
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Pediatr., 07 June 2024
Sec. Pediatric Critical Care
Volume 12 - 2024 | https://doi.org/10.3389/fped.2024.1397232
 Teresa B. Kortz1,2*
Teresa B. Kortz1,2* Rishi P. Mediratta3
Rishi P. Mediratta3 Audrey M. Smith4
Audrey M. Smith4 Katie R. Nielsen5
Katie R. Nielsen5 Asya Agulnik6
Asya Agulnik6 Stephanie Gordon Rivera2
Stephanie Gordon Rivera2 Hailey Reeves7Nicole F. O’Brien8
Hailey Reeves7Nicole F. O’Brien8 Jan Hau Lee9,10
Jan Hau Lee9,10 Qalab Abbas11
Qalab Abbas11 Jonah E. Attebery12,13
Jonah E. Attebery12,13 Tigist Bacha14Emaan G. Bhutta15
Tigist Bacha14Emaan G. Bhutta15 Carter J. Biewen1
Carter J. Biewen1 Jhon Camacho-Cruz16
Jhon Camacho-Cruz16 Alvaro Coronado Muñoz17
Alvaro Coronado Muñoz17 Mary L. deAlmeida18
Mary L. deAlmeida18 Larko Domeryo Owusu19
Larko Domeryo Owusu19 Yudy Fonseca20Shubhada Hooli21
Yudy Fonseca20Shubhada Hooli21 Hunter Wynkoop8
Hunter Wynkoop8 Mara Leimanis-Laurens22
Mara Leimanis-Laurens22 Deogratius Nicholaus Mally23
Deogratius Nicholaus Mally23 Amanda M. McCarthy24
Amanda M. McCarthy24 Andrew Mutekanga25Carol Pineda26
Andrew Mutekanga25Carol Pineda26 Kenneth E. Remy27
Kenneth E. Remy27 Sara C. Sanders28Erica Tabor29
Sara C. Sanders28Erica Tabor29 Adriana Teixeira Rodrigues30
Adriana Teixeira Rodrigues30 Justin Qi Yuee Wang31
Justin Qi Yuee Wang31 Niranjan Kissoon32Yemisi Takwoingi33
Niranjan Kissoon32Yemisi Takwoingi33 Matthew O. Wiens34,35,†
Matthew O. Wiens34,35,† Adnan Bhutta36,†
Adnan Bhutta36,†  for the Global Health Subgroup of the Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network
for the Global Health Subgroup of the Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network
In 2019, 80% of the 7.4 million global child deaths occurred in low- and middle-income countries (LMICs). Global and regional estimates of cause of hospital death and admission in LMIC children are needed to guide global and local priority setting and resource allocation but are currently lacking. The study objective was to estimate global and regional prevalence for common causes of pediatric hospital mortality and admission in LMICs. We performed a systematic review and meta-analysis to identify LMIC observational studies published January 1, 2005-February 26, 2021. Eligible studies included: a general pediatric admission population, a cause of admission or death, and total admissions. We excluded studies with data before 2,000 or without a full text. Two authors independently screened and extracted data. We performed methodological assessment using domains adapted from the Quality in Prognosis Studies tool. Data were pooled using random-effects models where possible. We reported prevalence as a proportion of cause of death or admission per 1,000 admissions with 95% confidence intervals (95% CI). Our search identified 29,637 texts. After duplicate removal and screening, we analyzed 253 studies representing 21.8 million pediatric hospitalizations in 59 LMICs. All-cause pediatric hospital mortality was 4.1% [95% CI 3.4%–4.7%]. The most common causes of mortality (deaths/1,000 admissions) were infectious [12 (95% CI 9–14)]; respiratory [9 (95% CI 5–13)]; and gastrointestinal [9 (95% CI 6–11)]. Common causes of admission (cases/1,000 admissions) were respiratory [255 (95% CI 231–280)]; infectious [214 (95% CI 193–234)]; and gastrointestinal [166 (95% CI 143–190)]. We observed regional variation in estimates. Pediatric hospital mortality remains high in LMICs. Global child health efforts must include measures to reduce hospital mortality including basic emergency and critical care services tailored to the local disease burden. Resources are urgently needed to promote equity in child health research, support researchers, and collect high-quality data in LMICs to further guide priority setting and resource allocation.
As of 2019, 73 countries had not achieved the United Nations Sustainable Development Goal (SDG) 3.2 (1) to “end preventable” child mortality (2). In that same year, 7.4 million infants, children, and adolescents died globally from primarily treatable causes (3). More than 80% of these deaths occurred in low- and middle-income countries (LMICs), representing a devastating global inequity (4).
Pediatric hospital mortality is also higher in LMICs compared to high-income countries (5–7). Most hospital deaths could be avoided with reliable, timely high-quality emergency and critical care services (8–11), which are limited due to underfinanced health systems and insufficient equipment, trained personnel, and medications (12). Recognizing this, the World Health Organization (WHO) recommended strengthening emergency and critical care globally (13, 14). A better understanding of reasons children are admitted to and die in LMIC hospitals is necessary to set a prioritized agenda and advocate for resources to target the greatest drivers of morbidity and mortality in hospitalized children.
Estimates of cause specific pediatric LMIC hospital mortality and admission by region and globally are unknown. Global child mortality data from the Global Burden of Disease (GBD) studies, WHO, and United Nations Children's Fund (UNICEF) include rates and causes of death (4, 15–17); however, these population-level estimates do not provide facility-level data (18). Additionally, these estimates may not be accurate due to imputation methods (19). Many studies have reported the epidemiology of acute pediatric illness in a single hospital or country, but fail to provide regional or global estimates (20–22). To address these gaps, we conducted a systematic review and meta-analysis to determine common causes of pediatric hospital mortality and admission in LMICs.
We followed published guidelines for systematic reviews of observational studies (CoCoPop framework), PRISMA and GATHER reporting standards (Supplementary Tables S1, S2) (23–25). The study was organized by the Pediatric Acute Lung Injury and Sepsis Investigator (PALISI) Global Health subgroup, reviewed by the PALISI Scientific Committee, and registered with PROSPERO (#230228). The multinational Working Group (WG) was comprised of subject matter and methodology experts. We identified eligible studies by searching MEDLINE, EMBASE, CINAHL, and LILACS using MeSH terms and keywords (Supplementary Table S3). Searches were performed by an academic librarian (SG) on November 6, 2019, with a gap analysis on March 1, 2021 (Supplementary Tables S4, S5). The protocol was published (26), and amendments are detailed in the (Supplementary Appendix S1).
The primary condition was the reported, principal cause of pediatric hospital mortality by organ system. We selected an organ system-based categorization for causes of death/admission to inform general resource requirements (Supplementary Table S6). For example, the “Respiratory System” includes common conditions (pneumonia, bronchiolitis, asthma) that require respiratory support (oxygen, mechanical ventilation). Multi-organ infections (malaria) were categorized as “Non-Organ Specific Infectious Diseases”. When more than one cause was listed (malaria with anemia), members of the WG determined the principal cause and attributed cases to only the principal cause.
Studies were eligible for inclusion if published between January 1, 2005 and February 26, 2021, and data were collected after 2000. We chose these criteria to reflect recent trends in pediatric hospitalization and mortality. We determined LMIC status using the GBD 2017 Socio-Demographic Index (SDI), a composite indicator of a country's development status that correlates with health outcomes (27). We included countries within the low-, lower-middle, and middle-SDI quintiles in the search terms. Studies that presented aggregated data representing multiple countries were included if country-specific data could be extracted. We excluded publications not representative of the LMIC setting (medical mission, foreign military hospital).
We included children admitted to a hospital (non-birth admission) in an LMIC aged 0 days-18 years. To focus on a general pediatric admission population instead of a neonatal population, we excluded studies conducted in newborn nurseries or neonatal intensive care units, any study where >50% of the sample were neonates (3, 15), and neonatal specific conditions (neonatal tetanus, birth asphyxia). Conditions not specific to neonates (tetanus, pneumonia) were categorized as described above.
Included studies reported total number of children admitted to the hospital. We excluded studies that sampled only specific patient populations and studies with exclusion criteria that resulted in a different case mix than a general pediatric hospital admission population. The WG evaluated publications from the same data source and, if the populations overlapped, we retained the most recent or relevant study. Full texts in Spanish, English, and French were included (Supplementary Figure S1).
We used Covidence (Veritas Health Innovation, Melbourne, Australia) for screening, text upload, and conflict resolution (28). Duplicates were removed, titles/abstracts and full texts were independently screened by two WG members, and conflicts were resolved by a third member. Two WG members extracted data using a case report form (Supplementary Table S7) in REDCap (29), and conflicts were adjudicated by a third member. We made no assumptions about missing or ambiguous data. We extracted data from studies reporting multiple sites as separate records if participant-level data were available for each site; studies with data aggregated across sites were extracted as one record. WG members independently assessed the risk of bias based on relevant domains adapted from the Quality in Prognosis Studies (QUIPS) tool (30): (1) study participation (generalizability to underlying population); (2) study attrition; and (3) factor measurement (cause of admission/death) (Supplementary Table S8). We resolved risk of bias assessment conflicts by consensus.
The primary outcome was cause-specific proportions for hospital mortality, reported per 1,000 pediatric hospital admissions. Secondary outcomes included case fatality rates (CFRs), calculated as the number of deaths per 1,000 pediatric hospital admissions with a given system-based illness, and cause-specific proportions for hospital admission, reported per 1,000 pediatric hospital admissions. Included studies provided raw data for the denominator and numerator to estimate proportions and 95% confidence intervals (CI). We summarized data according to study- and outcome-level characteristics. To generate a global estimate, data from more than one GBD region were required, while for regional estimates, more than one study per system was required, else data were labeled as “Not reported.” We excluded “other” diagnoses, which were a heterogeneous group of conditions that differed between studies and precluded comparisons across regions.
We anticipated heterogeneity and performed meta-analyses of causes of death, CFRs, and causes of admission using random-effects models with the Freeman-Tukey double arcsine transformation and fixed-effect models when data were limited (31). We assessed statistical heterogeneity using the variance estimates from the random-effects models. We did not use the I2 statistic because the mean-variance relationship of proportions can lead to misleadingly high values (32). We performed sensitivity analyses to confirm that the transformation method did not affect the main results.
We performed subgroup analyses by GBD super-region by using each covariate for stratification in the relevant meta-analysis. Additional subgroup analyses were not possible due to poor reporting of potential sources of heterogeneity. We reported summary estimates overall and according to GBD super-regions: Central Europe, Eastern Europe, and Central Asia (CE); Latin America and Caribbean (LA); North Africa and Middle East (NA); South Asia (SA); Southeast Asia, East Asia, and Oceania (SEA); and Sub-Saharan Africa (SSA) (33). A p-value < 0.05 was considered statistically significant. All analyses were performed using the STATA (version 17) metan command.
We identified 29,637 texts, removed 12,336 duplicates, screened 17,301 abstracts, and assessed 2,256 full texts for inclusion (Figure 1, Supplementary Appendix S2). Of the 253 publications included, the majority were cohort studies published after 2010. The highest number of studies came from Nigeria (N = 45, 15%), followed by Kenya (N = 27, 9%, Supplementary Figure S2). Included studies represented a total of 21,762,798 pediatric hospital admissions from 293 hospitals in 59 LMICs and six GBD super-regions (Supplementary Table S9). SSA had the highest number of sites of any super-region (N = 187, 64%). Twenty-six percent (N = 76) of sites were urban and 15% (N = 44) were rural; 59% (N = 173) of sites did not report urban or rural status. Among all study sites, 9% (N = 25) were conducted in children's hospitals while 46% (N = 135) were not; 45% (N = 133) did not report this information. A pediatric or general intensive care unit was present in 12% (N = 35) of study hospitals, and not present or not reported in 82% (N = 243). We observed heterogeneity in outcome estimates between studies and regions (see estimates of τ2 in the Supplementary tables).
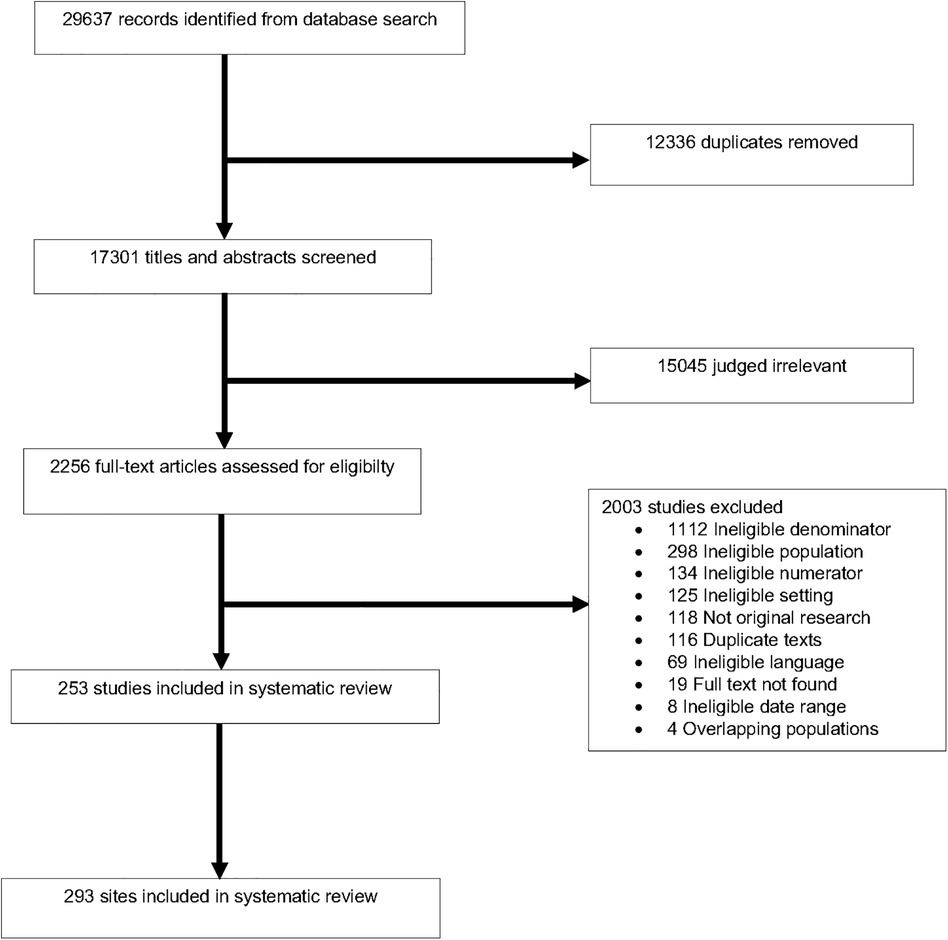
Figure 1. Study selection process. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA) flowchart for title and abstract screening and text selection from the final search (conducted March 1, 2021).
Over 60% of included studies had a low risk of bias in the three domains evaluated (Supplementary Figure S3). A high risk of bias was found in 8% (N = 21) of studies for “Study Participation”; 5% (N = 14) of studies for “Study Attrition”; and 13% (N = 33) of studies for “Measurement Bias”.
All-cause pediatric hospital mortality was 4.1% (95% CI 3.4%–4.7%), and summary estimates varied by region: SA had the highest all-cause hospital mortality [5.7% (95% CI 2.2–10.7%)] and NA had the lowest [1.5% (95% CI 0.5%–3.0%), Figure 2].
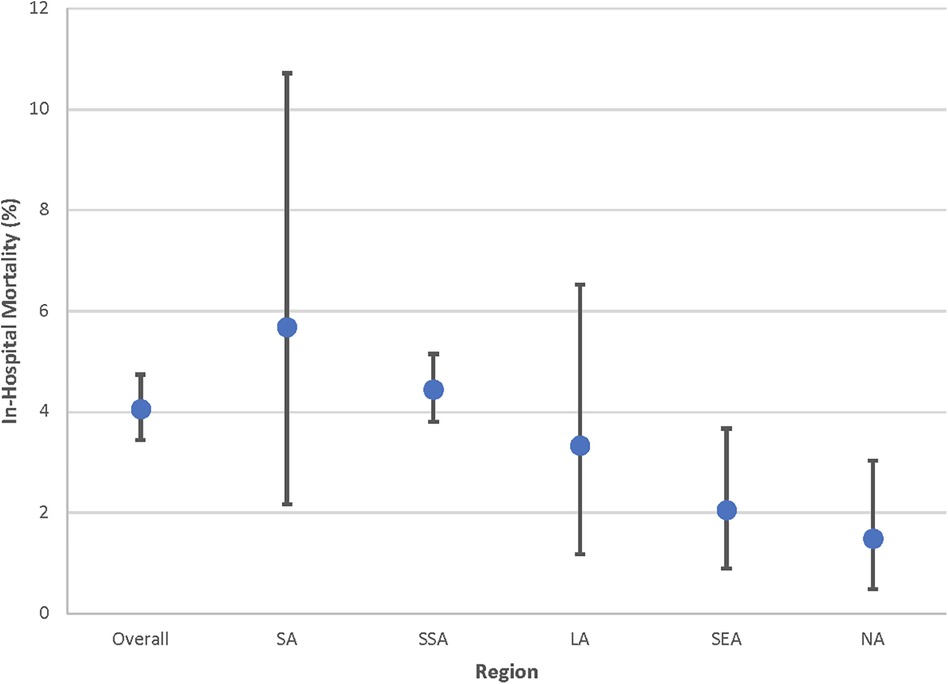
Figure 2. All-cause pediatric hospital mortality by Global Burden of Disease (GBD) super region. Point estimates and 95% confidence intervals shown. Estimates for Central Europe, Eastern Europe, and Central Asia (CE) are not included given limited data. LA, Latin America and Caribbean; NA, North Africa and Middle East; SA, South Asia; SEA, Southeast Asia, East Asia, and Oceania; SSA, Sub-Saharan Africa.
The most common causes of hospital death were non-organ specific infectious diseases, respiratory conditions, and gastrointestinal conditions (deaths/1,000 admission: 12 [95% CI 9–14]; 9 [95% CI 5–13], and 9 [95% CI 6–11], respectively) (Figure 3 and Supplementary Figure S4). The highest proportion of deaths due to non-organ specific infectious diseases occurred in SSA [14 deaths/1,000 admissions (95% CI 11–18)] and SA [13 deaths/1,000 admissions (95% CI 4–26)]. The highest proportion of deaths due to respiratory conditions also occurred in SA [10 deaths/1,000 admissions (95% CI 4–18)] and SSA [9 deaths/1,000 admissions (95% CI 6–12)]. The highest proportion of deaths due to gastrointestinal conditions occurred in NA [16 deaths/1,000 admissions (95% CI 13–20)].
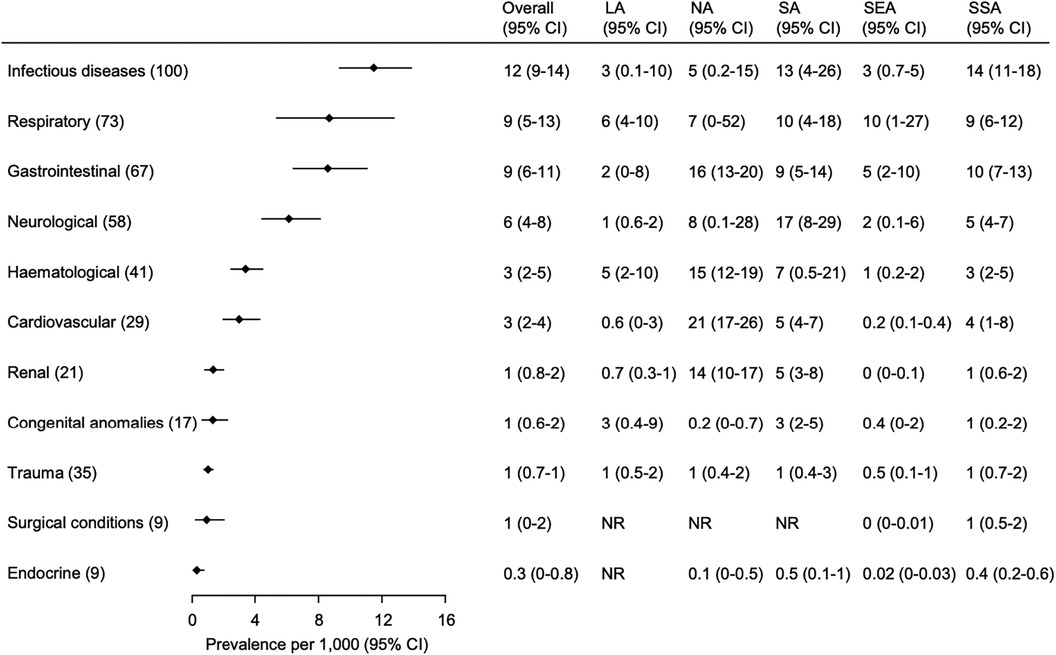
Figure 3. Common causes of hospital mortality in children by organ system and GBD super region. Organ systems are ordered according to the overall rate (number of children with a cause of death/1,000 children admitted) and the number in parenthesis next to each organ system represents the number of studies included in the analysis. Overall and GBD super region mortality rates are presented as pooled estimates from random-effects models with 95% confidence intervals (CI). Estimates for Central Europe, Eastern Europe, and Central Asia (CE) are not included given limited data. The hematological category includes oncological conditions. The numbers in () next to each category in the left column are the number of studies included in the overall analysis shown on the right. The categories are sorted according to the overall proportion across the super regions. The hematological category includes oncological conditions. LA, Latin America and Caribbean; NA, North Africa and Middle East; SA, South Asia; SEA, Southeast Asia, East Asia, and Oceania; SSA, Sub-Saharan Africa; CI, Confidence Interval; NR, not reported.
The highest overall CFRs occurred in neurological, cardiovascular, and congenital anomalies-related conditions (13% [95% CI 9%–18%], 11% [95% CI 6%–16%], and 8% [95% CI 4%–12%], respectively) (Figure 4 and Supplementary Figure S5). Neurological conditions had the highest CFR in NA [40% (95% CI 27%–53%)], while cardiovascular conditions and congenital anomalies had the highest CFR in SA (15% [95% CI 10%–22%] and 56% (95% CI 8%–98%), respectively).
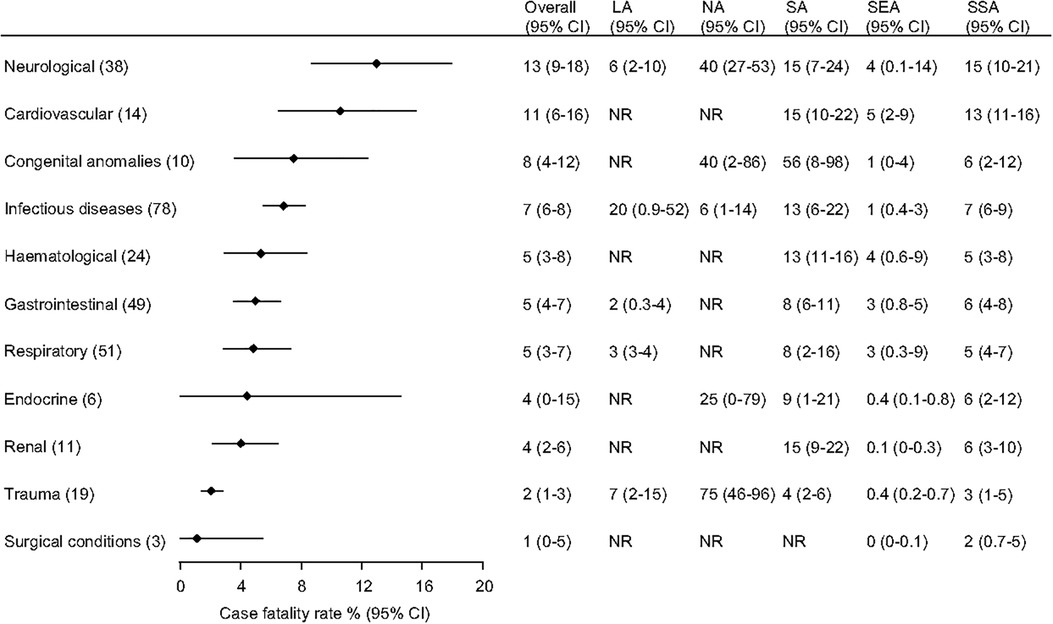
Figure 4. Case fatality rates in children admitted to hospital by organ system and Global Burden of Disease (GBD) super region. Organ systems are ordered according to the overall fatality (number of children with a specific cause of death/1,000 children admitted with that cause) and the number in parenthesis next to each organ system represents the number of studies included in the analysis. Overall and GBD super region case fatality rates are presented as pooled estimates from random-effects models with 95% confidence intervals (CI). Estimates for Central Europe, Eastern Europe, and Central Asia (CE) are not included given limited data. The hematological category includes oncological conditions. The numbers in () next to each category in the left column are the number of studies included in the overall analysis shown on the right. The categories are sorted according to the overall proportion across the super regions. The hematological category includes oncological conditions. LA, Latin America and Caribbean; NA, North Africa and Middle East; SA, South Asia; SEA, Southeast Asia, East Asia, and Oceania; SSA, Sub-Saharan Africa; CI, Confidence Interval; NR, not reported.
The most common causes of pediatric admissions were respiratory conditions, non-organ specific infectious diseases, and gastrointestinal conditions (cases/1,000 admissions: 255 [95% CI 231–280]; 214 [95% CI 193–234]; 166 [95% CI 143–190], respectively) (Figure 5 and Supplementary Figure S6). CE had the highest proportion of admissions due to respiratory conditions [680 cases/1,000 admissions (95% CI 644–716)], while SSA had the highest proportion due to non-organ specific infectious diseases [281 cases/1,000 admissions (95% CI 227–338)], and SA had the highest proportion due to gastrointestinal conditions [216 cases/1,000 admissions (95% CI 153–287)].
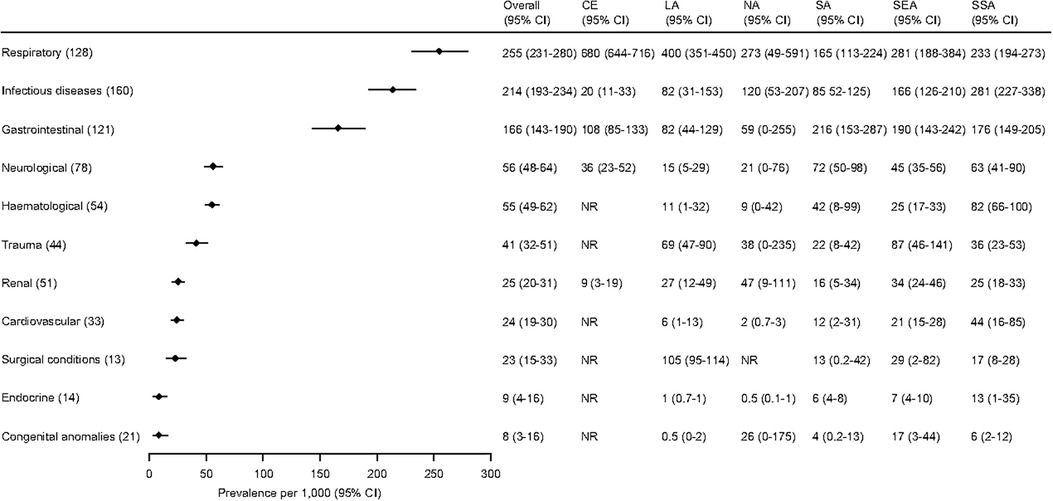
Figure 5. Common causes of hospital admission in children by organ system and Global Burden of Disease (GBD) super region. Organ systems are ordered according to the overall proportion of children with the cause of admission and the number in parenthesis next to each organ system represent the number of studies included in the analysis. Overall and GBD super region proportions are presented as pooled estimates from random-effects models with 95% confidence intervals (CI). Estimates for Central Europe, Eastern Europe, and Central Asia (CE) are based on a single study of 638 children. The hematological category includes oncological conditions. The numbers in () next to each category in the left column are the number of studies included in the overall analysis shown on the right. The categories are sorted according to the overall proportion across the super regions. The hematological category includes oncological conditions. CE, Central Europe, Eastern Europe, and Central Asia; LA, Latin America and Caribbean; NA, North Africa and Middle East; SA, South Asia; SEA, Southeast Asia, East Asia, and Oceania; SSA, Sub-Saharan Africa; CI, Confidence Interval; NR, not reported.
This is the first systematic review to comprehensively identify the most common causes of pediatric hospital mortality in LMICs. All-cause pediatric hospital mortality was 4%, consistent with data from East and West Africa and India (6%–12%) but in contrast to 0.8% and 0.05% in the United States and Scotland, respectively (34–39). Similar to data published by the WHO, UNICEF, and GBD, we observed differences in cause and burden of mortality across regions, and found that the major causes of pediatric acute illness (hospital admission and death) were due to non-organ specific infectious diseases, respiratory conditions, and gastrointestinal conditions (3, 4, 15–17). The conditions with the highest CFRs, however, differed from the most common causes of hospital admission and death. Neurological and cardiovascular conditions, while less common in pediatric compared to adult populations, can cause high mortality (40, 41); it is, therefore, not surprising that these conditions account for fewer cases of hospital admission and have the highest rates of mortality when they do occur (CFR). To have the greatest impact on pediatric hospital mortality, however, LMIC hospitals should focus on management of the most frequent causes of hospital admission and death as opposed to the conditions with the highest CFRs. For the greatest regional impact on outcomes, LA and SEA hospitals should focus on respiratory conditions, while SSA hospitals should focus on non-organ specific infectious diseases. Primary prevention through vaccination; water, sanitation, and hygiene programs; improved nutrition; and mosquito control efforts are effective at reducing pediatric hospital admission directly and mortality indirectly (42–48). However, public health interventions alone are insufficient; child health efforts must also include improvements in hospital care. Simple, cost-effective strategies exist to manage common causes of pediatric admission (9, 45, 49, 50); yet, hospital mortality remains high. Most hospital deaths and long-term morbidity can be avoided with adequate emergency and critical care resources (8, 9, 11, 37). In Sierra Leone, improving emergency care processes, staffing, and resource availability decreased paediatric hospital mortality from 12%–6% (37). The basic tools necessary to deliver basic emergency and critical care and to identify and treat hospitalized patients at high risk of mortality are effective, low-cost, and low-tech (8, 37). For example, most infectious disease-related deaths are due to sepsis, and sepsis bundles have been shown to reduce mortality (51–53). Respiratory conditions can progress to respiratory failure and death; effective management includes pulse oximetry, oxygen therapy, and non-invasive and invasive ventilation (5, 54). Gastrointestinal illnesses can progress to severe dehydration and death, which can be treated with oral rehydration solution and/or intravenous fluids (IVF) (50). A recent survey of 238 hospitals in 60 countries, however, identified inconsistent availability of key resources required to care for acutely ill children including sepsis bundle resources, basic respiratory support, and dextrose-containing IVF (12). There is an urgent need for basic pediatric emergency and critical care resources in LMIC hospitals to manage common causes of admission and reduce preventable mortality (Supplementary Table S10) (8, 12).
While our analysis demonstrated global trends and regional differences in hospital mortality, admission, and CFR, country socio-economic development also impacts child outcomes (55), and is associated with resource availability and access to care (12, 56). In a global study of paediatric severe sepsis and septic shock, Tan, et al. found that the pooled CFR was 32% in “less developed” compared with 19% in more developed countries (7). Likewise, McAllister, et al., found that the CFR for children hospitalized with pneumonia was higher in low- compared to middle-income countries (6). Collectively, these findings suggest that regional differences in disease burden, resource availability, and access to high-quality hospital care can impact child mortality. More research is needed to better understand the interplay and likely synergy between burden, resources, and access; interventions that address all three are likely to have the greatest impact on child health outcomes in LMICs.
There are notable strengths of this study. The results further and independently support WHO, UNICEF, and GBD findings for the top causes of global childhood mortality and, unlike prior, large-scale global studies, represent an exclusively hospitalized pediatric population of 21.8 million (3, 4, 15–17). The focus on organ systems allows for identification of required hospital resources to manage common conditions and reduce mortality. Furthermore, this systematic review relies on health facility-level data generated in LMICs, as opposed to estimates or imputation methods, a major criticism of previously published global health metrics (19).
There are also limitations. Our analysis was restricted to available, published data and, while the search criteria had no language restrictions, we were unable to evaluate full texts not in English, Spanish or French, which may have introduced a selection bias. Although some subgroups had few studies, which could lead to an inaccurate estimate of the between-study heterogeneity, the meta-analyses across subgroups for overall summary estimates had robust sample sizes. Though the study was designed to focus on a general pediatric population, it is important to note that neonatal subjects were included. This may have resulted in an underestimate of the causes of admission and death; neonates were accounted for in the denominator, but incompletely in the numerator. While this may have influenced summary estimates, excluding all studies with neonates would similarly have resulted in studies biased against other pediatric age groups (under five years). Observed regional differences may have been influenced by available data, study selection, local health systems, and health-seeking behaviors. While most included studies had a low risk of bias, risk due to missing results (arising from reporting biases) could not be assessed. Similar to other observational studies, we were limited to the reported cause of admission/death, often a clinician's diagnosis, which could result in misclassification and highlights the need for universal research methods including standard data elements and diagnostic definitions (57). Included studies represented LMICs disproportionately; some countries (Brazil) were overrepresented, while others (Sudan) contributed no data. Underrepresented countries tended to have fewer resources and political and/or economic instability, which can contribute to higher rates of childhood illness and mortality (3). We also excluded disease-specific studies that did not report total hospital admissions and outbreak studies, which may have resulted in an underestimation for certain diseases. We attempted to recategorize “other” diagnoses; however, many could not be recategorized, which may have resulted in an underestimate of disease burden. Finally, this study was designed to capture hospital admission and death and not pre-hospital or post-discharge death, which are significant contributors to morbidity and mortality in children in LMICs (58, 59). For these reasons, this large-scale systematic review, while the first of its kind, likely underestimates the overall burden of childhood hospital mortality in LMICs.
Common causes of pediatric hospital mortality in LMICs could be managed with basic, cost-effective emergency and critical care services. A coordinated global effort is required to address preventable child mortality by increasing access to care, deploying targeted interventions, allocating available resources strategically, and including emergency and critical care services in the global child health agenda (Figure 6). To further reduce global child mortality and achieve the SDG target, we need public health measures, health system strengthening, and increased hospital resources tailored to the local burden of disease (Supplementary Table S10). These findings are a call to action for increased, high-quality emergency and critical care resources in LMIC hospitals to prevent avoidable pediatric hospital mortality and effectively care for children with life-threatening conditions.

Figure 6. Actions to address preventable child mortality. This figure illustrates the coordinated global effort across multiple domains (e.g., healthcare quality) and levels (e.g., regional) that is required to address preventable child mortality.
The datasets presented in this study can be found in online repositories. The names of the repository and DOI can be found below: https://borealisdata.ca/dataverse/Pedi_SepsisCoLab; DOI: 10.5683/SP3/2UKUKW.
TK: Data curation, Project administration, Validation, Visualization, Writing – review & editing, Conceptualization, Funding acquisition, Methodology, Resources, Software, Supervision. RM: Conceptualization, Data curation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing, Formal Analysis. AS: Data curation, Validation, Visualization, Writing – original draft, Writing – review & editing, Project administration. KN: Data curation, Validation, Writing – review & editing, Conceptualization. AA: Writing – original draft, Writing – review & editing, Visualization. SG: Validation, Visualization, Writing – original draft, Writing – review & editing, Data curation, Project administration. HR: Data curation, Project administration, Validation, Writing – review & editing. NO: Conceptualization, Data curation, Validation, Writing – review & editing. JL: Conceptualization, Data curation, Validation, Writing – review & editing. QA: Validation, Writing – review & editing. JA: Data curation, Validation, Writing – review & editing. TB: Validation, Writing – review & editing. EB: Data curation, Validation, Writing – review & editing. CB: Validation, Writing – review & editing. JC-C: Validation, Writing – review & editing. AC: Conceptualization, Data curation, Validation, Writing – review & editing. MD: Data curation, Validation, Writing – review & editing. LD: Validation, Writing – review & editing. YF: Validation, Writing – review & editing. SH: Data curation, Validation, Writing – review & editing. HW: Data curation, Validation, Writing – review & editing. ML-L: Data curation, Validation, Writing – review & editing. DN: Validation, Writing – review & editing. AMM: Validation, Writing – review & editing. AM: Data curation, Validation, Writing – review & editing. CP: Data curation, Validation, Writing – review & editing. KR: Data curation, Validation, Writing – review & editing. SS: Data curation, Validation, Writing – review & editing. ET: Data curation, Validation, Writing – review & editing. AT: Validation, Writing – review & editing. JY: Validation, Writing – review & editing. NK: Conceptualization, Data curation, Validation, Writing – review & editing. YT: Formal Analysis, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. MW: Conceptualization, Data curation, Funding acquisition, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. AB: Conceptualization, Data curation, Funding acquisition, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
Research effort to create this publication was supported by the National Institute of Allergy and Infectious Diseases (award number K23AI144029, TK; award number 5U01AI126610, AB) of the National Institutes of Health (NIH), the Conquer Cancer Foundation (AA), the National Cancer Institute (award number R37CA276215, AA) of the NIH, the Eunice Kennedy Shriver National Institute of Child Health and Human Development (award number 1R21HD106252-01, NO) of the NIH, the National Institute of General Medical Sciences https://www.nigms.nih.gov/ (award number R01GM139046, KR) of the NIH, the Fogarty International Center (award Number D43TW012274, SH) of the NIH, the American Lung Association (award 920341, KR), the National Medical Research Council, Singapore (MOH-000446-00, JHL), the National Institute for Health Research (NIHR) Birmingham Biomedical Research Centre of the National Health Services (YT), and Grand Challenges Canada (NK). The views expressed are those of the author(s) and not necessarily those of the NIH, Singapore's MOH, NHS, NIHR, or the Department of Health and Social Care. The funders had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
We would like to thank Sue Groshong from Seattle Children's Hospital for help developing and executing the search strategy, and Maria Puerto Torres and Angela Puerta Torres from St. Jude for assistance in developing and refining the graphics.
JC-C speaker for Novamed and Tecnoquimicas; received financial travel support from BAGO to attend the Colombian Congress of Pediatrics; participated in an Advisory Board for ZambonColombia; acted as an investigator in phase 2 and 3 clinical trials of Merck Sharp and Dhome drugs (antibiotics and monoclonal antibodies) that do not interfere in the course of this study. JL stock options in MERCK and MODERNA.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor “CFO” declared a past co-authorship with the authors “NK & MOW”.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2024.1397232/full#supplementary-material
1. Sharrow D, Hug L, You D, Alkema L, Black R, Cousens S, et al. Global, regional, and national trends in under-5 mortality between 1990 and 2019 with scenario-based projections until 2030: a systematic analysis by the un inter-agency group for child mortality estimation. Lancet Glob Health. (2022) 10(2):e195–206. doi: 10.1016/s2214-109x(21)00515-5
2. United Nations. Global Indicator Framework for the Sustainable Development Goals and Targets of the 2030 Agenda for Sustainable Development Geneva. United Nations: Council EaS (2018).
3. Kassebaum N, Kyu HH, Zoeckler L, Olsen HE, Thomas K, Pinho C, et al. Child and adolescent health from 1990–2015: findings from the global burden of diseases, injuries, and risk factors 2015 study. JAMA Pediatr. (2017) 171(6):573–92. doi: 10.1001/jamapediatrics.2017.0250
4. Reiner RC Jr., Olsen HE, Ikeda CT, Echko MM, Ballestreros KE, Manguerra H, et al. Diseases, injuries, and risk factors in child and adolescent health, 1990–2017: findings from the global burden of diseases, injuries, and risk factors 2017 study. JAMA Pediatr. (2019) 173(6):e190337. doi: 10.1001/jamapediatrics.2019.0337
5. Khemani RG, Smith L, Lopez-Fernandez YM, Kwok J, Morzov R, Klein MJ, et al. Paediatric acute respiratory distress syndrome incidence and epidemiology (PARDIE): an international, observational study. Lancet Respir Med. (2019) 7(2):115–28. doi: 10.1016/S2213-2600(18)30344-8
6. McAllister DA, Liu L, Shi T, Chu Y, Reed C, Burrows J, et al. Global, regional, and national estimates of pneumonia morbidity and mortality in children younger than 5 years between 2000 and 2015: a systematic analysis. Lancet Glob Health. (2019) 7(1):e47–57. doi: 10.1016/s2214-109x(18)30408-x
7. Tan B, Wong JJ, Sultana R, Koh J, Jit M, Mok YH, et al. Global case-fatality rates in pediatric severe sepsis and septic shock: a systematic review and meta-analysis. JAMA Pediatr. (2019) 173(4):352–62. doi: 10.1001/jamapediatrics.2018.4839
8. Schell CO, Khalid K, Wharton-Smith A, Oliwa J, Sawe HR, Roy N, et al. Essential emergency and critical care: a consensus among global clinical experts. BMJ Glob Health. (2021) 6(9):e006585. doi: 10.1136/bmjgh-2021-006585
9. Baker T. Pediatric emergency and critical care in low-income countries. Paediatr Anaesth. (2009) 19(1):23–7. doi: 10.1111/j.1460-9592.2008.02868.x
10. Agulnik A, Cárdenas A, Carrillo AK, Bulsara P, Garza M, Alfonso Carreras Y, et al. Clinical and organizational risk factors for mortality during deterioration events among pediatric oncology patients in Latin America: a multicenter prospective cohort. Cancer. (2021) 127(10):1668–78. doi: 10.1002/cncr.33411
11. Kruk ME, Pate M. The lancet global health commission on high quality health systems 1 year on: progress on a global imperative. Lancet Glob Health. (2020) 8(1):e30–e2. doi: 10.1016/s2214-109x(19)30485-1
12. Muttalib F, González-Dambrauskas S, Lee JH, Steere M, Agulnik A, Murthy S, et al. Pediatric emergency and critical care resources and infrastructure in resource-limited settings: a multicountry survey. Crit Care Med. (2021) 49(4):671–81. doi: 10.1097/ccm.0000000000004769
13. Tadesse L, Abdullah NH, Awadalla HMI, D'Amours S, Davies F, Kissoon N, et al. A global mandate to strengthen emergency, critical and operative care. Bull World Health Organ. (2023) 101(4):231-a. doi: 10.2471/blt.23.289916
14. World Health Organization. Integrated emergency, critical and operative care for universal health coverage and protection from health emergencies. In: Executive Board 152nd Session. Geneva: World Health Organization (2023). p. 1–6.
15. Global Burden of Disease Child Mortality Collaborators. Global, regional, national, and selected subnational levels of stillbirths, neonatal, infant, and under-5 mortality, 1980–2015: a systematic analysis for the global burden of disease study 2015. Lancet. (2016) 388(10053):1725–74. doi: 10.1016/S0140-6736(16)31575-6
16. United Nations Children’s Fund. Unicef Data Warehouse: United Nations (cited July 20, 2023). Available online at: https://data.unicef.org/dv_index/
17. World Health Organization. The Global Health Observatory: World Health Organization (cited July 20, 2023). Available online at: https://www.who.int/data/gho
18. You D, Hug L, Ejdemyr S, Idele P, Hogan D, Mathers C, et al. Global, regional, and national levels and trends in under-5 mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the un inter-agency group for child mortality estimation. Lancet. (2015) 386(10010):2275–86. doi: 10.1016/s0140-6736(15)00120-8
19. Shiffman J, Shawar YR. Strengthening accountability of the global health metrics enterprise. Lancet. (2020) 395(10234):1452–6. doi: 10.1016/S0140-6736(20)30416-5
20. Bohn JA, Kassaye BM, Record D, Chou BC, Kraft IL, Purdy JC, et al. Demographic and mortality analysis of hospitalized children at a referral hospital in Addis Ababa, Ethiopia. BMC Pediatr. (2016) 16(1):168. doi: 10.1186/s12887-016-0709-4
21. Duke T, Yano E, Hutchinson A, Hwaihwanje I, Aipit J, Tovilu M, et al. Large-Scale data reporting of paediatric morbidity and mortality in developing countries: it can be done. Arch Dis Child. (2016) 101:392–7. doi: 10.1136/archdischild-2015-309353
22. Garg P. Pediatric hospitalizations at two different setting community hospitals in north India: implications for regionalization of care. Indian J Pediatr. (2009) 76(7):711–6. doi: 10.1007/s12098-009-0119-9
23. Munn Z, Moola S, Lisy K, Riitano D, Tufanaru C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int J Evid Based Healthc. (2015) 13(3):147–53. doi: 10.1097/xeb.0000000000000054
24. Stevens GA, Alkema L, Black RE, Boerma JT, Collins GS, Ezzati M, et al. Guidelines for accurate and transparent health estimates reporting: the gather statement. Lancet. (2016) 388(10062):e19–23. doi: 10.1016/s0140-6736(16)30388-9
25. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the prisma statement. Open Med. (2009) 3(3):e123–30. doi: 10.1371/journal.pmed.1000097
26. Kortz TB, Nielsen KR, Mediratta RP, Reeves H, O'Brien NF, Lee JH, et al. The burden of critical illness in hospitalized children in low- and middle-income countries: protocol for a systematic review and meta-analysis. Front Pediatr. (2022) 10:756643. doi: 10.3389/fped.2022.756643
27. Global Burden of Disease Network. Global Burden of Disease Study 2017 (GBD 2017) Socio-Demographic Index (SDI) 1950–2017. Seattle, WA: Institute for Health Metrics and Evaluation. (updated 2018; cited August 3, 2021). Available online at: http://ghdx.healthdata.org/record/ihme-data/gbd-2017-socio-demographic-index-sdi-1950%E2%80%932017
28. Covidence systematic review software. Melbourne, Australia: Veritas Health Innovation (2019). Available at www.covidence.org
29. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42(2):377–81. doi: 10.1016/j.jbi.2008.08.010
30. Hayden JA, van der Windt DA, Cartwright JL, Côté P, Bombardier C. Assessing bias in studies of prognostic factors. Ann Intern Med. (2013) 158:280–6. doi: 10.7326/0003-4819-158-4-201302190-00009
31. Barendregt JJ, Doi SA, Lee YY, Norman RE, Vos T. Meta-analysis of prevalence. J Epidemiol Community Health. (2013) 67(11):974–8. doi: 10.1136/jech-2013-203104
32. Rücker G, Schwarzer G, Carpenter JR, Schumacher M. Undue reliance on I(2) in assessing heterogeneity may mislead. BMC Med Res Methodol. (2008) 8:79. doi: 10.1186/1471-2288-8-79
33. Institute for Health Metrics and Evaluation. Global Burden of Disease Results. Seattle, WA: Institute for Health Metrics and Evaluation, University of Washington. (cited March 27, 2023). Available online at: https://vizhub.healthdata.org/gbd-results/
34. Gathara D, Malla L, Ayieko P, Karuri S, Nyamai R, Irimu G, et al. Variation in and risk factors for paediatric inpatient all-cause mortality in a low income setting: data from an emerging clinical information network. BMC Pediatr. (2017) 17(1):99. doi: 10.1186/s12887-017-0850-8
35. Santhanam I, Pai M, Kasturi K, Radhamani MP. Mortality after admission in the pediatric emergency department: a prospective study from a referral children’s hospital in Southern India. Pediatr Crit Care Med. (2002) 3(4):358–63. doi: 10.1097/00130478-200210000-00006
36. Sylverken J, Robison JA, Osei-Akoto A, Nguah SB, Addo-Yobo E, Balch A, et al. Decreased mortality after establishing a pediatric emergency unit at an urban referral hospital in Ghana. Pediatr Emerg Care. (2021) 37(7):e391–e5. doi: 10.1097/pec.0000000000001865
37. Clark M, Spry E, Daoh K, Baion D, Skordis-Worrall J. Reductions in inpatient mortality following interventions to improve emergency hospital care in Freetown, Sierra Leone. PLoS One. (2012) 7(9):e41458. doi: 10.1371/journal.pone.0041458
38. Colvin JD, Zaniletti I, Fieldston ES, Gottlieb LM, Raphael JL, Hall M, et al. Socioeconomic status and in-hospital pediatric mortality. Pediatrics. (2013) 131(1):e182–90. doi: 10.1542/peds.2012-1215
39. Barwise-Munro R, Al-Mahtot M, Turner S. Mortality and other outcomes after paediatric hospital admission on the weekend compared to weekday. PLoS One. (2018) 13(5):e0197494. doi: 10.1371/journal.pone.0197494
40. Fink EL, Kochanek PM, Tasker RC, Beca J, Bell MJ, Clark RS, et al. International survey of critically ill children with acute neurologic insults: the prevalence of acute critical neurological disease in children: a global epidemiological assessment study. Pediatr Crit Care Med. (2017) 18(4):330–42. doi: 10.1097/pcc.0000000000001093
41. Global Burden of Disease, Disease, Injury, Incidence, Prevalence, Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392(10159):1789–858. doi: 10.1016/S0140-6736(18)32279-7
42. Gunda R, Chimbari MJ. Cost-Effectiveness analysis of malaria interventions using disability adjusted life years: a systematic review. Cost Eff Resour Alloc. (2017) 15:10. doi: 10.1186/s12962-017-0072-9
43. Puett C, Sadler K, Alderman H, Coates J, Fiedler JL, Myatt M. Cost-Effectiveness of the community-based management of severe acute malnutrition by community health workers in southern Bangladesh. Health Policy Plan. (2013) 28(4):386–99. doi: 10.1093/heapol/czs070
44. Jha P, Bangoura O, Ranson K. The cost-effectiveness of forty health interventions in Guinea. Health Policy Plan. (1998) 13(3):249–62. doi: 10.1093/heapol/13.3.249
45. Rajabi T, Schell SK, Agapova SE, Hassan A, Zalta M, Wegner DR, et al. Supplementary feeding of moderately wasted children in Sierra Leone reduces severe acute malnutrition and death when compared with nutrition counseling: a retrospective cohort study. J Nutr. (2022) 152(4):1149–58. doi: 10.1093/jn/nxab451
46. Ahmed MC, Heukelbach J, Weddih A, Filali-Maltouf A, Sidatt M, Makhalla K, et al. Reduction of hospitalizations with diarrhea among children aged 0–5 years in Nouakchott, Mauritania, following the Introduction of rotavirus vaccine. Vaccine. (2019) 37(11):1407–11. doi: 10.1016/j.vaccine.2019.01.078
47. Amare AT, Kebede ZT, Welch HD. Epidemiology of bacterial meningitis in children admitted to gondar university hospital in the post pneumococcal vaccine era. Pan Afr Med J. (2018) 31:193. doi: 10.11604/pamj.2018.31.193.10254
48. Berezin EN, Jarovsky D, Cardoso MRA, Mantese OC. Invasive pneumococcal disease among hospitalized children in Brazil before and after the introduction of a pneumococcal conjugate vaccine. Vaccine. (2020) 38(7):1740–5. doi: 10.1016/j.vaccine.2019.12.038
49. Kortz TB, Herzel B, Marseille E, Kahn JG. Bubble continuous positive airway pressure in the treatment of severe paediatric pneumonia in Malawi: a cost-effectiveness analysis. BMJ Open. (2017) 7(7):e015344. doi: 10.1136/bmjopen-2016-015344
50. Khan AM, Wright JE, Bhutta ZA. A half century of oral rehydration therapy in childhood gastroenteritis: toward increasing uptake and improving coverage. Dig Dis Sci. (2020) 65(2):355–60. doi: 10.1007/s10620-019-05921-y
51. Barochia AV, Cui X, Vitberg D, Suffredini AF, O'Grady NP, Banks SM, et al. Bundled care for septic shock: an analysis of clinical trials. Crit Care Med. (2010) 38(2):668–78. doi: 10.1097/CCM.0b013e3181cb0ddf
52. Paul R, Neuman MI, Monuteaux MC, Melendez E. Adherence to pals sepsis guidelines and hospital length of stay. Pediatrics. (2012) 130(2):e273–80. doi: 10.1542/peds.2012-0094
53. Evans IVR, Phillips GS, Alpern ER, Angus DC, Friedrich ME, Kissoon N, et al. Association between the New York sepsis care mandate and in-hospital mortality for pediatric sepsis. JAMA. (2018) 320(4):358–67. doi: 10.1001/jama.2018.9071
54. Rahman AE, Ameen S, Hossain AT, Perkins J, Jabeen S, Majid T, et al. Introducing pulse oximetry for outpatient management of childhood pneumonia: an implementation research adopting a district implementation model in selected rural facilities in Bangladesh. EClinicalMedicine. (2022) 50:101511. doi: 10.1016/j.eclinm.2022.101511
55. Kyu HH, Pinho C, Wagner JA, Brown JC, Bertozzi-Villa A, Charlson FJ, et al. Global and national burden of diseases and injuries among children and adolescents between 1990 and 2013: findings from the global burden of disease 2013 study. JAMA Pediatr. (2016) 170(3):267–87. doi: 10.1001/jamapediatrics.2015.4276
56. Peters DH, Garg A, Bloom G, Walker DG, Brieger WR, Rahman MH. Poverty and access to health care in developing countries. Ann N Y Acad Sci. (2008) 1136:161–71. doi: 10.1196/annals.1425.011
57. Mawji A, Li E, Chandna A, Kortz T, Akech S, Wiens MO, et al. Common data elements for predictors of pediatric sepsis: a framework to standardize data collection. PLoS One. (2021) 16(6):e0253051. doi: 10.1371/journal.pone.0253051
58. Illness CA, Network N. Childhood mortality during and after acute illness in Africa and South Asia: a prospective cohort study. Lancet Glob Health. (2022) 10(5):e673–e84. doi: 10.1016/S2214-109X(22)00118-8
Keywords: global health, resource-limited settings, low- and middle-income countries, hospital death, hospital admission, acute illness, critical illness
Citation: Kortz TB, Mediratta RP, Smith AM, Nielsen KR, Agulnik A, Gordon Rivera S, Reeves H, O’Brien NF, Lee JH, Abbas Q, Attebery JE, Bacha T, Bhutta EG, Biewen CJ, Camacho-Cruz J, Coronado Muñoz A, deAlmeida ML, Domeryo Owusu L, Fonseca Y, Hooli S, Wynkoop H, Leimanis-Laurens M, Nicholaus Mally D, McCarthy AM, Mutekanga A, Pineda C, Remy KE, Sanders SC, Tabor E, Teixeira Rodrigues A, Yuee Wang JQ, Kissoon N, Takwoingi Y, Wiens MO and Bhutta A (2024) Etiology of hospital mortality in children living in low- and middle-income countries: a systematic review and meta-analysis. Front. Pediatr. 12:1397232. doi: 10.3389/fped.2024.1397232
Received: 7 March 2024; Accepted: 20 May 2024;
Published: 7 June 2024.
Edited by:
Claudio Flauzino de Oliveira, Latin American Sepsis Institute, BrazilReviewed by:
Elizabeth M. Molyneux, University of Malawi, Malawi© 2024 Kortz, Mediratta, Smith, Nielsen, Agulnik, Gordon Rivera, Reeves, O’Brien, Lee, Abbas, Attebery, Bacha, Bhutta, Biewen, Camacho-Cruz, Coronado Muñoz, deAlmeida, Domeryo Owusu, Fonseca, Hooli, Wynkoop, Leimanis-Laurens, Nicholaus Mally, McCarthy, Mutekanga, Pineda, Remy, Sanders, Tabor, Teixeira Rodrigues, Yuee Wang, Kissoon, Takwoingi, Wiens and Bhutta. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Teresa B. Kortz, dGVyZXNhLmtvcnR6QHVjc2YuZWR1
†These authors have contributed equally to this work and share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.