 Tomislav Ćaleta1,†Martin J. Ryll2,†Katarina Bojanić3Nada Sindičić Dessardo1Darrell R. Schroeder4Juraj Sprung2Toby N. Weingarten2Milan Radoš5
Tomislav Ćaleta1,†Martin J. Ryll2,†Katarina Bojanić3Nada Sindičić Dessardo1Darrell R. Schroeder4Juraj Sprung2Toby N. Weingarten2Milan Radoš5 Ivica Kostović5
Ivica Kostović5 Ruža Grizelj1,6*
Ruža Grizelj1,6*
- 1Department of Pediatrics, School of Medicine University of Zagreb, University Hospital Centre Zagreb, Zagreb, Croatia
- 2Department of Anesthesiology and Perioperative Medicine, Mayo Clinic College of Medicine and Science, Rochester, MN, United States
- 3Division of Neonatology, Department of Obstetrics and Gynecology, University Hospital Merkur, Zagreb, Croatia
- 4Health Sciences Research, Division of Epidemiology, Mayo Clinic College of Medicine and Science, Rochester, MN, United States
- 5Croatian Institute for Brain Research, School of Medicine University of Zagreb, Zagreb, Croatia
- 6Center for Research on Perinatal Etiopathogenesis of Neurological and Cognitive Diseases, School of Medicine University of Zagreb, Zagreb, Croatia
Objective: To examine whether variation of regional cerebral oxygen saturation (rScO2) within three days after delivery predicts development of brain injury (intraventricular/cerebellar hemorrhage or white matter injury) in preterm infants.
Study design: A prospective study of neonates <32 weeks gestational age with normal cranial ultrasound admitted between 2018 and 2022. All received rScO2 monitoring with near-infrared spectroscopy at admission up to 72 h of life. To assess brain injury a magnetic resonance imaging was performed at term-equivalent age. We assessed the association between rScO2 variability (short-term average real variability, rScO2ARV, and standard deviation, rScO2SD), mean rScO2 (rScO2MEAN), and percentage of time rScO2 spent below 60% (rScO2TIME<60%) during the first 72 h of life and brain injury.
Results: The median [IQR] time from birth to brain imaging was 68 [59-79] days. Of 81 neonates, 49 had some form of brain injury. Compared to neonates without injury, in those with injury rScO2ARV was higher during the first 24 h (P = 0.026); rScO2SD was higher at 24 and 72 h (P = 0.029 and P = 0.030, respectively), rScO2MEAN was lower at 48 h (P = 0.042), and rScO2TIME<60% was longer at 24, 48, and 72 h (P = 0.050, P = 0.041, and P = 0.009, respectively). Similar results were observed in multivariable logistic regression. Although not all results were statistically significant, increased rScO2 variability (rScO2ARV and rScO2SD) and lower mean values of rScO2 were associated with increased likelihood of brain injury.
Conclusions: In preterm infants increased aberration of rScO2 in early postdelivery period was associated with an increased likelihood of brain injury diagnosis at term-equivalent age.
1 Introduction
Brain injury in the preterm infant results from the combined developmental and destructive effects on the maturing nervous system due to multisystemic diseases and conditions from prenatal to postnatal life (1). Pre-conceptional maternal toxic stress and pregnancy-related illnesses affecting the maternal-placental-fetal triad can disrupt fetal brain development, contributing to preterm birth and/or increasing risks for peripartum brain injuries (1, 2). Various postnatal injurious triggers such as respiratory insufficiency and hemodynamic instability secondary to severe respiratory disease, recurrent apneic spells, hemodynamically significant ductus arteriosus, late-onset sepsis or conditions such as necrotizing enterocolitis further increase the risk and promote subsequent brain injury (3, 4).
Intracranial hemorrhage and white matter injury (WMI) are frequent pathologies (20%–30%) in preterm infants (5–8). Intraventricular hemorrhage (IVH) usually originates in the subependymal germinal matrix, a richly vascularized collection of neuronal-glial precursor cells in the developing brain (9). The risk of hemorrhage is inversely proportional to gestational age (GA), with most of IVH occurring in infants less than 32 weeks of gestation (10). Factors primarily related to dysregulation of cerebral blood flow and pressure in the microvascular bed of the germinal matrix play a major contributory pathogenic role (9, 11, 12). Most IVH events occur within the first week of delivery, and in the majority (90%) can be detected within the first 72 h of life (13). Cerebellar hemorrhage is also a common form of brain injury in preterm infants. Detection of these injuries by magnetic resonance imaging (MRI) has been reported in up to 37% of infants less than 33 weeks GA (14). WMI represents a spectrum of disease that ranges from focal necrotic lesions deep in the white matter, with or without subsequent cyst formation, to the more common, diffuse, and nondestructive WMI (15). The injury is believed to be induced by cerebral ischemia, infection and/or inflammation (16). Several fundamental physiological factors related to cerebral blood flow, including oxygenation, hypocarbia, levels of glucose and its metabolites, and a variety of inflammatory factors, likely influence the severity of WMI (17).
Considering that prevalent types of brain injury among preterm infants often coincide with hypoxic, ischemic, and reperfusion events in the early postdelivery period, it is of utmost importance to be able to assess adequacy of cerebral blood flow to improve managements designed to mitigate the risk for injury. Near-infrared spectroscopy (NIRS) monitors regional cerebral oxygen saturation (rScO2), provides non-invasive information on hemodynamics, real time brain oxygen delivery (18), and is considered to be a surrogate marker for cerebral blood flow (19–21). NIRS uses multiple wavelengths of near-infrared light and relies on the absorption spectra of oxygenated and deoxygenated hemoglobin to calculate relative concentrations of each, which are then used to calculate rScO2. Since NIRS makes no distinction between brain blood compartments, rScO2 estimates hemoglobin oxygen saturation in a mixed arterial, capillary, and venous compartments (22). The association between rScO2 measurements and development of brain injury is not well explored. In the current study we hypothesize that variability in rScO2 recorded from NIRS in the early postdelivery period may predict brain injury assessed from MRI at term-equivalent age (TEA). We especially focus on short-term average real variability (ARV) of rScO2 during early postdelivery period as a potential culprit for brain injury. This hypothesis was tested on preterm infants by rScO2 monitoring with NIRS for the first 72 h after birth. An improved understanding of the relationship between altered rScO2 and development of brain injury may be used in future management strategies designed to improve neonatal outcomes.
2 Methods
2.1 Settings
This study was conducted in the University Hospital Centre (UHC) and the Croatian Institute for Brain Research, Zagreb, Croatia as a part of a multidisciplinary, longitudinal research project. The UHC is the largest Croatian tertiary referral center for neonatal care and does not have a maternity ward. The hospital admits preterm infants from hospitals that do have maternity wards but do not have the capacity to manage high-risk neonates. Therefore, all neonates in the current study are outborns.
2.2 Patient population, inclusion/exclusion criteria
This is a prospective study of all consecutive newborn admissions to the Neonatal Intensive Care Unit (NICU) at the UHC Zagreb between May 1st, 2018, and June 31st, 2022. The infants were eligible for enrollment if they were less than 32 weeks’ GA at birth and had a normal cranial ultrasound (cUS) on admission. Preterm infants with chromosomal or congenital anomalies, and those with delayed transfer (>12 h) from outside institutions were excluded.
2.3 Study design, NIRS monitoring and study aims
Upon NICU admission cUS was performed to exclude the presence of brain injury. All qualified infants (i.e., no brain injury on cUS) received rScO2 monitoring using NIRS immediately on admission for up to 72 h of life. A 72-hour period has been accepted as a suitable time frame for NIRS monitoring in premature infants (23), as majority of IVH in premature infants happens within the first 3 days of life (24). In our study a two wavelength (730 and 810 nm) near-infrared spectrometer (INVOS 5100, Covidien, Mansfeld, MA) was used by firmly attaching a small neonatal sensor (Covidien, Mansfield, MA) on the left side of the infant's forehead. Four rScO2 summary statistics were considered: (1) short-term rScO2 average real variability (rScO2ARV) using following equation:
(2) rScO2 standard deviation (rScO2SD), (3) rScO2 mean (rScO2MEAN), and 4) the percentage of time neonate spent with rScO2<60% (rScO2TIME<60%) all during 72 h after birth. The primary aim was to assess the association between variability of rScO2 (rScO2ARV and rScO2SD) and brain injury, and secondary aims were to assess the association between average rScO2, (rScO2MEAN) and percentage of time spent at oxygen saturation below 60% (rScO2TIME<60%) and brain injury.
2.4 Data collection
We reviewed obstetric, demographic and neonatal data from the hospital records: sex, GA, birth weight, type of delivery (natural delivery vs. Cesarean section), antenatal corticosteroid treatment, Apgar scores, age at hospital admission, Scores for Neonatal Acute Physiology Perinatal Extension II (SNAPPE-II); variables related to treatment: primary respiratory support, duration of mechanical ventilation, surfactant administration, transfusion of blood and blood products, use of inotropes; and prematurity related complications: pneumothorax, bronchopulmonary dysplasia, necrotizing enterocolitis, infection/sepsis, retinopathy of prematurity.
2.5 Grading of brain injuries
Brain imaging at TEA was done using a 3T MRI scanner (Magnetom, PrismaFIT, Siemens). MRI scanning was performed after regular feeding, infants were wrapped with linen diapers and a blanket. A neuroradiologist blinded to clinical data evaluated the MRI findings. WMI grades considered are: Grade I—punctate lesions; Grade II—small periventricular cysts; Grade III—extensive periventricular cysts; Grade IV—extensive subcortical cysts—also called multicystic encephalomalacia (25–27). IVH was classified according to Papile classification: Grade I—hemorrhage limited to germinal matrix; Grade II—extension into normal-sized ventricles; Grade III—extensive hemorrhage with dilatation of the ventricles; Grade IV—parenchymal involvement (28, 29). Cerebellar hemorrhage was noted as present or absent.
2.6 Statistical analysis
Raw rScO2 NIRS measurements were recorded every 5–15 s. To exclude outliers, we aggregated raw rScO2 data as a mean over 5-minute intervals for the four features of interest. The aggregated rScO2 measurements were analyzed for 24-, 48-, and 72-hour intervals following birth. We examined the association between four rScO2 features (time-weighted rScO2ARV, rScO2SD, rScO2MEAN, and rScO2TIME<60%) and brain injury at TEA. The rScO2ARV was calculated as the average of absolute differences between consecutive rScO2 measurements during the observed time frame using a previously described equation (30, 31). rScO2ARV feature accounts for the order in which the respective rScO2 measurements occurred and corrects for limitations of the commonly used measures of variability such as standard deviation, which accounts only for the dispersion of values around the mean, and not for the order of the respective readings (31). Patients with >50% missing rScO2 values during the predetermined time intervals following admission were assigned a missing value for the respective feature. For calculating the rScO2ARV and rScO2SD, the rScO2 ceiling-value of 95% was handled by excluding any of the aggregated 95% measurements, that were flanked on both sides by 95% measurements. For calculating the rScO2MEAN and the rScO2TIME<60% these 95%-measurements were not excluded.
For univariable analysis, rScO2 features were compared between those with and without brain injury using the two-sample t-test or Mann Whitney U-test as appropriate. For the multivariable logistic regression analysis, our cohort size allows for two covariates aside from our feature of interest, for which we chose GA and birth weight. Results from the multivariable logistic regression model are summarized as odds ratio and 95% confidence interval for the given rScO2 feature. There was no evidence of significant non-linearity of GA, birth weight, and all rScO2 features, as tested by comparing a univariable linear and a univariable restricted cubic spline model (with knots at the 5th, 50th, and 95th or 15th, 50th, and 95th percentile) via the likelihood ratio test for each variable. A P-value <0.05 was determined statistically significant throughout. All statistical analyses were performed with Python v.3.9 (Python Software Foundation, Wilmington, Delaware, USA).
3 Results
3.1 Cohort characteristics
Between May 1st, 2018, and June 31st, 2022, 81 neonates met criteria and were included in the study. The median [IQR] time from birth to initiation of NIRS monitoring was 2.5 [1.4–3.6] hours, and from birth to MRI at TEA 68 [59–79] days. MRI at TEA ruled out the presence of brain injury in 32 neonates, while 49 were diagnosed with single or multiple brain injuries (all were mild, grades I or II): 33 (40.7%) neonates had IVH, 28 (34.6%) had WMI, and 8 (10%) had cerebellar hemorrhage (Figure 1). Table 1 shows neonatal characteristics, overall and according to the presence or absence of brain injury. There were no significant differences in characteristics between infants with and without injury: GA at delivery (P = 0.555), Apgar scores at 1 and 5 min (P = 0.673 and 0.899, respectively), and main comorbidities (sepsis, P > 0.99; need for respiratory support, P = 0.155; necrotizing enterocolitis, P = 0.462; bronchopulmonary dysplasia, P = 0.590; or retinopathy, P = 0.511).
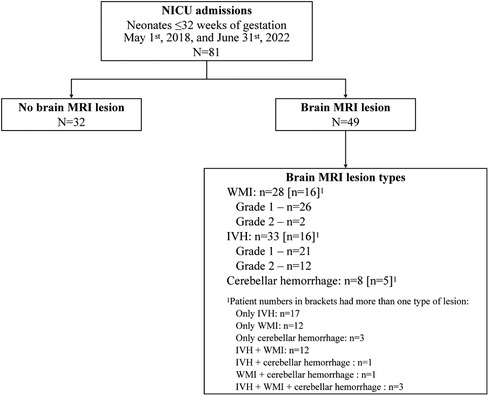
Figure 1 Summary of 81 preterm infants according to MRI results at term-equivalent age. IVH, intraventricular hemorrhage; WMI, white matter injury.
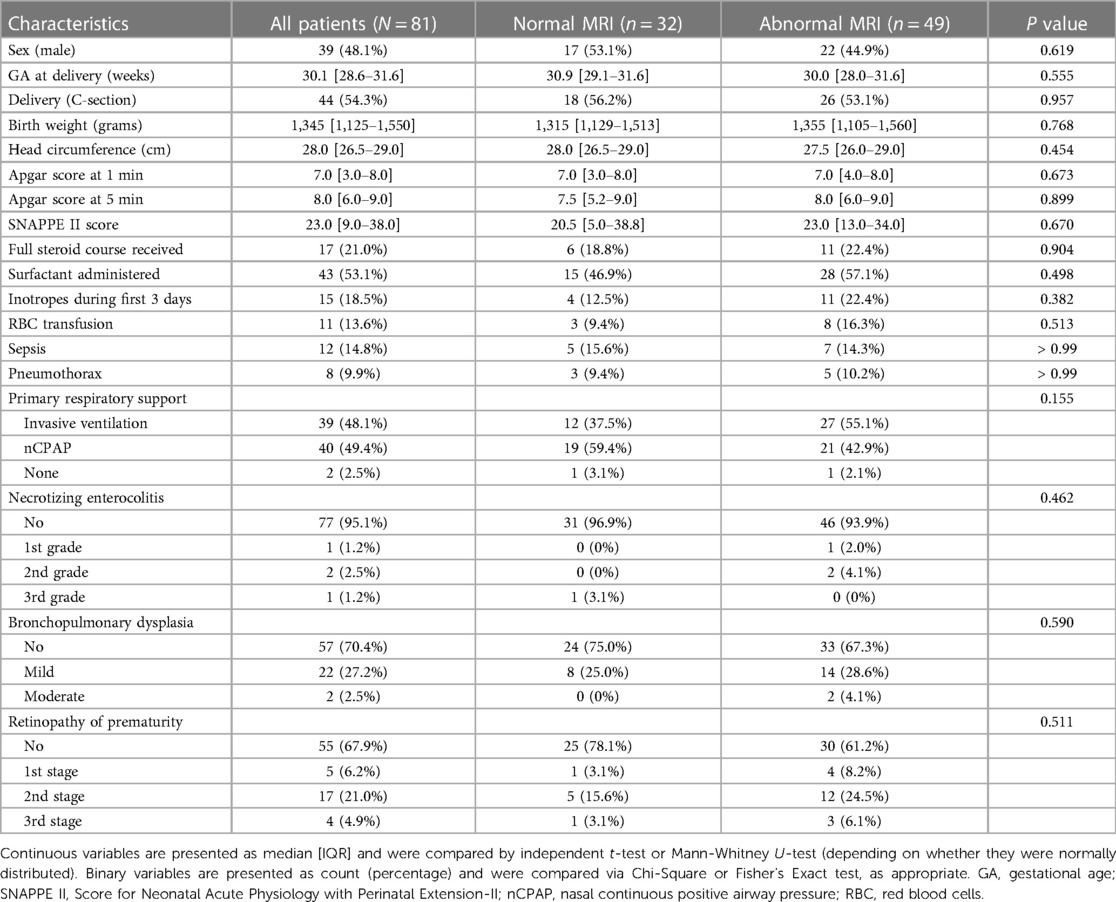
Table 1 Demographic and clinical characteristics of preterm infants in our cohort.
3.2 Association of rScO2 features with brain injury at TEA
Of the 81 neonates, 72, 77, and 80 had sufficient rScO2 data (continuous NIRS monitoring for >50% of the timeframe) for the 24-, 48-, and 72-hours after birth, respectively. Compared to neonates without brain injury, rScO2ARV was higher during the first 24 h in those diagnosed with brain injury, P = 0.026 (Table 2, Figure 2). Similarly, rScO2SD was higher at 24 and 72 h (P = 0.029 and P = 0.030, respectively) in those with injury. The rScO2MEAN was lower at 48 h (P = 0.042) in those with injury, and the percentage of time neonates spent at rScO2TIME<60% was higher in those with injury (P = 0.050, P = 0.041, and P = 0.009 at 24-, 48-, and 72-hours, respectively) (Table 2, Supplementary Figure S1). Similar results were observed from logistic regression analysis adjusted for GA and birth weight (Table 2). Although not all results were significant, increased rScO2 variability (rScO2ARV, rScO2SD) was consistently associated with increased likelihood of brain injury at TEA. Also, lower values of rScO2 (rScO2MEAN and rScO2TIME<60%) were associated with increased likelihood of brain injury (Table 2 and Figure 2).
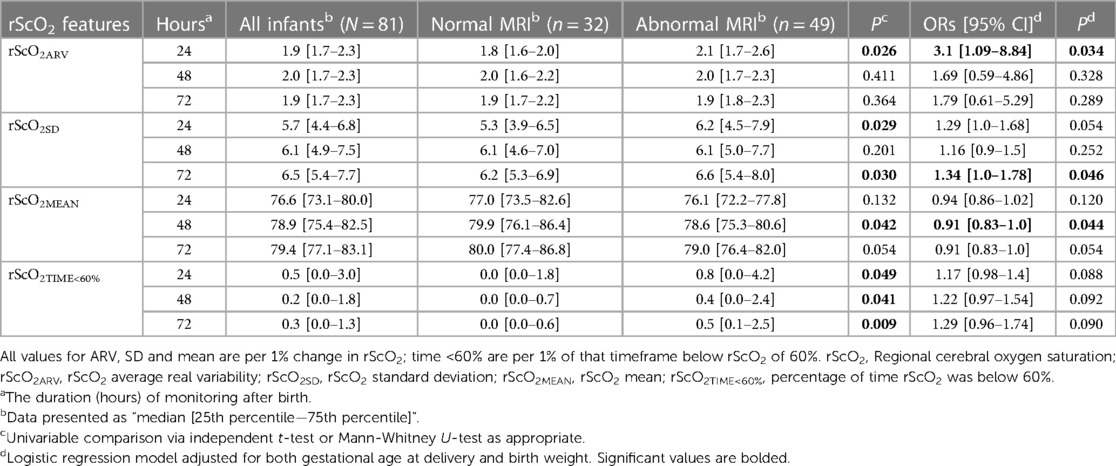
Table 2 Comparison of four rScO2 features during the first 72 h of life in infants with and without brain injury as seen on magnetic resonance imaging at term-equivalent age.
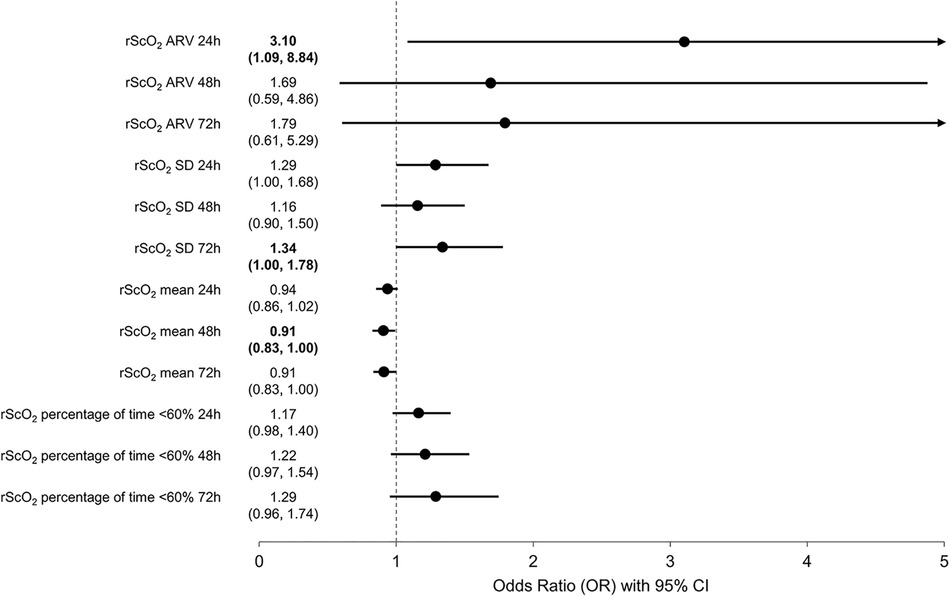
Figure 2 Results of logistic regression analysis showing the association between rScO2 features (average real variability; rScO2ARV; standard deviation, rScO2SD; mean, rScO2MEAN; and percentage of time below 60%, rScO2TIME<60%) and brain injury at term-equivalent age. Values >1 indicate increased likelihood for brain injury at term-equivalent age.
4 Discussion
The most important findings of this study are that increased variability of regional cerebral oxygen saturation, lower mean saturation, and longer time neonates spent at saturation below 60% in the early postdelivery period were associated with an increased likelihood for being diagnosed with brain injury at TEA. Our results cannot distinguish if this association is consequential (rScO2 pattern reflects presence of injury) or causative (rScO2 pattern contributed to development of injury), therefore our study provides direction for future research.
Variations in cerebral perfusion and oxygenation are considered to be the key risk factors for brain injury in preterm infants (9, 11, 12). Continuous assessment of rScO2 can identify infants with altered cerebral oxygenation (32). Although NIRS is increasingly used by neonatologists for rScO2 monitoring, there are no reports that consistently establish the rScO2 references or cut-off values for adverse outcomes related to altered brain oxygenation (23, 33). Alderliesten et al. (23) published reference values of rScO2 during the first three days of life in 999 preterm infants (GA <32 weeks) and found that at NICU admission the average rScO2 was ∼65% and continued to increase with GA at a mean rate of 1% per week, following a parabolic curve in relation to postnatal age with a peak at −36 h. It is important to note, Alderliesten et al. (23) references were obtained mostly from measurements using small adult sensors (983 small adult sensors and 16 neonatal sensors). In order to convert neonatal sensor readings to the small adult sensor equivalent, the obtained rScO2 values were interpolated using statistical modelling tools (23). It is well established that rScO2 values depend on the type of NIRS sensor used (e.g., adult, neonatal, pediatric) (23, 34). In comparison to adult sensors, neonatal rScO2 sensor readings are consistently higher, but the difference is not fixed and is less at the threshold indicative of cerebral hypoxia; the neonatal sensor difference is approximately 10% when adult sensors read 85%, but nearly similar (58.8%) when adult sensors read 55% (35). The SafeBoosC-III study evaluating the benefit of an interventional strategy to reduce cerebral hypoxia using NIRS-derived rScO2 monitoring demonstrate no significant difference between group in rates of death or severe brain injury at 36 weeks post-menstrual age (36). The study used at least 5 different device and sensor combinations with varying hypoxia thresholds based on linear transformations obtained in an in vitro model. Although the trial did not show evidence of decreased mortality or severe brain injury, concerns remain that the selected thresholds were not equivalent across devices due to proprietary algorithms and the nonlinear nature of human physiology (37). Therefore, in order to properly interpret rScO2 cut-off values, it is of utmost importance to specify the type of sensor when comparing the data between studies.
Because low brain blood flow is associated with reduced oxygenation it poses a risk for development of brain injury. Specifically, Alderliesten et al. (34) found that a rScO2<55% (using a small adult sensor) increased risk for grade III/IV IVH with an odds ratio of 1.017 per one percent (95%CI 1.007–1.026, GA corrected) of time spent below 55%, as well as in neonates who spent at least 20% of time below 55% in the first 72 h following delivery. Furthermore, Alderliesten et al. (34) found that a rScO2<55% was associated with unfavorable cognitive outcomes at 24 months with an OR of 1.4 (CI 1.1–1.7) for neonates who spent at least 20% of time below that threshold during the first 3 days after delivery. Chock et al. (38) measured rScO2 with neonatal sensors and reported that infants with adverse outcomes had significantly lower mean rScO2 (67 ± 9%) compared with those without adverse outcomes (72 ± 7%), and that rScO2 below 50% could be identified as a cut-off point for identifying infants with adverse outcome with an area under the curve of 0.76. Verhagen et al. (39), using pediatric sensors, demonstrated that preterm infants with IVH, compared to those without IVH, had lower median rScO2 during the first two weeks following birth, suggesting that lower cerebral blood flow in those with injuries remains present for a longer period than just the first few hours after birth. However, it remains unknown whether this lower blood flow and oxygenation contributed to injury or rather reflects the presence of hemorrhage. In our cohort few infants had rScO2 below 50%, therefore we examined the time spent with rScO2 below 60% during 72 postdelivery hours. Using this cut-off point in unadjusted analysis we found a positive association between rScO2TIME<60% and brain injury, however after adjusting for weight and GA the significance was lost, but the trend towards positive association remained.
A short-term ARV represents measurement-to-measurement, within-subject variability in the parameter (in our study parameter of interest was rScO2) that accounts for the order in which measurements has occurred (31). In cardiovascular research short-term ARV was shown to be an independent risk factor for severity of organ damage (40, 41), cardiovascular morbidity and mortality (30, 42). The precision of estimates from ARV is dependent on frequency of sequential readings (measurements), and in the current study data were recorded every 5–15 s, and ARV was aggregated over 5-minute intervals during 72-hours after delivery. Therefore, our frequency of measurements provides a reliable assessment of rScO2ARV features in regard to the outcome sought. It is well known that inadequate or fluctuating cerebral perfusion and oxygenation contribute to IVH and WMI (10, 12, 38, 43–47). Preterm infants are at high risk for early hemodynamic instability and many factors may contribute to fluctuations in systemic blood pressure in the first few days of life. Moreover, cerebral autoregulation has limited capacity and is thought to be particularly fragile in the immature brain (48). A number of factors that influence vascular reactivity are likely to promote the pressure passive state (hypoxia, hypocarbia, hypercarbia), significantly perturb cerebral blood flow and increase the risk for WMI and intracranial hemorrhage (49–52). The proportion of infants with impaired cerebral autoregulation and increased periods of pressure-passive cerebral circulation appear to be substantial (53, 54). As the pressure-passive state can fluctuate over time and can occur without markedly low blood pressures, it could be readily overlooked with routine monitoring (54). On the other side, increases in systemic blood pressure, especially abrupt increases, could lead to cerebral hyperperfusion and hemorrhagic complications. Since oscillations of systemic blood pressure create variations in regional blood flow which can be assessed with NIRS (55), rScO2 ARV emerges as an attractive approach to assess the adequacy of regional brain perfusion and oxygenation. To the best of our knowledge rScO2ARV using NIRS has never been examined in assessing the association between rScO2 and brain injury. Our study suggests that increased short-term rScO2ARV, early following delivery of preterm infants may be either a predictor or a marker for increased likelihood of brain injury.
4.1 Strengths and limitations
A strength of this study is prospective enrollment of consecutive neonates who fulfilled the research criteria. To examine more precisely the relationship between rScO2 and brain injury only neonates with a normal cUS on admission were included. Another strength of our study is the use of MRI over cUS to detect the severity and extension of brain injury. Compared with cUS, MRI is more sensitive for detection of low grade IVH, non-cystic WMI, especially punctate white matter lesions which correspond to small periventricular necroses of apparent ischemic or hemorrhagic nature, as well as cerebellar hemorrhage, particularly small punctate hemorrhages (56, 57).
Our study must be interpreted in the context of several limitations. First, we focused on rScO2 monitoring in the first 3 days following birth. While most brain injuries (70%) are expected to occur within the first 72 h following birth (13), this monitoring window may not be adequate to capture injuries that occur later (of note, it is estimated that 95% of brain injuries occur by day 7, with a very small additional percentage between days 7 and 10) (24). Our study assumes that the majority of injuries occurred during 72-hour time frame after birth, as well that these injuries may be associated with altered rScO2. Second, our study assumes that early occurring brain injuries remain detectable with MRI at TEA, and ignores the possibility that some may have resolved in interim. Third, there was a substantial variability in measured rScO2 values which limits the statistical power of consistently detecting differences. Although we found evidence that rScO2 in early postdelivery period is associated with brain injury at TEA, as well that the time spent below 60% saturation is associated with increased risk for brain injury, our study is not large enough to provide the exact cut-off point for critical rScO2 levels. Therefore, future studies are needed to define critical rScO2 values and examine whether interventions designed to optimize rScO2 can prevent brain injury in infants.
5 Conclusion
In conclusion, our results suggest that features of increased rScO2 variability in preterm infants, as well as lower rScO2MEAN and increased percentage of time spent <60% within the first three days following delivery may be associated with increased likelihood for brain injury at TEA. Our study design does not allow to discern whether the observed association between rScO2 and brain injury is causative or is rather a marker of its presence. Therefore, our study opens an intriguing question and provides direction for future research.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Institutional Ethics Committee of the University Hospital Centre Zagreb and Institutional Ethics Committee of the School of Medicine University of Zagreb. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
TĆ: Investigation, Methodology, Writing – original draft. MR: Data curation, Writing – review & editing, Formal Analysis, Validation. KB: Writing – review & editing. ND: Writing – review & editing, Investigation. DS: Data curation, Writing – review & editing, Formal Analysis, Validation. JS: Writing – review & editing, Data curation, Methodology, Supervision. TW: Writing – review & editing. MR: Investigation, Writing – review & editing, Funding acquisition. IK: Investigation, Writing – review & editing. RG: Investigation, Methodology, Project administration, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article.
This publication was supported by Croatian Science Foundation projects IP-2020-02-7166; co-financed by the Scientific Centre of Excellence for Basic, Clinical and Translational Neuroscience project "Experimental and clinical research of hypoxic-ischemic damage in perinatal and adult brain"; GA KK01.1.1.01.0007 funded by the European Union through the European Regional Development Fund.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2024.1426874/full#supplementary-material
Abbreviations
ARV, average real variability; cUS, cranial ultrasound; GA, gestational age; IQR, interquartile range; IVH, intraventricular hemorrhage; MRI, magnetic resonance imaging; NICU, Neonatal Intensive Care Unit; NIRS, near infrared spectroscopy; rScO2, Regional cerebral oxygen saturation; rScO2ARV, rScO2 average real variability; rScO2MEAN, Mean rScO2; rScO2SD, rScO2 standard deviation; rScO2TIME<60%, percentage of time neonate had rScO2 below 60%; SD, standard deviation; TEA, term-equivalent age; WMI, white matter injury.
References
1. Scher MS. “The first thousand days” define a fetal/neonatal neurology program. Front Pediatr. (2021) 9:683138. doi: 10.3389/fped.2021.683138
2. Scher MS. Interdisciplinary fetal-neonatal neurology training applies neural exposome perspectives to neurology principles and practice. Front Neurol. (2024) 14:1321674. doi: 10.3389/fneur.2023.1321674
3. Kartam M, Embaireeg A, Albalool S, Almesafer A, Hammoud M, Al-Hathal M, et al. Late-onset sepsis in preterm neonates is associated with higher risks of cerebellar hemorrhage and lower motor scores at three years of age. Oman Med J. (2022) 37(2):e368. doi: 10.5001/omj.2022.41
4. Lu J, Martin CR, Claud EC. Neurodevelopmental outcome of infants who develop necrotizing enterocolitis: the gut-brain axis. Semin. Perinatol. (2023) 47(1):151694. doi: 10.1016/j.semperi.2022.151694
5. Kusters CD, Chen ML, Follett PL, Dammann O. “Intraventricular” hemorrhage and cystic periventricular leukomalacia in preterm infants: how are they related? J Child Neurol. (2009) 24(9):1158–70. doi: 10.1177/0883073809338064
6. Stoll BJ, Hansen NI, Bell EF, Shankaran S, Laptook AR, Walsh MC, et al. Neonatal outcomes of extremely preterm infants from the NICHD neonatal research network. Pediatrics. (2010) 126(3):443–56. doi: 10.1542/peds.2009-2959
7. Arulkumaran S, Tusor N, Chew A, Falconer S, Kennea N, Nongena P, et al. MRI findings at term-corrected age and neurodevelopmental outcomes in a large cohort of very preterm infants. AJNR Am J Neuroradiol. (2020) 41(8):1509–16. doi: 10.3174/ajnr.A6666
8. Kostović I, Kostović-Srzentić M, Benjak V, Jovanov-Milošević N, Radoš M. Developmental dynamics of radial vulnerability in the cerebral compartments in preterm infants and neonates. Front Neurol. (2014) 5:139. doi: 10.3389/fneur.2014.00139
9. Ballabh P, de Vries LS. White matter injury in infants with intraventricular haemorrhage: mechanisms and therapies. Nat Rev Neurol. (2021) 17(4):199–214. doi: 10.1038/s41582-020-00447-8
10. Lou HC, Lassen NA, Friis-Hansen B. Impaired autoregulation of cerebral blood flow in the distressed newborn infant. J Pediatr. (1979) 94(1):118–21. doi: 10.1016/s0022-3476(79)80373-x
11. Inder TE, Perlman JM, Volpe JJ. Preterm intraventricular hemorrhage/posthemorrhagic hydrocephalus. In: Volpe JJ, editor. Neurology of the Newborn. Philadelphia: Elsevier (2018). p. 637–98.
12. Lu H, Wang Q, Lu J, Zhang Q, Kumar P. Risk factors for intraventricular hemorrhage in preterm infants born at 34 weeks of gestation or less following preterm premature rupture of membranes. J Stroke Cerebrovasc Dis. (2016) 25(4):807–12. doi: 10.1016/j.jstrokecerebrovasdis.2015.12.011
13. McCrea HJ, Ment LR. The diagnosis, management, and postnatal prevention of intraventricular hemorrhage in the preterm neonate. Clin Perinatol. (2008) 35(4):777–92. doi: 10.1016/j.clp.2008.07.014
14. Gano D, Ho ML, Partridge JC, Glass HC, Xu D, Barkovich AJ, et al. Antenatal exposure to magnesium sulfate is associated with reduced cerebellar hemorrhage in preterm newborns. J Pediatr. (2016) 178:68–74. doi: 10.1016/j.jpeds.2016.06.053
15. Inder TE, Anderson NJ, Spencer C, Wells S, Volpe JJ. White matter injury in the premature infant: a comparison between serial cranial sonographic and MR findings at term. AJNR Am J Neuroradiol. (2003) 24(5):805–9. PMID: 12748075; PMCID: PMC7975772.12748075
16. Back SA. White matter injury in the preterm infant: pathology and mechanisms. Acta Neuropathol. (2017) 134(3):331–49. doi: 10.1007/s00401-017-1718-6
17. Back SA, Volpe JJ. Encephalopathy of prematurity: pathophysiology. In: Volpe JJ, editor. Neurology of the Newborn. Philadelphia: Elsevier (2018). p. 405–24.
18. Zhang Y, Liu D, Mao Y, Gao Q, Xiong T. Cerebral near-infrared spectroscopy monitoring to predict periventricular-intraventricular haemorrhage and neurodevelopmental outcomes in preterm infants: a protocol for a systematic review and meta-analysis. BMJ Paediatr Open. (2023) 7(1):e001859. doi: 10.1136/bmjpo-2023-001859
19. Zweifel C, Castellani G, Czosnyka M, Helmy A, Manktelow A, Carrera E, et al. Noninvasive monitoring of cerebrovascular reactivity with near infrared spectroscopy in head-injured patients. J Neurotrauma. (2010) 27(11):1951–8. doi: 10.1089/neu.2010.1388
20. Brady K, Joshi B, Zweifel C, Smielewski P, Czosnyka M, Easley RB, et al. Real-time continuous monitoring of cerebral blood flow autoregulation using near-infrared spectroscopy in patients undergoing cardiopulmonary bypass. Stroke. (2010) 41(9):1951–6. doi: 10.1161/STROKEAHA.109.575159
21. Caicedo A, De Smet D, Naulaers G, Ameye L, Vanderhaegen J, Lemmers P, et al. Cerebral tissue oxygenation and regional oxygen saturation can be used to study cerebral autoregulation in prematurely born infants. Pediatr Res. (2011) 69(6):548–53. doi: 10.1203/PDR.0b013e3182176d85
22. Watzman HM, Kurth CD, Montenegro LM, Rome J, Steven JM, Nicolson SC. Arterial and venous contributions to near-infrared cerebral oximetry. Anesthesiology. (2000) 93(4):947–53. doi: 10.1097/00000542-200010000-00012
23. Alderliesten T, Dix L, Baerts W, Caicedo A, van Huffel S, Naulaers G, et al. Reference values of regional cerebral oxygen saturation during the first 3 days of life in preterm neonates. Pediatr Res. (2016) 79(1-1):55–64. doi: 10.1038/pr.2015.186
24. Hand IL, Shellhaas RA, Milla SS, Committee on Fetus and Newborn, Section on Neurology, Section on Radiology. Routine neuroimaging of the preterm brain. Pediatrics. (2020) 146(5):e2020029082. doi: 10.1542/peds.2020-029082
25. de Vries LS, Eken P, Dubowitz LM. The spectrum of leukomalacia using cranial ultrasound. Behav Brain Res. (1992) 49(1):1–6. doi: 10.1016/s0166-4328(05)80189-5
26. Dorner RA, Burton VJ, Allen MC, Robinson S, Soares BP. Preterm neuroimaging and neurodevelopmental outcome: a focus on intraventricular hemorrhage, post-hemorrhagic hydrocephalus, and associated brain injury. J Perinatol. (2018) 38(11):1431–43. doi: 10.1038/s41372-018-0209-5
27. Agut T, Alarcon A, Cabañas F, Bartocci M, Martinez-Biarge M, Horsch S, et al. Preterm white matter injury: ultrasound diagnosis and classification. Pediatr Res. (2020) 87(Suppl 1):37–49. doi: 10.1038/s41390-020-0781-1
28. Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr. (1978) 92(4):529–34. doi: 10.1016/s0022-3476(78)80282-0
29. Starr R, De Jesus O, Shah SD, Borger J. Periventricular and Intraventricular Hemorrhage. in StatPearls. Treasure Island, FL: StatPearls Publishing (2023). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK538310/ (accessed April 21, 2024).
30. Mena L, Pintos S, Queipo NV, Aizpúrua JA, Maestre G, Sulbarán T. A reliable index for the prognostic significance of blood pressure variability. J Hypertens. (2005) 23(3):505–11. doi: 10.1097/01.hjh.0000160205.81652.5a
31. Mena LJ, Maestre GE, Hansen TW, Thijs L, Liu Y, Boggia J, et al. How many measurements are needed to estimate blood pressure variability without loss of prognostic information? Am J Hypertens. (2014) 27(1):46–55. doi: 10.1093/ajh/hpt142
32. Alderliesten T, Lemmers PM, Smarius JJ, van de Vosse RE, Baerts W, van Bel F. Cerebral oxygenation, extraction, and autoregulation in very preterm infants who develop peri-intraventricular hemorrhage. J Pediatr. (2013) 162(4):698–704.e2. doi: 10.1016/j.jpeds.2012.09.038
33. Hyttel-Sorensen S, Pellicer A, Alderliesten T, Austin T, van Bel F, Benders M, et al. Cerebral near infrared spectroscopy oximetry in extremely preterm infants: phase II randomised clinical trial. Br Med J. (2015) 350:g7635. doi: 10.1136/bmj.g7635
34. Alderliesten T, van Bel F, van der Aa NE, Steendijk P, van Haastert IC, de Vries LS, et al. Low cerebral oxygenation in preterm infants is associated with adverse neurodevelopmental outcome. J Pediatr. (2019) 207:109–116.e2. doi: 10.1016/j.jpeds.2018.11.038
35. Variane GFT, Dahlen A, Noh CY, Zeng J, Yan ES, Kaneko JS, et al. Cerebral oxygen saturation in neonates: a bedside comparison between neonatal and adult NIRS sensors. Pediatr Res. (2023) 94(5):1810–6. doi: 10.1038/s41390-023-02705-z
36. Hansen ML, Pellicer A, Hyttel-Sørensen S, Ergenekon E, Szczapa T, Hagmann C, et al. Cerebral oximetry monitoring in extremely preterm infants. N Engl J Med. (2023) 388(16):1501–11. doi: 10.1056/NEJMoa2207554
37. Chock VY, Vesoulis ZA, El-Dib M, Austin T, van Bel F. The future of neonatal cerebral oxygenation monitoring: directions after the SafeBoosC-III trial. J Pediatr. (2024) 270:114016. doi: 10.1016/j.jpeds.2024.114016
38. Chock VY, Kwon SH, Ambalavanan N, Batton B, Nelin LD, Chalak LF, et al. Cerebral oxygenation and autoregulation in preterm infants (early NIRS study). J Pediatr. (2020) 227:94–100.e1. doi: 10.1016/j.jpeds.2020.08.036
39. Verhagen EA, Ter Horst HJ, Keating P, Martijn A, Van Braeckel KN, Bos AF. Cerebral oxygenation in preterm infants with germinal matrix-intraventricular hemorrhages. Stroke. (2010) 41(12):2901–7. doi: 10.1161/STROKEAHA.110.597229
40. Sega R, Corrao G, Bombelli M, Beltrame L, Facchetti R, Grassi G, et al. Blood pressure variability and organ damage in a general population: results from the PAMELA study (pressioni arteriose monitorate E loro associazioni). Hypertension. (2002) 39(2 Pt 2):710–4. doi: 10.1161/hy0202.104376
41. Li CL, Liu R, Wang JR, Yang J. Relationship between blood pressure variability and target organ damage in elderly patients. Eur Rev Med Pharmacol Sci. (2017) 21(23):5451–5. doi: 10.26355/eurrev_201712_13934
42. Del Giorno R, Balestra L, Heiniger PS, Gabutti L. Blood pressure variability with different measurement methods: reliability and predictors. A proof of concept cross sectional study in elderly hypertensive hospitalized patients. Medicine (Baltimore). (2019) 98(28):e16347. doi: 10.1097/MD.0000000000016347
43. Aspide R. Relationship between brain tissue oxygen and near-infrared spectroscopy in patients with nontraumatic subarachnoid hemorrhage: invited commentary. Neurocrit Care. (2022) 37(3):616–7. doi: 10.1007/s12028-022-01566-4
44. Ballabh P. Pathogenesis and prevention of intraventricular hemorrhage. Clin Perinatol. (2014) 41(1):47–67. doi: 10.1016/j.clp.2013.09.007
45. Noori S, McCoy M, Anderson MP, Ramji F, Seri I. Changes in cardiac function and cerebral blood flow in relation to peri/intraventricular hemorrhage in extremely preterm infants. J Pediatr. (2014) 164(2):264–70.e703. doi: 10.1016/j.jpeds.2013.09.045
46. Sorensen LC, Maroun LL, Borch K, Lou HC, Greisen G. Neonatal cerebral oxygenation is not linked to foetal vasculitis and predicts intraventricular haemorrhage in preterm infants. Acta Paediatr. (2008) 97(11):1529–34. doi: 10.1111/j.1651-2227.2008.00970.x
47. Vesoulis ZA, Whitehead HV, Liao SM, Mathur AM. The hidden consequence of intraventricular hemorrhage: persistent cerebral desaturation after IVH in preterm infants. Pediatr. Res. (2021) 89(4):869–77. doi: 10.1038/s41390-020-01189-5
48. Volpe JJ. Brain injury in the premature infant: neuropathology, clinical aspects, and pathogenesis. Ment. Retard Dev Disabil Res Rev. (1997) 5(3):3–12. doi: 10.1002/(SICI)1098-2779(1997)3:1%3C3::AID-MRDD2%3E3.0.CO;2-U
49. Fabres J, Carlo WA, Phillips V, Howard G, Ambalavanan N. Both extremes of arterial carbon dioxide pressure and the magnitude of fluctuations in arterial carbon dioxide pressure are associated with severe intraventricular hemorrhage in preterm infants. Pediatrics. (2007) 119(2):299–305. doi: 10.1542/peds.2006-2434
50. Erickson SJ, Grauaug A, Gurrin L, Swaminathan M. Hypocarbia in the ventilated preterm infant and its effect on intraventricular haemorrhage and bronchopulmonary dysplasia. J Paediatr Child Health. (2002) 38(6):560–2. doi: 10.1046/j.1440-1754.2002.00041.x
51. Greisen G, Vannucci RC. Is periventricular leucomalacia a result of hypoxic-ischaemic injury? Hypocapnia and the preterm brain. Biol Neonate. (2001) 79(3-4):194–200. doi: 10.1159/000047090
52. Pryds O. Control of cerebral circulation in the high-risk neonate. Ann Neurol. (1991) 30(3):321–9. doi: 10.1002/ana.410300302
53. Tsuji M, Saul JP, du Plessis A, Eichenwald E, Sobh J, Crocker R, et al. Cerebral intravascular oxygenation correlates with mean arterial pressure in critically ill premature infants. Pediatrics. (2000) 106(4):625–32. doi: 10.1542/peds.106.4.625
54. Soul JS, Hammer PE, Tsuji M, Saul JP, Bassan H, Limperopoulos C, et al. Fluctuating pressure-passivity is common in the cerebral circulation of sick premature infants. Pediatr Res. (2007) 61(4):467–73. doi: 10.1203/pdr.0b013e31803237f6
55. Alderliesten T, Lemmers PM, van Haastert IC, de Vries LS, Bonestroo HJ, Baerts W, et al. Hypotension in preterm neonates: low blood pressure alone does not affect neurodevelopmental outcome. J Pediatr. (2014) 164(5):986–91. doi: 10.1016/j.jpeds.2013.12.042
56. Woodward LJ, Anderson PJ, Austin NC, Howard K, Inder TE. Neonatal MRI to predict neurodevelopmental outcomes in preterm infants. N Engl J Med. (2006) 355(7):685–94. doi: 10.1056/NEJMoa053792
Keywords: neonates, preterm infants, magnetic resonance imaging, intraventricular hemorrhage, white matter injury, near-infrared spectroscopy, regional cerebral oxygen saturation
Citation: Ćaleta T, Ryll MJ, Bojanić K, Dessardo NS, Schroeder DR, Sprung J, Weingarten TN, Radoš M, Kostović I and Grizelj R (2024) Regional cerebral oxygen saturation variability and brain injury in preterm infants. Front. Pediatr. 12: 1426874. doi: 10.3389/fped.2024.1426874
Received: 15 May 2024; Accepted: 9 July 2024;
Published: 22 July 2024.
Edited by:
Graeme R. Polglase, Monash University, AustraliaReviewed by:
Mark Steven Scher, Case Western Reserve University, United StatesFrank Van Bel, University Medical Center Utrecht, Netherlands
© 2024 Ćaleta, Ryll, Bojanić, Dessardo, Schroeder, Sprung, Weingarten, Radoš, Kostović and Grizelj. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ruža Grizelj, cnV6YS5ncml6ZWxqQGtiYy16YWdyZWIuaHI=
†These authors have contributed equally to this work and share first authorship