 Yu Zhang1,†
Yu Zhang1,† Haihong Li
Haihong Li
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Pediatr. , 31 August 2023
Sec. Neonatology
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1198730
Background: Massage therapy for preterm newborns has received increasing attention in recent years due to its beneficial clinical outcomes. However, disagreements persist in different investigations.
Method: We performed a systematic literature search in the Cochrane Library, Embase, PubMed, Web Science, and CINAHL to retrieve randomized controlled trials of premature infants receiving massage therapy and its impact on maternal and infant outcomes. Outcomes were mother-infant attachment, oxygen saturation, motor funtion, reflex, temperature, and calorie intake. The tool developed by the Cochrane collaboration assessed risk bias. With a 95% confidence interval (CI), the integration's results were presented as the mean difference or standardized mean difference. The registration number was CRD42022337849.
Results: Of 940 records retrieved, 15 trials were included. Massage therapy increased oxygen saturation (standardized mean difference (SMD) = 2.00, 95% CI [1.17 to 2.83], P < 0.0001). Massage therapy can strengthen mother-infant attachment [SMD = 2.83, 95% CI (2.31 to 3.35), P < 0.00001]. Other outcomes, including motor activity, relaxation, caloric intake, and temperature, did not differ significantly.
Conclusion: Massage therapy can significantly improve oxygen saturation and strengthen maternal-infant attachment. However, prior to making a recommendation, additional research with a larger sample size and more rigorous design should be conducted due to the heterogeneity of studies in several outcomes.
More than 1 in 10 babies are born prematurely worldwide each year, which means that there are 15 million premature births each year (1). Preterm birth accounts for an increased risk of mortality and morbidity both in the short and long term (2). In developed countries, advanced maternal age, twin pregnancies, assisted reproduction, and other factors have led to an increase in the rate of premature births (3). Preterm infants and children born with low birth weights exhibit unfavorable growth and development in the future, which is a crucial determinant of the subsequent development of adult diseases (4). While many preterm infants are present in developed countries, mortality for a preterm infant born in a low-income or middle-income country (LMIC) is eight times higher than in Europe (5). Thus, it can be shown that in low- and middle-income countries and regions, there may be a lack of adequate preterm care, which puts the lives of many preterm infants at risk (1). Therefore, early care for preterm infants is extremely important (6).
Several studies have shown the variety of benefits of massage therapy for preterm infants, such as weight gain, immune enhancement, cognitive improvement, neurodevelopment, and shorter hospital stays. Whether as a primary or secondary outcome, weight gain is the most commonly assessed outcome in randomized controlled trials of massage for preterm infants (7). The mechanism of action of massage therapy on weight gain in preterm infants is not completely clear. Related studies suggest that massage may increase the amount of muscle and limb activity, leading to an increase in the infant's metabolism, which promotes the synthesis of glycogen, fat, and protein to increase their body weight (8), and it has been suggested that increased vagal activity induced by massage may lead to increased gastric motility in preterm infants and thus is thought to be a potential mechanism for the greater weight gain in infants receiving massage therapy (9, 10). In a related study, the effect of massage therapy on immunity in preterm infants may derive from the finding that natural killer (NK) cell activity was higher in preterm infants who received massage (11). Studies related to cognitive and neurodevelopment in preterm infants found that preterm infants who received massage had higher cognitive scores at the corrected age of 12 months (12) and higher higher mental development scores at 6 months of age (13). Procianoy compared the neurodevelopment of preterm infants who received massage during hospitalization with that of a control group at 2 years of age and found that preterm infants who received massage therapy had higher Mental Development Index (MDI) scores at 2 years of age (14). Massage therapy for preterm infants can also affect the length of hospitalization of preterm infants, and studies have shown that preterm infants who received massage therapy had a significantly lower length of hospitalization than control preterm infants (15), and infants who received massage were 1.85 times more likely to be discharged from the hospital earlier than control infants (16).
Our search of the relevant literature revealed that previous systematic evaluations and reviews have reported the facilitating effect of massage therapy on the above outcome indicators (weight gain, enhanced immunity, improved cognition, etc.) (17–19); however, there is still controversy as to whether massage therapy can improve mother-infant attachment (20, 21), calorie intake (22), motor function (23, 24), reflexes (23, 25), body temperature (26, 27), and oxygen saturation (24, 28) in preterm infants. Therefore, this study conducted a meta-analysis of the above indicators to assess the efficacy of massage therapy in preterm infants.
1) Preterm infants: Infants born less than 37 weeks or 259 days gestational age (29).
2) Low birth weight: Birth weight less than 2,500 g (30).
3) Massage Therapy: Skin massage is considered a therapeutic touch intervention that involves the planned and purposeful application of tactile stimuli through the person's hands (31). Massage therapy for preterm infants is usually performed using the Field protocol, which lasts for five days, three times a day, one hour after feeding. Massage usually lasts 15 min and is divided into three phases: five minutes of tactile stimulation, five minutes of kinesthetic stimulation, and five minutes of tactile stimulation (26). In addition to this, there are the Vimala protocol (15) and the Vaymal protocol (32). Massage is usually performed by massage therapists, systematically trained researchers, or parents of premature infants (21, 25, 27).
4) Mother-infant attachment: An intimate relational bond formed between mother and infant, specifically, the emotional connection that the mother makes with the infant, and the basis for the infant to build his or her own attachment system (33).
5) Caloric intake: The daily caloric intake of preterm infants per kilogram, usually in kilocalories or joules.
1) Type of participants: Preterm neonates born at a gestation age (GA) under 37 weeks or with low birth weight (<2,500 g); 2) Treatment group: Massage therapy for premature infants; 3) Control group: Preterm infants that are routinely treated; 4) Research type: Randomized controlled trial (RCT); 5) At least one of the following outcome measures was included in the study: mother-infant attachment, oxygen saturation, motor, reflex, temperature, and calorie intake.
1) Retrospective studies, prospective observational studies, narrative review letters, editorials, and commentaries; 2) Literature with identical content; 3) RCTs without a control group; 4) RCTs with a combination of interventions; 5) non-English-language literature; 6) Outcome indicators that could not be extracted or inferred.
We performed a systematic literature search in PubMed, the Cochrane Library, Embase, CINAHL, and Web of Science from their inception until 25 April 2022 for RCTs of massage therapy and routinely treated for preterm infants, using combinations of the following terms: “Massage Therapy,” “Zone Therapy,” “Massage Therapies,” “Zone Therapies,” “Premature Infant,” “Neonatal Prematurity,” “Premature baby,” “Premature births,” and “Randomized Controlled Trial.” In addition, the references in all selected articles were screened for any potential eligible studies. Detailed information on the search strategies are provided in Supplementary Table S1.
Two reviewers independently evaluated whether each study met the inclusion and exclusion criteria. Disagreements between two reviewers were resolved by discussion with a third reviewer when necessary. Eligibility for inclusion was determined after reading the abstract and consensus was reached through discussion. The extraction of statistics from eligible research was performed by three impartial reviewers who employed standardized tables to ensure consistency. A team of two reviewers was responsible for the data extraction process of the study. To resolve any and all disputes, an additional reviewer was employed as a means of reaching a resolution. The reviewers carefully extracted pertinent information, including interventions and outcome indicators, ensuring a comprehensive analysis of the research. The random effects model was selected for its versatility in accounting for varying degrees of heterogeneity among studies. To combine the results, the effect estimates of the meta-analysis were converted to SMDs and weighted to account for any major study overlaps, ensuring a more accurate and comprehensive summary of the findings. We extracted the baseline data of the articles and the outcome indicators of interest, including the author, title, publication year, general information of the research subjects, and outcome indicators. We created a pre-extraction table taking Valizadeh's article as an example (Table 1).

Table 1. Pre-extraction table .
The methodological quality of RCTs was assessed by the Cochrane “Risk of Bias Assessment Tool” (34). Independent assessments of the risk of bias (ROB) were conducted by two authors (Z.Y and D.C.L). The domains assessed include random number generation, allocation concealment, blinding of intervention and outcome assessors, completeness of follow-up, and other potential sources of bias. Conflicting results were re-evaluated by a third author (C.L.Y). Differences in opinion were resolved by consensus after a team dialogue involving all authors.
The amalgamation of data was achieved utilizing the complete meta-analysis software program RevMan (version 5.3). We performed statistical analysis to determine the magnitude of change and variability in our outcome metrics of interest. We estimated the SMD and 95% CI for these outcomes. Typically, SMD is used when the studies all assess the same outcome but measure it in a different way or using a different scale. We therefore used the SMD to measure mother-infant attachment and calorie intake. We used the mean difference (MD) to measure motor, body temperature, and reflex. Finally, subgroup analyses of oxygen saturation were performed on different intervention days. The chi-square test and I2 were used to evaluate the statistical heterogeneity between massage therapy effects across the trials. For ease of reporting, we tentatively assigned low I2 values of 25%–50%, moderate I2 values of 51%–75%, and high I2 values of 76%–100% (35).
This meta-analysis adhered to the 2009 Priority Reporting Items for Systematic Review and Meta-analysis Guidelines and was registered on PROSPERO. The registration number was CRD42022337849 (36).
By sourcing data from five different databases, a total of 940 studies were identified. After removing 296 duplicates using EndNote software, the remaining 644 articles were reviewed for titles and abstracts, and 595 articles were excluded because the intervention, study personnel, study results, and study type did not meet the inclusion criteria. The full text of the remaining 49 articles was reviewed to assess compliance and inclusion criteria. Finally, 15 studies (15, 21–28, 32, 37–41) were selected as they met all the inclusion criteria and were included in the meta-analyses (Figure 1).
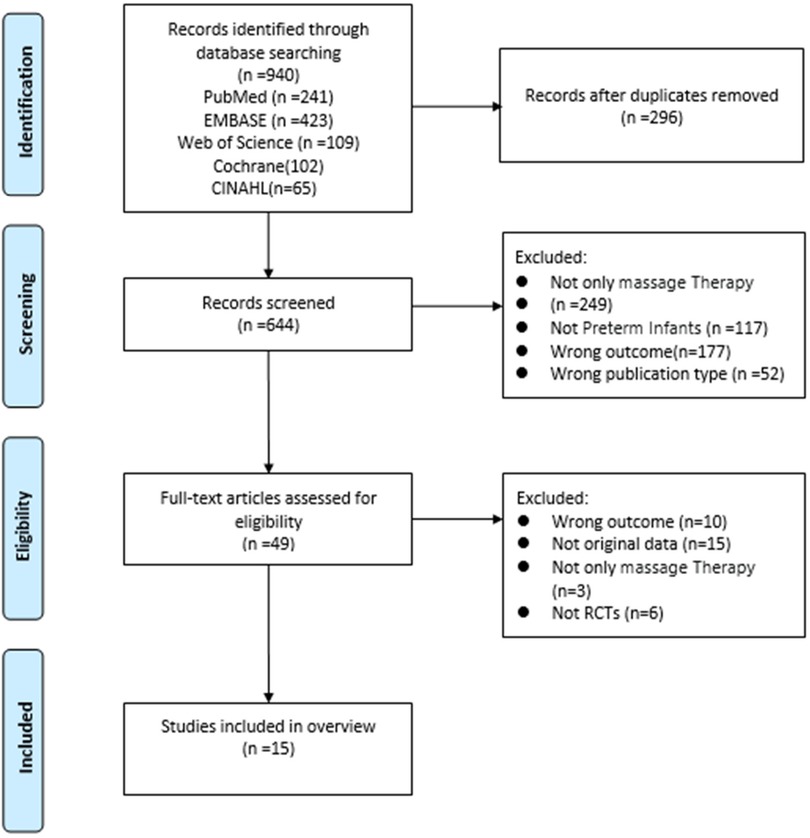
Figure 1. Flowchart of study selection.
Overall, a total of 15 studies were published between 2001 and 2021, which satisfied the inclusion criteria. In the eligible studies, the sample size ranged from 20 to 90 participants, gestational age from 32 to 37 weeks, and birth weight of participants from 800 to 2000g. Table 2 describe the study and patient baseline characteristics.
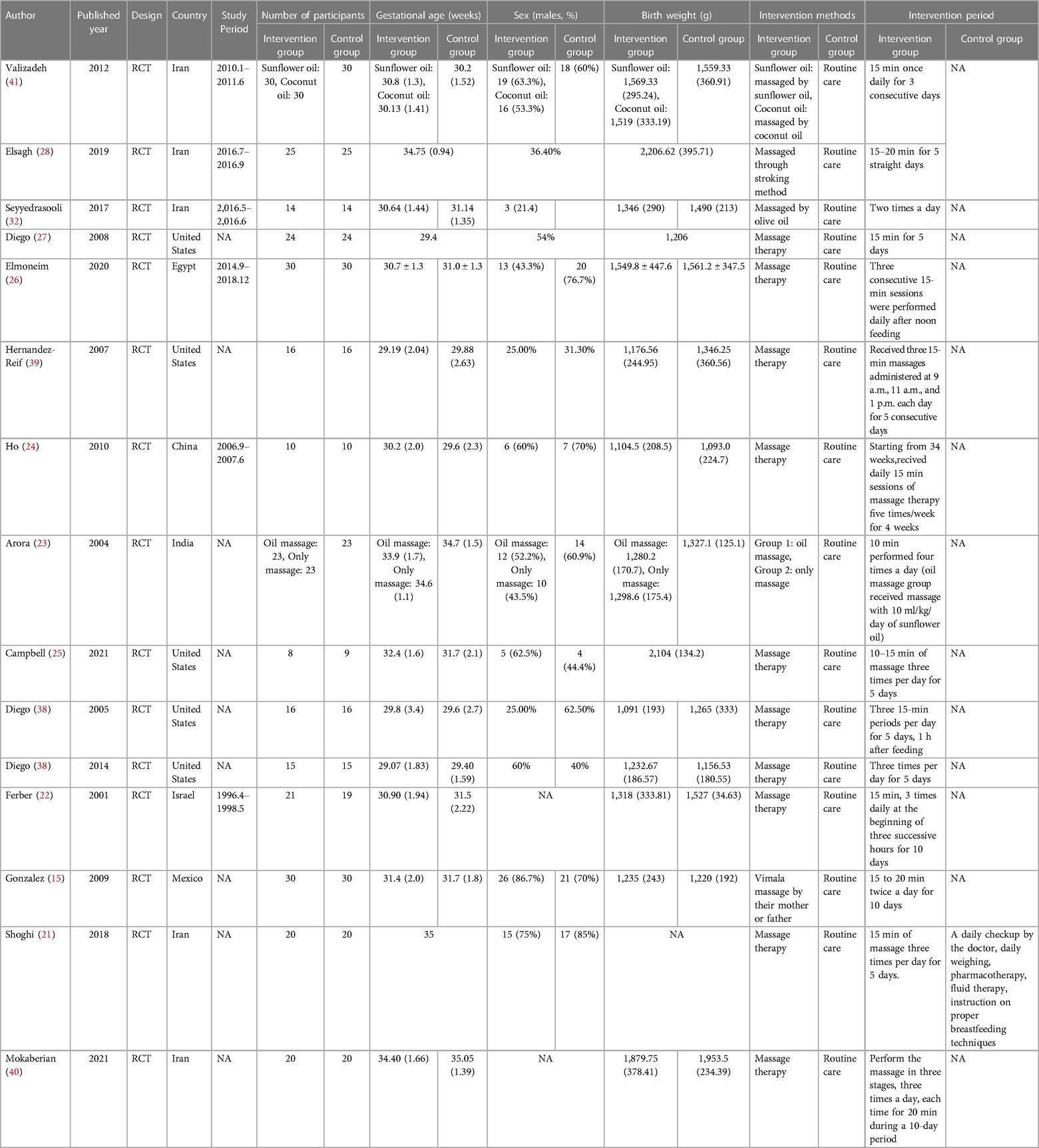
Table 2. Article baseline data (n = 15).
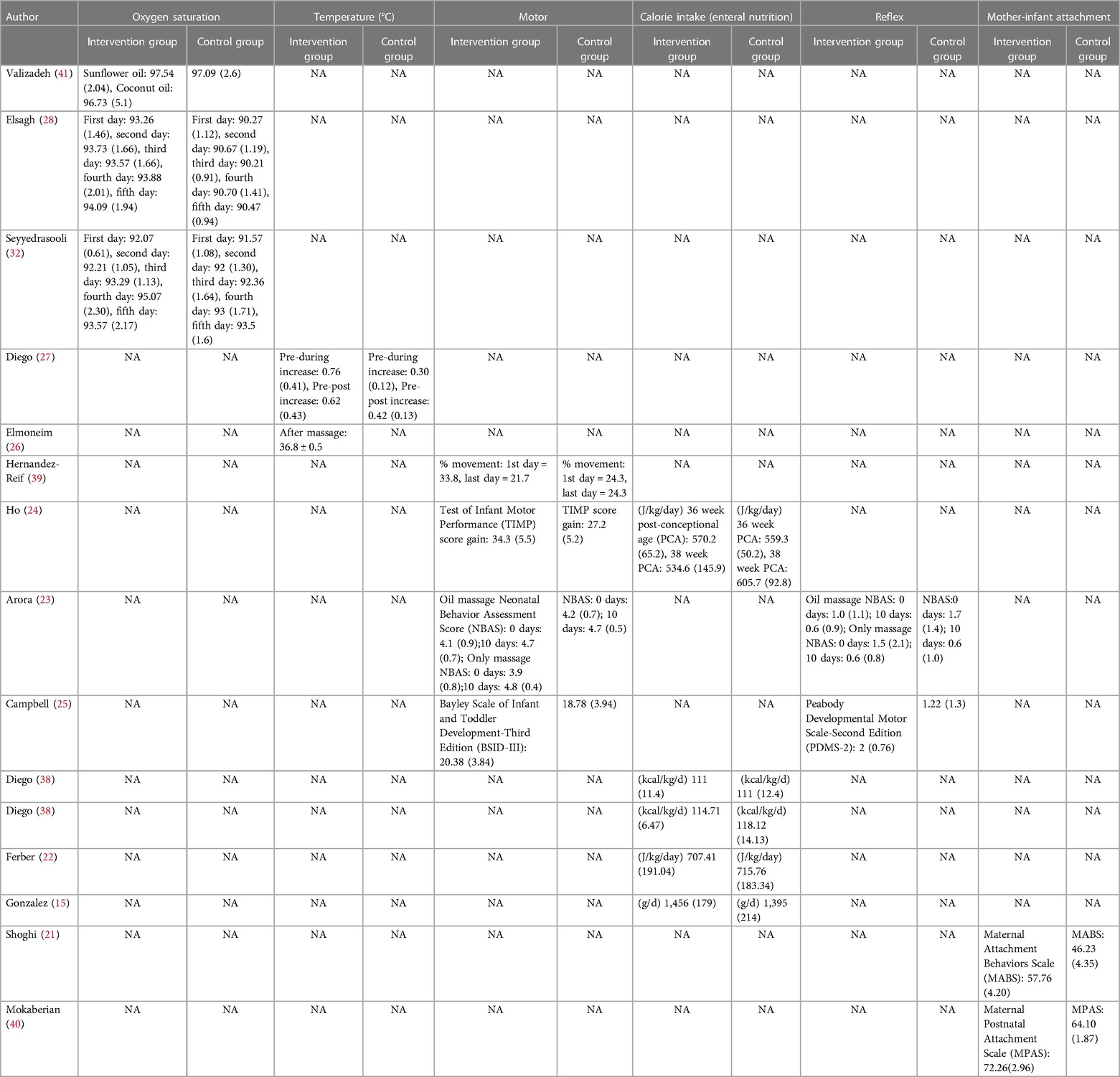
Table 2. Continued (outcomes of articles).
The results of the ROB assessment are reported in Table 3. Six trials used some form of a random sequence generation method. Allocation concealment was not clear in five trials; the risk of selective reporting of results and other biases was low in all trials.
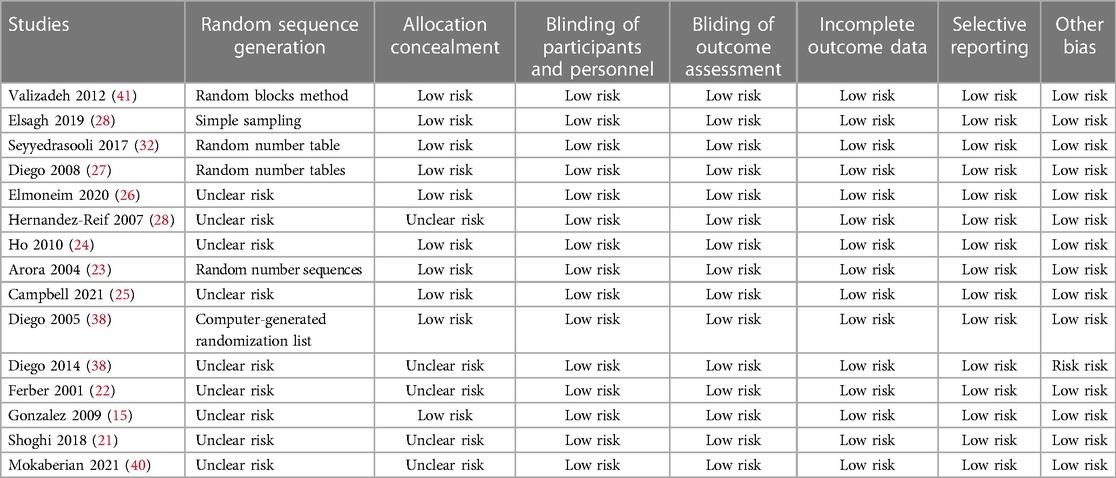
Table 3. Overview of risk of bias (n = 15).
The table of characteristics of the included studies comprehensively summarizes the study population characteristics, including reflex, motor, maternal-infant attachment, and oxygen saturation in order to assess the inherent heterogeneity. Statistical heterogeneity was estimated using the I2 statistic (42). Assessment of publication bias was conducted utilizing a funnel plot (43). The funnel plot depicted a symmetrical distribution, indicating the absence of publication bias, as exemplified in Figure 2 and Figure 3.
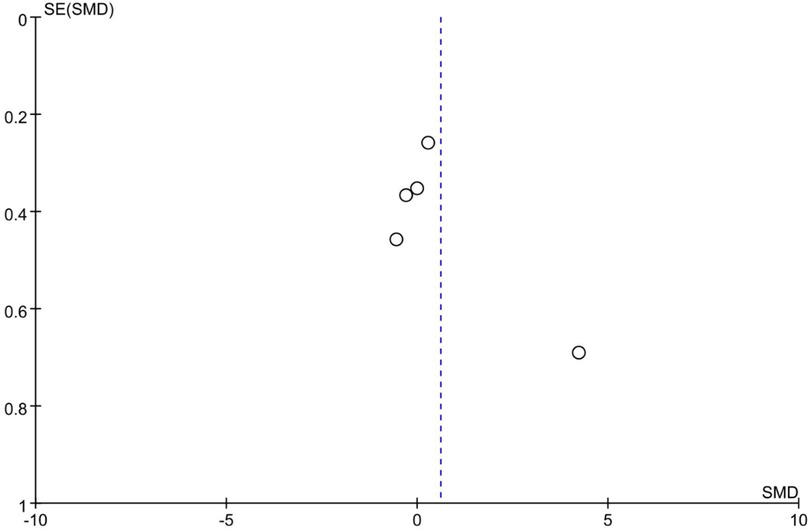
Figure 2. Funnel plot of calorie intake.
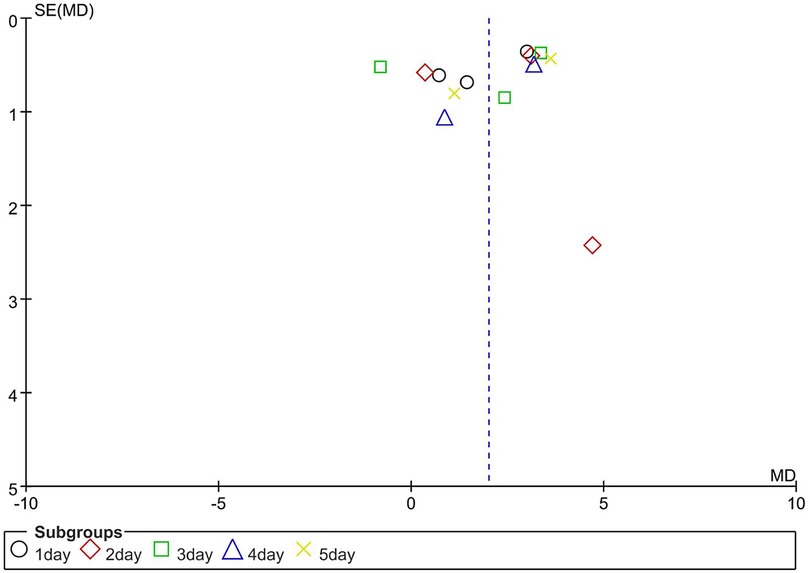
Figure 3. Funnel plot of oxygen saturation.
Only two studies have reported the effect of massage therapy on mother-infant attachment. Among them, Mokaberian (40) used the Maternal Postnatal Attachment Scale (MPAS) and Shoghi (21) used the Maternal Attachment Behavior Scale (MABS). The two scholars used different instruments to measure maternal-infant attachment. As shown in Figure 4, there was a significant increase in the level of mother-infant attachment [SMD = 2.83, 95% CI (2.31 to 3.35), P < 0.0001]. It was observed that the heterogeneity was relatively minor across these studies. (I2 = 0%, P = 0.34).

Figure 4. Forest plot of some primary outcomes. (A) Mother-child attachment. (B) Calorie intake. (C) Motor function. (D) Reflex. (E) Body temperature.
The evaluation of five studies revealed an insignificant impact of massage therapy on calorie intake compared to the control group [MD = 0.60, 95% CI (−0.46 to 1.67), P = 0.27], with a high degree of heterogeneity (I2 = 90%, P < 0.00001). Figure 4 depicts the results of these studies.
Motor function was defined in this study as motor control and organization of posture and movement for functional activities. Four studies reported the effect of massage therapy on motor function in preterm infants. Two of these studies (23, 24) used Neonatal Behavior Assessment Scores (NBAS) and Test of Infant Motor Performance (TIMP) to assess the motor function of preterm infants before and after receiving the intervention. One study used the Bayley Scales of Infant and Toddler Development-Third Edition (BSID-III) (25), while the other study (39) used direct observation of infant limb and trunk movements to assess whether massage therapy improved motor function in preterm infants. Massage therapy had no statistically significant effect on improving the motor function in preterm infants, according to the four studies that evaluated its effectiveness on motor function in preterm infants. [SMD = 0.11, 95% CI (−0.16 to 0.38), P = 0.43], with low heterogeneity (I2 = 0%, P = 0.64), as depicted in Figure 4.
The effect of massage therapy on the reflexes of preterm infants was evaluated in two studies. Of these, Arora's study used the Neonatal Behavior Assessment Scores (NBAS), while Campbell's study used the Peabody Developmental Motor Scales-Second Edition (PDMS-2). The results of the two studies on whether massage therapy affects reflexes in preterm infants were inconsist. As shown in Figure 4, the pooled results indicated that massage therapy had no statistically significant effect on the reflex of preterm infants [MD = 0.18, 95% CI (−0.30 to 0.65), P = 0.147], with moderate heterogeneity (I2 = 45%, P = 0.18).
Two studies have estimated the effect of massage therapy on body temperature. The results indicated that massage therapy had no statistically significant active effect on body temperature, with moderate heterogeneity (I2 = 45%, P = 0.18), as depicted in Figure 4.
To research the effect of massage therapy on oxygen saturation in preterm neonates, each day of receiving massage therapy was used as the basis for subgroup classification, and the literature results were divided into five subgroups. Subgroup analysis was performed to compare the effect of massage therapy at different time points. Massage therapy showed a significant effect compared to the control [SMD = 2.00, 95% CI (1.17 to 2.83), P < 0.00001], and the test for subgroup differences was significant (I2 = 86, P < 0.00001), as shown in Figure 5.
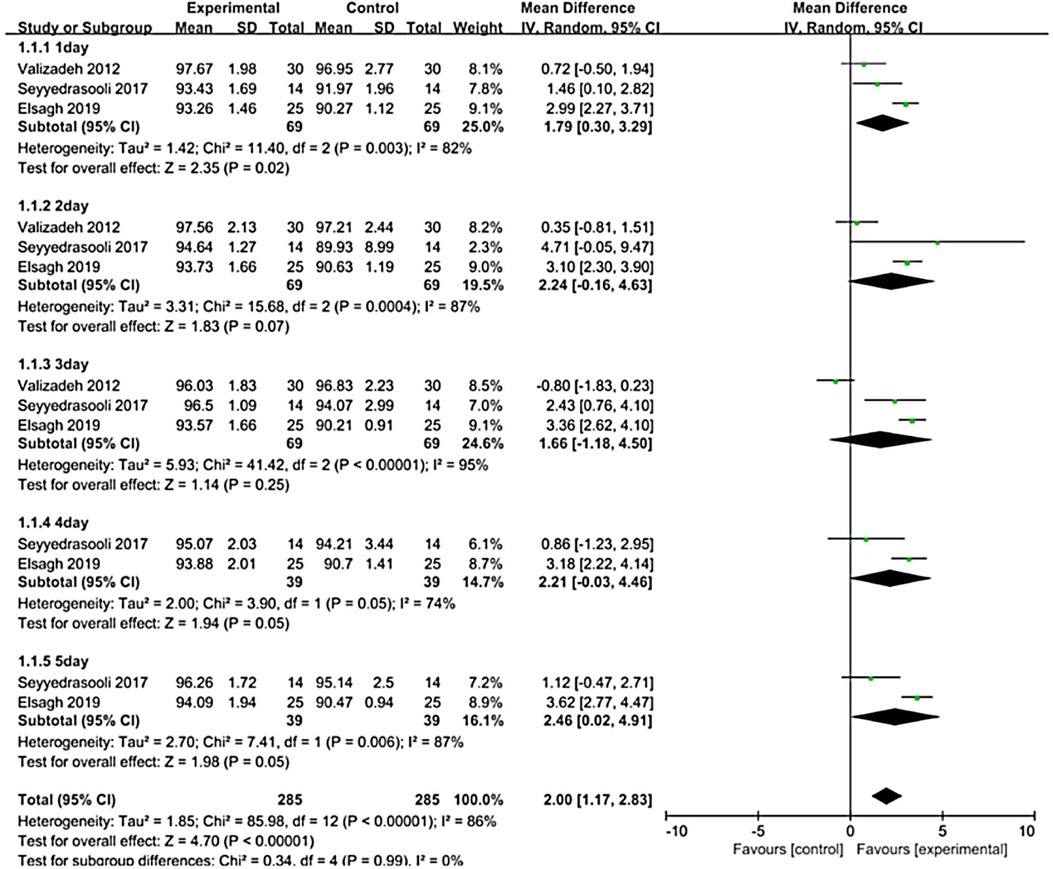
Figure 5. Forest plot of massage therapy vs. standard care on oxygen saturation.
The findings of the current meta-analysis demonstrated that massage therapy can strengthen the maternal-infant attachment and increase oxygen saturation; however, there was no significant effect of massage therapy on motor, reflex, temperature, or calorie intake.
The effects of massage therapy on preterm infants and their parents have long been of interest, and prior systematic reviews reported the effects of massage therapy on weight gain (44) and maternal and neonatal fatigue (44, 45) in neonatal intensive care units, but did not specifically focus on mother-infant attachment, motor function, reflexes, caloric intake, oxygen saturation levels, or body temperature.
All 15 included studies used massage therapy as an intervention for preterm infants. Twelve of these studies used the Field protocol (21–23, 25–28, 37–41), which consists of massage therapy starting at a corrected gestational age of 35 weeks for five consecutive days, one hour after feeding, three times a day for 15 min. Each treatment was divided into 5 min of tactile stimulation, followed by 5 min of kinesthetic stimulation, and then another 5 min of tactile stimulation (46). One study used a massage protocol developed by the researcher himself (23), the main elements of which were that the massage was first performed on both shoulders, starting at the neck, with the infant in the prone position. The massage was then moved from the upper back to the lumbar region. Subsequently, the two upper and lower limbs were massaged in the supine position. In each area, the massage consisted of 20 gentle strokes. One study used the Vimala protocol (15), which is a massage protocol used primarily in full-term infants, where the infant's torso is divided into six regions: face, upper extremities, chest, abdomen, lower extremities, and back, ending with stretching of the limbs (47). One study used abdominal massage (32), which was performed twice a day for 5 days, at 9 a.m. and 9 p.m., before feeding (48).
This meta-analysis showed a statistically significant effect of massage therapy on maternal-infant attachment; however, due to the small sample size, a positive effect of massage therapy on maternal-infant attachment could not be fully demonstrated. Nevertheless, all of the included studies aimed to demonstrate the effectiveness of massage therapy as an intervention. Effective intervention measures can mitigate maternal anxiety, foster mother-infant attachment, and ameliorate the developmental delay experienced by preterm infants (49, 50). Mokaberian (40) studied the anxiety and association of physical massage with Iranian mothers of preterm infants. The results showed that maternal attachment levels increased significantly in the experimental group. Therefore, massage therapy may be useful as a low-cost, non-pharmacological treatment to improve the psychological state of mothers. Lai's research has also shown that massage has a positive impact on the mother-infant relationship and the neurological development of premature infants (51), consistent with previous research (21, 52).
Developmental care of preterm infants is a current concern. Massage therapy is one of the more effective care strategies (52). This systematic review confirmed that there was a statistically significant difference in oxygen saturation in preterm infants after massage therapy [SMD = 2.00, 95% CI (1.17 to 2.83), P < 0.001]. A comparison of the mean daily oxygen saturation of preterm infants who underwent a 5-day massage with control infants showed that there was no statistical difference between the two groups before the start of the massage. On the first day of receiving the massage, the experimental group of infants had an average of 2.99 times higher oxygen saturation than the control infants, and this number increased to 3.62 on the fifth day of receiving the massage (39). Infant massage has been clinically recommended for decades (53). A study by Valizadeh (43) showed that prone position massage in preterm infants was effective in increasing oxygen saturation, which is consistent with the results of the present study.
Some studies have shown that massage therapy can improve reflexes in preterm infants, for example, Solkoff (54) conducted a trial assessing the effect of tactile stimulation using the Brazelton's Neonatal Behavior Assessment Score (NBAS), which demonstrated the beneficial effects of massage in improving neurobehavior in preterm infants. After 10 days of stimulation, the difference in a number of indicators, including habituation and reflexes, was greater than two points, which is inconsistent with the results of the meta-analysis in this article, and there are studies using the same scale to assess whether massage improves neurobehavioral development in preterm infants that have shown no significant improvement in the response to massage therapy in preterm infants (23). Further clinical studies are needed because of the small amount of relevant research.
Caloric intake is usually studied along with weight gain; however, caloric intake does not equate to weight gain, and several randomized controlled trials have shown that massage therapy in preterm infants promotes weight gain but does not significantly affect caloric intake (15, 55). A systematic review also showed that massage in preterm infants did not promote increased caloric intake (56). This is consistent with the results of the present study. However, one study found that preterm infants who received massage had an increase in caloric intake, with no difference in weight gain between the two groups (38). Massage therapy is effective as a low-cost, non-pharmacological intervention to improve physical and motor development in newborns (57), which is consistent with the results of this systematic review. It was concluded that very low birth weight infants who received massage had a higher improvement in motor performance scores (Test of Infant Motor Performance, TIMP) (P = 0.043), suggesting that massage may positively affect motor outcomes in a subgroup of very low birth weight infants with lower motor abilities (24). In this study, we found that temperature assessment of preterm neonates randomly assigned to either the control or massage therapy group did not show a statistically significant difference in temperature change between the two groups [MD = 0.11, 95% CI (−0.08 to 0.31), P = 0.25], which is in line with the results of a previous study (26). However, a related study concluded that there was no significant difference in temperature between infants who received massage and control infants during the treatment period, but there was a statistically significant difference in temperature changes before and after massage in preterm infants who received massage therapy, with the post-treatment temperature significantly higher than the pre-treatment temperature (P < 0.001) (27).
The main limitation of this systematic review is that, in most of the pooled studies, some of the outcomes were not the primary outcomes of interest. Examples include indicators such as weight gain and breastfeeding status. Moreover, in this systematic study, the sample of included studies was small and only two papers reported on maternal-infant attachment among the outcome indicators of interest to us; further studies with expanded sample sizes are needed.
In conclusion, this systematic review and meta-analysis suggests that preterm infants may benefit from massage therapy because of its potential to improve oxygen saturation, maternal-child attachment, and quality of life in preterm infants. However, due to the limited sample size, further research is needed on the use of massage therapy in the preterm infant population.
YZ: Conception and design, drafting of the manuscript, and critical revision of the manuscript for important intellectual content. CD: Substantial contributions to interpretation of data for the work and drafting the work or revising it critically for important intellectual content. LC: Acquisition of data and analysis and interpretation of data. HL: Final approval of the version to be published and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
This study was sponsored by a grant from the project 22JR4ZA023, supported by Science and Technology Department of Gansu province.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fped.2023.1198730/full#supplementary-material
1. World Health New global estimates on preterm birth published. (2018). Available at: https://www.who.int/reproductivehealth/global-estimates-preterm-birth/en/
2. Vogel JP, Chawanpaiboon S, Moller AB, Watananirun K, Bonet M, Lumbiganon P. The global epidemiology of preterm birth. Best Pract Res Clin Obstet Gynaecol. (2018) 52:3–12. doi: 10.1016/j.bpobgyn.2018.04.003
3. Hossain Z, Qasem WA, Friel JK, Omri A. Effects of total enteral nutrition on early growth, immunity, and neuronal development of preterm infants. Nutrients. (2021) 13(8):2755. doi: 10.3390/nu13082755
4. Strydom K, Van Niekerk E, Dhansay MA. Factors affecting body composition in preterm infants: assessment techniques and nutritional interventions. Pediatr Neonatol. (2019) 60(2):121–8. doi: 10.1016/j.pedneo.2017.10.007
5. Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. (2012) 379(9832):2162–72. doi: 10.1016/S0140-6736(12)60820-4
6. Barker DJ. The fetal and infant origins of adult disease. Br Med J. (1990) 301(6761):1111. doi: 10.1136/bmj.301.6761.1111
7. Niemi AK. Review of randomized controlled trials of massage in preterm infants. Children (Basel). (2017) 4(4):21. doi: 10.3390/children4040021
8. Stephens BE. Neurodevelopmental outcome of the preterm infant pediatric clinics of North America. Pediatr Clin. North Am. (2009) 56:631–46.19501696
9. Liao YC, Wan YH, Chen PH, Hsieh LY. Efficacy of medium-chain triglyceride oil massage on growth in preterm infants: a randomized controlled trial: a CONSORT-compliant article. Medicine (Baltimore). (2021) 100(30):e26794. doi: 10.1097/MD.0000000000026794
10. Field T. Massage therapy research review. Complement Ther Clin Pract. (2014) 20(4):224–9. doi: 10.1016/j.ctcp.2014.07.002
11. Ang JY, Lua JL, Mathur A, Thomas R, Asmar BI, Savasan S, et al. A randomized placebo-controlled trial of massage therapy on the immune system of preterm infants. Pediatrics. (2012) 130:1549–58. doi: 10.1542/peds.2012-0196
12. Abdallah B, Badr LK, Hawwari M. The efficacy of massage on short term and long term outcomes in preterm infants. Infant Behav Dev. (2013) 36:662–9. doi: 10.1016/j.infbeh.2013.06.009
13. Field T. Massage therapy research review. Complement Ther Clin Pract. (2016) 24:19–31. doi: 10.1016/j.ctcp.2016.04.005
14. Procianoy RS, Mendes EW, Silveira RC. Massage therapy improves neurodevelopment outcome at two years corrected age for very low birth weight infants. Early Hum Dev. (2010) 86:7–11. doi: 10.1016/j.earlhumdev.2009.12.001
15. Gonzalez AP, Vasquez-Mendoza G, García-Vela A, Guzmán-Ramirez A, Salazar-Torres M, Romero-Gutierrez G. Weight gain in preterm infants following parent-administered vimala massage: a randomized controlled trial. Am J Perinatol. (2009) 26:247–52. doi: 10.1055/s-0028-1103151
16. Mendes EW, Procianoy RS. Massage therapy reduces hospital stay and occurrence of late-onset sepsis in very preterm neonates. J Perinatol. (2008) 28:815–20. doi: 10.1038/jp.2008.108
17. Mrljak R, Arnsteg Danielsson A, Hedov G, Garmy P. Effects of infant massage: a systematic review. Int J Environ Res Public Health. (2022) 19(11):6378. doi: 10.3390/ijerph19116378
18. Mollà-Casanova S, Sempere-Rubio N, Muñoz-Gómez E, Aguilar-Rodríguez M, Serra-Añó P, Inglés M. Effects of massage therapy alone or together with passive mobilisations on weight gain and length of hospitalisation in preterm infants: systematic review and meta-analysis. Early Hum Dev. (2023) 182:105790. doi: 10.1016/j.earlhumdev.2023.105790
19. Field T, Diego M, Hernandez-Reif M. Preterm infant massage therapy research: a review. Infant Behav Dev. (2010) 33(2):115–24. doi: 10.1016/j.infbeh.2009.12.004
20. Lindensmith R. Interventions to improve maternal-infant relationships in mothers with postpartum mood disorders. MCN Am J Matern Child Nurs. (2018) 43(6):334–40. doi: 10.1097/NMC.0000000000000471
21. Shoghi M, Sohrabi S, Rasouli M. The effects of massage by mothers on mother-infant attachment. Altern Ther Health Med. (2018) 24(3):34–39.29101776
22. Ferber SG, Kuint J, Weller A, Feldman R, Dollberg S, Arbel E, et al. Massage therapy by mothers and trained professionals enhances weight gain in preterm infants. Early Hum Dev. (2002) 67(1-2):37–45. doi: 10.1016/s0378-3782(01)00249-3
23. Arora J, Kumar A, Ramji S. Effect of oil massage on growth and neurobehavior in very low birth weight preterm neonates. Indian Pediatr. (2005) 42(11):1092–100.16340050
24. Ho YB, Lee RS, Chow CB, Pang MY. Impact of massage therapy on motor outcomes in very low-birthweight infants: randomized controlled pilot study. Pediatr Int. (2010) 52(3):378–85. doi: 10.1111/j.1442-200X.2009.02964.x
25. Campbell M, Jacobs L. The effect of parent-administered infant massage on the developmental outcomes of premature infants. South African Journal of Occupational Therapy. (2021) 51(1):36–43. doi: 10.17159/2310-3833/2021/vol51n1a6
26. Elmoneim MA, Mohamed HA, Awad A, El-Hawary A, Salem N, El Helaly R, et al. Effect of tactile/kinesthetic massage therapy on growth and body composition of preterm infants. Eur J Pediatr. (2021) 180(1):207–15. doi: 10.1007/s00431-020-03738-w
27. Diego MA, Field T, Hernandez-Reif M. Temperature increases in preterm infants during massage therapy. Infant Behav Dev. (2008) 31(1):149–52. doi: 10.1016/j.infbeh.2007.07.002
28. Elsagh A, Lotfi R, Amiri S, Gooya HH. Comparison of massage and prone position on heart rate and blood oxygen saturation level in preterm neonates hospitalized in neonatal intensive care unit: a randomized controlled trial. Iran J Nurs Midwifery Res. (2019) 24(5):343–7. doi: 10.4103/ijnmr.IJNMR_34_18
29. World Health Organization. International classification of diseases and related health problems, 10th revision(2007). Available at: http://www.who.int/classifications/apps/icd/icd10online
30. Nakano Y. Adult-Onset diseases in low birth weight infants: association with adipose tissue maldevelopment. J Atheroscler Thromb. (2020) 27(5):397–405. doi: 10.5551/jat.RV17039
31. Vickers A, Ohlsson A, Lacy JB, Horsley A. Massage for promoting growth and development of preterm and/or low birth-weight infants. Cochrane Database Syst Rev. (2000) (2):CD000390. doi: 10.1002/14651858.CD000390
32. Seyyedrasooli A, Asadollahi M, Babaei H, Musavi S, Kiani S. Effects of Abdominal Massage and Non-Nutritive Sucking on Physiological Parameters of Preterm Infants: A Randomized Clinical Trial (RCT). Int J Pediatr-Massha. (2017) 5(6):5167–81. doi: 10.22038/ijp.2017.23025.1928
33. Jacobsen H, Ivarsson T, Wentzel-Larsen T, Smith L, Moe V. Attachment security in young foster children: continuity from 2 to 3 years of age. Attach Hum Dev. (2014) 16(1):42–57. doi: 10.1080/14616734.2013.850102
34. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. (2011) 343:d5928. doi: 10.1136/bmj.d5928
35. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327(7414):557–60. doi: 10.1136/bmj.327.7414.557
36. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. (2009) 6(7):e1000100. doi: 10.1371/journal.pmed.1000100
37. Diego MA, Field T, Hernandez-Reif M. Vagal activity, gastric motility, and weight gain in massaged preterm neonates. J Pediatr. (2005) 147(1):50–5. doi: 10.1016/j.jpeds.2005.02.023
38. Diego MA, Field T, Hernandez-Reif M. Preterm infant weight gain is increased by massage therapy and exercise via different underlying mechanisms. Early Hum Dev. (2014) 90(3):137–40. doi: 10.1016/j.earlhumdev.2014.01.009
39. Hernandez-Reif M, Diego M, Field T. Preterm infants show reduced stress behaviors and activity after 5 days of massage therapy. Infant Behav Dev. (2007) 30(4):557–61. doi: 10.1016/j.infbeh.2007.04.002
40. Mokaberian M, Noripour S, Sheikh M, Mills PJ. Examining the effectiveness of body massage on physical status of premature neonates and their mothers' psychological status. Early Child Dev Care. (2021) 192(14):2311–25. doi: 10.1080/03004430.2021.2006194
41. Valizadeh S, Hosseini MB, Asghari Jafarabadi M, Ajoodanian N. The effects of massage with coconut and sunflower oils on oxygen saturation of premature infants with respiratory distress syndrome treated with nasal continuous positive airway pressure. J Caring Sci. (2012) 1(4):191–9. doi: 10.5681/jcs.2012.027
42. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21(11):1539–58. doi: 10.1002/sim.1186
43. Sterne JA, Sutton AJ, Ioannidis JP, Terrin N, Jones DR, Lau J, et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ. (2011) 343:d4002. doi: 10.1136/bmj.d4002
44. Lu LC, Lan SH, Hsieh YP, Lin LY, Chen JC, Lan SJ. Massage therapy for weight gain in preterm neonates: A systematic review and meta-analysis of randomized controlled trials. Complement Ther Clin Pract. (2020) 39:101168. doi: 10.1016/j.ctcp.2020.101168
45. Abadian L, Pouraboli B, Ranjbar H, Shariat M, Otadi K, Nia NA. Comparison of the effect of massage and music on fatigue in mothers with premature newborns admitted to the neonatal intensive care unit: a randomized clinical trial. J Chiropr Med. (2020) 19(4):241–8. doi: 10.1016/j.jcm.2020.06.003
46. Field TM, Schanberg SM, Scafidi F, Bauer CR, Vega-Lahr N, Garcia R, et al. Tactile/kinesthetic stimulation effects on preterm neonates. Pediatrics. (1986) 77(5):654–8. doi: 10.1542/peds.77.5.654
47. McClure V. Infant massage: A handbook for loving parents. 3rd ed. New York: Bantam Books (2002). 69–128.
48. Tekgündüz KŞ, Gürol A, Apay SE, Caner İ. Effect of abdomen massage for prevention of feeding intolerance in preterm infants. Ital J Pediatr. (2014) 40(1):89. doi: 10.1186/s13052-014-0089-z
49. Kraft KE, Jaschke AC, Ravensbergen AG, Feenstra-Weelink A, van Goor MEL, de Kroon MLA, et al. Maternal Anxiety, infant stress, and the role of live-performed music therapy during NICU stay in The Netherlands. Int J Environ Res Public Health. (2021) 18(13):7077. doi: 10.3390/ijerph18137077
50. Schmücker G, Brisch KH, Köhntop B, Betzler S, Österle M, Pohlandt F, et al. The influence of prematurity, maternal anxiety, and infants' neurobiological risk on mother-infant interactions. Infant Ment Health J. (2005) 26(5):423–41. doi: 10.1002/imhj.20066
51. Lai MM, D'Acunto G, Guzzetta A, Boyd RN, Rose SE, Fripp J, et al. PREMM: preterm early massage by the mother: protocol of a randomised controlled trial of massage therapy in very preterm infants. BMC Pediatr. (2016) 16(1):146. doi: 10.1186/s12887-016-0678-7
52. Bennett C, Underdown A, Barlow J. Massage for promoting mental and physical health in typically developing infants under the age of six months. Cochrane Database Syst Rev. (2013) 2013(4):CD005038. doi: 10.1002/14651858
53. Massaro AN, Hammad TA, Jazzo B, Aly H. Massage with kinesthetic stimulation improves weight gain in preterm infants. J Perinatol. (2009) 29(5):352–7. doi: 10.1038/jp.2008.230
54. Solkoff N, Matuszak D. Tactile stimulation and behavioral development among low birth weight infants. Child Psychiat Hum Dev. (1973) 6:33–7. doi: 10.1007/BF01434430
55. Field T, Diego M, Hernandez-Reif M, Dieter JN, Kumar AM, Schanberg S, et al. Insulin and insulin-like growth factor-1 increased in preterm neonates following massage therapy. J Dev Behav Pediatr. (2008) 29:463–6. doi: 10.1097/DBP.0b013e3181856d3b
56. Álvarez MJ, Fernández D, Gómez-Salgado J, Rodríguez-González D, Rosón M, Lapeña S. The effects of massage therapy in hospitalized preterm neonates: a systematic review. Int J Nurs Stud. (2017) 69:119–36. doi: 10.1016/j.ijnurstu.2017.02.009
Keywords: massage therapy, mothers, preterm infants, meta-analysis, systematic review
Citation: Zhang Y, Duan C, Cheng L and Li H (2023) Effects of massage therapy on preterm infants and their mothers: a systematic review and meta-analysis of randomized controlled trials. Front. Pediatr. 11:1198730. doi: 10.3389/fped.2023.1198730
Received: 2 April 2023; Accepted: 4 August 2023;
Published: 31 August 2023.
Edited by:
Gianluca Terrin, University of Rome La Sapienza, ItalyReviewed by:
Giovanni Boscarino, Ospedale Universitario di Parma, Italy© 2023 Zhang, Duan, Cheng and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Haihong Li OTM5NTEzMTE1QHFxLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.