
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Pediatr., 17 July 2023
Sec. Neonatology
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1192268
This article is part of the Research TopicSARS-CoV-2: Implications for Maternal-Fetal-Infant and Perinatal Mortality, Morbidity, Pregnancy Outcomes and Well-BeingView all 15 articles
 Yi-Heng Dai1,†Caihuan Li2,†Guilong Yuan3,†Wenhui Mo4,†
Yi-Heng Dai1,†Caihuan Li2,†Guilong Yuan3,†Wenhui Mo4,† Jun Chen1Runzhong Huang5Zhonghe Wan6Duohua Lin7Xiangming Zhong8Huanqiong Li9Ling Liu10
Jun Chen1Runzhong Huang5Zhonghe Wan6Duohua Lin7Xiangming Zhong8Huanqiong Li9Ling Liu10 Jipeng Shi1*
Jipeng Shi1*
Objective: To investigate the clinical characteristics and outcomes of newborns infected with coronavirus disease 2019 (COVID-19) during the Omicron wave.
Methods: From December 1, 2022, to January 4, 2023, clinical data were collected from neonates with COVID-19 who were admitted to 10 hospitals in Foshan City, China. Their epidemiological histories, clinical manifestations and outcomes were analysed. The neonates were divided into symptomatic and asymptomatic groups. The t test or χ2 test was used for comparisons between groups.
Results: A total of 286 children were diagnosed, including 166 males, 120 females, 273 full-term infants and 13 premature infants. They were 5.5 (0–30) days old on average when they were admitted to the hospital. These children had contact with patients who tested positive for COVID-19 and were infected through horizontal transmission. This study included 33 asymptomatic and 253 symptomatic patients, among whom 143 were diagnosed with upper respiratory tract infections and 110 were diagnosed with pneumonia. There were no severe or critical patients. Fever (220 patients) was the most common clinical manifestation, with a duration of 1.1 (1–6) days. The next most common clinical manifestations were cough with nasal congestion or runny nose (4 patients), cough (34 patients), poor appetite (7 patients), shortness of breath (15 patients), and poor general status (1 patient). There were no significant abnormalities in routine blood tests among the neonates infected with COVID-19 except for mononucleosis. However, compared with the asymptomatic group, in the symptomatic group, the leukocyte and neutrophil granulocyte counts were significantly decreased, and the monocyte count was significantly increased. C-reactive protein (CRP) levels were significantly increased (≥10 mg/L) in 9 patients. Myocardial enzyme, liver function, kidney function and other tests showed no obvious abnormalities.
Conclusions: In this study, neonates infected with the Omicron variant were asymptomatic or had mild disease. Symptomatic patients had lower leucocyte and neutrophil levels than asymptomatic patients.
The coronavirus disease 2019 (COVID-19) pandemic that started in 2019 spread worldwide, and the COVID-19 epidemic in China is still ongoing. In particular, at the end of 2022, the Omicron variant spread to mainland China. The rapid spread of COVID-10 posed a great threat to a vast number of adults, children and newborns (1, 2). Some studies have shown that infection with COVID-19 is not commonly observed in hospitalized newborns (3). The majority of newborns have mild clinical manifestations and only require short-term hospitalization for treatment and most newborns present with symptoms of fever, upper respiratory tract infections, and lower respiratory tract infections (4). Multiple studies from different countries and regions and a meta-analysis have shown that the typical clinical manifestations of children with COVID-19 infection are fever, cough, and shortness of breath (1, 2, 5). Some studies have shown that common symptoms in newborns after contracting COVID-19 include shortness of breath and fever, and most newborns who are infected with the virus are asymptomatic or have mild symptoms and do not require respiratory support (6, 7). Another study showed that the most common symptoms observed in newborns infected with COVID-19 were fever, feeding intolerance, and cough, with myocarditis being the most common complication in those with severe-critical illness (8).
Previous studies showed that after COVID-19 infection, newborns generally had only mild clinical manifestations and did not need special treatment (9, 10). Nevertheless, certain studies have revealed severe scenarios. For instance, a study conducted in Brazil revealed that neonates who contracted COVID-19 during the initial phase of the pandemic experienced more severe clinical manifestations, which led to higher mortality rates. Such newborns displayed accelerated disease progression, longer hospital stays, and more pronounced respiratory distress, laryngospasm, and cough (11). Laboratory tests indicated a normal range of white blood cells and reduced lymphocyte levels (1, 2, 5, 6). However, newborns often have abnormal test results and imaging findings, including positive results for neutropenia and/or mononucleosis but not lymphocytopenia (12). There are also studies reporting that after infection with COVID-19, a reduction in platelet, lymphocyte, haemoglobin, eosinophil, and basophil counts and an increase in the neutrophil count, neutrophil-to-lymphocyte ratio, and platelet-to-lymphocyte ratio were commonly observed, and these indicators were associated with clinical prognosis (13, 14).
The clinical presentation and severity of COVID-19 have changed with the emergence of the Alpha, Beta, Delta and Omicron SARS-CoV-2 variants in different infection waves. Most published studies of neonatal COVID-19 infection were conducted before the Omicron wave. There is limited information on the clinical characteristics of neonatal COVID-19 infection caused by the Omicron variant. In this study, the data of neonates with COVID-19 who were admitted to 10 hospitals in Foshan from December 1, 2022, to January 4, 2023, were collected and analysed to investigate clinical characteristics and outcomes to provide some reference for the prevention and management of Omicron among newborns during the epidemic.
During the Omicron variant wave, it is recommended that all hospitalized newborns undergo routine COVID-19 testing. Furthermore, if a mother exhibits any symptoms of a respiratory tract infection, such as fever or cough, her newborn must be closely monitored in the maternal-child ward and undergo COVID-19 testing. Between December 1, 2022, and January 4, 2023, 286 neonates infected with COVID-19 were admitted to 10 hospitals. These newborns infected with COVID-19 were in the same room as their mothers after birth. If these newborns develop respiratory symptoms such as cough and fever, they should be admitted to the neonatology department for further observation. If a mother has symptoms of respiratory tract infection or has a history of contact with COVID-19-positive patients, the mother needs to take protective measures such as wearing a mask and washing hands before contact with children.
The inclusion criteria were as follows: (1) full-term infant age <28 days, preterm infant corrected gestational age <40 weeks; (2) pharyngeal swab results of COVID-19 nucleic acid test were positive or antigen-positive. Ethics approval was obtained from Foshan Maternity and Child Healthcare Hospital (approval number: FSFY-MEC-2023-022) in accordance with the Declaration of Helsinki.
There were a total of 13 premature infants included in this study. Any infant whose corrected gestational age exceeded 40 weeks did not meet our admission criteria for the neonatology department.
Pharyngeal swab samples were analysed at COVID-19 laboratories in several participating hospitals. The main kit used was the novel coronavirus pneumonia Nucleic Acid Detection Kit of Wuhan Mingde Biotechnology Co., Ltd. (National Instrument Note 20203400212), which uses PCR-fluorescence probe technology for detection. The procedures were performed according to the technical specifications and quality control specifications of the China National Clinical Laboratory Center.
Antigens in throat swab samples were detected by the Novel Coronavirus (2019-nCoV) Antigen Detection Kit (colloidal gold method) of Xiamen Aode Biotechnology Co., Ltd. The results are analysed as follows: if two dark or light red or purple bands appear, one in the testing area (T) and the other in the quality control area (C), this indicates a positive result. If only one red or purple band appears in the quality control area (C) and no band appears in the detection area (T), this indicates a negative result. If there is no red or purple band in the quality control area (C), regardless of whether there is a band in the detection area (T), the result is invalid, and retesting is necessary.
The hospitalized neonates were registered, and information such as sex, age, gestational age, birth weight, epidemiological history, clinical symptoms, laboratory results, imaging results, treatment and length of stay were collected, and a clinical database was established.
The COVID-19 Pneumonia (Trial Version 9) criteria issued by the National Health Commission are used for the diagnosis and classification of cases (15). Asymptomatic infection was defined as those whose nucleic acid test met the diagnostic criteria but without any symptoms or signs; mild infection was defined as only mild clinical manifestations without imaging manifestations of pneumonia. Clinical and imaging manifestations of pneumonia were considered signs of general infection. Severe infection was defined as persistent high fever for more than 3 days, shortness of breath, hypoxemia, dyspnoea, lethargy, convulsion, food resistance or feeding difficulty with significant imaging findings of pulmonary inflammation. A critical infection was defined as secondary respiratory failure requiring respiratory support, shock, or a combination of other organ failures. The date when symptoms of COVID-19 infection appeared and the nucleic acid or COVID-19 antigen result was positive was considered the onset date.
According to the discharge conditions stated in the Perinatal and Neonatal COVID-19 Infection Prevention and Control Plan (third edition), patients could be discharged once the patient's condition was stable, vital signs such as respiration and body temperature were normal, feeding tolerance was achieved, the family could provide reasonable care, and the discharge criteria were met (16, 17).
We used SPSS 20.0 for statistical analysis, and measurement data are expressed as x̅ ± S, minimum values and maximum value if necessary. Comparisons between groups were performed by t test or t'. The chi-square test or Fisher's exact probability method was used to compare the groups based on the statistical data. A bilateral value of P < 0.05 was considered statistically significant.
Most of the 286 patients had a contact history with family members who were positive for COVID-19. There were 166 male and 120 female patients, including 13 premature infants. Of the 286 newborns infected with COVID-19, 39 patients lacked data on amniotic fluid status. These infants had an average gestational age of 38.7 (29–41) weeks and an average birth weight of 2,949.4 ± 971.9 g. In total, 97 of the newborns were delivered by caesarean section, and 189 patients were delivered naturally. At admission, the average age of the patients was 5.5 (0–30) days. Among them, 134 newborns were exclusively breastfed, 14 newborns were fed formula, and 138 newborns received mixed feeding, as shown in Table 1.
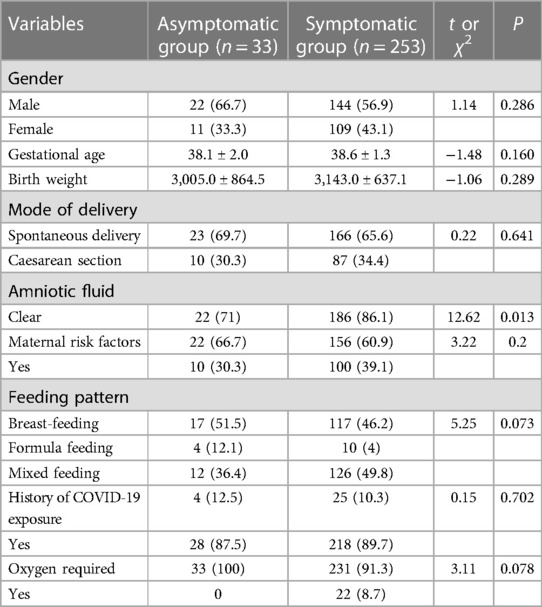
Table 1. Baseline characteristics of neonates infected with COVID-19.
Chest x-ray was performed for 227 patients; 64 patients showed no abnormality or thickened texture, 6 patients showed bronchitis-like changes, 157 (110 patients diagnosed with pneumonia and 47 who did not meet the diagnostic criteria for pneumonia) patients showed pneumonia-like changes, and 2 were diagnosed with pneumonia by chest CT examination. All children were given routine symptomatic treatment after admission and were discharged after their condition improved. The median length of stay was 5.6 (2–13) days.
Patients with fever, cough, nasal congestion or gastrointestinal symptoms were all regarded as symptomatic infected persons. There were 253 (88.5%) newborns with symptoms (Table 2). Among the children with symptomatic infection, 143 patients had mild infection, and 110 patients had common infections, such as fever (220 cases), cough with nasal congestion or runny nose (4 cases), cough (34 cases), poor appetite (7 cases), shortness of breath (15 cases), and poor general status (1 case). Fever was the most common clinical manifestation of COVID-19 infection, with fever occurring in 220 patients (76.9%), while 66 patients (23.1%) did not have a fever. Of those with fever, 181 had symptoms of fever alone. Some newborns exhibited noticeable respiratory symptoms, such as rapid breathing and breathing difficulties, necessitating respiratory support such as mechanical ventilation or noninvasive ventilation with a breathing machine, as shown in Table 2. No deaths occurred among these infants.
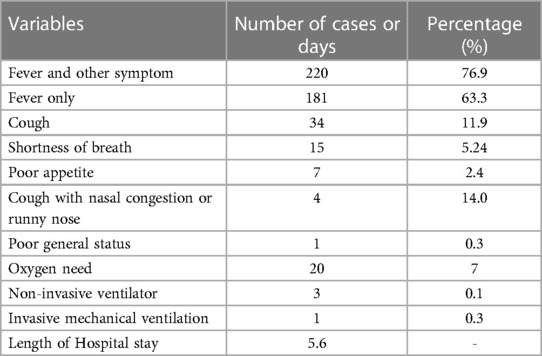
Table 2. Clinical symptom, treatment and short-term outcomes.
The total number of white blood cells (9.7 ± 4.6) × 109/L in the neonates infected with COVID-19 was within the normal range. However, the total number of leukocytes in symptomatic neonates was lower than that in asymptomatic neonates (9.4 ± 4.6 vs. 11.7 ± 4.2) × 109/L), and the absolute value of neutrophils in the symptomatic neonates was lower than that in the asymptomatic neonates (3.7 ± 2.5 vs. 6.1 ± 3.6) × 109/L). Neonates infected with COVID-19 had significantly higher monocyte counts (2.2 ± 1.5) × 109/L than normal neonates. The absolute monocyte count was significantly higher in symptomatic neonates (2.2 ± 1.5) × 109/L than in asymptomatic neonates (1.7 ± 1.1) × 109/L. The percentage of monocytes was also significantly higher in the symptomatic group than in the asymptomatic group (22.8 ± 7.3 vs. 15.4 ± 9.1) × 109/L, and the differences were statistically significant (P < 0.05).
The procalcitonin (PCT) level of neonates infected with COVID-19 was 0.9 ± 6.5 ng/ml, which was within the normal range. The CRP levels were normal (3.4 ± 9.7 mg/L) in the majority of patients, and only 9 patients had a significant increase in CRP levels (≥10 mg/L), suggesting the possibility of bacterial infection due to elevated levels of CRP. However, the blood culture results for these patients were negative. Myocardial enzyme CK-MB, alanine aminotransferase, aspartate aminotransferase, uric acid, urea, creatinine and other indexes in blood biochemistry were all within the normal range, as shown in Table 3.
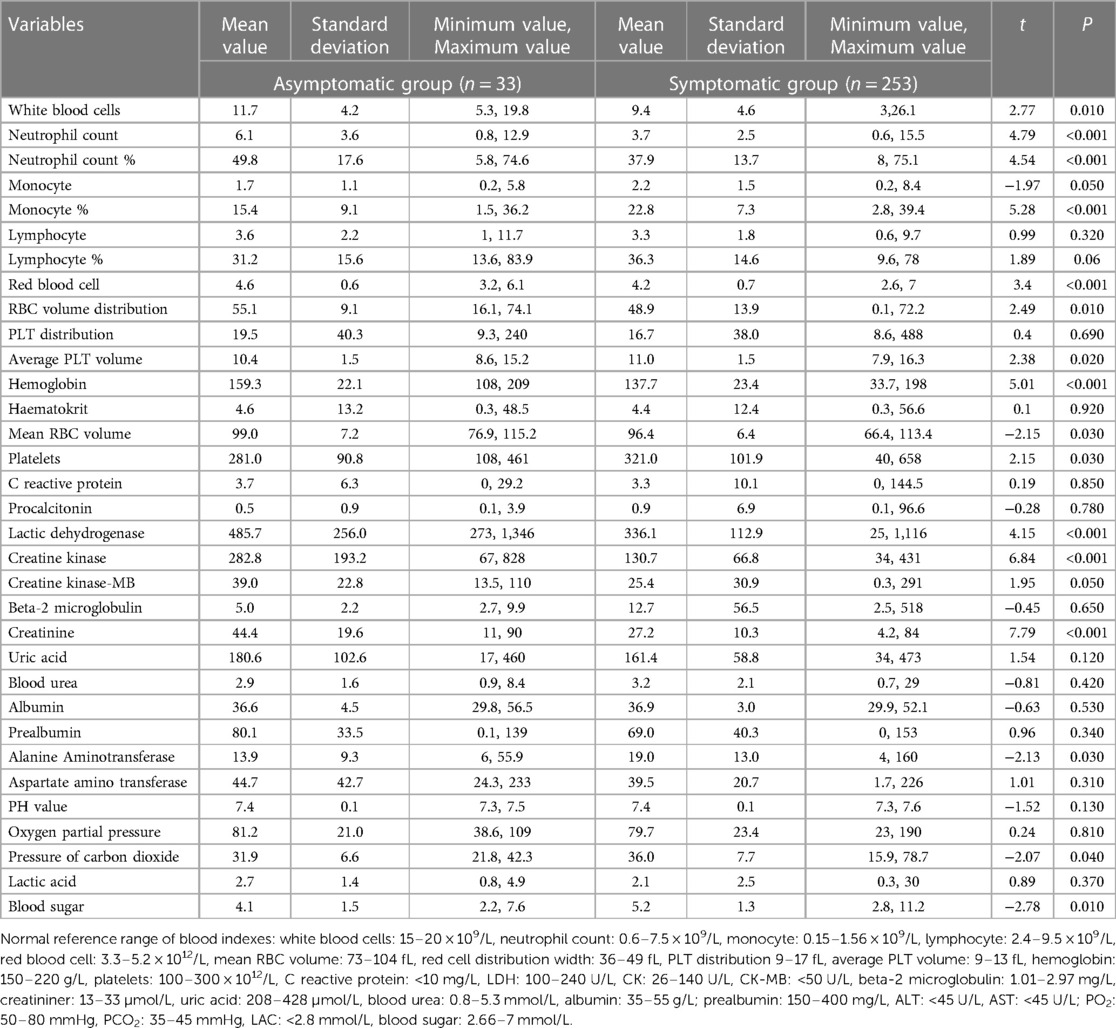
Table 3. Laboratory test results.
A total of 286 children were admitted to the hospital after routine symptomatic treatment, and they were discharged after their condition improved. The average duration of hospitalization for neonates infected with COVID-19 was 5.6 (2.1–13) days.
In the neonatology department, some treatments were routinely given. Newborns with fever were typically managed with physical cooling methods, such as the application of ice pillows or reduction of the temperature of warm boxes. The use of drugs such as ibuprofen to lower fever in newborns was uncommon. When newborns experienced cough symptoms, they were often treated with a nebulized budesonide suspension, while oral ambroxol hydrochloride expectorant medication was recommended for newborns with phlegm. However, importantly, this treatment approach may not be considered completely standardized.
A total of 109 patients were treated with antibiotics prophylactically upon admission, the infection index became normal within 3 days, and the antibiotics were stopped after bacterial infection was excluded. No definitive evidence of bacterial infection was found in newborns with COVID-19 infection. In the study, prophylactic antibiotics were used for newborns with fever if bacterial infections could not be ruled out for some time. The commonly used drugs were ampicillin (50 mg/kg, q12h or q8h, depending on gestational age and postnatal age), piperacillin tazobactam (100 mg/kg, q12h or q8h), ceftazidime (50 mg/kg, q12h or q8h) and cefotaxime (50 mg/kg, q12h or q8h).
Some newborns and premature infants in this study were fed by nasogastric feeding due to their need for respiratory support or poor sucking ability. Once these newborns were weaned off mechanical ventilation or had developed a stronger suckling ability, the nasogastric tube was removed and replaced with self-suction.
During the COVID-19 pandemic, numerous published studies on COVID-19 infection in children, including newborns, were conducted prior to the Omicron variant outbreak. Because they have generally low immune function, newborns are more likely to suffer from COVID-19, so they need more attention. COVID-19 has mutated several times. The Omicron variant has become widespread, and the World Health Organization has defined it as the fifth variant of concern (18, 19). In a systematic review that included all articles published from December 1, 2019, to May 12, 2020, a quarter of newborns were asymptomatic, and the rest showed typical acute respiratory infections and/or gastrointestinal symptoms. Most did not need oxygen support, their average length of hospital stay was 10 days, and their prognoses were good (20). However, there have been few reports of newborn infections during the Omicron epidemic, and the clinical characteristics and prognoses of these newborns are not very clear.
The Foshan outbreak was caused by a variant of Omicron, which infected the vast majority of the population. The clinical symptoms in children after infection are not the exact same as those in adults (21). The main manifestations in children are fever, cough, sputum, nasal congestion, runny nose, headache, diarrhoea, abdominal distension, and anorexia, and some severe patients may have convulsion (5, 22). There have been scattered reports of COVID-19 infections among newborns in China (23, 24). The data are limited, and epidemiological investigations and clinical case analyses are lacking. In contrast, in most cohort studies of neonates, mild symptoms were reported, with common symptoms including shortness of breath, respiratory distress, fever, and symptoms related to gastrointestinal disorders (10, 25). In this study, the vast majority of newborns were in the same room as their mother and were breastfed. Mothers who have been infected with COVID-19 or those who have come into contact with COVID-19 patients routinely take some protective measures. There was no clear evidence of vertical transmission, which is consistent with other research results (26).
This study found that the vast majority of neonates infected with the Omicron variant showed symptoms, which is inconsistent with previous studies suggesting that most neonates infected with COVID-19 were asymptomatic and had mild symptoms (6, 7). A total of 110 neonates were diagnosed with pneumonia, and no severe or critical cases were observed. However, it should be noted that the diagnosis of pneumonia in this study may have been too broad, and the clinical manifestations were not serious, so the prognosis was not significantly different from that of neonates infected with upper respiratory tract infection. Notably, according to the clinical manifestations, chest radiographs and CT reports, a considerable number of infected neonates were diagnosed with pneumonia, but their clinical manifestations were mild. There was no significant difference in treatment or length of stay between the two groups.
In this study, fever was the most common clinical manifestation of COVID-19 infection, which is similar to many past studies (5). This was followed by cough, shortness of breath, poor appetite, cough with nasal congestion or runny nose, and poor spirit. The clinical manifestations of symptomatic neonates were generally not severe, and the duration of symptoms was not long, which is consistent with the reports of most previous studies (4, 5). Due to the limited long-term follow-up of these studies, current evidence cannot be used to conclude that there is no harm to neonates following infection with COVID-19. In this study, a few newborns with underlying diseases (such as persistent pulmonary hypertension, neonatal pneumonia, and malnutrition in premature infants) developed clinically unexplained severe conditions after infection with COVID-19, which resulted in a prolonged duration of severe symptoms (such as long-term mechanical ventilation, noninvasive ventilator-assisted ventilation, and oxygen inhalation) and hospital stay, but no serious complications were found in other infected children. A limitation of this study is that the diagnosis of neonatal pneumonia may have a problem with scope. In this study, the diagnosis of pneumonia was mainly based on clinical symptoms such as shortness of breath and cough plus chest radiograph or CT results because the symptoms of neonatal pneumonia are not typical.
There has not been much research on the laboratory testing of neonates infected with COVID-19, and these neonates may have normal or reduced white blood cell counts, a decreased neutrophil count that can persist for several months and/or lymphocytopenia (27–30). Previous studies have shown that newborns infected with COVID-19 have normal or decreased white blood cell counts and decreased lymphocyte levels compared with uninfected newborns (5, 6, 31). In contrast to previous studies, this study investigated the blood test results of symptomatic and asymptomatic newborns infected with COVID-19. In this study, the white blood cell counts and neutrophil levels were significantly decreased in neonates infected with COVID-19, but they were basically within the normal range, and these results were not entirely consistent with those reported in previous studies (1, 2, 5, 6). However, as previously reported, there was a significant decrease in the levels of leukocytes, neutrophils, and lymphocytes in newborns infected with COVID-19 who exhibited symptoms compared to those who were asymptomatic (29). This study had a larger patient sample size, and our research indicates that symptomatic neonates infected with the Omicron variant experience a significant decrease in the levels of neutrophils and lymphocytes.
Studies have shown that the monocyte levels of newborns infected with COVID-19 are increased (12). The proliferation of monocytes in this study was a noteworthy feature. Monocytes, a subset of white blood cells, mainly originate from myeloid progenitor cells in bone marrow, exist in the bloodstream and can differentiate into macrophages and dendritic cells (DCS) in tissues. As a result of pathological conditions, including viral infection, monocytes are activated and recruited by inflammatory mediators, migrate into affected tissues, and recruit macrophages and DC-like phenotypes. To realize the effector function of proinflammatory and anti-inflammatory activity, antigen presentation and tissue remodelling occur (32). They play an important role in host defence and excessive inflammation (19). Study results are inconsistent regarding changes in the number of monocytes in the blood during coronavirus infection. In some studies, flow cytometry analysis of blood samples from COVID-19 patients showed no change in the number of monocytes; however, the monocytes were larger than normal, which was related to the inflammatory phenotype (20). There are also studies showing that the number of monocytes in the blood of COVID-19 patients is significantly reduced (33). In the study by Andonegui-Elguera et al., the number of monocytes in the blood was increased, and the numbers of other cells, including lymphocytes, neutrophils, natural killer (NK) cells, and T cells, decreased significantly (34). In this study, it was found that the absolute value and percentage of monocytes increased significantly after COVID-19 infection, suggesting that monocytes may play an important role in neonates infected with COVID-19. Although mononucleosis is a double-edged sword, it does not cause serious cytokine storms in neonatal cases, its clinical symptoms are relatively mild, and its short-term prognosis is good.
Other indicators, such as CRP and PCT, in infected neonates were within the normal range, which was consistent with the typical characteristics of viral infection. According to previous studies, after adult infection with COVID-19, TNF-α, interleukin and other indicators have significant changes, and even some severely infected individuals have excessive inflammation and cytokine storm phenomena (34). Cytokines were not detected in this study, so further research is needed.
In previous studies, the transmission of COVID-19 was mostly horizontal, but the possibility of vertical transmission cannot be ruled out (24, 35). Maternal vaccination is a very important measure to prevent neonatal infection (36). Additionally, if the mother or other family members are infected with COVID-19, they should take protective measures, such as wearing a mask, washing their hands, and ventilating the room. Current research shows that if mothers take appropriate preventive measures, it is safe to allow newborns to be in the same room as their mothers and receive breast milk care directly (26). The main limitations of this study are the lack of information on the vaccination status of pregnant women and evidence of vertical transmission (e.g., COVID-19 status of mothers during delivery, placental examination, umbilical cord blood PCR, etc.). The other limitation of this study was the insufficient data available on maternal vaccination. This missing information could possibly provide insight into whether vaccinated mothers offer protection to their newborns.
In conclusion, newborns with COVID-19 infection caused by the omicron variant may be asymptomatic or have mild symptoms with a short duration and have a good short-term prognosis. However, long-term follow-up on physical and neurological development is still needed.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethics Committee of Affiliated Foshan Women and Children Hospital, Southern Medical University (approval number: FSFY-MEC-2023-022). Written informed consent for participation was not provided by the participants’ legal guardians/next of kin because: This is retrospectively collected data study, and the datasets were fully anonymized prior to analysis. The need for consent was waived by the Academic Board of the Hospital.
Y-HD and JS designed this research and drafted the manuscript. CL, GY, WM, RH, ZW, DL, XZ, HL and LL collected the samples; JC provided help in the statistical analysis. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hong H, Wang Y, Chung H-T, Chen C-J. Clinical characteristics of novel coronavirus disease 2019 (COVID-19) in newborns, infants and children. Pediatr Neonatol. (2020) 61:131–2. doi: 10.1016/j.pedneo.2020.03.001
2. Wei M, Yuan J, Liu Y, Fu T, Yu X, Zhang Z-J. Novel coronavirus infection in hospitalized infants under 1 year of age in China. J Am Med Assoc. (2020) 323:1313. doi: 10.1001/jama.2020.2131
3. Gale C, Quigley MA, Placzek A, Knight M, Ladhani S, Draper ES, et al. Characteristics and outcomes of neonatal SARS-CoV-2 infection in the UK: a prospective national cohort study using active surveillance. Lancet Child Adolesc Health. (2021) 5:113–21. doi: 10.1016/S2352-4642(20)30342-4
4. Zimmermann P, Uka A, Buettcher M, Fougère Y, Plebani M, Relly C, et al. Neonates with SARS-CoV-2 infection: spectrum of disease from a prospective nationwide observational cohort study. Swiss Med Wkly. (2022) 152:w30185. doi: 10.4414/smw.2022.w30185
5. Cui X, Zhao Z, Zhang T, Guo W, Guo W, Zheng J, et al. A systematic review and meta-analysis of children with coronavirus disease 2019 (COVID-19). J Med Virol. (2021) 93:1057–69. doi: 10.1002/jmv.26398
6. Devin J, Marano R, Mikhael M, Feaster W, Sanger T, Ehwerhemuepha L. Epidemiology of neonatal COVID-19 in the United States. Pediatrics. (2022) 150:e2022056297. doi: 10.1542/peds.2022-056297
7. Barnes E, Van Groningen K, Ngo V, Nunez D, Mykhaylov N, Ryan A, et al. Clinical characteristics and outcomes of SARS-CoV-2 positive neonates born to persons with SARS-CoV-2 infection in pregnancy in Los Angeles county, California, May 22, 2020–February 22, 2021. Pediatr Infect Dis J. (2023) 42:418–22. doi: 10.1097/INF.0000000000003858
8. Akin IM, Kanburoglu MK, Tayman C, Oncel MY, Imdadoglu T, Dilek M, et al. Epidemiologic and clinical characteristics of neonates with late-onset COVID-19: 1-year data of Turkish neonatal society. Eur J Pediatr. (2022) 181:1933–42. doi: 10.1007/s00431-021-04358-8
9. Dávila-Aliaga C, Torres-Marcos E, Paucar-Zegarra R, Hinojosa-Pérez R, Espinoza-Vivas Y, Mendoza-Ibáñez E, et al. Clinical and epidemiological characterization in the follow-up of newborns with COVID-19: a descriptive study. Medwave. (2021) 21:e002141. doi: 10.5867/medwave.2021.11.002141
10. More K, Chawla D, Murki S, Tandur B, Deorari AK, Kumar P, et al. Outcomes of neonates born to mothers with coronavirus disease 2019 (COVID-19)—national neonatology forum (NNF) India COVID-19 registry. Indian Pediatr. (2021) 58:525–31. doi: 10.1007/s13312-021-2234-2
11. Leung C. The younger the milder clinical course of COVID-19: even in newborns? Pediatr Allergy Immunol. (2021) 32:358–62. doi: 10.1111/pai.13371
12. Spoulou V, Noni M, Koukou D, Kossyvakis A, Michos A. Clinical characteristics of COVID-19 in neonates and young infants. Eur J Pediatr. (2021) 180:3041–5. doi: 10.1007/s00431-021-04042-x
13. Palladino M. Complete blood count alterations in COVID-19 patients. Biochem Med. (2021) 31:403–15. doi: 10.11613/BM.2021.030501
14. Lucas F, Sadigh S. Hematopathology of severe acute respiratory syndrome coronavirus 2 infection and coronavirus disease-19. Surg Pathol Clin. (2023) 16:197–211. doi: 10.1016/j.path.2023.01.007
15. National Health Commission of the PRC. Guideline on diagnosis and treatment of novel coronavirus pneumonia (interim 9th edition). Infect Dis Inf. (2022) 35:97–106. doi: 10.3969/j.issn.1007-8134.2022.02.001
16. Working Group for the Prevention and Control of Neonatal SARS-CoV-2 Infection in the Perinatal Period of the Editorial Committee of Chinese Journal of Contemporary Pediatrics. Perinatal and neonatal management plan for prevention and control of SARS-CoV-2 infection (3rd edition). Zhongguo Dang Dai Er Ke Za Zhi. (2023) 25:1–4. doi: 10.7499/j.issn.1008-8830.2212074
17. Fierman AH. Foreword: neonatal intensive care unit preparedness for the novel coronavirus disease-2019 pandemic: a New York city hospital perspective. Curr Probl Pediatr Adolesc Health Care. (2020) 50:100801. doi: 10.1016/j.cppeds.2020.100801
18. Karim SSA, Karim QA. Omicron SARS-CoV-2 variant: a new chapter in the COVID-19 pandemic. Lancet. (2021) 398:2126–8. doi: 10.1016/S0140-6736(21)02758-6
19. Callaway E. Heavily mutated omicron variant puts scientists on alert. Nature. (2021) 600:21. doi: 10.1038/d41586-021-03552-w
20. Trevisanuto D, Cavallin F, Cavicchiolo ME, Borellini M, Calgaro S, Baraldi E. Coronavirus infection in neonates: a systematic review. Arch Dis Child Fetal Neonatal Ed. (2021) 106:330–5. doi: 10.1136/archdischild-2020-319837
21. Meo SA, Meo AS, Al-Jassir FF, Klonoff DC. Omicron SARS-CoV-2 new variant: global prevalence and biological and clinical characteristics. Eur Rev Med Pharmacol Sci. (2021) 25:8012–8. doi: 10.26355/eurrev_202112_27652
22. Cao Q, Chen Y-C, Chen C-L, Chiu C-H. SARS-CoV-2 infection in children: transmission dynamics and clinical characteristics. J Formos Med Assoc. (2020) 119:670–3. doi: 10.1016/j.jfma.2020.02.009
23. Li SJ, Zhang L, Yuan H, Zhang XB, Wang CQ, Liu GB, et al. Management and short-term outcomes of neonates born to mothers infected with SARS-CoV-2 omicron variant. Zhonghua Er Ke Za Zhi. (2022) 60:1163–7. doi: 10.3760/cma.j.cn112140-20220613-00545
24. Zhang K, Jiang SY, Yan K, Zhang P, Gao RW, Zhao J, et al. Clinical characteristics of 16 neonates infected with SARS-CoV-2 during omicron variant outbreak. Zhonghua Er Ke Za Zhi. (2022) 60:1158–62. doi: 10.3760/cma.j.cn112140-20220617-00561
25. Ambike DA, Haribhakta SV, Soni SP, Mundlod S, Sayyad R, Bijraniya K. Symptomatic neonatal SARS-CoV-2 infection in a tertiary care teaching hospital: an observational prospective study. Int J Contemp Pediatr. (2021) 8:1200. doi: 10.18203/2349-3291.ijcp20212472
26. Salvatore CM, Han J-Y, Acker KP, Tiwari P, Jin J, Brandler M, et al. Neonatal management and outcomes during the COVID-19 pandemic: an observation cohort study. Lancet Child Adolesc Health. (2020) 4:721–7. doi: 10.1016/S2352-4642(20)30235-2
27. Hu Z, Song C, Xu C, Jin G, Chen Y, Xu X, et al. Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China. Sci China Life Sci. (2020) 63:706–11. doi: 10.1007/s11427-020-1661-4
28. Zimmermann P, Curtis N. Coronavirus infections in children including COVID-19. Pediatr Infect Dis J. (2020) 39:355–68. doi: 10.1097/INF.0000000000002660
29. Scholz AS, Wallwiener S, Pöschl J, Kuss N. Case report: prolonged neutropenia in premature monoamniotic twins with SARS-CoV-2 infection acquired by vertical transmission. Front Pediatr. (2022) 10:877954. doi: 10.3389/fped.2022.877954
30. Sankaran D, Nakra N, Cheema R, Blumberg D, Lakshminrusimha S. Perinatal SARS-CoV-2 infection and neonatal COVID-19: a 2021 update. Neoreviews. (2021) 22(5):e284–95. doi: 10.1542/neo.22-5-e1001
31. García H, Allende-López A, Morales-Ruíz P, Miranda-Novales G, Villasis-Keever MÁ. COVID-19 in neonates with positive RT–PCR test. Systematic review. Arch Med Res. (2022) 53:252–62. doi: 10.1016/j.arcmed.2022.03.001
32. Developmental and functional heterogeneity of monocytes - PubMed. Available at: https://pubmed.ncbi.nlm.nih.gov/30332628/ (Accessed February 1, 2023).
33. Paliogiannis P, Zinellu A, Scano V, Mulas G, De Riu G, Pascale RM, et al. Laboratory test alterations in patients with COVID-19 and non COVID-19 interstitial pneumonia: a preliminary report. J Infect Dev Ctries. (2020) 14:685–90. doi: 10.3855/jidc.12879
34. olecular alterations prompted by SARS-CoV-2 infection: induction of hyaluronan, glycosaminoglycan and mucopolysaccharide metabolism - Pubmed. Available at: https://pubmed.ncbi.nlm.nih.gov/32611485/ (Accessed February 1, 2023).
35. Kulkarni R, Rajput U, Dawre R, Valvi C, Nagpal R, Magdum N, et al. Early-onset symptomatic neonatal COVID-19 infection with high probability of vertical transmission. Infection. (2021) 49:339–43. doi: 10.1007/s15010-020-01493-6
Keywords: neonates, coronavirus disease 2019, omicron wave, clinical features, routine blood tests
Citation: Dai Y-H, Li C, Yuan G, Mo W, Chen J, Huang R, Wan Z, Lin D, Zhong X, Li H, Liu L and Shi J (2023) A multicentre study on the clinical characteristics of newborns infected with coronavirus disease 2019 during the omicron wave. Front. Pediatr. 11:1192268. doi: 10.3389/fped.2023.1192268
Received: 23 March 2023; Accepted: 19 June 2023;
Published: 17 July 2023.
Edited by:
Balaji Govindaswami, Valley Medical Center Foundation, United StatesReviewed by:
Dongli Song, Santa Clara Valley Medical Center, United States© 2023 Dai, Li, Yuan, Mo, Chen, Huang, Wan, Lin, Zhong, Li, Liu and Shi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jipeng Shi amlwZW5nc2hpQDEyNi5jb20=
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.