 Sara R. Kim
Sara R. Kim Alpana Waghmare1,2,3
Alpana Waghmare1,2,3 Diego R. Hijano
Diego R. Hijano
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pediatr., 18 January 2024
Sec. Pediatric Infectious Diseases
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1339239
This article is part of the Research TopicClinical Challenges in Pediatric Transplant Infectious DiseasesView all 11 articles
The management of respiratory viruses prior to hematopoietic cell transplant (HCT) can be controversial and requires special consideration of host factors, transplant parameters, and the specific respiratory virus (RV). In the setting of adenovirus (ADV), human metapneumovirus (HMPV), influenza, parainfluenza virus (PIV), and respiratory syncytial virus (RSV) detection prior to hematopoietic cell transplant (HCT), clinical practice guidelines recommend transplant delay when possible; however, there is much more ambiguity when other respiratory viruses, such as seasonal coronaviruses (CoVs), human rhinovirus (HRV), and SARS-CoV-2, are detected. Our aims for this review include detailing clinical practical guidelines and reviewing current literature on pre-transplant respiratory viral infections (RVIs), including antiviral therapies and prevention strategies, when available. We will center our discussion on three representative clinical scenarios, with the goal of providing practical guidance to clinicians.
Patients who will receive or have undergone hematopoietic cell transplant (HCT) are at high risk of experiencing severe illness due to respiratory viral infections (RVIs) caused by chemotherapy-induced myelosuppression, impaired T-cell immunity, lymphopenia, and the use of immunosuppressive regimens (1–6). Prompt and accurate identification of viral respiratory pathogens is crucial for ensuring the best possible care for these patients. The symptoms of different RVIs are similar and do not help to differentiate pathogens. Therefore, patients suspected of having a RVI should be tested for a range of pathogens, allowing for targeted therapy where treatments exist, prompt implementation of appropriate infection control measures, appropriate monitoring of secondary infections, and minimization of empirical treatment for alternative conditions of concern.
One-year-old child with acute megakaryoblastic leukemia is a candidate for unrelated, mismatched cord transplant. Seven days before the start of conditioning, the patient tested positive for human rhinovirus (HRV) in routine multiplex PCR testing. The patient was asymptomatic at the time of positive PCR results and transplant conditioning.
The role of systematic testing of patients before transplant in the absence of symptoms has been proposed and implemented by many groups (7–9). This approach provides an opportunity for treatment if available, as well as implementation of infection prevention measures to mitigate spread within the unit. With the availability of highly sensitive multiplexed PCR assays, this practice has led to many questions, particularly related to the clinical relevance of multiple viral co-infections and whether changes in management (delay, treatment when available) should be recommended for asymptomatic detection of respiratory viruses (10–13). This is particularly challenging in immunocompromised children, in whom respiratory viruses are detected more frequently than in adults, and in those who can shed viruses for prolonged periods of time (14–16). In addition, transplant delay decisions are affected by the type of conditioning, transplant, donor, specific virus, and availability of antiviral agents. It is well established that myeloablative conditioning, allogeneic transplant, and matching unrelated or haploidentical donors are associated with an increased risk of poor outcome (17–25). A classification of respiratory viruses based on their potential for severe diseases and complications in these populations has been proposed. Respiratory syncytial virus (RSV), human metapneumovirus (HMPV), parainfluenza virus (PIV), influenza A and B, and adenovirus (ADV) have been grouped among the viruses most likely to cause severe disease, whereas human rhinoviruses (HRVs), human seasonal coronaviruses (CoVs), and human bocavirus are less frequently associated with severe disease (7, 26, 27). In a study of pediatric HCT recipients, pre-HCT detection of respiratory viruses, including HRVs, was associated with increased hospitalization within the first 100 days (7). Campbell et al. performed a large prospective study of children and adults undergoing HCT. They found that asymptomatic patients who had surveillance samples viral testing performed and detected, had no increase in bronchoscopy incidence or overall mortality, whereas those patients with respiratory symptoms had increased mortality compared to symptomatic individuals with no virus detective, irrespective of the virus (26). These data suggest that respiratory viruses, particularly in the presence of symptoms, may affect the transplant outcomes. Although there is a clear benefit from testing every patient with symptoms, the use of asymptomatic viral surveillance testing prior to HCT remains controversial and institutions vary in their approach.
Molecular amplification techniques have become the gold standard for detecting and identifying viruses, surpassing cell culture as the preferred method (28, 29). Antigen-based detection is commonly used in acute care settings because of its faster turnaround time, but it has lower sensitivity and specificity than molecular methods. Polymerase Chain Reaction (PCR) remains the most widely used amplification technique, and several Food and Drug Administration (FDA) approved tests are available to detect the most common respiratory viral pathogens. These tests range from single-analyte assays to multiplex panels (30–34). Multiplex PCR enables the amplification of multiple target sequences in a single reaction. Multiplex assays are advantageous because they save time, cost, and samples. However, multiplexing has limitations, particularly in terms of design, optimization, and the need for modifications. Targeted PCR assays are less complex, and there is no risk of competition between targets during PCR. However, multiple reactions may be required to detect multiple targets, which can result in higher costs for materials and labor, as well as the consumption of more samples per reaction (28–31, 33–36). A multiplex broad panel can be beneficial for immunocompromised individuals because symptoms can be unusual or subtle, and most of these viruses will present in a similar way, making it difficult to clinically diagnose the cause of the illness. Additionally, co-infections with multiple viruses are possible, particularly in children (8, 36, 37). The benefits of multiplex PCR testing outweigh the latter point and are recommended when available.
Viral load determination in the blood and the clinical management of viruses, such as cytomegalovirus or Epstein-Barr virus, has been facilitated by the implementation of validated quantitative assays. Furthermore, the use of WHO standards has made reporting and comparison across assays possible, facilitating clinical studies and advancing the field (38–40). Currently, no quantitative respiratory viral assays are available for clinical care. With the emergence of SARS-CoV-2, many groups have started using cycle threshold (Ct) values as a surrogate for viral RNA quantity in clinical samples to guide clinical decisions (41–45). The use of RT-PCR Ct values as a substitute for RNA concentration may result in inaccuracies due to a non-linear correlation with the quantity of viral RNA load within the analytical measurement range (AMR) of a given assay (46–48). Within-assay variability across the AMR paired with poor inter-assay agreement and lack of linear correlation limits the generalizability of the results (47). While numerous scientific societies, including the Infectious Diseases Society of America (IDSA) and the Association of Molecular Pathology (AMP), have advised caution when presenting clinical data that utilize Ct values or rely on Ct values to determine active infection, disease severity, or transmissibility, the utilization of Ct values in these contexts persists (49, 50). Progress in quantifying viral loads in respiratory samples will advance if a model similar to that of double-stranded DNA viruses is developed.
The development of molecular assays has led to an increase in the duration of detectable viral shedding, which can be prolonged in immunocompromised patients [16–18]. Decreased antiviral immunity due to underlying disease conditions and treatments such as high-dose steroids, myeloablative conditioning, and post-engraftment immunosuppression increases the risk of prolonged viral shedding (14–16). In addition, the majority of patients who shed respiratory viruses for over 4 weeks are allogeneic transplant recipients, and those with lower respiratory tract infection (LRTI) tend to have even longer periods of asymptomatic shedding (51). Several groups have reported prolonged viral shedding in HCT recipients, with a median duration of 5 weeks for HRVs, 4 weeks for CoVs, and 2 weeks for PIV. Some patients experienced prolonged shedding for more than 3 months (3, 52–54). Immunocompromised individuals with prolonged shedding are reservoirs for viral mutations, often resulting in antiviral drug resistance (6, 55–62). Although the risk of nosocomial spread during periods of asymptomatic shedding is unknown, outbreaks of these viruses in transplant units have been described, and the general recommendation is to continue contact isolation and droplet throughout the duration of the illness or hospitalization, and per institutional guidelines thereafter (1, 63–72). Finally, the clinical significance of prolonged viral shedding before transplant is unclear and it is unknown whether it increases the risk of recurrent symptoms, severe disease, or death. Therefore, decisions around delaying or proceeding with HCT in asymptomatic shedding require further study.
A 6-year-old child with polycythemia vera was evaluated for HCT from an unrelated, matched donor. Two weeks before the planned start of conditioning therapy, the patient developed cough and rhinorrhea. A nasal swab was collected for respiratory viral testing, and the results were positive for the parainfluenza virus 3.
HCT candidates that develop symptomatic RVIs prior to transplant represent a challenging clinical scenario. There is concern for poor transplant outcomes related to the infection itself, and a delay in transplant may be considered until the patient has recovered. However, the primary diagnosis for which transplant is being performed may include aggressive hematologic malignancies, for which a delay represents a significant risk of disease progression. Furthermore, depending on the cell source, there may be logistical considerations regarding donor and/or product availability, as well as other scheduling considerations. Given this complexity, transplant delay decisions must be approached carefully, considering both infection and disease status, along with other patient-specific factors.
Given that current guidelines recommend considering transplant delay when RVs are detected in HCT candidates (12, 73, 74), most transplant centers will consider transplant delay for viruses associated with severe diseases, such as RSV, influenza, HMPV, ADV, PIV, and SARS-CoV-2. This is an important consideration when interpreting contemporary studies to evaluate the impact of pre-HCT RVIs on transplant outcomes, as most are conducted in the setting of a recommendation to delay HCT. Campbell et al. collected pre-HCT and weekly post-HCT nasal washes through day 100 from 458 adults and children undergoing HCT with and without symptoms. Samples were tested by multiplex PCR. Patients with a RV detected prior to transplant had fewer days alive and out of the hospital, and higher mortality at day 100 after transplant compared to patients without a virus detected (26). Importantly, this effect was observed in patients with HRV detected alone, the most commonly detected RV. A follow up study in a larger cohort of 1,643 adult HCT recipients who underwent testing with multiplex PCR if they had symptoms, sought to further characterize the risk by stratifying by the presence of symptoms and the location of the infection (upper vs. lower respiratory tract infection) (9). Here, pre-HCT upper respiratory tract infection with any RV, including HRV, was not associated with increased overall mortality or fewer days alive and out the hospital. However, LRTI due to any virus, including HRV alone, were associated with increased overall mortality and fewer days alive and out of the hospital. The effect was driven primarily by allogeneic HCT recipients receiving myeloablative conditioning.
Data on pediatric HCT recipients are limited. As in adults, HRV is the most common RV detected, both before and after transplant. In a study of pediatric HCT candidates who underwent multiplex PCR surveillance testing pre-HCT, regardless of symptoms, those with pre-HCT HRV detection (N = 22) had outcomes at day 100 post-HCT comparable to those that were negative for all viruses (N = 34), including requirement for ventilatory support, length of stay, mortality, or days alive and out of the hospital (75). Children with LRTI were found to have fewer days alive and out of the hospital within the first 100 days post-HCT. In another study of 535 children undergoing allogeneic HCT, of which 75 had a positive RV test prior to transplant, patients with a positive RV result had lower overall survival and increased transplant related mortality (13). HRV was the most commonly detected virus, although it represented only 29% of the cases. In comparing patients in which transplant was delayed vs. not, the delayed patients had improved survival, although details on the reasons for delay are not clear. Though these data are suggestive of an association between pre-HCT RV detection and poor post-HCT outcomes, larger studies are needed to further define the effect of specific viruses, presence of symptoms, infection location, and transplant factors including cell source and conditioning regimen.
Our practice is to consider delay of transplant in any HCT recipient who have evidence of LRTI due to any RV, and in patients with symptomatic upper respiratory tract infection due to RSV, influenza, HMPV, ADV, PIV or SARS-CoV-2. Patients infected with treatable viruses should be started on therapy as outlined below. Delays are not routinely recommended for patients with HRV or non-SARS-CoV-2 coronaviruses. Individual patient factors including severity of underlying disease, urgency of transplant, level of anticipated immunosuppression, and other logistical issues were taken into consideration, and multidisciplinary approach was taken. If delay is feasible, the recommendation is to postpone HCT by at least 2 weeks with resolution of, or at least significant improvement in, symptoms. Ideally, the RV should no longer be detectable; however, this is not always achievable (Table 1). If viral load data is available, a decrease in viral load may also be reassuring to proceed to transplant, although no data to support this are currently available. Similarly, data on the optimal duration of delay are not known.
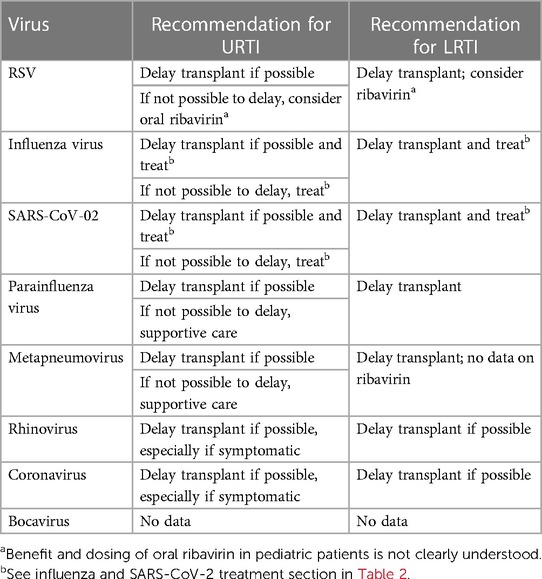
Table 1. Recommendations for respiratory viral infections before transplant.
14-year-old adolescent with relapsed ALL, who has a planned lymphodepletion in 2 weeks for chimeric antigen receptor (CAR) T-cell therapy, presents to clinic with a mild sore throat, cough, and low-grade fever. Physical examination revealed mild posterior pharyngeal erythema and rhinorrhea, but the lungs were clear to auscultation bilaterally with no oxygen requirement. A nasopharyngeal swab for a multiplex PCR of different respiratory viruses was positive for SARS-CoV-2. Prior to diagnosis, the patient was administered voriconazole for antifungal prophylaxis. While outpatient, the adolescent was started on ritonavir boosted nirmatrelvir for 5 days. After completing therapy, repeat SARS-CoV-2 PCR remained positive. Voriconazole was continued without any modifications, and hepatic function was monitored during treatment without any notable changes. Due to persistent SARS-CoV-2 positivity, the decision was made to delay HCT.
There are limited therapies available to prevent and/or treat RVIs in HCT recipients (Table 2). Most studies have been conducted in adults, immunocompetent children, and/or during the post-HCT period; therefore, the efficacy of these therapies is inferred in pediatric HCT candidates. In this section, we review the prophylactic and therapeutic alternatives available for children undergoing HCT. Of note, there are no US-market-approved therapies available for HMPV, PIV, HRV, or non-SARS-CoV-2 COVs.
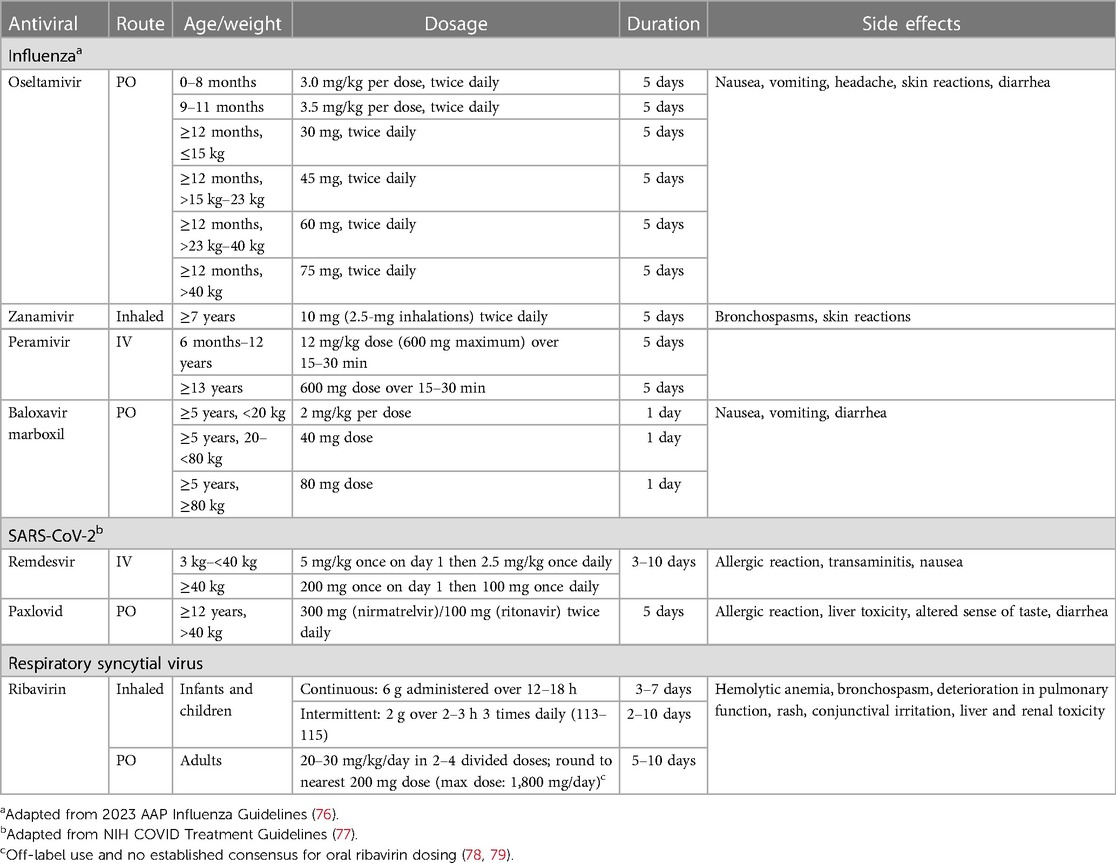
Table 2. Available therapeutic agents for respiratory viruses.
Cancer patients and HCT recipients are at high risk for influenza-related complications, including severe pneumonia and acute respiratory distress syndrome (80); therefore, annual vaccination and early initiation of antiviral therapy are recommended for maximal protection. Immunocompromised patients may present atypically and may shed influenza for a prolonged period. Exposure to influenza antivirals in the setting of prolonged shedding can promote antiviral resistance (6). With emerging resistance, the landscape of influenza antivirals continues to evolve, but the currently available influenza antivirals in the market are neuraminidase inhibitors (NAI) and one endonuclease inhibitor.
The first-line therapy for influenza are neuraminidase inhibitors (NAI), which are active against Influenza A and B (55, 81, 82). Oseltamivir (Tamiflu) is an oral NAI approved for children ≥2 weeks of age. It is generally well-tolerated, with nausea, emesis, and diarrhea being the most common side effects reported. Zanamivir, an inhaled NAI, is FDA approved for children ≥7 years but should be used in caution in patients with chronic lung disease and requires appropriate inhaler education. Parenteral NAIs include Zanamivir (currently in clinical trials) and Peramivir (approved as a single dose in children ≥6 months of age). In high-risk children, clinical guidelines recommend the treatment of influenza with NAIs, even if the symptom onset was greater than 48 h (76, 80). Treatment for uncomplicated influenza is recommended for 5 days but can be extended to 10 days in immunocompromised hosts (80).
Endonuclease inhibitors represent a new class of influenza antivirals that inhibit viral replication. Baloxavir marboxil (baloxavir) can be orally administered as a single dose in children ≥12 years of age and has been shown to be noninferior to NAIs in immunocompetent individuals with uncomplicated influenza (83, 84). However, the Centers for Disease Control and Prevention (CDC) does not recommend baloxavir in immunocompromised individuals due to limited studies and concerns regarding the development of resistance (85); baloxavir has been used in HCT recipients in the setting of NAI-resistant variants, severe infection, or failed first-line therapy (86–88). However, it should be avoided as stand-alone therapy. Combining baloxavir with NAIs, albeit well-tolerated, did not result in superior clinical outcomes compared with NAIs alone in patients hospitalized with severe influenza (89). Additional studies are needed to determine the role of combination therapy in immunocompromised children.
Despite the disease burden in both immunocompetent children and immunocompromised HCT recipients, there are no targeted antivirals against RSV currently available in the market. Ribavirin, a broad-spectrum guanosine nucleoside analogue, can inhibit viral replication of different RNA and DNA viruses, including RSV. Although inhaled ribavirin is FDA-approved for the treatment of RSV LRTI in pediatric patients, a systematic review of ribavirin use in infants with RSV LRTI did not lead to a decrease in mechanical ventilation or hospitalization in immunocompetent infants (90). However, a separate systematic review and meta-analysis of RSV LRTI, that included HCT recipients, showed a statistically significant decrease in mortality in mostly adult patients with hematologic disorders (91). Although there are a lack of randomized control trials prescribing ribavirin to immunocompromised and HCT recipients on ribavirin, the consensus and recommendations from international guidelines are to treat HCT recipients with RSV LRTI with inhaled or systemic ribavirin (12). However, the cost of aerosolized ribavirin ($29,953 per day) (92) and the mode of administration can be a barrier to treatment (78, 93, 94), and the IV ribavirin can only be obtained through an FDA Emergency Investigationa New Drug (EIND) application. Alternatively, oral ribavirin has been used in high-risk adult patients with RSV infection and has shown similar outcomes to aerosolized ribavirin in HCT recipients and immunocompromised patients (79, 93, 95–97). Considering its lower cost and ease of administration, oral ribavirin is a potential alternative for selected candidates. The safety profile often limits its use; hemolytic anemia, nephrotoxicity, drug rash, lactic acidosis, and altered mental status have been described with oral ribavirin. In addition, a boxed warning exists regarding the teratogenic effects of ribavirin observed in animal studies. Pregnancy should be avoided during and for 6 months after treatment in both female patients and the female partners of male patients treated with ribavirin (98–100).
Similar to influenza, the recommendation is to identify SARS-CoV-2 early in immunocompromised patients to provide prompt treatment before progression to COVID-19. Patients with hematologic malignancies are considered to be at a high risk for progression, and antiviral therapy should be considered in the HCT candidates. Ritonavir-boosted nirmatrelvir (Paxlovid) has an FDA EUA for treatment of non-hospitalized, high-risk adolescents greater than 12 years of age and weighing greater than or equal to 40 kg (77). In a randomized control trial of adults at risk for severe COVID-19, the EPIC-HR trial found an 89% relative risk reduction in COVID-19-related hospitalization or all-cause mortality in subjects receiving Paxlovid compared to placebo (101). A separate European study of patients with hematologic malignancies showed decreased mortality with Paxlovid use (102). However, Paxlovid has several drug-drug interactions due to ritonavir being a strong cytochrome P450 (CYP) 3A4 inhibitor; therefore, a thorough review of the patient's medication history is needed to assess potential changes, modifications, or discontinuation of certain drugs while receiving therapy (77). In reference to case 3, the patient was on voriconazole, which is also a CYP3A4 inhibitor, but based on the NIH guidelines, it is not a contraindication for Paxlovid administration (77). Given the oral formulation and the widespread availability of Paxlovid in local pharmacies, the patient was given Paxlovid for ease of administration and to avoid further hospital visits.
Remdesivir is a nucleotide prodrug of an adenosine analog that binds to viral RNA-dependent RNA polymerase and inhibits viral replication. It is approved by the FDA for treatment of COVID-19 in pediatric patients older than 28 days and weighing greater than or equal to 3 kg. In the PINETREE trial, patients at high risk for progression, including patients with hematologic malignancies, that received remdesivir had a decreased risk for hospitalization within 14 days after infection; however, there were no deaths reported in either the placebo or remdesivir group at 28 days post infection (103). As an alternative to Paxlovid, especially in patients with drug-drug interactions, remdesivir can be administered intravenously in the outpatient setting on 3 consecutive days; however, this may be logistically difficult in low-resource settings.
For high-risk children (i.e., immunocompromised) 12–18 years of age hospitalized for COVID-19, remdesivir should considered. If these patients require oxygen, remdesivir should be given for 5 days or until hospital discharge, whichever comes first. However, treatment course may be extended for up to 5 additional days (total duration of 10 days) (77). Dexamethasone is indicated when oxygen supplementation is needed or with increasing respiratory requirements (high flow, non-invasive ventilation, mechanical ventilation, or ECMO). The use of baricitinib may be an alternative for patients in whom steroids are not feasible. If there are concerns for a dysregulated immune/inflammatory response, then biologics, such as baricitinib or tocilizumab, can be considered for children older than 2 years of age (77).
Previously, several monoclonal antibodies have been used for outpatient treatment of mild SARS-CoV-2 infections in children ≥12 years and older, but with the currently circulating variants, there is no available monoclonal antibody for neither treatment nor pre-exposure prophylaxis.
In a 2014 guideline, the Infectious Diseases Society of America recommends the inactivated influenza vaccine (IIV) for children older than 6 months of age with hematologic and solid organ malignancies, except in patients receiving anti B-cell antibodies or intensive chemotherapy due to low vaccine response in these populations (104). However, HCT candidates and those receiving intensive chemotherapy are at increased risk for complications related to influenza; therefore, given the seasonality of influenza and the low side effect profile of IIV in cancer patients, IIV may be considered to provide some adaptive immunity against seasonal influenza. Given the low response to the vaccine, some institutions require 2 doses at least 28 days apart, in this population (105). Vaccination is recommended for all family members, close contacts, and healthcare workers who care for immunocompromised children.
Chemoprophylaxis with NAIs is recommended for any child at high risk for influenza complications after close contact with an influenza positive patient or during an outbreak, regardless of vaccination status (76). Chemoprophylaxis with NAIs should be started within 48 h of exposure for 7 day duration (76). However, given the risk for poor outcomes in this population, prophylaxis should be considered even if beyond 48 h from exposure.
Palivizumab is a humanized monoclonal antibody against the RSV fusion (F) glycoprotein, which has been in the market since 1998 for high-risk infants and young children. However, it requires costly, monthly injection during RSV season. The discovery of RSV pre-fusion F structure unveiled an epitope site targeted by neutralization antibodies and has been the target of current RSV vaccines and alternative therapies.
Nirsevimab is a novel monoclonal antibody that targets the RSV pre-fusion glycoprotein and lasts 6 months after one intramuscular injection. Studies in preterm and immunocompetent infants showed lower rates of RSV LRTI in the nirsevimab group compared to placebo (106). As of July 2023, the FDA has approved nirsevimab in infants born during or entering their first RSV season and in children up to 24 months of age who remain vulnerable to severe RSV disease through their second RSV season, including immunocompromised children undergoing HCT (107). The MUSIC study evaluated the safety and tolerability for nirsevimab in immunocompromised children. It was an open label phase 2b clinical trial involving 100 participants. Serious adverse events were uncommon and no medically attended RSV-LRTI was observed during the study period (108).
Currently, there are two RSV vaccines available for adults greater than 60 years of age, one of which is also available for pregnant people. However, none of these are available for children. Further studies are needed to evaluate the efficacy of RSV vaccines in pediatric HCT candidates and recipients.
There are three approved FDA SARS-CoV-2 vaccines in children. The mRNA vaccines from Pfizer/BioNTech and Moderna are approved for children 6 months of age or older, and the protein subunit vaccine from Novavax is approved for children ≥12 years of age. The efficacy of these vaccines has varied in immunocompetent children (109, 110). There is limited data on vaccine immunogenicity in immunocompromised and pre-HCT children, but in a study of immunocompromised adults, there were lower rates of seroconversion in HCT and solid organ recipients (111). Despite the lower vaccine efficacy in immunocompromised patients, vaccination of all cancer patients and HCT candidates and recipients older than 6 months of age as well as all family members and close contacts should be considered. Updated boosters targeting the Omicron XBB.1.5 subvariant have been developed, authorized, and recommended. For the latest up to date guidance on updated vaccines, please refer to the CDC recommendations (110). There are no pre-exposure prophylaxis agents for SARS-CoV-2 approved in the US at the time of this publication.
The COVID-19 pandemic has provided valuable lessons for the transplant infectious diseases community. Identifying patients at risk for progression to severe disease from a respiratory virus and providing appropriate care can prevent hospitalization and decrease mortality. The rapid implementation of the SARS-CoV-2 vaccine and the development of therapies (monoclonal antibodies and antivirals) have likely saved many immunocompromised children's lives. However, the same advancements are needed for other respiratory viruses and identifying risk factors as well as biomarkers for progression to severe disease is necessary. Additionally, further multicenter studies and randomized control trials that include immunocompromised children are needed to allow for more equitable, data-driven recommendations in this vulnerable population, especially in regard to pre-HCT RVIs.
SK: Conceptualization, Writing – original draft, Writing – review & editing. AW: Conceptualization, Writing – original draft, Writing – review & editing. DH: Conceptualization, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
AW reports grant support from Ansun Biopharma, Allovir, GSK, Vir, and Pfizer and is an Advisory Board Member for Vir.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Anak S, Atay D, Unuvar A, Garipardic M, Agaoglu L, Ozturk G, et al. Respiratory syncytial virus infection outbreak among pediatric patients with oncologic diseases and/or Bmt. Pediatr Pulmonol. (2010) 45(3):307–11. doi: 10.1002/ppul.21184
2. Kim YJ, Guthrie KA, Waghmare A, Walsh EE, Falsey AR, Kuypers J, et al. Respiratory syncytial virus in hematopoietic cell transplant recipients: factors determining progression to lower respiratory tract disease. J Infect Dis. (2014) 209(8):1195–204. doi: 10.1093/infdis/jit832
3. Ogimi C, Greninger AL, Waghmare AA, Kuypers JM, Shean RC, Xie H, et al. Prolonged shedding of human coronavirus in hematopoietic cell transplant recipients: risk factors and viral genome evolution. J Infect Dis. (2017) 216(2):203–9. doi: 10.1093/infdis/jix264
4. Waghmare A, Campbell AP, Xie H, Seo S, Kuypers J, Leisenring W, et al. Respiratory syncytial virus lower respiratory disease in hematopoietic cell transplant recipients: viral RNA detection in blood, antiviral treatment, and clinical outcomes. Clin Infect Dis. (2013) 57(12):1731–41. doi: 10.1093/cid/cit639
5. Waghmare A, Xie H, Kimball L, Yi J, Ozkok S, Leisenring W, et al. Supplemental oxygen-free days in hematopoietic cell transplant recipients with respiratory syncytial virus. J Infect Dis. (2017) 216(10):1235–44. doi: 10.1093/infdis/jix390
6. Carr S, Ilyushina NA, Franks J, Adderson EE, Caniza M, Govorkova EA, et al. Oseltamivir-resistant influenza a and B viruses pre- and postantiviral therapy in children and young adults with cancer. Pediatr Infect Dis J. (2011) 30(4):284–8. doi: 10.1097/INF.0b013e3181ff863b
7. Kim YJ, Waghmare A, Kuypers JM, Jerome KR, Pergam SA, Xie H, et al. Impact of pretransplant respiratory virus detection through universal screening in children undergoing hematopoietic cell transplantation (HCT). Biol Blood Marrow Transplant. (2017) 23(3):S190–1. doi: 10.1016/j.bbmt.2016.12.370
8. Srinivasan A, Gu Z, Smith T, Morgenstern M, Sunkara A, Kang G, et al. Prospective detection of respiratory pathogens in symptomatic children with cancer. Pediatr Infect Dis J. (2013) 32(3):e99–104. doi: 10.1097/INF.0b013e31827bd619
9. Kim YJ, Waghmare A, Xie H, Holmberg L, Pergam SA, Jerome KR, et al. Respiratory viruses in hematopoietic cell transplant candidates: impact of preexisting lower tract disease on outcomes. Blood Adv. (2022) 6(18):5307–16. doi: 10.1182/bloodadvances.2021004915
10. Peck AJ, Corey L, Boeckh M. Pretransplantation respiratory syncytial virus infection: impact of a strategy to delay transplantation. Clin Infect Dis. (2004) 39(5):673–80. doi: 10.1086/422994
11. Peck AJ, Englund JA, Kuypers J, Guthrie KA, Corey L, Morrow R, et al. Respiratory virus infection among hematopoietic cell transplant recipients: evidence for asymptomatic parainfluenza virus infection. Blood. (2007) 110(5):1681–8. doi: 10.1182/blood-2006-12-060343
12. Hirsch HH, Martino R, Ward KN, Boeckh M, Einsele H, Ljungman P. Fourth European conference on infections in leukaemia (ECIL-4): guidelines for diagnosis and treatment of human respiratory syncytial virus, parainfluenza virus, metapneumovirus, rhinovirus, and coronavirus. Clin Infect Dis. (2013) 56(2):258–66. doi: 10.1093/cid/cis844
13. Ottaviano G, Lucchini G, Breuer J, Furtado-Silva JM, Lazareva A, Ciocarlie O, et al. Delaying haematopoietic stem cell transplantation in children with viral respiratory infections reduces transplant-related mortality. Br J Haematol. (2020) 188(4):560–9. doi: 10.1111/bjh.16216
14. de Lima CR, Mirandolli TB, Carneiro LC, Tusset C, Romer CM, Andreolla HF, et al. Prolonged respiratory viral shedding in transplant patients. Transpl Infect Dis. (2014) 16(1):165–9. doi: 10.1111/tid.12167
15. Gooskens J, Jonges M, Claas EC, Meijer A, Kroes AC. Prolonged influenza virus infection during lymphocytopenia and frequent detection of drug-resistant viruses. J Infect Dis. (2009) 199(10):1435–41. doi: 10.1086/598684
16. Lehners N, Tabatabai J, Prifert C, Wedde M, Puthenparambil J, Weissbrich B, et al. Long-term shedding of influenza virus, parainfluenza virus, respiratory syncytial virus and nosocomial epidemiology in patients with hematological disorders. PLoS One. (2016) 11(2):e0148258. doi: 10.1371/journal.pone.0148258
17. Chemaly RF, Hanmod SS, Rathod DB, Ghantoji SS, Jiang Y, Doshi A, et al. The characteristics and outcomes of parainfluenza virus infections in 200 patients with leukemia or recipients of hematopoietic stem cell transplantation. Blood (2012) 119(12):2738–45; quiz 969. doi: 10.1182/blood-2011-08-371112
18. Choi SM, Boudreault AA, Xie H, Englund JA, Corey L, Boeckh M. Differences in clinical outcomes after 2009 influenza A/H1N1 and seasonal influenza among hematopoietic cell transplant recipients. Blood. (2011) 117(19):5050–6. doi: 10.1182/blood-2010-11-319186
19. Ghosh S, Champlin R, Couch R, Englund J, Raad I, Malik S, et al. Rhinovirus infections in myelosuppressed adult blood and marrow transplant recipients. Clin Infect Dis. (1999) 29(3):528–32. doi: 10.1086/598627
20. Hutspardol S, Essa M, Richardson S, Schechter T, Ali M, Krueger J, et al. Significant transplantation-related mortality from respiratory virus infections within the first one hundred days in children after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. (2015) 21(10):1802–7. doi: 10.1016/j.bbmt.2015.06.015
21. Piñana JL, Tridello G, Xhaard A, Wendel L, Montoro J, Vazquez L, et al. Upper and/or lower respiratory tract infection caused by human metapneumovirus after allogeneic hematopoietic stem cell transplantation. J Infect Dis. (2023):1–12. doi: 10.1093/infdis/jiad268. [Epub ahead of print].
22. Seo S, Campbell AP, Xie H, Chien JW, Leisenring WM, Englund JA, et al. Outcome of respiratory syncytial virus lower respiratory tract disease in hematopoietic cell transplant recipients receiving aerosolized ribavirin: significance of stem cell source and oxygen requirement. Biol Blood Marrow Transplant. (2013) 19(4):589–96. doi: 10.1016/j.bbmt.2012.12.019
23. Seo S, Xie H, Campbell AP, Kuypers JM, Leisenring WM, Englund JA, et al. Parainfluenza virus lower respiratory tract disease after hematopoietic cell transplant: viral detection in the lung predicts outcome. Clin Infect Dis. (2014) 58(10):1357–68. doi: 10.1093/cid/ciu134
24. Shah DP, Shah PK, Azzi JM, Chemaly RF. Parainfluenza virus infections in hematopoietic cell transplant recipients and hematologic malignancy patients: a systematic review. Cancer Lett. (2016) 370(2):358–64. doi: 10.1016/j.canlet.2015.11.014
25. Shah JN, Chemaly RF. Management of RSV infections in adult recipients of hematopoietic stem cell transplantation. Blood. (2011) 117(10):2755–63. doi: 10.1182/blood-2010-08-263400
26. Campbell AP, Guthrie KA, Englund JA, Farney RM, Minerich EL, Kuypers J, et al. Clinical outcomes associated with respiratory virus detection before allogeneic hematopoietic stem cell transplant. Clin Infect Dis. (2015) 61(2):192–202. doi: 10.1093/cid/civ272
27. Kim YJ, Boeckh M, Englund JA. Community respiratory virus infections in immunocompromised patients: hematopoietic stem cell and solid organ transplant recipients, and individuals with human immunodeficiency virus infection. Semin Respir Crit Care Med. (2007) 28(2):222–42. doi: 10.1055/s-2007-976494
28. Mahony JB. Detection of respiratory viruses by molecular methods. Clin Microbiol Rev. (2008) 21(4):716–47. doi: 10.1128/cmr.00037-07
29. Mahony JB, Petrich A, Smieja M. Molecular diagnosis of respiratory virus infections. Crit Rev Clin Lab Sci. (2011) 48(5–6):217–49. doi: 10.3109/10408363.2011.640976
30. Rand KH, Rampersaud H, Houck HJ. Comparison of two multiplex methods for detection of respiratory viruses: FilmArray RP and xTAG RVP. J Clin Microbiol. (2011) 49(7):2449–53. doi: 10.1128/jcm.02582-10
31. Hammond SP, Gagne LS, Stock SR, Marty FM, Gelman RS, Marasco WA, et al. Respiratory virus detection in immunocompromised patients with FilmArray respiratory panel compared to conventional methods. J Clin Microbiol. (2012) 50(10):3216–21. doi: 10.1128/jcm.00538-12
32. Hayden RT, Yan X, Wick MT, Rodriguez AB, Xiong X, Ginocchio CC, et al. Factors contributing to variability of quantitative viral PCR results in proficiency testing samples: a multivariate analysis. J Clin Microbiol. (2012) 50(2):337–45. doi: 10.1128/jcm.01287-11
33. Popowitch EB, O'Neill SS, Miller MB. Comparison of the biofire filmarray rp, genmark esensor rvp, luminex Xtag Rvpv1, and luminex Xtag rvp fast Multiplex assays for detection of respiratory viruses. J Clin Microbiol. (2013) 51(5):1528–33. doi: 10.1128/jcm.03368-12
34. Salez N, Vabret A, Leruez-Ville M, Andreoletti L, Carrat F, Renois F, et al. Evaluation of four commercial multiplex molecular tests for the diagnosis of acute respiratory infections. PLoS One. (2015) 10(6):e0130378. doi: 10.1371/journal.pone.0130378
35. Caliendo AM. Multiplex PCR and emerging technologies for the detection of respiratory pathogens. Clin Infect Dis. (2011) 52(Suppl 4):S326–30. doi: 10.1093/cid/cir047
36. Hayden RT, Gu Z, Rodriguez A, Tanioka L, Ying C, Morgenstern M, et al. Comparison of two broadly multiplexed PCR systems for viral detection in clinical respiratory tract specimens from immunocompromised children. J Clin Virol. (2012) 53(4):308–13. doi: 10.1016/j.jcv.2011.12.020
37. Torres JP, De la Maza V, Kors L, Villarroel M, Piemonte P, Izquierdo G, et al. Respiratory viral infections and coinfections in children with cancer, fever and neutropenia: clinical outcome of infections caused by different respiratory viruses. Pediatr Infect Dis J. (2016) 35(9):949–54. doi: 10.1097/inf.0000000000001209
38. Hayden RT, Gu Z, Ingersoll J, Abdul-Ali D, Shi L, Pounds S, et al. Comparison of droplet digital PCR to real-time PCR for quantitative detection of cytomegalovirus. J Clin Microbiol. (2013) 51(2):540–6. doi: 10.1128/JCM.02620-12
39. Hayden RT, Sun Y, Tang L, Procop GW, Hillyard DR, Pinsky BA, et al. Progress in quantitative viral load testing: variability and impact of the who quantitative international standards. J Clin Microbiol. (2017) 55(2):423–30. doi: 10.1128/jcm.02044-16
40. Hayden RT, Tang L, Su Y, Cook L, Gu Z, Jerome KR, et al. Impact of fragmentation on commutability of Epstein-Barr virus and cytomegalovirus quantitative standards. J Clin Microbiol. (2019) 58(1):1–22. doi: 10.1128/jcm.00888-19
41. Aranha C, Patel V, Bhor V, Gogoi D. Cycle threshold values in RT-PCR to determine dynamics of SARS-CoV-2 viral load: an approach to reduce the isolation period for COVID-19 patients. J Med Virol. (2021) 93(12):6794–7. doi: 10.1002/jmv.27206
42. Camargo JF, Lin RY, Komanduri KV. Lack of correlation between the SARS-CoV-2 cycle threshold [C(T)] value and clinical outcomes in patients with COVID-19. J Med Virol. (2021) 93(10):6059–62. doi: 10.1002/jmv.27171
43. Fox-Lewis A, Fox-Lewis S, Beaumont J, Drinković D, Harrower J, Howe K, et al. SARS-CoV-2 viral load dynamics and real-time RT-PCR cycle threshold interpretation in symptomatic non-hospitalised individuals in New Zealand: a multicentre cross sectional observational study. Pathology. (2021) 53(4):530–5. doi: 10.1016/j.pathol.2021.01.007
44. Lee LYW, Rozmanowski S, Pang M, Charlett A, Anderson C, Hughes GJ, et al. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infectivity by viral load, S gene variants and demographic factors, and the utility of lateral flow devices to prevent transmission. Clin Infect Dis. (2022) 74(3):407–15. doi: 10.1093/cid/ciab421
45. Waudby-West R, Parcell BJ, Palmer CNA, Bell S, Chalmers JD, Siddiqui MK. The association between SARS-CoV-2 RT-PCR cycle threshold and mortality in a community cohort. Eur Respir J. (2021) 58(1):1–3. doi: 10.1183/13993003.00360-2021
46. Schnuriger A, Perrier M, Marinho V, Michel Y, Saloum K, Boukli N, et al. Caution in interpretation of SARS-CoV-2 quantification based on RT-PCR cycle threshold value. Diagn Microbiol Infect Dis. (2021) 100(3):115366. doi: 10.1016/j.diagmicrobio.2021.115366
47. Rhoads D, Peaper DR, She RC, Nolte FS, Wojewoda CM, Anderson NW, et al. College of American Pathologists (CAP) microbiology committee perspective: caution must be used in interpreting the cycle threshold (Ct) value. Clin Infect Dis. (2021) 72(10):e685–6. doi: 10.1093/cid/ciaa1199
48. Poon KS, Wen-Sim Tee N. Caveats of reporting cycle threshold values from severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) qualitative polymerase chain reaction assays: a molecular diagnostic laboratory perspective. Clin Infect Dis. (2021) 73(9):e2851–2. doi: 10.1093/cid/ciaa1399
49. IDSA and AMP joint statement on the use of SARS-CoV-2 PCR cycle threshold (Ct) values for clinical decision-making: infectious diseases Society of America and Association for molecular pathology. (2021). Available at: https://www.idsociety.org/globalassets/idsa/public-health/covid-19/idsa-amp-statement.pdf (Cited 2022 April 4th, 2022).
50. AACC recommendation for reporting SARS-CoV-2 cycle threshold (Ct) values: the American Association for Clinical Chemistry (AACC). (2021). Available at: https://www.aacc.org/science-and-research/covid-19-resources/statements-on-covid-19-testing/aacc-recommendation-for-reporting-sars-cov-2-cycle-threshold-ct-values (Cited 2022 April 4th).
51. Nichols WG, Corey L, Gooley T, Davis C, Boeckh M. Parainfluenza virus infections after hematopoietic stem cell transplantation: risk factors, response to antiviral therapy, and effect on transplant outcome. Blood. (2001) 98(3):573–8. doi: 10.1182/blood.v98.3.573
52. Milano F, Campbell AP, Guthrie KA, Kuypers J, Englund JA, Corey L, et al. Human rhinovirus and coronavirus detection among allogeneic hematopoietic stem cell transplantation recipients. Blood. (2010) 115(10):2088–94. doi: 10.1182/blood-2009-09-244152
53. Ogimi C, Xie H, Leisenring WM, Kuypers JM, Jerome KR, Campbell AP, et al. Initial high viral load is associated with prolonged shedding of human rhinovirus in allogeneic hematopoietic cell transplant recipients. Biol Blood Marrow Transplant. (2018) 24(10):2160–3. doi: 10.1016/j.bbmt.2018.07.006
54. Tabatabai J, Schnitzler P, Prifert C, Schiller M, Weissbrich B, von Lilienfeld-Toal M, et al. Parainfluenza virus infections in patients with hematological malignancies or stem cell transplantation: analysis of clinical characteristics, nosocomial transmission and viral shedding. PLoS One. (2022) 17(7):e0271756. doi: 10.1371/journal.pone.0271756
55. Chemaly RF, Shah DP, Boeckh MJ. Management of respiratory viral infections in hematopoietic cell transplant recipients and patients with hematologic malignancies. Clin Infect Dis. (2014) 59(Suppl 5):S344–51. doi: 10.1093/cid/ciu623
56. Anton A, Lopez-Iglesias AA, Tortola T, Ruiz-Camps I, Abrisqueta P, Llopart L, et al. Selection and viral load kinetics of an oseltamivir-resistant pandemic influenza A (H1N1) virus in an immunocompromised patient during treatment with neuraminidase inhibitors. Diagn Microbiol Infect Dis. (2010) 68(3):214–9. doi: 10.1016/j.diagmicrobio.2010.08.003
57. Couturier BA, Bender JM, Schwarz MA, Pavia AT, Hanson KE, She RC. Oseltamivir-resistant influenza a 2009 H1N1 virus in immunocompromised patients. Influenza Other Respir Viruses. (2010) 4(4):199–204. doi: 10.1111/j.1750-2659.2010.00144.x
58. Fraaij PL, Schutten M, Javouhey E, Burleigh L, Outlaw R, Kumar D, et al. Viral shedding and susceptibility to oseltamivir in hospitalized immunocompromised patients with influenza in the influenza resistance information study (IRIS). Antiviral Ther. (2015) 20(6):633–42. doi: 10.3851/imp2957
59. Hamada N, Imamura Y, Hara K, Kashiwagi T, Imamura Y, Nakazono Y, et al. Intrahost emergent dynamics of oseltamivir-resistant virus of pandemic influenza A (H1N1) 2009 in a fatally immunocompromised patient. J Infect Chemother. (2012) 18(6):865–71. doi: 10.1007/s10156-012-0429-0
60. Renaud C, Pergam SA, Polyak C, Jain R, Kuypers J, Englund JA, et al. Early emergence of an H275Y mutation in a hematopoietic cell transplant recipient treated with intravenous peramivir. Transpl Infect Dis. (2010) 12(6):513–7. doi: 10.1111/j.1399-3062.2010.00582.x
61. van der Vries E, Stittelaar KJ, van Amerongen G, Veldhuis Kroeze EJ, de Waal L, Fraaij PL, et al. Prolonged influenza virus shedding and emergence of antiviral resistance in immunocompromised patients and ferrets. PLoS Pathog. (2013) 9(5):e1003343. doi: 10.1371/journal.ppat.1003343
62. Weinstock DM, Gubareva LV, Zuccotti G. Prolonged shedding of multidrug-resistant influenza a virus in an immunocompromised patient. N Engl J Med. (2003) 348(9):867–8. doi: 10.1056/nejm200302273480923
63. Champlin RE, Whimbey E. Community respiratory virus infections in bone marrow transplant recipients: the M.D. Anderson cancer center experience. Biol Blood Marrow Transplant. (2001) 7 (Suppl):8s–10. doi: 10.1053/bbmt.2001.v7.pm11777103
64. Chu HY, Englund JA, Podczervinski S, Kuypers J, Campbell AP, Boeckh M, et al. Nosocomial transmission of respiratory syncytial virus in an outpatient cancer center. Biol Blood Marrow Transplant. (2014) 20(6):844–51. doi: 10.1016/j.bbmt.2014.02.024
65. Garcia R, Raad I, Abi-Said D, Bodey G, Champlin R, Tarrand J, et al. Nosocomial respiratory syncytial virus infections: prevention and control in bone marrow transplant patients. Infect Control Hosp Epidemiol. (1997) 18(6):412–6. doi: 10.1086/647640
66. Geis S, Prifert C, Weissbrich B, Lehners N, Egerer G, Eisenbach C, et al. Molecular characterization of a respiratory syncytial virus outbreak in a hematology unit in Heidelberg, Germany. J Clin Microbiol. (2013) 51(1):155–62. doi: 10.1128/jcm.02151-12
67. Greninger AL, Zerr DM, Qin X, Adler AL, Sampoleo R, Kuypers JM, et al. Rapid metagenomic next-generation sequencing during an investigation of hospital-acquired human parainfluenza virus 3 infections. J Clin Microbiol. (2017) 55(1):177–82. doi: 10.1128/jcm.01881-16
68. Houlihan CF, Frampton D, Ferns RB, Raffle J, Grant P, Reidy M, et al. Use of whole-genome sequencing in the investigation of a nosocomial influenza virus outbreak. J Infect Dis. (2018) 218(9):1485–9. doi: 10.1093/infdis/jiy335
69. Jones BL, Clark S, Curran ET, McNamee S, Horne G, Thakker B, et al. Control of an outbreak of respiratory syncytial virus infection in immunocompromised adults. J Hosp Infect. (2000) 44(1):53–7. doi: 10.1053/jhin.1999.0666
70. Kassis C, Champlin RE, Hachem RY, Hosing C, Tarrand JJ, Perego CA, et al. Detection and control of a nosocomial respiratory syncytial virus outbreak in a stem cell transplantation unit: the role of palivizumab. Biol Blood Marrow Transplant. (2010) 16(9):1265–71. doi: 10.1016/j.bbmt.2010.03.011
71. Lehners N, Schnitzler P, Geis S, Puthenparambil J, Benz MA, Alber B, et al. Risk factors and containment of respiratory syncytial virus outbreak in a hematology and transplant unit. Bone Marrow Transplant. (2013) 48(12):1548–53. doi: 10.1038/bmt.2013.94
72. Zhu Y, Zembower TR, Metzger KE, Lei Z, Green SJ, Qi C. Investigation of respiratory syncytial virus outbreak on an adult stem cell transplant unit by use of whole-genome sequencing. J Clin Microbiol. (2017) 55(10):2956–63. doi: 10.1128/jcm.00360-17
73. Waghmare A, Englund JA, Boeckh M. How I treat respiratory viral infections in the setting of intensive chemotherapy or hematopoietic cell transplantation. Blood. (2016) 127(22):2682–92. doi: 10.1182/blood-2016-01-634873
74. Tomblyn M, Chiller T, Einsele H, Gress R, Sepkowitz K, Storek J, et al. Guidelines for preventing infectious complications among hematopoietic cell transplantation recipients: a global perspective. Biol Blood Marrow Transplant. (2009) 15(10):1143–238. doi: 10.1016/j.bbmt.2009.06.019
75. Mowrer C, Lee BR, Goyal R, Selvarangan R, Schuster JE. Outcome of children with rhinovirus detection prior to allogeneic hematopoietic cell transplant. Pediatr Transplant. (2018) 22(8):e13301. doi: 10.1111/petr.13301
76. Committee on Infectious D. Recommendations for prevention and control of influenza in children, 2023–2024. Pediatrics. (2023) 152(4):1–29. doi: 10.1542/peds.2023-063773
77. Coronavirus disease 2019 (COVID-19) treatment guidelines. National Institutes of Health. Available at: https://www.covid19treatmentguidelines.nih.gov/ (Cited 2023 October 23).
78. Dallas RH, Rains JK, Wilder K, Humphrey W, Cross SJ, Ghafoor S, et al. The Aerogen(®) solo is an alternative to the small particle aerosol generator (SPAG-2) for administration of inhaled ribavirin. Pharmaceutics. (2020) 12(12):1–6. doi: 10.3390/pharmaceutics12121163
79. Gorcea CM, Tholouli E, Turner A, Saif M, Davies E, Battersby E, et al. Effective use of oral ribavirin for respiratory syncytial viral infections in allogeneic haematopoietic stem cell transplant recipients. J Hosp Infect. (2017) 95(2):214–7. doi: 10.1016/j.jhin.2016.11.012
80. Uyeki TM, Bernstein HH, Bradley JS, Englund JA, File TM, Fry AM, et al. Clinical practice guidelines by the infectious diseases society of America: 2018 update on diagnosis, treatment, chemoprophylaxis, and institutional outbreak management of seasonal influenzaa. Clin Infect Dis. (2019) 68(6):895–902. doi: 10.1093/cid/ciy874
81. Casper C, Englund J, Boeckh M. How I treat influenza in patients with hematologic malignancies. Blood. (2010) 115(7):1331–42. doi: 10.1182/blood-2009-11-255455
82. Fiore AE, Fry A, Shay D, Gubareva L, Bresee JS, Uyeki TM, et al. Antiviral agents for the treatment and chemoprophylaxis of influenza — recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. (2011) 60(1):1–24. doi: 10.15585/mmwr.mm6626a7
83. Baker J, Block SL, Matharu B, Burleigh Macutkiewicz L, Wildum S, Dimonaco S, et al. Baloxavir marboxil single-dose treatment in influenza-infected children: a randomized, double-blind, active controlled phase 3 safety and efficacy trial (miniSTONE-2). Pediatr Infect Dis J. (2020) 39(8):700–5. doi: 10.1097/INF.0000000000002747
84. Taieb V, Ikeoka H, Wojciechowski P, Jablonska K, Aballea S, Hill M, et al. Efficacy and safety of baloxavir marboxil versus neuraminidase inhibitors in the treatment of influenza virus infection in high-risk and uncomplicated patients—a Bayesian network meta-analysis. Curr Med Res Opin. (2021) 37(2):225–44. doi: 10.1080/03007995.2020.1839400
85. Influenza antiviral drug baloxavir marboxil. Centers for Disease Control and Prevention, National Center for Immunization and Respiratory Diseases (NCIRD). Available at: https://www.cdc.gov/flu/treatment/baloxavir-marboxil.htm (Cited 2023 October 23).
86. Angelidakis G, Khawaja F, Mulanovich VE, Dailey-Garnes N, Ariza-Heredia E, Chemaly RF. Combination of baloxavir and oseltamivir for treatment of severe influenza infection in hematopoietic cell transplant recipients: a novel treatment strategy for a high-risk population. Microbes Infect. (2022) 24(3):104895. doi: 10.1016/j.micinf.2021.104895
87. Harada N, Shibata W, Koh H, Takashita E, Fujisaki S, Okamura H, et al. Successful treatment with baloxavir marboxil of a patient with peramivir-resistant influenza A/H3N2 with a dual E119D/R292K substitution after allogeneic hematopoietic cell transplantation: a case report. BMC Infect Dis. (2020) 20(1):478. doi: 10.1186/s12879-020-05205-1
88. Salvatore M, Laplante JM, Soave R, Orfali N, Plate M, van Besien K, et al. Baloxavir for the treatment of influenza in allogeneic hematopoietic stem cell transplant recipients previously treated with oseltamivir. Transpl Infect Dis. (2020) 22(4):e13336. doi: 10.1111/tid.13336
89. Kumar D, Ison MG, Mira JP, Welte T, Hwan Ha J, Hui DS, et al. Combining baloxavir marboxil with standard-of-care neuraminidase inhibitor in patients hospitalised with severe influenza (flagstone): a randomised, parallel-group, double-blind, placebo-controlled, superiority trial. Lancet Infect Dis. (2022) 22(5):718–30. doi: 10.1016/S1473-3099(21)00469-2
90. Ventre K, Randolph A. Ribavirin for respiratory syncytial virus infection of the lower respiratory tract in infants and young children. Cochrane Database Syst Rev. (2004) 4:CD000181. doi: 10.1002/14651858.CD000181.pub2
91. Tejada S, Martinez-Reviejo R, Karakoc HN, Pena-Lopez Y, Manuel O, Rello J. Ribavirin for treatment of subjects with respiratory syncytial virus-related infection: a systematic review and meta-analysis. Adv Ther. (2022) 39(9):4037–51. doi: 10.1007/s12325-022-02256-5
92. Chemaly RF, Aitken SL, Wolfe CR, Jain R, Boeckh MJ. Aerosolized ribavirin: the most expensive drug for pneumonia. Transpl Infect Dis. (2016) 18(4):634–6. doi: 10.1111/tid.12551
93. Englund JA, Piedra PA, Ahn YM, Gilbert BE, Hiatt P. High-dose, short-duration ribavirin aerosol therapy compared with standard ribavirin therapy in children with suspected respiratory syncytial virus infection. J Pediatr. (1994) 125(4):635–41. doi: 10.1016/s0022-3476(94)70026-5
94. Chemaly RF, Torres HA, Munsell MF, Shah DP, Rathod DB, Bodey GP, et al. An adaptive randomized trial of an intermittent dosing schedule of aerosolized ribavirin in patients with cancer and respiratory syncytial virus infection. J Infect Dis. (2012) 206(9):1367–71. doi: 10.1093/infdis/jis516
95. Foolad F, Aitken SL, Shigle TL, Prayag A, Ghantoji S, Ariza-Heredia E, et al. Oral versus aerosolized ribavirin for the treatment of respiratory syncytial virus infections in hematopoietic cell transplant recipients. Clin Infect Dis. (2019) 68(10):1641–9. doi: 10.1093/cid/ciy760
96. Trang TP, Whalen M, Hilts-Horeczko A, Doernberg SB, Liu C. Comparative effectiveness of aerosolized versus oral ribavirin for the treatment of respiratory syncytial virus infections: a single-center retrospective cohort study and review of the literature. Transpl Infect Dis. (2018) 20(2):e12844. doi: 10.1111/tid.12844
97. Stamouli M, Tsonis I, Gkirkas K, Economopoulou C, Siafakas N, Pournaras S, et al. Oral ribavirin is a highly effective treatment for lower respiratory tract infections due to respiratory syncytial virus or parainfluenza after allogeneic stem cell transplantation. Bone Marrow Transplant. (2021) 56(2):511–3. doi: 10.1038/s41409-020-01022-x
98. Park SY, Baek S, Lee SO, Choi SH, Kim YS, Woo JH, et al. Efficacy of oral ribavirin in hematologic disease patients with paramyxovirus infection: analytic strategy using propensity scores. Antimicrob Agents Chemother. (2013) 57(2):983–9. doi: 10.1128/aac.01961-12
99. Marcelin JR, Wilson JW, Razonable RR. Oral ribavirin therapy for respiratory syncytial virus infections in moderately to severely immunocompromised patients. Transpl Infect Dis. (2014) 16(2):242–50. doi: 10.1111/tid.12194
100. Chakrabarti S, Collingham KE, Holder K, Fegan CD, Osman H, Milligan DW. Pre-emptive oral ribavirin therapy of paramyxovirus infections after haematopoietic stem cell transplantation: a pilot study. Bone Marrow Transplant. (2001) 28(8):759–63. doi: 10.1038/sj.bmt.1703216
101. Hammond J, Leister-Tebbe H, Gardner A, Abreu P, Bao W, Wisemandle W, et al. Oral nirmatrelvir for high-risk, nonhospitalized adults with COVID-19. N Engl J Med. (2022) 386(15):1397–408. doi: 10.1056/NEJMoa2118542
102. Salmanton-Garcia J, Marchesi F, Gomes da Silva M, Farina F, Davila-Valls J, Bilgin YM, et al. Nirmatrelvir/ritonavir in COVID-19 patients with haematological malignancies: a report from the epicovideha registry. EClinicalMedicine. (2023) 58:101939. doi: 10.1016/j.eclinm.2023.101939
103. Gottlieb RL, Vaca CE, Paredes R, Mera J, Webb BJ, Perez G, et al. Early remdesivir to prevent progression to severe COVID-19 in outpatients. N Engl J Med. (2022) 386(4):305–15. doi: 10.1056/NEJMoa2116846
104. Rubin LG, Levin MJ, Ljungman P, Davies EG, Avery R, Tomblyn M, et al. 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin Infect Dis. (2014) 58(3):309–18. doi: 10.1093/cid/cit816
105. Hijano DR, Maron G, Hayden RT. Respiratory viral infections in patients with cancer or undergoing hematopoietic cell transplant. Front Microbiol. (2018) 9:3097. doi: 10.3389/fmicb.2018.03097
106. Hammitt LL, Dagan R, Yuan Y, Baca Cots M, Bosheva M, Madhi SA, et al. Nirsevimab for prevention of RSV in healthy late-preterm and term infants. N Engl J Med. (2022) 386(9):837–46. doi: 10.1056/NEJMoa2110275
107. FDA approves new drug to prevent RSV in babies and toddlers. U. S. Food and Drug Administration. Available at: https://www.fda.gov/news-events/press-announcements/fda-approves-new-drug-prevent-rsv-babies-and-toddlers (Updated July 17, 2023; Cited 2023 October 23).
108. Evaluate the safety and tolerability, for nirsevimab in immunocompromised children (music). Available at: https://clinicaltrials.gov/study/NCT04484935?intr=Nirsevimab&rank=1#locations (Cited 2023 October 23).
109. Waghmare A, Hijano DR. SARS-CoV-2 infection and COVID-19 in children. Clin Chest Med. (2023) 44(2):359–71. doi: 10.1016/j.ccm.2022.11.014
110. National Center for Immunization and Respiratory Diseases (NCIRD). Stay up to date with COVID-19 vaccines. Center for Disease Control and Prevention. Available at: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/stay-up-to-date.html#recommendations (Cited 2023 November 2).
111. Bergman P, Blennow O, Hansson L, Mielke S, Nowak P, Chen P, et al. Safety and efficacy of the mRNA Bnt162b2 vaccine against SARS-CoV-2 in five groups of immunocompromised patients and healthy controls in a prospective open-label clinical trial. EBioMedicine. (2021) 74:103705. doi: 10.1016/j.ebiom.2021.103705
Keywords: respiratory virus, children, immunocompromised, cancer, hematopoietic cell transplant
Citation: Kim SR, Waghmare A and Hijano DR (2024) Approach to hematopoietic cell transplant candidates with respiratory viral detection. Front. Pediatr. 11:1339239. doi: 10.3389/fped.2023.1339239
Received: 15 November 2023; Accepted: 19 December 2023;
Published: 18 January 2024.
Edited by:
Monica I. Ardura, Nationwide Children’s Hospital, United StatesReviewed by:
Desiree Caselli, Azienda Ospedaliero Universitaria Consorziale Policlinico di Bari, Italy© 2024 Kim, Waghmare and Hijano. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Diego R. Hijano ZGllZ28uaGlqYW5vQHN0anVkZS5vcmc=
Abbreviations RV, respiratory virus; RVIs, respiratory viral infections; ADV, adenovirus; HMPV, human metapneumovirus; PIV, parainfluenza virus; RSV, respiratory syncytial virus; CoVs, seasonal coronaviruses; HRV, human rhinovirus; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; COVID-19, coronavirus disease; FDA, Food and Drug Administration; HCT, hematopoietic cell transplant; Ct, cycle threshold; PCR, polymerase chain reaction; RT-PCR, real time polymerase chain reaction; ALL, acute lymphoblastic leukemia; EUA, emergency use authorization; AMR, analytical measurement range; ICU, intensive Care Unit; BAL, bronchoalveolar lavage; CDC, Centers for Disease Control and Prevention.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.