 María Salcedo-Perez-Juana1
María Salcedo-Perez-Juana1 Domingo Palacios-Ceña1*
Domingo Palacios-Ceña1* Ana San-Martín-Gómez1Ángel Aledo-Serrano2,†
Ana San-Martín-Gómez1Ángel Aledo-Serrano2,† Lidiane Lima Florencio3,†
Lidiane Lima Florencio3,†
- 1Research Group of Humanities and Qualitative Research in Health Science (Hum&QRinHS), Department of Physical Therapy, Occupational Therapy, Physical Medicine and Rehabilitation, Universidad Rey Juan Carlos, Madrid, Spain
- 2Epilepsy and Neurogenetics Programme, Vithas Madrid La Milagrosa University Hospital, Vithas Hospital Group, Madrid, Spain
- 3Research Group of Manual Therapy, Dry Needling and Therapeutic Exercise (GITM-URJC), Department of Physical Therapy, Occupational Therapy, Physical Medicine and Rehabilitation, Universidad Rey Juan Carlos, Madrid, Spain
Background: Developmental and Epileptic Encephalopathies (DEEs) occur in childhood and are associated with severe epileptic seizures and neurological impairment. The aim of this study was to combine quantitative and qualitative methodologies to comprehensively describe factors related to quality of life, impact on the family and psychosocial factors in parents of children with TSC, STXBP1 and SYNGAP1 variants.
Methods: A convergent parallel mixed design including parents of children with DEE. In the cross-sectional study, 20 parents (10STXBP1, five SYNGAP1, five TSC) were given questionnaires on quality of life, impact on the family and psychological factors. In the descriptive qualitative study, in-depth interviews were conducted with 18 parents (nine STXBP1, five TSC, four SYNGAP1) using a semi-structured questionnaire. A thematic analysis was carried out. The results of the two studies were combined by showing similarities and differences through tables, figures, accounts, and joint displays.
Results: In terms of quality of life, the integrated results were consistent in highlighting the importance of family interaction, although in the qualitative section the influence of the relationship between the children's siblings, the relationship with health professionals and the difficulties in obtaining public aid were highlighted. In terms of impact, the integrated results show that the illness has a significant impact on the family; the financial burden is highlighted, and the experience of the illness is discussed in depth. Finally, the psychological aspects, symptoms such as anxiety, stress and strain, were consistent. Most of the participants reported sleep disturbance, as identified in the questionnaire, although not mentioned in the interviews.
Conclusions: The combined results of the mixed method provide an in-depth analysis of the impact of DEEs on parents of children with STXBP1, SYNGAP1 and TSC.
1. Introduction
Developmental and Epileptic Encephalopathies (DEEs) are a group of rare diseases that present in childhood, with severe and difficult-to-treat epileptic seizures associated with learning difficulties, behavioral problems, and motor impairment (1–3). These diseases are also associated with high mortality and morbidity (3). In recent years, genetic variants in epilepsy have been identified, such as STXBP1, SYNGAP1, tuberous sclerosis complex 1 and 2 (TSC), SCN1A, KCNQ2, CDKL5, GNAO1, PCDH19, SHANK3 and Dup 15, which cause genetic epilepsy with onset in the first three years of life (4).
Severe epileptic seizures and neurodevelopmental problems (cognitive, motor) are common in DEEs, however, symptoms and their response to treatment vary (1, 2). For example, the STXBP1 variant has a very early onset, with refractory seizures, movement disorders and severe learning disabilities (4). TSC is characterized by early-onset epilepsy with associated neurodevelopmental problems, and the SYNGAP1 variant presents with refractory myoclonic seizures, absences, and varying degrees of autism spectrum disorder (4, 5). This variability in symptoms and their management has a major impact on the parents and families of children with DEEs (6, 7). Children affected by DEEs and their families experience difficulties with diagnosis and genetic identification, carer burden, and financial and social difficulties related to the disability (6, 7). These difficulties in caring for children with DEEs cause significant physical (exhaustion), mental (stress, anxiety, insomnia) and social (lack of resources) strain on parents, which can lead to health problems and reduced quality of life (6, 8–12). The European Commission, through the European Joint Programme on Rare Diseases (13), and the Orphanet network initiative (14) for rare diseases, has highlighted the need for further research into the diagnosis, treatment, and impact of rare diseases on patients, their families, and their social environment.
Therefore, the aims of this mixed methods research were to: describe the quality of life, family impact and psychosocial factors of parents of children with TSC, STXBP1 and SYNGAP1 variants; describe their experiences on these dimensions; and combine the findings to gain a better and broader understanding of the impact of the illness from the parents' perspective. To the best of our knowledge, this is the first study to attempt to describe the impact of DEE on parents of children with TSC, STXBP1 and SYNGAP1 using mixed methods research to analyze the impact of DEE from the parents' perspective.
2. Material and methods
2.1. Design
A convergent (concurrent) parallel mixed methods approach was used (15–17) (Table 1, Supplementary File S1). This included a quantitative (QUAN) observational cross-sectional study and a qualitative (QUAL) descriptive study, with data collection and analysis of both methods conducted simultaneously. The aim of a mixed methods research is to provide in-depth and contextualized answers to health science questions, by combining different approaches to overcome the limitations of a single method or methodological perspective (18). Previous studies (19–22) have demonstrated the use of mixed methods research to analyze the experiences of parents of children with rare neurodegenerative diseases such as MPS IIIA and Dravet (11, 20), to improve the health care and assessment of children with TSC (21, 23), and to assess the management and support of families with children with spinal muscular atrophy (19, 22).
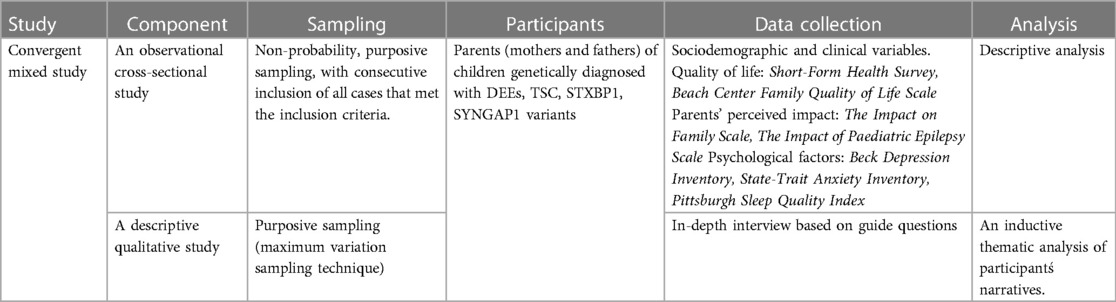
Table 1. Convergent (concurrent) parallel mixed method study summary.
Five researchers (three women) participated in this study, including one researcher nurse (DPC), three physiotherapists (LLF, MSPJ, ASMG), and one neurologist (AASN). None were involved in clinical activity, nor did they have any prior relationship with the patients included. Two researchers (ASMG, AAS) had clinical experience with DEEs. The National Institutes of Health guidelines for mixed methods research in health sciences were followed (24). In addition, the observational study followed the STROBE recommendations (25), and the qualitative study followed the SRQR and COREQ recommendations (26, 27).
2.2. Observational cross-sectional study (QUAN)
Cross-sectional studies are observational in nature and provide a snapshot of the characteristics of the study subjects at a single point in time. However, they do not have a follow-up period and cannot provide a cause-effect relationship (25).
2.2.1. Sample and eligibility criteria
Parents of children with the TSC, STXBP1 and SYNGAP1 variants were recruited from the respective associations in Spain. Participants were recruited and assessed between February 2023 and July 2023.
As DEEs are rare diseases, the number of cases of each of the variants in Spain is low and/or may be underdiagnosed (28). In Spain, the most recent estimation of prevalence is 1906 for TSC (29), 20 for STBX1 (30) and 38 for SYNGAP1 (31). Non-probability convenience sampling was used, with consecutive inclusion of all available individuals who met the inclusion criteria.
Inclusion criteria: (a) Parents (mothers and fathers) of children diagnosed (with genetic diagnosis) with TSC, STXBP1, SYNGAP1 variants; (b) Parents of children with DEEs (afore mentioned variants) aged between 4 and 10 years (both included); (c) Parents living in Spain and belonging to one of the following patient associations: Asociación española de esclerosis tuberosa, Asociación del síndrome STXBP1 and Asociación SYNGAP1 España.
Exclusion criteria: (a) Parents who did not wish to participate in the study; (b) Parents of children with DEEs with different genetic variants; (c) Parents of an affected child who was undergoing an acute medical process that required hospital admission during the study; d) Parents of a child who did not present epileptic seizures in the previous month.
2.2.2. Sociodemographic and clinical variables
The sociodemographic variables were age and sex of the parent, parent's educational level, number of children, age, and sex of the son/daughter, affected gene, age of onset of epileptic seizures, time to diagnosis. The following clinical variables were recorded: active epilepsy (seizures in the last 3 months), hospital admission (last year), number of visits to the hospital emergency department (last year), conduct disorder, and number of current anti-epileptic drugs.
2.2.3. Quality of life
The Short-Form Health Survey (SF-12-v2) was used to assess parents' perceived quality of life (32, 33). This scale has 12 items assessing physical and mental health over the past 4 weeks, with scores ranging from 0 (worst) to 100 (best). Scores < 50 for the mental and physical components were considered below the norm for the general Spanish population (32).
The Beach Center Family Quality of Life (BCFQOL) Scale (34, 35), one of the most widely used scales in children with disabilities (36), was used to assess the family's quality of life. It consists of 25 items with five subscales: Family Interaction; Parenting; Emotional Wellbeing; Physical/Material Wellbeing; and Disability. The mean of the total item scores is obtained for each factor, on a Likert scale from 1 (very dissatisfied) to 5 (very satisfied). Higher scores indicate a better quality of life for the family.
2.2.4. Parental perceived impact
The impact of the illness on the family was assessed using the Impact on Family Scale questionnaire (37, 38), which consists of 24 items with a 4-point Likert scale response. Four subscales are included: family/social impact (items 1–9, 9–36 points); personal impact (items 10–15; 6–24 points); experience of the illness (items 16–20; 5–20 points) and financial burden (items 21–24: 4–16 points). The score for each subscale can be reported separately or as an overall impact score (24–96 points), with higher scores indicating lower impact.
The Impact of Paediatric Epilepsy Scale (IPES) (39, 40) was also used. This scale enables parents to rate the influence of epilepsy on the daily life and quality of life of the family and child, currently and over the past 3 months. It considers 11 areas: general health, relationships within and outside the family, number of activities, schoolwork, self-esteem, loss of hope and family activities. They are scored from “very much” (3 points) to “not at all” (0 points), with a range of 0 to 33 points. Higher scores indicate a greater impact.
2.2.5. Psychological factors
The Beck's Depression Inventory (BDI-II) (41, 42) and the State-Trait Anxiety Inventory (STAI) (43, 44) were used. The BDI-II consists of 21 questions to identify depression and is scored from 0 to 3 points. The final score determines the degree of depression identified: minimal (0–13 points), mild (14–19 points), moderate (20–28 points) and severe (29–63 points) (41, 42). The STAI assesses symptoms of anxiety with 40 items, with response options ranging from “not at all” to “very much” (from 0 to 3 points) (43, 44). The STAI is divided into two subscales, STAI-state and STAI-trait, with higher scores indicating greater state or trait anxiety.
The Pittsburgh Sleep Quality Index (PSQI) was also used (45, 46). It assesses sleep quality over 1 month and includes 19 items that form 7 component scores: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction. The sum of the scores for each component is converted into an overall score (0–21 points), with a higher score indicating poorer sleep quality. Scores of 5 points or more indicate poor sleep quality (45).
2.2.6. Analysis
The descriptive analysis of the data was carried out (by LLF, ASMG). As we could not confirm the normal distribution of all data (using histogram, normal Q–Q plots, and Shapiro-Wilk test); the continuous variables were described using the median and interquartile range or the frequency of observations. The variables have been described considering a total sample, understanding that they are parents of children with DEE, in addition to the description of the variables by subgroup of each genetic variant (TSC, STXBP1, SYNGAP1). No inferential analysis was performed due to the small sample size of the subgroups.
2.3. A qualitative study (QUAL)
A qualitative descriptive study was conducted (47). This type of qualitative design provides a rich description of the phenomenon of interest under study, informed by the experiences of the participants. Also, a descriptive qualitative study can help identify an event or critical situation (47).
2.3.1. Participants and sampling strategies
Inclusion/exclusion criteria were the same as for the observational study. In the present qualitative study, a purposive sampling approach was used (48) based on the maximum variation sampling technique (49). This technique is used when the researcher wants to (a) select a purposive sample that is as representative as possible of a broader group of cases or (b) make comparisons between different types of cases. In the present study, the criterion to ensure variation was the different genetic variants of DEEs. In qualitative research there are also a variety of proposals for justifying and determining sample size (50, 51). Furthermore, there is no formula for calculating the sample size in advance (47). Due to this variability of criteria and the unavailability of many cases of each variant, the authors established the sample size based on pragmatic considerations (difficulty accessing participants because it is a RD). As a result, all available cases of each variant were included to enrich the data.
2.3.2. Data collection
In-depth semi-structured interviews were conducted (48) with an open-ended follow-up question to collect the detailed descriptions (52). Table 2 Semi-structured interview question guide.
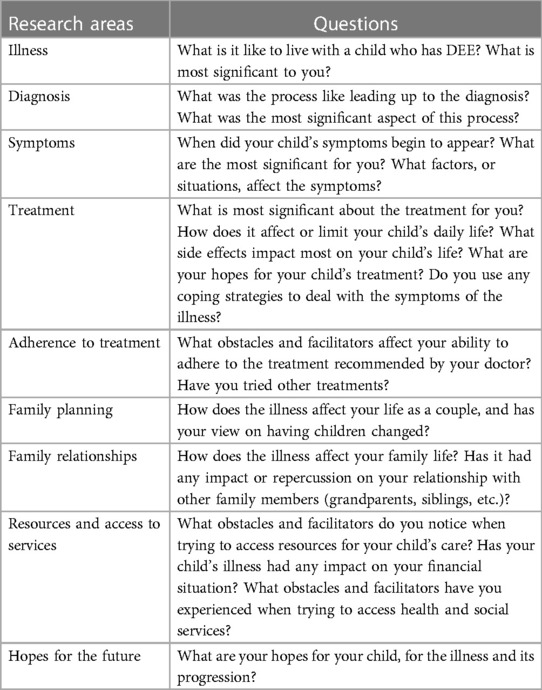
Table 2. Semi structured interview guide questions.
The interview question guide was developed based on previous studies concerning DEE (11, 12, 53–56) where a pilot test was conducted (52, 57). All interviews were conducted by two researchers (MSPJ and DPC), with experience in developing qualitative studies using in-depth interviews and not involved in the care of the participants' children. All interviews (n = 18; 9 STXBP1, 5 TSC, 4 SYNGAP1) were audio-recorded, recording a total of 1,632 min of interviews (the average duration of each interview was 90.67 min).
2.3.3. Data analysis
Inductive thematic analysis was used (47, 48, 58). Full transcriptions were made of each of the interviews. Thematic analysis consisted of identifying the most descriptive content to obtain meaningful units (codes), and then reducing and identifying the most common meaningful groups (categories) (47, 48, 58). Thus, groups of codes were formed, i.e., similar points or content that enabled the emergence of themes that offered a detailed perspective of the study participants. The analysis was carried out separately for each interview (by DPC, MSPJ). Joint team meetings were held to combine the results of the analysis. In the case of a divergence of opinion, the identification of the results was based on consensus among the members of the research team. For the analysis, Excel spreadsheets were used to organize and share the coding process. See Supplementary File S2 Data analysis and coding procedure.
2.3.4. Rigor
The application procedures used to control the trustworthiness of the qualitative study are described in Supplementary File S3. Trustworthiness criteria (59).
2.4. Integration procedure for quantitative and qualitative content
Data were integrated through a mixed concurrent design, where simultaneous data collection and analysis of the QUAN and QUAL studies were carried out (60), and the findings were interpreted and reported through accounts and joint displays (61–63). Data integration was performed after the analysis of each study by the four investigators (LLF, ASMG, DPC, MSPJ). The results of The QUAN and QUAL are reported in the same section and a table has been used for joint display of the data integration.
3. Results
The results are reported in the following order: (1) quantitative and qualitative results, and (2) mixed method findings (integration) (61–63). The accounts or narratives for each dimension studied, which explain the qualitative results, can be found in Supplementary File S4. Joint display of quotes organized by study dimensions.
3.1. Sociodemographic data
Twenty parents completed the questionnaires, and 18 parents participated in the interviews. The socio-demographic characteristics of the participants and the clinical characteristics of the children with DEE are shown in Table 3.
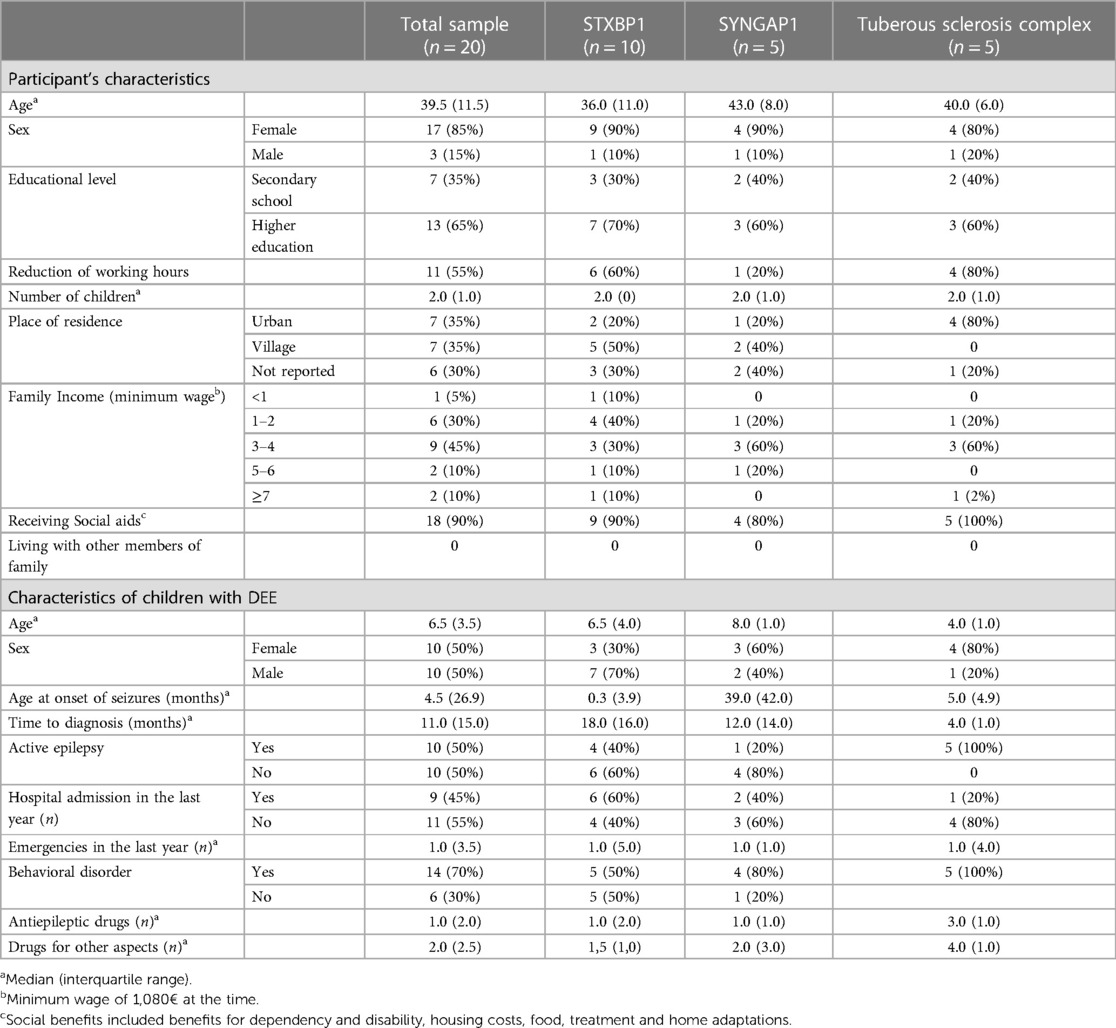
Table 3. Sociodemographic data of the parents of children with developmental and epileptic encephalopathy variants STXBP1 and SYNGAP1 and tuberous sclerosis complex and clinical variables of their child.
3.2. Quality of life
3.2.1. Quantitative data
The median of SF-12 scores for the whole sample is close to the cut-off point of the norm value of 50 for the general Spanish population in both components, however, the mental component of group of parents of children with SYNGAP1 and the physical and mental components for the TSC group are below this cut-off (Figure 1 and Supplementary File S5).
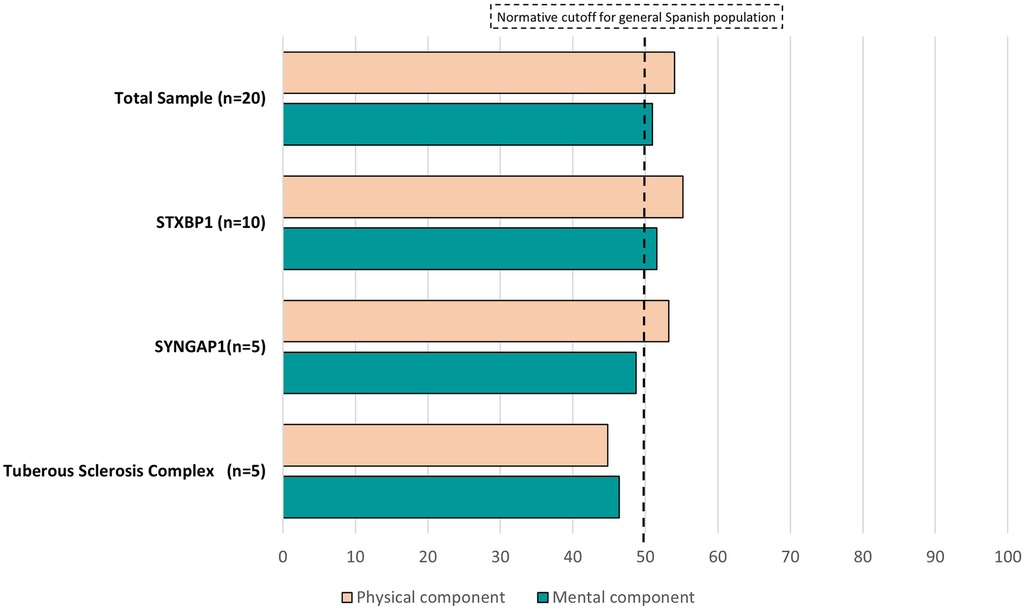
Figure 1. Quality of life, measured by the short-form health survey (SF-12), of the parents of children with developmental and epileptic encephalopathy variants STXBP1 and SYNGAP1 and tuberous sclerosis complex.
In terms of family quality of life, according to the BCFQOL, family interaction and disability-related support are the dimensions that participants rated as the most important, although there was an even distribution of importance across all dimensions (Figure 2A, Supplementary File S5). Also, participants were most satisfied with the family interaction and least satisfied with the emotional wellbeing dimensions (Figure 2B, Supplementary File S5).
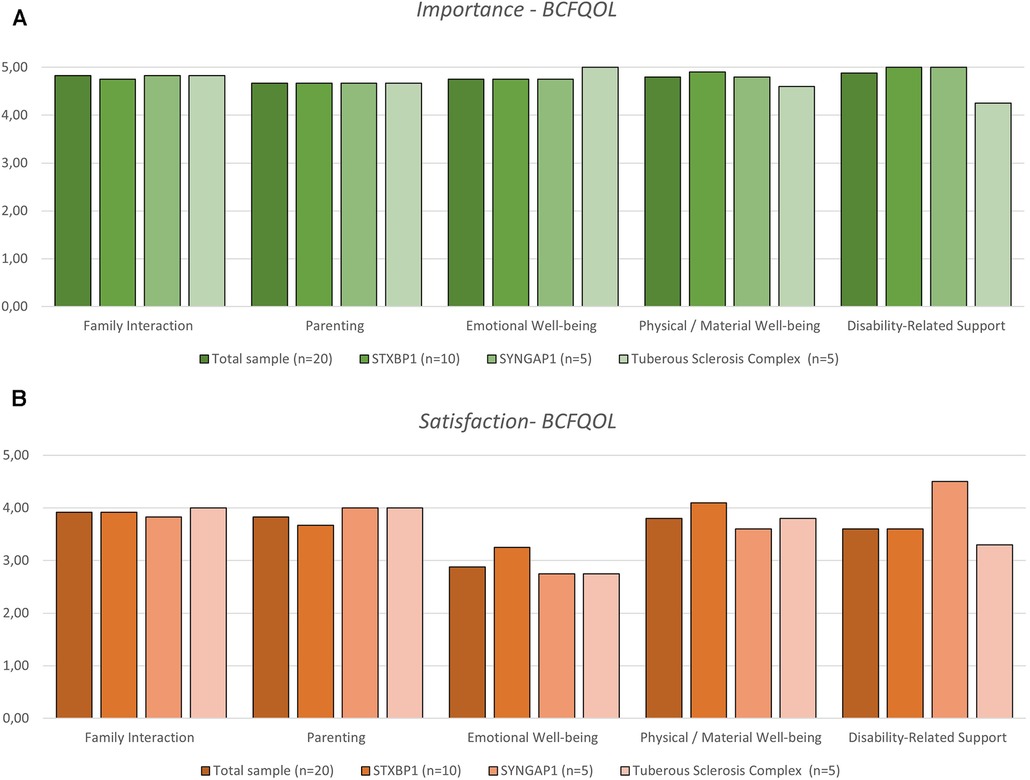
Figure 2. Family quality of life reported by the parents of children with developmental and epileptic encephalopathy variants STXBP1 and SYNGAP1 and tuberous sclerosis complex, measured by the beach center family quality of life (BCFQOL) scale. The parents’ perspective is divided by importance (A) and satisfaction (B) with each dimension of the scale.
3.2.2. Qualitative data
Qualitative interviews demonstrated the following contents regarding quality of life. Parents related that it was key to establish good relations within the family structure (parents-children) and to avoid the family rejecting their child. In all variants, there were cases of rejection (avoiding contact) or lack of understanding by the family (not recognizing the illness). For the parents, the remaining family (parents, siblings, grandparents, etc.) also had to experience their own grief, and take their own time to accept it. Conversely, there were also cases where the family was fully supportive and contributed towards the child's care. Moreover, it brings joy and relief to the parents when siblings accept the child with DEE; when they show love, support, and help; when there is a normal relationship; and when they know that they can count on the siblings in their absence.
All the parents rated the associations positively as a source of help and support, understanding, guidance and advice throughout the process.
There are positive experiences with professionals in all variants, however, most parents reported that the care should improve in terms of sensitivity and empathy of professionals, support for families, knowledge of the illness, concern for the children, and their difficulties. In children with SYNGAP1, parents considered that the process of obtaining a diagnosis should improve, together with the assessment of the information provided by parents about symptoms. This was especially the case when parents showed video recordings of epileptic seizures to professionals as evidence to support their claims. In TSC, parents felt that communication between professionals was lacking, also, they complained of insufficient follow-up of their children, the important role of the doctor as a guide for care, and the need to increase the time available for consultations, recommending that professionals should interact with children with DEE, and pay attention to them, not treat them like objects.
The obstacles identified by the parents included: restrictions on social assistance due to the lack of recognition of DEE as eligibility criterion, the high degree of bureaucracy, lack of information about resources, restricted access to buildings, waiting lists for public health care, and delays in care between specialists. In SYNGAP1, parents hired private professionals (physiotherapists, psychologists) and pointed out that children with learning and/or sensory disabilities had fewer opportunities. Some TSC cases highlighted the lack of coordination between public and private hospitals, which forced them to travel long distances to seek hospital help.
3.3. Impact on the family
3.3.1. Quantitative data
The median scores of the Impact on Family Scale are shown in Figure 3 and in Supplementary File S5. Proportionally, the subscales “experience with the illness” and “economic burden” were the most affected in the total sample. In the total score, the subgroup of parents of children with TSC had the highest impact.
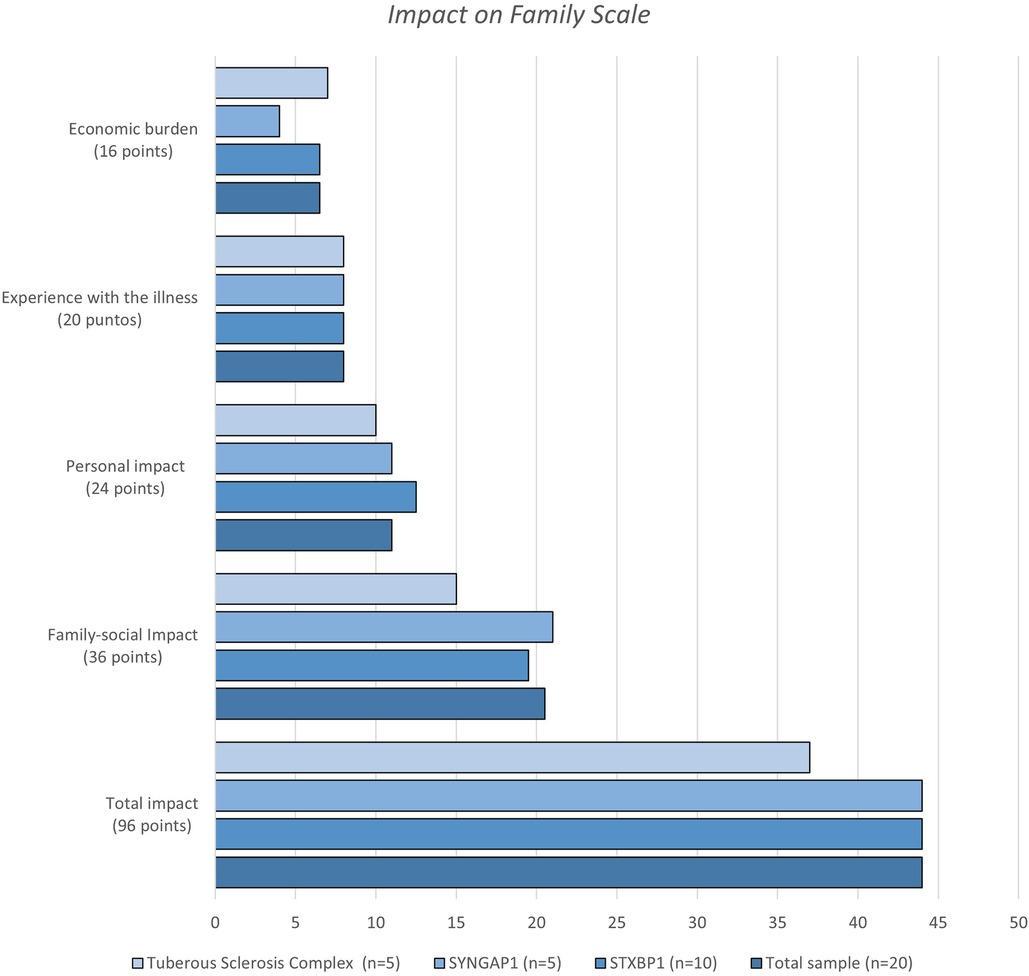
Figure 3. Impact of family scale scores of the parents of children with developmental and epileptic encephalopathy variants STXBP1 and SYNGAP1 and tuberous sclerosis complex.
Two participants answered “not applicable” to all 11 items of the Impact of Paediatric Epilepsy Scale and were not included in the descriptive analysis. The subgroup with the highest total score were the parents of children with TSC (Figure 4A, Supplementary File S5). For the total sample, the impact was higher in general health, number of activities and at school (Figure 4B). It is noteworthy that the low scores for self-esteem and loss of hope in the child are a result of the high rate of “not applicable” responses between 50%–55% of the sample for these two items.
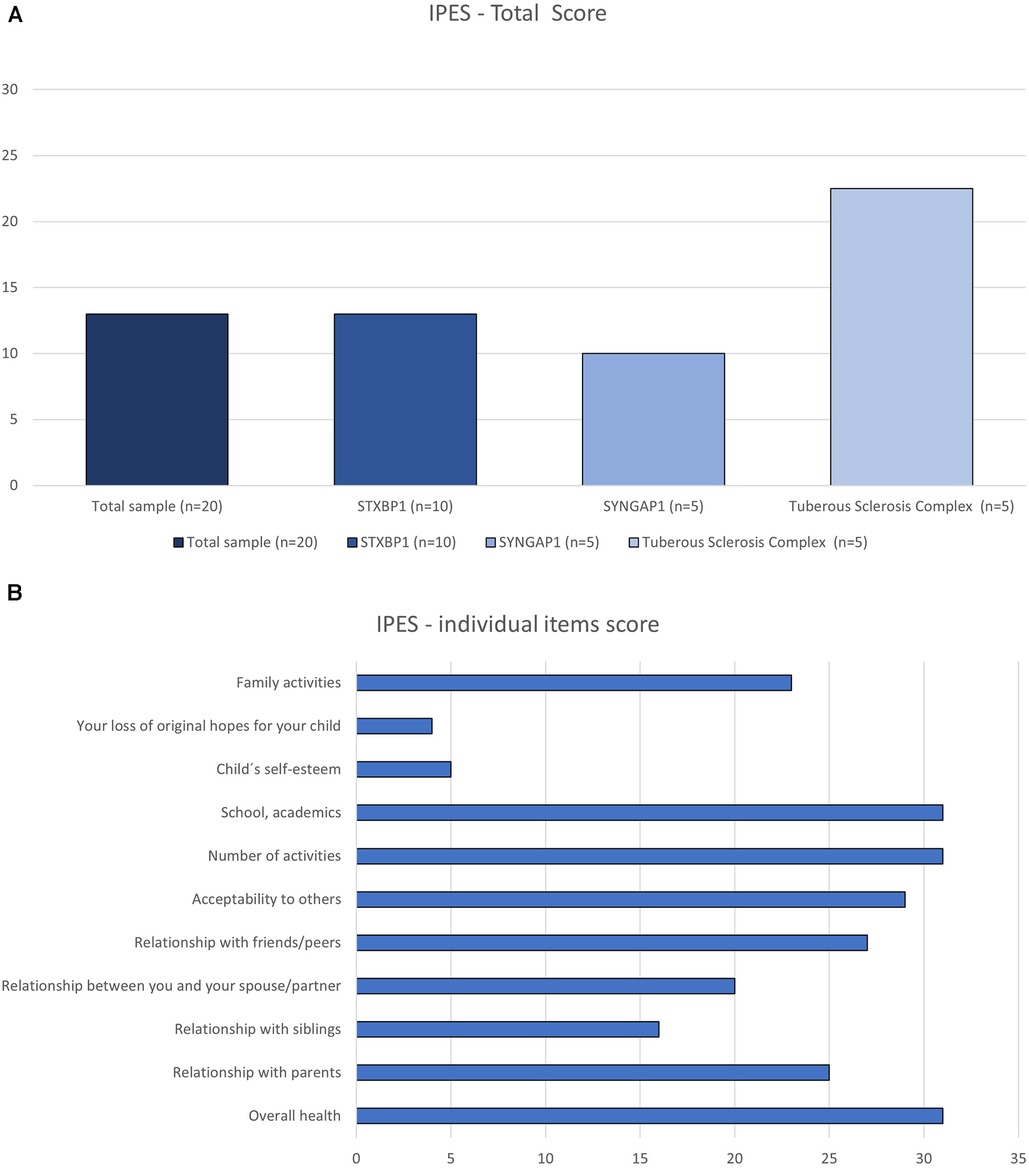
Figure 4. Impact of paediatric epilepsy scale (IPES) rated by the parents of children with developmental and epileptic encephalopathy variants STXBP1 and SYNGAP1 and tuberous sclerosis complex. Data is displayed as total score (A) and the sum of parents’ scores of each item on the scale (B).
3.3.2. Qualitative data
The main change brought about by the illness was that all the parents' time and attention was focused on the children. All family life (work, leisure, school) revolved around them. All children required constant monitoring for symptoms, however, there were some specific features; in STXBP1, parents highlighted the difficulty of managing the child physically, whereas in SYNGAP1 and TSC, parents highlighted the difficulty of managing behavior, with harsh reactions (shouting), violent (hitting, pinching), and angry behavior.
In all variants, there were changes in social relationships and friendships. In some cases, a lack of understanding of the illness led to distancing, while in others, the new family situation meant that they no longer attended social and/or fun gatherings.
In all variants, DEE also affected siblings. The main change was a reduction in time and activities shared with the parents. Nonetheless, there were also other consequences, such as psychological care for the siblings due to poor grief management, rejection, shame in being with the family, denial of responsibility for the care of the sibling with DEE in the future. However, other parents also found siblings to be supportive and helpful, mature, the most faithful and loving companions of the child with DEE. To lessen the responsibility on siblings, some parents (STXBP1) saved money to ensure the future care of their child with DEE and avoid becoming a financial burden on their siblings. Others reported the importance of ensuring that the child's siblings had their own space and life trajectory (TSC).
The parents of children with STXBP1 and SYNGAP1 variants reported difficulties in finding temporary carers to allow parents to perform other tasks and/or take a break. The reasons for this were: difficulty in managing children with DEE (“conduct disorder”), constant availability, lack of knowledge about the illness, and lack of training in managing epileptic seizures. In addition, some parents admitted that they found it difficult to leave their children in the care of others.
The parents talked about how they had learned to respect others, to appreciate the little things, to enjoy every moment and to be flexible in the face of unforeseen events.
There was conflict between the couple due to reduced time together, physical and mental exhaustion, and overload of care responsibilities. This led to distancing, stress, tension, and arguments. The participants reported how this phase could be overcome, resulting in a strengthening of the couple and a greater bond.
Regardless of the variant, some participants stated that they would consider having another child, while others clearly refused having another child. The reasons for having another child included: wanting to be a mother again, wanting a child without illness, wanting the child with DEE to have a carer in the future, and wanting a new lease of life. Conversely, reasons for not wanting to have another child were because they did not want to spend less time with their current children, because they did not have the time, because of a lack of money, and because they were afraid another child would have DEE again.
Financial burden appeared in all variants. Families paid for additional treatments (physiotherapy, occupational therapy), medicines, special diets (ketogenic diet), orthopedic products, home adaptations to cope and private consultations with medical specialists. In all variants, one of the parents had to ask for a reduction in working hours, in order to have time to care for their child, adding to the financial burden.
3.4. Psychological factors
3.4.1. Quantitative data
Table 4 displays the descriptive analysis of anxiety, depression, and sleep quality. Up to 40% of the participants presented at least mild signs of depression. Moreover, 75% had poor sleep quality. Parents of children with TSC presented a higher median score for the STAI-trait, BDI-II and the PSQI; whereas SYNGAP1 and STXBP1 subgroups presented more state-anxiety.

Table 4. Psychological aspects (anxiety, depression and sleep quality) of the parents of children with developmental and epileptic encephalopathy variants STXBP1 and SYNGAP1 and tuberous sclerosis complex.
3.4.2. Qualitative data
Many parents reported feeling anxious about their children's future as they grew older. In the SYNGAP1 subgroup, they worried that their child would become unmanageable, and that institutionalization would be considered. Parents acknowledged feelings of loneliness when they felt overwhelmed and overburdened by tasks (care, work, managing consultations, etc.). Parents experienced a constant feeling of uncertainty as the child's health can change suddenly. They live with stress because they cannot plan anything, and therefore they feel uncertain about the treatment, and are frustrated by their child's dependency. In some cases of TSC, parents described feeling tied down by the illness, even feeling like they were imprisoned. Many were continually exhausted by the constant vigilance their children required.
In all variants, there was no hope for the future, no goals, no long-term planning, living from day to day, focusing on daily achievements. They also described a period of prolonged mourning and/or grief, because of the impact of the illness and all the lost hopes and dreams. Parents in all variants described their experience as hard, painful, and intense, however, they acknowledged that certain rewarding moments of great happiness exist, related to the great love they feel towards their sick children, family togetherness and learning to cope with the illness together.
Parents of children with all variants experienced some sense of guilt. For example, when they must travel (for work) they feel that they are abandoning their children, or because they feel responsible for making their siblings live with the illness (STXBP1). When the children are in hospital and the parents go home to rest, or when they think that they may have been responsible for the illness (SYNGAP1). They also felt guilty when siblings had problems at school, or for not spending enough time with them (TSC). In extreme moments of feeling emotionally exhausted and in crisis, some parents wished their child would die because it would be a liberation. In these cases, this thought was accompanied by a strong sense of guilt. The emotions are so intense that, during a crisis, not only do parents wish their child were dead, they also become disconnected from their care and/or reject them. One participant (C3) described how life was unbearable when their child with SYNGAP1 shouted and hit them when he was angry. Another parent (B1) reported that there were times when they rejected their child with TSC, and at these times they were unable or unwilling to care for their child.
In all variants, reducing working hours to care for their children was a difficult decision, and was accompanied by anger, feelings of worthlessness, loss of job opportunities, and difficulty in accepting leaving work (STXBP1). Parents also experienced feelings of shame because they felt that they did not deserve their salary, together with frustration, and fear of being fired (TSC). In contrast, there were cases in STXBP1 and SYNGAP1 where the reduction in hours was experienced positively, as they had more time for their child and partner.
3.5. Mixed method findings (integration)
The results of the integration showed similarities and differences (56, 58, 59) between QUAL and QUAN results (Table 5).
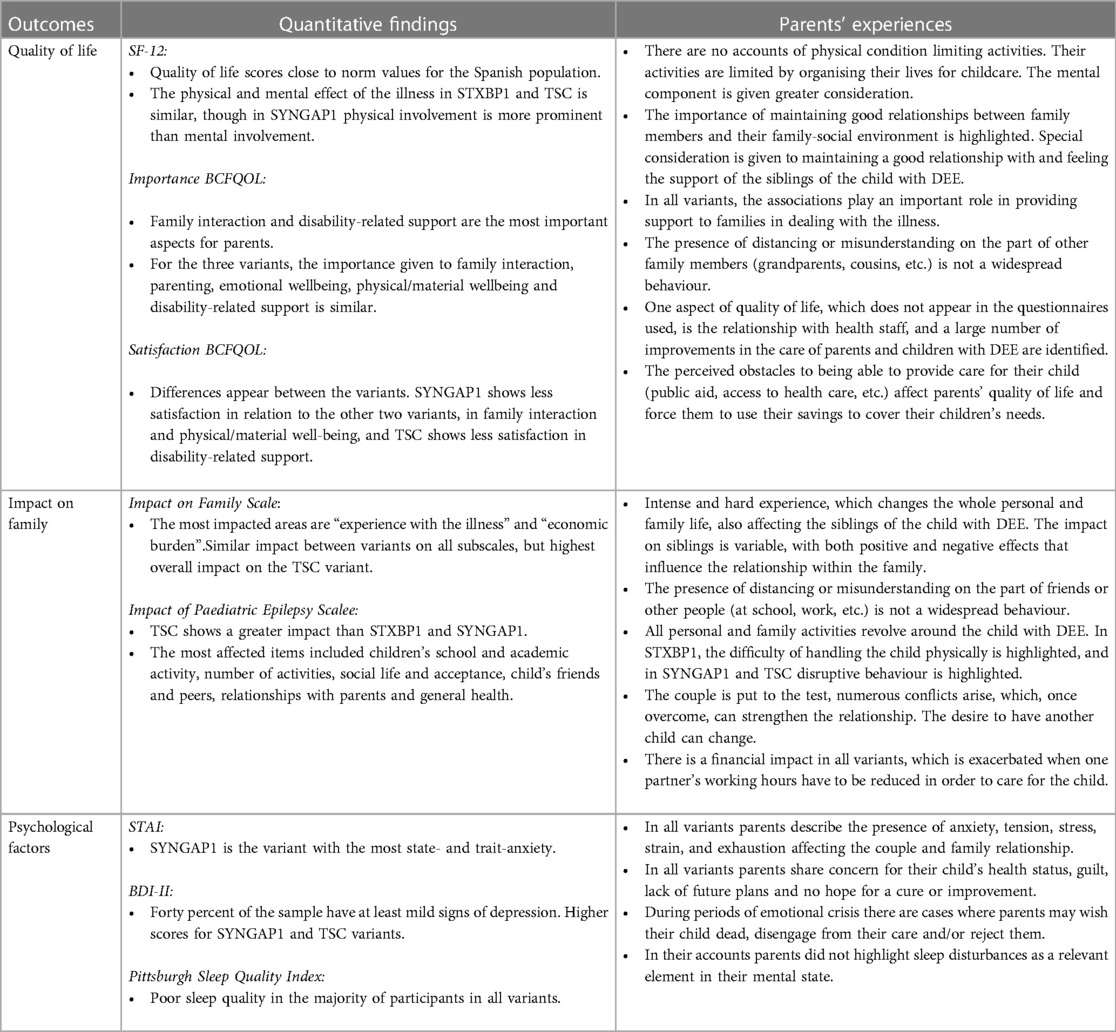
Table 5. Combined display of the quantitative and qualitative findings.
4. Discussion
This mixed-method study provides a broader, in-depth perspective of parents with DEE. (1) In terms of quality of life, our findings suggest that individual questionnaires may not properly reflect their experience and family quality of life may be more appropriate; however, none of the quantitative tools addressed aspects such as the experience with professionals and the role of the associations, which are aspects that emerged from the interviews. (2) Results of QUAN and QUAL studies about impact on the family dimension were convergent, affecting familýs time and financial burden. QUAL also highlights the parent`s concerns regarding the siblings and the decision to have another child. (3) Psychological aspects, such as anxiety, depression, stress, guilty, anger and feelings of worthlessness were identified. Moreover, QUAN results demonstrate high rates of sleep disorders that were not mentioned by the parents during the interviews. This integrative perspective has never been addressed before in parents of children with the variants studied.
4.1. Quality of life
Previous studies on DEEs (12, 53) have shown how parents' lives “stop” to focus on their children, and day-to-day life is a constant adaptation requiring parents to be alert.
Carers of children with TSC have lower health-related quality of life (HRQL) than the general population (64–67), spending an average of 104 h per week caring. The more time spent caring, the lower the family functioning (p = 0.01) and the lower their' HRQL (p = 0.03) (68). In addition, neuropsychiatric comorbidities in children with TSC were also associated with lower family functioning (p = 0.02) and carer HRQL (p < 0.01). This decrease in carer and family HRQL occurs because the daily routines of the entire family change as they focus on the needs of the sick child (65, 66), such as monitoring seizures, assessing risk of injury, managing disruptive behavior, and changing work shifts for medical appointments, affecting their daily planning or their social activities (8, 65, 66). Thus, carers need time for themselves to maintain their quality of life.
Our results show how the illness causes changes in relationships with family (grandparents, cousins, etc.). In DEEs, family relationships can be affected, with feelings of isolation, lack of support/understanding, and regular family crises (69, 70). Family of children with TSC reported that isolation allowed them to explore alternatives and/or to build a protective “glass dome” around the child (66). In other DEEs (70, 71), parents stopped attending family gatherings to avoid inappropriate looks or questions and lost contact with friends as well as ceasing to go on social outings.
The relationship with health professionals is not an item that appears in the quality of life and family impact questionnaires. Discrepancies in the treatment families expect from professionals may be due to professionals focusing on different aspects of the child's care than those expected by carers (72). Sullivan et al. (73) demonstrated how professionals prioritize motor and developmental delay, movement disorders and tremor in the care of children with STXBP1 over other problems (considered essential by carers) such as behavioral problems and nutrition. Similarly, in TSC, Zöllner et al. (72) showed that there were discrepancies in the prioritization of the management of psychiatric and neurological symptoms between physicians and carers. Previous studies (12, 54, 74) in DEEs have shown the importance of the relationship with the healthcare professional for parents. For parents of children with SCN1A, KCNQ2, CDKL5, PCDH19, and GNAO1, the relationship was negative when professionals prioritized bureaucracy, ignored information provided by the family, communicated without empathy, judged the quality of home care, did not relate to their children, and did not understand the illness (12).
The major role of support associations has already been reported in DEEs and rare diseases (70, 71, 75, 76) as they help and support families, act as a filter of information, allow sharing of experiences, and improve quality of life of families. However, access to associations should take place progressively to avoid information overload and stress. Graffigna et al. (66) described how families of children with TSC used the association as a primary form of support, information, and engagement with other families as they learned to accept their child's disability.
Our qualitative results showed obstacles for obtaining social support, which is in line with a previous report of parents of children with rare diseases and DEEs (55, 77–80). Bureaucracy is an ongoing struggle and parents feel powerless and sometimes forgotten by support providers (55, 79).
4.2. Impact on the family
The multiple symptoms and the disability associated with DEEs impact parents' lives in multiple ways. A conceptual model of the STXBP1 shows that the symptoms that most affected parents were developmental delay and behavioral problems, however, their emotions are also affected and their daily activities are limited (73). For carers of children with TSC, the most bothersome symptoms are the seizures, disruptive behavior, and cognitive problems (72). For SYNGAP1, most parents were concerned about language impairment, behavioral problems, lack of autonomy in their children, and increasing family and financial burden (81). Also, in SYNGAP1, parents struggled with distress-related behaviors in everyday life, where children displayed frustration and aggression when they were denied something, did not get their own way or were unable to understand the situation. Very often this aggression could lead to violence towards themselves or towards others (5).
Despite this situation, parents of this study and carers of children with other DEEs are able to experience happiness and joy, as well as learn from their children (53, 70, 72, 80, 82). This change in their outlook on life seems to be related to a better knowledge of the illness, its management, and their expectations, a process of readjustment in which they manage to reach an acceptable level of emotional well-being.
Nonetheless, living with these DEEs may negatively impact the couple's relationship, leading to separation and/or divorce (66). Caring for children with DEEs involves making decisions, changing roles, and limiting activities that provoke conflict in the couple and affect their sex life (6, 70). The key to strengthening the couple is communication, “team building”, respect, patience and recognizing that both partners are suffering (70). One source of conflict was the decision to have more children. Doubt about having another child is also seen in Phelan-McDermid syndrome (PMS) (53, 54), where the decision was accompanied by fear and uncertainty.
The reduction of working hours observed in our participants for all variants is a common strategy described among carers of children with TSC (65, 72), carers' professional careers and/or productivity is affected because they must leave work (resignation or dismissal) and/or reduce their working hours in order to care for their sick children. Consequently, there is an increase in the economic burden, which is already large considering the costs of orthopedic products, nappies, and arranging treatments (physiotherapy, occupational therapy) (54, 80, 83).
In the case of TSC, Zöllner et al. (72) described how children with cognitive impairment and severe forms of epilepsy have a higher risk of hospitalization, admission to intensive care units and undergo more diagnostic procedures than the rest of the population, regardless of the health care system. In addition, these children require more effort and many expenses must be met to cover rehabilitation, physiotherapy, and speech therapy. In terms of direct costs, a patient with TSC incurs an average total cost of £12,681 (PPP-$17,629) over a three-year period, compared to £4,777 (PPP-$6641) per patient in the general population. Previous studies on Dravet (84, 85), reported a mean direct and indirect cost of €6,043 and €4,399 per year, respectively. The most significant financial burden was associated with hospitalization, care services, and anti-epileptic drugs. In addition, the cost increased if the child had frequent seizures, hospitalizations, home visits, severe symptoms and/or required nursing care (84, 85).
4.3. Psychological factors
The findings highlight parents' despair and lack of hope for the future. Previous studies (86–90) have shown that managing “hope” in parents of children with rare neurological disorders should be a priority for healthcare professionals. Feelings of losing control, being “stuck in a maze” or “having no escape from the illness” have been reported in parents of children with TSC (73). Similarly, parents of children with PMS also had little hope for the future, their hopes were diminished, and they preferred to live from day to day (53).
In relation to TSC, carers show more depressive symptoms than the general population, understanding that neuropsychiatric disorders, behavioral problems, and seizures significantly increased parental stress (65, 72). Parents are anxious about the appearance of new symptoms and side effects of treatments and fearful about the future and the progression of symptom, especially if they are unable to care for their child or if they die (65, 66). These parents feel emotionally overwhelmed, overburdened by the intensity of care for psychiatric and neurological problems, and feel that they have scarce psychological support (72), Similar results were found for PMS, where thinking about the future of their child's care and leaving the responsibility of caring to the siblings caused parents distress (53).
Our results show differences between the sleep disturbance data from the questionnaire and the absence of parental accounts. Hesdorffer et al. (89) showed how caring for and continuously monitoring children with DEE affected sleep quality (aOR 95% CI, 1.7–2.6) and caused fatigue (aOR 95% CI, 1.5–2.2) in carers. Fatigue and poor sleep quality, in turn, increased carers' risk of anxiety (aOR 95% CI, 3.6–6.0) and depression (aOR 95% CI, 2.8–6.0). Gonçalves et al. (90) showed that carers of children with Dravet had a higher incidence of depression and anxiety compared to carers of other patients with epilepsy. These problems were associated with carer fatigue and sleep disturbance.
4.4. Strengths and limitations
The presence of multiple genetic variants and the small number of affected individuals were the main challenges of this study, which limited recruitment and consequently may limit the generalization of this study. Another possible limitation is that all participants were recruited from patient associations. This means that participants may have access to more support and information about managing the DEE disorders than families who are not engaged with the patient associations. Although these results should be treated with caution, the strength of this study is that it is the first study to describe the reality of parents of children with STXBP1, TSC and SYNGAP1, using a mixed methods approach with multiple data collection and analysis strategies to increase the depth and credibility of the findings (61, 91). The advantage of a mixed concurrent design is that it enables the integration of data of different natures simultaneously, unlike previous studies carried out with only one type of quantitative (7, 8) and/or qualitative methodology (12). An attempt to cover the objectives of the present study by conducting an observational study and a qualitative study separately, would mean that each method would present its own partial view of the results without integrating the responses to the questionnaires and the individual narrative perspective of the parents. This mixed concurrent design allows for a greater understanding of the phenomenon (having children with DEE) by being able to compare and identify similarities and differences in the responses and behaviors of parents of children with DEE using both qualitative and quantitative data simultaneously (15, 16). The simultaneity of the information is the advantage of using the concurrent mixed design to achieve our objective, since the sequential mixed designs (exploratory or explanatory), must first conduct a phase of the research (QUAN and/or QUAL) and achieve its objectives, to proceed with the next methodological phase, and finally integrate the data (15, 61, 91). In the exploratory approach, the second method (qualitative/quantitative) is needed to answer a research question within a larger quantitative or qualitative study. Moreover, explanatory sequential designs use the results of first method (usually qualitative) to inform the second method (identify variables, develop instrument-QUAN) (15).
In conclusion, our results help to analyze and compare the quality of life, the impact on the family and the self-perceived mental health of parents of children with TSC, STXBP1 and SYNGAP1, with their first-person narrated experiences. This study also identifies areas for improvement, differences among the questionnaires and helps to understand the context in which parents responded to the questionnaires. These results may help professionals to identify gaps in care and improve support and services for these families. These dimensions should be further studied in other genetic variants of DEEs. Future lines of research include: (a) mixed studies focusing on as many genetic variants as possible (e.g., CDKL5, SHANK3, DUP15, SCN1A, KCNQ2, GNAO1, PCDH19) in order to have a quantitative and qualitative comparative basis to integrate and understand the disease from the parents' perspective, (b) including the perspective of professionals who care for children and parents in these studies, and (c) longitudinal studies that consider psychological aspects of caregivers, especially sleep quality, to verify if they are related risk factors for long-term disability of the parent or child, worse family quality of life or worse prognosis of the affected child.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Local Ethical Committee of Universidad Rey Juan Carlos (code: 1802202308123). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MS-P-J: Data curation, Formal analysis, Validation, Visualization, Writing – review & editing. DP-C: Conceptualization, Formal analysis, Funding acquisition, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing. AS-M-G: Data curation, Formal analysis, Validation, Visualization, Writing – review & editing. ÁA-S: Conceptualization, Investigation, Methodology, Project administration, Supervision, Visualization, Writing – review & editing. LF: Conceptualization, Formal analysis, Funding acquisition, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This project was funded by the Universidad Rey Juan Carlos's “Impulso a la investigación” program (register number A514), in the 2022 call for proposals. Universidad Rey Juan Carlos had no role in the study design, data collection or analysis.
Acknowledgments
We thank the participants for their kind collaboration and participation in this research study. We would also like to thank the following associations: Asociación española de esclerosis tuberosa (http://esclerosistuberosa.org/), Asociación del síndrome STXBP1 (https://stxbp1.es/), Asociación SYNGAP1 España (https://www.syngap1.es/), for their immense work and support to all families.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2023.1285377/full#supplementary-material
References
1. Scheffer IE, Liao J. Deciphering the concepts behind “epileptic encephalopathy” and “developmental and epileptic encephalopathy”. Eur J Paediatr Neurol. (2020) 24:11–4. doi: 10.1016/j.ejpn.2019.12.023
2. Specchio N, Curatolo P. Developmental and epileptic encephalopathies: what we do and do not know. Brain. (2021) 144(1):32–43. doi: 10.1093/brain/awaa371
3. Beltrán-Corbellini Á, Aledo-Serrano Á, Møller RS, Pérez-Palma E, García-Morales I, Toledano R, et al. Epilepsy genetics and precision medicine in adults: a new landscape for developmental and epileptic encephalopathies. Front Neurol. (2022) 13:777115. doi: 10.3389/fneur.2022.777115
4. Symonds JD, Zuberi SM, Stewart K, McLellan A, O'Regan M, MacLeod S, et al. Incidence and phenotypes of childhood-onset genetic epilepsies: a prospective population-based national cohort. Brain. (2019) 142(8):2303–18. doi: 10.1093/brain/awz195
5. Wright D, Kenny A, Eley S, McKechanie AG, Stanfield AC. Clinical and behavioural features of SYNGAP1-related intellectual disability: a parent and caregiver description. J Neurodev Disord. (2022) 14(1):34. doi: 10.1186/s11689-022-09437-x
6. Pasquini TLS, Goff SL, Whitehill JM. Navigating the U.S. health insurance landscape for children with rare diseases: a qualitative study of parents’ experiences. Orphanet J Rare Dis. (2021) 16(1):313. doi: 10.1186/s13023-021-01943-w
7. Aledo-Serrano A, Mingorance A. Analysis of the family impact and needs of Dravet's syndrome in Spain. Rev Neurol. (2020) 70(3):75–83. doi: 10.33588/rn.7003.2019310
8. Robertson EG, Kelada L, Best S, Goranitis I, Pierce K; CoGENeS Groupet al.Quality of life in caregivers of a child with a developmental and epileptic encephalopathy. Dev Med Child Neurol. (2023). doi: 10.1111/dmcn.15695
9. McKeon G, Palmer EE, Macintosh R, Nevin SM, Wheatley L, Rosenbaum S. Feasibility of a mental health informed physical activity intervention for the carers of children with developmental and epileptic encephalopathy. Epilepsy Behav. (2021) 121:108022. doi: 10.1016/j.yebeh.2021.108022
10. Brandt M, Johannsen L, Inhestern L, Bergelt C. Parents as informal caregivers of children and adolescents with spinal muscular atrophy: a systematic review of quantitative and qualitative data on the psychosocial situation, caregiver burden, and family needs. Orphanet J Rare Dis. (2022) 17(1):274. doi: 10.1186/s13023-022-02407-5
11. Juandó-Prats C, James E, Bilder DA, McNair L, Kenneally N, Helfer J, et al. Parent caregivers of children with dravet syndrome: perspectives, needs, and opportunities for clinical research. Epilepsy Behav. (2021) 122:108198. doi: 10.1016/j.yebeh.2021.108198
12. Palacios-Ceña D, Güeita-Rodríguez J, Gil-Nagel A, Jimenez-Antona C, García-Bravo C, Velarde-García JF, et al. Health care concerns in parents of children with different genetic developmental and epileptic encephalopathies: a qualitative study. Dev Med Child Neurol. (2023). doi: 10.1111/dmcn.15712
13. European Joint Programme on Rare Diseases. Available at: https://www.ejprarediseases.org/ (Accessed 2 August, 2023).
14. Orphanet network. Available at: https://www.orpha.net/consor/cgi-bin/index.php?lng=EN (Accessed 2 August, 2023).
15. Das MK. An introduction to qualitative and mixed methods study designs in health research. Indian Pediatr. (2022) 59(5):416–23. doi: 10.1007/s13312-022-2523-4
16. Creswell JW. A concise introduction to mixed methods research. 2ed Thousand Oaks: SAGE Publications (2022).
18. Johnson SL. Impact, growth, capacity-building of mixed methods research in the health sciences. Am J Pharm Educ. (2019) 83(2):7403. doi: 10.5688/ajpe7403
19. Nguyen CQ, Kariyawasam D, Alba-Concepcion K, Grattan S, Hetherington K, Wakefield CE, et al. ‘Advocacy groups are the connectors’: experiences and contributions of rare disease patient organization leaders in advanced neurotherapeutics. Health Expect. (2022) 25(6):3175–91. doi: 10.1111/hex.13625
20. Lanar S, Parker S, O'Neill C, Marrel A, Arnould B, Héron B, et al. Understanding disease symptoms and impacts and producing qualitatively-derived severity stages for MPS IIIA: a mixed methods approach. Orphanet J Rare Dis. (2022) 17(1):75. doi: 10.1186/s13023-022-02208-w
21. Stuart C, Fladrowski C, Flinn J, Öberg B, Peron A, Rozenberg M, et al. Beyond the guidelines: how we can improve healthcare for people with tuberous sclerosis complex around the world. Pediatr Neurol. (2021) 123:77–84. doi: 10.1016/j.pediatrneurol.2021.07.010
22. Willems J, Farin-Glattacker E, Langer T. Evaluation of a case management to support families with children diagnosed with spinal muscular atrophy-protocol of a controlled mixed-methods study. Front Pediatr. (2021) 9:614512. doi: 10.3389/fped.2021.614512
23. Leclezio L, Jansen A, Whittemore VH, de Vries PJ. Pilot validation of the tuberous sclerosis-associated neuropsychiatric disorders (TAND) checklist. Pediatr Neurol. (2015) 52(1):16–24. doi: 10.1016/j.pediatrneurol.2014.10.006
24. Creswell JW, Klassen AC, Plano Clark VL, Smith KC. National Institutes of Health Office of Behavioral and Social Sciences Research. Best practices for mixed methods research in the health sciences. (2018). Available at: https://obssr.od.nih.gov/sites/obssr/files/Best_Practices_for_Mixed_Methods_Research.pdf (Accessed 2 August, 2023).
25. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP, et al. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Br Med J. (2007) 335(7624):806–8. doi: 10.1136/bmj.39335.541782.AD
26. O'Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. (2014) 89(9):1245–51. doi: 10.1097/ACM.0000000000000388
27. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. (2007) 19(6):349–57. doi: 10.1093/intqhc/mzm042
28. Federación Española de Enfermedades Raras. Available at: https://www.enfermedades-raras.org/ (Accessed October 16, 2023).
29. Registro Estatal de Enfermedades Raras. Available at: https://www.sergas.es/Asistencia-sanitaria/Documents/1405/InformeEpidemiologicoAnual_2022.pdf (Accessed October 16, 2023) (2022).
30. Murillo E. Características de las personas con el síndrome STXBP1 en españa: implicaciones para el diagnóstico [characteristics of people with the STXBP1 syndrome in Spain: implications for diagnosis]. An Pediatr. (2020) 92(2):71–8. doi: 10.1016/j.anpedi.2019.04.008
31. SYNGAP1 España. Available at: https://www.syngap1.es/que-es-syngap1/ (Accessed October 16, 2023).
32. Vilagut G, Valderas JM, Ferrer M, Garin O, López-García E, Alonso J. Interpretación de los cuestionarios de salud SF-36 y SF-12 en españa: componentes físico y mental [interpretation of SF-36 and SF-12 questionnaires in Spain: physical and mental components]. Med Clin. (2008) 130(19):726–35. doi: 10.1157/13121076
33. Ware J Jr, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. (1996) 34(3):220–33. doi: 10.1097/00005650-199603000-00003
34. Balcells-Balcells A, Giné C, Guàrdia-Olmos J, Summers JA. Family quality of life: adaptation to Spanish population of several family support questionnaires. J Intellect Disabil Res. (2011) 55(12):1151–63. doi: 10.1111/j.1365-2788.2010.01350.x
35. Hoffman L, Marquis J, Poston D, Summers JA, Turnbull A. Assessing family outcomes: psychometric evaluation of the beach center family quality of life scale. J Marriage Fam. (2006) 68(4):1069–83. doi: 10.1111/j.1741-3737.2006.00314.x
36. Alnahdi GH, Alwadei A, Woltran F, Schwab S. Measuring family quality of life: scoping review of the available scales and future directions. Int J Environ Res Public Health. (2022) 19(23):15473. doi: 10.3390/ijerph192315473
37. Nieto-Eugenio I, Romero-Saldaña M, Guler-Caamaño I, Rich-Ruiz M. Validation of the impact on family scale (spanish version) and predictive variables in parents of children with severe food allergy. J Pediatr Nurs. (2021) 56:e93–9. doi: 10.1016/j.pedn.2020.08.011
38. Stein R, Jessop D. The impact on family scale revisited: further psychometric data. J Dev Behav Paediatr. (2003) 24(1):9–16. doi: 10.1097/00004703-200302000-00004
39. Camfield C, Breau L, Camfield P. Impact of pediatric epilepsy on the family: a new scale for clinical and research use. Epilepsia. (2001) 42(1):104–12. doi: 10.1046/j.1528-1157.2001.081420.x
40. Garófalo Gómez N, Fernández Concepción O, Gómez García AM. Reliability and validity of a Spanish version of the impact of pediatric epilepsy scale in a cuban population. Epilepsy Behav. (2013) 29(2):357–60. doi: 10.1016/j.yebeh.2013.07.023
41. Beck AT, Steer RA, Brown GK. Manual for the beck depression inventory-II. San Antonio: Psychological Corporation (1996).
42. Magán I, Sanz J, García-Vera MP. Psychometric properties of a Spanish version of the beck anxiety inventory (BAI) in general population. Span J Psychol. (2008) 11(2):626–40. doi: 10.1017/S1138741600004637
43. Guillén-Riquelme A, Buela-Casal G. Actualización psicométrica y funcionamiento diferencial de los ítems en el state trait anxiety inventory (STAI) [psychometric revision and differential item functioning in the state trait anxiety inventory (STAI)]. Psicothema. (2011) 23(3):510–5. Available at: https://www.psicothema.com/pdf/3916.pdf
44. Spielberger CD. State-trait anxiety inventory: A comprehensive bibliography. Palo Alto: Consulting Psychologists Press (1989).
45. Buysse DJ, Reynolds CF, Monk TH 3rd, Monk TH, Berman SR, Kupfer DJ. The pittsburgh sleep quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. (1989) 28:193–213. doi: 10.1016/0165-1781(89)90047-4
46. Hita-Contreras F, Martínez-López E, Latorre-Román PA, Garrido F, Santos MA, Martínez-Amat A. Reliability and validity of the Spanish version of the pittsburgh sleep quality index (PSQI) in patients with fibromyalgia. Rheumatol Int. (2014) 34(7):929–36. doi: 10.1007/s00296-014-2960-z
47. Jack SM, Phoenix M. Qualitative health research in the fields of developmental medicine and child neurology. Dev Med Child Neurol. (2022) 64(7):830–9. doi: 10.1111/dmcn.15182
48. Moser A, Korstjens I. Series: practical guidance to qualitative research. part 3: sampling, data collection and analysis. Eur J Gen Pract. (2018) 24(1):9–18. doi: 10.1080/13814788.2017.1375091
49. Teddlie C, Yu F. Mixed methods sampling: a typology with examples. J Mix Methods Res. (2007) 1(1):77–100. doi: 10.1177/1558689806292430
50. Vasileiou K, Barnett J, Thorpe S, Young T. Characterising and justifying sample size sufficiency in interview-based studies: systematic analysis of qualitative health research over a 15-year period. BMC Med Res Methodol. (2018) 18(1):148. doi: 10.1186/s12874-018-0594-7
51. Sim J, Saunders B, Waterfield J, Kingstone T. Can sample size in qualitative research be determined a priori? Int J Soc Res Methodol. (2018) 21(5):619–34. doi: 10.1080/13645579.2018.1454643
52. DeJonckheere M, Vaughn LM. Semistructured interviewing in primary care research: a balance of relationship and rigour. Fam Med Community Health. (2019) 7(2):e000057. doi: 10.1136/fmch-2018-000057
53. García-Bravo C, Palacios-Ceña D, Huertas-Hoyas E, Pérez-Corrales J, Serrada-Tejeda S, Pérez-de-Heredia-Torres M, et al. Your life turns upside down": a qualitative study of the experiences of parents with children diagnosed with Phelan-McDermid syndrome. Children. (2022) 10(1):73. doi: 10.3390/children10010073
54. García-Bravo C, Martínez-Piédrola RM, García-Bravo S, Huertas-Hoyas E, Pérez-De-Heredia-Torres M, Palacios-Ceña D. Experiences surrounding the diagnostic process and care among parents of children diagnosed with phelan-McDermid syndrome: a qualitative study. Dev Med Child Neurol. (2023) 65(7):908–16. doi: 10.1111/dmcn.15485
55. Güeita-Rodriguez J, Famoso-Pérez P, Salom-Moreno J, Carrasco-Garrido P, Pérez-Corrales J, Palacios-Ceña D. Challenges affecting access to health and social care resources and time management among parents of children with rett syndrome: a qualitative case study. Int J Environ Res Public Health. (2020) 17(12):4466. doi: 10.3390/ijerph17124466
56. Demarest S, Marsh R, Treat L, Fisher MP, Dempsey A, Junaid M, et al. The lived experience of Parents’ receiving the diagnosis of CDKL5 deficiency disorder for their child. J Child Neurol. (2022) 37(6):451–60. doi: 10.1177/08830738221076285
57. Jordan J, Clarke SO, Coates WC. A practical guide for conducting qualitative research in medical education: part 1-how to interview. AEM Educ Train. (2021) 5(3):e10646. doi: 10.1002/aet2.10646
58. Miles MB, Huberman AM, Saldaña J. qualitative data analysis. A methods sourcebook. 3 edn Thousand Oaks: SAGE Publications (2014).
59. Korstjens I, Moser A. Series: practical guidance to qualitative research. Part 4: trustworthiness and publishing. Eur J Gen Pract. (2018) 24(1):120–4. doi: 10.1080/13814788.2017.1375092
60. Kaur N, Vedel I, El Sherif R, Pluye P. Practical mixed methods strategies used to integrate qualitative and quantitative methods in community-based primary health care research. Fam Pract. (2019) 36(5):666–71. doi: 10.1093/fampra/cmz010
61. Curry L, Nunez-Smith M. Mixed methods in health sciences research: a practical primer. Thousand Oaks: SAGE Publications (2015).
62. Guetterman TC, Fetters MD, Creswell JW. Integrating quantitative and qualitative results in health science mixed methods research through joint displays. Ann Fam Med. (2015) 13:554–61. doi: 10.1370/afm.1865
63. Fetters MD, Curry LA, Creswell JW. Achieving integration in mixed methods designs-principles and practices. Health Serv Res. (2013) 48:2134–56. doi: 10.1111/1475-6773.12117
64. Willems LM, Schubert-Bast S, Grau J, Hertzberg C, Kurlemann G, Wiemer-Kruel A, et al. Health-related quality of life in children and adolescents with tuberous sclerosis complex and their caregivers: a multicentre cohort study from Germany. Eur J Paediatr Neurol. (2021) 35:111–22. doi: 10.1016/j.ejpn.2021.10.003
65. Lo SH, Marshall J, Skrobanski H, Lloyd A. Patient and caregiver health state utilities in tuberous sclerosis complex. Pharmacoecon Open. (2022) 6(1):105–21. doi: 10.1007/s41669-021-00296-1
66. Graffigna G, Bosio C, Cecchini I. Assisting a child with tuberous sclerosis complex (TSC): a qualitative deep analysis of parents’ experience and caring needs. BMJ Open. (2013) 3(12):e003707. doi: 10.1136/bmjopen-2013-003707
67. Rentz AM, Skalicky AM, Pashos CL, Liu Z, Magestro M, Pelletier CL, et al. Caring for children with tuberous sclerosis complex: what is the physical and mental health impact on caregivers? J Child Neurol. (2015) 30(12):1574–81. doi: 10.1177/0883073815575364
68. Skrobanski H, Vyas K, Bowditch S, Hubig L, Dziadulewicz E, Fish L, et al. The burden of caring for individuals with tuberous sclerosis complex (TSC) who experience epileptic seizures: a descriptive UK survey. Pharmacoecon Open. (2023) 7(2):299–312. doi: 10.1007/s41669-023-00387-1
69. Verberne EA, van den Heuvel LM, Ponson-Wever M, de Vroomen M, Manshande ME, Faries S, et al. Genetic diagnosis for rare diseases in the Dutch Caribbean: a qualitative study on the experiences and associated needs of parents. Eur J Hum Genet. (2022) 30:587–94. doi: 10.1038/s41431-022-01039-4
70. García-Bravo C, Palacios-Ceña D, García-Bravo S, Pérez-Corrales J, Pérez-de-Heredia-Torres M, Martínez-Piédrola RM. Social and family challenges of having a child diagnosed with phelan-McDermid syndrome: a qualitative study of parents’ experiences. Int J Environ Res Public Health. (2022) 19(17):10524. doi: 10.3390/ijerph191710524
71. Sartore GM, Pourliakas A, Lagioia V. Peer support interventions for parents and carers of children with complex needs. Cochrane Database Syst Rev. (2021) 12:CD010618. doi: 10.1002/14651858.CD010618
72. Zöllner JP, Franz DN, Hertzberg C, Nabbout R, Rosenow F, Sauter M, et al. A systematic review on the burden of illness in individuals with tuberous sclerosis complex (TSC). Orphanet J Rare Dis. (2020) J15(1):23. doi: 10.1186/s13023-019-1258-3
73. Sullivan KR, Ruggiero SM, Xian J, Thalwitzer KM, Ali R, Stewart S, et al. A disease concept model for STXBP1-related disorders. Epilepsia Open. (2023) 8(2):320–33. doi: 10.1002/epi4.12688
74. Nabbout R, Auvin S, Chiron C, Thiele E, Cross H, Scheffer IE, et al. Perception of impact of Dravet syndrome on children and caregivers in multiple countries: looking beyond seizures. Dev Med Child Neurol. (2019) 61(10):1229–36. doi: 10.1111/dmcn.14186
75. Halley MC, Young JL, Fernandez L, Kohler JN, Undiagnosed Diseases Network, Bernstein JA, et al. Perceived utility and disutility of genomic sequencing for pediatric patients: perspectives from parents with diverse sociodemographic characteristics. Am J Med Genet A. (2022) 188:1088–101. doi: 10.1002/ajmg.a.62619
76. Giusti F, Cioppi F, Fossi C, Marini F, Masi L, Tonelli F, et al. Quality of life in Italian patients with multiple endocrine neoplasia type 1 (MEN 1): results of an extensive survey. Orphanet J Rare Dis. (2021) 16:16. doi: 10.1186/s13023-020-01650-y
77. Cardinali P, Migliorini L, Rania N. The caregiving experiences of fathers and mothers of children with rare diseases in Italy: challenges and social support perceptions. Front Psychol. (2019) 10:1780. doi: 10.3389/fpsyg.2019.01780
78. Baumbusch J, Mayer S, Sloan-Yip I. Alone in a crowd? parents of children with rare diseases’ experiences of navigating the healthcare system. J Genet Couns. (2019) 28:80–90. doi: 10.1007/s10897-018-0294-9
79. Currie G, Szabo J. ‘It would be much easier if we were just quiet and disappeared’: parents silenced in the experience of caring for children with rare diseases. Health Expect. (2019) 22:1251–9. doi: 10.1111/hex.12958
80. Palacios-Ceña D, Famoso-Pérez P, Salom-Moreno J, Carrasco-Garrido P, Pérez-Corrales J, Paras-Bravo P, et al. “Living an obstacle course”: a qualitative study examining the experiences of caregivers of children with rett syndrome. Int J Environ Res Public Health. (2019) 16:41. doi: 10.3390/ijerph16010041
81. Barco T L, De Gaetano L, Santangelo E, Bravi T, Proietti J, Cantalupo G, et al. SYNGAP1-related developmental and epileptic encephalopathy: the impact on daily life. Epilepsy Behav. (2022) 127:108500. doi: 10.1016/j.yebeh.2021.108500
82. Currie G, Szabo J. Social isolation and exclusion: the parents’ experience of caring for children with rare neurodevelopmental disorders. Int J Qual Stud Health Well-Being. (2020) 15:1725362. doi: 10.1080/17482631.2020.1725362
83. Uhlenbusch N, Löwe B, Depping MK. Perceived burden in dealing with different rare diseases: a qualitative focus group study. BMJ Open. (2019) 9(12):e033353. doi: 10.1136/bmjop-2019-033353
84. Strzelczyk A, Kalski M, Bast T, Wiemer-Kruel A, Bettendorf U, Kay L, et al. Burden-of-illness and cost-driving factors in Dravet syndrome patients and carers: a prospective, multicenter study from Germany. Eur J Paediatr Neurol. (2019) 23(3):392–403. doi: 10.1016/j.ejpn.2019.02.014
85. Sullivan J, Deighton AM, Vila MC, Szabo SM, Maru B, Gofshteyn JS, et al. The clinical, economic, and humanistic burden of dravet syndrome—a systematic literature review. Epilepsy Behav. (2022) 130:108661. doi: 10.1016/j.yebeh.2022.108661
86. Palmer EE, Sachdev R, Beavis E, Macintosh R, Le Marne FA, Nevin SM, et al. Hope in the uncertainties and certainty for parents of children with rare neurological disorders. Part I (of 3): uncertainty. J Paediatr Child Health. (2022) 58(10):1718–21. doi: 10.1111/jpc.16165
87. Nevin SM, Beavis E, Macintosh R, Palmer EE, Sachdev R, Le Marne FA, et al. Hope in the uncertainties and certainty for parents of children with rare neurological disorders: part 2 (of 3): certainty. J Paediatr Child Health. (2022) 58(10):1722–25. doi: 10.1111/jpc.16202
88. Bye AM, Le Marne FA, Beavis E, Macintosh R, Nevin SM, Palmer EE, et al. Hope in the uncertainties and certainty for parents of children with rare neurological disorders: part 3 (of 3): hope. J Paediatr Child Health. (2022) 58(10):1726–28. doi: 10.1111/jpc.16187
89. Hesdorffer DC, Kroner BL, Shen J, Farrell K, Roberds S, Fureman B, et al. Factors associated with caregiver sleep quality related to children with rare epilepsy syndromes. J Pediatr X. (2020) 2:100021. doi: 10.1016/j.ympdx.2020.100021
90. Gonçalves C, Martins S, Fernandes L. Dravet syndrome: effects on informal caregivers’ mental health and quality of life—a systematic review. Epilepsy Behav. (2021) 122:108206. doi: 10.1016/j.yebeh.2021.108206
Keywords: neurodevelopmental disorders, genetic epilepsy, pediatrics, carers, tuberous sclerosis complex, STXBP1, SYNGAP1, mixed methods research
Citation: Salcedo-Perez-Juana M, Palacios-Ceña D, San-Martín-Gómez A, Aledo-Serrano Á and Florencio LL (2023) Quality of life, socioeconomic and psychological concerns in parents of children with tuberous sclerosis complex, STXBP1 and SYNGAP1 encephalopathies: a mixed method study. Front. Pediatr. 11:1285377. doi: 10.3389/fped.2023.1285377
Received: 29 August 2023; Accepted: 27 October 2023;
Published: 9 November 2023.
Edited by:
Carl E. Stafstrom, Johns Hopkins University, United StatesReviewed by:
Theresa V. Strong, Foundation for Prader-Willi Research, United StatesDaiana Priscila Rodrigues-de-Souza, University of Cordoba, Spain
Paula Paras Bravo, University of Cantabria, Spain
Francisco Alburquerque-Sendín, University of Cordoba, Spain
Juan Francisco Velarde García, Red Cross University School of Nursing, Spain
© 2023 Salcedo-Perez-Juana, Palacios-Ceña, San-Martín-Gómez, Aledo-Serrano and Florencio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Domingo Palacios-Ceña ZG9taW5nby5wYWxhY2lvc0B1cmpjLmVz
†These authors have contributed equally to this work and share last authorship