
21. Ali SZ, Baloch ZW, Cochand-Priollet B, Schmitt FC, Vielh P, VanderLaan PA. The 2023 Bethesda system for reporting thyroid cytopathology. Thyroid. (2023) 33:1039–44. doi: 10.1089/thy.2023.0141
22. Jenny B, Radovanovic I, Haenggeli C-A, Delavelle J, Rüfenacht D, Kaelin A, et al. Association of multiple vertebral hemangiomas and severe paraparesis in a patient with a PTEN hamartoma tumor syndrome. Case report. J Neurosurg. (2007) 107:307–13. doi: 10.3171/PED-07/10/307
23. Rizwan A, Saad M, Fatima S, Ameen A, Akhter S. Medullary thyroid carcinoma in the background of non-neoplastic toxic nodular goiter. AACE Clinical Case Reports. (2024) 10:249–52. doi: 10.1016/j.aace.2024.08.008
24. Pal A, Barber TM, Van de Bunt M, Rudge SA, Zhang Q, Lachlan KL, et al. PTEN mutations as a cause of constitutive insulin sensitivity and obesity. N Engl J Med. (2012) 367:1002–11. doi: 10.1056/NEJMoa1113966
25. Iida S, Ono A, Sayama K, Hamaguchi T, Fujii H, Nakajima H, et al. Accelerated decline of blood glucose after intravenous glucose injection in a patient with cowden disease having a heterozygous germline mutation of the PTEN/MMAC1 gene. Anticancer Res. (2000) 20:1901–4.10928124
26. Yehia L, Plitt G, Tushar AM, Joo J, Burke CA, Campbell SC, et al. Longitudinal analysis of cancer risk in children and adults with germline PTEN variants. JAMA Netw Open. (2023) 6:e239705. doi: 10.1001/jamanetworkopen.2023.9705
27. Plitt G, Brewer T, Yehia L, Jin J, Shin J, Eng C. Development and progression of thyroid disease in PTEN hamartoma tumor syndrome: refined surveillance recommendations. Thyroid. (2022) 32:1094–100. doi: 10.1089/thy.2022.0181
28. Plamper M, Gohlke B, Woelfle J. PTEN hamartoma tumor syndrome in childhood and adolescence-a comprehensive review and presentation of the German pediatric guideline. Mol Cell Pediatr. (2022) 9:3. doi: 10.1186/s40348-022-00135-1
29. Ngeow J, Eng C. PTEN in hereditary and sporadic cancer. Cold Spring Harb Perspect Med. (2020) 10:a036087. doi: 10.1101/cshperspect.a036087
30. Davidson L, Maccario H, Perera NM, Yang X, Spinelli L, Tibarewal P, et al. Suppression of cellular proliferation and invasion by the concerted lipid and protein phosphatase activities of PTEN. Oncogene. (2010) 29:687–97. doi: 10.1038/onc.2009.384
31. Bandargal S, Rajab M, Forest V-I, Pusztaszeri MP, Hier MP, da Silva SD, et al. Characteristics of PTEN mutation in thyroid tumours: a retrospective chart review. Cancers (Basel). (2023) 15:1575. doi: 10.3390/cancers15051575
32. Santarpia L, El-Naggar AK, Cote GJ, Myers JN, Sherman SI. Phosphatidylinositol 3-kinase/akt and ras/raf-mitogen-activated protein kinase pathway mutations in anaplastic thyroid cancer. J Clin Endocrinol Metab. (2008) 93:278–84. doi: 10.1210/jc.2007-1076
33. Balinisteanu I, Panzaru M-C, Caba L, Ungureanu M-C, Florea A, Grigore AM, et al. Cancer predisposition syndromes and thyroid cancer: keys for a short two-way street. Biomedicines. (2023) 11:2143. doi: 10.3390/biomedicines11082143
Keywords: Cowden syndrome, childhood, thyroid pathologies, PTEN variant, hyperfunctioning nodule
Citation: Garcia M, Oliver Petit I, Franchet C, Abbo O, Cartault A and Savagner F (2025) Atypical thyroid manifestation in Cowden disease: a case report and literature review. Front. Pediatr. 13:1499664. doi: 10.3389/fped.2025.1499664
Received: 21 September 2024; Accepted: 17 February 2025;
Published: 3 March 2025.
Edited by:
Ronald Cohen, The University of Chicago, United StatesReviewed by:
Hernan G. Valdes-Socin, University Hospital of Liège, BelgiumCopyright: © 2025 Garcia, Oliver Petit, Franchet, Abbo, Cartault and Savagner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Frédérique Savagner, c2F2YWduZXIuZkBjaHUtdG91bG91c2UuZnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.