
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr. , 07 May 2024
Sec. Children and Health
Volume 12 - 2024 | https://doi.org/10.3389/fped.2024.1279033
 Amudha Pattabi1
Amudha Pattabi1 Ananth Nazarene2*
Ananth Nazarene2* Sejo Varghese2Samiya Mohamud Hassan1
Sejo Varghese2Samiya Mohamud Hassan1 Abdulqadir J. Nashwan3Surekha Kiran Patil1Kalpana Singh4
Abdulqadir J. Nashwan3Surekha Kiran Patil1Kalpana Singh4
Background: “Patient-centered” care positions the patient at the core and emphasizes fulfilling their unique needs, preferences, and values. This approach is particularly significant in the context of children. Although widely recognized as necessary, this approach is not universally implemented. The children find themselves in hospital wards where they are required to follow protocols and systems designed primarily for adults. In the appropriate atmosphere, children often express themselves more effectively through words, body language, and play, leading to a richer understanding of their needs. There is growing recognition of the importance of addressing children's concerns regarding hospital environments.
Aim: This study investigates children's satisfaction with the physical aspect of the hospital environment. Insights from this exploration could provide valuable input for creating hospital environments centered around children's needs and preferences.
Methods: This mixed-methods study involves children aged 6–14 years with parental consent from a premiere healthcare provider in the state of Qatar. The survey used nine items to gauge satisfaction with the existing hospital environment as a “child-friendly hospital” and another nine items to explore their expectations for such environments. The Mann–Whitney U and Kruskal–Wallis tests as well as thematic analyses were employed to assess the statistical significance of differences in satisfaction levels and children's expectations of the hospital's physical environment.
Results: A total of 398 children participated in the study. Of them, 40.3% were aged 6–8 years; 60.3% had experienced two to five hospital visits; 55.8% of children participated during their outpatient service visit; and 31.7% were Asian. Children's satisfaction levels with various aspects of the hospital environment—including its physical appearance, signage, lounge, consultant rooms, corridors, bedrooms, TV content, toys, and staff uniforms—were in the range of 42.9%–59%. The children expressed a desire for a hospital environment that is spacious, colorful, attractive, and filled with cartoon characters and toys in the children's hospital from the front lounge to the inpatient units.
Conclusion: The findings underline the importance of considering the perspectives of children in evidence-based healthcare design. The study reveals that children's satisfaction with the hospital environment is generally average or below average. Ultimately, a “child-friendly hospital environment” integrates children's rights into healthcare to significantly improve outcomes.
General hospitals are built to meet the expectations of the population they are designed to serve (1). In the context of children, a vulnerable population with complex health needs (2), their preferences are seldom asked during significant decision-making processes (3). Moreover, children are reticent (4) and overwhelmed with fear and anxiety during their hospital visits because of the unfavorable environment (5).
Hospitals are designed per experts’ plans based on the provisions and perspectives of staff and policymakers (6). Incorporating patients’ views is vital while designing a hospital (7). The hospital visit rate for children is comparatively higher than that of other population groups (8); however, children's perspectives on how the hospital environment should be are often ignored (9) or the least heard (7), despite their greater sensitivity to the hospital environment compared to other populations (10).
Despite their significant differences from adults both mentally and physically (11), children are often provided with the standard hospital environment (12), yet children are uniquely sensitive to the hospital environment in a way that distinguishes them from adults (10). For example, they often experience stress during their hospital visits, and if any medical procedure is involved, their stress levels have been reported as high (13). According to Boucher et al. (14), play is a highly valued therapy for resolving these hospitalization-related problems. However, it is infrequently used during hospital visits or short stays due to its limited age range of application for children. In addition, the dynamic healthcare environment poses a significant challenge to the uniform implementation of play therapy (15).
“Patient-centered” care has introduced challenges to healthcare providers. This transformative approach places the patient at the forefront, focusing on meeting individual needs, preferences, and values (16). Planetree prioritizes crafting an outstanding environment for children, aiming to bolster their sense of security (17). Although unconventional, this approach is widely recognized for its effectiveness (18). When children are provided with a friendly physical environment, they communicate effectively through words, body language, and play; this in turn aids clinicians in understanding the children (14) and enables them to deliver care that is better received and accepted. In the hospital environment, children are timid, unwell, and quiet, and they can develop anxieties about the hospital atmosphere (12, 19). Incorporating children's input in shaping their hospital environment is vital (20); however, children are often overlooked (9), even if research has investigated children's hospital experiences for decades (7). A child-friendly environment must take into account various factors, such as sound (21), color (22), artwork (23), lighting (24), furniture (25), green spaces, conditions that allow for the presence of the children's families (26), and the atmosphere (27). Although much research has focused on patient satisfaction in hospital settings (28–30), few studies offer in-depth insight into hospital physical environments (31).
Though the “baby-friendly hospital” is a well-known concept around the world (32), a “child-friendly hospital environment” is an emerging concept and has not been fully explored (26). The current generation of children has numerous demands regarding their hospital stays (8). Several studies have explored parents’ expectations (33), concerns (34), perceptions (35), and needs (36) regarding their hospitalized child, but children have been relatively underrepresented in assessments of the same areas (8). When it comes to the physical environment of an institution, though the institution is designed for them, children's voices are often unheard.
Hamad Medical Corporation (HMC) is the principal public healthcare provider in the State of Qatar. Hamad General Hospital (HGH) provides highly specialized and complex care, including child healthcare. The aim of the present study was to learn directly from participants about HMC’s physical environment and their expectations for the features of the facility they use. This study strives to catch a glimpse inside the children's reality to determine what they need. Current research provides evidence of what characterizes the best healthcare service in Qatar (37, 38), and the authors firmly believe that even minor changes in the delivery setting can further enhance healthcare services. This is a foundational step in transitioning from traditional pediatric environments to child-friendly hospitals so that “best healthcare service” is not just a label but a reality.
This study uses a mixed-methods, convergent parallel design and includes children who visited/were admitted to the pediatric (pediatric inpatient medical and surgical unit, day-care, and outpatient unit) facility of HGH during the study period. Children were aged 6–14 years and required consent from their parents to participate.
The authors surveyed the pediatric facility (pediatric inpatient medical and surgical unit, day-care, and outpatient unit) in HGH during the study period. Both the qualitative and quantitative questionnaires were self-reporting questionnaires. In the qualitative questionnaire, the participants were expected to write their opinions and views on the listed questions.
The questionnaire contained three sections: section I consisted of seven questions regarding participants’ demographic details; section II consisted of nine questions to assess the level of satisfaction with existing hospital settings in terms of being a “child-friendly hospital” environment; and section III consisted of nine questions to determine participants’ expectations for a “child-friendly hospital.”
In section II, a self-reported questionnaire was adapted from another study (39) and duly prepared (in English and Arabic) by the researchers to assess the level of children's satisfaction with the hospital environment. The responses use a 5-point Likert scale score ranging from 0 to 5 (very poor to excellent).
In section III, a self-reported questionnaire was adapted from another study (39) and duly prepared (in Arabic and English) by the researchers for this study. Participants were asked to write down their opinions and views on the listed questions to collect qualitative data (40).
The section II and section III questionnaire responses were prepared with simple language and smileys representing the 5-point Likert scale to facilitate the children's understanding.
The Institutional Review Board (IRB) at HMC reviewed and approved the study with the study number MRC-01-21-779.
A purposive sampling technique was used to harvest the study samples. The sample size for the survey was calculated with a 95% confidence interval (CI) and a 5% margin of error. The authors enrolled 398 participants for the quantitative survey (sections 1 and II). In addition, a qualitative questionnaire was completed by 30 participants (section III).
The data were analyzed using Statistical Package STATA 17.0 software. Quantitative data were elegantly presented using the median [interquartile range (IQR)], while categorical data were conveyed with clarity, expressed as numbers and percentages. The Mann–Whitney U and/or Kruskal–Wallis tests determined the association between demographic variables. p < 0.05 was considered statistically significant.
During the initial steps of coding and categorization of the qualitative data, two researchers (AN and SV) evaluated the qualitative data independently. Any discrepancy in coding or categorization was resolved by discussion between the two researchers. These steps were employed to enhance the validity and reliability of the thematic analysis. The thematic analysis in this study was inductive and driven by participant data. The thematic analysis focused on extracting and understanding the critical aspects of the hospital environment that impact children's satisfaction based on their direct feedback and perspectives. This approach aligns with the principles of patient-centered care and provides valuable insights for designing child-friendly hospital environments.
The analysis identified five key themes representing children's preferences for hospital environments: (1) colorful and attractive—emphasizing vibrant colors for visual engagement; (2) pictures and cartoon characters—highlighting the need for familiar, entertaining visuals for comfort; (3) spacious and big—indicating a preference for ample space associated with freedom and comfort; (4) toys—underscoring the importance of play and entertainment to engage and distract children; and (5) clinicians’ uniforms—emphasizing the impression of clinicians is crucial for children in establishing a therapeutic alliance.
A total of 398 children took part in the study. Of them, approximately 40.3% were aged 6–8 years, 33.9% were aged 9–11 years, and 25.8% were aged 12–14 years. Approximately half of the children (51%) were girls; 44.7% were in grade 1; 27.5% were in grades 4–6; and 27.8% were in grades 7–9. More than half of the children (60.3%) had visited the hospital 2–5 times, 29.9% were making their first visit, and 9.9% had made more than five visits. Of the children, 55.8% used outpatient services, 37.9% used inpatient medical services, and 6.2% used inpatient surgical services. Of the children, 41.3% were the firstborn in their family, 35.3% were the second born, and 23.5% were the third born or more among their siblings. Regarding nationality, 22.1% were from the Middle East and North Africa (MENA) region, excluding Qatar, 19.6% were Qataris, and 31.7% were Asian (Table 1).
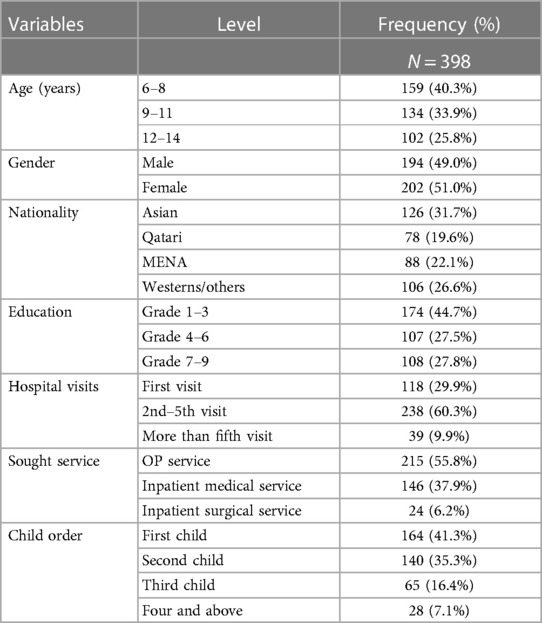
Table 1. Sociodemographic characteristics of participants.
The degree of satisfaction among children is displayed in Table 2. According to 33.2% of children, appearance was good/excellent, while 58.7% reported an average appearance. In addition, 32.3% of children agreed that signage was good/excellent, whereas 42.9% reported average satisfaction with signage. Furthermore, 26.5% agreed that the front lounge was excellent/good, and more than half thought it was average; regarding the consulting room, 33.5% felt it was excellent/good, while 50.6% thought it was average. A total of 31.7% thought the hallways were good/excellent, and 53.4% thought it was average. For hospital bedrooms, 27.5% said the bedrooms were excellent/good, whereas 59% described them as average. In addition, 60.0% of respondents thought the television content was average, while 22.3% said it was exceptional or good. In terms of toys, 57.4% of children thought the toys displayed were mediocre, while 21.7% thought they were great or good. Finally, 35.4% of children reported that the clinicians’ uniforms were excellent or good, and 52.5% reported them as average.
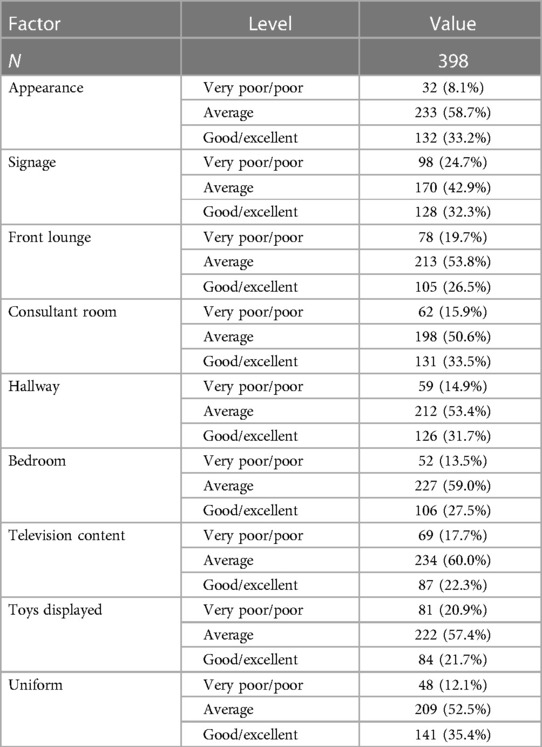
Table 2. Hospital environment satisfaction level.
The children's responses on nine-item open-ended questionnaires were reviewed, and the preliminary data coding was done using deductive codes drawn from the research questions. The initial codes were grouped into five categories: (1) colorful and attractive; (2) pictures and cartoon characters; (3) spacious and big; (4) toys; and (5) staff uniforms (41).
Color can uplift, engage, calm, and heal, and children in particular might be more susceptible to the effects of color (42). In this study, children expected almost everything to be colorful, including the walls of the hospital, chairs in the lounge, designs in the hallway, examination beds in the consulting room, beds and bedsheets in the inpatient room, and colorful lights throughout the hospital. Creating a child-friendly and welcoming environment in hospitals is essential to helping ease their anxiety and empower them (43). When children see vibrant colors and fun designs, it can distract them from the medical setting, reduce stress, and create a sense of comfort. Children across cultures appreciate color, though color preference is multifactorial. In this study, children expressed that the colors they expected in hospitals were blue and pink. Though there are gendered associations with these two colors, their calming and relaxing properties should not be ignored (42). Children anticipated an appealing hospital lounge featuring a green garden, expansive play area, and engaging elements, such as balloons, cartoons, rhymes, and simplified health educational videos on television. They also desired a welcoming atmosphere with staff offering simple candies.
Children are very excited about pictures and cartoons, which are vital to their cognitive development (44). Studies have revealed the distractive abilities of photographs and cartoons, and this can therefore benefit children during their hospital visits (45). In this study, children shared their expectations that the hallway, waiting room, and even the consulting and inpatient units have pictures of cartoon characters. They added that hospital signage should have animal or cartoon characters and smileys, and they asked for children's drawings to be displayed on the hospital walls.
Children need space to walk and run as their imaginations are vast (46). For children, space is seen as an area to play, and the children expressed the same sentiment in this study. They did not want the hospital to look congested or crowded; they expected it to be spacious. Moreover, they expressed interest in a play area in the lounge or waiting room. Another concern was the size of the televisions; they wanted them to be big and play children's entertainment content in English or with subtitles. Even the signage is prominent, with animated letters on the cartoon characters and animals. Space is a significant concern for the children, especially in the waiting room (47). They also shared their thoughts on the chairs and noted that they would be happy if they were bigger and child-friendly, as opposed to traditional hospital chairs that make the environment look like a frightening emergency department.
Toys significantly impact children's lives. It is therefore essential to consider this fact when choosing toys (48). Hospitals are unpleasant for children, and toys are the primary means of overcoming those negative perceptions and winning their confidence (49). The participants in this study reflected this notion. They expected toys at the front desk, in the hallway, hanging on the wall, in the signage, in the consulting room (rather than needles and other frightening medical devices), and in the hospital bed. In addition, they asked for age-appropriate, soft, educational, and interactive toys during their hospital stay. The consideration of children's perspectives on toys is essential, as the boost in a child's self-esteem and happiness, along with the facilitation of therapeutic relationships with health professionals, is achieved through toys, thereby benefiting the healing process (49).
When a nurse and a child first meet, the nurse's uniform and color scheme immediately cause a substantial amount of emotional upheaval. Uniforms are a non-verbal communication tool (50). The participants expressed that nurses’ uniforms bring needles to mind. They reported a preference for nurse uniforms that are pink or blue and have cartoons, flowers, or animals on them. While a white nurse uniform seems professional to adults, this attire is a source of fear, negative emotions, and anxiety for children and increases the perception of pain from treatments (51).
The satisfaction score was determined by summing the answers to nine questions that gauged how satisfied respondents were with the current hospital settings as a “child-friendly hospital” environment. The total mean satisfaction score was 28.86 ± 6.81 (range 8–45).
Table 3 illustrates the relationship between demographic characteristics and children's levels of satisfaction. Children who received inpatient surgical treatment were more satisfied than those who received inpatient medical care (median 31.0; IQR 26.0–37.5) and outpatient (OP) services (median 27.0, IQR 25.0–36.0). In terms of the relationship between satisfaction level and age, sex, nationality, education, hospital visits, and child order, we did not discover any statistically significant differences (Table 3).
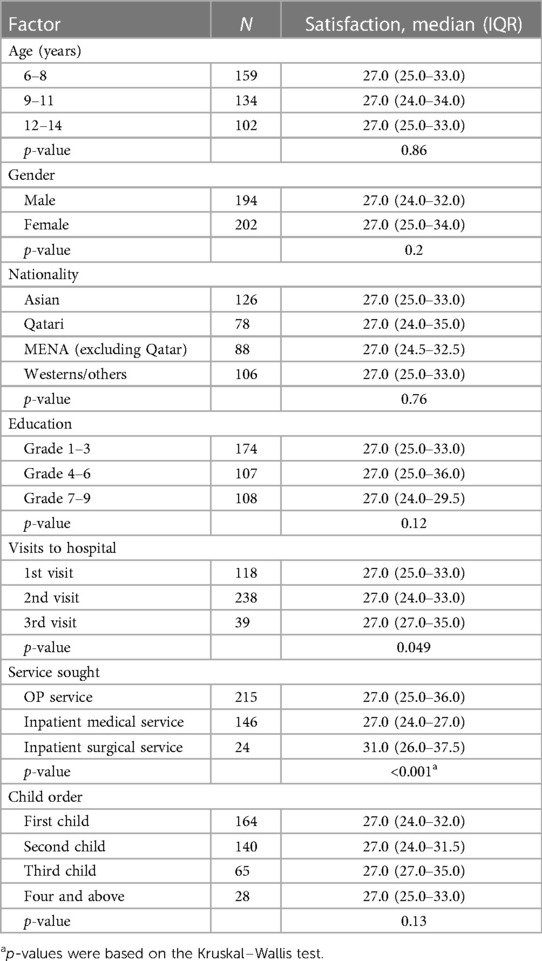
Table 3. Factors associated with children's levels of satisfaction and selected demographic variables.
Patient- and family-centered care is essential in pediatric healthcare systems worldwide (52). Patient satisfaction is significant in ensuring healthcare quality (53). The evolution of an efficient and long-lasting healthcare system depends on maintaining a patient-centered care model. Patient satisfaction and experience have traditionally been used to gauge healthcare quality (54). While studies on parental satisfaction in pediatric hospitals exist, they predominantly focus on the care perspective (55) rather than addressing the physical environment (56). Notably, children are often overlooked in expressing their experiences (57). Despite the traditional approach of surveying parental satisfaction, there is a growing trend to directly engage children in satisfaction surveys, recognizing their unique perspective (58).
Children can offer insightful comments about their experiences receiving medical care, and—more critically—children have a different perspective on receiving medical care than adults (59).
This study assessed satisfaction with the hospital's physical environment among children receiving medical services in the pediatric unit. A substantial amount of evidence supports that the physical environment of a healthcare facility has a more significant impact on treatment and recovery (60). Hence, all hospitals must strive to make their pediatric wings enjoyable and child-friendly (61).
Children's first impression of the hospital is crucial as it sets the tone for their entire stay. A welcoming and comforting environment from the outset is essential to ensuring a positive and satisfying patient experience right up until discharge (62). This study reveals that children's satisfaction with the hospital environment in the pediatric facility in this study is average regarding the hospital entrance, front lounge, and hallway appearance. The presence of parents during the data collection may explain this and could be perceived as a constraint to children sharing their negative views (63). The opposite trend was reported in a study from Taiwan, where a hospital environment featuring vivid, warm, and comfortable elements was added specifically for the children. It includes an open-air hanging garden, outdoor sculptures in the hospital's outer premises, a decorated waiting area, a donut-shaped lounge, turf, and warm sunlight in the hallway (64). The green, lush, nature-enriched hospital outer premises can counter the worry and fear of hospitals, as supported by decades of healthcare literature (65, 66). Regarding the physical setting, ventilation, lighting, and acoustics all proved significant for overall satisfaction (47). Children's expectations for a child-friendly hospital environment include a green garden with play facilities; a spacious, attractive lounge with surprise rewards; colorful chairs; and toys that facilitate meaningful engagement and distract from fear and anxiety.
Most children in this study reported average satisfaction with the hospital's physical structure and designs, and the same trend emerged regarding the content played on televisions placed in the waiting area, consulting room, and inpatient rooms. This indicates that participants were neither satisfied nor dissatisfied, and insistence on displaying cartoon movies plays a vital role in diverting their attention away from their distress and pain (67). Participants’ expectations regarding the televisions in the children's hospital were that they should be big and play cartoons, educational content, and simplified child-friendly health information in English or with English subtitles. Echoing the value of such entertainment, a study in Turkey revealed that animated cartoons displayed during painful procedures effectively reduced distress and pain (68), and an Italian study came to the same conclusion (69). Indeed, several studies have revealed that video distraction is an effective method of reducing anxiety in hospitalized children, comparable to oral midazolam or parental presence (70).
The toys and activities in the study hospital playroom are meant for the children during their hospital stay (7). However, the participants felt average satisfaction with the toys displayed and the activities they experienced during their hospital stays. Moreover, they expected colorful, soft, interactive, cartoon character-based toys to be placed in almost every area of the hospital, from the front lounge to inpatient beds. A study from Iran strengthened the evidence of the impact of toys and playrooms on hospitalized children (71).
An uncomfortable sleeping environment might significantly impact children's experience in hospital (72); unless addressed, this may negatively impact both the child and the parent (73). Study participants expressed average satisfaction with the bedroom provisions; this may have been due to their expectations that the bed and bedsheets feature cartoon characters and to find age-appropriate toys in the bedroom. A study reported the negative impact on children’s satisfaction as the hospital bedrooms failed to attract children (47).
Past evidence has supported children's desire for themed and colored-patterned uniforms (50) for healthcare workers. In the present study, more than half of the children stated that their satisfaction was average, while 10% reported poor satisfaction and 30% reported good satisfaction. This may be because they expected clinicians’ uniforms to be colorful and include cartoon characters, animals, or flowers.
A Swedish study (74) reported that children's fear compromises their satisfaction in the consulting room. It also reported the need for paintings, various kinds of animals, funny things to talk about, puzzles, and riddles. The lack of these features in the consulting room in this study could be the reason for half of the participating children's average level of satisfaction.
Children's age and sex are reported to be statistically significant in their satisfaction with a hospital's physical environment (64). However, the other demographic variables were not proven to have significance in our study regarding satisfaction with the hospital's physical environment.
Children have had limited and narrow attention in hospital experience surveys. However, this study is one of the few conducted in the Middle Eastern region. A traditional, adult-style questionnaire was used to collect data from the child participants; though this could pose a limitation, the authors used emoji icons for children to express their satisfaction levels. The presence of parents during the survey may play a significant role in more neutral responses than others. Studies have proven that parents have ambivalent attitudes toward considering children's opinions, which may have imposed pressure on the participants to complete the questionnaire faster. Nevertheless, using mixed methods to strengthen the quantitative findings is the strength of the study.
The results of this study promote child-centered research approaches and the development of age-appropriate survey tools, and the findings also encourage more studies worldwide focused on enhancing the quality of pediatric healthcare services.
Ideally, the perspectives of children and parents utilizing healthcare facilities should be integrated into the development of policies, design strategies, and healthcare management for children; this approach will facilitate the creation of hospital environments that are supportive and tailored to the needs of children and adolescents, minimizing reliance on adults’ assumptions about children's requirements. Furthermore, careful planning of the physical environment, including elements like lighting, color schemes, sound attenuation, adequate ventilation, and artwork, can significantly contribute to children's wellness and healing processes.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Institutional Review Board, Medical Research Center, Hamad Medical Corporation. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
AP: Writing – review & editing, Writing – original draft, Project administration, Investigation, Conceptualization. AN: Writing – review & editing, Writing – original draft, Methodology, Conceptualization. SV: Writing – original draft, Investigation, Conceptualization. SH: Writing – review & editing, Resources. AJN: Writing – review & editing, Supervision, Resources, Funding acquisition. SP: Writing – review & editing. KS: Writing – review & editing, Software, Formal Analysis, Data curation.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article from the Medical Research Centre (MRC), at Hamad Medical Corporation (HMC) (Grant: MRC-01-21-779).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bhatt J, Bathija P. Ensuring access to quality health care in vulnerable communities. Acad Med. (2018) 93(9):1271–5. doi: 10.1097/ACM.0000000000002254
2. Brenner M, Kidston C, Hilliard C, Coyne I, Eustace-Cook J, Doyle C, et al. Children’s complex care needs: a systematic concept analysis of multidisciplinary language. Eur J Pediatr. (2018) 177(11):1641–52. doi: 10.1007/s00431-018-3216-9
3. Ghosh N, Afroze S, Sultana A. Child friendly hospital environment: a demand of time. JMRKSH. (2020) 1(2):62–6.
4. Campbell H, Duke T, Weber M, English M, Carai S, Tamburlini G, et al. Global initiatives for improving hospital care for children: state of the art and future prospects. Paediatrics. (2008) 121(4):e984–92. doi: 10.1542/peds.2007-1395
5. Oliveira L, Gomes C, Bacelar Nicolau L, Ferreira L, Ferreira R. Environment in paediatric wards: light, sound, and temperature. Sleep Med. (2015) 16(9):1041–8. doi: 10.1016/j.sleep.2015.03.015
6. Gesler W, Bell M, Curtis S, Hubbard P, Francis S. Therapy by design: evaluating the UK hospital building program. Health Place. (2004) 10(2):117–28. doi: 10.1016/S1353-8292(03)00052-2
7. Karisalmi N, Stenhammar H, Kaipio J. What constitutes the patient experience of children? Findings from the photo elicitation and the video diary study. Patient Exp J. (2018) 5(2):54–68. doi: 10.35680/2372-0247.1292
8. Clarke S. An exploration of the child’s experience of staying in hospital from the perspectives of children and children’s nurses using child-centred methodology. Compr Child Adolesc Nurs. (2022) 45(1):105–18. doi: 10.1080/24694193.2021.1876786
9. Watkins N, Keller A. Lost in translation: bridging gaps between design and evidence-based design. HERD. (2008) 1(2):39–46. doi: 10.1177/193758670800100205
10. Ozcan H. Healing Design: A Holistic Approach to Social Interaction in Paediatric Intensive Care Units in the United States and Turkey. USA: Texas A&M University (2006). Retrieved from: https://api.semanticscholar.org/CorpusID:204877063 on 9/5/2022
11. William Li HC, Lopez V, Lee TLI. Effects of preoperative therapeutic play on outcomes of school-age children undergoing day surgery. Res Nurs Health. (2007) 30(3):320–32. doi: 10.1002/nur.20191
12. Scanlon M. Human factors and ergonomics in paediatrics. In: Carayon P, editor. Handbook of Human Factors and Ergonomics in Health Care and Patient Safety. (2nd ed). Mahwah, NJ: CRC Press (2011). p. 865–82. doi: 10.1201/b11219
13. Öztürk Şahin Ö, Topan A. Investigation of the fear of 7–18-year-old hospitalized children for illness and hospital. J Relig Health. (2019) 58(3):1011–23. doi: 10.1007/s10943-018-0688-x
14. Boucher S, Downing J, Shemilt R. The role of play in children’s palliative care. Children. (2014) 1(3):302–17. doi: 10.3390/children1030302
15. Gjærde LK, Hybschmann J, Dybdal D, Topperzer MK, Schrøder MA, Gibson JL, et al. Play interventions for paediatric patients in hospital: a scoping review. BMJ Open. (2021) 11(7):e051957. doi: 10.1136/bmjopen-2021-051957
16. Sun L, Yamin M, Mushi C, Liu K, Alsaigh M, Chen F. Information analytics for healthcare service discovery. J Healthc Eng. (2014) 5(4):457–77. doi: 10.1260/2040-2295.5.4.457
18. Abbas MY, Ghazali R. Healing environment: paediatric wards—status and design trend. Procedia Soc Behav Sci. (2012) 49:28–38. doi: 10.1016/j.sbspro.2012.07.003
19. Livesley J, Long T. Children’s experiences as hospital in-patients: voice, competence and work. Messages for nursing from a critical ethnographic study. Int J Nurs Stud. (2013) 50(10):1292–303. doi: 10.1016/j.ijnurstu.2012.12.005
20. Huisman ER, Morales E, van Hoof J, Kort HS. Healing environment: a review of the impact of physical environmental factors on users. Build Environ. (2012) 58:70–80. doi: 10.1016/j.buildenv.2012.06.016
21. Biley FC. Hospitals: healing environments? Complement Ther Nurs Midwifery. (1996) 2(4):110–5. doi: 10.1016/S1353-6117(96)80087-4
22. Ananth S. The natural next step. Explore (NY). (2008) 4(4):273–4. doi: 10.1016/j.explore.2008.04.010
23. Daykin N, Byrne E, Soteriou T, O’Connor S. The impact of art, design, and environment in mental healthcare: a systematic review of the literature. J R Soc Promot Health. (2008) 128(2):85–94. doi: 10.1177/1466424007087806
24. Beauchemin KM, Hays P. Sunny hospital rooms expedite recovery from severe and refractory depressions. J Affect Disord. (1996) 40(1–2):49–51. doi: 10.1016/0165-0327(96)00040-7
25. Baldwin S. Effects of furniture rearrangement on the atmosphere of wards in a maximum-security hospital. Hosp Community Psychiatry. (1985) 36(5):525–8.4007807
26. Nourmusavi Nasab S, Karimiazeri A, Mirbazel S. Effective environmental factors for reducing children’s fear in children’s hospital: using parent’s attitudes. ICONARP International Journal of Architecture and Planning. (2020) 8(1):1–19. doi: 10.15320/ICONARP.2020.102
27. Halim Babbu A, Haque M. A framework for the design of pediatric healthcare environment using the Delphi technique. Ain Shams Med J. (2023) 14(5):101975. doi: 10.1016/j.asej.2022.101975
28. Altimier LB. Healing environments: for patients and providers. Newborn Infant Nurs Rev. (2004) 4(2):89–92. doi: 10.1053/j.nainr.2004.03.001
29. Andrade C, Lima ML, Fornara F, Bonaiuto M. Users’ views of hospital environmental quality: validation of the perceived hospital environment quality indicators (PHEQIs). J Environ Psychol. (2012) 32(2):97–111. doi: 10.1016/j.jenvp.2011.12.001
30. Crow R, Gage H, Hampson S, Hart J, Kimber A, Storey L, et al. The measurement of satisfaction with health care: implications for practice from a systematic review of the literature. Health Technol Assess. (2002) 6(32):1–244. doi: 10.3310/hta6320
31. Mourshed M, Zhao Y. Healthcare providers’ perception of design factors related to physical environments in hospitals. J Environ Psychol. (2012) 32(4):362–70. doi: 10.1016/j.jenvp.2012.06.004
32. Chehab MA, Selim NAA, Itani R. The baby-friendly hospital initiative and Qatar, 2016. J Taibah Univ Med Sci. (2018) 13(3):309–10. doi: 10.1016/j.jtumed.2018.03.001
33. Kahabuka C, Moland KM, Kvåle G, Hinderaker SG. Unfulfilled expectations to services offered at primary health care facilities: experiences of caretakers of underfive children in rural Tanzania. BMC Health Serv Res. (2012) 12(1):158. doi: 10.1186/1472-6963-12-158
34. Hitt T, Ginsburg KR, Cousounis P, Lipman TH, Cucchiara AJ, Stallings VA, et al. Concerns and expectations of parents seeking subspecialist care for their child’s short stature. Horm Res Paediatr. (2019) 92(5):311–8. doi: 10.1159/000506739
35. Thébaud V, Dargentas M, Sizun J. Perceptions and expectations of parents regarding their position in a French NICU: quantitative and qualitative approaches. BMJ Open. (2022) 12(7):e052044. doi: 10.1136/bmjopen-2021-052044
36. Mohamed AR, Khaled WZ. Needs and expectations of parents having children with cancer from nurses. Med J Cairo Univ. (2019) 87(March):483–95. doi: 10.21608/mjcu.2019.52411
37. Ali FMH, Nikoloski Z, Reka H. Satisfaction and responsiveness with health-care services in Qatar—evidence from a survey. Health Policy. (2015) 119(11):1499–505. doi: 10.1016/j.healthpol.2015.09.012
38. AlYafei NA, Jaleel BNF, AlYafei NA, Jaleel BNF. Preparing to meet the oral health needs of the elderly in Qatar: a model for domiciliary oral health care services. World J Adv Res Rev. (2020) 8(3):184–91. doi: 10.30574/wjarr.2020.8.3.0459
39. Bany Hamdan A, Alshammary S, Tamani J, Peethambaran S, Hussein M, Alharbi M. The impact of creating a child-friendly hospital environment for paediatric cancer patients and their families in the Comprehensive Cancer Center at King Fahad Medical City. Curr Pediatr Rev. (2016) 20:47–54.
40. Badanapurkar A, Nelson D, Varghese S, Singh R, Haddad PM. Support and attitudes of Qatar mental health professionals to a proposed mental health inpatient smoking ban: results of a cross-sectional survey. J Psychiatr Ment Health Nurs. (2022) 29(2):327–45. doi: 10.1111/jpm.12777
41. Saldaña J. The Coding Manual for Qualitative Researchers. (2nd ed). SAGE (2013). ISBN 978-1-4462-4736-5; 978-1-4462-4737-2
42. Ajilian Abbasi M, Talaei A, Talaei A, Rezaei A. The use of appropriate colours in the design of children’s rooms: a short review. Int J Pediatr. (2014) 2(4.1):305–12. doi: 10.22038/ijp.2014.3204
43. Lerwick JL. Minimizing paediatric healthcare-induced anxiety and trauma. World J Clin Pediatr. (2016) 5(2):143–50. doi: 10.5409/wjcp.v5.i2.143
44. Strouse GA, Nyhout A, Ganea PA. The role of book features in young children’s transfer of information from picture books to real-world contexts. Front Psychol. (2018) 9:50. doi: 10.3389/fpsyg.2018.00050
45. van der Heijden MJE, Mevius H, van der Heijde N, van Rosmalen J, van As S, van Dijk M. Children listening to music or watching cartoons during ER procedures: a RCT. J Pediatr Psychol. (2019) 44(10):1151–62. doi: 10.1093/jpepsy/jsz066
46. Scott S, Gray T, Charlton J, Millard S. The impact of time spent in natural outdoor spaces on children’s language, communication, and social skills: a systematic review protocol. Int J Environ Res Public Health. (2022) 19(19):12038. doi: 10.3390/ijerph191912038
47. Qi Y, Yan Y, Lau SS, Tao Y. Evidence-based design for waiting space environment of paediatric clinics—three hospitals in Shenzhen as case studies. Int J Environ Res Public Health. (2021) 18(22):11804. doi: 10.3390/ijerph182211804
48. Dag NC, Turkkan E, Kacar A, Dag H. Children’s only profession: playing with toys. North Clin Istanb. (2021) 8(4):414–20. doi: 10.14744/nci.2020.48243
49. Ciuffo LL, de Souza TV, de Freitas TM, de Moraes JRMM, dos Santos KCO, dos Santos RDO. The use of toys by nursing as a therapeutic resource in the care of hospitalized children. Rev Bras Enferm. (2023) 76(2):e20220433. doi: 10.1590/0034-7167-2022-0433
50. Sanna P, Sollami A, Nicosia G, Dicembrino RB, Gandolfi R, Primosa F, et al. The nurses’ uniform in paediatrics, the opinion of children and nurses. Acta Bio Medica Atenei Parm. (2020) 91:67–76. doi: 10.23750/abm.v91i2-S.9212
51. Pakseresht M, Hemmatipour A, Gilavand A, Zarea K, Poursangbor T, Sakei-malehi A. The effect of nurses uniform colour on situational anxiety in school-age inpatient children (2019). Available online at: https://www.jrmds.in/articles/the-effect-of-nurses-uniform-colour-on-situational-anxiety-in-the-school-age-inpatients-children-5667.html (accessed 26 July 2023).
52. Bele S, Teela L, Zhang M, Rabi S, Ahmed S, van Oers HA, et al. Use of patient-reported experience measures in paediatric care: a systematic review. Front Pediatr. (2021) 9:753536. doi: 10.3389/fped.2021.753536
53. Selvarajah TM, Yamamoto E, Saw YM, Kariya T, Hamajima N. Satisfaction with health care services at the paediatric specialist clinic of the national referral center in Malaysia: a cross-sectional study of caregivers’ perspectives. JMIRx Med. (2022) 3(2):e33025. doi: 10.2196/33025
54. Ali H, Fatemi Y, Cole A, Tahat S, Ali D. Listening to the voice of the hospitalized child: comparing children’s experiences to their parents. Children. (2022) 9(12):1820. doi: 10.3390/children9121820
55. Loureiro F, Antunes V. Instruments to evaluate hospitalised children parents’ satisfaction with nursing care: a scoping review. BMJ Paediatr Open. (2022) 6(1):e001568. doi: 10.1136/bmjpo-2022-001568
56. Alazmah A, Parekh S, Bhatia S, Ashley P. Developing a child patient satisfaction survey: a quality improvement project. Eur Arch Paediatr Dent. (2021) 22(2):209–17. doi: 10.1007/s40368-020-00567-1
57. Gómez-de-Terreros-Guardiola M, Lozano-Oyola JF, Lanzarote-Fernández MD, Rupérez Bautista R, Avilés-Carvajal I, Schoenfelder T, et al. A measurement scale to assess children’s satisfaction with hospitalization in the Andalusian population. Int J Environ Res Public Health. (2019) 16(17):3110. doi: 10.3390/ijerph16173110
58. Butragueño Laiseca L, González Martínez F, Oikonomopoulou N, Pérez Moreno J, Toledo Del Castillo B, González Sánchez MI, et al. Survey of adolescent perception of hospital admission. The importance of hospital humanisation. Rev Chil Pediatr. (2016) 87(5):373–9. doi: 10.1016/j.rchipe.2016.04.003
59. Hargreaves DS, Sizmur S, Pitchforth J, Tallett A, Toomey SL, Hopwood B, et al. Children and young people’s versus parents’ responses in an English national inpatient survey. Arch Dis Child. (2018) 103(5):486–91. doi: 10.1136/archdischild-2017-313801
60. Jacobs K. Patient satisfaction by design. Semin Hear. (2016) 37(4):316–24. doi: 10.1055/s-0036-1593999
61. Casimir G. Why children’s hospitals are unique and so essential. Front Pediatr. (2019) 7:305. doi: 10.3389/fped.2019.00305
62. Medical Economics. Practice Pointers Your Waiting Room: Create a First-Rate Impression. Cranbury, NJ: Medical Economics (2003). Available online at: https://www.medicaleconomics.com/view/practice-pointersyour-waiting-room-create-first-rate-impression (Accessed May 25, 2023).
63. Singh I. Capacity and competence in children as research participants. EMBO Rep. (2007) 8(1):S35–9. doi: 10.1038/sj.embor.7401018
64. Woo JC, Lin YL. Kids’ perceptions toward children’s ward healing environments: a case study of Taiwan University Children’s Hospital. J Healthc Eng. (2016) 2016:8184653. doi: 10.1155/2016/8184653
65. Gaminiesfahani H, Lozanovska M, Tucker R. A scoping review of the impact on children of the built environment design characteristics of healing spaces. HERD Health Environ Res Des J. (2020) 13:193758672090384. doi: 10.1177/1937586720903845
66. Sherman SA, Varni JW, Ulrich RS, Malcarne VL. Post-occupancy evaluation of healing gardens in a paediatric cancer center. Landsc Urban Plan. (2005) 73(2):167–83. doi: 10.1016/j.landurbplan.2004.11.013
67. Cohen LL, Blount RL, Panopoulos G. Nurse coaching and cartoon distraction: an effective and practical intervention to reduce child, parent, and nurse distress during immunizations. J Pediatr Psychol. (1997) 22(3):355–70. doi: 10.1093/jpepsy/22.3.355
68. Bergomi P, Scudeller L, Pintaldi S, Molin AD. Efficacy of non-pharmacological methods of pain management in children undergoing venipuncture in a paediatric outpatient clinic: a randomized controlled trial of audiovisual distraction and external cold and vibration. J Pediatr Nurs. (2018) 42:e66–72. doi: 10.1016/j.pedn.2018.04.011
69. Cerne D, Sannino L, Petaan M. A randomised controlled trial examining the effectiveness of cartoons as a distraction technique. Nurs Child Young People. (2015) 27(3):28–33. doi: 10.7748/ncyp.27.3.28.e534
70. Liu PP, Sun Y, Wu C, Xu WH, Zhang RD, Zheng JJ, et al. The effectiveness of transport in a toy car for reducing preoperative anxiety in preschool children: a randomised controlled prospective trial. Br J Anaesth. (2018) 121(2):438–44. doi: 10.1016/j.bja.2018.02.067
71. Ghabeli F, Moheb N, Hosseini Nasab SD. Effect of toys and preoperative visits on reducing children’s anxiety and their parents anxiety before surgery and satisfaction with the treatment process. J Caring Sci. (2014) 3(1):21–8. doi: 10.5681/jcs.2014.003
72. Peirce LB, Orlov NM, Erondu AI, Anderson SL, Chamberlain M, Gozal D, et al. Caregiver and staff perceptions of disruptions to paediatric inpatient sleep. J Clin Sleep Med. (2018) 14(11):1895–902. doi: 10.5664/jcsm.7488
73. Stickland A, Clayton E, Sankey R, Hill CM. A qualitative study of sleep quality in children and their resident parents when in hospital. Arch Dis Child. (2016) 101(6):546–51. doi: 10.1136/archdischild-2015-309458
Keywords: child satisfaction, child-friendly hospital environment, child expectation, children hospital, children
Citation: Pattabi A, Nazarene A, Varghese S, Hassan SM, Nashwan AJ, Patil SK and Singh K (2024) Assessing child satisfaction and expectations for developing a child-friendly environment at the pediatric department in a general hospital in Qatar. Front. Pediatr. 12:1279033. doi: 10.3389/fped.2024.1279033
Received: 17 August 2023; Accepted: 1 April 2024;
Published: 7 May 2024.
Edited by:
Momcilo Jankovic, Fondazione MBBM, ItalyReviewed by:
Valentino Conter, Fondazione MBBM, Italy© 2024 Pattabi, Nazarene, Varghese, Hassan, Nashwan, Patil and Singh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ananth Nazarene YW5hemFyZW5lQGhhbWFkLnFh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.