
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Pediatr. , 17 April 2023
Sec. Neonatology
Volume 11 - 2023 | https://doi.org/10.3389/fped.2023.1172799
This article is part of the Research Topic Neonatal Sepsis: Current Insights and Challenges View all 11 articles
 Elisenda Moliner-Calderón1
Elisenda Moliner-Calderón1 Sergio Verd2,3*
Sergio Verd2,3* Alfonso Leiva4Gemma Ginovart5Pia Moll-McCarthy6Josep Figueras-Aloy7
Alfonso Leiva4Gemma Ginovart5Pia Moll-McCarthy6Josep Figueras-Aloy7
Background: Regarding neonatal hypotension, there is no certainty as to whether inotrope properties are beneficial or whether they may be harmful. However, given that the antioxidant content of human milk plays a compensatory role in neonatal sepsis and that human milk feeding has direct effects in modulating the cardiovascular function of sick neonates, this research hypothesized that human milk feeds might predict lower requirements of vasopressors in the management of neonatal septic shock.
Method: Between January 2002 and December 2017, all late preterm and full-term infants attending a neonatal intensive care unit, with clinical and laboratory findings of bacterial or viral sepsis, were identified in a retrospective study. During their first month of life, data on feeding type and early clinical characteristics were collected. A multivariable logistic regression model was constructed to determine the impact of human milk on the use of vasoactive drugs in septic newborns.
Results: 322 newborn infants were eligible to participate in this analysis. Exclusively formula-fed infants were more likely to be delivered via C-section, to have a lower birth weight and a lower 1-minute Apgar score than their counterparts. Human milk-fed newborns had 77% (adjusted OR = 0.231; 95% CI: 0.07–0.75) lower odds of receiving vasopressors than exclusively formula-fed newborns.
Conclusion: We report that any human milk feeding is associated with a decrease in the need for vasoactive medications in sepsis-affected newborns. This observation encourages us to undertake further research to determine whether human milk feeds mitigate the use of vasopressors in neonates with sepsis.
Recent research (1) that aimed to reduce the use of inotropes resulted in a reduction of brain morbidities in premature babies; these findings add to serious efforts to clarify whether cerebral perfusion is improved or reduced with any inotrope use. Unfortunately, despite decades of use, we still have little evidence regarding the outcome of the various inotropes accepted for treating neonatal hypotension. A limited number of observational studies have addressed the long-term effects of vasoactive drugs. However, recruiting sick neonates for randomized controlled trials when they are unstable and require prompt intervention is extremely challenging (2). Given this, it is wise of us to try and find more ways to narrow the use of agents that may be of no benefit or potentially have adverse consequences.
Although neonates generate a relatively lower amount of inflammatory cytokines than adults, neonates with septic shock have dysregulated cytokine production, which is linked to illness severity (3). Inflammatory pathways activated in septic shock directly impact the vascular tone and cardiac function. The release of inflammatory mediators can compromise endothelial wall integrity; subsequent endothelial leakage lowers circulating blood volume and, subsequently, cardiac preload (4, 5). Bacteremic neonates have been found to have higher levels of nitric oxide and endothelin compared to their non-infected counterparts. High levels of endothelin have been correlated with myocardial dysfunction in sepsis (6).
Remarkably, systemic inflammatory response and additional compromise to perfusion occur when anti-inflammatory mechanisms do not adequately counteract pro-inflammatory pathways. Antioxidant and anti-inflammatory defenses mature during late gestation (7). Thus, preterm neonates have diminished anti-inflammatory mechanisms at birth. On the other hand, the process leading to septic shock is maintained by a cascade of inflammatory mechanisms and simultaneous increased production of free radicals. Since human milk (HM) possesses a much more potent antioxidant potential than infant formula (8), it appears to serve as the primary antioxidant source for preterm or sick neonates. Although we have not found previous research on the link between HM feeding and an overall decline in the use of vasoactive medications, the antioxidant role of HM and the critical role that oxidative stress plays in worsening the hemodynamic presentation of neonatal sepsis generate the hypothesis that HM feeding might predict lower requirements of vasopressors in the management of neonatal septic shock.
In this regard, we have analyzed the link between HM feeding and the use of vasopressors in a long-term cohort of newborn infants with sepsis admitted to our neonatal unit.
This is a secondary analysis of data collected for a doctoral thesis intended to explore the clinical and laboratory characteristics of neonates with viral or bacterial sepsis (9). Previous research contains complete details of the methodological processes (10). In brief, this study was carried out using a retrospective review of electronic medical records of late preterm and full-term newborn infants.
Between January 2002 and December 2017, all late preterm and full-term infants up to 28 days of age with clinical and laboratory findings of bacterial or viral sepsis were identified in a cohort study. All of them attended the neonatal intensive care unit (NICU) of Sant Pau Hospital, a tertiary referral unit in Barcelona, Spain, with approximately 350 admissions per year and a bed occupancy rate of 90%; the unit consists of 10 intensive care and 7 high-care beds.
The NICU's computerized system provided retrospective data on maternal parity and gravida, maternal diseases, infant demographic and perinatal characteristics, feeding type, and early clinical features. In addition, data on any HM or exclusive formula feeding (EF) were collected during the first month of life. All HM was mother's own milk; donor's milk is reserved for very premature infants. Fresh or frozen mother's own milk was used. These infants were not admitted to the NICU from home but from the Maternity unit. We chose to focus on the first month of life because it significantly impacts short-term outcomes. For exploratory analyses, we examined the use of antihypotensive treatments until hospital discharge.
The primary outcome of this study was to examine the use of vasopressors in newborn infants with a history of sepsis, intending to evaluate if exclusive formula feeding predicts vasopressor support practices. In this preliminary analysis, infant feeding type was an independent variable, and vasopressor support was a dependent variable.
Secondary outcomes included the following clinical characteristics based on feeding type. Neonatal status at birth, metabolic and/or respiratory acidosis, hypotension, abnormal neurological examination, abnormal brain scan, meningitis, positive blood cultures, blood cells count, type of respiratory support, discharge weight, and days spent in the hospital. The clinical information from birth until Hospital discharge has been gathered in a database, but a detail of the timing of each clinical characteristic was not available.
We used descriptive statistics to generate counts and percentages for the mode of feeding among newborn infants in the registry. Fisher's Exact or t-tests were used to compare infant and maternal characteristics or outcomes; p-values were obtained from bivariate comparisons as a function of each individual risk factor. A multivariable logistic regression model was constructed to determine the impact of milk type on the primary outcome and the independent contribution of each factor to neonatal outcomes. This model included variables associated with exposure or variables highly predictive of the primary outcomes. Backward selection was used to remove these covariables from the multivariable logistic regression model if they no longer had significance when added to the model. Because of collinearity, heart failure was not included in the adjusted model. Outcomes were compared between the HM and EF groups with odds ratios calculated with logistic regression fit by generalized estimating equations to account for paired data. There were no methods used to account for any potential bias. The SPSS software version 21.0 (SPSS Chicago, IL, United States) was used for statistical analysis and data management.
The Santa Creu & Sant Pau University Hospital's Clinical Studies Ethics Committee approved this study on December 20, 2020, with decision number: IIBSP-ENT-2020-152.
Because the study was conducted retrospectively over a two-decade period, and the data was scanned from patient files, no informed consent was obtained.
During the study period (2002–2017), 4,210 neonates were admitted to the participating NICU, 7.6% (n = 322; 260 in HM group and 62 in EF group) of whom met inclusion criteria and were eligible to participate in the final analysis. Similar to what was published in an earlier study of these cohorts examining the relationship between type of feeding and type of respiratory support (10), baseline characteristics of neonates who received any amount of HM and neonates who received only formula are summarized in Table 1. The mean age of newborns on admission to the neonatal unit was 4.3 days in cases of bacterial sepsis and 12.9 days in cases of viral sepsis, and 20% of infants with bacterial sepsis required vasoactive support compared to 2% of infants with viral sepsis. EF infants were more likely to be delivered via C-section, had a lower birth weight, and had a lower 1 min Apgar score than HM infants. However, these relationships did not persist when introduced in the multivariate model. We found no other background differences in bivariate analysis.
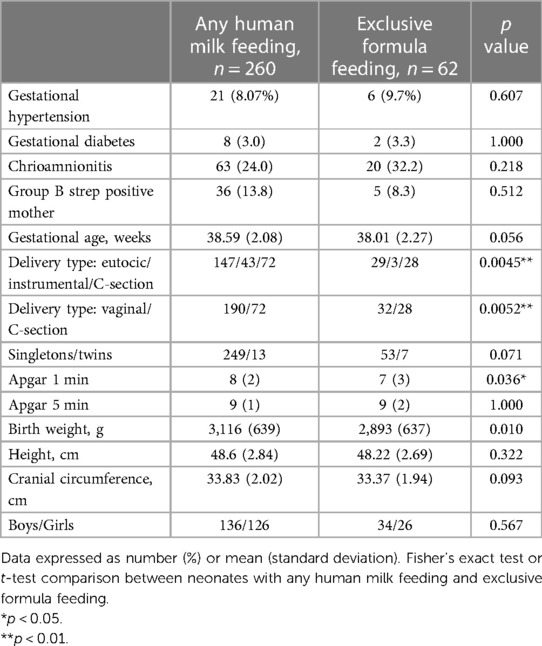
Table 1. Patents’ characterstics.
Table 2 compares short-term neonatal outcomes by feeding method. On bivariate analysis, there was a higher proportion of hipotonia among EF infants than among HM infants (54% vs. 23%, p = 0.045); and the proportion of respiratory distress was higher among EF infants than among HM infants (56% vs. 39%, p = 0.020). As a result, the same applied to the proportion of infants needing some form of respiratory support (43% vs. 27%, p = 0.019). On the other hand, the neutrophil blood count was higher among EF infants than among HM infants (10,358/µl vs. 7,623/µl, p = 0.005). Interestingly, 22% of EF infants had confirmed viral or bacterial meningitis vs. 42% of HM infants (p = 0.038). Finally, 8.7% of HM neonates required vasopressor support, compared to 25% of EF neonates (OR = 0.28; 95% CI: 0.14–0.59; p < 0.001). Other short-term neonatal outcomes did not differ between the two groups.
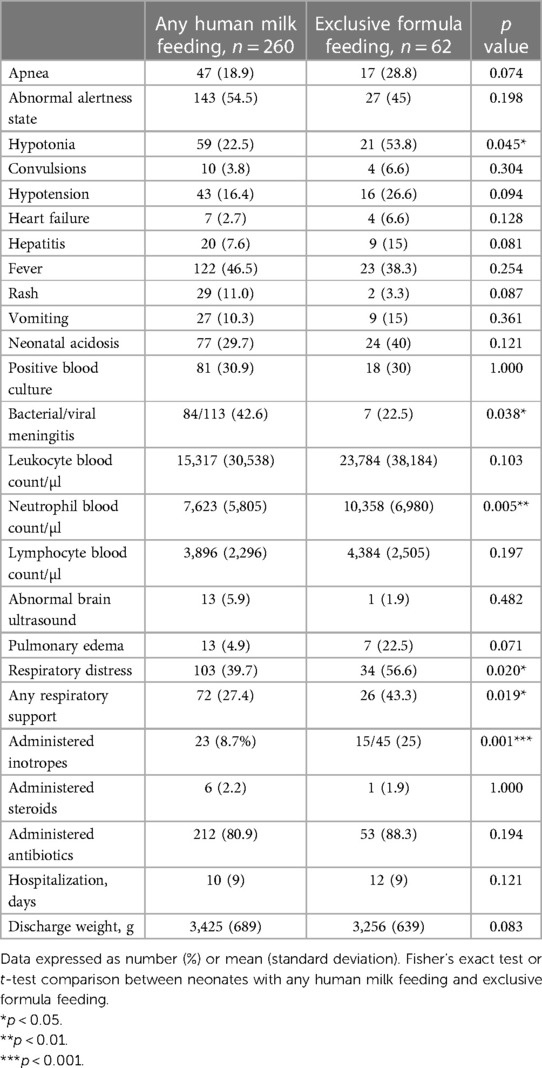
Table 2. Clinical or laboratory outcomes by feeding type.
Logistic regression models were developed to examine the association between the use of vasopressors and feeding type. Meningitis, lower muscle tone, C-section, or postnatal steroids treatment were covariates that remained significant in the final model (Table 3). However, even when controlling for these covariates, HM newborns had 77% (adjusted OR = 0.231; 95% CI: 0.07–0.75) lower odds of receiving vasopressors than EF newborns.
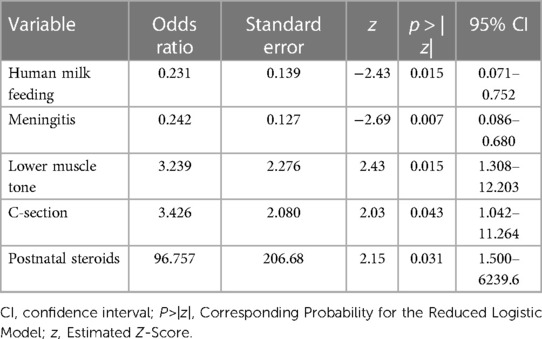
Table 3. Multivariate logistic regression analysis of factors associated with higher vasopressor support.
We found that any HM is linked to much better cardiovascular outcomes than EF. Data on exclusive HM feeding are not available in this study. However, the protecting role of any HM is supported by systematic reviews, which show that a minimum intake of 7 ml/kg/day of HM during the first 42 days is linked to a lower incidence of bronchopulmonary dyspasia and that there is conflicting evidence regarding the impact of high vs. low doses of HM on both this condition or retinopathy of prematurity (11).
This retrospective study at the level of a single NICU has explored the link between early feeding type and the administration of vasopressors. Following our initial hypothesis, after adjusting for confounding by indication, infants in the EF groups received vasopressor treatment more frequently than the HM group. As far as we know, this is the pioneer descriptive study in this field. In addition, this analysis included a large number of newborn infants and used multivariable statistical methods, which contributed to the findings' external validity.
We also found a positive association between any HM feeding and the rate of meningitis, a negative association between any HM feeding and hypotonia, and neutrophil counts were significantly higher in EF neonates than in HM neonates. We do not have an explanation for our results on meningitis. We also found a positive association between any HM feeding and the rate of meningitis, a negative association between any HM feeding and hypotonia, and neutrophil counts were significantly higher in EF neonates than in HM neonates. We do not have an explanation for our results on meningitis. Concerning hypotonia, no evidence that proves a direct link between lack of breastfeeding and low muscle neonatal tone but scattered data from different sources show that many neural outcomes are facilitated by HM feeding (12). On the one side, it has been reported that a high proportion of floppy infants also show shallow measurements of muscle strength (13, 14), and systematic reviews confirm the positive association between breastfeeding and body strength or balance beyond infancy (15, 16). In particular, in the long-term, adolescents who were breastfed build stronger muscles than those who were not breastfed (17). In the medium-term or short-term, there is substantial evidence of the positive impact of breastfeeding on masseter muscle function among toddlers or infants (18, 19). The combination of the negative correlation between hypotonia and muscle strength and the positive correlation between the history of breastfeeding and subsequent muscle strength may suggest some degree of correlation between lack of HM feeding and neonatal hypotonia.
Regarding our findings on neutrophil counts, we can refer to the well-known link between reactive oxygen species and high neutrophil-to-lymphocyte ratios. This association has been seen in critically ill patients, which is accompanied by a cascade of events that leads to tissue damage and increases the severity of the condition (20). In this field of study, we report no differences between the two groups of infants for the rest of the leukocytes.
While low arterial blood pressure of neonates with sepsis is linked to an increased risk of adverse outcomes (21), treating neonatal hypotension using vasopressors remains controversial (22–24). Hence, there is a consensus to promote a thorough examination of the pathophysiological mechanisms underlying low systemic perfusion to help clinicians decide which treatment strategy to use (25).
Preterm infants have myocardial dysfunction as well as immature vasculature (26). We are still learning HM feeding can have cardioprotective effects on sick neonates. The mechanism by which HM may reverse those cardiovascular changes is one of the crucial elements that is still absent. Our study may add to robust data on the benefits of HM exposure for the cardiovascular morphology of the high-risk newborn and is also consistent with findings on oxidative stress-related diseases in newborns.
The link between HM feeds and enhanced brain or lung development among high-risk neonates (27, 28) has prompted a renewed interest in optimal feeding to improve the cardiovascular health of such neonates. Preterm infants with higher exposure to HM show enhanced cardiovascular performance by age one year (29) and a more favorable cardiac structure during adolescence and adulthood (30, 31). Our study provides further evidence of the beneficial association between early HM feeding and cardiovascular function across the neonatal developmental stage of sick neonates, which is characterized by systolic and diastolic dysfunction coupled with maladaptive vasculature (32, 33).
The massive release of pro-inflammatory molecules noted among newborn infants with bloodstream infection leads to systemic inflammatory reaction (34) in organs distant from the initial insult, involves the endothelial cells, and affects the vascular tone (3, 4, 35). Ideally, this inflammatory response is followed by a compensatory anti-oxidative response, which represents the biological attempt to prevent inflammation from becoming the dominant reaction and leading to multiorgan dysfunction (5, 36).
An increased oxidized to reduced glutathione (GSSG/GSH) ratio in blood is considered a sign of oxidative stress (37). GSSG/GSH ratios are significantly higher in each phase of septic shock in infants or children; they spike during the overspill inflammatory state and then level off (38). Accordingly, significantly higher levels of GSSG are found among critically ill infants than among matched controls. On the other hand, premature birth removes the fetus from the protected, hypoxic intrauterine milieu. It exposes the sick preterm infant to free radical injury from using high-inspired oxygen fractions or inhaled nitric oxide or from reactive oxidative species produced by septic shock (39).
Furthermore, the lack of transfer of antioxidants across the placenta during the last stages of pregnancy, coupled with their weakened capacity to synthesize antioxidant defenses, renders such infants more vulnerable to oxidative stress. As expected, it has been confirmed that preterm newborns have lower plasma GSH than full-term newborns (40). Thus, the only compensatory mechanism for the sick neonate to cope with these compromised or incomplete antioxidant systems is the free radicals scavenging ability provided by HM (41).
Studies on adults over the past two decades report that the introduction of enteral nutrition, even if the patient requires continued inotropic support, improves both cardiac index and splanchnic blood flow while restores the gastrointestinal dysfunction and reduces hospital mortality rate, which is more visible in patients treated with multiple inotropes (42–44). In respect of Pediatric Intensive Care Units, when early enteral feeding was started in critically ill children with heterogeneous diagnoses, retrospective investigations showed a decreased length of stay in the unit, decreased mortality, and reduced use of inotropes (45, 46). Consistently, the consensus is that inotropes are not a contraindication in carefully monitored early enteral feeding of unstable adults (47). Recent pediatric sepsis guidelines encourage the start of early enteral nutrition based on the child's clinical situation, given that the scant literature on the subject suggests that it is both safe and beneficial (48).
Attention should be drawn to the lack of clinical trials on early enteral feeding of neonates on inotropes. To our knowledge, only a recent randomized trial has addressed this topic. Rao et al. (49) conducted a study on 200 late preterm infants on inotropes randomly assigned to an enteral feed study group or an intravenous (IV) fluid group (one hundred each). After the infant had stable circulation for 6 h, the enteral feed group began feeding with expressed breast milk. The feeding guidelines were individualized based on the infant's clinical status, and there was no increase in the initial volume for at least 24 h. When babies were fed 80 ml/kg/day, feeding intervals of 4 h were replaced with 2 h intervals. From 100 to 160 ml/kg/day, feed volumes were advanced at less than 30 ml/kg/day. Neonates in the IV fluid group were not given any feed. All neonates in enteral feed group were expressed breast milk-fed and were closely monitored until death or discharge. Mortality in the IV fluid group was significantly higher than in the enteral group (30.4% vs. 11.7%, respectively; p = 0.002), and the mean duration of hospital stay was longer in the IV fluid group (15.5 days vs. 13.4 days in the enteral feed group; p = 0.013). As a result, the authors conclude that neonates can tolerate enteral feed up to dopamine 10 mcg/kg/min and dobutamine 7.5 mcg/kg/min. The practical advice is that enteral feed can be safely administered to neonates on inotropes.
According to currently limited evidence on unstable neonates, some neonatal guidelines favor withholding feeds for babies on inotropes (50), while others prefer to continue enteral feeds even if inotropic support occurs (51). Concerning clinical practice, a survey of 60 Spanish NICUs unveils that 100% delay enteral feeding when there is a hemodynamic failure (52). Considering that we analyzed data from a purely observational cohort, our findings do not allow at this stage to suggest different approaches to minimize inotrope treatments with uncertain cognitive outcomes (53). However, this study contributes evidence on the potential role of very early HM feeding in improving the quality of care of newborn infants with signs of shock and might boost further research on the most effective feeding practices for this group of neonates.
Our study has several limitations. First, we acknowledge that data collection on HM needs to be more specific regarding the vast variability of what this could constitute over the first weeks of life. However, the association between breastfeeding and short- or long-term health outcomes has received considerable scrutiny. A number of studies have suggested that ever vs. never HM feeding may be associated with a decreased risk of mother's carcinoma (54), cardiovascular health in schoolchildren (55), or retinopathy of prematurity among neonates (56), even after adjustment for potential confounders. Second, our study was limited because we did not include feeding duration in our definition of HM feeding. From a methods perspective, we had no information on the feeds in temporal relation to the treatment decision. Previous studies have shown that the rate of breastfeeding initiation may be the same for infants admitted to the well-newborn nursery and the NICU and also that early cessation of breastfeeding is due to the newborn's sickness in less than 5% of cases (57). Hence, other authors have pointed to links between feeding type and neonatal conditions that are rare during the first week of life, based on data similar to ours, despite the lack of detailed information on the periods in which their patients were fed HM (56).
Third, we also had no information on the number of doses and the timeline of any vasopressor treatment. Moreover, the questionnaire did not collect the name of the vasopressor used. The reasons for prescribing vasopressors were also missing, although probably was due to hypotension. Fourth, the study reflects practices from a long time, which might have changed a decade later. Fifth, as this is a descriptive study, residual confounding may not have been identified. Sixth, we did not account for social characteristics that could impact the outcomes. Seventh, if further clinical, laboratory, or ultrasound data could be examined, our results would have been conclusive, but we must admit that hypotension was the only sign of compromised cardiovascular function that was collected.
Our results show that any HM feeding is associated with a decrease in the need for vasoactive medications in sepsis-affected newborns. This observation suggests that the antioxidant system that is part of HM may protect against inflammatory pathways that impact the vascular tone in sepsis and encourages further research to determine whether HM feeds directly affect neonatal cardiovascular maturation patterns.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by IIBSP-ENT-2020-152. Written informed consent for participation was not provided by the participants’ legal guardians/next of kin: Because the study was conducted retrospectively over a two-decade period, and the data was scanned from patient files, no informed consent form was obtained.
EM and SV had full access to all the data in the study and take responsibility for the integrity of the data. Study concept and design: JF and SV. Acquisition, analysis, or interpretation of data: JF and AL. Literature review and drafting of the manuscript: EM, GG and PM. All authors contributed to the article and approved the submitted version.
The authors acknowledge all the parents and infants for their participation. Further, the authors are grateful to the staff of Sant Pau NICU Hospital for excellent cooperation. We also appreciate the skilled voluntary help from staff of the Balearic Medical Library Bibliosalut.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
EF, exclusive formula feeding; GSH, reduced glutathione; GSSG, oxidized glutathione; HM, any human milk feeding; IV, intravenous; NICU, Neonatal Intensive Care Unit.
1. Gurram Venkata SKR, Srivastava A, Murthy P, et al. Hemodynamic quality improvement bundle to reduce the use of inotropes in extreme preterm neonates. Paediatr Drugs. (2022) 24(3):259–67. doi: 10.1007/s40272-022-00502-5
2. Dempsey EM. Under pressure to treat? Arch Dis Child Fetal Neonatal Ed. (2015) 100(5):F380–1. doi: 10.1136/archdischild-2015-308667
3. Kurul Ş, Simons SHP, Ramakers CRB, De Rijke YB, Kornelisse RF, Reiss IKM, et al. Association of inflammatory biomarkers with subsequent clinical course in suspected late onset sepsis in preterm neonates. Crit Care. (2021) 25(1):12. doi: 10.1186/s13054-020-03423-2
4. Kharrat A, Jain A. Hemodynamic dysfunction in neonatal sepsis. Pediatr Res. (2022) 91(2):413–24. doi: 10.1038/s41390-021-01855-2
5. Noori S, Seri I. Pathophysiology of newborn hypotension outside the transitional period. Early Hum Dev. (2005) 81(5):399–404. doi: 10.1016/j.earlhumdev.2005.03.007
6. Goto T, Hussein MH, Kato S, Daoud GA, Kato T, Kakita H, et al. Endothelin receptor antagonist attenuates inflammatory response and prolongs the survival time in a neonatal sepsis model. Intensive Care Med. (2010) 36(12):2132–9. doi: 10.1007/s00134-010-2040-0
7. Shoji H, Koletzko B. Oxidative stress and antioxidant protection in the perinatal period. Curr Opin Clin Nutr Metab Care. (2007) 10(3):324–8. doi: 10.1097/MCO.0b013e3280a94f6d
8. Hanson C, Lyden E, Furtado J, Van Ormer M, Anderson-Berry A. A comparison of nutritional antioxidant content in breast milk, donor milk, and infant formulas. Nutrients. (2016) 8(11):681. doi: 10.3390/nu8110681
9. Moliner-Calderón E. Major role of enteroviral infection in neonates [Ph.D. Thesis]. Barcelona: Universidad Autónoma (2021). Available at: https://www.tdx.cat/bitstream/handle/10803/673836/emc1de1.pdf?sequence=1&isAllowed=y (Accessed January 2, 2023).
10. Moliner-Calderón E, Verd S, Leiva A, Ponce-Taylor J, Ginovart G, Moll-McCarthy P, et al. Human milk feeding for septic newborn infants might minimize their exposure to ventilation therapy. Children (Basel). (2022) 9(10):1450. doi: 10.3390/children9101450
11. Miller J, Tonkin E, Damarell RA, et al. A systematic review and meta-analysis of human milk feeding and morbidity in very low birth weight infants. Nutrients. (2018) 10(6):707. doi: 10.3390/nu10060707
12. Krol KM, Rajhans P, Missana M, Grossmann T. Duration of exclusive breastfeeding is associated with differences in infants’ brain responses to emotional body expressions. Front Behav Neurosci. (2015) 8:459. doi: 10.3389/fnbeh.2014.00459
13. Capodaglio P, Vismara L, Menegoni F, Baccalaro G, Galli M, Grugni G. Strength characterization of knee flexor and extensor muscles in prader-willi and obese patients. BMC Musculoskelet Disord. (2009) 10:47. doi: 10.1186/1471-2474-10-47
14. Heshmati J, Sepidarkish M, Shidfar F, et al. Effect of breastfeeding in early life on cardiorespiratory and physical fitness: a systematic review and meta-analysis. Breastfeed Med. (2018) 13(4):248–58. doi: 10.1089/bfm.2018.0001
15. Berlanga-Macías C, Álvarez-Bueno C, Martínez-Hortelano JA, Garrido-Miguel M, Pozuelo-Carrascosa DP, Martínez-Vizcaíno V. Relationship between exclusive breastfeeding and cardiorespiratory fitness in children and adolescents: a meta-analysis. Scand J Med Sci Sports. (2020) 30(5):828–36. doi: 10.1111/sms.13622
16. Zaqout M, Michels N, Ahrens W, Börnhorst C, Molnár D, Moreno LA, et al. Associations between exclusive breastfeeding and physical fitness during childhood. Eur J Nutr. (2018) 57(2):545–55. doi: 10.1007/s00394-016-1337-3
17. Artero EG, Ortega FB, España-Romero V, et al. Longer breastfeeding is associated with increased lower body explosive strength during adolescence. J Nutr. (2010) 140(11):1989–95. doi: 10.3945/jn.110.123596
18. Pires SC, Giugliani ER, Caramez da Silva F. Influence of the duration of breastfeeding on quality of muscle function during mastication in preschoolers: a cohort study. BMC Public Health. (2012) 12(1):934. doi: 10.1186/1471-2458-12-934
19. França EC, Sousa CB, Aragão LC, Costa LR. Electromyographic analysis of masseter muscle in newborns during suction in breast, bottle or cup feeding. BMC Pregnancy Childbirth. (2014) 14:154. doi: 10.1186/1471-2393-14-154
20. Laforge M, Elbim C, Frère C, Hémadi M, Massaad C, Nuss P, et al. Tissue damage from neutrophil-induced oxidative stress in COVID-19. Nat Rev Immunol. (2020) 20(9):515–6. doi: 10.1038/s41577-020-0407-1
21. Faust K, Hartel C, Preuss M, Rabe H, Roll C, Emeis M, et al. Short-term outcome of very-low-birthweight infants with arterial hypotension in the first 24 h of life. Arch Dis Child Fetal Neonatal Ed. (2015) 100:F388–92. doi: 10.1136/archdischild-2014-306483
22. Batton B, Li L, Newman NS, Das A, Watterberg KL, Yoder BA, et al. Use of antihypotensive therapies in extremely preterm infants. Pediatrics. (2013) 131:e1865–73. doi: 10.1542/peds.2012-2779
23. Dempsey EM, Al Hazzani F, Barrington KJ. Permissive hypotension in the extremely low birthweight infant with signs of good perfusion. Arch Dis Child Fetal Neonatal Ed. (2009) 94:F241–4. doi: 10.1136/adc.2007.124263
24. Durrmeyer X, Marchand-Martin L, Porcher R, Gascoin G, Roze JC, Storme L, et al. Abstention or intervention for isolated hypotension in the first 3 days of life in extremely preterm infants: association with short-term outcomes in the EPIPAGE 2 cohort study. Arch Dis Child Fetal Neonatal Ed. (2017) 102:490–6. doi: 10.1136/archdischild-2016-312104
25. Singh Y, Tissot C, Fraga MV, Yousef N, Cortes RG, Lopez J, et al. International evidence-based guidelines on point of care ultrasound (POCUS) for critically ill neonates and children issued by the POCUS working group of the European society of paediatric and neonatal intensive care (ESPNIC). Crit Care. (2020) 24:65. doi: 10.1186/s13054-020-2787-9
26. Telles F, McNamara N, Nanayakkara S, et al. Changes in the preterm heart from birth to young adulthood: a meta-analysis. Pediatrics. (2020) 146(2):e20200146. doi: 10.1542/peds.2020-0146
27. Vasu V, Durighel G, Thomas EL, et al. Preterm nutritional intake and MRI phenotype at term age: a prospective observational study. BMJ Open. (2014) 4(5):e005390. doi: 10.1136/bmjopen-2014-005390
28. Ogbuanu IU, Karmaus W, Arshad SH, Kurukulaaratchy RJ, Ewart S. Effect of breastfeeding duration on lung function at age 10 years: a prospective birth cohort study. Thorax. (2009) 64(1):62–6. doi: 10.1136/thx.2008.101543
29. El-Khuffash A, Lewandowski AJ, Jain A, Hamvas A, Singh GK, Levy PT. Cardiac performance in the first year of age among preterm infants fed maternal breast milk. JAMA Netw Open. (2021) 4(8):e2121206. doi: 10.1001/jamanetworkopen.2021.21206
30. Singhal A, Cole TJ, Lucas A. Early nutrition in preterm infants and later blood pressure: two cohorts after randomised trials. Lancet. (2001) 357(9254):413–9. doi: 10.1016/S0140-6736(00)04004-6
31. Lewandowski AJ, Lamata P, Francis JM, et al. Breast milk consumption in preterm neonates and cardiac shape in adulthood. Pediatrics. (2016) 138(1):e20160050. doi: 10.1542/peds.2016-0050
32. Levy PT, Patel MD, Choudhry S, Hamvas A, Singh GK. Evidence of echocardiographic markers of pulmonary vascular disease in asymptomatic infants born preterm at one year of age. J Pediatr. (2018) 197:48–56.e2. doi: 10.1016/j.jpeds.2018.02.006
33. Levy PT, El-Khuffash A, Patel MD, et al. Maturational patterns of systolic ventricular deformation mechanics by two-dimensional speckle tracking echocardiography in preterm infants over the first year of age. J Am Soc Echocardiogr. (2017) 30(7):685–698.e1. doi: 10.1016/j.echo.2017.03.003
34. Oikonomakou MZ, Gkentzi D, Gogos C, Akinosoglou K. Biomarkers in pediatric sepsis: a review of recent literature. Biomark Med. (2020) 14(10):895–917. doi: 10.2217/bmm-2020-0016
35. Paulus P, Jennewein C, Zacharowski K. Biomarkers of endothelial dysfunction: can they help us deciphering systemic inflammation and sepsis? Biomarkers. (2011) 16(Suppl 1):S11–21. doi: 10.3109/1354750X.2011.587893
36. Bone RC. Toward a theory regarding the pathogenesis of the systemic inflammatory response syndrome: what we do and do not know about cytokine regulation. Crit Care Med. (1996) 24(1):163–72. doi: 10.1097/00003246-199601000-00026
37. Zitka O, Skalickova S, Gumulec J, et al. Redox status expressed as GSH:gSSG ratio as a marker for oxidative stress in paediatric tumour patients. Oncol Lett. (2012) 4(6):1247–53. doi: 10.3892/ol.2012.931
38. Németh I, Boda D. Xanthine oxidase activity and blood glutathione redox ratio in infants and children with septic shock syndrome. Intensive Care Med. (2001) 27(1):216–21. doi: 10.1007/s001340000791
39. Chen Y, Fantuzzi G, Schoeny M, Meier P, Patel AL. High-Dose human milk feedings decrease oxidative stress in premature infant. JPEN J Parenter Enteral Nutr. (2019) 43(1):126–32. doi: 10.1002/jpen.1178
40. Jain A, Mehta T, Auld PA, et al. Glutathione metabolism in newborns: evidence for glutathione deficiency in plasma, bronchoalveolar lavage fluid, and lymphocytes in prematures. Pediatr Pulmonol. (1995) 20(3):160–6. doi: 10.1002/ppul.1950200306
41. Friel JK, Martin SM, Langdon M, Herzberg GR, Buettner GR. Milk from mothers of both premature and full-term infants provides better antioxidant protection than does infant formula. Pediatr Res. (2002) 51(5):612–8. doi: 10.1203/00006450-200205000-00012
42. Revelly JP, Tappy L, Berger MM, Gersbach P, Cayeux C, Chioléro R. Early metabolic and splanchnic responses to enteral nutrition in postoperative cardiac surgery patients with circulatory compromise. Intensive Care Med. (2001) 27(3):540–7. doi: 10.1007/s001340100855
43. Khalid I, Doshi P, DiGiovine B. Early enteral nutrition and outcomes of critically ill patients treated with vasopressors and mechanical ventilation. Am J Crit Care. (2010) 19(6):488. doi: 10.4037/ajcc2010197
44. Mancl EE, Muzevich KM. Tolerability and safety of enteral nutrition in critically ill patients receiving intravenous vasopressor therapy. JPEN J Parenter Enteral Nutr. (2013) 37(5):641–51. doi: 10.1177/0148607112470460
45. Meinert E, Bell MJ, Buttram S, et al. Initiating nutritional support before 72 hours is associated with favorable outcome after severe traumatic brain injury in children: a secondary analysis of a randomized, controlled trial of therapeutic hypothermia. Pediatr Crit Care Med. (2018) 19(4):345–52. doi: 10.1097/PCC.0000000000001471
46. Greathouse KC, Sakellaris KT, Tumin D, et al. Impact of early initiation of enteral nutrition on survival during pediatric extracorporeal membrane oxygenation. JPEN J Parenter Enteral Nutr. (2018) 42(1):205–11. doi: 10.1002/jpen.1032
47. Yang S, Wu X, Yu W, Li J. Early enteral nutrition in critically ill patients with hemodynamic instability: an evidence-based review and practical advice. Nutr Clin Pract. (2014) 29(1):90–6. doi: 10.1177/0884533613516167
48. Tume LN, Valla FV, Joosten K, et al. Nutritional support for children during critical illness: european society of pediatric and neonatal intensive care (ESPNIC) metabolism, endocrine and nutrition section position statement and clinical recommendations. Intensive Care Med. (2020) 46(3):411–25. doi: 10.1007/s00134-019-05922-5
49. Rao YK, Saxena R, Midha T, Rao N, Saxena V. Clinical outcome of enteral nutrition versus IV fluids in newborns on inotropes: a randomized study. J Clin Neonatol. (2020) 9:261–5. doi: 10.4103/jcn.JCN_48_20
50. Neonatology coordinating group. Neonatology guidelines. Enteral Feeding Initiation and Progression. Government of Western Australia (2021). Available at: https://www.cahs.health.wa.gov.au/-/media/HSPs/CAHS/Documents/Health-Professionals/Neonatology-guidelines/Enteral-Feeding-Initiation-and-Progression.pdf (Accessed January 11, 2023).
51. Enteral Feeding and Nutrition for the Preterm and High Risk Neonate Winnipeg Health Authority (2020). Available at: https://professionals.wrha.mb.ca/old/extranet/eipt/files/EIPT-035-031.pdf (Accessed January 11, 2023).
52. Moreno Algarra MC, Fernández Romero V, Sánchez Tamayo T, Espinosa Fernández MG, Salguero García E; Red SEN-1500. Variability in enteral feeding practices of preterm infants among hospitals in the SEN1500 spanish neonatal network. An Pediatr (Barc). (2017) 87(5):245–52. doi: 10.1016/j.anpedi.2016.09.009
53. Doucette SM, Kelly EN, Church PT, Lee S, Shah V; Canadian Neonatal Network (CNN) Investigators and CNFUN Investigators and Steering Committee. Association of inotrope use with neurodevelopmental outcomes in infants <29 weeks gestation: a retrospective cohort study. J Matern Fetal Neonatal Med. (2022) 35(25):6044–52. doi: 10.1080/14767058.2021.1904872
54. Chowdhury R, Sinha B, Sankar MJ, et al. Breastfeeding and maternal health outcomes: a systematic review and meta-analysis. Acta Paediatr. (2015) 104(467):96–113. doi: 10.1111/apa.13102
55. Martin RM, Ness AR, Gunnell D, Emmett P, Davey Smith G; ALSPAC Study Team. Does breast-feeding in infancy lower blood pressure in childhood? The avon longitudinal study of parents and children (ALSPAC). Circulation. (2004) 109(10):1259–66. doi: 10.1161/01.CIR.0000118468.76447.CE
56. Hylander MA, Strobino DM, Pezzullo JC, Dhanireddy R. Association of human milk feedings with a reduction in retinopathy of prematurity among very low birthweight infants. J Perinatol. (2001) 21(6):356–62. doi: 10.1038/sj.jp.7210548
Keywords: neonate, premature infant, breast-feeding, human milk, sepsis, hypotension, oxidative stress, dopamine
Citation: Moliner-Calderón E, Verd S, Leiva A, Ginovart G, Moll-McCarthy P and Figueras-Aloy J (2023) The role of human milk feeds on inotrope use in newborn infants with sepsis. Front. Pediatr. 11:1172799. doi: 10.3389/fped.2023.1172799
Received: 23 February 2023; Accepted: 16 March 2023;
Published: 17 April 2023.
Edited by:
Rozeta Sokou, Nikaia General Hospital “Aghios Panteleimon”, GreeceReviewed by:
Andreas G. Tsantes, National and Kapodistrian University of Athens, Greece© 2023 Moliner-Calderón, Verd, Leiva, Ginovart, Moll-McCarthy and Figueras-Aloy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sergio Verd ZHJzdmVyZEBnbWFpbC5jb20=
Specialty Section: This article was submitted to Neonatology, a section of the journal Frontiers in Pediatrics
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.