 N. Blair
N. Blair P. Patil2
P. Patil2 D. Nguyen
D. Nguyen F. Iorember
F. Iorember
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pediatr. , 11 April 2024
Sec. Pediatric Nephrology
Volume 12 - 2024 | https://doi.org/10.3389/fped.2024.1379895
The predominant use of intravenous catheters as primary access type in the pediatric hemodialysis population is associated with an increased risk of catheter related blood stream infections. While strict adherence to catheter placement and long-term care guidelines have helped to decrease the incidence of these infections, blood stream infections remain an infection burden in pediatric patients with long term hemodialysis catheters. The formation of biofilms on the surfaces of these catheters has been shown to be a source of microbes causing blood stream infections. One of the strategies for preventing bacterial colonization, inhibiting microbial multiplication, and suppressing the seeding of these microbes from biofilms upon maturation, has been the use of antibiotic-based lock solutions in-between dialysis treatments. Although clinical guidelines for the use of antibiotic lock solutions are yet to be developed, available evidence suggests a beneficial role of antibiotic lock solutions in the management of catheter related blood stream infections. Additionally, a clear understanding of how biofilms are formed and their role in the pathogenesis of catheter related bloodstream infection will facilitate the development of solutions that can prevent biofilm formation and inhibit their multiplication, maturation and seeding into the bloodstream.
In the 2016 United States Renal Data System annual report (USRDS), 81.4% of incident pediatric kidney failure patients aged 0–21 years, needing renal replacement therapy, were initiated on hemodialysis through a central venous catheter (CVC) (1). This observation has been corroborated by the international pediatric hemodialysis network (IPHN) registry. Of the 404 pediatric patients entered into the registry from December 2012 through September 2017, 73% of them initiated hemodialysis through a CVC (2). Catheter related blood stream infections (CRBSI) are associated with CVC use and a significant cause of morbidity and mortality in hemodialysis patients (3–5). In its 2014 report, the National Healthcare Safety Network reported that most bloodstream infections (63.0%) and access-related bloodstream infections (69.8%) occurred in hemodialysis patients with a CVC (5). The cost of ambulatory care of CRBSI, and hospitalization of pediatric hemodialysis patients with CRBSI is substantial, ranging between $11,584–36,266 per patient, with higher costs in patients needing intensive care unit stay and CVC replacement (6, 7). Microbial colonization and biofilm formation on the surface of CVC occurs frequently in hemodialysis patients dialyzed through CVC, and has been identified as a source of the microorganisms causing CRBSI (8–11). Strategies to prevent CRBSI include sterile vascular access practices as recommended by the Centers for Disease Control (CDC), the use of sterile catheter locking solutions and more recently, anti-adhesive or bactericidal catheter surface modification (12–14). While arteriovenous fistulas and arteriovenous grafts have been shown to be associated with lower rates of access-related sepsis, improved patency rates, improved dialysis adequacy and overall lower morbidity and mortality compared to CVC, their placement is often hindered by age and small vessel size in the pediatric population (15, 16). In this narrative review article, we examine available evidence on biofilm characteristics and the benefits of antibiotic lock therapy (ALT) in the treatment and prevention of CRBSI in pediatric hemodialysis patients.
Multiple risk factors have been identified and implicated in the pathogenesis of blood stream infections in pediatric patients with indwelling CVC and hemodialysis catheters including non-sterile technics during catheter use, the presence of gastrointestinal disease and young age (5, 17). Gram positive organisms are the cause of catheter related blood stream infections in 25.8%–63% of cases, depending on the study, with Staph. aureus and Staph. epidermidis being the predominant organisms identified in these infections (2, 3, 14). In the largest international pediatric hemodialysis cohort, CRBSI occurred in 1.3/1,000 catheter-days, with 63% of pathogens identified as gram positive organisms, and 17% as culture negative (2). In the standardized care to improve outcomes in pediatric ESKD (SCOPE) collaborative study, gram positive organisms were identified in 49.7% of cases, and gram negative organisms in 27.5% (3). Although less common, fungal pathogens such as Candida albicans also cause these infections. The sources of these organisms include colonization at the catheter insertion site, contamination of the catheter hub and hematogenous seeding of organisms from catheter biofilms and other infected sites (18–21).
The biofilm is an organized and complex aggregate of microorganisms living within an extracellular polymeric matrix that they produce, from which bacterial seeding can occur (8, 9). The process of biofilm formation starts with the attachment of microorganisms to the surface of catheters, followed by multiplication of the microorganisms, maturation, and synthesis of a polymeric matrix. Upon maturation, the bacteria detach and disseminate into the blood stream, predisposing to systemic infection (Figure 1). In hemodialysis catheters, biofilms form on both extraluminal and intraluminal surfaces and are an important source of microorganisms in CRBSI (22–24). In an adult prospective observational study, Ramanathan and colleagues demonstrated the presence of bacterial growth on the inner and outer surfaces of cultured hemodialysis catheters in 62% bacteremic and 30% nonbacteremic patients. Bacteremic patients had thicker biofilms on all catheter surfaces, with the extraluminal segment outer surface biofilms being thicker, compared to the luminal surface (p < 0.001) (25). In another prospective study and using quantitative PCR (qPCR) targeting 16S rRNA, intraluminal bacterial colonization was detected in 60% of hemodialysis catheters (26). It is suggested that biofilm formation can occur in less than 3 days after catheter insertion (27) and promote the development of antibiotic resistance (28–30), leading to persistent or recurrent blood stream infections. Efforts to eradicate the biofilm have included the use of antibiotic lock solutions, first described by Messing et al. in 1988 in which the antibiotic lock technique was associated with shortening of the time to obtaining negative cultures and decreased length of hospital stay (31, 32).
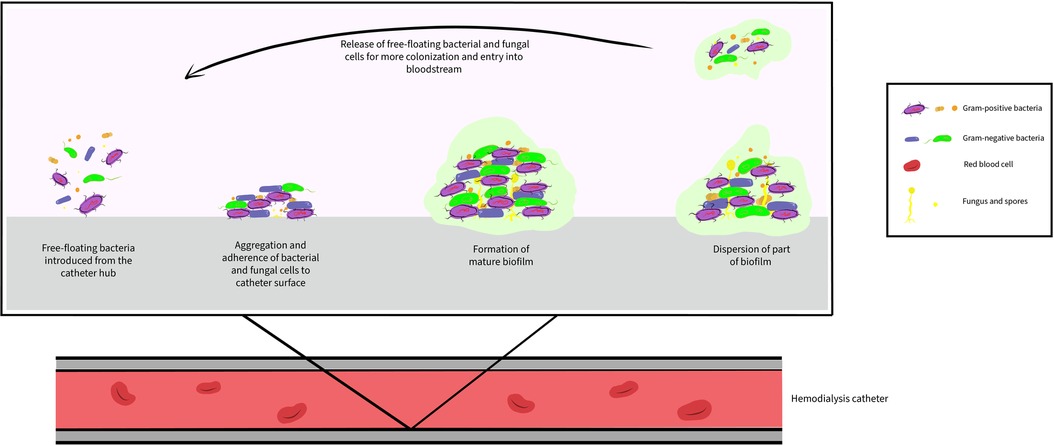
Figure 1. Biofilm formation on the intraluminal surface of hemodialysis catheter.
Current CRBSI treatment approaches include the use of systemic antibiotic therapy alone or in combination with antimicrobial catheter lock solutions, removal and subsequent replacement of catheters or catheter exchange over a guidewire (33–35). The use of systemic antibiotics alone may be insufficient to eradicate bacteremia and has been shown to be associated with higher recurrence rate of CRBSI (34, 36). After appropriate blood cultures have been drawn, current recommendations are to initiate broad antibiotic coverage with Vancomycin and a third-generation cephalosporin or an aminoglycoside, while culture and sensitivity results are being awaited. Cefazolin may be used in place of Vancomycin in dialysis units with low prevalence of methicillin-resistant staphylococcus. When a catheter-related infection is documented and a specific pathogen is identified, systemic antimicrobial therapy should be narrowed based on sensitivity results and consideration given for antibiotic lock therapy, if the catheter is not removed. Recommended treatment duration is 3 weeks for uncomplicated bacteremia and 6 weeks for patients with metastatic infection such as endocarditis and osteomyelitis (34, 37).
Strategies to reduce the risk of CRBSI in hemodialysis patients include decreasing the number of patients utilizing a hemodialysis catheter for chronic hemodialysis and the use of aseptic techniques during the connection and disconnection process of the hemodialysis procedure (38). More recently, the preemptive use of antibiotic lock therapy (ALT), a process of instilling high concentrations of an antimicrobial solution, typically along with an anticoagulant, to dwell in the catheter lumen when the CVC is not in use, has shown promise in helping decrease the rates of CRBSI (39–42). In a systematic review and meta-analysis of available randomized controlled trials that compared single or combination antimicrobial catheter lock solutions with non-antibiotic antimicrobial (antiseptic) solutions for the prevention of CRBSI in patients undergoing hemodialysis, antibiotic lock solutions were shown to significantly reduce the rate of CRBSI and catheter removal (43). In hemodialysis patients with established CRBSI, the adjunctive use of ALT was shown to be superior to systemic antibiotics alone in treatment of CRBSI (44). Data from Pediatric hemodialysis patients also shows that ALT is a viable option for attempting catheter salvage in CRBSI (45). The challenges with effective treatment of CRBSI in hemodialysis patients likely reflects the issues with achieving therapeutic antibiotic concentrations to successfully eliminate microbial biofilms on the surfaces of catheters (41, 46). Biofilms exhibit mechanisms which promote the survival of bacteria within the extracellular matrix including antibiotic efflux, reduced permeability to antibiotics, activities of enzymes that modify or destroy antibiotics, and modification of the antibiotic target through mutation, enzymatic action, or the presence of an alternate target (47). It is now understood that the bacteria within biofilms can withstand high concentrations of antibiotics and resist killing even when they are susceptible to the antimicrobial agents in vitro, making bacterial eradication challenging in clinical settings, and putting the patient at risk for recurrent CRBSI. High concentrations of antimicrobial solutions are an effort to address biofilm resistance and tolerance (47, 48). To improve the penetration and successful killing of biofilm bacteria, antibiotics must be at 100–1000 times the typical concentration (49, 50). Attempting to salvage an infected catheter with systemic therapy alone may not be enough and may increase the risk of complications such as endocarditis and epidural abscess, thus, the recommendation to fill catheter lumens with supratherapeutic antimicrobial concentrations and allow to dwell for hours to days, also known as antibiotic locks (51–56). Antibiotics are often mixed with heparin to help maintain lumen patency while the solution dwells. The mixture compatibility and stability are important factors in determining efficacy of antibiotic lock solutions (37, 45, 52, 57–60, 61, 62, 63). The ultimate choice of ALT depends on the microorganisms recovered on blood culture and their sensitivies to antibiotics. Commonly used antibiotic solutions and their characteristics can be found in Table 1.
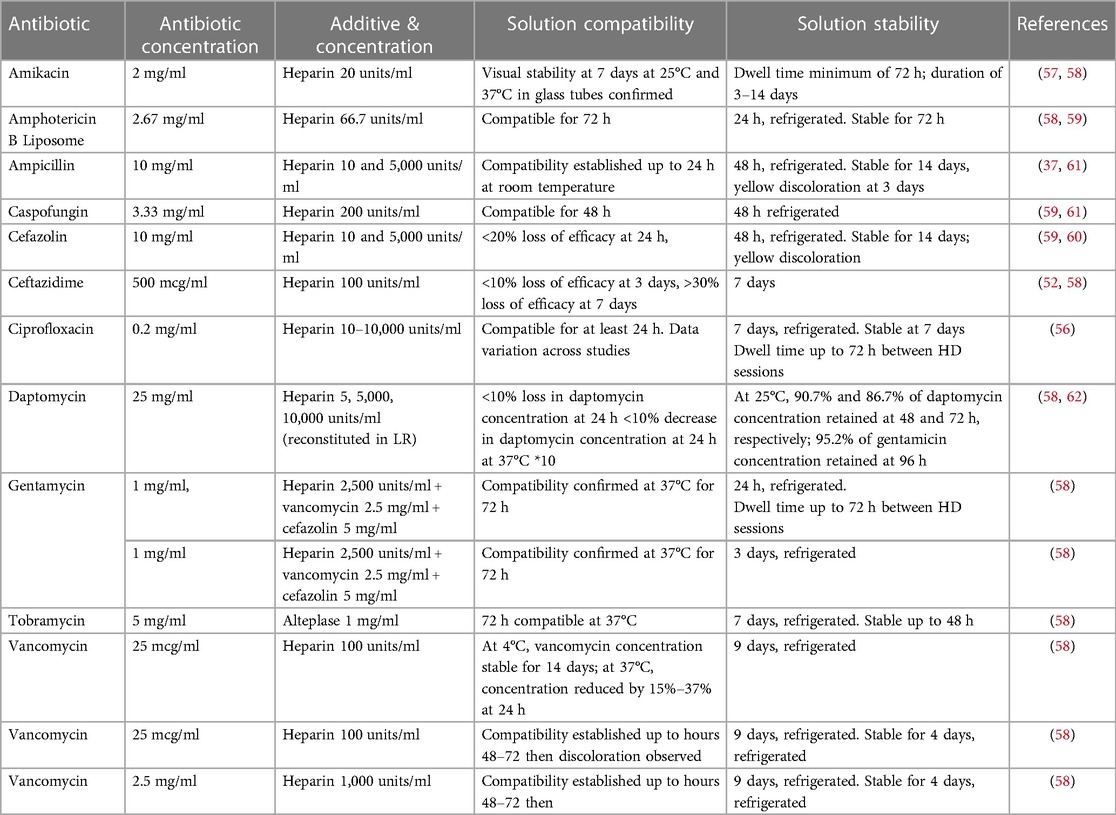
Table 1. Antibiotic lock solution characteristics.
Biofilms are difficult to eradicate and their successful clearance requires an understanding of their survival strategies and the use of high concentrations of antimicrobials over a sustained duration of time to allow deep penetration of the biofilm matrix (29, 64). The high concentration of antibiotics is necessary for inhibition of bacterial growth and eradication of the biofilm. These solutions could be used not only as adjunct therapy for CRBSI but also for the prevention of biofilm formation. The pre-emptive use of ALT in adult hemodialysis patients has been shown to lead to fewer CRBSI rate and prolonged catheter patency in some randomized controlled studies (40, 65). In their randomized prospective study, Al-Hweish et al. compared infection rates in one group with pre-emptive ALT with Vancomycin-gentamicin-heparin based solution and a second group with routine hemodialysis catheter lock therapy. The incidence of bacteremia and sepsis was significantly lower in the ALT group compared to the routine hemodialysis catheter care group (40). In a similar study, Saxena et al. demonstrated an infection-free and thrombosis-free survival advantage in catheters pre-emptively locked with Cefotaxime-heparin solutions, compared to heparin alone (65). In the largest study to date, comparing the effectiveness of prophylactic antibiotic lock therapy on clinical outcomes in 555 hemodialysis patients, the group whose catheters were locked with a gentamicin/citrate containing solution had significantly less CRBSI rates compared to heparin alone (66). As a result of the heterogeneity of patient population, study quality and design, the most recent Centers for Disease Control (CDC) guidelines do not recommend the routine use of ALT for prevention of CRBSI in long term CVC (67). However, more recent publications provide compelling evidence to the benefit of ALT in the prevention of CRBSI. Moreover, recent large systematic review and meta-analysis of randomized controlled trials have shown ALT to be safe and efficacious in reducing the rates of CRBSI in adult and pediatric patients with CVC (68, 69). These and similar findings are likely to lead to a revision of future guidelines to support routine use of ALT on patients with long term CVCs. In patients with established CRBSI, Khosroshahi et al. demonstrated a significant difference in the success rate of clearing catheter infection in hemodialysis patients with use of 60% ethanol-lock (antiseptic solution) along with systemic antibiotic therapy, and suggested this for routine use (70). A recent meta-analysis of pediatric data showed the addition of ALT to be superior to systemic antibiotics alone for the management of CRBSI and was also associated with less recurrence when compared to patients who were treated with systemic antibiotics alone (35). Although these were mostly oncology patients, the biofilm formation process is likely similar in all patient populations with implantable devices, including CVCs. In the pediatric hemodialysis population, the use of ALT has been shown to be a viable option for reducing systemic antibiotic exposure and antibiotic resistance (71). Although there have been concerns about the emergence of antimicrobial resistance from routine use of ALT in long term CVC, available data suggests the risk to be low (43). Factors that determine the choice of ALT include empiric therapy, culture and sensitivity results, how often the catheter is accessed, stability of the ALT solution, ALT volume variation and inconsistent practices for the documentation of size and length of the catheters, which might lead to subtherapeutic or supratherapeutic dosing. Adverse events associated with the use of ALT are uncommon and are largely related to the individual antimicrobial components of the solutions and could be avoided if solutions are adequately aspirated when accessing the catheters. Although clear guidelines on the role of ALT in the prevention and treatment of CRBSI are currently lacking, available evidence is promising, and future well designed multicenter studies might provide more evidence on the clinical utility of ALT. A list of antibiotic lock formulations and their antibiotic-biofilm interactions can be found in Table 2.
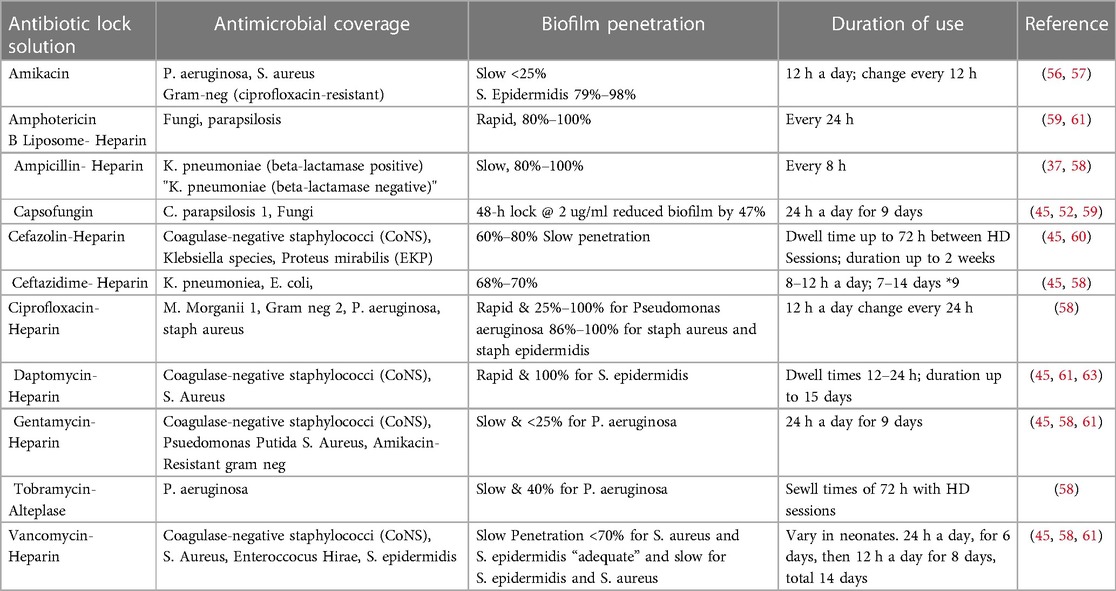
Table 2. Antibiotic lock solution-biofilm interaction.
In patients with confirmed CRBSI, antibiotic lock therapy should be initiated concomitantly with appropriate systemic antibiotic therapy. Lock therapies should be individualized based on identified organisms and their susceptibilities. If cultures confirm methicillin-resistant S. aureus infection, early catheter removal and replacement is recommended. This is the current practice at our center. Catheter salvage and ALT should be pursued only if central venous access is problematic in the patient. Infections with methicillin-susceptible S. aureus can be treated with cefazolin lock therapy and if patients remain febrile and continue to have bacteremia 72 h into therapy, the catheter should be replaced. In fungal blood stream infections, infected catheters should always be removed (37). Antibiotic lock solutions should dwell up to 48 h, depending on frequency of catheter use. The catheter should be filled with the volume of antimicrobial solution that fills the entire length of the catheter lumen and this varies depending on the length/ type of catheter and lumen size. The recommended volume is often provided by the manufacturer of the catheter. While the lock solutions dwell in the catheter lumen, the catheter cannot be used until it is aspirated or flushed. The authors recommend aspiration of the instilled volume and avoid flushing of the solution into the patient, to prevent adverse effects. Treatment duration should follow guidelines for systemic antibiotic duration– 3 weeks for uncomplicated bacteremia and 6 weeks for metastatic infection (34, 37). Given the favorable role of ALT in the treatment of CRBSI, the design of clinical pathways and creation of standardized and/or institution specific roadmaps and protocols would be helpful in promoting a wider usage in routine clinical practice.
The clinical burden of CRBSI in pediatric patients with kidney failure dialyzed through a catheter necessitates the development of strategies for the prevention and eradication of biofilms on the surfaces of hemodialysis catheters is paramount. Biofilm formation involves a complex development process and is a survival strategy for pathologic microorganisms. ALT holds promise as a biofilm preventative and eradication tool for clinicians, and although the role of ALT in the management of CRBSI is yet to be clearly defined, available evidence shows clinical advantage in the treatment of these infections. Furthermore, the ability to salvage catheters and avoid catheter removal is of benefit to patients with limited access. Future research must focus on identifying the most effective solutions for preventing catheter colonization and biofilm formation, predicting biofilm susceptibility, and overcoming biofilm resistance. Standardization of practices will be helpful in the design of studies and the development of ALT protocols for use in the pediatric HD population. Adequately randomized studies comparing ALTs with placebo and/or non-antimicrobial solutions, looking at various outcomes such as number of hospitalizations for CRBSI, loss of productive days, care giver time, quality of life and other patient reported outcomes could help justify need for routine ALT therapies.
NB: Writing – original draft. PP: Writing – review & editing, Writing – original draft. DN: Writing – original draft. BP-N: Writing – original draft. FI: Writing – review & editing, Writing – original draft, Supervision, Conceptualization.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Saran R, Robinson B, Abbott KC, Agodoa LYC, Albertus P, Ayanian J, et al. US renal data system 2016 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis. (2017) 69(3 Suppl 1):A7–8. doi: 10.1053/j.ajkd.2016.12.004
2. Borzych-Duzalka D, Shroff R, Ariceta G, Yap Y-C, Paglialonga F, Xu H, et al. Vascular access choice, complications, and outcomes in children on maintenance hemodialysis: findings from the international pediatric hemodialysis network (IPHN) registry. Am J Kidney Dis. (2019) 74(2):193–202. doi: 10.1053/j.ajkd.2019.02.014
3. Ruebner RL, de Souza HG, Richardson T, Bedri B, Marsenic O, Iorember F, et al. Epidemiology and risk factors for hemodialysis access-associated infections in children: a prospective cohort study from the SCOPE collaborative. Am J Kidney Dis. (2022) 80(2):186–195.e1. doi: 10.1053/j.ajkd.2021.11.008
4. Kumbar L, Yee J. Current concepts in hemodialysis vascular access infections. Adv Chronic Kidney Dis. (2019) 26(1):16–22. doi: 10.1053/j.ackd.2018.10.005
5. Nguyen DB, Shugart A, Lines C, Shah AB, Edwards J, Pollock D, et al. National healthcare safety network (NHSN) dialysis event surveillance report for 2014. Clin J Am Soc Nephrol. (2017) 12(7):1139–46. doi: 10.2215/CJN.11411116
6. Wasik HL, Neu A, Warady B, Crawford B, Richardson T, De Souza HG, et al. The cost of hospitalizations for treatment of hemodialysis catheter-associated blood stream infections in children: a retrospective cohort study. Pediatr Nephrol. (2023) 38(6):1915–23. doi: 10.1007/s00467-022-05764-2
7. Rinke ML, Oyeku SO, Ford WJH, Heo M, Saiman L, DeLaMora P, et al. Costs of ambulatory pediatric healthcare-associated infections: central-line-associated bloodstream infection (CLABSIs), catheter-associated urinary tract infection (CAUTIs), and surgical site infections (SSIs). Infect Control Hosp Epidemiol. (2020) 41(11):1292–7. doi: 10.1017/ice.2020.305
8. Jamal M, Ahmad W, Andleeb S, Jalil F, Imran M, Nawaz MA, et al. Bacterial biofilm and associated infections. J Chin Med Assoc. (2018) 81(1):7–11. doi: 10.1016/j.jcma.2017.07.012
9. Wolcott R. Biofilm and catheter-related bloodstream infections. Br J Nurs. (2021) 30(8):S4–9. doi: 10.12968/bjon.2021.30.8.S4
10. Gupta V, Yassin MH. Infection and hemodialysis access: an updated review. Infect Disord Drug Targets. (2013) 13(3):196–205. doi: 10.2174/1871526511313030008
11. Passerini L, Lam K, Costerton JW, King EG. Biofilms on indwelling vascular catheters. Crit Care Med. (1992) 20(5):665–73. doi: 10.1097/00003246-199205000-00020
12. Golestaneh L, Mokrzycki MH. Prevention of hemodialysis catheter infections: ointments, dressings, locks, and catheter hub devices. Hemodial Int. (2018) 22(S2):S75–82. doi: 10.1111/hdi.12703
13. Balikci E, Yilmaz B, Tahmasebifar A, Baran ET, Kara E. Surface modification strategies for hemodialysis catheters to prevent catheter-related infections: a review. J Biomed Mater Res B Appl Biomater. (2021) 109(3):314–27. doi: 10.1002/jbm.b.34701
14. Marsenic O, Rodean J, Richardson T, Swartz S, Claes D, Day JC, et al. Tunneled hemodialysis catheter care practices and blood stream infection rate in children: results from the SCOPE collaborative. Pediatr Nephrol. (2020) 35(1):135–43. doi: 10.1007/s00467-019-04384-7
15. Stefanidis CJ. Prevention of catheter-related bacteremia in children on hemodialysis: time for action. Pediatr Nephrol. (2009) 24(11):2087–95. doi: 10.1007/s00467-009-1254-2
16. Shroff R, Calder F, Bakkaloğlu S, Nagler EV, Stuart S, Stronach L, et al. Vascular access in children requiring maintenance haemodialysis: a consensus document by the European society for paediatric nephrology dialysis working group. Nephrol Dial Transplant. (2019) 34(10):1746–65. doi: 10.1093/ndt/gfz011
17. Paioni P, Kuhn S, Strässle Y, Seifert B, Berger C. Risk factors for central line-associated bloodstream infections in children with tunneled central venous catheters. Am J Infect Control. (2020) 48(1):33–9. doi: 10.1016/j.ajic.2019.06.027
18. Mermel LA. What is the predominant source of intravascular catheter infections? Clin Infect Dis. (2011) 52(2):211–2. doi: 10.1093/cid/ciq108
19. Katneni R, Hedayati SS. Central venous catheter-related bacteremia in chronic hemodialysis patients: epidemiology and evidence-based management. Nat Clin Pract Nephrol. (2007) 3(5):256–66. doi: 10.1038/ncpneph0447
20. Mermel LA. What is the evidence for intraluminal colonization of hemodialysis catheters? Kidney Int. (2014) 86(1):28–33. doi: 10.1038/ki.2013.527
21. Pascual A. Pathogenesis of catheter-related infections: lessons for new designs. Clin Microbiol Infect. (2002) 8(5):256–64. doi: 10.1046/j.1469-0691.2002.00418.x
22. Dasgupta MK. Biofilms and infection in dialysis patients. Semin Dial. (2002) 15(5):338–46. doi: 10.1046/j.1525-139X.2002.00084.x
23. Cangui-Panchi SP, Ñacato-Toapanta AL, Enríquez-Martínez LJ, Reyes J, Garzon-Chavez D, Machado A. Biofilm-forming microorganisms causing hospital-acquired infections from intravenous catheter: a systematic review. Curr Res Microb Sci. (2022) 3:100175. doi: 10.1016/j.crmicr.2022.100175
24. Almenara-Tejederas M, Rodríguez-Pérez MA, Moyano-Franco MJ, de Cueto-López M, Rodríguez-Baño J, Salgueira-Lazo M. Tunneled catheter-related bacteremia in hemodialysis patients: incidence, risk factors and outcomes. A 14-year observational study. J Nephrol. (2023) 36(1):203–12. doi: 10.1007/s40620-022-01408-8
25. Ramanathan V, Riosa S, Al-Sharif AH, Mansouri MD, Tranchina A, Kayyal T, et al. Characteristics of biofilm on tunneled cuffed hemodialysis catheters in the presence and absence of clinical infection. Am J Kidney Dis. (2012) 60(6):976–82. doi: 10.1053/j.ajkd.2012.06.003
26. Onder AM, Cuff CF, Liang X, Billings AA, Onder S, Yu JJ, et al. Detecting the prevalence of bacterial colonization on tunneled cuffed hemodialysis catheters using quantitative PCR targeting 16S rRNA and scanning electron microscopy. J Vasc Access. (2022) 23(5):743–53. doi: 10.1177/11297298211009016
27. Anaissie E, Samonis G, Kontoyiannis D, Costerton J, Sabharwal U, Bodey G, et al. Role of catheter colonization and infrequent hematogenous seeding in catheter-related infections. Eur J Clin Microbiol Infect Dis. (1995) 14(2):134–7. doi: 10.1007/BF02111873
28. Bowler P, Murphy C, Wolcott R. Biofilm exacerbates antibiotic resistance: is this a current oversight in antimicrobial stewardship? Antimicrob Resist Infect Control. (2020) 9(1):162. doi: 10.1186/s13756-020-00830-6
29. Donlan RM. Biofilm elimination on intravascular catheters: important considerations for the infectious disease practitioner. Clin Infect Dis. (2011) 52(8):1038–45. doi: 10.1093/cid/cir077
30. Marcus RJ, Post JC, Stoodley P, Hall-Stoodley L, McGill RL, Sureshkumar KK, et al. Biofilms in nephrology. Expert Opin Biol Ther. (2008) 8(8):1159–66. doi: 10.1517/14712598.8.8.1159
31. Messing B, Peitra-Cohen S, Debure A, Beliah M, Bernier JJ. Antibiotic-lock technique: a new approach to optimal therapy for catheter-related sepsis in home-parenteral nutrition patients. JPEN J Parenter Enteral Nutr. (1988) 12(2):185–9. doi: 10.1177/0148607188012002185
32. Messing B, Man F, Colimon R, Thuillier F, Beliah M. Antibiotic-lock technique is an effective treatment of bacterial catheter-related sepsis during parenteral nutrition. Clin Nutr. (1990) 9(4):220–5. doi: 10.1016/0261-5614(90)90023-L
33. Almeida BM, Moreno DH, Vasconcelos V, Cacione DG. Interventions for treating catheter-related bloodstream infections in people receiving maintenance haemodialysis. Cochrane Database Syst Rev. (2022) 4(4):CD013554. doi: 10.1002/14651858.CD013554.pub2
34. Allon M. Treatment guidelines for dialysis catheter–related bacteremia: an update. Am J Kidney Dis. (2009) 54(1):13–7. doi: 10.1053/j.ajkd.2009.04.006
35. Buonsenso D, Salerno G, Sodero G, Mariani F, Pisapia L, Gelormini C, et al. Catheter salvage strategies in children with central venous catheter-related or -associated bloodstream infections: a systematic review and meta-analysis. J Hosp Infect. (2022) 125:1–20. doi: 10.1016/j.jhin.2022.03.010
36. Marr KA, Sexton DJ, Conlon PJ, Corey GR, Schwab SJ, Kirkland KB. Catheter-related bacteremia and outcome of attempted catheter salvage in patients undergoing hemodialysis. Ann Intern Med. (1997) 127(4):275–80. doi: 10.7326/0003-4819-127-4-199708150-00003
37. Mermel LA, Allon M, Bouza E, Craven DE, Flynn P, O'Grady NP, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 update by the Infectious Diseases Society of America. Clin Infect Dis. (2009) 49(1):1–45. doi: 10.1086/599376
38. Fisher M, Golestaneh L, Allon M, Abreo K, Mokrzycki MH. Prevention of bloodstream infections in patients undergoing hemodialysis. Clin J Am Soc Nephrol. (2019) 15(1):132–51. doi: 10.2215/CJN.06820619
39. Blanco-Di Matteo A, Garcia-Fernandez N, Aguinaga Pérez A, Carmona-Torre F, Oteiza AC, Leiva J, et al. Pre-emptive antimicrobial locks decrease long-term catheter-related bloodstream infections in hemodialysis patients. Antibiotics (Basel). (2022) 11(12):1692. doi: 10.3390/antibiotics11121692
40. Al-Hwiesh AK, Abdul-Rahman IS. Successful prevention of tunneled, central catheter infection by antibiotic lock therapy using vancomycin and gentamycin. Saudi J Kidney Dis Transpl. (2007) 18(2):239–47. 17496402
41. Arechabala MC, Catoni MI, Claro JC, Rojas NP, Rubio ME, Calvo MA, et al. Antimicrobial lock solutions for preventing catheter-related infections in haemodialysis. Cochrane Database Syst Rev. (2018) 4(4). doi: 10.1002/14651858.CD010597.pub2
42. Mortazavi M, Alsaeidi S, Sobhani R, Salimi F, Atapour A, Sharif N, et al. Successful prevention of tunneled, central catheter infection by antibiotic lock therapy using cefotaxime. J Res Med Sci. (2011) 16(3):303–9. 22091249; PMCID: PMC3214338
43. Yahav D, Rozen-Zvi B, Gafter-Gvili A, Leibovici L, Gafter U, Paul M. Antimicrobial lock solutions for the prevention of infections associated with intravascular catheters in patients undergoing hemodialysis: systematic review and meta-analysis of randomized, controlled trials. Clin Infect Dis. (2008) 47(1):83–93. doi: 10.1086/588667
44. Aslam S, Vaida F, Ritter M, Mehta RL. Systematic review and meta-analysis on management of hemodialysis catheter-related bacteremia. J Am Soc Nephrol. (2014) 25(12):2927–41. doi: 10.1681/ASN.2013091009
45. Signorino C, Fusco E, Galli L, Chiappini E. Effectiveness of antimicrobial lock therapy for the treatment of catheter-related and central-line-associated bloodstream infections in children: a single center retrospective study. Antibiotics (Basel). (2023) 12(5):800. doi: 10.3390/antibiotics12050800
46. Andris DA, Krzywda EA, Edmiston CE, Krepel CJ, Gohr CM. Elimination of intraluminal colonization by antibiotic lock in silicone vascular catheters. Nutrition. (1998) 14(5):427–32. doi: 10.1016/S0899-9007(98)00013-6
47. Lebeaux D, Ghigo J-M, Beloin C. Biofilm-related infections: bridging the gap between clinical management and fundamental aspects of recalcitrance toward antibiotics. Microbiol Mol Biol Rev. (2014) 78(3):510–43. doi: 10.1128/MMBR.00013-14
48. Anderl JN, Franklin MJ, Stewart PS. Role of antibiotic penetration limitation in Klebsiella pneumoniae biofilm resistance to ampicillin and ciprofloxacin. Antimicrob Agents Chemother. (2000) 44(7):1818–24. doi: 10.1128/AAC.44.7.1818-1824.2000
49. Sedlacek MJ, Walker C. Antibiotic resistance in an in vitro subgingival biofilm model. Oral Microbiol Immunol. (2007) 22(5):333–9. doi: 10.1111/j.1399-302X.2007.00366.x
50. Macià MD, Rojo-Molinero E, Oliver A. Antimicrobial susceptibility testing in biofilm-growing bacteria. Clin Microbiol Infect. (2014) 20(10):981–90. doi: 10.1111/1469-0691.12651
51. Campos RP, do Nascimento MM, Chula DC, Riella MC. Minocycline-EDTA lock solution prevents catheter-related bacteremia in hemodialysis. J Am Soc Nephrol. (2011) 22(10):1939–45. doi: 10.1681/ASN.2010121306
52. Anthony TU, Rubin LG. Stability of antibiotics used for antibiotic-lock treatment of infections of implantable venous devices (ports). Antimicrob Agents Chemother. (1999) 43(8):2074–6. doi: 10.1128/AAC.43.8.2074
53. Members of the Sous les Verrous Study Group. Antibiotic lock therapy for the conservative treatment of long-term intravenous catheter-related infections in adults and children: when and how to proceed? Guidelines for clinical practice 2020. Infect Dis now. (2021) 51(3):236–46. doi: 10.1016/j.idnow.2021.02.004
54. Krishnasami Z, Carlton D, Bimbo L, Taylor ME, Balkovetz DF, Barker J, et al. Management of hemodialysis catheter-related bacteremia with an adjunctive antibiotic lock solution. Kidney Int. (2002) 61(3):1136–42. doi: 10.1046/j.1523-1755.2002.00201.x
55. McIntyre CW, Hulme LJ, Taal M, Fluck RJ. Locking of tunneled hemodialysis catheters with gentamicin and heparin. Kidney Int. (2004) 66(2):801–5. doi: 10.1111/j.1523-1755.2004.00806.x
56. Haddadin Y, Annamaraju P, Regunath H. Central Line–Associated Blood Stream Infections. Treasure Island, FL: StatPearls (2023).
57. Fernandez-Hidalgo N, Almirante B, Calleja R, Ruiz I, Planes AM, Rodriguez D, et al. Antibiotic-lock therapy for long-term intravascular catheter-related bacteraemia: results of an open, non-comparative study. J Antimicrob Chemother. (2006) 57(6):1172–80. doi: 10.1093/jac/dkl103
58. Justo JA, Bookstaver PB. Antibiotic lock therapy: review of technique and logistical challenges. Infect Drug Resist. (2014) 7:343–63. doi: 10.2147/IDR.S51388
59. Imbert C, Rammaert B. What could be the role of antifungal lock-solutions? From bench to bedside. Pathogens. (2018) 7(1):6. doi: 10.3390/pathogens7010006
60. Silva TNV, Mendes ML, Abrão JMG, Caramori JT, Ponce D. Successful prevention of tunneled central catheter infection by antibiotic lock therapy using cefazolin and gentamicin. Int Urol Nephrol. (2013) 45(5):1405–13. doi: 10.1007/s11255-012-0339-1
61. Vassallo M, Dunais B, Roger P-M. Antimicrobial lock therapy in central-line associated bloodstream infections: a systematic review. Infection. (2015) 43(4):389–98. doi: 10.1007/s15010-015-0738-1
62. Yen H-W, Yang W-C, Tarng D-C, Yang C-Y, Chuang C-L, Huang L-J, et al. Daptomycin antibiotic lock therapy for hemodialysis patients with gram-positive bloodstream infections following use of tunneled, cuffed hemodialysis catheters: retrospective single center analysis. Hemodial Int. (2016) 20(2):315–20. doi: 10.1111/hdi.12378
63. Stewart PS, Davison WM, Steenbergen JN. Daptomycin rapidly penetrates a Staphylococcus epidermidis biofilm. Antimicrob Agents Chemother. (2009) 53(8):3505–7. doi: 10.1128/AAC.01728-08
64. Sharma D, Misba L, Khan AU. Antibiotics versus biofilm: an emerging battleground in microbial communities. Antimicrob Resist Infect Control. (2019) 8:76. doi: 10.1186/s13756-019-0533-3
65. Saxena AK, Panhotra BR, Sundaram DS, Morsy MNF, Al-Ghamdi AMA-A. Enhancing the survival of tunneled haemodialysis catheters using an antibiotic lock in the elderly: a randomised, double-blind clinical trial. Nephrology (Carlton). (2006) 11(4):299–305. doi: 10.1111/j.1440-1797.2006.00563.x
66. Moore CL, Besarab A, Ajluni M, Soi V, Peterson EL, Johnson LE, et al. Comparative effectiveness of two catheter locking solutions to reduce catheter-related bloodstream infection in hemodialysis patients. Clin J Am Soc Nephrol. (2014) 9(7):1232–9. doi: 10.2215/CJN.11291113
67. O'Grady NP, Alexander M, Burns LA, Dellinger EP, Garland J, Heard SO, et al. Guidelines for the prevention of intravascular catheter-related infections. Clin Infect Dis. (2011) 52(9):e162–93. doi: 10.1093/cid/cir257
68. Zacharioudakis IM, Zervou FN, Arvanitis M, Ziakas PD, Mermel LA, Mylonakis E. Antimicrobial lock solutions as a method to prevent central line-associated bloodstream infections: a meta-analysis of randomized controlled trials. Clin Infect Dis. (2014) 59(12):1741–9. doi: 10.1093/cid/ciu671
69. Sheng KX, Zhang P, Li JW, Cheng J, He YC, Böhlke M, et al. Comparative efficacy and safety of lock solutions for the prevention of catheter-related complications including infectious and bleeding events in adult haemodialysis patients: a systematic review and network meta-analysis. Clin Microbiol Infect. (2020) 26(5):545–52. doi: 10.1016/j.cmi.2019.12.003
70. Khosroshahi HT, Mahdipur H, Parkhideh S, Basmenji S, Khalilzadeh M, Tozihi M. The effectiveness of systemic antibiotic therapy with and without ethanol-locked solution in the treatment of hemodialysis-related catheter infection. Saudi J Kidney Dis Transpl. (2015) 26(3):477–81. doi: 10.4103/1319-2442.157315
71. Onder AM, Billings AA, Chandar J, Nield L, Francoeur D, Simon N, et al. Antibiotic lock solutions allow less systemic antibiotic exposure and less catheter malfunction without adversely affecting antimicrobial resistance patterns. Hemodial Int. (2013) 17(1):75–85. doi: 10.1111/j.1542-4758.2012.00717.x
Keywords: catheter related blood stream infections, antibiotic lock solutions, hemodialysis, antibiotic lock therapy, biofilm, hemodialysis catheter colonization
Citation: Blair N, Patil P, Nguyen D, Paudyal-Nepal B and Iorember F (2024) Antibiotic lock solutions as adjunct therapy for catheter-related blood stream infections in pediatric hemodialysis patients. Front. Pediatr. 12:1379895. doi: 10.3389/fped.2024.1379895
Received: 31 January 2024; Accepted: 2 April 2024;
Published: 11 April 2024.
Edited by:
Constantinos J. Stefanidis, "Mitera" Children’s Hospital, GreeceReviewed by:
Evelien Snauwaert, Ghent University Hospital, Belgium© 2024 Blair, Patil, Nguyen, Paudyal-Nepal and Iorember. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: F. Iorember ZnJhbmNhLmlvcmVtYmVyQGRjaHN0eC5vcmc=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.