
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Pediatr., 25 March 2024
Sec. Pediatric Cardiology
Volume 12 - 2024 | https://doi.org/10.3389/fped.2024.1376360
 Michaela Höck1*
Michaela Höck1* Anna Posod1
Anna Posod1 Irena Odri Komazec2
Irena Odri Komazec2 Elke Griesmaier1Elisabeth Ralser1Ulrike Pupp-Peglow1
Elke Griesmaier1Elisabeth Ralser1Ulrike Pupp-Peglow1 Ursula Kiechl-Kohlendorfer1
Ursula Kiechl-Kohlendorfer1
Introduction: Due to improvements in perinatal care, survival rates of preterm infants have improved during the last decades. However, these infants remain at risk of developing cardiovascular sequelae later in life. This study aimed to investigate the cardiac biomarkers and left ventricular systolic function in former preterm infants in comparison with term controls at preschool age.
Methods: The study included children aged 5–7 years old born below 32 weeks of gestational age. The control group consisted of same-age children born at term. Basic data of study participants were collected using questionnaires and follow-up databases. During the study visit, we recorded anthropometric data and blood pressure readings, determined high-sensitive cardiac troponin T (hs-cTnT) and N-terminal pro-B-type natriuretic peptide (NT-pro-BNP) concentrations, and calculated fractional shortening (FS) and left ventricular mass (LVM).
Results: Term-born (n = 25; median gestational age, 40.1 weeks) compared with preterm-born infants (n = 80; median gestational age 29.6 weeks) showed no significant differences in the median concentration of hs-cTnT [median, 3.5 (IQR 3.5; 3.5) vs. 3.5 (3.5; 3.5) ng/L, p = 0.328] and the median concentration of NT-pro-BNP [median, 91.0 (IQR 40.8; 150.3) vs. 87.5 (50.1; 189.5) ng/L, p = 0.087]. FS and LVM/LVMI were not significantly different between the two groups.
Conclusion: At preschool age, we observed no significant differences in cardiac biomarkers and left ventricular systolic function in preterm infants. Further studies are warranted to explore the potential of cardiac biomarkers as a prognostic tool for subclinical cardiac alterations after preterm birth.
Advances in neonatal care have led to an increased survival rate for preterm infants over the past decades (1). However, prematurity and low birth weight are associated with an unfavorable cardiovascular risk profile, not only in the neonatal period but also at preschool age, adolescence, and adult life (2, 3). The major determinants of cardiovascular disease are increased blood pressure, hyperglycemia, lipid alterations, and overweight/obesity, which particularly occurs after premature birth (4). Another risk factor for cardiovascular disease is altered myocardial remodeling and accelerated cardiovascular aging, which is associated with preterm birth (5). With regard to diagnosis, prognosis, and monitoring of cardiac distress, there is a strong evidence for cardiac biomarkers that provide a view into the structure and functioning of the heart (6). The most used cardiac biomarkers are troponins and natriuretic peptides. Marked elevations in cardiac troponin are sensitive biomarkers of functional and structural damage in the cardiovascular system, while a slightly increased high-sensitive cardiac troponin T (hs-cTnT) might be indicative of subclinical cardiac injury (7). N-terminal pro-B-type natriuretic peptide (NT-pro-BNP) is released by the stressed myocardium in response to volume and pressure load and is a good screening tool for detecting chronic ventricular dysfunction and heart failure (8). Elevated cardiac biomarker concentrations are associated with poor myocardial contractility and low cardiac output and correlate with echocardiographic measures of cardiac performance (9).
Prematurity entails an adverse cardiovascular risk profile, but sparse knowledge exists on cardiac biomarkers, that could identify and monitor former preterm infants with early cardiac damage already at preschool age.
This study aimed to investigate differences in cardiac biomarkers (hs-cTnT and NT-pro-BNP), left ventricular systolic function, and left ventricular mass (LVM) in former preterm infants in comparison with term controls at preschool age.
The current analysis is part of the cross-sectional study “Preterm infants and early markers for an increased risk of cardiovascular disease,” which examined former very preterm infants and term-born controls at preschool age at the Department of Paediatrics, Innsbruck University Hospital, Austria, from May 2012 to March 2015. All participants undergoing blood sampling after a minimum overnight fasting period of 8 h at the study visit were considered eligible for cardiac markers measurements. The study protocol has been published in detail previously (3). Basic data of study participants were collected using questionnaires and follow-up databases. During the study visit, we recorded anthropometric data and blood pressure readings and determined hs-cTnT and NT-pro-BNP concentrations in plasma blood samples at the Central Institute for Medical and Chemical Laboratory Diagnosis (University Hospital of Innsbruck) using an electrochemiluminescence immunoassay (ECLIA). The limit of detection of the Elecsys hs-cTnT assay (cobas e 402 and 801 analyzer) is <3 ng/L with a measuring range of 3–10.000 ng/L. The limit of blank is 2.5 ng/L, and the limit of quantification is 13 ng/L (EP17-A2, Clinical and Laboratory Standards Institute, CLSI). The limit of detection of the Elecsys pro-BNP assay (cobas e 402 and 801 analyzer) is <5 ng/L with a measuring range of 5–35.000 pg/ml. The limit of blank is 3 pg/ml and the limit of quantification is 50 pg/ml (EP17-A2, CLSI). In statistical analysis of the data, the values of cardiac markers below the limit of detection were censored by imputed values of the method detection limit divided by the square root of two (10). Pediatric-specific reference intervals and cutoffs for Roche's Elecsys hs-cTnT and NT-pro-BNP assay were published in the Canadian Laboratory Initiative on Paediatric Reference Intervals (CALIPER) cohort (11). For 1–18 years, the lower limit of hs-cTnT (90% CI) is <3 (<3, <3) ng/L, and the 99th percentile cutoff (90% CI) is 11 (11, 14) ng/L. For NT-pro-BNP the lower limit (90% CI) is <5 (<5, 7) ng/L, and the 99th percentile cutoff (90% CI) is 216 (82, 250) ng/L (12).
A transthoracic echocardiographic examination was performed by experienced staff, using a Siemens ultrasound system equipped (ACUSON SC2000, Siemens Medical Solutions, PA, USA) with a 4- or 8-MHz transducer. Assessment of left ventricular systolic function included measurement of systolic fractioning shortening (FS), which was obtained non-invasively using M-mode echocardiography tracings. The left ventricular end-diastolic dimension (LVEDD) was measured at the R-wave of the cardiac cycle and the left ventricular end-systolic dimension (LVESD) at the end of the T-wave. FS was calculated using the following equation: FS (%) = LVEDD—LVESD / LVEDD × 100 (13). FS values of 26%–45% were defined as normal function (14). The left ventricular mass (LVM) was calculated using the Devereux's formula: LVM (g) = 0.8 × 1.04 × [(IVSD + LVIDD + LVPWD)3—LVIDD3] + 0.6 (15). The left ventricular mass index (LVMI) (g/m2) = LV Mass / Body Surface Area (BSA, Mosteller) (16).
Data analysis was performed using SPSS, version 29.0 for Windows (IBM Corp., Chicago, IL, USA). Descriptive statistics were used to characterize the individual variables and to determine the distribution of data. Values were expressed as numbers (frequencies, %), mean with standard deviation, and median with interquartile range. The Mann–Whitney U-test, Student's t-test, and the χ2 test were used where appropriate. A p-value p < 0.05 was considered statistically significant.
This study was approved by the ethics committee of the Medical University of Innsbruck (Approval No. AN 4491). Verbal consent was obtained from all study participants and written informed consent from all legal guardians prior to inclusion in the study.
Cardiac biomarker measurements were available in 25 former term and 80 former preterm infants and included in this study. In the preterm group, a total number of 23 children (28.7%) were extremely preterm-born (gestational age, <28 weeks), and 57 children (71.3%) were very preterm-born (gestational age, 28–32 weeks). FS and LVM measurements were performed in 18 (72%) former term and 70 (88%) former preterm infants. With regard to sex distribution, birth weight, and maternal educational status, the study groups did not differ from respective reference populations. Gestational age in the preterm group was similar to all very preterm infants in the survey area (17). Perinatal and postnatal characteristics of all children are given in Table 1.
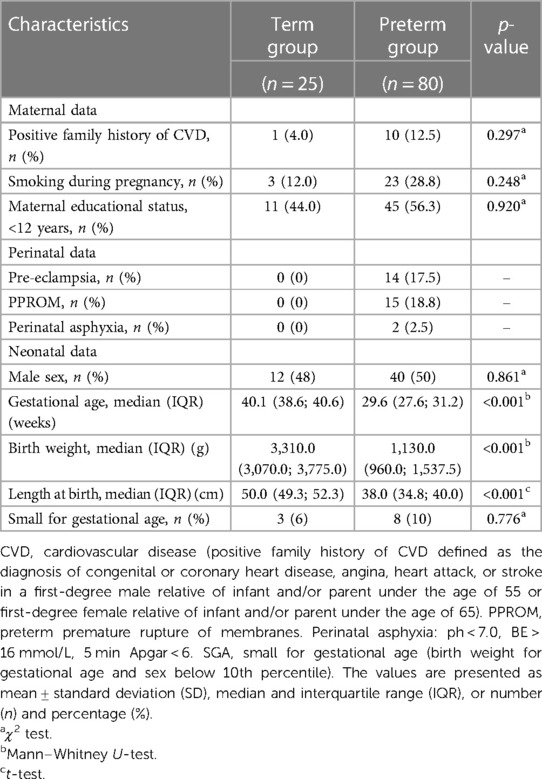
Table 1. Perinatal characteristics of the study population.
Former preterm infants had significantly lower weight and body mass indices and significantly higher systolic blood pressure readings than their term counterparts. No significant differences in mean and diastolic blood pressure were observed. There were no significant differences in the median concentration of hs-cTnT and the median concentration of NT-pro-BNP in both groups. FS and LVM/LVMI did not significantly differ between former term and former preterm infants. Detailed findings are presented in Table 2.
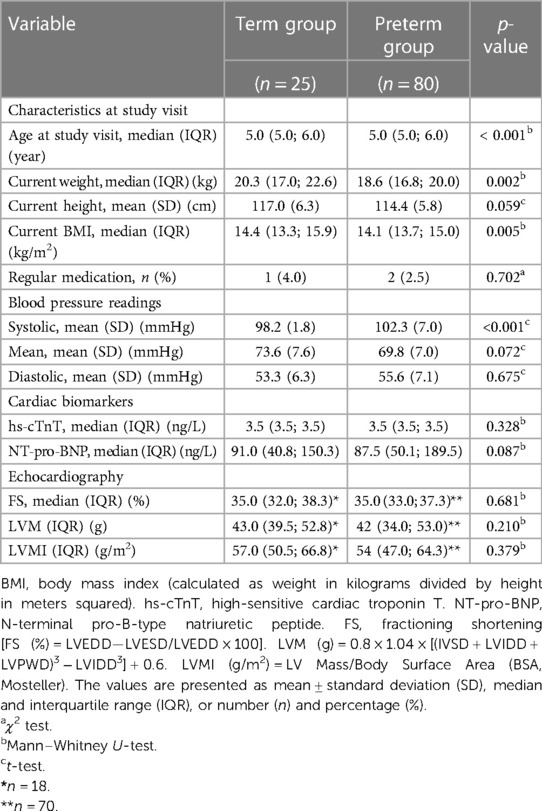
Table 2. Characteristics at the study visit.
No sex-specific differences were detected for blood pressure readings: (50 females, 47 males) systolic (101.3 vs. 101.1, p = 0.925), mean (70.8 vs. 71.5, p = 0.675), and diastolic (55.8 vs. 55.7, p = 0.980); cardiac biomarkers: (53 females, 52 males) hs-cTnT (3.5 vs. 3.5, p = 0.479), and NT-pro-BNP (110.5 vs. 77.0, p = 0.452); and echocardiographic findings: (46 females, 42 males) FS (35.0. vs. 36.0, p = 0.158), IVM (42.0 vs. 42.0, p = 0.575), and IVMI (53.0 vs. 56.0, p = 0.430) in the complete study population.
In the current study, only one former preterm-born child had an elevated hs-cTnT absolute value of 12.1 ng/L and thus above the normal range (99th percentile cutoff = 11), 16 children showed an elevated NT-pro-BNP above the normal range [99th percentile cutoff (90% CI) = 216], and the highest level detected was 797.0 ng/L. Fifteen out of the children with elevated values were former preterm infants (p = 0.073).
There were no significant differences between children with or without elevated NT-pro-BNP in this cohort, with regard to a positive family history of cardiovascular disease, maternal educational status, smoking during pregnancy, preterm complications (chronic lung disease, brain injury, necrotizing enterocolitis, sepsis, persistent ductus arteriosus or persistent pulmonary hypertension), or risk factors for alterations in cardiac function such as pre-eclampsia, pPROM, and asphyxia. Children with minor cardiac anomalies such as patent foramen ovale (n = 13), atrial septal aneurysm (n = 1), and dysplastic aortic valve (n = 2) and children after ductal ligation in the neonatal period (n = 3) showed significantly higher NT-pro-BNP levels (p = 0.045).
Concentrations of hs-cTnT were within a normal range (p = 0.396), and FS and LVM/LVMI showed normal values and no significant difference between children with or without elevated NT-pro-BNP levels. Findings are presented in Supplementary Table S1.
Former preterm infants have an unfavorable cardiovascular risk profile already at preschool age with higher systolic and diastolic blood pressure readings, elevated glucose and cholesterol levels, and decreased elastic properties of the descending abdominal aorta (3, 18, 19). Recently, an association between very preterm birth and decreased markers of platelet activation among preschoolers was reported, which can also predispose to cardiovascular events (20).
With regard to diagnosis, prognosis, and monitoring of cardiac distress in former preterm infants, there is a need for an additional tool, which provides insight into the structure and functioning of the heart. Thus, we investigated whether preterm birth is associated with altered cardiac biomarkers and left ventricular systolic function at preschool age. Hs-cTnT and NT-pro-BNP are the most commonly used cardiac biomarkers in clinical care because they correspond with cardiac function, and reference values for the pediatric cohort are well established (6, 11).
Our study revealed no significant difference in the concentrations of hs-cTnT and NT-pro-BNP between former term and preterm infants. Only one patient had an elevated hs-cTnT absolute value of 12.1 ng/L and thus slightly above the normal range—a male child born small for gestational age at 31 weeks with mild respiratory distress syndrome. His NT-pro-BNP concentration (55.0 ng/L) and his FS (33%) were in a normal range, therefore clinically not significant. In the general population, a minimally increased concentration of hs-cTnT, especially when approaching the lower detection limit, may be indicative of subclinical cardiac injury (7). This could be of importance if this alteration can be detected over a longer period of time. Of the study cohort, 16 patients showed an elevated NT-pro-BNP above the normal range. Six children out of this group (37%) had minor cardiac anomalies such as a patent foramen ovale, an atrial septal aneurysm, a dysplastic aortic valve, or a ductal ligation in the neonatal period. The highest values were found in two patients: 797 ng/L in a male former preterm with 31 weeks of gestational age and mild respiratory distress syndrome and 789 ng/L in a female former preterm with 30 weeks of gestational age, who was small for gestational age and had mild respiratory distress syndrome. Their hs-cTnT concentrations were <5 ng/L and FS of 35% and 37%, respectively, again all within the normal range. Of the 16 patients with elevated NT-pro-BNP levels in our study, 15 patients were born preterm. Preterm infants are prone to different insults such as sepsis or inflammation, hypotension, or oxidant injury, which can also affect myocardial cells and result in elevated cardiac biomarkers (21). It is also known that asphyxiated neonates and infants with respiratory distress syndrome have higher levels of cardiac biomarkers (22), low cardiac output, and poor myocardial contractility (23). We could not find a significant difference between children with and without elevated NT-pro-BNP levels with regard to perinatal asphyxia, sepsis, chronic lung disease, or other known complications of preterm infants at preschool age. The reason for this outcome might be that the elevation of cardiac biomarkers occurs immediately after the damaging event and normalizes after cardiac recovery.
Previous studies reported sex-specific differences in cardiac biomarkers in childhood and adolescence (1–18 years) with higher concentrations in males (12). However, we found no significant differences between males and females for hs-cTnT or NT-pro-BNP. This might be explained by the fact that our study focused on preschool-age children. Sipola-Leppänen et al. (24) observed sex-specific differences in cardiovascular risk profiles later in adolescents. Thus, it is possible that sex-specific differences in cardiac biomarkers also become noticeable in our population after the onset of puberty, as it is already known that circulating levels of cardiac natriuretic peptides are higher in fertile women and conversely men have on average higher circulating levels of cardiac troponin (25). In contrast to the strong evidence for cardiac biomarkers in adult populations with regard to diagnosis, prognosis, and monitoring of cardiac distress, their clinical value in pediatrics is not well defined. Until now it is unclear if a slight increase in these cardiac biomarkers observed might reflect a subclinical cardiac damage already in childhood. Hs-cTnT and NT-pro-BNP are used to identify subclinical cardiac damage in adults, and those with elevated levels appear to have an associated decrease in left ventricular function, determined by echocardiography (26). Previous studies have shown a reduction in myocardial function including altered ventricular structures, left ventricular hypertrophy, and reduced systolic and diastolic function in former very preterm infants later in life, independently of elevated cardiac biomarkers (5, 27). To complete our investigation, we performed echocardiography to see if we could detect a decrease in left ventricular systolic function or left ventricular mass. Well-established normal values for FS exist for infants and children born term, that's why we focused on former preterm-born children (13). A unique cardiac phenotype characterized by smaller left ventricles with altered systolic and diastolic functions of former preterm compared to same-age children born at term at 6 years of age has been reported previously (28, 29). We used conventional echocardiography to assess left ventricular systolic function in preterm infants and compared the results with term controls and found no significant difference, which is in line with a recent study, with no significant differences in left ventricular structure and function at preschool age either (30). These findings indicate that myocardial function indices showed no sustained difference between preterm and term-born infants and a normalized cardiac function after postnatal maturation (31). The echocardiographic measurement of LVM is important in the stratification of cardiovascular risk and could be predictive of outcomes. Concordant with systolic blood pressure readings, which showed only prehypertensive values, although significantly different in the two groups, the findings in left ventricular mass index were not altered in our study group yet. Even if our analysis did not find differences between blood-based cardiac biomarkers, left ventricular systolic function, and LVM/LVMI of preterm- and term-born children, it might be a good prognostic tool of subclinical cardiac alterations for a patient group, which is steadily increasing.
The main limitation of our study pertains to the small sample size, which was mostly due to the difficulty of obtaining blood samples from healthy children. Thus, clinically relevant findings could have been missed because of limited statistical power. Another limitation is that we used FS to assess left ventricular function; however, FS is dependent on preload and afterload, as well as contractility. Therefore, contractility may not be accurately described by FS (32). To evaluate ventricular function in an underfilled heart or to detect a left ventricular diastolic dysfunction, new advanced and load-independent techniques such as tissue Doppler imaging (TDI) strain and strain rate (SR) and 3D echocardiography would be appropriate (14).
In conclusion, we found no differences in blood-based cardiac biomarkers and left ventricular systolic function between former preterm- and term-born infants at preschool age. Further and larger studies are warranted focusing on cardiac biomarkers as potential prognostic tools for subclinical cardiac alteration after preterm birth.
The original contributions presented in the study are included in the article/Supplementary Material, and further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the Ethics Committee of Innsbruck Medical University (UN 4491). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
MH: Writing – original draft, Conceptualization, Formal Analysis, Investigation, Data curation, Methodology. AP: Conceptualization, Supervision, Writing – review and editing, Data curation. IO: Investigation, Writing – review and editing. EG: Supervision, Writing – review and editing. ER: Writing – review and editing. UP-P: Writing – review and editing. UK-K: Conceptualization, Funding acquisition, Investigation, Writing – review and editing, Supervision.
The authors declare that financial support was received for the research, authorship, and/or publication of this article.
This study was supported by funds from the Austrian National Bank (Project No. 14570) and the Austrian Heart Foundation. UK-K was also supported by the excellence initiative (Competence Center for Excellent Technologies, COMET) of the Austrian Research Promotion Agency FFG: “Research Center of Excellence in Vascular Ageing-Tyrol, VASCage” (K-Project No. 843536) funded by BMVIT, BMWFW, Wirtschaftsagentur Wien, and Standortagentur Tirol.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2024.1376360/full#supplementary-material
1. Stoll BJ, Hansen NI, Bell EF, Walsh MC, Carlo WA, Shankaran S, et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993-2012. JAMA. (2015) 314(10):1039–51. doi: 10.1001/jama.2015.10244
2. Eriksson JG, Forsen T, Tuomilehto J, Winter PD, Osmond C, Barker DJ. Catch-up growth in childhood and death from coronary heart disease: longitudinal study. Br Med J. (1999) 318(7181):427–31. doi: 10.1136/bmj.318.7181.427
3. Posod A, Komazec IO, Kager K, Peglow UP, Griesmaier E, Schermer E, et al. Former very preterm infants show an unfavorable cardiovascular risk profile at a preschool age. PLoS One. (2016) 11(12). doi: 10.1371/journal.pone.0168162
4. D'Agostino RB Sr, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circulation. (2008) 117(6):743–53. doi: 10.1161/CIRCULATIONAHA.107.699579
5. Schubert U, Muller M, Abdul-Khaliq H, Norman M. Preterm birth is associated with altered myocardial function in infancy. J Am Soc Echocardiogr. (2016) 29(7):670–8. doi: 10.1016/j.echo.2016.03.011
6. Bohn MK, Steele S, Hall A, Poonia J, Jung B, Adeli K. Cardiac biomarkers in pediatrics: an undervalued resource. Clin Chem. (2021) 67(7):947–58. doi: 10.1093/clinchem/hvab063
7. Wallace TW, Abdullah SM, Drazner MH, Das SR, Khera A, McGuire DK, et al. Prevalence and determinants of troponin T elevation in the general population. Circulation. (2006) 113(16):1958–65. doi: 10.1161/CIRCULATIONAHA.105.609974
8. Abassi Z, Karram T, Ellaham S, Winaver J, Hoffman A. Implications of the natriuretic peptide system in the pathogenesis of heart failure: diagnostic and therapeutic importance. Pharmacol Ther. (2004) 102(3):223–41. doi: 10.1016/j.pharmthera.2004.04.004
9. El-Khuffash A, Davis PG, Walsh K, Molloy EJ. Cardiac troponin T and N-terminal-pro-B type natriuretic peptide reflect myocardial function in preterm infants. J Perinatol. (2008) 28(7):482–6. doi: 10.1038/jp.2008.21
10. Succop PA, Clark S, Chen M, Galke W. Imputation of data values that are less than a detection limit. J Occup Environ Hyg. (2004) 1(7):436–41. doi: 10.1080/15459620490462797
11. Lam E, Higgins V, Zhang L, Chan MK, Bohn MK, Trajcevski K, et al. Normative values of high-sensitivity cardiac troponin T and N-terminal pro-B-type natriuretic peptide in children and adolescents: a study from the CALIPER cohort. J Appl Lab Med. (2021) 6(2):344–53. doi: 10.1093/jalm/jfaa090
12. Bohn MK, Higgins V, Kavsak P, Hoffman B, Adeli K. High-sensitivity generation 5 cardiac troponin T sex- and age-specific 99th percentiles in the CALIPER cohort of healthy children and adolescents. Clin Chem. (2019) 65(4):589–91. doi: 10.1373/clinchem.2018.299156
13. Gutgesell HP, Paquet M, Duff DF, McNamara DG. Evaluation of left ventricular size and function by echocardiography. Results in normal children. Circulation. (1977) 56(3):457–62. doi: 10.1161/01.CIR.56.3.457
14. Tissot C, Singh Y, Sekarski N. Echocardiographic evaluation of ventricular function-for the neonatologist and pediatric intensivist. Front Pediatr. (2018) 6:79. doi: 10.3389/fped.2018.00079
15. Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I, et al. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol. (1986) 57(6):450–8. doi: 10.1016/0002-9149(86)90771-X
16. Mizukoshi K, Takeuchi M, Nagata Y, Addetia K, Lang RM, Akashi YJ, et al. Normal values of left ventricular mass index assessed by transthoracic three-dimensional echocardiography. J Am Soc Echocardiogr. (2016) 29(1):51–61. doi: 10.1016/j.echo.2015.09.009
17. Gnigler M, Neubauer V, Griesmaier E, Zotter S, Kager K, Kiechl-Kohlendorfer U. Very preterm children are at increased risk of reduced processing speed at 5 years of age, predicted by typical complications of prematurity and prenatal smoking. Acta Paediatr. (2015) 104(3):e124–9. doi: 10.1111/apa.12859
18. Posod A, Pechlaner R, Yin X, Burnap SA, Kiechl SJ, Willeit J, et al. Apolipoprotein profiles in very preterm and term-born preschool children. J Am Heart Assoc. (2019) 8(8):e011199. doi: 10.1161/JAHA.118.011199
19. Odri Komazec I, Posod A, Schwienbacher M, Resch M, Pupp Peglow U, Kiechl S, et al. Aortic elastic properties in preschool children born preterm. Arterioscler Thromb Vasc Biol. (2016) 36(11):2268–74. doi: 10.1161/ATVBAHA.116.308144
20. Pechlaner R, Posod A, Yin X, Burnap SA, Kiechl SJ, Mayr M, et al. Very preterm birth results in later lower platelet activation markers. Pediatr Res. (2021) 89(5):1278–82. doi: 10.1038/s41390-020-1070-8
21. Nuyt AM, Lavoie JC, Mohamed I, Paquette K, Luu TM. Adult consequences of extremely preterm birth: cardiovascular and metabolic diseases risk factors, mechanisms, and prevention avenues. Clin Perinatol. (2017) 44(2):315–32. doi: 10.1016/j.clp.2017.01.010
22. Clark SJ, Newland P, Yoxall CW, Subhedar NV. Sequential cardiac troponin T following delivery and its relationship with myocardial performance in neonates with respiratory distress syndrome. Eur J Pediatr. (2006) 165(2):87–93. doi: 10.1007/s00431-005-0001-3
23. Evans N, Kluckow M. Early determinants of right and left ventricular output in ventilated preterm infants. Arch Dis Child Fetal Neonatal Ed. (1996) 74(2):F88–94. doi: 10.1136/fn.74.2.F88
24. Sipola-Leppanen M, Vaarasmaki M, Tikanmaki M, Hovi P, Miettola S, Ruokonen A, et al. Cardiovascular risk factors in adolescents born preterm. Pediatrics. (2014) 134(4):e1072–81. doi: 10.1542/peds.2013-4186
25. Mir TS, Flato M, Falkenberg J, Haddad M, Budden R, Weil J, et al. Plasma concentrations of N-terminal brain natriuretic peptide in healthy children, adolescents, and young adults: effect of age and gender. Pediatr Cardiol. (2006) 27(1):73–7. doi: 10.1007/s00246-005-1022-4
26. Bosello S, De Luca G, Berardi G, Canestrari G, de Waure C, Gabrielli FA, et al. Cardiac troponin T and NT-proBNP as diagnostic and prognostic biomarkers of primary cardiac involvement and disease severity in systemic sclerosis: a prospective study. Eur J Intern Med. (2019) 60:46–53. doi: 10.1016/j.ejim.2018.10.013
27. Burchert H, Lewandowski AJ. Preterm birth is a novel, independent risk factor for altered cardiac remodeling and early heart failure: is it time for a new cardiomyopathy? Curr Treat Options Cardiovasc Med. (2019) 21(2):8. doi: 10.1007/s11936-019-0712-9
28. Mohlkert LA, Hallberg J, Broberg O, Rydberg A, Halvorsen CP, Liuba P, et al. The preterm heart in childhood: left ventricular structure, geometry, and function assessed by echocardiography in 6-year-old survivors of periviable births. J Am Heart Assoc. (2018) 7(2). doi: 10.1161/JAHA.117.007742
29. Saleemi MS, El-Khuffash A, Franklin O, Corcoran JD. Serial changes in myocardial function in preterm infants over a four week period: the effect of gestational age at birth. Early Hum Dev. (2014) 90(7):349–52. doi: 10.1016/j.earlhumdev.2014.04.012
30. Mikkola K, Leipala J, Boldt T, Fellman V. Fetal growth restriction in preterm infants and cardiovascular function at five years of age. J Pediatr. (2007) 151(5):494–499.2. doi: 10.1016/j.jpeds.2007.04.030
31. Breatnach CR, El-Khuffash A, James A, McCallion N, Franklin O. Serial measures of cardiac performance using tissue Doppler imaging velocity in preterm infants <29weeks gestations. Early Hum Dev. (2017) 108:33–9. doi: 10.1016/j.earlhumdev.2017.03.012
Keywords: preterm infants, cardiac biomarker, N-terminal pro-B-type natriuretic peptide, high-sensitive cardiac troponin T, left ventricular systolic function
Citation: Höck M, Posod A, Odri Komazec I, Griesmaier E, Ralser E, Pupp-Peglow U and Kiechl-Kohlendorfer U (2024) Cardiac biomarkers and left ventricular systolic function in former very preterm infants and term controls at preschool age. Front. Pediatr. 12:1376360. doi: 10.3389/fped.2024.1376360
Received: 30 January 2024; Accepted: 11 March 2024;
Published: 25 March 2024.
Edited by:
Inga Voges, University Medical Center Schleswig-Holstein, GermanyReviewed by:
Petru Liuba, Lund University, Sweden© 2024 Höck, Posod, Odri Komazec, Griesmaier, Ralser, Pupp-Peglow and Kiechl-Kohlendorfer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michaela Höck bWljaGFlbGEuaG9lY2tAaS1tZWQuYWMuYXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.