
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 25 June 2024
Sec. Pediatric Urology
Volume 12 - 2024 | https://doi.org/10.3389/fped.2024.1409608
 Santiago Vallasciani1,2*
Santiago Vallasciani1,2* Ahmed Al Saeedi3
Ahmed Al Saeedi3 Ibrahim A. Khalil3
Ibrahim A. Khalil3 Reem Babiker Mohamed4Eshan Muneer4
Reem Babiker Mohamed4Eshan Muneer4 Nadra Abdelmaguid4Joao Luiz Pippi Salle1
Nadra Abdelmaguid4Joao Luiz Pippi Salle1
Introduction: Lower urinary tract dysfunction (LUTD) in cerebral palsy (CP) and other neuromuscular diseases can present with chronic retention that leads to hydronephrosis, recurrent urinary tract infections (UTI), and stone formation. Whenever the conservative treatment of LUTD fails for any reason, it is considered to be complicated LUTD, in which a surgical approach is warranted. Cutaneous vesicostomy (CV) is a simple, well-tolerated, and potentially reversible procedure that protects the upper tracts. We describe our experience using CV for this complex population.
Materials and methods: Children with CP and other neuromuscular diseases admitted to pediatric long-term care units for palliative care between 2015 and 2019 were included in the study. They present multi-system involvement, polypharmacy, and Gross Motor Function Classification System levels of 4 or 5. We retrospectively studied this population's indications and results of CV.
Results: Of the 52 admitted patients, 18 presented LUTD with UTI (n:18; 100%), stones (n:5; 28%), progressive hydroureteronephrosis (n:3; 17%), or stones (n:2; 11%). Conservative initial management (catheterizations, prophylaxis antibiotics) was effective in half the cases. The remaining nine were defined as complicated LUTD and underwent CV. After a mean follow-up of 11.3 months, the follow-up showed improved hydronephrosis in all nine (100%) patients. Recurrent UTIs were no longer seen in eight of nine patients, although three patients required bladder irrigations; bladder stones did not recur after CV; the kidney stones needed further intervention. Revision of the CV was required in two (11%) cases at 12 and 24 months postoperatively due to stoma stenosis.
Conclusion: CV is a relatively simple and effective procedure representing a pragmatic solution for managing complicated LUTD in complex long-term institutionalized pediatric palliative care patients with neuropathic bladders.
Children with chronic life-limiting diseases and dependent on respiratory technology are a growing subset within the category of children with special health needs (CSHN). There is a general perception that the number of these children living with chronic life-limiting medical conditions is increasing due to all recent advances in medicine and medical technology. These children form a very heterogeneous group based on their diagnoses. A recent study from the United States showed that children with chronic complex conditions encompass an increasing proportion of the inpatient population and are high-intensity users of hospital resources (1).
Children with chronic and life-limiting diseases that involve multiple systems and organs are usually admitted to long-term facilities to provide palliative care when indicated. Those patients tend to have a poorer quality of life. Lower urinary tract dysfunction (LUTD) in those patients is mainly characterized by chronic retention that leads to progressive hydronephrosis, recurrent urinary tract infection (UTI), stone formation, and chronic kidney disease, all of which are complex problems to manage in this compromised population (2–5).
The management of LUTD in these patients is complex. It ranges from conservative measures, such as clean intermittent catheterization (CIC) and continuous antibiotic prophylaxis (CAP) that are attempted initially. Still, many fail due to complications or institutional difficulties in maintaining the program (4). These cases can be defined as complicated LUTD as a surgical approach is warranted to decompress the bladder and stabilize their condition after failure using conservative means. Cutaneous vesicostomy (CV) is an available option to decompress the bladder in these circumstances (6, 7).
Herein, we describe our experience using CV for this complex population. We hypothesize that CV is a practical and efficient alternative for managing neurogenic bladder, improving symptoms of LUTD, and stabilizing the upper urinary tract not only in newborns but even in older children and adolescents.
After approval from the institutional review board (IRB no. 1592907), we performed a retrospective chart review of cerebral palsy (CP) patients with LUTD managed between 2015 and 2019.
The definitions are as follows:
- LUTD was defined as chronic retention of urine observed by dribbling and or residual urine in the bladder higher than 20% of the expected bladder capacity by age (measured by ultrasound, bladder scan, and/or voiding cystourethrogram). Other ultrasound findings, such as bladder thickness of more than 5 mm and or irregularity/trabeculation of the bladder wall and stones, were also considered identifiers of LUTD. We defined complicated LUTD as those cases of LUTD that required surgical intervention after failure using conservative treatment.
- Study population: children with CP and chronic and life-limiting diseases necessitate admission to pediatric long-term care units as a step down from high dependency units to allow for continuity of care and provide palliative care when indicated. The study population shares common characteristics like multi-system involvement, polypharmacy, Gross Motor Function Classification System (GMFCS) levels of 4 or 5, frequent and prolonged hospital admissions, and the need for optimal care coordination.
- All patients were kept in diapers, and urinary tract investigations were only performed when LUTD was suspected because of recurrent febrile UTI. Ultrasound with an assessment of the post-void residual urine, voiding cystourethrogram, and nuclear scans were performed for them. Initial management included CIC, bladder washouts, and antibiotic prophylaxis. If, despite the initial management, the patient developed further UTI, they were defined as complicated LUTD and underwent CV using the Blockson technique, modified by Krahn and Johnson by advancing more of the posterior bladder wall up to the skin, and suturing the bladder detrusor to the anterior rectus fascia and skin (6).
The primary outcome was a complete resolution of the signs of complicated LUTD. Secondary outcomes were the need for further conservative measures necessary to treat the persistence of symptoms of complicated LUTD after CV.
During the period studied, 52 patients were admitted to the long-term complex care facility. Of them, 50 were at GMFCS level 4–5. Of these 50 patients, 18 (36%) presented with signs and symptoms of LUTD with one or more of the following: UTI in 18 (36%), stones in 2 (11%), or progressive hydroureteronephrosis (SFU grade 3 or 4, ureters diameter 7 mm or more) in 3 (6%). They were then categorized as symptomatic LUTD. Of them, nine (50%) developed complicated LUTD and underwent CV.
Patient demographics and clinical features are presented in Table 1. After a mean of 11.3 months after CV (range 6–24 months), all the patients were emptying the bladder well.
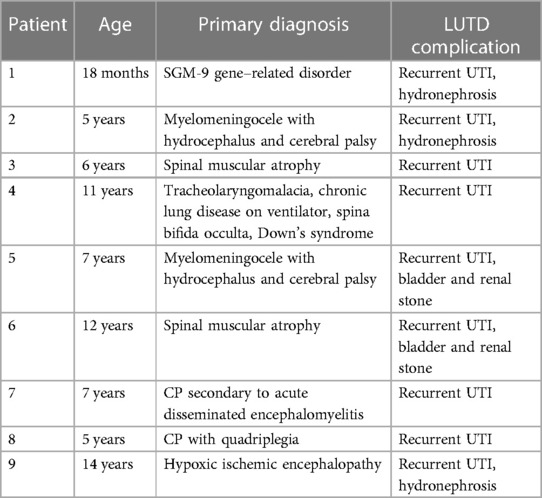
Table 1 Age and the primary diagnosis of the patients with LUTD.
Preoperative hydronephrosis was reduced in all the patients after CV. Five patients (55%) had complete resolution of recurrent UTIs without further maneuvers. Three of the remaining four patients were managed using bladder irrigation with gentamycin for 7 days followed by normal saline irrigation through vesicostomy to avoid further UTI. Bladder stones were removed at the time of vesicostomy and none recurred; however, the kidney stones were managed separately later. Revision of the vesicostomy was required in two (11%) cases at 12 and 24 months postoperatively due to stoma stenosis. No other significant complications (Clavien–Dindo grade 2 and above) were recorded.
The flow chart of patients included in the study is outlined in Figure 1.
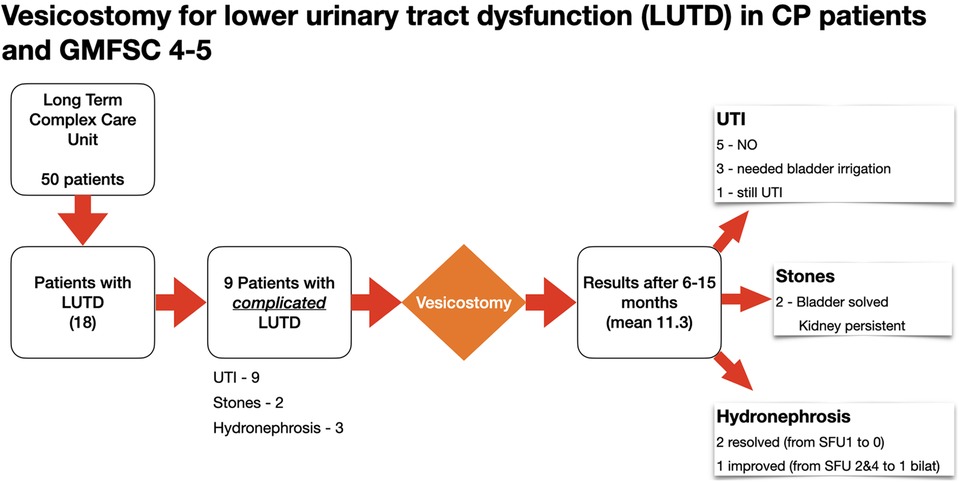
Figure 1 Flow chart of patients included in the study and the outcome.
LUTD is not uncommon among patients with CP. In their review, Samijn et al. (2) found that about half of patients with CP present LUTD secondary to detrusor overactivity rather than pelvic floor overactivity. The former has a higher impact in the upper tracts with hydronephrosis, secondary reflux, and pyelonephritis. It seems more frequent in high levels of GMFCS, as observed by Bross et al. (3). LUTD can be classified according to the cause for neurogenic and non-neurogenic LUTD (8); in our population the presence of high GMFCS levels in 50 out of 52 patients explains why symptomatic LUTD was present in 36% and half of them were complicated LUTD. In addition, as our population had neuroanatomic or neuromuscular diseases, a neuropathic etiology was proposed even if urodynamic studies were not carried out in our study population, as invasive urodynamics is difficult to perform or interpret in this fragile bedridden population.
The management of LUTD in this complicated patient category varies and ranges from review and modification of patients’ medications, such as discontinuation of anticholinergic medications or addition of alpha-adrenergic blockers, along with other conservative measures, such as CIC to CV or even more sophisticated alternatives such as the construction of abdominal catheterizable stomas (Mitrofanoff channel). However, they are more complex procedures that require significant involvement of specialized care and CIC (9, 10).
The CV, as described by Blockson and modified by Krahn and Johnson (6), is a relatively simple surgical procedure to treat LUTD in complex patients with minimal morbidity (7, 11). The modification of the CV by Krahn and Johnson results in fewer stomal complications, such as stenosis and prolapse, and reduces the need for intermittent stoma catheterization (6). The CV also presents stable results over time with reduced stoma stenosis. In our series, the two cases that needed surgical revision were both post-pubertal patients. As previously reported, it may be hypothesized that skin healing characteristics may have played a role (12). Another possible reason for stenosis/CV revision in older patients, as in our cases, is the larger size of the patient and the need to span a longer distance from the retropubic space to the skin. This could affect the vascularity of the exposed stoma.
As seen in our study, CV was instrumental in decompressing the urinary tract and significantly diminishing the number of recurrent UTIs. In addition, it allowed for irrigation of the bladder with antibiotics through the stoma in the more recalcitrant cases. Salih et al. found similar results in the resolution of UTI, hydronephrosis, and improvement of functional outcome after CV for bladder outlet obstruction in patients with CP (11).
Although the CV is safe and effective, it should not be considered for all patients with neurogenic bladders who preferably should be decompressed using CIC with or without continent catheterizable stoma (9, 10). However, in our particular population of institutionalized long-term care patients, often with other significant comorbidities, those complex procedures are risky and demand special postoperative care (1, 5).
The present study has some limitations. These include the small number of patients, the retrospective design, and that no patient underwent urodynamics studies; however, it provides a pragmatic alternative for such a complex and unfortunate population. The initial results encourage us to propose CV for management and possible validation by other healthcare providers involved in the care of long-term institutionalized patients with LUTD.
CV is a simple and effective procedure for complicated LUTD in complex institutionalized long-term patients with neuropathic bladders. As well as effective urinary decompression, it also provides alternative access for bladder washouts whenever necessary for the management of recurrent UTIs.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the Institutional Review Board (IRB) of Sidra Medicine. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin as this was a retrospective study with no impact on the individuals’ management plan. Written informed consent was not obtained from the minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article because of the IRB-approved waiver of consent.
SV: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Writing – original draft. AA: Data curation, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. IK: Data curation, Investigation, Methodology, Writing – original draft. RM: Supervision, Writing – review & editing. EM: Supervision, Writing – review & editing. NA: Supervision, Writing – review & editing. JP: Conceptualization, Investigation, Methodology, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
Publication was funded by Sidra Medicine.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Simon TD, Berry J, Feudtner C, Stone BL, Sheng X, Bratton SL, et al. Children with complex chronic conditions in inpatient hospital settings in the United States. Pediatrics. (2010) 126:647–55. doi: 10.1542/peds.2009-3266
2. Samijn B, Van Laecke E, Renson C, Hoebeke P, Plasschaert F, Vande Walle J, et al. Lower urinary tract symptoms and urodynamic findings in children and adults with cerebral palsy: a systematic review. Neurourol Urodyn. (2017) 36:541–9. doi: 10.1002/nau.22982
3. Bross S, Honeck P, Kwon ST, Badawi JK, Trojan L, Alken P. Correlation between motor function and lower urinary tract dysfunction in patients with infantile cerebral palsy. Neurourol Urodyn. (2007) 26:222–7. doi: 10.1002/nau.20329
4. Murphy KP, Boutin SA, Ide KR. Cerebral palsy, neurogenic bladder, and outcomes of lifetime care. Dev Med Child Neurol. (2012) 54:945–50. doi: 10.1111/j.1469-8749.2012.04360.x
5. Reid CJ, Borzyskowski M. Lower urinary tract dysfunction in cerebral palsy. Arch Dis Child. (1993) 68:739–42. doi: 10.1136/adc.68.6.739
6. Krahn CG, Johnson HW. Cutaneous vesicostomy in the young child: indications and results. Urology. (1993) 41:558–63. doi: 10.1016/0090-429590104-i
7. Prudente A, Reis LO, França Rde P, Miranda M, D'ancona CA. Vesicostomy as a protector of upper urinary tract in long-term follow-up. Urol J. (2009) 6:96–100. doi: 10.22037/uj.v6i2.250
8. Ginsberg DA, Boone TB, Cameron AP, Gousse A, Kaufman MR, Keays E, et al. The AUA/SUFU guideline on adult neurogenic lower urinary tract dysfunction: diagnosis and evaluation. J Urol. (2021) 206(5):1097–105. doi: 10.1097/JU.0000000000002235
9. Nast KJ, Chiang G, Marietti S. Vesicostomy button: how is it placed, in whom, and how is quality of life affected? Int Braz J Urol. (2019) 45:807–14. doi: 10.1590/S1677-5538.IBJU.2018.0686
10. Narwade SS, Sawant AS, Tamhankar AS, Patil SR, Patil KR. Mitrofanoff urinary diversion in a patient with cerebral palsy. Pediatric Urology Case. (2017) 4:320–4. doi: 10.14534/PUCR.2017327013
11. Salih EM, Abdrabuh AM, Okasha AH, Galal H. Temporary vesicostomy in pediatrics: what are the potential predictors of functional and morphological improvement of the upper urinary tract? J Pediatr Urol. (2021) 17:834–1. doi: 10.1016/j.jpurol.2021.09.016
Keywords: vesicostomy, lower urinary tract dysfunction (LUTD), neuropathic bladder, cerebral palsy, neurogenic bladder dysfunction, chronic life-limiting disease, neuromuscular disease
Citation: Vallasciani S, Al Saeedi A, Khalil IA, Mohamed RB, Muneer E, Abdelmaguid N and Pippi Salle JL (2024) Permanent cutaneous vesicostomy: a pragmatic approach to safely manage lower urinary tract dysfunction in pediatric patients with chronic and life-limiting conditions and neuropathic bladders. Front. Pediatr. 12:1409608. doi: 10.3389/fped.2024.1409608
Received: 30 March 2024; Accepted: 28 May 2024;
Published: 25 June 2024.
Edited by:
Ezekiel E. Young, University at Buffalo, United StatesReviewed by:
John Samuel Wiener, Duke University, United States© 2024 Vallasciani, Al Saeedi, Khalil, Mohamed, Muneer, Abdelmaguid and Pippi Salle. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Santiago Vallasciani, c2FudGlhZ28udmFsbGFzY2lhbmlAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.