 Maria Pérez-Torres Lobato1,2
Maria Pérez-Torres Lobato1,2 Maria Isabel Benitez-Carabante1,2
Maria Isabel Benitez-Carabante1,2 Laura Alonso1,2
Laura Alonso1,2 Silvia Torrents3Nerea Castillo Flores3
Silvia Torrents3Nerea Castillo Flores3 Maria Luz Uria Oficialdegui1,2
Maria Luz Uria Oficialdegui1,2 Melissa Panesso1,2Carla Alonso-Martínez4
Melissa Panesso1,2Carla Alonso-Martínez4 Maria Oliveras4
Maria Oliveras4 Berta Renedo-Miró4
Berta Renedo-Miró4 Joaquim Vives2,3,5
Joaquim Vives2,3,5 Cristina Diaz-de-Heredia1,2*
Cristina Diaz-de-Heredia1,2*
- 1Department of Paediatric Oncology and Haematology, Vall D'Hebron University Hospital, Barcelona, Spain
- 2Vall D'Hebron Research Institute (VHIR), Barcelona, Spain
- 3Banc de Sang I Teixits, Barcelona, Spain
- 4Department of Pharmacy, Vall D'Hebron University Hospital, Barcelona, Spain
- 5Department of Medicine, Faculty of Medicine, Autonomous University of Barcelona, Barcelona, Spain
Objectives: To describe mesenchymal stromal cells (MSCs) in the treatment of hematopoietic stem cell transplantation (HSCT) complications and to assess its safety and efficacy.
Methods: Single-center retrospective study (2016–2023). Patients under 20 years who received MSCs for the treatment of HSCT-related complications were included.
Results: Thirty patients (53.7% boys), median age at transplant 11 years (range 2–19) were included. MSCs indications were: graft-vs.-host disease (GVHD) in 18 patients (60%), of them 13 had acute GVHD (43.3%) and 5 chronic GVHD (16.7%); Grade 3–4 hemorrhagic cystitis (HC) in 4 (13.3%); poor graft function (PGF) in 6 (20%), 5 of them receiving MSCs with a CD34 stem cell-boost coinfusion; graft failure (GF) in 2 (6.7%), to enhance engraftment after a subsequent HSCT. Infusion-related-adverse-events were not reported. Overall response (OR) was 83% (25/30); 44% of responders (11/25) showed complete response (CR). OR for GVHD, HC, PGF and GF was 83.3%, 100%, 66.7% and 100% respectively. Response rate was 40% (95% CI: 20–55) and 79% (95% CI: 57–89) at 15 and 30 days. With a median follow-up of 21 months (IQR11–52.5), overall survival (OS) was 86% (95% CI: 74–100) and 79% (95% CI: 65–95) at 6 and 12 months post-MSCs infusion.
Conclusion: In our study, the most frequent indication of MSCs was refractory aGVHD (43.3%). Response rates were high (OR 83%) and safety profile was good.
Introduction
Advanced Therapy Medicinal Products (ATMP) represent a new category of medicines with a wide therapeutic potential for treating different types of hereditary and acquired diseases. ATMP encompass gene therapy, somatic cell therapy (SCT), and tissue-engineered products (1, 2). SCT refers to autologous or allogeneic cellular material that has been manipulated to change their biological characteristics and then is transferred into a patient for medical purposes (3–5). One type of SCT are mesenchymal stromal cells (MSCs). MSCs are multipotent, non-hematopoietic stem cells able to differentiate into various cell types, such as adipocytes, osteocytes, chondrocytes, and cells present in other connective tissues (6, 7). MSCs, which are present in adult and fetal tissues, can be derived from numerous sources such as adult bone marrow (BM), umbilical cord blood (UCB) or adipose tissue (8). However, BM and UCB are the most common sources for clinical use (9, 10). MSCs exhibit plasticity, self-renewal, immunomodulation, and anti-inflammatory properties. For example, they are able to secrete cytokines and growth factors at sites of tissue injury and inflammation or induce immunosuppressive effects by direct cell-to-cell interaction and paracrine signalling (11, 12). Additionally, they play an essential role in the BM niche, as they have the ability to support hematopoietic stem cell survival and proliferation (6). These properties have prompted their clinical use in the setting of regenerative medicine and hematopoietic stem cell transplantation (HSCT) (7, 8, 10).
HSCT is an established curative treatment modality for patients with severe hematological and non-hematological diseases (13, 14). Given the biological properties of MSCs, preclinical and clinical studies showed promising results in the treatment of HSCT complications, such as GVHD (15–17), GF, poor graft function (PGF) (18–21) and hemorrhagic cystitis (HC) (22). However, available clinical trials are scarce (15, 17, 23), and the efficacy of MSCs in a transplantation setting is so far unclear.
Methods
Study aims
The aim of this study was to describe the clinical use of allogenic MSCs in the treatment of HSCTs complications (GVHD, HC, GF or PGF) in the real-world practice.
The secondary objectives were to determine:
- The safety profile of MSCs during and immediately after infusion [infusion-related adverse events (AE)].
- The efficacy of MSCs therapy in terms of response rate [overall response (OR), complete response (CR), partial response (PR), probability of response, no response (NR)] and overall survival (OS).
Study design and inclusion criteria
Retrospective descriptive study between January 2016 and January 2023. Patients under 20 years of age who had received MSCs for the treatment of the above-mentioned HSCT-related complications were included. They all had at least 3 months of follow-up after MSCs infusions. All patients were treated in a single-center Pediatric Bone Marrow Transplant Unit. Neither patient received MSCs within a clinical trial, but off label. Given that the efficacy of MSCs in the transplantation setting is still unclear, they received MSCs when first line-therapies failed, which is the standard of care in our center.
For acute and chronic GVHD, MSCs were used in patients diagnosed with steroid-refractory (SR) GVHD after at least two previous lines of treatment. During MSCs treatment, previous immunosuppressive therapies were not discontinued, unless clinically indicated.
For patients with HC, MSCs therapy was indicated in case of grade 3 or 4 HC. As with GVHD, previous supportive therapies were not discontinued during MSCs treatment.
For patients diagnosed with PGF or GF, indication of MSC therapy was made based on the definitions below (24, 25).
Data sources and ethics
Anonymized clinical data were collected from the clinical records at Vall d’Hebron Hospital (VHH). Patients and/or legal tutors gave written consent for the transplantation procedure and to record patient´s anonymized transplantation-related data for studies. Legal tutors and/or patients signed the inform consent to receive compassionate use MSCs therapy. Good clinical practice according to Helsinki Declaration were applied. The study was approved by the Ethics Committee of VHH.
Mesenchymal stromal cells
Non-crossed matched allogenic MSCs were used in all cases. MSCs doses were manufactured in Banc de Sang i Teixits (BST) Barcelona, Spain. The dose was the same for all indications. However, there could be a little variation of the viable cells/kg dose (between 0.7 and 1.3 × 106), which depended on the manufacturing and culture expansion process. In this study, the median dose that patients received was 1.1 viable cells/kg (range 0.8–1.3 × 106 cells/kg).
Considering that we treated different HSCT-complications and a standardized dose and infusion schedule for MSC therapy has not yet been established the dosing and infusion schedule was based on previous publications (25–28). MSCs infusion scheme for each post-HSCT complication is summarized in Table 1.
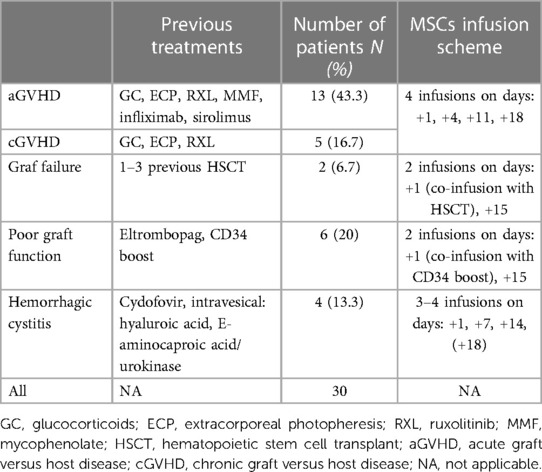
Table 1. MSCs therapy indications and infusion scheme.
MSCs source was either umbilical cord or bone marrow. MSC from different tissue sources complied with minimal identity criteria established by the International Society for Cell and Gene Therapy (29).
Wharton's Jelly (WJ)-MSCs were derived, expanded and characterized following Good Manufacturing Practice (GMP)-compliant procedures and appropriate donor informed consent as reported extensively elsewhere (30–32). Briefly, a fragment of umbilical cord tissue was cut longitudinally and the WJ was scrapped with a surgical scalpel, spread uniformly over the plastic surface of a T-flask with re-closable lid (TPP, Trasadingen, Switzerland), and incubated for 30 min at 37°C. After the incubation, 10 ml of Dulbecco's modified Eagle's medium (DMEM; Gibco, Carlsbad, CA, USA) containing 2 mmol/L glutamine was added and supplemented with 2 × 104 UI/ml penicillin (Invitrogen, New York, NY, USA), 20 mg/ml streptomycin (Invitrogen), 120 µg/ml amphotericin B (Invitrogen), and 10%–20% human serum B (hSerB, Banc de Sang i Teixits, Barcelona, Spain). After 2–5 days, a washing step with saline solution was performed, and 10 ml of fresh medium was added. From this point, the culture medium was replaced every 3–4 days. Cells were further expanded in vitro by seeding cell culture flasks at (1–3) × 103 cell/cm2. When the total number of cells reached at least 5 × 106, they were frozen in cryovials producing the master cell bank (MCB). Further expansion was performed after thawing for the generation of either working cell bank (WCB) or drug product (DP) directly. Final product (FP) was defined as the cell suspension resulting from thawing a DP, washed and conditioned for administration in patients.
MSC identity was confirmed as CD45–CD105+, CD31–CD73+, CD90+, HLA-DR−. MSC immune potency was confirmed by their capacity to inhibit proliferation of stimulated lymphocytes in co-culture.
Bone Marrow (BM)-MSCs were obtained under GMP conditions using a bioprocess that included a derivation step of MSC from BM aspirates and ex vivo expansion in an approximately 21-days. BM samples were harvested from the posterior iliac crest of donors and nucleated cells (NC) were isolated using an automated Sepax device (Biosafe) and Ficoll- Paque reagent (GE Healthcare). Then NC were washed and plated at 2 × 105 cells/cm2 onto cell culture vessels (CellSTACK) with DMEM supplemented with 10%. All cultures were maintained at 37°C and 5% CO2 in humidified incubators. The medium was changed every 3–4 days and at day 10, cells were trypsinized using 0.05% Trypsin/ethylenediaminetetraacetic acid (EDTA; Gibco, Life Technologies), when 70%–90% confluence was reached. Then cells were reseeded at 1 × 103 cells/cm2. Finally on day 21, cells were harvested and washed with a saline solution (Plasmalyte; Baxter) and were frozen in cryovials.
During the process, intermediate products and finally doses were analyzed to verify compliance with the established criteria according to GMP regulations (33). All MSC products tested negative for bacteria and Mycoplasma, and endotoxin levels were always below 0.5 EU/ml.
Definitions
Acute GVHD (aGVHD) was graded according to MAGIC criteria (34), which goes from 1 to 4, depending on the number of organs involved [skin, liver, lower gastrointestinal tract (GI) and upper GI] and its severity. Chronic GVHD (cGVHD) was graded according to the 2014 NIH criteria (35, 36). The overall severity of cGVHD was classified as mild, moderate, or severe based on organ-specific grading.
For HC diagnosis (22, 37), bacterial and fungal infections were ruled out. HC was categorized as grade 1: isolated microscopic hematuria; grade 2: macroscopic hematuria; grade 3; macroscopic hematuria with blood clots; grade 4: hemorrhage causing blood transfusion dependence, urethral obstruction, or renal function damage.
Primary graft failure was defined as the lack of achievement of an absolute neutrophil count (ANC) 0.5≥ × 109/L by day +28 after peripheral blood/bone marrow allo-HSCT and by day +42 after umbilical cord blood transplantation (24, 25, 38).
PGF was defined as: cytopenia in at least two hematopoietic lines [ANC <1 × 109/L, platelet count <30 × 109/L, hemoglobin (Hb) <10 g/dl] lasting for more than two consecutive weeks in the presence of stable donor chimerism and hypocellular bone marrow. Other explanations (such as disease relapse, drugs, or infections) were ruled out (24, 25, 38).
Response and survival
OR was defined as the proportion of patients who presented a PR or CR to MSC therapy. For GVHD CR was reached when the disease resolved completely and no other treatments after MSC infusion were needed. PR was defined as improvement in staging of at least one involved organ, grade or score (in case of cGVHD) and at least steady state on other symptoms (39). For GF, CR was achieved when ANC ≥0.5 × 109/L was recovered. PGF CR was defined as ANC >1 × 109/L, platelet count >30 × 109/L, Hb >10 g/dl (20). Response in at least 1 hematopoietic cell lineage was considered as PR. For HC, CR was achieved when gross hematuria disappeared. If it persisted but improved in at least one grade, it was was considered PR (38). Overall response, overall survival and event-free survival were calculated from first MSC infusion.
Safety assessment
Patients were monitored throughout the MSC infusion and 4 h after the procedure; during the infusion, non-invasive continuous cardiac and respiratory monitoring was performed, and vital signs were recorded hourly for up to 4 h after infusion. Premedication was not administered to any patient.
Since this was not a clinical trial, but an observational retrospective study, only AEs occurring during 4 h after MSCs infusion were considered, as this information was specifically documented in the patient clinical charts. However, patients’ medical charts were carefully reviewed in search of other possible AEs during the follow-up period.
Statistical analyses
Statistical analyses were performed in SPSS (version 28.0). Significance was set at a p level of 0.05 (two-tailed). Qualitative results were expressed as absolute and relative frequencies and quantitative variables, as median and interquartile range (IQR) or range. To test if quantitative data was normally distributed, Shapiro-Wilk Test was used. Mann-Whitney U-test was applied to analyze if time from 1st MSCs infusion to OR was associated with better response (PR or CR). Kaplan Meier (KM) estimator was used to evaluate and graphically display OS. Cumulative incidence was used to estimate the probabilities of partial and complete response. Probabilities were reported as percent with a 95% confidence interval (CI).
Results
Patient characteristics
Thirty patients (53.7% boys, 46.3% girls), median age at transplant 11 years (range 2–19) treated at a single institution were included. One patient was included twice (patient 2 Tables 2, 3), as she received MSCs for 2 different indications at separated time-periods; first she received two MSC infusion due to GF, and 2 months later, 3 weekly MSCs infusions were administered to treat aGVHD.
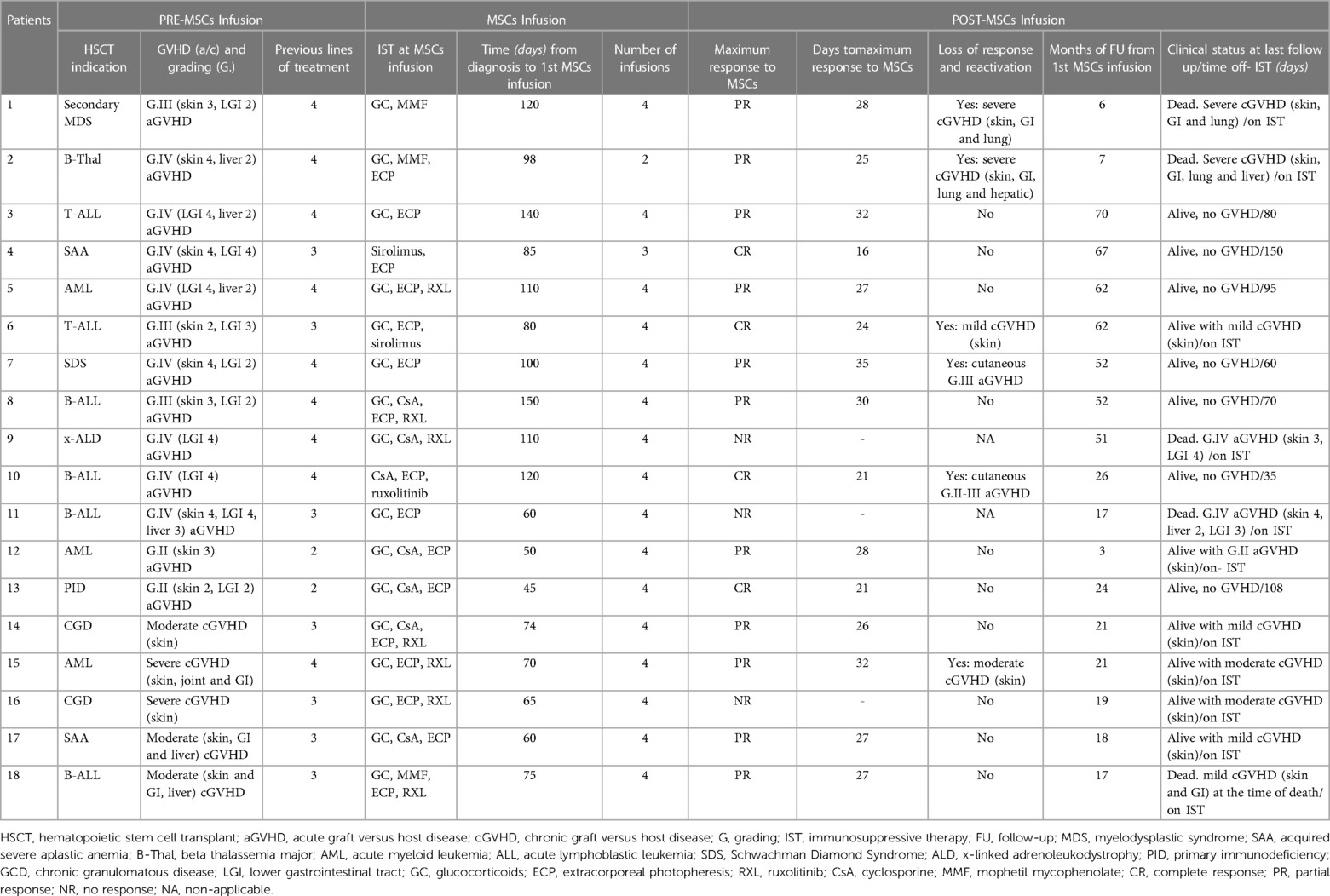
Table 2. MSC therapy in patients with GVHD.
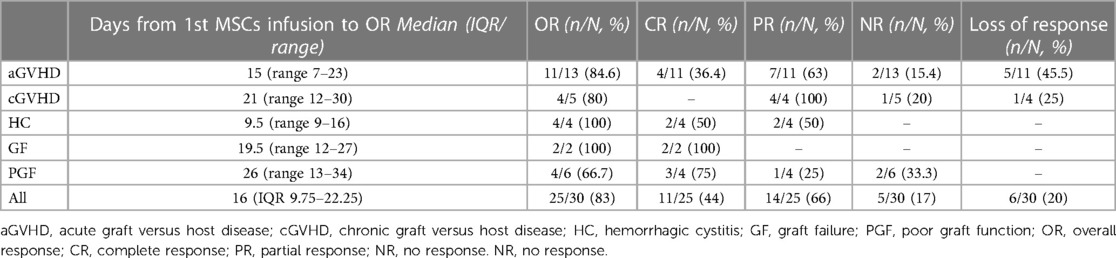
Table 3. Evaluation of response to MSC therapy according to the indication of MSCs.
Patients received an HSCT due to a malignant disease (n = 16, 53.3%) or a non-malignant disease (n = 14, 46.6%). Most common malignant condition was acute lymphoblastic leukemia (n = 13, 81.2%) and most frequent non-malignant disorders were bone marrow failure (n = 4, 28.5%) and primary immunodeficiency (n = 4, 28.5%).
MSCs indications, characteristics and dosage
MSCs therapy indications and infusion scheme are summarized in Table 1. MSCs therapy and patients characteristic for each specific indication is summarized in Supplementary Table S1 (HC), Supplementary Table S2 (GF and PGF) and Table 2 (GVHD). There were two patients with GVHD that did not strictly followed the infusion scheme for his/her specific MSCs indication (patients 2 and 4, Table 2); patient 4 received 3 doses instead of 4, as he showed CR shortly after the second MSC infusion. Patient 2 received 2 MSCs doses, as she has previously got 2 MSCs infusion due to graft failure.
MSCs source was umbilical cord (56.7%) or bone marrow (43.3%). The median number of infusions was 4 (IQR 2–4).
MSCs indications were: GVHD in 18 patients (60%), 13 of them had aGVHD and 5 cGVHD; Grade 3–4 HC in 4 patients (13.3%), all cases being due to BK virus; PGF in 6 patients (20%), of whom 5 were co-infused with a CD34 + stem cell boost; primary GF in 2 (6.7%), to enhance engraftment after a subsequent HSCT. All patients receiving a boost of CD34 cells were non-conditioned and the CD34 boost was administered on the same day of first MSC infusion. For both patients with GF, MSC first infusion was administered on the same day of the HSCT. The second MSC infusion was administered 2 weeks later (please see dosing schedule for patients with GF in Table 1).
Patient 1 (Supplementary Table S2) had previously undergone 3 allo-HSCT. Due to GF diagnosis, she received a 4th allo-HSCT from a different donor (unmanipulated haploidentical donor) and same stem cell source (peripheral blood). Conditioning consisted of fludarabine, cyclophosphamide, anti-thymocyte globulin and rituximab. Graft vs. host disease (GVHD) prophylaxis consisted of cyclosporine and methotrexate. Patient 2 (Supplementary Table S2) had undergone a previous allo-HSCT. After GF diagnosis, she received a second transplant from a different donor (mismatched unrelated donor, 9/10) and same source (peripheral blood). Conditioning consisted of fludarabine, cyclophosphamide and anti-thymocyte globulin. GVHD prophylaxis consisted of cyclosporine and mophetil mycophenolate (MMF).
Regarding previous lines of treatment, in case of GVHD, median lines were 4 (range 2–5). Of note, cyclosporine (CsA) was not considered a line of treatment, as it was part of GVHD prophylaxis during HSCT in all patients. MMF was neither considered a new line of treatment when referring to “previous lines of treatment” if patients had received it as GVHD prophylaxis (patients 2, 3, 8, 13 and 17). MSCs therapy for GVHD is summarized in Table 2.
Before the indication of MSCs therapy for PGF, one patient received a boost of donor CD34 + cells 50 days before first MSC infusion and another was treated with Eltrombopag but none of them responded. Eltrombopag was discontinued one month before MSCs infusion.
Response analysis
Response assessment is summarized in Table 3.
OR was 83% (25/30): 44% of responders showed CR (11/25) and 66% had PR (14/25). OR for aGVHD, cGVHD, HC, PGF and GF was 84.6%, 80%, 100%, 66.7% and 100% respectively.
Median time from first MSCs infusion to any OR was 16 days (IQR 10–22). For aGVHD it was 15 days (range 7–23), for cGVHD 21 days (range 12–30), for HC 9.5 days (range 9–16), for PGF 26 days (range 13–34) and for GF, 20 days (range 12–27), respectively. In case of GVHD, median time from first MSCs infusion to any OR in patients with CR was 8 days (IQR 12–20). Median time to maximum response in patients with GVHD and CR was 25 days (range −24).
The probability of response at 15 and 30 days was 40% (95% CI: 20–55) and 79% (95% CI: 57–89), respectively. After 34 days, probability of response reached a plateu [87.5%, 95% CI: 65–94)] and did not further increase (Figure 1). Five patients (17%) did not respond to MSC therapy. Loss of response (LR) was documented in 6 patients (20%) and median time from OR to LR was 2 months (IQR 2–5). All patients who showed LR had received MSCs due to GVHD.

Figure 1. Kaplan-Meier plot probability of response. The x-axis represents days of follow up after the first MSC infusion, while the y-axis is the proportion of subjects who shows response after MSC therapy. Probability of response was 40% at 15 days (95% CI: 20–55), 79% at 30 days (95% CI: 57–89). Observe that, after 34 days, probability of response reaches a plateu and does not further increase.
When analyzing time from first MSCs infusion to any OR and type of response (PR/CR), statistical significance was observed, showing that patients with an earlier response had better response [12 days to OR (IQR 8–20.5) in cases of CR vs. 19 days to OR (IQR 15–23) in patients with PR; p = 0.038]. These differences were also observed when GVHD (acute and chronic) was analyzed separately [8 days (IQR 7–16) to CR vs. 20.5 days (IQR 16–23) to PR; p = 0.009].
Safety
No patients experienced adverse events during or immediately after MSC infusion. No other AEs were retrospectively associated with MSCs therapy during the follow-up period.
Survival analysis
With a median follow-up of 21 months (IQR 11–52.5) from first MSCs infusion OS was 90% at 3 months (CI: 79–100), 86% at 6 months (CI:74–100) and 79% at twelve months (CI:65–95) post MSCs infusion (Figure 2). In case of GVHD (Supplementary Figure S1), OS was 82% (95% CI: 10–100), 77% (95% CI: 65–95) and 72% (95% CI: 59–889) at 6, 9 and 12 months respectively.
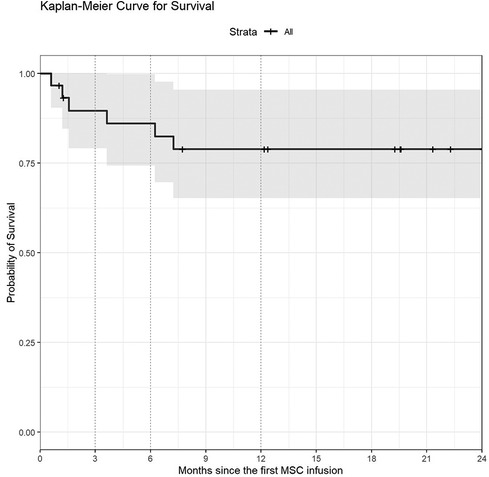
Figure 2. Kaplan-Meier plot of overall survival (OS) or probability of survival. The x-axis is months of follow up after the first MSC infusion until death occurs, while the y-axis is the proportion of subjects surviving. OS was 90% at 3 months (95% CI: 79–100), 86% at 6 months (95% CI: 74–100) and 79% at one year (95% CI: 65–95).
Overall survival for patients with NR was 53% (95% CI 21–100) at 6 and 12 months post MSCs infusion. In the PR group, OS were 80% (95% CI 60–100) and 60% (95% CI 36–100) at 6 and 12 months, respectively.
Overall 7 patients (24%) died, but in none of them death was related to MSC therapy. No deaths were observed in the CR group (Figure 3). Causes of death are summarized in Table 4.
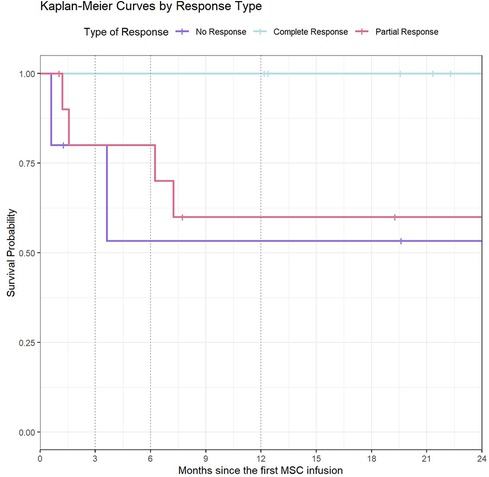
Figure 3. Kaplan-Meier curves by type of response. This graph represents the survival time (in months) from 1st MSC infusion, in relation to each type of treatment response. For patients with NR, OS was 53% (95% CI: 21–100) at 6 months of follow-up onwards. In the PR group, OS was 80% (95% CI: 60–100) at 6 months of follow-up and 60% (95% CI: 36–100) from 12 months onwards. Since no death were observed in the CR group, the survival probability was 100%.
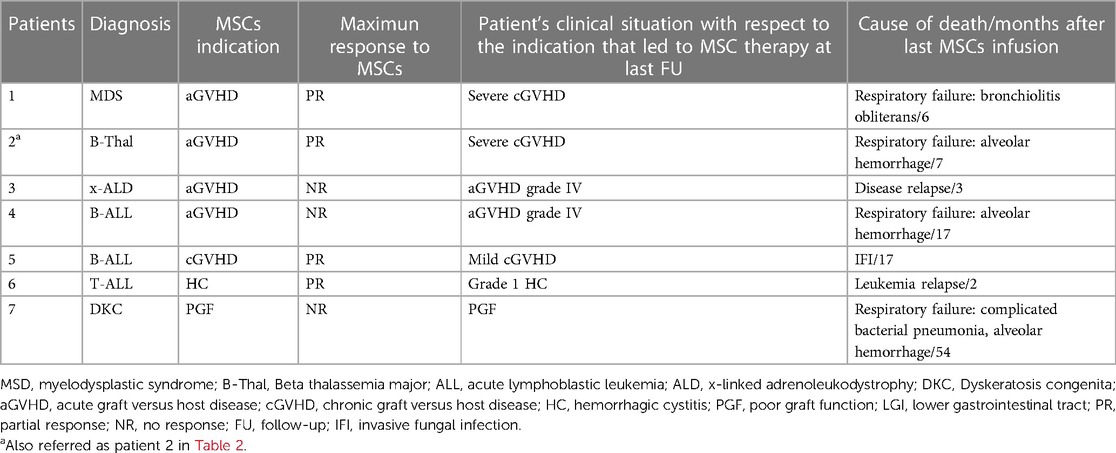
Table 4. Deaths and causes of death.
Discussion
In the present study, we describe MSCs as a therapy for HSCT-related complications in a series of 30 pediatric patients. The most frequent indication was refractory aGVHD (43.3%, n = 13/30). In general, response rates were high (OR 83%) and, similar to other studies (17, 18, 22), safety profile was good.
Regarding GVHD, clinical studies of MSC therapy in patients with SR-aGVHD have demonstrated favorable clinical response rates with an acceptable safety profile (40–45). For example, Kurtzberg et al. (46) recently reported on 241 children with grade II–IV SR-aGVHD who were on additional second-line treatments. The 28-day OR rate was 65% with a 14% CR. The 100-day OR was not assessed. In another study (47), the same group analyzed 54 children with primary SR-aGVHD who were naive to other immunosuppressant therapies and were treated with MSC product (remestemcel-L). A 70.4% OR was achieved, and response was sustained through day 100, including an increase in CR from 29.6% at day 28 to 44.4% at day 100. In the present study, patients with aGVHD had comparable response rates, with 84% OR and 36.4% CR. Nonetheless, 20% of all patients (4 of them with aGVHD) presented loss of response. Of note, two patients who received MSCs due to aGVHD developed severe cGVHD and died of respiratory failure. Although they had previously shown PR to MSCs, they were certainly at risk of developing cGVHD, since both of them had prior severe aGVHD (grade III and IV) (48). As opposed to the 2nd study of Kurtzberg et al. (42), patient population in our study were highly pretreated and refractory to previous treatments, which might have worsened response.Some authors (42, 44, 49) have also showed that, when MSCs were applied in an earlier stage of SR-aGVHD, the CR rates were higher. For example, Le Blanc et al. (42), in their study of a group of SR grade II-IV patients, described 55% CR and 16% PR. For that reason, taking into account the side effects of second line immunosuppression for GVHD and the good safety profile of MSCs (even in severely affected children), earlier use of MSCs therapy could be considered for patients with acute SR-GVHD.
Compared to aGVHD, there is limited use of MSCs therapy in cGVHD, probably because, in many cases, the chronic fibrotic processes of cGVHD are irreversible (49). In our study, MSCs therapy was more effective in aGVHD than in cGVHD (84% OR with 36.4% CR vs. 80% OR with no CR). Similar to previous report (49–52), most patients showed response, although only PR were observed.
Another indication for MSC is HC (22, 53, 54). Although there is limited clinical experience and it is mainly used in adults, some pediatric studies have shown promising results; for example, Tong et al. (22) reported thirteen pediatric patients with severe BKV-HC (grade 3–4) who presented 100% OR with rapid symptoms improvement. These results are consistent with our series, where OR was 100% (50% CR) and no loss of response was observed.
MSCs have also been used to reverse graft failure and enhance engraftment both in children and adults (18–21, 55, 56). In a meta-analysis by Li et al. (18), studies comparing MSC co-transplantation in allo-HSCT with allo-HSCT alone where analyzed (19 clinical trials), showing that MSC co-infusion generally improved engraftment without increasing mortality or relapse. In another study by Servais et al., (20). MSC were administered as a single i.v. infusion at a dose of 1–2 million(s) cells/kg body weight in patients with PGF. Within 90 days post-MSC infusion, OR was 53% with 37% CR, observing a response rate increase to 67% OR and 53% CR within 180 days after MSC infusion. In our series, all patients with GF and MSC co-transplantation presented CR. Compared to Servais et al., most cases of PGF received a CD34 + cells co-infusion, observing response rates were higher (OR 66% with 75% CR) and more rapid [26 days from first MSC infusion (range 13–34)]. Certainly, the CD34 + boost or the subsequent HSCT have most probably improved response rates in our study. Therefore, more evidence is needed to confirm the real impact of MSCs on engraftment and graft function, alone (in case of PGF) or as a co-adjuvant therapy.
Regarding survival analysis, and according to literature, OS rates varies between 50 and 80%, depending on MSCs indication and time-point of analysis, among others (18, 20, 22, 46, 47). In our study, OS was 90% at 3 months (95% CI: 79–100) and 79% at one year (95% CI: 65–95). Notably, similar to Kurtzberg et al. (47), we observed survival was higher in responders compared with non-responders [none of the responders died while, in the non-responder's group, OS was 53% (95% CI: 21–100) at 6 months of follow-up onwards]. For that reason, especially in the case of aGVHD (the most frequent MSCs indication in our study), considering that early use of MSCs seems to improve response and consequently, survival, with no identified safety concerns (even in gravely ill children such as our cohort), we believe that, despite possibly being a promising therapeutic tool, there is certainly room for improvement in the use of MSCs.
Regarding the causes of death (Table 4), three patients died of respiratory failure and alveolar hemorrhage. We believe these deaths were not related to MSCs therapy since MSCs infusions occurred more than 6 months before either death (7, 17 and 54 months in patients 2, 7 and 4 respectively). Additionally, all these patients had previous risk factors of pulmonary bleeding. For example, the patient with dyskeratosis congenital (patient 7, Table 4) maintained platelet count between 30 and 50.000 and developed empyema and pulmonary hemorrhage after chest tube drainage, which prompted death. The other two patients (one with beta-thalassemia and the other with B-acute lymphoblastic leukemia) developed severe cytomegalovirus pneumonitis and diffuse alveolar hemorrhage as a consequence, which led to death.
Limitations of our study stem in the small number of patients, the sample heterogeneity with variable follow-up periods, the retrospective design of the study, the lack of control group against which to assess the efficacy and safety of MSCs and the fact that it was single-center. Additionally, the possibility that some patients might have responded to other concomitant therapies rather than MSCs cannot be excluded. There are some confounding factors when comparing results between studies that we should also acknowledge, such as variability in MSCs donor types, MSCs dose per infusion, and number of infusions per patient—even within the same trial in some instances.
In conclusion, our study supports that MSCs seem to be a safe and effective therapy in the treatment of pediatric patients with HSCT-related complications. Further adequately powered prospective studies and clinical trials are required to confirm efficacy and establish the place and infusion schedule of MSCs therapy in each specific HSCT-related complication.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Vall d´Hebron Hospital Ethic Comitte. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
MPL: Conceptualization, Data curation, Formal Analysis, Methodology, Writing – original draft, Writing – review & editing. MB-C: Data curation, Methodology, Writing – review & editing. LA: Data curation, Methodology, Writing – review & editing. ST: Data curation, Writing – review & editing. NC: Data curation, Writing – review & editing. MU: Data curation, Writing – review & editing. MP: Data curation, Writing – review & editing. CA-M: Data curation, Writing – review & editing. MO: Data curation, Writing – review & editing. BR-M: Data curation, Writing – review & editing. JV: Data curation, Methodology, Writing – review & editing. CDH: Conceptualization, Data curation, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors thank BST, Red Española de Terapias Avanzadas (RICORS TERAV, expedient no. RD21/0017/0022, IP: Joaquim Vives) funded by Instituto de Salud Carlos III (ISCIII) in the context of Next Generation EU's Recovery, Transformation and Resilience Plan, and the joint BST-VHIR Musculoskeletal Tissue Engineering group, a Consolidated Research Group by Generalitat de Catalunya (2021-SGR-00877).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2024.1375493/full#supplementary-material
Supplementary Figure S1Kaplan-Meier curves in GVHD. This graph represents the probability of survival of patients with GVHD from 1st MSC infusion (purple curve), and the probability of survival of all the patients treated with MSCs in this study (black curve). For patients with GVHD, OS was 82% (95%CI: 10–100), 77% (95%CI: 65–95) and 72% (95%CI: 59-889) at 6, 9-and 12-months post MSCs infusion. For all the patients OS was a little higher; 90% at 3 months (95%CI: 79–100), 86% at 6 months (95%CI: 74–100) and 79% at twelve months (CI:65-95) post MSCs infusion.References
1. Hanna E, Rémuzat C, Auquier P, Toumi M. Advanced therapy medicinal products: current and future perspectives. J Mark Access Health Policy. (2016) 25:4. doi: 10.3402/jmahp.v4.31036
2. American Society of Gene and Cell Therapy. Gene & Cell Therapy FAQs. (2021). Available online at: https://asgct.org/education/more-resources/gene-and-cell-therapy-faqs (accessed April 24, 2021).
3. El-Kadiry AE, Rafei M, Shammaa R. Cell therapy: types, regulation, and clinical benefits. Front Med (Lausanne). (2021) 8:756029. doi: 10.3389/fmed.2021.756029
4. Mount NM, Ward SJ, Kefalas P, Hyllner J. Cell-based therapy technology classifications and translational challenges. Philos Trans R Soc Lond B Biol Sci. (2015) 370(1680):20150017. doi: 10.1098/rstb.2015.0017
5. Golchin A, Farahany TZ. Biological products: cellular therapy and FDA approved products. Stem Cell Rev Reports. (2019) 15:166–75. doi: 10.1007/s12015-018-9866-1
6. Crippa S, Bernardo ME. Mesenchymal stromal cells: role in the BM niche and in the support of hematopoietic stem cell transplantation. Hemasphere. (2018) 2(6):e151. doi: 10.1097/HS9.0000000000000151
7. Musiał-Wysocka A, Kot M, Majka M. The pros and cons of mesenchymal stem cell-based therapies. Cell Transplant. (2019) 28(7):801–12. doi: 10.1177/0963689719837897
8. Pevsner-Fischer M, Levin S, Zipori D. The origins of mesenchymal stromal cell heterogeneity. Stem Cell Rev Rep. (2011) 7(3):560–8. doi: 10.1007/s12015-011-9229-7
9. Horwitz EM, Maziarz RT, Kebriaei P. MSCs in hematopoietic cell transplantation. Biol Blood Marrow Transplant. (2011) 17:S21–9. doi: 10.1016/j.bbmt.2010.11.026
10. Malgieri A, Kantzari E, Patrizi MP, Gambardella S. Bone marrow and umbilical cord blood human mesenchymal stem cells: state of the art. Int J Clin Exp Med. (2010) 3(4):248–69. PMID: 21072260.21072260
11. Bernardo ME, Fibbe WE. Mesenchymal stromal cells and hematopoietic stem cell transplantation. Immunol Lett. (2015) 168:215–21. doi: 10.1016/j.imlet.2015.06.013
12. Galipeau J, Sensébé L. Mesenchymal stromal cells: clinical challenges and therapeutic opportunities. Cell Stem Cell. (2018) 22(6):824–33. doi: 10.1016/j.stem.2018.05.004
13. Bacigalupo A. Mesenchymal stem cells and haematopoietic stem cell transplantation. Best Pract Res Clin Haematol. (2004) 17:387–99. doi: 10.1016/j.beha.2004.06.003
14. Khaddour K, Hana CK, Mewawalla P. Hematopoietic stem cell transplantation. In: Aboubakr S, editor. StatPearls. Treasure Island, FL: StatPearls Publishing (2023).
15. Fisher SA, Cutler A, Doree C, Brunskill SJ, Stanworth SJ, Navarrete C, et al. Mesenchymal stromal cells as treatment or prophylaxis for acute or chronic graft-versus-host disease in haematopoietic stem cell transplant (HSCT) recipients with a haematological condition. Cochrane Database Syst Rev. (2019) 1(1):CD009768. doi: 10.1002/14651858.CD009768.pub2
16. Kelly K, Rasko JEJ. Mesenchymal stromal cells for the treatment of graft versus host disease. Front Immunol. (2021) 12:761616. doi: 10.3389/fimmu.2021.761616
17. Ringdén O, Gustafsson B, Sadeghi B. Mesenchymal stromal cells in pediatric hematopoietic cell transplantation a review and a pilot study in children treated with decidua stromal cells for acute graft-versus-host disease. Front Immunol. (2020) 11:567210. doi: 10.3389/fimmu.2020.567210
18. Li T, Luo C, Zhang J, Wei L, Sun W, Xie Q, et al. Efficacy and safety of mesenchymal stem cells co-infusion in allogeneic hematopoietic stem cell transplantation: a systematic review and meta-analysis. Stem Cell Res Ther. (2021) 12(1):246. doi: 10.1186/s13287-021-02304-x
19. Fernández-García M, Yañez RM, Sánchez-Domínguez R, Hernando-Rodriguez M, Peces-Barba M, Herrera G, et al. Mesenchymal stromal cells enhance the engraftment of hematopoietic stem cells in an autologous mouse transplantation model. Stem Cell Res Ther. (2015) 6(1):165. doi: 10.1186/s13287-015-0155-5
20. Servais S, Baron F, Lechanteur C, Seidel L, Baudoux E, Briquet A, et al. Multipotent mesenchymal stromal cells as treatment for poor graft function after allogeneic hematopoietic cell transplantation: a multicenter prospective analysis. Front Immunol. (2023) 14:1106464. doi: 10.3389/fimmu.2023.1106464
21. Ringdén O. Mesenchymal stromal cells as first-line treatment of graft failure after hematopoietic stem cell transplantation. Stem Cells Dev. (2009) 18(9):1243–46. doi: 10.1089/scd.2009.1809.edi
22. Tong J, Liu H, Zheng C, Zhu X, Tang B, Wan X, et al. Effects and long-term follow-up of using umbilical cord blood-derived mesenchymal stromal cells in pediatric patients with severe BK virus-associated late-onset hemorrhagic cystitis after unrelated cord blood transplantation. Pediatr Transplant. (2020) 24(2):e13618. doi: 10.1111/petr.13618
23. Stenger E, Giver CR, Langston A, Kota D, Das PK, Chinnadurai R, et al. Safety of autologous freshly expanded mesenchymal stromal cells for the treatment of graft-versus-host disease. Front Immunol. (2022) 13:959658. doi: 10.3389/fimmu.2022.959658
24. Kharfan-Dabaja MA, Kumar A, Ayala E, Aljurf M, Nishihori T, Marsh R, et al. Standardizing definitions of hematopoietic recovery, graft rejection, graft failure, poor graft function, and donor chimerism in allogeneic hematopoietic cell transplantation: a report on behalf of the American society for transplantation and cellular therapy. Transplant Cell Ther. (2021) 27(8):642–9. doi: 10.1016/j.jtct.2021.04.007
25. Stasia A, Ghiso A, Galaverna F, Raiola AM, Gualandi F, Luchetti S, et al. CD34 selected cells for the treatment of poor graft function after allogeneic stem cell transplantation. Biol Blood Marrow Transplant. (2014) 20(9):1440–3. doi: 10.1016/j.bbmt.2014.05.016
26. Sánchez-Guijo FM, López-Villar O, López-Anglada L, Villarón EM, Muntión S, Díez-Campelo M, et al. Allogeneic mesenchymal stem cell therapy for refractory cytopenias after hematopoietic stem cell transplantation. Transfusion. (2012) 52(5):1086–91. doi: 10.1111/j.1537-2995.2011.03400.x
27. Wang Z-, Yu H-, Cao F-, Liu Z-, Liu Z-, Feng W-, et al. Donor-derived marrow mesenchymal stromal cell co-transplantation following a haploidentical hematopoietic stem cell transplantation trail to treat severe aplastic anemia in children. Ann Hematol. (2019) 98(2):473–9. doi: 10.1007/s00277-018-3523-2
28. Sánchez-Guijo F, Caballero-Velázquez T, López-Villar O, Redondo A, Parody R, Martínez C, et al. Sequential third-party mesenchymal stromal cell therapy for refractory acute graft-versus-host disease. Biol Blood Marrow Transplant. (2014) 20(10):1580–5. doi: 10.1016/j.bbmt.2014.06.015
29. Dominici M, Le Blanc K, Mueller I, Slaper-Cortenbach I, Marini F, Krause D, et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The international society for cellular therapy position statement. Cytotherapy. (2006) 8(4):315–7. doi: 10.1080/14653240600855905
30. Oliver-Vila I, Coca MI, Grau-Vorster M, Pujals-Fonts N, Caminal M, Casamayor-Genescà A, et al. Evaluation of a cell-banking strategy for the production of clinical grade mesenchymal stromal cells from Wharton’s jelly. Cytotherapy. (2016) 18(1):25–35. doi: 10.1016/j.jcyt.2015.10.001
31. Torrents S, Del Moral AE, Codinach M, Rodríguez L, Querol S, Vives J. Optimized reagents for immunopotency assays on mesenchymal stromal cells for clinical use. Immunol Res. (2023) 71(5):725–34. doi: 10.1007/s12026-023-09385-1
32. García-Muñoz E, Vives J. Towards the standardization of methods of tissue processing for the isolation of mesenchymal stromal cells for clinical use. Cytotechnology. (2021) 73(3):513–22. doi: 10.1007/s10616-021-00474-3
33. Codinach M, Blanco M, Ortega I, Lloret M, Reales L, Coca MI, et al. Design and validation of a consistent and reproducible manufacture process for the production of clinical-grade bone marrow-derived multipotent mesenchymal stromal cells. Cytotherapy. (2016) 18:1197–208. doi: 10.1016/j.jcyt.2016.05.012
34. Harris AC, Young R, Devine S, Hogan WJ, Ayuk F, Bunworasate U, et al. International, multicenter standardization of acute graft-versus-host disease clinical data collection: a report from the mount Sinai acute GVHD international consortium. Biol Blood Marrow Transplant. (2016) 22(1):4–10. doi: 10.1016/j.bbmt.2015.09.001
35. Jagasia MH, Greinix HT, Arora M, Williams KM, Wolff D, Cowen EW, et al. National institutes of health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: i. The 2014 diagnosis and staging working group report. Biol Blood Marrow Transplant. (2015) 21(3):389–401. doi: 10.1016/j.bbmt.2014.12.001
36. Pidala J, Vogelsang G, Martin P, Chai X, Storer B, Pavletic S, et al. Overlap subtype of chronic graft-versus-host disease is associated with an adverse prognosis, functional impairment, and inferior patient-reported outcomes: a chronic graft-versus-host disease consortium study. Haematologica. (2012) 97(3):451–8. doi: 10.3324/haematol.2011.055186
37. Bedi A, Miller B, Hanson J, Goodman S, Ambinder R, Charache P, et al. Association of BK virus with failure of prophylaxis against hemorrhagic cystitis following bone marrow transplantation. J Clin Oncol. (1995) 13:1103–9. doi: 10.1200/JCO.1995.13.5.1103
38. Sureda A, Carpenter PA, Bacigalupo A, Bhatt VR, de la Fuente J, Ho A, et al. Harmonizing definitions for hematopoietic recovery, graft rejection, graft failure, poor graft function, and donor chimerism in allogeneic hematopoietic cell transplantation: a report on behalf of the EBMT, ASTCT, CIBMTR, and APBMT. Bone Marrow Transplant. (2024). doi: 10.1038/s41409-024-02251-0
39. Krasowska-Kwiecien A, Gozdzik J, Jarocha D, Wozniak M, Czogala W, Wiecha O, et al. Mesenchymal stem cells as a salvage treatment for severe refractory graft-vs-host disease in children after bone marrow transplantation. Transplant Proc. (2019) 51(3):880–9. doi: 10.1016/j.transproceed.2019.01.023
40. Bonig H, Kuçi Z, Kuçi S, Bakhtiar S, Basu O, Bug G, et al. Children and adults with refractory acute graft-versus-host disease respond to treatment with the mesenchymal stromal cell preparation “MSC-FFM"-outcome report of 92 patients. Cells. (2019) 8(12):1577. doi: 10.3390/cells8121577
41. Bader P, Kuçi Z, Bakhtiar S, Basu O, Bug G, Dennis M, et al. Effective treatment of steroid and therapy-refractory acute graft-versus-host disease with a novel mesenchymal stromal cell product (MSC-FFM). Bone Marrow Transplant. (2018) 53(7):852–62. doi: 10.1038/s41409-018-0102-z
42. Le Blanc K, Frassoni F, Ball L, Locatelli F, Roelofs H, Lewis I, et al. Mesenchymal stem cells for treatment of steroid-resistant, severe, acute graft-versus-host disease: a phase II study. Lancet. (2008) 371:1579–86. doi: 10.1016/S0140-6736(08)60690-X
43. Kebriaei P, Isola L, Bahceci E, Holland K, Rowley S, McGuirk J, et al. Adult human mesenchymal stem cells added to corticosteroid therapy for the treatment of acute graft-versus-host disease. Biol Blood Marrow Transplan. (2009) 15:804–11. doi: 10.1016/j.bbmt.2008.03.012
44. Lucchini G, Introna M, Dander E, Rovelli A, Balduzzi A, Bonanomi S, et al. Platelet-lysate-expanded mesenchymal stromal cells as a salvage therapy for severe resistant graft-versus-host disease in a pediatric population. Biol Blood Marrow Transplant. (2010) 16:1293–301. doi: 10.1016/j.bbmt.2010.03.017
45. Ball LM, Bernardo ME, Roelofs H, van Tol MJ, Contoli B, Zwaginga JJ, et al. Multiple infusions of mesenchymal stromal cells induce sustained remission in children with steroid-refractory, grade III-IV acute graft-versus-host disease. Br J Haematol. (2013) 163:501–9. doi: 10.1111/bjh.12545
46. Kurtzberg J, Prockop S, Chaudhury S, Horn B, Nemecek E, Prasad V, et al. Study 275: updated expanded access program for remestemcel-L in steroid-refractory acute graft-versus-host disease in children. Biol Blood Marrow Transplant. (2020) 26(5):855–64. doi: 10.1016/j.bbmt.2020.01.026
47. Kurtzberg J, Abdel-Azim H, Carpenter P, Chaudhury S, Horn B, Mahadeo K, et al. A phase 3, single-arm, prospective study of remestemcel-L, ex vivo culture-expanded adult human mesenchymal stromal cells for the treatment of pediatric patients who failed to respond to steroid treatment for acute graft-versus-host disease. Biol Blood Marrow Transplant. (2020) 26(5):845–54. doi: 10.1016/j.bbmt.2020.01.018
48. Grube M, Holler E, Weber D, Holler B, Herr W, Wolff D. Risk factors and outcome of chronic graft-versus-host disease after allogeneic stem cell transplantation-results from a single-center observational study. Biol Blood Marrow Transplant. (2016) 22(10):1781–91. doi: 10.1016/j.bbmt.2016.06.020
49. Ringden O, Keating A. Mesenchymal stromal cells as treatment for chronic GVHD. Bone Marrow Transplant. (2011) 46:163–4. doi: 10.1038/bmt.2010.275
50. Weng JY, Du X, Geng SX, Peng YW, Wang Z, Lu ZS, et al. Mesenchymal stem cell as salvage treatment for refractory chronic GVHD. Bone Marrow Transplant. (2010) 45:1732e40.
51. Introna M, Lucchini G, Dander E, Galimberti S, Rovelli A, Balduzzi A, et al. Treatment of graft versus host disease with mesenchymal stromal cells: a phase I study on 40 adult and pediatric patients. Biol Blood Marrow Transplant. (2014) 20(3):375–81. doi: 10.1016/j.bbmt.2013.11.033
52. Ringdén O, Leblanc K. Pooled MSCs for treatment of severe hemorrhage. Bone Marrow Transplant. (2011) 46:1158–60. doi: 10.1038/bmt.2010.262
53. Ringden O, Le Blanc K. Mesenchymal stem cells for treatment of acute and chronic graft-versus-host disease, tissue toxicity and hemorrhages. Best Pract Res Clin Haematol. (2011) 24:65–72. doi: 10.1016/j.beha.2011.01.003
54. Kallekleiv M, Larun L, Bruserud Ø, Hatfield KJ. Co-transplantation of multipotent mesenchymal stromal cells in allogeneic hematopoietic stem cell transplantation: a systematic review and meta-analysis. Cytotherapy. (2016) 18(2):172–85. doi: 10.1016/j.jcyt.2015.11.010
55. Ning H, Yang F, Jiang M, Hu L, Feng K, Zhang J, et al. The correlation between cotransplantation of mesenchymal stem cells and higher recurrence rate in hematologic malignancy patients: outcome of a pilot clinical study. Leukemia. (2008) 22(3):593–99. doi: 10.1038/sj.leu.2405090
Keywords: mesenchymal stromal cells, hematopoietic stem cell transplantation, graft vs. host disease, graft failure, poor graft function, hemorrhagic cystitis, children
Citation: Pérez-Torres Lobato M, Benitez-Carabante MI, Alonso L, Torrents S, Castillo Flores N, Uria Oficialdegui ML, Panesso M, Alonso-Martínez C, Oliveras M, Renedo-Miró B, Vives J and Diaz-de-Heredia C (2024) Mesenchymal stromal cells in the treatment of pediatric hematopoietic cell transplantation-related complications (graft vs. host disease, hemorrhagic cystitis, graft failure and poor graft function): a single center experience. Front. Pediatr. 12:1375493. doi: 10.3389/fped.2024.1375493
Received: 23 January 2024; Accepted: 28 March 2024;
Published: 9 May 2024.
Edited by:
Victor Aquino, University of Texas Southwestern Medical Center, United StatesReviewed by:
Elizabeth Stenger, Emory University, United StatesAlexander Ngwube, Phoenix Children’s Hospital, United States
© 2024 Pérez-Torres Lobato, Benitez-Carabante, Alonso, Torrents, Castillo Flores, Uria Oficialdegui, Panesso, Alonso-Martínez, Oliveras, Renedo-Miró, Vives and Diaz-de-Heredia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cristina Diaz-de-Heredia Y3Jpc3RpbmEuZGlhemRlaGVyZWRpYUB2YWxsaGVicm9uLmNhdA==